patient safety and experience receive questions from the public in ... patient safety and experience...
TRANSCRIPT

1
Meeting Title
East Leicestershire and Rutland Clinical Commissioning Group – Governing Body
Date Tuesday 9 September 2014
Meeting no. 16. Time 12:30pm – 3:30pm
Chair Mr Graham Martin Venue /
Location PERA Innovation Park, Melton Mowbray, Leicestershire, LE13 OPB
AGENDA ITEM ACTION PRESENTER PAPER TIMING
B/14/156 Welcome and Introductions
Graham Martin 12:30pm
B/14/157 To receive questions from the Public in relation to items on the agenda
To receive
Graham Martin 12:30pm
B/14/158
Apologies for Absences: Dr Richard Hurwood, GP Locality Lead
MRH Sue Staples, Healthwatch Leicestershire
To receive
Graham Martin 12:40pm
B/14/159 Declarations of Interest on Agenda Topics To
receive Graham Martin 12:40pm
B/14/160 Minutes of the meeting held on 12 August 2014
To approve
Graham Martin
A 12:45pm
B/14/161 Matters Arising: Update on actions from the meeting held on 12 August 2014
To receive
Graham Martin
B 12:55pm
B/14/162 Notification of Any Other Business To
receive Graham Martin
verbal 1:00pm
REPORTS B/14/163
Chair’s Report To receive
Graham Martin C 1:00pm
B/14/164
Accountable Officer’s Corporate Report To receive
Dr Dave Briggs D 1:10pm
PATIENT SAFETY AND EXPERIENCE B/14/165 Patient Stories: progress report of follow up
actions To
receive Carmel O’Brien
E 1:20pm
B/14/166 Learning Lessons to improve care
To receive
Carmel O’Brien
verbal 1:35pm
FINANCE AND PERFORMANCE
B/14/167 Performance Assurance Report
To receive
Jane Chapman F 1:50pm

2
AGENDA ITEM ACTION PRESENTER PAPER TIMINGB/14/168
Finance Report: Month 4
To receive Karen English G 2:05pm
STRATEGY AND COMMISSIONING B/14/169
Locality Chairs’ Report:
Oadby and Wigston Melton, Rutland and Harborough Blaby and Lutterworth
To receive
Locality Chairs
H
2:20pm
B/14/170 ELR CCG IM&T Strategy Development Plan To receive
Tim Sacks I 2:40pm
B/14/171 Arriva Transport Solutions Ltd, (Non Emergency Patient Transport Service), Contract Year Three Agreement (July/ 1/ 2014 – June /30/ 2015)
To approve
Dr Dave Briggs
J
2:55pm
B/14/172 Better Care Together update
To receive
Dr Dave Briggs / Geoff Rowbotham
K 3:05pm
B/14/173 Better Care Funds: Leicestershire and Rutland
To receive
Jane Chapman
L 3:15pm
B/14/174 Summary report from the Strategy, Planning and Commissioning Committee
To receive
Dr Andy Ker M 3:30pm
DATE OF NEXT MEETING
B/14/175
The next meeting of the East Leicestershire and Rutland CCG Governing Body will take place on Tuesday 14th October 2014, venue to be confirmed.
3:30pm


Blank Page

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
1
LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
Minutes of the Governing Body Meeting held on Tuesday 12 August 2014 at 09.30am at the Council Chamber, Blaby District
Council, Desford Road, Narborough, LE19 2EP
Present: Mr Graham Martin Independent Lay Chair Dr Dave Briggs Managing Director Dr Andy Ker Clinical Vice Chair Dr Richard Palin Clinical Vice Chair Dr Graham Johnson GP, Blaby and Lutterworth Locality Lead Dr Richard Hurwood GP, Melton, Rutland and Harborough Locality Lead Dr Hilary Fox GP, Melton, Rutland and Harborough Locality Lead Dr Tabitha Randell Secondary Care Clinician Mr Alan Smith Independent Lay Member Mr Tim Sacks Chief Operating Officer Mrs Carmel O’Brien Chief Nurse and Quality Officer Mrs Karen English Chief Finance Officer Mrs Jane Chapman Chief Strategy and Planning Officer In Attendance: Dr Tim Daniel Consultant Public Health Ms Jennifer Fenelon Healthwatch Rutland Ms Sue Staples Healthwatch Leicestershire Ms Emma Rogers Head of Communications and Engagement Mrs Daljit K. Bains Head of Corporate Governance and Legal Affairs Mrs Poonam Beeharry Corporate Affairs Officer (minutes) Ms Sue Simms Collaborative Contracting Lead, GEM CSU (Paper K
only) Members of the Public: Mariam Broomhead Mr Tony Avalon
ITEM DISCUSSION LEAD RESPONSIBLE
B/14/133 Welcome and Introductions Mr Graham Martin, Chair, welcomed all to the East Leicestershire and Rutland CCG (ELR CCG) August Governing Body meeting. Mr Martin welcomed Ms Mariam Broomhead who was in attendance as a member of the public. Mr Tony Avalon letter attended as a member of the public.
B/14/134 To Receive Questions from the Public in Relation to Items on the Agenda There were no questions received from members of the public.

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
2
ITEM DISCUSSION LEAD RESPONSIBLE
B/14/135 Apologies for Absence: Apologies for absences were noted from:
Mr Warwick Kendrick, Independent Lay Member Dr Nick Glover, GP, Blaby and Lutterworth, Locality Lead
B/14/136 Declarations of Interest All GP members declared an interest in any items
relating to primary care where a potential conflict may arise and also where there are any items concerning the Leicester, Leicestershire and Rutland Provider Arm where GP members’ are minor shareholders.
In addition, Dr Richard Palin declared an interest in relation to any items relation to Leicestershire Partnership Trust (LPT).
Dr Richard Hurwood declared an interest in Paper K, Commissioning Policy for In Vitro Fertilisation (IVF)/ Intracytoplasmic Sperm Injection (ICSI) within tertiary Infertility Services as a member of his family is undergoing the treatment.
Mr Martin formally introduced Dr Richard Palin in his new role as Clinical Vice Chair for ELR CCG.
B/14/137 Minutes of the Meeting Held on Tuesday 13 May 2014. Subject to the following amendments the minutes of the meeting held on Tuesday 8 July 2014 (Paper A) were accepted as an accurate record of the meeting: Ms Sue Staples formal apologies were not noted in the minutes. It was RESOLVED TO:
APPROVE the minutes subject to the amendment above.
B14/138 Matters Arising: Update on Actions from the Meeting held on Tuesday 13 May 2014. The action log (Paper B) was received and some actions noted as complete. Updates against outstanding actions were noted as follows: B/14/39 - To present a report on the IM&T strategy to the Governing Body in June 2014. It was noted this was due to be presented in September 2014. B/14/115 – Patient story, To provide a follow up on the patient stories that have been shown to date to ascertain if
TS COB

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
3
ITEM DISCUSSION LEAD RESPONSIBLE
the issues raised have now been addressed. It was confirmed an update would be provided in September. B/14/125 – To confirm if EBS2: Cancelled Operations (page 4 of performance report) of the recovery action plans have been with UHL. Mrs Carmel O’Brien confirmed this has been agreed with UHL. It was RESOLVED to:
- RECEIVE the matters arising.
B/14/139 Notification of Any Other Business There were no notifications of Any Other Business.
B/14/140 Chair’s Report Mr Graham Martin, Independent Lay Chair, presented the report (Paper C) providing an overview and update of some of the key constitutional or strategic areas that affect the Governing Body and meetings that have been attended over the last month. Mr Martin drew attention to: Governing Body members The GP Locality Lead positions for Oadby and Wigston locality and Market Harborough sub-locality have been appointed to, with both GP Locality Leads likely to be in post by October. Annual General Meeting Plans are underway to hold the CCG’s first Annual General Meeting on Tuesday 2 September 2014 at Leicester Oadby Racecourse. Information in relation to the Annual General Meeting has been circulated to patients and members of the public. It was RESOLVED to:
RECEIVE the contents of the report.
B/14/141 Accountable Officer’s Corporate Report Dr Dave Briggs, Managing Director, presented the Accountable Officer’s Corporate Report (Paper D) providing an overview of the key activities of the Corporate Management Team (CMT) since the last meeting of the Governing Body in July 2014. Dr Briggs drew attention to:
National Institute for Health and Care Excellence (NICE) Safe Staffing Guidelines: NICE published the

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
4
ITEM DISCUSSION LEAD RESPONSIBLE
first guideline in this new work programme, Safe staffing for nursing in adult inpatient wards in acute hospitals. This guidance makes recommendations on safe staffing for nursing in adult inpatient wards in acute hospitals, based on the best available evidence. Dr Briggs welcomed the guidance in a move to increase transparency.
Primary Care 5 year plan: A steering group has been
set up which has already progressed this plan and a series of member, patient and stakeholder events will be taking place between now and 11 September 2014 to ensure the CCG have the views of everyone concerned.
Dr Richard Hurwood queried how the Sign up to Safety campaign was being publicised. Mrs O’Brien explained the campaign was for providers provisionally with the CCGs supporting. Mr Alan Smith queried when the Terms of Reference (ToR) for the Corporate Management Team meetings would be shared. Dr Briggs advised the ToR would be shared outside of the meeting. Ms Jennifer Fenelon noted that the sign-off date for Primary Care Strategy was tight (September 2014) and queried how the public were going to be involved given the tight timeframe. Mr Tim Sacks explained a steering group will be set up, to which Healthwacth will be invited. Further to this, Chairs of the Patient Representative Groups would be asked to comment. Mr Sacks explained that this was a high level strategy and if any changes were necessary, the strategy would be subject to a much wider campaign of engagement. It was RESOLVED to:
RECEIVE the contents of the report
DELEGATE authority to the Primary Care Steering Group to sign-off the Primary Care 5 year Plan on behalf of the Governing Body for the submission in September 2014.
Mrs Daljit Kaur Bains
B/14/142 Quality and Clinical Governance Committee summary report Mrs Carmel O’Brien, Chief Nurse and Quality Officer, provided a summary of the items discussed at the Quality and

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
5
ITEM DISCUSSION LEAD RESPONSIBLE
Governance Committee held on Tuesday 22 July 2014 (Paper E). Mrs O’Brien drew attention to:
The draft Concordat (NHS England (Leicestershire and Lincolnshire Area)) for the Sharing of Information and the Management of Concerns relating to the Professional and Contractual Performance of Primary Medical Practitioners was presented. The document details how information or quality concerns regarding practices can be triangulated and shared between ELR CCG and NHS England. It was reiterated that the concordat does not cover individual practitioners, as performance is managed by NHS England. It was noted that the Quality and Clinical Governance Committee is included in the Concordat as being part of the framework for raising concerns. It was agreed that, Mr Tim Sacks and Mrs Carmel O’Brien would be taking this forward.
The outcomes of the Cancer Deep Dive meeting were
shared, recovery plans are currently being reviewed, and the issue around the backlog of some appointment types has been escalated to the Contract Performance Meeting.
Referral to Treatment times (RTT) - It was noted that
although improvements have been seen in Referral to Treatment times, UHL is unlikely to achieve the 90% compliance target by September 2014. It was noted the Governing Body was aware of the situation and this has been escalated to NHS England.
Improving Access To Physiological Therapies (IAPT)
Concerns were raised about IAPT performance in the county, it was noted that a new self-referral scheme will be piloted in two sites, with performance monitored and improvements expected.
Ms Fenelon noted that in relation to the cancer deep dive, concerns around the cancer targets not being met appeared to be continuing. Ms Sue Staples explained Healthwatch had some concerns in relation to the way two care homes were administering medication. Mrs O’Brien explained a piece of work was currently underway around care homes and will link this work back to the Local Authority to target specific improvements identified.

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
6
ITEM DISCUSSION LEAD RESPONSIBLE
It was RESOLVED to:
RECEIVE the report for information
B/14/143 Learning Lessons to Improve Care Mrs Carmel O’Brien / Dr Richard Hurwood presented the report (Paper F) which details the findings of a clinical audit commissioned by health organisations in Leicester, Leicestershire and Rutland to examine the quality care of patients and the action plan to address the areas of improvement identified. Mr Graham Martin explained that the study found some areas of good practice, however highlighted the significant variances in quality of care. The study provided clear evidence that healthcare was not joined up across Leicester, Leicestershire and Rutland (LLR) and on behalf of the ELR CCG’s Governing Body offered an apology to those patient who standard of care was below acceptable. The aim of the study was to learn lessons. Mrs O’Brien and Dr Hurwood provided an overview of the study covering:
The rationale for the audit The audit methodology Audit findings Examples of findings from the top three themes, which
include, Do Not Attempt Resuscitation (DNAR) , Clinical reasoning and Palliative Care
What the findings mean Review recommendations The duty of candour – In the spirit of the duty of candour,
a decision to contact the next of kin for all 381 patients involved in the review was made. A helpline was collaboratively established and run by University Hospitals of Leicester (UHL), Leicester Partnership Trust (LPT) and the 3 CCGs across Leicester, Leicestershire and Rutland. It was noted that 55 calls were received via the helpline and outcomes of those who contacted the helpline differed. Some families wanted to have a meeting with the relevant trust/ provider, some wanted further information about the review and some families felt the letter re-opened emotional distress. Offers to meet were offered to those families who wanted it. Locally, issues relating to primary care are beginning to filer through to CCG;s and Dr Hurwood has contacted a practice as a result.
The five point action plan - there is work already in place

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
7
ITEM DISCUSSION LEAD RESPONSIBLE
in relation to the clinical leadership and task force with terms of reference being drawn up to oversee the implementation of the action plan.
Mr Martin queried whether the five point action plan included transforming End of Life care (EoLC). Dr Ker explained he was on a working group who were working on getting some consistency in the approach to EoLC. It was clear that understanding within the acute sectors about what is done in the community is missing. The group are working through the paperwork, changing simple things such as phrasing to ensure Do Not Attempt Resuscitation (DNAR) forms are understood by the acute sector. They are also developing structures to enable paperwork to go with patients. Dr Richard Palin added that in relation to the review, choosing specific case notes of patients who did not recover from a period of illness meant that it was expected to find issues that needed addressing. It was a pre-emptive piece of work to try and improve care and it was important to act upon the themes found and not become embroiled in the figures as these do not say much about patient experience. Ms Staples queried whether Dr Ker’s work in relation to EoLC was looking at EoLC in residential care homes as this is one area that could benefit form a consistent approach. Dr Ker advised that all CCGs were looking at care home work. Dr Ker explained the DNAR’s remain unchanged locally. Dr Ker explained relatives needed to be involved with setting up DNAR, however acknowledged that sometimes (specifically in relation to advanced care planning) it can be so advanced (in five years’ time), that patient would prefer to discuss this with family and therefore it was not always appropriate and as long as that was documented, the clinician remained covered. Dr Graham Johnson drew attention to the commitment of University Hospitals of Leicester (UHL) to invest in an additional 200 ward-based nurses. Dr Johnson raised concern over this following information found on the NHS choices website which showed 12 wards had less than 85% staffing. Dr Johnson also queried how the action plans relate to the examples of care highlighted in section 16. Mrs O’Brien explained this was the first month that staffing figures were available and explained that UHL were aware and recognised nursing recruitment was an issue. Mrs O’Brien explained that UHL has re-baselined to increase staffing and

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
8
ITEM DISCUSSION LEAD RESPONSIBLE
are working hard on an active recruitment campaign. Mrs O’Brien explained that every trust across the country is currently recruiting out of the same pool. In relation to the specific actions for the individual cases, Mrs O’Brien explained serious incident investigations would be undertaken and this process allows for broader investigations. This review produced high level action plans. Dr Hurwood added that the individual cases could be used as a learning lesson and could be broadcast widely. Mr Martin queried how the implementations of the action plans would be reported back to the Governing Body. Mrs O’Brien explained the terms of reference for the proposed clinical task force were being drawn up and would require a clinical representative from the Governing Body. Dr Briggs agreed it was important to monitor progress against this and acknowledged the review was difficult to read however recognised the hard work of all those involved. It was RESOLVED to:
RECEIVE the findings of the report and the Five Point Action Plan
APPROVE the Five Point Action Plan RESPOND to the learning lessons to improve care
oversight group demonstrating the board’s commitment to the improvements identified
B/14/144 Performance Assurance Report
Mrs Jane Chapman presented the Performance Assurance Report (Paper G) which provided an overview of performance for East Leicestershire and Rutland CCG and Leicester, Leicestershire and Rutland where data is available for June 2014. Updates against high risk indicators were noted as:
IAPT access – current performance is 12.8% against a local target of 16%. There is a robust action plan in place to increase access.
RTT – there is an RTT action group in place responding to the call from NHS England to return to the position of January 2013, Mrs Chapman noted this was a standard as opposed to a target.
Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
9
ITEM DISCUSSION LEAD RESPONSIBLE
UHL A&E 4 hour wait – current performance is still challenged.
Cancer 2 week wait - There has been a significant increase in breast referrals, this is seen when there has been media focus on this area. A Cancer action group is in place to recover the position.
Cancelled operations – For July have been at an all-time low.
Handover times between ambulance and A&E – remains challenged.
Mr Martin queried UHL 4 hour wait data for other trusts such as Peterborough and Kettering. Mrs Chapman advised Peterborough was also challenged but did not have any information about Kettering to hand. Dr Johnson queried what the specific issues are for cancer 62 wait as it was significantly below the target. Mrs Chapman deferred the question to Dr Palin who advised he would make enquiries at the Clinical Quality Reference group. It was RESOLVED to:
RECEIVED the contents of the report
Dr Richard Palin
B/14/145 Finance Report Month 3 Mrs Karen English, Chief Finance Officer, presented the report (paper H) which provides an update on the 2014/15 year to date and forecast outturn financial position for East Leicestershire and Rutland Clinical Commissioning Group (ELR CCG). The report is based on activity for two months with a one month estimate. The CCG is on plan with most areas across the acute sector and most the non acute contracting areas. High risk areas and overspend were noted against:
- CHC - Changes in the way activity is recorded for the acute
sector has shown a spike in outpatient activity. The contingency for the year is already being maximised. Dr Johnson queried the outturn positions for out of county and independent sectors. Mrs English explained that in order to report a balanced position, contingency monies have been used. Mrs English added that there has been some additional money to deal with RTT and part of the financial challenge was

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
10
ITEM DISCUSSION LEAD RESPONSIBLE
to ensure all of the money did not go solely to UHL as some of the out of county providers were also tackling the same issues and therefore some RTT funds would need to be provided to them. Mr Smith queried whether the previously unidentified QIPP had been resolved. Mrs Chapman explained the Strategy, Planning and Commissioning Committee meeting in July 2014 was dedicated to identifying the QIPP to close the gap and as a result the Head of Strategy and Planning was doing some further work. Mr Smith queried whether any thought had been given to QIPP for the following year. Dr Briggs advised the following year’s QIPP will feature peer to peer review processes for acute admissions, falls and ambulance trusts and extending community service hours to bring it in line with seven day working. It was RESOLVED to :
RECEIVE for information the contents of the report and the appendices attached.
B/14/146
Emergency Department Performance Update Dr Dave Briggs presented the report (Paper I) which seeks to update the Governing Body in relation to performance of the local urgent and emergency care system, in particular UHL’s performance against the national four-hour standard for A&E, and a series of actions taken by both the three LLR CCGs collectively and the wider health economy to address the underlying issues affecting performance. Dr Briggs drew attention to key updates as follows:
Clinical engagement and standards is the area focused upon
Clinicians are now leading pathway redesign and setting own standards.
Trusts are concentrating on harm events, getting the diagnosis right, discharge and reducing the number of complaints.
Key indicators are:
Reducing mortality rate, Discharged to their place of choice (home) Increasing amount of re-ablement and rehabilitation Reduction in number of people 75 or older who stay 10

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
11
ITEM DISCUSSION LEAD RESPONSIBLE
days or more Reduction in number of people coming in following a fall.
The improvement programme will run over 6 months. Dr Johnson raised concern in relation the reference of lack of optimal substantive staffing levels as one of the key reasons for under performance in the paper. Dr Johnson queried how staff were going to be attracted to the department without substantive staff. Dr Briggs explained the plan has a much bigger focus around discharge and clinical assessments. They are looking for clinicians to make decisions to move patients on. If that is addressed, it will give the ED capacity to deliver. Dr Briggs explained Mr Sturgess’s review was entering its second phase which includes understanding the community impact and Primary Care involvement. It was RESOLVED to:
RECEIVE the contents of the paper.
B/14/147 Locality Chairs Report Mr Tim Sacks, Chief Operating Officer, introduced the report (Paper J) which provides an overview of the monthly GP Locality meetings held across Blaby and Lutterworth, Oadby and Wigston and Melton, Rutland and Harborough. Mr Sacks highlighted the meetings are key to the CCG development and allow member practices an opportunity to debate current general practice and highlight themes they wish to inform the Governing Body. MELTON RUTLAND AND HARBOROUGH – Chair Dr Richard Hurwood Dr Richard Hurwood presented key areas of discussion as: Better Care Together - Discussions were focussed on how and what services and resources need to be put in place at Primary Care level to support the delivery of the Better Care Together programme, discussions also covered the impact this programme will have on Primary Care practices. The discussion generated some good ideas. BLABY AND LUTTERWORTH – Chair Dr Nick Glover Dr Graham Johnson presented key areas of discussion as:

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
12
ITEM DISCUSSION LEAD RESPONSIBLE
Community Nursing - A discussion was had as part of the Better Care Together item, which for this system of change to be successful there needed to be a robust confidence in Community Nursing so that patients could be successful looked after in their own homes. H Pylori - Issues with the H Pylori service that started on 1f July 2014 were raised and the robustness of the AQP process was a concern. Particular issues raised were:
The service is not on the Choose and Book System No standardised referral form All providers are not aware of the test GP providers were limiting the service to their own
patients Service not running effectively on 1st of July 2014
Anglia ICE (Radiology and Cardiology) - The Radiology and Cardiology departments at UHL do not send back results to the GP requesting the tests, instead results go back to the GP that UHL has on their database which in most cases is not the requesting GP. This has clinical governance implications. Mr Graham Martin queried whether Dr Johnson had any information about NHS England’s GP recruitment process. Dr Johnson explained he was not aware of any specific information, however noted there was that with the extra shift in work, there did not appear to be a resource match. Dr Briggs commented that there would not be enough GPs to deliver the traditional primary care model and the primary care strategy would need to describe innovation on how to delivery primary care in this health economy. Dr Johnson added that a key issue was extra non-clinical demands placed upon GPs. Reducing this would take some of the pressure of GPs in the short term. OADBY AND WIGSTON – Chair Dr Richard Palin Dr Richard Palin presented key areas of discussion as: The appointment of a GP Locality Lead position for Oadby and Wigston went through an election process and Dr Vivek Varakantam, from The Croft Medical Centre (Oadby), received

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
13
ITEM DISCUSSION LEAD RESPONSIBLE
the majority votes. It was RESOLVED to
RECEIVE the report
B/14/148 Commissioning Policy for In Vitro Fertilisation (IVF)/ Intracytoplasmic Sperm Injection (ICSI) within tertiary Infertility Services Dr Dave Briggs introduced report (Paper K) which provides a summary of the review of the IVF/ICSI policy which had taken place following the issue of the National Institute for Health and Care Excellence’s (NICE) revised guidelines (CG156) published in January 2013. The guidelines recommended changes in particular around the upper age limit and reiterated a previous recommendation about the number of cycles for which NHS funding should be offered. Dr Briggs noted the minutes appended to Paper E, Quality and Clinical Governance Committee summary reflected the comments made by the committee in relation to the policy. Key points to note from the revised policy were highlighted as:
The revised policy now includes funding for women aged 40-42 years.
There has been no change to the policy of funding one full cycle of IVF.
Dr Johnson noted that the NICE guideline recommended that 3 cycles should be funded for those under 40, however within the report, it stated that the decision was to continue to fund one cycle had been made for two reasons one of which was because of evidence provided by NICE that the chances of a successful outcome decreased with the number of unsuccessful cycles. Dr Johnson queried how that statement had been used to influence the decision about funding 3 cycles. Mrs Sue Sims, Collaborative Contracting Lead, GEM CSU, provided some context behind the revised policy. Mrs Sims explained that the NICE recommendation to fund three cycles was not new, but had also been included in the previous guideline (CG11) that was issued in 2004. On behalf of the CCGs in the East Midlands, GEM CSU had commissioned Public Health Solutions to review CG156 and compare it to the previous East Midlands Specialised Commissioning Group policy particularly in relation to any new recommendations or evidence. The report was then considered by a working group comprising representatives from across the CCGs across the

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
14
ITEM DISCUSSION LEAD RESPONSIBLE
patch. Mrs Sims quoted from data published by the Human Fertilisation and Embryology Authority that for a woman in her 20’s and early 30’s the chances of a successful outcome was 32.3%. This reduced with age to 13.6% for the over 40’s. In addition a recommendation, new to NICE in 2013, had been that people should be informed that the overall chance of a live birth following IVF treatment falls as the number of unsuccessful cycles increases. Data from two studies on this topic had been included in the guideline to support the recommendation. Dr Briggs highlighted the financial impact of funding three cycles and informed that at IVF was not a priority detailed within the CCG’s commissioning intentions. However the revised policy meant there was increased access to IVF for women aged 40-42. Ms Fenelon queried what consultation had taken place in 2013 as Healthwatch were not aware any consultation. Mrs Sims explained it was not a full scale public consultation as this was an update to a policy as opposed to a new policy. The consultation had followed the same process as that carried out by the East Midlands Specialised Commissioning Group (EMSCG) previously. The consultation included providers of IVF, CCGs and a number of groups who had an interest in IVF. Ms Sue Staples noted there had been no voluntary sector or Healthwatch input. These groups would have been able to provide local opinion and requested this was considered for the future. Dr Johnson acknowledged that extending the age range was good, but also noted that this meant that more money was being spent on potentially less successful outcomes as opposed to funding more cycles with a higher success rate. Dr Briggs emphasised that the East Midlands CCGs had taken the same approach which eliminated any potential postcode lottery and in addition access to IVF treatment had increased by extending the age range. Dr Briggs thanked Mrs Sims for attending.
It was RESOLVED to:
APPROVE the policy

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
15
ITEM DISCUSSION LEAD RESPONSIBLE
B/14/149 Any Qualified Provider Domiciliary Care CHC Services for Adults and Older People in LLR Mrs Jane Chapman presented the report (Paper L) which details the outcome of Phase 4 – Any Qualified Provider (AQP) Domiciliary Care Continuing Healthcare (CHC) Services from September 2014 Mrs Chapman explained the process was led by GEM, however there was senior input throughout the process which was rigorous and noted the they were all AQP contracts. Mrs Chapman confirmed that the Board was not approving a contract award but approving the qualification of the twelve providers through the process who may now enter into a contract for service provision subject to agreement with CCG terms and conditions It was RESOLVED to:
RECEIVE the procurement process and AGREE the approval of twelve providers listed in
section 2.3 for the provision of CHC Domiciliary Care services for adults and older people, with a potential contract implementation date of September 2014 subject to agreement as above
B/14/150 Better Care Together (BCT) Update Dr Dave Briggs presented the report (Paper M) which provides an update on the progress on the Better Care Together plans. Dr Briggs explained Paper M describes work underway to add the detail and granularity to the high level directional plans. Key updates were noted as:
Clinical leads have been identified for all of the workstreams.
The Project Management Office (PMO) still needs further work and clarity
There have been changes in governance of Better Care Together board
Dr Hurwood queried whether there would be a change in personnel in the BCT. Dr Briggs explained the current Programme Lead is an interim and will need to be replaced, however that will only occur after the appointment of the Chair. Dr Briggs agreed to share the date of interview outside of the meeting. Senior Responsible Officers (SROs) have also been

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
16
ITEM DISCUSSION LEAD RESPONSIBLE
appointed: Mr John Adler and Mr Toby Sanders. Mr Martin queried the cost of participating. Mrs English advised costs will be shared across 6 organisations and discussions are underway to agree fair share costs. It was RESOLVED to:
RECEIVE the report for information
B/14/151 LLR Operational Resilience Plan Mrs Jane Chapman introduced the report (Paper N) which details operational resilience and capacity planning guidance for 2014/15 bringing together the non-elective and elective elements of delivery into one planning process to ensure the whole health and care system works together in delivering services to patients. Key points to note: Winter funding for the traditional A&E has been combined with elective care processes in resilience funding. Total Central Resilience Funding has been allocated to Leicester, Leicestershire & Rutland as below:
・ Non-elective care: £6 million
・ Elective care: £3.978 million
There are two plans appended the report for elective and non elective care. Dr Briggs highlighted key points from the non elective care as:
Work is underway on another version of plan. The narrative in section one needs further work, a revised narrative will be released early next week.
Of the £6m, £3m will be invested in UHL. This will look at supporting the falls service.
In terms of specific CCG investment, this will cover such things as peer review.
A small investment in adult social care to ensure staff are available in line with 7 day working.
Investment in NHS 111 to make winter more robust Investment in mental health triage.
Dr Johnson queried the 340k put against additional capacity for Primary Care (section 2 of appendix to paper N) and asked where the money was being spent.

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
17
ITEM DISCUSSION LEAD RESPONSIBLE
Dr Briggs stated primary care investment of £340k is to be invested in schemes, such as peer review, to reduce emergency admissions. The details are in the process of being developed Mrs Chapman highlighted key points for elective care as follows:
Central resilience fund of £3.978m has been allocated to LLR to support delivery of the three RTT standards in September and sustainably beyond that. It has already been through the process to have the plans agreed in principal and work is already on going.
Contracts have also been increased to ensure capacity and demand match.
Mr Martin queried whether the RTT board were going to monitor the effective use of the money. Mrs Chapman explained how the funding will flow through the system. 50% is available upon a plan being agreed (for LLR this is subject to tripartite review), the next 25% is available on achievement of key milestones (which relate to validation of the waiting list and reduction in backlog) and the final 25% is available on standards being achieved. Mrs Chapman noted that achieving payment of the final 25% for this Health economy, was a risk. Dr Johnson noted that no 18 in section 2 talked about staffing and lack of staffing. DR Johnson queried where these doctors and nurses would be coming from. Mrs Chapman explained the terminology advising that £9m does not pay for additional doctors and nurses, it pays for additional activity. As part of that tariff, providers are investing in nurses and doctors. A significant number of staff have been appointed. Currently there are locums in place, however, There is an expectation to see the full impact to in September/ October 2014. Dr Any Ker noted that on the last page, (point 18) there was reference to developing a MDT triage service and that they were commencing with ophthalmology as proof of concept. Dr Ker queried whether this was a pilot. Mrs Chapman confirmed it was a pilot as there was already a single point of access for ophthalmology. Mrs Chapman added that Ophthalmology for RTT has been a significant win, highlighting that if all elements of a plan come together, they can achieve the standard ahead of time. The plans for all specialities are similar. However Mrs Chapman acknowledged the degree of difficulty does vary depending on speciality.

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
18
ITEM DISCUSSION LEAD RESPONSIBLE
Mrs English asked how the CCG was going to access the RTT money. Mrs Chapman advised the RTT money would be coming to CCGs at month 4. It was RESOLVED to:
APPROVE the LLR Operational Resilience and Capacity Plan.
B/14/152 Better Care Fund (BCF) New Guidance Implications
Mrs Jane Chapman presented the report (Paper O) which summarises the new BCF guidance published on 25th July 2014 and makes recommendations in terms of the next steps and timescales for the resubmission of the Leicestershire and Rutland BCF Plan. Key challenges were highlighted as:
3.5% reduction in all admissions A date of 19 September 2014 for resubmission of plans
means an increased pressure on teams. Dr Hurwood noted that for admissions, the CCG was already below average. Dr Briggs explained that whilst that number of primary care admissions was lower, the number of overall admissions was not. Mrs Chapman noted the final submission would be brought back to next month’s board. It was RESOLVED to
RECEIVE for information
B/14/153 Summary report from the Strategy, Planning and Commissioning Committee Dr Any Ker presented the report (Paper P) which provides a summary of key areas of discussion and outcomes from the Strategy, Planning and Commissioning (SPC) Committee held on Tuesday 15 July 2014. Approved minutes from the 17 June 2014 meeting are appended to the report. It was noted that the majority of the Governing Body were present at the July meeting. Key areas discussed were:
Draft Five Year Strategic Plan Update

Paper A East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
19
ITEM DISCUSSION LEAD RESPONSIBLE
Better Care Funds Plan QIPP challenge CHC Fast Track Challenge – Mr Robin Wintle, (insert job
title) presented some ideas on how to alleviate the pressures on the current overspend.
It was noted that these topics had already been discussed by the Governing Body. It was RESOLVED to:
RECEIVE the report for information
B/14/154 Update from the Commissioning Collaborative Board (CCB) Dr Dave Briggs presented the report (Paper Q) which provides an update of the meeting of the Commissioning Collaborative Board held on 31st July 2014 It was RESOLVED to:
RECEIVE the report for information
B/14/155 Date of next meeting The next meeting of the East Leicestershire and Rutland CCG Governing Body will be take place on Tuesday 9 September 2014 at PERA Innovation Park, Melton Mowbray, Leicestershire, LE13 OPB.


Blank Page
Paper B East Leicestershire and Rutland Clinical Commissioning Group Governing Body Meeting
9 September 2014
1
NHS EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
ACTION NOTES
Minute No. Meeting Item Responsible
Officer Action Required To be
completed by
Progress as at September 2014
Status
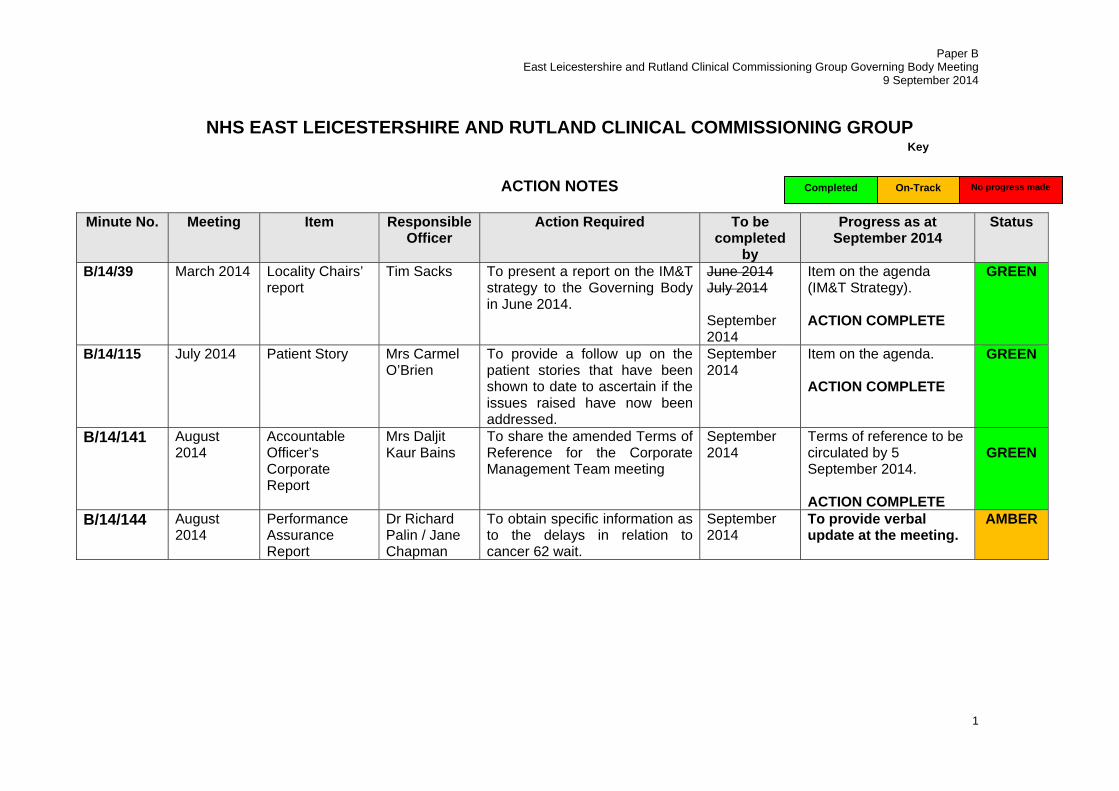
B/14/39 March 2014 Locality Chairs’ report
Tim Sacks To present a report on the IM&T strategy to the Governing Body in June 2014.
June 2014 July 2014 September 2014
Item on the agenda (IM&T Strategy). ACTION COMPLETE
GREEN
B/14/115 July 2014 Patient Story Mrs Carmel O’Brien
To provide a follow up on the patient stories that have been shown to date to ascertain if the issues raised have now been addressed.
September 2014
Item on the agenda. ACTION COMPLETE
GREEN
B/14/141 August 2014
Accountable Officer’s Corporate Report
Mrs Daljit Kaur Bains
To share the amended Terms of Reference for the Corporate Management Team meeting
September 2014
Terms of reference to be circulated by 5 September 2014. ACTION COMPLETE
GREEN
B/14/144 August 2014
Performance Assurance Report
Dr Richard Palin / Jane Chapman
To obtain specific information as to the delays in relation to cancer 62 wait.
September 2014
To provide verbal update at the meeting.
AMBER
No progress made On-Track Completed
Key


Blank Page
Paper C East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
1
NHS EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
GOVERNING BODY MEETING
9 September 2014
Chairman’s Report Introduction 1. The purpose of this report is to provide an overview and update of some of the
key constitutional or strategic areas that affect the Governing Body and meetings that I have attended over the last month.
Governing Body members 2. I would like to welcome Dr Girish Purohit who has been appointed as GP
Locality Lead for the Market Harborough sub-locality of Melton, Rutland and Harborough. Dr Purohit is a partner at the Jubilee Medical Practice, Syston Health Centre, Syston.
3. Dr Purohit has held a number of leadership positions, including his appointment as the Clinical Lead for Service Innovation and Improvement for Hammersmith and Fulham Primary Care Trust where he was involved in service development projects.
4. I would also like to welcome Dr Vivek Varakantam who has been elected as the
GP Locality Lead for Oadby and Wigston Locality. Dr Varakantam is a partner at The Croft Medical Centre, 2 Glen Road, Oadby.
5. Dr Varakantam, was a GP Appraiser; and also the clinical lead for the Oadby and Wigston locality.
Annual General Meeting
6. More than 80 people attended our first Annual General Meeting (AGM) on 2 September at Oadby Racecourse. I would like to thank everyone who came along and those who contributed to making it such a success.
7. The event included a ‘marketplace’ area in the foyer, where CCG staff demonstrated what our CCG does for patients in many creative and interactive ways. Members of the public also had the opportunity to share their views on local health services and discover ways they can become involved in shaping the future of local healthcare. We also welcomed our partners Healthwatch Leicestershire and Healthwatch Rutland, who ran a stand to offer the public opportunities to learn more and get involved.
8. The formal part of the meeting started at 6pm with a presentation focusing on
the CCG’s achievements over the last year including details of the progress we have made in improving services for people with long-term conditions including

Paper C East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
2
COPD, diabetes, dementia and mental health. We also shared details on progress in improving the quality of care in light of the Francis Report and our commitment to, and methods for, involving local people in the development of services. The presentation concluded with an overview of the challenges ahead and our support for the Better Care Together Programme along with plans for improving primary care and community services.
9. The public question session saw the panel dealing with challenges about plans
for people with learning difficulties, weekend urgent care opening in Oadby, UHL’s deficit and its £40m A&E redevelopment scheme, patient choice, the quality of GPs’ surgery buildings and services, as well as the performance of Arriva’s non-emergency patient transport service.
10. A summary of the presentation and question and answer session will be
available on the CCG website shortly and will be circulated to those who attended.
Recommendations The East Leicestershire and Rutland CCG Governing Body is requested to: RECEIVE the contents of the report.


Blank Page

Paper D East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
Dr Dave Briggs 1 Accountable Officer
NHS EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
GOVERNING BODY MEETING 9 September 2014
Accountable Officer’s Corporate Report
Introduction 1. This report sets out to the Governing Body some of the key activities the
Corporate Management Team (CMT) and I have been involved in since the last meeting of the Governing Body in August 2014.
Update from Commissioning Collaborative Board (CCB) meeting 2. The CCB received an update on East Midlands Ambulance Service (EMAS). It
was noted that this year represented the third year of the additional transformation funding. The CCB also received an update from the three CCGs regarding their Primary Care Medical Plans. An update on the progress of these plans is to be brought back to the CCB in October with a view to identifying common themes that could be logically best be undertaken jointly.
3. The CCB received an update on the progress of contractual discussions with Arriva and the impact on this wider health economy. It was noted that there is a public meeting with Arriva to take place on 17 September 2014.
NURSING, QUALITY AND CORPORATE AFFAIRS 4. The Accountable Officer and Chief Nurse and Quality Officer represent the CCG
as members of the Leicestershire Quality Surveillance Group (QSG) convened by the NHS England Leicestershire and Lincolnshire Area Team. There have been two recent QSG meetings: an extraordinary QSG convened on 11 June 2014 specifically to review high risk within University Hospitals of Leicester; and a routine QSG on 23 June 2014. The public summaries of outcomes from these meetings are appended to this report for information.
STRATEGY AND PLANNING Development of a Community Services Strategy 5. National policy, evidence and best practice tells us that innovation and creativity
is required in order to achieve the transformation element of the community services policy. Locally, people tell us they want care closer to home and out of hospital care. This only works if alternative community solutions are in place. The CCG is therefore in the early stages of drafting a community services discussion document/strategy to begin the dialogue with stakeholders, patients and the public about how we do this locally and what it will look like.
Health Foundation ‘Scaling up improvement’ 6. The CCG is submitting a bid in response to the Health Foundation ‘Scaling Up
Improvement’ call for bids. The initial bid was circulated to members of the

Paper D East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
Dr Dave Briggs 2 Accountable Officer
Strategy, Planning and Commissioning Committee in June 2014 and they will receive the full bid at the September meeting. The Governing Body is asked to support the bid submission, which relates to the development of integrated care planning and is in line with strategic objectives.
PRIMARY CARE Primary Care 5 year plan 7. As part of the CCG’s long term plan for improving the health of the population of
East Leicestershire and Rutland, the future of primary care and in particular, Primary Medical Services, it is important to have a detailed and robust plan of how we commission services and how our members provide healthcare now and in the future.
8. The Better Care Together / 5 year strategy has set out some aspirational targets
to reduce the level of care provided in an acute setting. It is necessary for the CCG and its members to respond to this challenge of how this care can be provided in an out of hospital setting. The aim of the Primary Care Plan is to achieve this goal and also to ensure robust and viable primary medical services now and in the future.
9. To fully understand the challenge facing primary care and the solutions
necessary to meet the needs of our population over the coming years, we have embarked upon a series of conversations, events and workshops with our members led by a multi-agency steering group. So far we have held detailed telephone interviews with 32/34 of our practices, held an all day workshop attended by a wide group of GPs and undertaken a GP, Nurse and practice manager session on designing solutions. There are two more events to take place in September to further develop the plan, which will form the initial submission in October to the Better Care together programme.
PUBLICATIONS 10. Publications and updates published by NHS England via its fortnightly newsletter
Bulletin for CCGs can be found at the following http://www.england.nhs.uk/publications/bulletins/bulletin-for-ccgs/. The Corporate Management Team undertake a regular review of the content of the Bulletin and ensure actions are taken accordingly. Assurances and updates are reported through to the Governing Body as evident on the agenda and through updates in the Accountable Officer’s report.
Recommendation The East Leicestershire and Rutland CCG Governing Body is requested to: RECEIVE the contents of the report. SUPPORT the bid submission for Health Foundation ‘Scaling Up Improvement’.

Briefing for the members of the Quality Surveillance Group (QSG) Leicestershire Extra-Ordinary QSG meeting held on 11 June, 2014
Overview of Local Information
This report provides a summary of the views of each organisation at the meeting and a conclusion about the way forward.
Thematic Discussion
‘University Hospitals of Leicester NHS Trust’
Leicestershire and Lincolnshire Area Team • Continued failure to meet the 4 hour target for
A&E.
• No doubt there is an elevated risk
• No doubt there are improvements, however where these exist, it is patchy
• There is clear line of sight of improvement by the NHS Trust Development Authority which is corroborated by Health Education East Midlands
East Leicestershire & Rutland CCG • Two new serious incident reported within the
Emergency Department at UHL
• Anxiety around the Emergency Department and not the wider Trust.
West Leicestershire CCG • New information is available to the QSG
• CCG Boards are anxious about UHL
Leicester City CCG • Acknowledge improvements in relation to the
62 day wait for cancer services
Care Quality Commission (CQC) • Improvement action plan received from UHL
following the inspection in January 2014.
• CQC final report will be published in July 2014.
• Emergency Department remains an elevated risk on the CQC monitoring but no new concerns identified.
NHS Trust Development Authority (TDA)
• Against the NHS TDA assurance framework UHL are at level 2 due to financial performance
Leicestershire and Lincolnshire

and A&E target.
• The TDA will take UHL through the action plan following the CQC Chief Inspectors report in to compliancy.
• The Trust has recently demonstrated good governance in relation to challenges.
• The Emergency Care Intensive Support Team is due to revisit UHL to review improvements.
Healthwatch
• Identified two incidents of poor patient experience.
• Potential lack of public confidence. • Five potential risk summit trigger points
identified but further information required.
Conclusion • No new potential triggers satisfied and no risk
summit will be called today. • UHL will remain on enhanced surveillance to be
reviewed through Leicestershire QSG meeting and the need to call a UHL risk summit will continue to be reviewed.
• A detailed report of the considerations of this QSG will be made to the Regional QSG on 17 June 2014 recommending no risk summit.
C

PAPER J
Briefing for the members of the Quality Surveillance Group (QSG) Leicestershire QSG meeting held on 23 June, 2014
Overview of Local Information
Area Team Update
Leicestershire and Lincolnshire Area Team – Ms Manjit Darby
• Following the review of the QSG, the following actions have been agreed :
o To extend the QSG to reflect on the processes that we use to ensure honest, open and transparent conversations
o To ensure there is a process to support challenge and difficult conversations
o To agree a process for surveillance and risk in a more uniformed way
o To consider that relationships in the room are important and to get to know you better
o To execute a tidy-up of administration for this QSG
Areas of Good Practice
Leicestershire and Lincolnshire Area Team – Dr David Sharp
• Extraordinary QSG meeting held on 11 June - A discussion was held regarding how QSG can manage its time more effectively whilst at the same time remaining inclusive. Everyone had an opportunity to voice their opinions during the 2 hour discussion.
• The NHS Trust Development Authority feel they have oversight of University Hospitals of Leicester NHS Trust (UHL).
East Leicestershire and Rutland Clinical Commissioning Group (CCG) – Carmel O’Brien
• University Hospitals of Leicester NHS Trust (UHL) - high level nursing metrics were implemented last year at which now need to be reviewed in terms of what happens operationally when ED is busy
• Work has been commissioned externally ‘what it is like for patients who spend a long time on a trolley’.
Leicestershire and Lincolnshire

PAPER J
‘Review of QSG’
QSG Updates
Leicestershire and Lincolnshire Area Team – Ms Manjit Darby
• The National Quality Board has undertaken a review of the QSG model and updated guidance on how to run an effective QSG was published in March 2014. At the last QSG meeting it was agreed that a more in-depth review should take place including the issue of a survey to all attendees.
• Results of the survey were shared with the QSG in relation to attendance, what aspects of the QSG work well, not so well and what could be done differently to make the QSG more effective. A discussion was held concerning business planning recommendation, the sharing of completed reporting templates prior to meetings, trend analysis and facilitates time out for QSG meetings.
• The Terms of Reference needs to be more explicit as regards the role of the Chair especially during difficult debates and discussions.
Leicestershire and Lincolnshire Area Team – Dr David Sharp
• Extraordinary QSG meeting held on 11 June 2014 – an update was provided by Dr David Sharp who described this as an interesting meeting which showed that QSG methodology is difficult to execute and no single organisation present in the room held sway. There is no doubt that strongly expressed polarised views were apparent during the meeting.
NHS Trust Development Authority – Ms Helen Hendley
• Leicestershire Partnership NHS Trust (LPT) has made significant progress and quality monitoring will return to business as usual.
C
Reports from Other Agencies
Additional information participants wished to share
Derbyshire Quality Surveillance Group • EMAS Briefing for April 2014
Health Education East Midlands • University Hospitals of Leicester NHS Trust
Acute Trust Information Report
• March 2014 Workforce Intelligence Benchmark Report
• East Midlands Staff Survey 2013 analysis • Triangulation of NHS Workforce, Clinical

PAPER J
Activity and Finance for University Hospitals of Leicester NHS Trust


Blank Page
Paper E East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
GOVERNING BODY MEETING
Front Sheet
REPORT TITLE: Patient Stories: progress report of follow up actions
MEETING DATE: 9 September 2014
REPORT BY: Fiona Fretter, Quality Lead
SPONSORED BY: Carmel O’Brien, Chief Nurse and Quality Officer
PRESENTER: Carmel O’Brien, Chief Nurse and Quality Officer
PURPOSE OF THE REPORT:
The report sets out the actions taken following the presentation of Patient Stories at the East Leicestershire and Rutland Governing Body meetings.
RECOMMENDATIONS:
The East Leicestershire and Rutland CCG Governing Body is requested to: RECEIVE the report for information.
REPORT SUPPORTS THE FOLLOWING STRATEGIC AIM(S) 2013 – 2014: Transform services and enhance quality of life for people with long-term conditions
Improve integration of local services between health and social care; and between acute and primary/community care.
Improve the quality of care – clinical effectiveness, safety and patient experience
Listening to our patients and public – acting on what patients and the public tell us.
Reduce inequalities in access to healthcare Living within our means using public money effectively
Implementing key enablers to support the strategic aims (e.g. constitutional and governance arrangements, communications and patient engagement).
EQUALITY ANALYSIS
Equality Analysis has not been completed as part of Committee summary report.
RISK ANALYSIS AND LINK TO BOARD ASSURANCE FRAMEWORK:
Links to Board Assurance Framework Reference: 3.1 and 6.4.

Paper E East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
GOVERNING BODY MEETING
Patient Stories: progress report of follow up actions INTRODUCTION 1. By showing patient stories at the ELR CCG Governing Body meeting, the CCG is
able to support our aim of keeping the patient voice at the heart of everything we do. The power of hearing a patient story told in the patient’s own word can spark clinical discussion at governing body meetings and allow the governing body to think more creatively about the services being commissioned.
2. Patient stories are real life accounts of a patient’s experience, given in their own words. Patients are filmed telling their story, from their point of view, explaining the different interactions they had throughout their journey, and what went well and what could have been done better throughout their experience.
3. Patient story films are shown at the public section of the governing body meeting,
with specific time allowed for clinical discussion following the presentation. During these discussions, pathway changes or actions for providers may be identified, these are then fed back to providers or commissioning colleagues.
4. Appendix 1 provides a summary of the patient stories presented since these were
introduced in October 2013, it highlights the issues identified and progress against follow up actions.
5. It should be noted that some actions require longer term oversight as they relate
to integration agenda and some pathway development which will be taken through the Better Care Together Work streams.
Recommendation: The East Leicestershire and Rutland CCG Governing Body is requested to: RECEIVE the report and note progress to date

Appendix 1
Summary of follow up actions following presentation of Patient Stories to ELRCCG Governing Body Month Story Issues identified Progress October 2013 A patient story relating to
infection control and clostridium difficile spanning the patient journey from primary to secondary care.
The patient in the DVD was not happy with the care received at various points in the journey. The importance of GPs capturing this feedback and to better encourage that the patient voice is heard was noted. The excellent care seen on some wards in the DVD was noted. The significance of building on the learning from good areas and sharing learning across poorer areas was discussed.
A Leicester, Leicestershire and Rutland health economy clostridium difficile action plan is now in place to across health and social care to improve clinical outcomes for patients diagnosed clostridium difficile. ELR CCG also has an individual action plan to support the aims and objectives of the LLR action plan and support further reduction of clostridium difficile infections and support clinical outcomes for patients. A number of additional programmes have also been introduced, including antibiotic prescribing audits in primary care. The re-launch of the Reporting of Poor Quality Care system means that GPs are now able to easily log concerns about the experiences of their patients. These concerns are then investigated by providers, and analysed to share learning across the health community and make improvements in the quality of care.
December-13 The story captures the experience of an elderly gentleman who sustained a fractured neck of femur and describes his experience in hospital on Ward 32
Ward based packs for patients and carers have been introduced including information on bus routes and visiting times. A full time activities coordinator to engage with patients with dementia is now in place Six wards at Leicester Royal Infirmary have now received the Elder Friendly Quality Mark in recognition of the high quality of

Appendix 1
Summary of follow up actions following presentation of Patient Stories to ELRCCG Governing Body care they provide to older people. The wards received the mark after patients aged 65 and over answered questions on the quality of care, comfort, food and drink, support from staff as well as privacy and dignity.
March 2014 The story was about a self-harm patient who talks about the level of support they previously received in their home town and the support they currently receive after moving to Leicestershire.
The patient explained that in Hull, they had access to a self-harm team who would provide support in times of need, however in Leicestershire this service was not provided and the patient found this difficult. The patient described very positively the support received from her GP practice.
Commissioners recognised that there appeared to be a lack of continuity of care in relation to crisis and home treatment, which is imperative to mental health patients. As part of the Mental Health Pathway redesign, it has been noted that the current Crisis and Home Treatment Service is not focussed on crisis treatment, many patients going through the service do not necessarily need to be treated at this point of the pathway. The redesign aims for less demand on the crisis response home treatment service, correct staffing levels for the service and increased continuity of care for patients. Some of the changes include:
- The Crisis House is due to open shortly, providing 4 to 6 inpatient beds and a drop in facility for patients in crisis, meaning that patients have somewhere short term to go to during a crisis.
- Discussions are taking palace about the development of an urgent outpatient and GP Hotline providing access to advice from LPT psychiatrists for GPs with patients in

Appendix 1
Summary of follow up actions following presentation of Patient Stories to ELRCCG Governing Body crisis. This will enable GPs to be equipped to deal with more patients in crisis, reducing pressure on the CRHT service.
- Staffing requirements are being considered as part of the review, to ensure that staffing levels allow the service to achieve the Crisis Concordat, namely that all patients in a crisis are seen within 24 hours.
- A post inpatient admission step down facility will monitor patients before discharge, resulting in more bed availability at the main inpatient sites and support to patients post admission before being discharged into the community.
May-14 The story of a child who, as a
result of being deprived of oxygen at birth, suffered from serious disabilities. The story was told from the point of view of the mother and the impact of her daughter’s disability on the family.
The mother in the video noted how difficult it was sometimes, having to attend numerous appointments with different clinicians. It was suggested that it may be helpful to look towards a care coordinator role.
Leicestershire Partnership Trust are now progressing an integrated community model, working by locality with other professionals, including education and social care. The Better Care Together strategy includes an integration model between acute and community paediatricians. Both of these initiatives will result in more coordinated care for families with children with complex conditions, and therefore a better experience of care.
July-14 The story focused on the care a patient received following diagnosis of Bowel Cancer and
The story highlighted the lack of coordination of services when moving through the
A copy of the patient story DVD was shared with the Chief Nurse of the provider, along with a summary of the board discussion.

Appendix 1
Summary of follow up actions following presentation of Patient Stories to ELRCCG Governing Body their journey from screening, diagnosis to treatment.
healthcare system. Poor quality care on specific wards was also identified.
The provider has confirmed that actions are being taken to progress the issues identified. As a CCG we recognised that there are still issues in managing coordinated care across different providers and there is work in progress about managing cross border issues.


Blank Page

Paper F East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
1
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
GOVERNING BODY MEETING
Front Sheet
REPORT TITLE: Performance Assurance Report
MEETING DATE: 9 September 2014
REPORT BY: Alison Buteux, Performance Manager, GEM
SPONSORED BY: Jane Chapman, Chief Strategy & Planning Officer
PRESENTER: Jane Chapman, Chief Strategy & Planning Officer
PURPOSE OF THE REPORT: This report provides an overview of performance for East Leicestershire & Rutland CCG and LLR where data is available for July 2014.
RECOMMENDATIONS: The East Leicestershire and Rutland CCG Board is requested to: NOTE the contents of the report.
REPORT SUPPORTS THE FOLLOWING STRATEGIC AIM(S) 2014 – 2015: Transform services and enhance quality of life for people with long-term conditions
Improve integration of local services between health and social care; and between acute and primary/community care
Improve the quality of care – clinical effectiveness, safety and patient experience
Listening to our patients and public – acting on what patients and the public tell us
Reduce inequalities in access to healthcare Living within our means using public money effectively
Implementing key enablers to support the strategic aims (e.g. constitutional and governance arrangements, communications and patient engagement)
EQUALITY ANALYSIS An Equality Analysis and due regard to the positive general duties of the Equality Act 2010 has not been undertaken in the development of this report as it is judged that it is not proportionate on the basis that the Performance Assurance reporting underpins the commissioning strategy and priorities of the CCG.
This completes the due regard required.
RISK ANALYSIS AND LINK TO BOARD ASSURANCE FRAMEWORK: This report aligns to “1.1 Failure to meet performance against targets due to limited capacity to deliver resulting in deteriorating position and inability to demonstrate good performance.

Paper F East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
2
EAST LEICESTERSHIRE AND RUTLAND CCG
BOARD MEETING
Performance Assurance Report July 2013/14
INTRODUCTION
1. As part of the new performance and planning cycle for 2014/2015, guidance has been published by NHS England. This guidance ensures that service levels are maintained or improved following local strategic intentions, and standards or targets are in place. It provides the focus for NHS England’s Area Team assurance process during the year.
2. The performance report is the vehicle to ensure that an appropriate governance and assurance process is in place for CCGs. It focuses on a set of dashboards covering:
Everyone Counts Guidance NHS Outcomes Framework Quality Premium
3. Where standards or targets are not being achieved, these high risk exceptions will
be documented in depth, including monthly performance levels and actions being undertaken either by service providers, commissioners or CCGs.
HIGH RISK EXCEPTIONS 2014/15
4. The high risk exceptions (appendix one) highlight those indicators that are “red” or “amber” from Everyone Counts, NHS Outcomes Framework, and Local Priority. This report provides delivery actions against each. These are outlined within the relevant sections of this report.
EVERYONE COUNTS DASHBOARD
5. There are 39 indicators within Everyone Counts. The local priority indicator has been removed from everyone counts and is listed separately below. At July 2014 the position is as follows:
B G A R
8 14 8 9Indicator RAG Rated for July 14
Last month’s position was as follows:
B G A R
9 19 3 8Indicator RAG Rated for June 14

Paper F East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
3
6. 8 indicators are rated as “blue” as data is not yet available. This is due to either the timeliness of the data or the indicator is in development.
6 indicators have changed ratings from last month;
Composite measure on avoidable emergency admissions moved from
blue to red;
Cancer 31 Day Waits - patients receiving subsequent treatment for cancer within 31 days where that treatment is radiotherapy treatment course, moved from green to amber;
Cancer 62 Day Waits - % of patients receiving first definitive treatment for
cancer within 62 days of an urgent GP referral for suspected cancer, moved from green to amber; and
EMAS Red 1, Red 2 and A19 indicators have moved from green to amber. 14 indicators are rated as “green” and are as follows:
Friends and family; IAPT recovery; MRSA & CDIFF; RTT non-admitted and incomplete pathways; Diagnostic test waiting time; Cancer 31 waits for surgery & drug regimen; Cancer 62 day wait to upgrade their priority status; Care programme approach (CPA); 52 week RTT; 12 hour trolley waits in A&E; and Urgent ops cancelled for a second time.
9 indicators are rated as “red” and 8 are rated as amber. The following provides an update on the actions against the ‘red’ and ‘amber’ indicators for 2014/15 activity.
Indicator Action in Place IAPT Access – 13.8% against 16% target. (July 14 YTD) Red
Performance for July has improved. DNA text reminders have now been implemented and 2 pilot self-referrals have been started in Melton Mowbray. Additional initiatives are due to be brought forward to develop the service further and to aid in the number of referrals being generated in order to achieve the target.Clinical time has been increased to 22 hours to absorb additional demand. A full telephone triage system will be operational by November due to infrastructure remodelling. Additionally the service will be implementing self-referrals for older people via Age concern in Q3. Additional opportunities are being investigated with 'Clash' (Community Leicester Arthritis group), Dementia Carers Group and 'Breathe Easy'.

Paper F East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
4
Indicator Action in Place Composite measure on avoidable emergency admissions of - Unplanned hospitalisation for chronic ambulatory care sensitive conditions Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s Emergency admissions for acute conditions that should not usually require hospital admission Emergency admissions for children with lower respiratory tract infections (LRTI) 1692.3 against 1438.0 (May 14 FOT)
This is a new indicator for 14/15. The monthly standard has been based on 1/12th of the annual target only. Actions to be provided next month.
RTT - Admitted patients to start treatment within a maximum of 18 weeks from referral 83.0% against 90% target. (June 14 YTD) Red
Overall performance against recovery plan is monitored by the RTT Working Group (UCWG), chaired by Dr Simon Freeman, MD Leicester City CCG. Actions underway include (1) Expanding the weekly monitoring to incorporate the additional measures needed to recover bottom line position by end August for delivery in September and refresh overarching plans (2) The establishment of a task and finish group to reduce all backlogs for all specialties (except orthopaedics and general surgery) - including pushing ophthalmology and ENT further than previously agreed in RAP (3) Additional activity being moved by sub-contracting and point of referral to IS and other NHS providers for Adult Ophthalmology, General Surgery and Orthopaedics (5) 4 additional validation staff now in post.
UHL A&E 4 Hour Wait – 88.52% against 95% target. (YTD 18/08/14) Red
Performance has shown an improvement during the first part of August with YTD position at 87.04%. The work of Dr Ian Sturgess is undertaking with UHL and wider system through clinical engagement appears to be having an impact. Work on inflow and discharge continues to support system change. The breaches are predominantly due to bed availability or ED process. There has been a reduction in the numbers of patients waiting for a bed each morning which has positively impacted on flow.

Paper F East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
5
Indicator Action in Place Cancer 2 Week Wait - % of patients seen within two weeks of an urgent GP referral for suspected cancer (All Providers) 92.9% against 93% target (June 14 YTD) Amber Cancer 2 Week Wait - % of patients seen within two weeks of an urgent referral for breast symptoms where cancer is not initially suspected (All Providers) 91.8% against 93% target (June 14 YTD) Amber Cancer 31 Day Waits - % of patients receiving first definitive treatment within 31 days of a cancer diagnosis (All Providers) 91.2% against 96% target (June 14 YTD) Amber Cancer 31 Day Waits - % of patients receiving subsequent treatment for cancer within 31 days where that treatment is radiotherapy treatment course (All Providers) 93.0% against 94% target (June 14 YTD) Amber Cancer 62 Day Waits - % of patients receiving first definitive treatment for cancer within 62-days of an urgent GP referral for suspected cancer (All Providers) 83.9% against 85% target (June 14 YTD) Amber
Cancer 62 Day Waits - % of patient receiving first definitive treatment for cancer within 62 days of referral from an NHS Cancer Screening Service (All Providers) 72.4% against 90% target (June 14 YTD) Red
Two biggest areas of risk due to volumes are breast and gynaecology. No buffer within clinics to gain extra capacity as all cancer patients. In addition to the current Cancer Board a weekly cancer action meeting has recently been formed. Individual patient breaches and potential breaches are also being investigated and a new way of patient tracking list (PTL) Management has been implemented via the Cancer Action Board with individual tumour sites reporting. Patients are being treated in breach date order. Extra consultant resource and theatre time has been sourced.
EMAS Category A (Red 1) 8 minute response time 73.84% against 75% target (July 14 YTD) Amber Category A (Red 2) 8 minute response time 74.34% against 75% target (July 14 YTD) Amber Category A 19 minute transportation time 94.75% against 95% target (July 14 YTD) Amber
The existing Performance Management (weekly quality/performance meeting plus weekly assurance meeting) and Governance (Partnership Board [PB], Collaborative Commissioning Meeting [CCM], Quality Assurance Group [QAG], and Finance Information Group [FIG]) arrangements are on-going for 2014/15. EMAS have focused their resources on delivering the targets and in April achieved this at Trust level in line with the contract. Performance for EMAS as a whole in June has improved but still failed to meet target in July. Handover continues to be a major issue

Paper F East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
6
Indicator Action in Place but UHL and EMAS are working together to
address issues impacting on handover. We have been advised by EMAS that additional factors include a general increase across the system in relation to call volumes reflected in their escalation status, evidence of this will be requested for the next EMAS Locality meeting. At a meeting with EMAS on the 25th June EMAS advised Commissioners that they were undertaking further recruitment and were addressing the issues with Handover and Turnaround which together would assist with performance. EMAS is continuing its’ major recruitment drive although this will not produce required productivity increase until beginning Q3 which means that the requirement to achieve targets by 1st July 2014 has not been met. Fines/Penalties are limited to activity/performance post Q3 as per contract provisions. Therefore there are no financial implications to EMAS at present.
Mixed Sex Accommodation 4 against zero tolerance target (June 14 YTD)
Breaches occurred in April & May for EL&R CCG.
Cancelled Operations - % of patients readmitted within 28 days. 95.0% against a target of 100%. (June 14 YTD) Red
A new standard to contact the patient within 48 hrs of cancellation and rebook TCI date within 21 days has been initiated with associated escalation processes. Daily cancelled operations patient level report will be e-mailed via automated route to service and operational managers, highlighting 21 day re-book date. Weekly monitoring of performance against Trust 21 day and national 28 day standard, capturing of reasons for failure against the standard. Escalation of all at risk patients for 28 day re-booking to CMG Clinical Directors and General Managers. Embedding cancellation operations policy – theatre booking/planning incrementally to 6 weeks – review actual booking of patients >3 weeks in advance. Dedicated project manager appointed.
Handover times between ambulance & A&E within 30 mins. 16.4% against a zero tolerance target (June 14 YTD) Red Handover times between ambulance & A&E within 60 mins. 3.1% against a zero tolerance target (June 14 YTD) Red
Activity has seen significant increase of circa 20-25% activity from NHS 111. EL&R EMAS contract manager to work collaboratively with EMAS, NHS 111 provider and contract manager to understand why and what actions can be undertaken. Performance for EMAS as a whole in June has improved but still fails to meet KPIs. Handover continues to be a major issue but UHL and EMAS are working together to

Paper F East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
7
Indicator Action in Place address issues impacting on handover.
EMAS is continuing its’ major recruitment drive although this will not produce required productivity increase until beginning Q3 which means that the requirement to achieve targets by 1st July 2014 has not been met. Fines/Penalties are limited to activity/performance post Q3 as per contract provisions. Therefore there are no financial implications to EMAS at present. Joint investigation about data for Hear and Treat for 2013/14 and beginning of 2014/15 is underway due to concerns as to the coding issues compromising last year’s figures.
CCG LOCAL PRIORTY KPI
7. For 14/15 there is one local key performance indicator, which was set by the CCG as part of the planning round. This is deaths at usual place of residence measured through deaths at home, nursing homes, residential homes and hospices. Deaths data is provided by the Local Authority, most recent data provided is April 13-Feb 14. This is currently achieving target at 49.8% against 48.5% target as at February 14. Due to data sharing ceasing between ONS and Public Health, no updated deaths data has been received. Public Health continues to chase ONS for agreement to be reconnected.
NHS OUTCOMES FRAMEWORK
8. There are 65 indicators within the NHS outcomes framework: 11 indicators are rated “green” and are as follows:
IAPT entering treatment; Unplanned admissions for asthma, diabetes; MRSA & CDIFF; 4 PROMS (health gain as assessed by patients for elective procedures); Emergency admissions from children with lower respiratory tract infections
(LRTI); Friends and family test; and Access to NHS dental services
6 indicators are rated as “red” and are as follows;
Employment of people with long term conditions (The difference in employment rate between England population and people with a long term condition);
Unplanned hospitalisation for chronic ambulatory care sensitive conditions;
Employment of people with mental illness (The difference in employment rate between England population and people with mental illness);

Paper F East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
8
Emergency admissions for acute conditions that should not usually require hospital admission;
Overall experience of NHS Dental Services; and Access to GP Services.
The remaining indicators are “blue, this is because the KPIs are nationally in development and waiting for further guidance.
QUALITY PREMIUM 2014/15
9. As at July 14, 6 indicators have data available and are as follows: 3 are rated as “red” for IAPT access, composite measure for avoidable emergency admissions and A&E waits; 2 are rated as amber for cancer 2 week waits from urgent GP referral to first out-patient appointment and EMAS red 1; 1 is rated green for RTT incomplete pathways. The remaining indicators are “blue”. This is because the KPIs are nationally in development and waiting for further guidance, data will be reported when this becomes available.
RECOMMENDATIONS: The Governing Board is requested to NOTE the contents of the report.

EAST LEICESTERSHIRE & RUTLAND CCG
Governing Body Performance Report, August 2014
(Reporting period - July 2014)
1

TABLE OF CONTENTS
SECTION 1 HIGH RISK EXCEPTIONS
IAPT Entering treatment 3‐8
Composite measure on avoidable emergency admissions
RTT 18 week admitted patients
A&E four hour waits
Cancer 2 week wait ‐ urgent GP referral for suspected cancer
Cancer 2 week wait ‐ urgent referral for breast symptoms where cancer is not initially suspected
Cancer 2 week wait ‐ urgent referral for breast symptoms
Cancer 31 day ‐ patients receiving first definitive treatment within 31 days of a cancer diagnosis
Cancer 31 day ‐ patients receiving subsequent treatment for cancer within 31 days where that
treatment is radiotherapy treatment course
Cancer 62 day wait ‐ patients receiving first definitive treatment for cancer within 62‐days of an
urgent GP referral for suspected cancer
Cancer 62 day wait ‐ first definitive treatment from NHS Cancer Screening Service
EMAS ‐ EMAS Category A (Red 1) 8 minutes, (Red 2) 8 miniutes and Cat A 19 minutes
Mixed Sex Accommodation
Cancelled Ops ‐ not readmitted within 28 days
Ambulance handover time ‐ Number of handover delays of over 30 minutes
Ambulance handover time ‐ Number of handover delays of over 1 hour
2

SECTION 1
B G A R
8 14 8 9 39 39 39
IndicatorQuality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
IAPT See above 16% N/A Jul‐14 13.8%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 15% 15% 15% 15% 15% 15% 15% 15% 15% 15% 15% 15% 15%
EL&R Patients 12.2% 12.8% 12.7% 12.7% 12.7% 13.0% 14.0% 14.3% 13.9% 14.6% 14.5% 14.5% 14.3%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 16% 16% 16% 16% 16% 16% 16% 16% 16% 16% 16% 16% 16%
EL&R Patients 12.6% 14.8% 11.4% 16.0% 13.8%
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Composite measure on avoidable
emergency admissions
1438.0
(119.8 per
month)
N/A
FOT based
on YTD May
14
1692.3
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan
EL&R Patients for all providers 131.2 133.4 117.1 128.4 108.7 117.4 136.5 134.0 161.2 149.0 143.1 152.7 1612.7
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 119 119 119 119 119 119 119 119 119 119 119 119 1438
EL&R Patients for all providers 145.6 136.5 1692.3
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
RTT ‐ Admitted patients to start
treatment within a maximum of 18
weeks from referral
See above 90% 85% Jun‐14 83.0%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
EL&R patients at all providers 90.8% 92.6% 89.6% 91.1% 89.5% 86.4% 87.2% 87.6% 86.4% 86.5% 85.4% 84.2% 88.1%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
EL&R patients at all providers 82.7% 82.2% 84.0% 83.0%
EA3: IAPT
Indicator2014/15
Indicator2013/14
Definition: Admitted patients to start treatment within a maximum of 18 weeks from referral (All providers at EL&R CCG level)
Indicator2013/14
Actions: Performance for July has improved. Did not attend "DNA" text reminder have now been implemented and two pilot self‐referrals have been started in Melton Mowbray. Additional
initiatives are due to be brought forward to develop the service further and to aid in the number of referrals being generated in order to achieve the target. Clinical time has been increased to
22 hours to absorb additional demand. A full telephone triage system will be operational by November due to infrastructure remodelling. Additionally the service are will be implementing self
referrals for older people via Age concern in Q3. Additional opportunities are being investigated with 'Clash' (Community Leicester Arthritis group), Dementia Carers Group and 'Breathe Easy'.
Definition: Composite indicator of ‐Unplanned hospitalisation for chronic ambulatory care sensitive conditions ‐ Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s ‐Emergency admissions
for acute conditions that should not usually require hospital admission ‐Emergency admissions for children with lower respiratory tract infections (LRTI)
Indicator2013/14
Indicator2014/15
Actions: This is a new indicator for 14/15. The monthly standard has been based on 1/12th of the annual target only. Actions to be provided next month.
New Measure for 2014/15
EB1: RTT Admitted Patients
PERFORMANCE ASSURANCE FRAMEWORK 2014/15
EAST LEICESTERSHIRE & RUTLAND CLINICAL COMMISSIONING GROUP
EVERYONE COUNTS KEY PERFORMANCE INDICATORS ‐ HIGH RISK EXCEPTIONS 2014/15
Indicator RAG Rated for July 14
Actions: Overall performance against recovery plan is monitored by the RTT Working Group (UCWG), chaired by Dr Simon Freeman, MD Leicester City CCG. Actions underway include (1)
Expanding the weekly monitoring to incorporate the additional measures needed to recover bottom line position by end August for delivery in September and refresh overarching plans (2) The
establishment of a task and finish group to reduce all backlogs for all specialties (except orthopaedics and general surgery) ‐ including pushing ophthalmology and ENT further than previously
agreed in RAP (3) Additional activity being moved by sub‐contracting and point of referral to IS and other NHS providers for Adult Ophthalmology, General Surgery and Orthopaedics (5) 4
additional validation staff now in post.
EA4: Composite measure on avoidable emergency admissions
Definition: IAPT Access ‐ Proportion of people that enter treatment against the level of need in the general population
Indicator2014/15
3

SECTION 1
PERFORMANCE ASSURANCE FRAMEWORK 2014/15
EAST LEICESTERSHIRE & RUTLAND CLINICAL COMMISSIONING GROUP
EVERYONE COUNTS KEY PERFORMANCE INDICATORS ‐ HIGH RISK EXCEPTIONS 2014/15
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
A&E Waiting Time ‐ % of people who
spend 4 hours or less in A&E See above
Zero
Tolerance90%
as at
18/08/1488.52%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
% of people who spend 4 hours or less
in A&E81.86% 88.29% 85.16% 90.27% 88.90% 89.50% 91.85% 88.18% 90.03% 93.58% 76.07% 89.31% 88.37%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
% of people who spend 4 hours or less
in A&E86.92% 83.12% 91.02% 92.52% 88.52%
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Cancer 2 Week Wait ‐ % of patients
seen within two weeks of an urgent GP
referral for suspected cancer
See above 93% 88% Jun‐14 92.9%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93%
EL&R patients at all providers 94.0% 95.4% 94.2% 94.3% 94.7% 92.7% 95.3% 95.8% 95.2% 94.8% 95.6% 94.5% 94.7%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93%
EL&R patients at all providers 89.3% 94.9% 94.6% 92.9%
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Cancer 2 Week Wait ‐ % of patients
seen within two weeks of an urgent
referral for breast symptoms where
cancer is not initially suspected
See above 93% 88% Jun‐14 91.8%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93%
EL&R patients at all providers 98.0% 93.8% 94.4% 94.4% 96.4% 96.8% 91.9% 91.7% 92.3% 95.2% 89.9% 96.1% 94.1%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93%
EL&R patients at all providers 80.0% 96.3% 97.0% 91.8%
Definition: % of patients seen within two weeks of an urgent referral for breast symptoms where cancer is not initially suspected
Indicator2013/14
EB6: Cancer 2 Week wait
Definition: % of patients seen within two weeks of an urgent GP referral for suspected cancer
Indicator2013/14
Indicator
Actions: Two biggest areas of risk due to volumes are breast and gynaecology. No buffer within clinics to gain extra capacity as all cancer patients. In addition to the current Cancer Board a
weekly cancer action meeting has recently been formed. Individual patient breaches and potential breaches are also being investigated and a new way of PTL Management has been
implemented via the Cancer Action Board with individual tumour sites reporting. Patients are being treated in breach date order. Extra consultant resource and theatre time has be sourced.
EB7: Cancer 2 Week wait
2014/15
Actions: Performance has shown an improvement during the first part of August with YTD position at 87.04%. The work of Dr Ian Sturgess is undertaking with UHL and wider system through
clinical engagement appears to be having an impact. Work on inflow and discharge continues to support system change. The breaches are predominantly due to bed availability or ED process.
There has been a reduction in the numbers of patients waiting for a bed each morning which has positively impacted on flow.
Indicator
EB5: A&E Four Hour Waiting TimeDefinition: % Patients should be admitted, transferred or discharged within 4 hours of their arrival at an A&E department
Indicator2013/14
2014/15
Indicator2014/15
Actions: As above
4

SECTION 1
PERFORMANCE ASSURANCE FRAMEWORK 2014/15
EAST LEICESTERSHIRE & RUTLAND CLINICAL COMMISSIONING GROUP
EVERYONE COUNTS KEY PERFORMANCE INDICATORS ‐ HIGH RISK EXCEPTIONS 2014/15
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Cancer 31 Day Waits ‐ % of patients
receiving first definitive treatment
within 31 days of a cancer diagnosis
See above 96% 91% Jun‐14 91.2%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96%
EL&R patients at all providers 98.1% 95.4% 98.4% 99.3% 99.2% 99.2% 98.5% 94.6% 100.0% 96.7% 100.0% 98.5% 98.2%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96%
EL&R patients at all providers 97.2% 88.8% 89.1% 91.2%
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Cancer 31 Day Waits ‐ % of patients
receiving subsequent treatment for
cancer within 31 days where that
treatment is radiotherapy treatment
course
See above 94% 89% Jun‐14 93.0%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94%
EL&R patients at all providers 100.0% 100.0% 98.0% 100.0% 100.0% 100.0% 95.5% 98.0% 100.0% 94.6% 96.3% 97.9% 98.2%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94%
EL&R patients at all providers 95.1% 93.9% 90.0% 93.0%
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Cancer 62 day wait ‐ % of patients
receiving first definitive treatment for
cancer within 62‐days of an urgent GP
referral for suspected cancer
See above 85% 80% Jun‐14 83.9%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85%
EL&R patients at all providers 81.4% 77.4% 83.3% 83.1% 80.6% 87.9% 84.2% 90.9% 88.7% 85.7% 87.1% 86.7% 84.7%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85%
EL&R patients at all providers 92.2% 90.5% 73.4% 83.9%
Indicator2014/15
Actions: As above
Indicator2013/14
EB7: Cancer 31 day wait
Definition: % of patients receiving first definitive treatment within 31 days of a cancer diagnosis
Indicator2013/14
Indicator2014/15
Actions: As above
EB11: Cancer 31 day wait
Definition: % of patients receiving subsequent treatment for cancer within 31 days where that treatment is radiotherapy treatment course
Indicator2014/15
Actions: As above
EB12: Cancer 62 Day Waits
Definition: % of patients receiving first definitive treatment for cancer within 62‐days of an urgent GP referral for suspected cancer
Indicator2013/14
5

SECTION 1
PERFORMANCE ASSURANCE FRAMEWORK 2014/15
EAST LEICESTERSHIRE & RUTLAND CLINICAL COMMISSIONING GROUP
EVERYONE COUNTS KEY PERFORMANCE INDICATORS ‐ HIGH RISK EXCEPTIONS 2014/15
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Cancer 62 Day Waits ‐ % of patient
receiving first definitive treatment for
cancer within 62 days of referral from
an NHS Cancer Screening Service
See above 90% 85% Jun‐14 72.4%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
EL&R patients at all providers 100.0% 95.0% 100.0% 92.9% 100.0% 77.8% 100.0% 96.8% 95.0% 100.0% 100.0% 85.7% 94.8%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
EL&R patients at all providers 86.7% 68.8% 66.7% 72.4%
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Category A (Red 1) 8 minute response
time See above 75% 70% Jul‐14 73.84%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75%
Category A (Red 1) 8 minute response
time71.20% 75.28% 77.63% 72.98% 69.27% 68.82% 69.04% 69.45% 66.22% 72.52% 68.68% 73.95% 71.26%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75%
Category A (Red 1) 8 minute response
time76.21% 73.97% 75.01% 70.71% 73.84%
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Category A (Red 2) 8 minute response
timeSee above 75% 70% Jul‐14 74.34%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75%
EL&R patients at all providers 75.39% 76.81% 75.05% 71.67% 70.43% 68.62% 69.16% 68.28% 65.52% 71.56% 69.77% 74.92% 71.46%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75%
EL&R patients at all providers 77.02% 74.59% 75.27% 71.60% 74.34%
EB13: Cancer 62 Day Waits
Definition: % of patient receiving first definitive treatment for cancer within 62 days of referral from an NHS Cancer Screening Service
Indicator2013/14
Indicator2014/15
Indicator2013/14
Indicator2014/15
Indicator2013/14
Indicator2014/15
Actions: As above
EB15 i: EMAS Category A (Red 1) 8 minute response time
EB15 ii: Category A (Red 2) 8 minute response time
Definition: Category A Red 1 incidents: presenting conditions that may be immediately life threatening and the most time critical and should receive an emergency response within 8 minutes irrespective of
location in 75% of cases.
Definition: Category A Red 2 incidents: presenting conditions that may be immediately life threatening but less time critical than Red 1 and should receive an emergency response within 8 minutes irrespective of
location in 75% of cases.
Actions: The existing Performance Management (weekly quality/performance meeting plus weekly assurance meeting) and Governance (Partnership Board [PB], Collaborative Commissioning
Meeting [CCM], Quality Assurance Group [QAG], and Finance Information Group [FIG]) arrangements are on‐going for 2014/15.
EMAS have focused their resources on delivering the targets and in April achieved this at Trust level in line with the contract. Performance for EMAS as a whole in June has improved but still
failed to meet target in July. Handover continues to be a major issue but UHL and EMAS are working together to address issues impacting on handover. We have been advised by EMAS that
additional factors include a general increase across the system in relation to call volumes reflected in their escalation status, evidence of this will be requested for the next EMAS Locality
meeting. At a meeting with EMAS on the 25th June EMAS advised Commissioners that they were undertaking further recruitment and were addressing the issues with Handover and
Turnaround which together would assist with performance. EMAS is continuing its’ major recruitment drive although this will not produce required productivity increase until beginning Q3
which means that the requirement to achieve targets by 1st July 2014 has not been met. Fines/Penalties are limited to activity/performance post Q3 as per contract provisions. Therefore
there are no financial implications to EMAS at present.
Actions: As above
6

SECTION 1
PERFORMANCE ASSURANCE FRAMEWORK 2014/15
EAST LEICESTERSHIRE & RUTLAND CLINICAL COMMISSIONING GROUP
EVERYONE COUNTS KEY PERFORMANCE INDICATORS ‐ HIGH RISK EXCEPTIONS 2014/15
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Category A 19 minute transportation
timeSee above 95% 90% Jul‐14 94.75%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Category A 19 minute transportation
time93.06% 94.51% 94.40% 92.91% 93.18% 92.91% 94.00% 93.54% 92.74% 94.65% 94.21% 95.52% 93.82%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Category A 19 minute transportation
time96.01% 95.09% 95.27% 93.22% 94.75%
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Mixed Sex Accommodation (MSA)
Breaches See above
Zero
ToleranceN/A Jun‐14 4
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 0 0 0 0 0 0 0 0 0 0 0 0 0
EL&R patients MSA breaches 0 0 0 0 0 0 0 0 1 0 0 1 2
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 0 0 0 0 0 0 0 0 0 0 0 0 0
EL&R patients MSA breaches 3 1 0 4
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Cancelled Operations ‐
% of patients not re‐admitted within
28 days at UHL level
See above 100% N/A Jun‐14 95.0%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
% readmitted in 28 days at UHL92% 90% 86% 99% 96% 98.5% 98.3% 97.6% 94.3% 94.3% 98.8% 94.2% 95.1%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
% readmitted in 28 days at UHL90.6% 96.1% 99.0% 95.0%
Actions: A new standard to contact the patient within 48 hrs of cancellation and rebook TCI date within 21 days has been initiated with associated escalation processes. Daily cancelled
operations patient level report will be e‐mailed via automated route to service and operational managers , highlighting 21 day re‐book date. Weekly monitoring of performance against Trust
21 day and national 28 day standard, capturing of reasons for failure against the standard. Escalation of all at risk patients for 28 day re‐booking to CMG Clinical Directors and General
Managers. Embedding cancellation operations policy – theatre booking/planning incrementally to 6 weeks – review actual booking of patients >3 weeks in advance. Dedicated project
manager appointment.
Indicator
2013/14
Definition: All providers of NHS funded care are expected to eliminate mixed sex accommodation, except where it is in the overall best interest for the patient, in accordance with the definitions.
Indicator
2014/15
Indicator2013/14
Actions: Breaches occurred in April & May for EL&R CCG.
Indicator2014/15
Actions: As above
Definition: Category A incidents: Presenting conditions, which may be immediately life threatening and should receive an ambulance response at the scene within 19 minutes irrespective of location in 95% of
cases.
EB16: Category A 19 minute transportation time
Indicator2013/14
EBS1: Mixed Sex Accommodation
Indicator2014/15
EBS2: Cancelled OperationsDefinition: % of patients not readmitted within 28 days
7

SECTION 1
PERFORMANCE ASSURANCE FRAMEWORK 2014/15
EAST LEICESTERSHIRE & RUTLAND CLINICAL COMMISSIONING GROUP
EVERYONE COUNTS KEY PERFORMANCE INDICATORS ‐ HIGH RISK EXCEPTIONS 2014/15
Indicator
Quality
Premium
Measure
Outcomes
Framew
ork
Description
Standard
Lower
Threshold
Latest
PeriodYTD Trend
Ambulance handover time ‐ Number of
handover delays of over 30 minutes See above
Zero
ToleranceN/A Jul‐14 16.4%
Ambulance handover time ‐ Number of
handover delays of over 1 hour See above
Zero
ToleranceN/A Jul‐14 3.1%
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 0% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0%
Number of handover delays of over 30
minutes11.2% 11.9% 12.2% 13.0%
9.1%
383
10.6%
484
14.1%
705
14.5%
689
15%
722
11.9%
573
18%
818
12.3%
601
12.9%
7075
Number of handover delays of over 1
hour2.6% 1.4% 1.0% 1.3%
0.4%
16
0.5%
21
0.5%
25
1.2%
59
2.1%
102
1.1%
52
4.6%
207
2.3%
111
1.6%
868
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar YTD
Standard/Plan 0% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0%
Number of handover delays of over 30
minutes17.5% 20.2% 14.0% 13.6% 16.4%
Number of handover delays of over 1
hour4.0% 5.0% 1.9% 1.30% 3.1%
Indicator2014/15
Actions: Activity has seen significant increase of circa 20‐25% activity from NHS 111. ELR EMAS contract manager to work collaboratively with EMAS, NHS 111 provider and contract manager
to understand why and what actions can be undertaken.
Performance for EMAS as a whole in June has improved but still fails to meet KPIs. Handover continues to be a major issue but UHL and EMAS are working together to address issues impacting
on handover.
EMAS is continuing its’ major recruitment drive although this will not produce required productivity increase until beginning Q3 which means that the requirement to achieve targets by 1st
July 2014 has not been met. Fines/Penalties are limited to activity/performance post Q3 as per contract provisions. Therefore there are no financial implications to EMAS at present.
Joint investigation about data for Hear and Treat for 2013/14 and beginning of 2014/15 is underway due to concerns as to the coding issues compromising last year’s figures.
EBS7i: Ambulance handover time ‐ Number of handover delays of over 30 minutes
EBS7ii: Ambulance handover time ‐ Number of handover delays of over 1 hour
Indicator2013/14
Definition: The number of handover days of longer than 30 minutes, and of those the number over one hour
8


Blank Page

Paper G East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
1
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
BOARD MEETING
Front Sheet
REPORT TITLE: Finance Report – July 2014 (month 4)
MEETING DATE: 9 September 2014
REPORT BY: Donna Enoux, Deputy Chief Finance Officer
SPONSORED BY: Karen English, Chief Finance Officer
PRESENTER: Karen English, Chief Finance Officer
PURPOSE OF THE REPORT: This report provides an update on the 2014/15 year to date and forecast outturn financial position for East Leicestershire and Rutland Clinical Commissioning Group (ELR CCG)
RECOMMENDATIONS: The ELR CCG Board is requested to:
Receive for information the contents of the report and the appendices attached
REPORT SUPPORTS THE FOLLOWING STRATEGIC AIM(S) 2014 – 2015: Transform services and enhance quality of life for people with long-term conditions
Improve integration of local services between health and social care; and between acute and primary/community care.
Improve the quality of care – clinical effectiveness, safety and patient experience
Listening to our patients and public – acting on what patients and the public tell us.
Reduce inequalities in access to healthcare
Living within our means using public money effectively
Implementing key enablers to support the strategic aims (e.g. constitutional and governance arrangements, communications and patient engagement).
EQUALITY ANALYSIS
An Equality Analysis and due regard to the positive general duties of the Equality Act 2010 has not been undertaken in the development of this report as it is judged that it is not proportionate on the basis that the financial reporting underpins the commissioning strategy and priorities of the CCG. The commissioning strategy and priorities have and continue to be equality impact assessed as the strategy is reviewed and refreshed and this includes the financial plans. This completes the due regard required.

Paper G East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
2
RISK ANALYSIS AND LINK TO BOARD ASSURANCE FRAMEWORK:
This report makes specific reference to ‘Risk 12’ within the Board Assurance Framework regarding UHL over performance and also highlights other main areas of financial risk under the “risks” section.

Paper G East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
3
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP BOARD MEETING
9 SEPTEMBER 2014
Finance Report
Introduction 1. This report provides details of the financial position for East Leicestershire and
Rutland Clinical Commissioning Group (ELR CCG) for month 4 (2014/15). Coloured dots (red, amber, green) indicate comparison of month 4 and month 3 year-end financial positions (worsened, equivalent, improved).
Allocations 2. The overall allocation for ELR CCG at month 4 has decreased by £118k since
month 3 which reflects the recurrent transfer of Armed Forces budget to the Derbys/Notts Area Team. An equivalent value of Armed Forces expenditure is expected to be charged by providers to Derbys/Notts Area Team rather than to the CCG during 2014/15. The current allocation and previous in year movements are detailed in Appendix A.
Financial Performance 3. The budget statement in Appendix B details performance against budget as at 31st
July 2014 and reflects a control total surplus to be carried forward of £1,102k at month 4 and £3,308k at year end which is in line with the financial plan.
Acute Commissioning 4. UHL - The month 4 forecast year to date spend for UHL is £40.9m which reflects
an overspend of £225k against the year to date budget based on the month 3 SLAM report. The forecast outturn position reflects an overspend of £750k against an annual budget of £122m.
5. Out Of County - The month 4 year to date position is mainly based on month 3
monitoring information and demonstrates an overspend of £412k, predominantly in relation to Peterborough & Stamford Hospitals and University Hospitals of Coventry & Warwick. The outturn position for Out of County providers is forecast as breakeven as there is currently not enough information to predict robust performance trends and there

Paper G East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
4
is uncertainty as to how much overspend can be attributed to RTT activity, and therefore potentially offset by RTT funding.
6. Independent Sector - The month 4 year to date position is based on month 3
monitoring information and demonstrates an overspend of £441k, predominantly in relation to Spire Healthcare and Woodland Hospital. These Independent Sector providers are currently forecast to overspend by £688k at year end.
Non-Acute Commissioning
7. The budget for Non-Acute Commissioning (excluding Integrated Care) is £35.3m
year to date and £105.8m annually against which expenditure is currently forecast to overspend by £1,558k and £1,357k respectively. Key areas of underspend and overspend within the net position are as follows:
8. Children’s Complex Care - This area is forecasting an overspend of £65k at month 4 and £44k at year end based on month 4 data and is due to additional unbudgeted cases.
9. Community Equipment - This area is forecasting an underspend of £28k at month 4
which increases to £83k at year end due to the budget phasing. This position is based on month 4 data.
10. Continuing Care – The month 4 year to date over performance is £1,320k and the
forecast outturn position reflects an over performance of £558k for Continuing Healthcare. This reduced over spend by year end reflects the in depth review currently being undertaken to put actions in place to prevent increased spending in future months.
11. Mental Health ECRs - This area is forecasting an overspend of £134k at month 4
and £497k at year end due to the un-budgeted addition of extra patients.
12. LD Pooled budget & Reablement - This area is forecasting an overspend of £55k at month 4 and £218k at year end due to the transitions from children’s to adult’s LD.
Primary Care Commissioning
13. The budget for Primary Care Commissioning is £17.4m year to date and £52.2m
annually against which an underspend of £228k year to date and £1.1m at year end are being reported.

Paper G East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
5
14. GP Prescribing – This area is under spending slightly at month 4 by £92k and by £798k at year end based on 2 months of PPA data.
Infrastructure 15. The infrastructure budgets are showing an underspend of £27k year to date but
are expected to breakeven by year end against the annual budget of £6.9m. The CCG are using the remaining £1m of the £7.9m Running Cost allocation to support Programme budgets during 2014/15.
Reserves 16. The reserves category on Appendix B outlines the following budgets:
Headroom (£7,985k) – 2.50% of the recurrent programme allocation has been set aside to invest in non-recurrent transformation schemes. Although further work is still required to refine the financial values of these schemes (hence currently there is an over commitment of £492k), there has been £1.7m of expenditure already incurred to date across several schemes. Further details of all these schemes are outlined in Appendix C.
Contingency (£1,652k) – 0.50% of the total allocation has been put aside as
a contingency to offset any overspends and in year cost pressures that may arise. Currently the full contingency has been committed in the year to date and year end forecast positions to offset overspends in the acute sector and achieve the required control total surpluses.
Further Efficiencies to be identified (£666k) – this represents the shortfall in
funding that exists within the CCG’s plan at month 4. Work is on-going within the CCG to identify further QIPP schemes or disinvestments that would offset this negative budget.
QIPP 17. The year to date budget for QIPP schemes as at month 4 is £1,566k and the
planned schemes for 2014/15 total £8,970k. The CCG is reporting all QIPP schemes are on target against ytd and forecast outturn positions. Within this total there is an element of unidentified QIPP (971k) for which specific scheme(s) are still to be created. Appendix D outlines the schemes in more detail.

Paper G East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
6
Better Payment Practice Code (BPPC)
18. The BPPC performance for the CCG as at month 4 is shown in Appendix E and demonstrates compliance with the cumulative BPPC 95% targets as follows:
NHS creditors (number) – 98.99% NHS creditors (value) – 99.92% Non NHS creditors (number) – 99.33% Non NHS creditors (value) – 99.38%
GEM Performance 19. The ‘Month End Summary CFO Report’ received from GEM CSU demonstrated all
KPI’s in relation to the finance service specification were achieved during month 3. Statement of Financial Position and Cash flow Statement
20. Appendix F outlines the Statement of Financial Position for ELR CCG as at month 4.
21. Appendix G outlines the Cash flow Statement for ELR CCG for 2014/15.
Risk
22. There are several financial risks that could adversely affect the financial position of the CCG. These are being closely monitored and mitigations being developed to address them. The main risk of over performance within the UHL contract is already reflected in the BAF, but other risks in existence are:
a. Closing the gap of unidentified QIPP b. Continuing Healthcare potential over performance (patient numbers and
costs) and particular cost pressures within palliative care c. Independent sector over performance d. Potential transfer of further funds to Area Team to support Military Health
and Prison expenditure Summary 23. The financial position of ELR CCG demonstrates a control total surplus to be
carried forward of £1,102k at month 4 and £3,308k at year end in line with the financial plan. However it must be noted that there are financial risks attached to the current forecasted position as highlighted in the paragraph above.

Paper G East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
7
Recommendation: The East Leicestershire and Rutland CCG Board is requested to: Receive for information the contents of the report and the appendices attached.

ELR CCG Allocation 2014/15 Appendix A
m1 m2 m3 m4Movement from m1
Recurrent allocation (programme)Recurrent baseline 309,415 309,415 309,415 309,415 0Growth @ 3.59% 11,100 11,100 11,100 11,100 0Inter Authority Transfers actioned after m7 in 2013/14 (1,112) (1,112) (1,112) (1,112) 0Armed Forces Transfer to Derbys & Notts AT (118) (118)Total recurrent allocation (programme) 319,403 319,403 319,403 319,285
Non recurrent allocation (programme)Return of previous year surplus 3,047 3,047 3,047 3,047 0GP IT 812 812 812Total non recurrent allocation (programme) 3,047 3,047 3,859 3,859
Total allocations (programme) 322,450 322,450 323,262 323,144
Recurrent allocation (running costs)Recurrent baseline 7,770 7,770 7,770 7,770 0Growth 93 93 93 93 0Total allocations (running costs) 7,863 7,863 7,863 7,863
TOTAL ALLOCATIONS 330,313 330,313 331,125 331,007 694

East Leicestershire & Rutland CCG Summary Month 4 Appendix B
Budget (£) Expenditure (£) Variance (£) Budget (£) Expenditure (£) Variance (£)
AllocationsProgramme allocation 108,556,139 108,556,139 0 323,144,000 323,144,000 0Running Costs allocation 2,620,867 2,620,867 0 7,863,000 7,863,000 0Total allocation 111,177,006 111,177,006 0 331,007,000 331,007,000 0
Programmed Expenditure
Acute CommissioningUHL Contract 40,650,310 40,875,628 225,318 121,950,939 122,700,939 750,000 Out of County Contracts 7,733,167 8,145,297 412,129 23,106,260 23,106,260 0 Non Contracted Activity 687,828 687,828 0 2,038,490 2,038,490 0 Independent Sector 1,955,064 2,395,841 440,777 5,865,247 6,553,193 687,946
Total Acute Commissioning 51,026,369 52,104,594 1,078,224 152,960,935 154,398,882 1,437,946
Non-acute CommissioningLPT Contract 16,465,391 16,431,584 (33,807) 49,396,215 49,396,215 0 Elective Alliance Contract 2,256,980 2,256,980 0 6,770,944 6,770,944 0 Out of County Contracts 127,010 124,286 (2,724) 381,066 378,332 (2,733)EMAS Contract 2,246,365 2,246,364 (1) 6,739,103 6,739,100 (3)Arriva Contract 644,080 660,943 16,863 1,932,241 1,963,631 31,390 Non Contracted Activity 98,896 98,896 0 296,711 296,711 0 Childrens Complex Care 388,544 453,291 64,747 1,165,652 1,209,892 44,240 Community Equipment 673,016 645,255 (27,761) 2,019,060 1,935,778 (83,282)Continuing Healthcare 7,269,075 8,588,646 1,319,571 21,807,263 22,365,748 558,485 ECRs 225,491 359,023 133,532 676,479 1,173,387 496,908 Voluntary Sector 1,209,630 1,209,718 88 3,629,124 3,629,378 254 Independent Sector 47,599 63,909 16,310 142,795 191,728 48,933 LD Pooled Budget & Reablement 2,070,661 2,125,161 54,500 6,211,992 6,429,992 218,000 Commissioning Scheme 244,085 265,361 21,276 732,322 796,023 63,701 Out Of Hours 985,980 985,981 1 2,957,945 2,936,438 (21,507)NHS 111 171,639 146,766 514,914 514,914 Home Oxygen 132,096 135,476 3,380 396,296 406,428 10,132 Other 10,515 2,978 (7,537) 31,557 24,020 (7,537)
Total Non-acute Commissioning 35,267,053 36,800,618 1,558,438 105,801,680 107,158,661 1,356,981
CCG PrescribingScriptswitch 50,648 50,648 0 151,947 151,947 0 Central Prescribing 387,724 351,460 (36,264) 1,163,176 1,057,313 (105,863)High Cost Drugs 357,120 321,612 (35,508) 1,071,367 967,519 (103,848)GP Prescribing 14,518,231 14,426,165 (92,066) 43,676,714 42,879,036 (797,678)
Total Practice Prescribing 15,313,723 15,149,885 (163,838) 46,063,205 45,055,816 (1,007,389)
Enhanced ServicesLocal Enhanced Services 641,912 641,912 0 1,925,813 1,925,813 (0)
Total Enhanced Services 641,912 641,912 0 1,925,813 1,925,813 (0)
OtherGP Support Framework 323,702 324,977 1,275 971,112 974,930 3,818 End of Life/ IOP & Other 214,351 214,387 36 643,056 643,160 104 Prescribing Incentive Scheme 107,175 61,085 (46,090) 321,528 183,258 (138,270)Minor Injury Units 353,677 353,679 2 1,061,085 1,060,997 (88)GP IT 270,666 270,666 0 812,000 812,000 0 East Intergrated Care 90,576 94,035 3,459 271,731 275,190 3,459 Personal Health Budgets 0 (610) (610) 0 0 0 Primary Care - Licenses, MacMillan & Other 55,616 33,783 (21,833) 166,859 163,974 (2,885)CHC GEM SLA 230,268 230,268 0 690,814 690,814 0 LCCCG Hosted Safeguarding team 33,740 25,521 (8,219) 101,231 99,555 (1,676)Patient Safety 24,584 36,119 11,535 73,751 73,751 0
Total Other 1,704,355 1,643,911 (60,444) 5,113,167 4,977,628 (135,539)
ReservesReserves - Headroom 2,379,000 1,695,241 (683,759) 7,985,000 7,985,000 0 Reserves - Contingency 1,652,000 0 (1,652,000) 1,652,000 0 (1,652,000)Further Efficiencies to be identified (197,607) (221,870) (24,263) (665,800) (665,800) 0
Total Reserves 3,833,393 1,473,371 (2,360,022) 8,971,200 7,319,200 (1,652,000)
Total Programmed Expenditure 107,786,805 107,814,289 52,357 320,836,000 320,836,000 0
Total Running Costs 2,287,534 2,260,696 (26,838) 6,863,000 6,863,000 0
GRAND TOTAL 110,074,339 110,074,985 25,519 327,699,000 327,699,000 0
SurplusProgramme control total 769,333 741,849 (27,484) 2,308,000 2,308,000 (0)Running Costs control total 333,333 360,171 26,838 1,000,000 1,000,000 0 Total control total 1,102,667 1,102,021 (646) 3,308,000 3,308,000 (0)
Year to Date Full Year Forecast
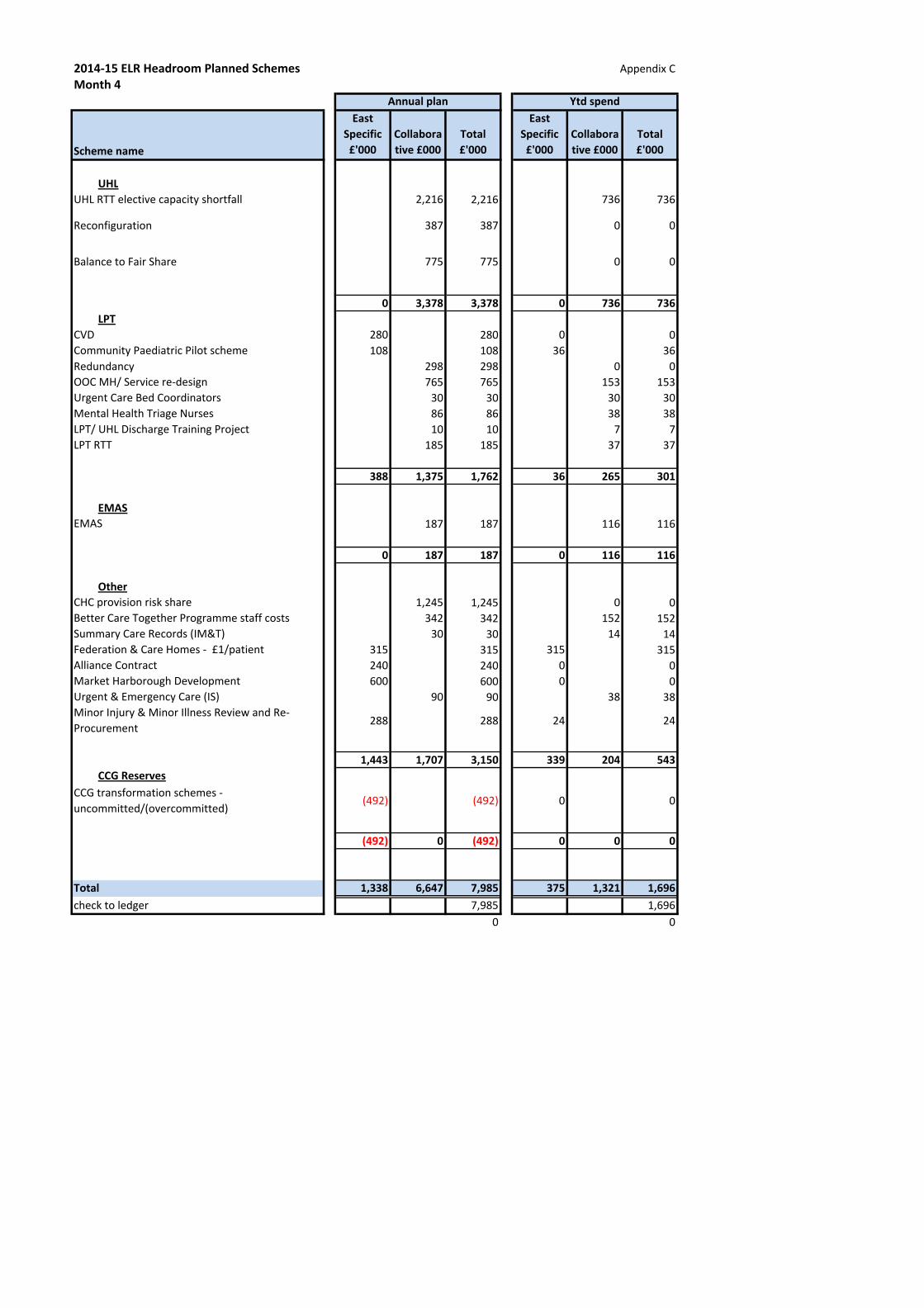
2014‐15 ELR Headroom Planned Schemes Appendix CMonth 4
Scheme name
East
Specific
£'000
Collabora
tive £000
Total
£'000
East
Specific
£'000
Collabora
tive £000
Total
£'000
UHL
UHL RTT elective capacity shortfall 2,216 2,216 736 736
Reconfiguration 387 387 0 0
Balance to Fair Share 775 775 0 0
0 3,378 3,378 0 736 736
LPT
CVD 280 280 0 0Community Paediatric Pilot scheme 108 108 36 36Redundancy 298 298 0 0OOC MH/ Service re‐design 765 765 153 153Urgent Care Bed Coordinators 30 30 30 30Mental Health Triage Nurses 86 86 38 38LPT/ UHL Discharge Training Project 10 10 7 7LPT RTT 185 185 37 37
388 1,375 1,762 36 265 301
EMAS
EMAS 187 187 116 116
0 187 187 0 116 116
Other
CHC provision risk share 1,245 1,245 0 0Better Care Together Programme staff costs 342 342 152 152Summary Care Records (IM&T) 30 30 14 14Federation & Care Homes ‐ £1/patient 315 315 315 315Alliance Contract 240 240 0 0Market Harborough Development 600 600 0 0Urgent & Emergency Care (IS) 90 90 38 38Minor Injury & Minor Illness Review and Re‐Procurement 288 288 24 24
1,443 1,707 3,150 339 204 543
CCG Reserves
CCG transformation schemes ‐ uncommitted/(overcommitted)
(492) (492) 0 0
(492) 0 (492) 0 0 0
Total 1,338 6,647 7,985 375 1,321 1,696
check to ledger 7,985 1,6960 0
Annual plan Ytd spend

QIPP Performance 2014/15Month 4
Plan Actual Variance Plan Actual Variance Plan Actual Variance
QIPP Schemes £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s
Transactional
Prescribing 125 125 0 500 500 0 1,500 1,500 0Alliance Contract (Derbyshire) 35 35 0 141 141 0 423 423 0
Total Transactional schemes 160 160 0 641 641 0 1,923 1,923 0
Transformational
East specific ‐ Admission avoidance (A&E) 2 2 0 7 7 0 22 22 0East specific ‐ Admission avoidance (IP emergency/EXBD/Short Stay) 89 89 0 355 355 0 1,065 1,065 0East specific ‐ COPD 0 0 0 0 0 0 14 14 0East specific ‐ CVD 0 0 0 0 0 0 72 72 0East specific ‐ Diabetes 8 8 0 32 32 0 97 97 0Continuing Healthcare 333 333 0 333 333 0 3,000 3,000 0Childrens Planned & Unscheduled Pathway Redesign 0 0 0 0 0 0 300 300 0GP OP referral threshold reduced to 12/13 levels 0 0 0 0 0 0 450 450 0
Total Transformation schemes 432 432 0 728 728 0 5,020 5,020 0
Other
0 0 00 0 0
Total Other schemes 0 0 0 0 0 0 0 0 0
Total QIPP Schemes 592 592 0 1,369 1,369 0 6,943 6,943 0
Health economy wide QIPP
LLR Ophthalmology annex iop 1 & 2 2 2 0 9 9 0 28 28 0LLR Single front Door annex 15 15 0 60 60 0 180 180 0LLR Parkinson's nurse extension annex (IP emergency) 2 2 0 7 7 0 20 20 0LLR Parkinson's nurse extension annex (OP follow up) 1 1 0 4 4 0 13 13 0LLR New to follow up ratios annex 21 21 0 21 21 0 191 191 0LLR ‐ Referral Thresholds annex (Daycase) 32 32 0 32 32 0 289 289 0LLR ‐ Referral Thresholds annex (IP elective) 7 7 0 7 7 0 64 64 0LLR Reduction in day case follow ups annex 17 17 0 17 17 0 155 155 0LLR BADS annex 10 10 0 39 39 0 117 117 0
Total Health economy wide QIPP 108 108 0 197 197 0 1,057 1,057 0
Unidentified QIPP
Unidentified QIPP 0 0 0 0 0 0 970 970 0
Total Unidentified QIPP 0 0 0 0 0 0 970 970 0
Total QIPP 700 700 0 1,566 1,566 0 8,970 8,970 0
Appendix D
Recurrent schemesIn Month Year to Date Forecast

Appendix E
A B C D E F A B C D E F
No of Bills Paid
Within Period
No of Bills Paid
Within Target
% of Bills Paid
Within Target
Value of Bills Paid Within
Period
Value of Bills Paid Within
Target
% Value of Bills
Paid Within Target
No of Bills Paid
Within Period
No of Bills Paid
Within Target
% of Bills Paid
Within Target
Value of Bills Paid
Within Period
Value of Bills Paid Within Target
% Value of Bills
Paid Within Target
No. No. % £'000 £'000 % No. No. % £'000 £'000 %April 226 224 99.12 17,736 17,736 100.00 873 861 98.64 2,960 2,945 99.48May 237 234 98.73 17,688 17,665 99.87 756 752 99.47 3,325 3,311 99.58June 205 203 99.02 19,867 19,834 99.83 689 688 99.85 2,780 2,772 99.73July 227 225 99.12 18,087 18,086 99.99 928 923 99.46 3,758 3,715 98.87AugSeptemberOctoberNovemberDecemberJanuaryFebruaryMarch
Totals 895 886 98.99 73,378 73,320 99.92 3,245 3,223 99.33 12,822 12,743 99.38
East Leicestershire & Rutland CCG
Better Payment Practice Code July 2014
NHS Creditors Non NHS Creditors

Appendix F
Balance
£'000sNon Current Assets:Premises, Plant, Fixtures & Fittings 750IM&T 42Other 0Long-term Receivables 0TOTAL Non Current Assets 792Current Assets:Inventories 0Trade and Other Receivables 3,881Cash and Cash Equivalents 135TOTAL Current Assets 4,016
TOTAL ASSETS 4,808Non Current Liabilities:Long-term payables 0Provisions 0Borrowings 0TOTAL Non Current Liabilities 0Current Liabilities:Trade and Other Payables (21,010)Other Liabilities 0Provisions (89)Borrowings 0Total Current Liabilities (21,099)
TOTAL LIABILITIES (21,099)
ASSETS LESS LIABILITIES (Total Assets Employed) (16,291)
TAXPAYERS EQUITYGeneral Fund (Opening Balance, Fixed) (18,752)Income & Expenditure (year to date) (110,075)Parliamentary Funding (year to date) 112,533Other Reserves 3Total (16,291)
Statement of Financial Position 31 July 2014

Appendix G
East Leics and Rutland03W
2014/15 April May June July August September October November December January February March
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Receipts
Balance b/fwd (308) (308) 74 78 70 135 200 200 200 200 200 200 200NCB‐Drawdown 302,172 23,000 22,300 24,500 29,600 29,000 24,300 24,600 25,700 24,385 25,500 24,300 24,987NCB‐Drawdown additional 0 0 0 0 0 0 0 0 0 0 0 0Other (including VAT) 4,436 465 397 2,290 534 50 100 100 100 100 100 100 100
Total Receipts 306,300 23,156 22,771 26,868 30,204 29,185 24,600 24,900 26,000 24,685 25,800 24,600 25,287
Payments
Creditors NHS 226,531 17,776 17,692 19,870 20,009 22,713 18,346 18,504 18,270 18,270 18,438 18,270 18,372Creditors CHAPS 68,172 4,200 4,275 6,253 9,354 5,550 4,935 5,017 6,411 5,174 6,150 5,172 5,681Salary CHAPS 2,209 183 180 178 193 194 183 183 183 183 183 183 183Pensions 723 62 58 58 55 56 62 62 62 62 62 62 62Tax & NI 1,080 91 90 86 81 94 91 91 91 91 91 91 91Standing Orders /Direct Debits 16 3 1 1 3 1 1 1 1 1 1 1 1PCS Payments 5,267 768 396 352 372 376 457 546 486 408 379 325 402Other 2,102 1 1 0 2 1 324 296 296 296 296 296 296
Total ‐ Expenditure 306,098 23,082 22,693 26,798 30,069 28,985 24,399 24,699 25,800 24,485 25,600 24,400 25,088
Balance c/fwd 74 78 70 135 200 200 200 200 200 200 200 200
Cashflow reportingMonth 4 2014/15
ForecastYear to date


Blank Page

Paper H East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
1
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
Front Sheet
REPORT TITLE: ELR CCG Locality Meeting Themes – August 2014
MEETING DATE: 9 September 2014
REPORT BY: Jamie Barrett, Head of Primary Care
SPONSORED BY: Tim Sacks, Chief Operating Officer
PRESENTERS: Dr Andy Ker, GP Locality Lead, Melton, Rutland and Harborough Dr Nick Glover, GP Locality Lead, Blaby & Lutterworth Dr Richard Palin, GP Locality Lead, Oadby & Wigston
PURPOSE OF THE REPORT: The purpose of this report is to provide an overview of the monthly GP Locality meetings held across Blaby and Lutterworth, Oadby and Wigston and Melton, Rutland and Harborough. These meetings are key to the CCG development and allow member practices an opportunity to debate current general practice and highlight themes they wish to inform the Board.
RECOMMENDATIONS: The East Leicestershire and Rutland CCG Governing Body is requested to: RECEIVE the report.
REPORT SUPPORTS THE FOLLOWING STRATEGIC AIM(S) 2014 – 2015: Transform services and enhance quality of life for people with long-term conditions
Y Improve integration of local services between health and social care; and between acute and primary/community care.
Y
Improve the quality of care – clinical effectiveness, safety and patient experience
Y Listening to our patients and public – acting on what patients and the public tell us.
Y
Reduce inequalities in access to healthcare Living within our means using public money effectively
Implementing key enablers to support the strategic aims (e.g. constitutional and governance arrangements, communications and patient engagement).
EQUALITY ANALYSIS An Equality Analysis and due regard to the positive general duties of the Equality Act 2010 has not been undertaken in the development of this report as it is judged that it is not proportionate on the basis that this purely an information summary of discussions which has occurred.
This completes the due regard required.

Paper H East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
2
RISK ANALYSIS AND LINK TO BOARD ASSURANCE FRAMEWORK: The report directly links to risk BAF 10 (Capacity of primary and community services to manage left shift).

Paper H East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
3
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
GOVERNING BODY MEETING 9 September 2014
GP Locality Meetings – August 2014
INTRODUCTION
1. The 34 GP practices across the CCG are split into 3 geographical localities,
Blaby and Lutterworth, Oadby and Wigston and Melton, Rutland and Harborough. The purpose of the locality structure is to provide a forum for member practices to feed into the CCG, feedback to their practices and discuss key issues and concerns. In addition the locality structure provides:
Meetings held monthly, 12 times a year A promotion of two-way discussion on all business and a mechanism for
GPs to be updated on CCG matters to inform commissioning and planning processes.
Share learning from adverse events e.g. safeguarding issues etc. Opportunities for clinical discussion and education Monitoring of performance and quality through the sharing of
benchmarked data and information.
LOCALITY MEETING CONTENT
2. These meetings are represented by each practice across the CCG. The theme for the August 2014 meetings can be split up as the following:
Clinical Topics
Emergency Care across LLR – Update into developments across the urgent care system. Lead by Dr Ian Sturgess Stop! Smoking - Update on the service to stop smoking service
Emerging Primary Care Strategy – feedback and discussion on CCG plans for primary care.
Reporting Poor Quality Care – concerns logged at the CCG were presented back to practices and a discussion had about the outcomes.
Anti Coagulation and NOACs – update on prescribing and new NICE Guidelines.

Paper H East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
4
Standing Agenda Items
Prescribing quality and assurance – prescribing quality and issues across
practices Monitoring of performance and quality through the sharing of
benchmarked data and information – activity information at practice level is presented and trends identified and discussed.
Safeguarding and GP Concerns – an opportunity to share any learning or raise concerns with peers
LOCALITY THEMES
3. The below represents the key themes from the Localities for the month of
August 2014.
MELTON RUTLAND AND HARBOROUGH – Chair Dr Richard Hurwood
4. Emergency Care across LLR - A detailed clinical discussion lead by Ian
Sturgess focussing on “New Thinking to solve the Emergency Department Problem at University Hospitals Leicester” took place. Discussions included understanding examples of the problems in the Emergency Department, examples of the impact on patient care, and suggestions for why the problems existed. Some preliminary talks began about the need for a whole systems approach to resolving the problems and the role of General Practice in this.
5. Practice Performance - Discussions took place regarding the current Performance of the MRH Locality practices. The practices were made aware of current increase in Emergency Admissions, Outpatient and Elective Care activity. It was emphasised that General Practice needed to focus where possible on peer review and audit as the current levels of over performance will have an impact on budgets and future investments across all contracts.
6. Anti-Coagulation - A clinical presentation on use of NOACS, and how to safely transfer patients onto these drugs was led by Gill Stead. This gave the GPs present an opportunity to ask questions and consider what patients on their lists could be safely transferred onto theses anticoagulation drugs.
7. Prescribing - Over prescribing/Pharmacy: One practice has raised its concerns through appropriate channels regarding third party ordering of repeat prescriptions; this may be an area the CCG wishes to monitor.
Paper H East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
5
BLABY AND LUTTERWORTH – Chair Dr Nick Glover
8. Emergency Care across LLR – A similar discussion was had to the other localities on this issue as Ian Sturgess presented his role in the LLR project of ‘New Thinking to solve the LLR ED Problem’. In the following discussion it was agreed that there needed to be a recognition that UHL had lower than average admissions from ED and that 30% of GP time was wasted. The group agreed that the Institute for Healthcare Improvement’s model of Rapid Cycle of Testing should be adopted in LLR and the CCG.
9. Community Services - The group voiced concerns that there had not been enough GP consultation of the LPT model of Community Services that is currently being implemented. However, it was recognised that there had been a positive change in consultation with GPs for the Primary Care Strategy work. LPT and Dr A Kerr made a commitment to agree a sensible timeframe for the model to ‘bed’ in and then to follow up with a survey for GPs to comment on how they think the model is working.
10. Reporting Poor Quality of Care - A Poor Quality of Care report was presented to the Locality by the Quality Team. The group agreed that the process was working well and the information gathered was useful and being progressed by the CCG. The group requested that a Reporting of Excellent Care option be added to the template so this could also be reported to enable feedback to providers on what they were doing well. The Locality received the NOAC update and noted the good practice of testing CDT.
OADBY AND WIGSTON – Chair Dr Richard Palin
11. NOACs Anti Coagulation - Gill Stead from UHL pharmacy presented NOAC
(new oral anticoagulant drugs) to the locality. GPs raised some concern over the shared care agreements currently used as these are often lengthy and the GPs felt it was not easy to identify where the key information that they need to be aware of is. ( There was concern that these drugs were already prescribed and locality where not aware of use of creatinine clearance rather than eGFR ) There was also discussion around the barriers to prescribing as there are quite a few steps to follow to ensure safe prescribing of these medications.
12. Reporting Poor Quality Care - The quarterly GP Concerns / reporting poor quality care report was discussed. There was acknowledgement that reporting had been low in the locality but GP’s reiterated that the new reporting system is not yet available to emis web practices which is the main clinical system for the area. GPs also raised concerns that reporting poor quality care could damage relationships with secondary care colleagues and discussion focused on practice experience of this and the concern that they would not wish this to

Paper H East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
6
escalate and result in breakdown of relationships. GPs felt that system failure should be highlighted via this method rather individuals.
13. Primary Care Strategy –GPs discussed possible suggestions for changes that could be made in primary and community care. GP suggestions included specialist nurses in the community and the need to strengthen relationships with community based nursing teams. It was felt that an increase in specialist nursing support could be a way to improve the care for the patient. The GPs felt that high quality independent prescribing nurses should be available for various specialties eg DM, heart failure, COPD , and be more part of the practice team. The number of nurses should NOT be diluted over OOH, but a good well funded core hours of service nursing team was required.
RECOMMENDATION: The East Leicestershire and Rutland CCG Governing Body is requested to: RECEIVE the report


Blank Page

Paper I ELR CCG Governing Body Meeting
9 September 2014
1
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
Front Sheet
REPORT TITLE: ELR CCG IM&T Strategy Development Plan
MEETING DATE: 9 September 2014
REPORT BY: Jamie Barrett, Head of Primary Care
Vikesh Tailor / Paul Greenhead (GEM CSU/Methods I.T Solutions)
SPONSORED BY: Tim Sacks, Chief Operating Officer
PRESENTER: Tim Sacks, Chief Operating Officer
PURPOSE OF THE REPORT: This report provides an initial briefing on the plan to develop a 5 year IM&T strategy for the CCG. This current document identifies:
The current landscape for the development of a strategy The existing IM&T governance structure with support from GEM CSU and
Leicestershire HIS. The new CCG responsibilities from April 2014 onwards Progress to date with IM&T initiatives.
The plan identifies key milestones for the full development of a CCG IM&T strategy that will take into consideration input from key stakeholders through a series of future workshops to be held in October 2014 (the strategy will align to the CCG two-year Operation Plan and Better Care Together 5 year plans). A national IM&T strategy including expectations for CCGs/GP I.T will be published by NHS England in the autumn of 2014 and development of this strategy will need to fully align to this hence the caveat that is not a complete strategy. Immediate next steps are:
For the CCG Board to agree the development and context of the IM&T strategy This to be progressed at pace throughout September and October 2014. Development sessions involving CCG staff and stakeholders to be arranged by
GEM CSU to inform an updated and detailed strategy

Paper I ELR CCG Governing Body Meeting
9 September 2014
2
RECOMMENDATIONS: The East Leicestershire and Rutland CCG Governing Body is requested to:
Note the strategy development plan and accept that a completed version will be submitted once the national strategy is available.
REPORT SUPPORTS THE FOLLOWING STRATEGIC AIM(S) 2014 – 2015: Transform services and enhance quality of life for people with long-term conditions
Improve integration of local services between health and social care; and between acute and primary/community care.
Y
Improve the quality of care – clinical effectiveness, safety and patient experience
Y Listening to our patients and public – acting on what patients and the public tell us.
Reduce inequalities in access to healthcare Y Living within our means using public money effectively
Y
Implementing key enablers to support the strategic aims (e.g. constitutional and governance arrangements, communications and patient engagement).
EQUALITY ANALYSIS Further equality analysis is required and it is recommended that the ELRCCG Board receives this in November 2014 prior to the publication of the full strategy.
RISK ANALYSIS AND LINK TO BOARD ASSURANCE FRAMEWORK: The report directly links to risk BAF 10 (Capacity of primary and community services to manage left shift).

1
East Leicestershire and Rutland Clinical Commissioning Group
Information Management and Technology Strategy Development Plan 2014-2019
Version: 0.3
Date: 3rd September 2014
Authors: Vikesh Tailor, Paul Greenhead and Jamie Barrett

2
Document Control
Issue No Issue Date Summary of Issue Version
0.1 02/09/14 Initial draft structure with limited content
0.1
0.2 3/09/14 Format and content amends 0.2
0.3 4/09/14 Format and content amends 0.3
Approvals
Name Title Date of Issue Version
Vikesh Tailor Head of Systems Enablement, GEM CSU
02/09/14 0.1
Jamie Barrett Head of Primary Care, ELR CCG
03/09/14 0.2
Tim Sacks COO, ELR CCG 04/09/14 0.3
Distribution
Name Title Date of Issue Version
Vikesh Tailor Head of Systems Enablement, GEM CSU
02/09/14 0.1
Jamie Barrett Head of Primary Care, East Leicestershire and Rutland Clinical Commissioning Group
02/09/14 0.1
Tim Sacks COO, ELR CCG 04/09/14 0.3
Daljit Kaur-Bains Head of Corporate Governance 04/09/14 0.3

3
Executive Summary This report provides an initial briefing on the plan to develop a 5 year IM&T strategy for the CCG. This current document identifies:
The current landscape for the development of a strategy The existing IM&T governance structure with support from GEM CSU and
Leicestershire HIS. The new CCG responsibilities from April 2014 onwards Progress to date with IM&T initiatives.
The plan identifies key milestones for the full development of a CCG IM&T strategy that will take into consideration input from key stakeholders through a series of future workshops to be held in October 2014 (the strategy will align to the CCG two-year Operation Plan and Better Care Together 5 year plans).
A national IM&T strategy including expectations for CCGs/GP I.T will be published by NHS England in the autumn of 2014 and development of this strategy will need to fully align to this hence the caveat that is not a complete strategy.
This version is an initial plan to start engaging with our key stakeholders.
Introduction Information management and technology is key component for the delivery of business and clinical outcomes. The ELR CCG Operational Plan identifies ‘Developing and enabling IT/digital platform as a key enabler of the operational plan. The purpose of this IM&T strategy is to set out how information and technology can support East Leicestershire and Rutland Clinical Commissioning Group to achieve their strategic organisational objectives.
Background The publication of the second edition of Securing Excellence in GP IT Operating Model highlighted the increasing importance of IM&T to CCG strategies and sets out new responsibilities for managing the delivery of GP IT. This document was the first of a series of national documents due to be released during the summer of 2014 aimed at providing guidance on CCG responsibilities in relation to IM&T, which include the:
CCG Practice IM&T Agreements General Practice IT Strategy CCG Data Strategy CCG estate IT Hardware
The release of the IT and Data Strategies have been delayed to the autumn by NHS England, with the expectation that they may be further aligned.
This national focus on IM&T underlines the fact that it is already a key enabler for the delivery of CCG strategic and operational plans, and will play an important role in

supporLLR.
The crecohereIM&T cenable
Princip
rting the CC
eation of aent strategicapabilitiese the achiev
ples of the To define
o A so Strao Ref
proThis docum
o Howo A d
planA g
o Setin re
o An o The
andStra
CG contrib
an IM&T Stc approach
s and invesvement of
Strategy an IM&T Strategy thaategy Durafresh procecess and gment showw it relatesiagram dens overnance
t out the spelation to Iearly versi
e plan will sd ‘whom’ thategy.
Figure
bution to th
trategy will h that alignstments arebusiness o
Strategy at describeation – 2 –ess and hogovernancws s to other dmonstratin
e TOR pecific goveM&T Operion of an IMset out thehat will deli
e 1: IM&T S
4
he Better C
enable ELns with nate clearly idobjectives.
es the ‘why5 years –
ow it will bece structure
documentsng the inter
ernance arrational anM&T Plane project aniver the IM
Strategy D
Care Toget
LR CCG totional and dentified, d.
y’ and the ‘haligned wi
e embeddees
/plans rrelationsh
rrangemennd Strategic
nd initiativeM&T Object
ocument C
her Partne
o ensure thlocal drivereveloped a
how’ th CCG Pl
ed into the
ips betwee
nts, role anc governan
es, the ‘whtives outlin
Context
ership acro
hat it develors to ensurand contro
lanning Cyregular IM
en strategi
nd responsnce archite
at, ‘when’ ed in the
oss
ops a re that olled to
ycles M&T
es and
sibilities ecture
‘where’

5
Strategic Local Context This section sets out the strategic context of the IM&T Strategy identifying national policy and local business drivers that the strategy is designed to enable.
This section identifies:
Current IM&T provision. Diagram demonstrating the local stakeholders (LATs, CCGs LHIS, GEM etc.) The General Practice landscape -number of Practices supported, IT systems
etc. Background on the Leicester ‘Challenged Health Economy’ and the Better
Care Together Partnership Particular challenges presented by a predominantly rural geography Describe the current suppliers of IM&T services to the CCGs, what are the
current GP clinical systems being utilised Major IM&T projects and programmes in progress
Existing Governance Architecture The existing governance architecture is set out in figure 2 below. The governance architecture has evolved in line with development of the CCG roles and emergence of collaborative initiatives within the local health economy. Whilst ultimate authority and accountability for IM&T rests with the ELR CCG Board, the IM&T Governance architecture is composed of the following structures:
Better Care Together (coordinating the overall LLR Health Economy direction)
ELR &WL CCG IM&T Steering Group: (Overview and Governance of local CCG IM&T
Project Board Day: (Updates on operational progress of projects)

The keLeicestThe steprovideThis reprogram
ELR Cand proare led
Whilst directiooperatifocuseengage
ey IM&T gotershire aneering groues oversighesponsibilitmme repo
CG fund oovide the p
d by a joint
the currenon and oveional directd on businement inclu
Service LePrimary CVirtual IM&Supplier R
Figure
overnance nd Rutland up has a cht of IM&T ty is supporting takes
one of the pprimary carEast and W
nt governanersight, thetion of IM&
ness as usuuding:
evel Managare Voice &T Networ
Review/ Ma
e 2: Existin
structure wand West
learly defininitiativesrted by the
s place.
practice mare voice toWest Leice
nce architeere are a nu&T could beual IM&T o
gement
rks anagement
6
g Governa
within this t Leicestersned membacross EL
e Project B
anagers too the steeriestershire
ecture provumber of ae strengtheoperational
t
ance Archit
architecturshire CCGership and
LR and WeBoard day,
o support wng group. CCG GP c
vides a struareas wherened. Thel service de
tecture
re is the joi IM&T Ste
d terms of rest Leiceste
where proj
with IM&T iThe goverclinical lead
ucture for tre the stratese are preelivery and
int East ering Groureference aershire CC
ojects and
mplementarnance strud.
the provisiotegic and edominantld operation
up. and
CG.
ation ucture
on of
y nal

7
Existing Service Architecture ELR currently receives IM&T Services from both GEM CSU and Leicester Health Informatics Services (LHIS). The table below sets out the IM&T services `provided by the respective suppliers:
Service Supplier IM&T Service Portfolio
Greater East Midlands Commissioning Support Unit
• Strategy & Planning
• Commissioning Support
• Procurement Support
• Information Governance
• Business Intelligence
• PMO
• Primary Care Facilitation
Leicester Health Informatics Service
• Core GP IT services
• Corporate IT services
• IT Projects
• Clinical Systems Training
• Technical Security
• Registration Authority
• Infrastructure services
Table 1:IM&T Services by Service Provider
(Service portfolio, SLAs and service contract costs and contract expiration dates to be clarified)
National Drivers The national drivers for CCG IM&T Strategy are encapsulated within a number of key national documents that have been published or scheduled for publication in autumn 2014. These include the following
Securing Excellence in GPIT Services – Operating Model 2nd Edition 2014/16 GP System of Choice (GPSoCR) – to be released shortly – awaiting final
supplier sign up (TPP S1) CCG Practice IM&T Agreement (Primary Care IT Service Schedule) –
expected Autumn 2014 General Practice IT Strategy – expected in Autumn 2014

8
CCG Date Strategy Guidance – expected in Autumn 2014
Securing Excellence in GPIT Services – Operating Model 2nd Edition 2014/16 Foremost among these key national document is Securing Excellence in GPIT Services – Operating Model sets out an updated operating model for GP IT services designed to:
“…achieve high quality primary care digital systems that support the provision of a more efficient, responsive and integrated services for patients whilst empowering them to have greater control over their health and care.”i
ELR CCG Specific GP I.T IM&T Responsibilities 2014-2016
The operating model outlines specific key responsibilities for CCGs in relation to GP IT Services that are envisaged to be in place by April 2016. These comprise of the following:
1. strong local leadership to drive the technology strategy associated with continuing service improvement
2. an equitable financing model for the delivery of GP IT and IT support services, based on practice population
3. an excellent universal core digital capability enabled by effective IT support services across the general practice estate
4. the effective procurement, delivery and exploitation of GP IT capability, across the whole of England
5. collaborative partnership working that has the freedom to innovate and redesign services effectively
6. value for money and efficiency, delivered through the combination of all of the aboveii
Securing Excellence in GP IT Services requires ELR CCG to develop a complete and detailed picture of core GP IT service delivery costs, identify relative levels of ‘digital maturity’ and ensure value for money in GP IT investments. The key point are outlined below: Key Points:
CCGs to retain delegated management responsibility for delivery of GPIT services on behalf of NHSE
Requirement for CCGs to commission GPIT services, as outlined in Operating Model
Funds allocated for GPIT investment, must only be used for primary care IT as defined in the GPIT Operating Model.
If CCGs forecast under spending in year, NHSE may decide to reallocate the funding. Clear standing financial instructions must be established between commissioners/delivery organisations.
CCGs to share detailed GPIT spend with NHSE – to inform Primary Care Digital Maturity Index (PCDMI)

9
CCGs will be required to manage and report GPIT assets in accordance with NHSE capital accounting guidance
GP Systems of Choice Framework (GPSoC) Health and Social Care Information Centre (HSCIC) have completed work to sign contracts with 17 suppliers of GP IT systems to enter into a new GP Systems of Choice Framework which will replace existing arrangements. New Contracts are due to be in place until December 2016. The GPSoC Framework is divided into 3 separate lots:
Lot 1: GPSoC : Principal and Subsidiary Clinical Systems Lot 2: GPSoC: Additional GP IT Services Lot 3: GPSoC: Cross Care Setting Interoperable Services
Additional services will become available in 2014. These include:
Patient access to records, appointment booking and ordering of repeat prescriptions
Advanced versions of document management/workflow software Mobile clinical applications, Decision support, Telehealth Data entry forms
ELR CCG current GP IT Portfolio Clinical Systems
Currently across ELR CCG two main clinical systems are in place as per the GPSoC these are EMIS Web (18/34 practices) and System 1 (16/34 practices)
CCG Practice IM&T Agreement (Primary Care IT Service Schedule)/GeneralPractice IT Strategy/CCG Data Strategy Guidance These key documents are crucial to the overall direction of the strategy and will inform much of what is needed to be taken forward. As indicated in the executive summary it is anticipated these will be available in the autumn of 2014 (therefore the strategy plan has the potential to significantly change. National Standards for IM&T: These set out the relevant national standards:
GP Systems Interface Mechanism Requirements V1 (HSIC) Information Governance and Security Standards IG Toolkit etc.
Local Drivers CCG Strategies The local drivers for the ELR CCG IM&T Strategy are principally drawn from the ELR CCG Two Year Operation Plan (2014/15 – 2015/16) and the Better Care Together Strategy and CCG Primary Care Plan.

10
ELR CCG Two Year Operational Plan 2014/15 and 2015/16 The ELR CCG Two Year Operation Plan sets of the clinical commissioning objectives and intentions that the IM&T Strategy is designed to enable:
Objectives: The LLR health and care community will achieve its goal by working together with a sustained focus on: 1. Helping people to stay healthy and well - to prevent people dying prematurely and reduce health inequalities. Impacting on the wider determinants of health environment and healthy lifestyles through primary prevention interventions that have the potential to both deliver short term benefits e.g. smoking cessation and impact longer term on the future burden of disease. 2. Identifying people earlier at risk of ill health or loss of independence - Target secondary prevention and early intervention (screening, case finding /risk profiling and early intervention) support for vulnerable people/at risk to help people to stay well reduce or delay the onset of ill health and/or deterioration in independence (e.g. falls) 3. Empowering patients with long term conditions to monitor and manage their own health – a systematic approach to routine management of long term conditions, including those with mental illness, putting in place care plans and empowering patients, families and their carers have greater control over their health and wellbeing to monitor, manage and stabilise their own conditions to get the best possible quality of life 4. Taking a proactive approach to co-ordinating care for people with multiple and complex conditions - patients with multiple, often complex, mental or physical long term conditions, often compounded by being elderly and frail, vulnerable 5. Reducing dependence on acute urgent and emergency care in hospital - enabling access to the highest quality urgent and emergency care. Expand the range and integration of step up / pre-hospital care to provide alternatives to acute hospital admission for patients, particularly the frail elderly, when their condition deteriorates/acute exacerbation. Earlier treatment at home or in the community to prevent people needing emergency care in hospital or care homes. 6. Driving a step change in elective efficiency - by providers reducing inappropriate clinical variation from GP referrals and prescribing, through to specialist intervention rates, theatre productivity, day case procedures 7. Concentrating specialised services in centres of excellence - for less common disorders where the highest quality can be delivered 8. Reducing the amount of time people spend in hospital – cutting down the length of stay in acute hospital, mental health and community hospital through better and more integrated care in the community and outside of hospital

11
9. Supporting patients to recover quickly and successfully following illness or injury - Expand the range and integration of step down / post-hospital care to support timely discharge, help people to remain independent and avoid readmission 10. Maximising the independence of elderly, frail and vulnerable people through continuing care support - increase the proportion of older people living independently at home following discharge from hospital. Ensure that people’s continuing health and social care needs are assessed and managed consistently and when they are in a non-acute environment in order to ensure that on-going packages of care maximise independence in the most appropriate setting 11. Helping people to have choice and dignity at the end of their life - Help people at the end of their life to die in the place of their choice with dignity through care plans that avoid unwanted treatment and acute hospital admission.
Current IM&T Initiatives Supporting CCG Objectives: This area has had significant focus particularly for primary care: Electronic Care Management Plan
A centralised electronic care plan will be used and a clinical portal available for S1 and EMIS Web so an electronic care plan can be completed at GP Practice level, communicated easily with patients and also with Out of Hours and NHS 111.
WIFI In Care Homes
A programme of installing WIFI in care homes across ELR will assist GPs accessing and updating patient records. This will also assist community services in updating care management plans. Practices have expressed the possibility of Skype consultations and the use of IPads which could tie in with ‘one home one practice’ care home allocation
Multi-Disciplinary Development (MDT)
To use a web based software to enable the MDT to be truly multi-disciplinary in that attendance is not required. Web/Tele conferencing and viewing a central desktop is all possible remotely. This allowing for more productive use of time of the individuals involved.
Telehealth
To explore the use of the ‘Flo’ text messaging service so routine results and care monitoring can be communicated without always a face to face consultation.
Medical Interoperability Gateway (MIG)
Exploring a preferred solution for record sharing across clinical systems. Time and training in primary care needs to be considered alongside the Healthcare Gateway.

12
Other IMT Initiatives Supporting Primary Care In addition there are a number of IM&T initiatives which the CCG are supporting the delivery of in conjunction with the Greater East Midlands CSU and Leicestershire Health Informatics Service (HIS). These are:
eDSM – Enhanced Data Sharing Model for system1 GP practices. This will enable the sharing of patient records across healthcare organisations obtaining patient consent
Summary Care Records (SCR) - a national programme and allows elements of a patient’s health record to be shared nationally should the need arise in an urgent care situation. A summary of patient medication and health status is included
Care.data - allows a patient’s health record to be shared and used for planning of services
GP2GP - this allows for electronic transfer of patient records between practices
Electronic Prescribing (EPS). To allow repeat prescriptions and also to deal with potential inaccuracies with handwritten scripts and to maintain a secure patient record
Reporting Poor Quality Care - more concise system of reporting concerns with patient care will be available on system1 and EMIS web.
Information governance – support to primary care in relation to information governance training, and data sharing. WIFI care homes – to ensure care homes with ELR CCG area are WIFI equipped so this will assist both primary care and community staff to update clinical records/administer prescriptions.
The below table represents all the initiatives currently active and whether these are a national/local priority: Project /Programme/ IMT work streams
National Local Active Notes
SCR Y Y GP practice enablement (IE record uplift) due to complete Q3 2014
EPS2 Y Y Completion Q12016 - looking to accelerate
GP2GP Y Y Emis complete Systemone ongoing due to complete Q4 2014 including CD transfer
e-referral Y Y planning phase re implementation. Further scope required for systems optimisation commissioners, e.g. reporting, self referral etc.
Polar (patient access) Y N not currently active under discussion

13
WIFI in care homes Y Y due to complete Q3 2014
Prism Y Y transition to live service requires further work
NHS number (primary idenitfying in systems)
Y Y GP element complete- focus on social care
Data sharing health and social care (MIG)
Y Y links to NHS number and PDS
Electronic care plans Y N pockets of work query further development
Common Templates Y N pockets of work query further development e.g. end of life is developed in areas
Out of Hours /ED UHL Y Y Access for ED and out of Hours to GP data
Risk Strat Y Y Gemima/HERA using ACG tool
ISA Y Y IG project due for completion Q32014
Telehealth Y Y pockets of work eg FLO
Mobile working Y Y GP laptops- Wi-Fi nursing homes patient homes currently out of scope
e-consultation Y N requires scoping
Label trace Y Y transitioning to BAU
EDSM Y Y transitioning to BAU
BI Y Y review/ scope additional requirements
ICT Roadmap for CCG/GPs
Y N review/ scope additional requirements
Clinical Systems optimisation
Y N review/ scope additional requirements
primary care data quality
Y N review/ scope additional requirements
NHSmail 2 Y Y watching brief on national developments e.g.SMS withdrawal
Spine2 Y Y watching brief on national developments

14
Minor ailments online assessment
Y Y Digital first- local consideration/review
Appointment booking online
Y Y part of Polar project
Direct booking (out of hours/ 111)
Y N under review/ scope
Primary care pr-eassessment
Y N Digital first- local consideration/review
Appointment reminders
Y N Digital first- local consideration/review
Friends & Family test Y Y Pilot phase
Patient experience dashboards
Y ? eg datix could scope further development. National dashboard development insight
IMT Governance support/arrangements
Y Y E.g Steering group LLR IM&T project board day
Procurement support Y Y IM&T support procurement of services eg AQP
Better Care together Y Y IM&T support / scope PMO
e-comms Y Y e-letters, e-discharge local facilitation support
ITK2 compliance Y Y
JIGSG Y Y Joint information governance sharing group (IG advice from GEM)
CCIO
This is in line with the GP IT Operating Model as published by NHS England which outlines the responsibilities of CCGs in commissioning GP IT services and driving integrated care through local IM&T Strategy. For assurance and to fulfil its obligations in the delivery of these, the IM&T steering group monitor these and currently all are progressing to plan

15
Better Care Together Strategy Strategic Objectives
1. High quality care – right place, right time, less time in hospital
2. Reduced inequalities in care, leading to longer life
3. More positive experience of care
4. Integration and use of assets to reduce duplication and eliminate waste
5. Financial sustainability for all health and social care organisations
6. Better use of workforce, new capacity and capabilities in people and technology
ELR CCG Primary Care Plan The CCG primary care vision is currently being established and significant engagement has been undertaken with GP practices to understand future models of care and what primary care may look like in the future.
This is due to be submitted as part of the Better Care Together chapter on Primary Care by September 2014. IM&T is a significant enabler and in some cases a barrier to practices working together and more efficiently. System optimisation and data sharing are themes which have emerged from the consultation.
IM&T Vision This section outlines East Leicestershire and Rutland Clinical Commissioning Group’s vision of the way in which information management and technology will enable the delivery of clinical outcomes for patients.
IM&T Strategic Vision Statement Create IM&T as an enabler for CCGs: This statement will be built from the Workshops and Board Development Session but aligned to the principles of:
Requirement for CCGs to ‘drive integrated care through IT Strategy’ Developing an enabling IT/digital platform – that shares information as
appropriate across health and social care providers, and between providers and commissioners, to supports information continuity, cost and outcome measurement, and empower citizens and patients to make the best choices for services and their care safer care and better experience as don't need to repeat details at every new contact.iii
Strategic Objectives The vision statements and strategic objectives should be to:
Drive integrated care through IT Strategy (Beverly Bryant – SEGP IT 2014) Create a paperless environment Mobile Working to improve efficiency

16
NHS England Strategic Systems and Technology Directorate Visions Priorities: Enabling and Supporting people to access and interact with their individual
health records online Facilitating the widespread adoption of modern safe standards of electronic
record keeping Re-launch Choose & Book by 2015 Enabling online GP booking of appointments and ordering of repeat
prescriptions Supporting hospitals to implement electronic prescribing Integrated digital Care Records (IDCRs) become universally available Facilitating the adoption of Electronic Transfer of Prescriptions EPS programme Commissioning national IT Infrastructure:
o Spine o N3 o NHS Mailiv
(This requires discussion and clarification at Stakeholder workshops and Board Development Session in the near future)
Draft IM&T Considerations 2014 and Onwards The below are an overview of the CCG Priorities for 2014/15 and where IM&T is an key enabler or can contribute to achieving outcomes. These will form the basis of the strategy plan once the national strategies are agreed.
Corporate IM&T Enablers/ Requirements Stable Infrastructure Mobile working
Transformation of Care Joint working between GP practices 7 day Services
Access Improve Management of Patient in own home Self-Management
Efficiencies Mobile and Flexible Working
Quality Requirements QOF CQUINS Primary Care Quality Indicators Patient Experience
General Practice Information Technology Framework and local landscape of systems Clinical System optimisation Roadmap to re-commissioning of Core GP IT Services (GPSoC Framework)

17
Clinical Priorities Equality of Care Case Management for over 75s/End of Life Care Care Homes Commissioning Intensions Dementia
o Early diagnosis o Share dementia pathway o Dementia Hub
Cancer Screening Programme Respiratory Disease (Asthma & COPD) CVD Pathway Mental Healthcare pathway Diabetes
Integration of Care Data Sharing
Governance and Assurance Including Governance Review
Strategic and Operational Governance This section covers governance arrangement for the delivery of key IM&T related activities.
Current strategic governance:
Better Care Together IM&T Enablement Group – Provides strategic direction to LLR enablement IM&T initiatives. Aligns IM&T priorities with the Better Care Together strategy.
CCG IM&T Steering Group – Provides oversight and direction to CCG led IM&T project and initiatives.
Project Boards – Provides operational governance to individual projects.
JIGSG – Provides assurance from an IG perspective
There may be scope to extend and revise the governance structures.
Technical Governance This section covers technical governance in relation to IT projects. Technical Governance is currently provided to the CCG by Leicestershire HIS and GEM CSU. The process ensures that the right technical solutions are procured for the purpose of business change and benefits realisation.
Information Governance (IG) Information governance support is provided to CCG on a number of levels:

18
CCG Senior Information Risk Owner (SIRO) – Daljit Kaur Bains. This role is responsible for making key decisions on behalf of the CCG regarding information risk.
IG advice and guidance – This is currently provided by GEM CSU. This includes support for the IG toolkits.
IG support for patients – This is currently provided by the Area Team and covers access to patient records requests.
Assurance Project Assurance sits independently from a project and ensures that projects are delivery to time, to budget and within financial tolerances. This is currently provided by GEM CSU.
Information Management Information management for commissioning and risk stratification is provided by GEM CSU. This is in the form of HERA and will be superseded by GEMIMA.
Information Security This covers any information breaches from our network and existing systems. This support is currently provided by Leicestershire HIS.
Service Management This covers help desk support and ongoing support to clinical systems. This is currently provided by Leicestershire HIS.
Infrastructure This section looks at technical infrastructure to support HQ and GP practices. This includes networks and telephoney. This is currently provided by Leicestershire HIS.
Networks This looks at the network provided to support services within the CCG and GP practices. Ensuring that appropriate services are received and that downtime is limited. This is currently provided by Leicestershire HIS.
Communications This looks at the telephoney set up for the CCG and GP practices. This is currently provided by Leicestershire HIS.
Data and Storage This sections covers data, storage and availability of the correct amounts of data. It also looks at the management of data. This is currently provided by Leicestershire HIS.
Integration/Interoperability Requirement for CCGs to ‘drive integrated care through IT Strategy’

19
Strategy to Technology Alignment Map This section will be built from the Stakeholder Workshops that have been scheduled for October. This section will identify and detail which IM&T enablers and capabilities will support the delivery of the National and Local Priorities.
Funding Clarify the National and local funding available:
Tech Fund bid PM Challenge Nursing Fund Better Care Together Funding Revenue Allocation
o GPIT revenue monies - £812k LHIS allocation to spend against – GPIT / call off funds
o Capital depreciation Transitional Funding GPIT Capital Funds GPIT Joint Flex Funding:
o East CCG - £110k, which includes £62k Transition Monies
IM&T High-level Roadmap This section will set out the Roadmap derived from the Strategy to Technology Alignment Workshops. The Roadmap will include a combination of the existing project and programme portfolio and new initiatives that are required to support deliver of the strategy.
Conclusion This document provides an overview of the current situation with regards to the commissioning of IM&T services, relationships with GEM CSU/HIS, the overall governance structure, how IM&T support current CCG priorities and also considerations for the future. A final version will be developed in conjunction with the national IT strategies.
i Securing Excellence in GP IT Services: Operating Model 2nd Edition (2016-16) (p6) ii Securing Excellence in GP IT Services: Operating Model 2nd Edition (2016-16) (p9) iii ELR CCG Two-Year Operational Plan 2014/15 to 2015/16 iv NHS England: Strategic Systems and Technology Directorate Strategic Priorities


Blank Page

Paper J East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
1
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
Front Sheet
REPORT TITLE: Arriva Transport Solutions Ltd, (Non Emergency Patient Transport Service), Contract Year Three Agreement (July/ 1/ 2014 – June /30/ 2015)
MEETING DATE: 9 September 2014
REPORT BY: Connie Atugonza – Head of Finance
SPONSORED BY: Dr David Briggs, Managing Director, East Leicestershire and Rutland Clinical Commissioning Group
PRESENTER: Robin Wintle, Associate Director of Contracts and Provider Performance
PURPOSE OF THE REPORT:
This report details the outcome of the Contract Year Three review and negotiations of the Arriva contract which runs from 1st July 2014 to the 30th June 2015. Key issues addressed were the higher mobility mix and relative cost differentials, activity levels and escorts charging mechanism.
RECOMMENDATIONS: The East Leicestershire and Rutland CCG Governing Body is requested to: RECEIVE and APPROVE the agreed contract price and activity for Year Three.
REPORT SUPPORTS THE FOLLOWING STRATEGIC AIM(S) 2014 – 2015: Transform services and enhance quality of life for people with long-term conditions
Improve integration of local services between health and social care; and between acute and primary/community care.
Improve the quality of care – clinical effectiveness, safety and patient experience
Listening to our patients and public – acting on what patients and the public tell us.
Reduce inequalities in access to healthcare Living within our means using public money effectively
x
Implementing key enablers to support the strategic aims (e.g. constitutional and governance arrangements, communications and patient engagement).
EQUALITY ANALYSIS As this paper is for information only an equality impact assessment has not been undertaken.
RISK ANALYSIS AND LINK TO BOARD ASSURANCE FRAMEWORK:
As above.

Paper J East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
2
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
The Arriva Contract The Arriva contract is a block contract arrangement that spans five years from 2012/13 to 2016/17 with a provision for annual review of activity and price. Table 1 shows the Activity and Financial Performance for Contract Year One and Contract Year Two, as well as the agreed Contract Year Three position for core activity. Table 1
The Extra Contractual Journey activity, which was unplanned at the start of the contract term, was a cost pressure for both Contract Year One and Two and as such a provision has been made for it in Year 3. This ECJ cost pressure arises from the fact that the Points of Care stipulated in the original contract amounted to 36 in total but to date Arriva has identified over 140 additional points of care since taking on the service. In addition to this, Arriva pointed out that the mobility types which are determined by acuity of patients substantially vary from the information provided during the tendering process. There is a much higher case mix of patients in wheel chairs and those requiring stretchers and a lower number of ‘Walkers’ (see table 2). In addition there was a variation in activity distance as well with more journeys over 20 miles when compared to the original contract conditions. All this created an operational cost pressure for Arriva as their initial planning for the service was based on activity profiles and distances provided in the tender process. Arriva has therefore presented a case for additional funding to cover the increased costs arising from the case mix variation in Contract Year Three, amounting to 191k.
Contract Year
(June‐July) Activity Outturn Activity Outturn Activity* Outturn
Core 154,900 5,600,776£ 156,195 5,232,621£ 157,500 5,138,032£ Aborts 12,923 14,115 12,424
Escorts 30,782 28,690 28,690 161,968£ Sub total 198,605 5,600,776 199,000 5,232,621 198,614 5,300,000
Abort Incentive 5% 28,004£ 26,163£ 26,500£ Extra Contractural Journey's 10,304 834,407£ 14,288 968,160£ 14,288 968,160£ Total 208,909 6,463,187£ 213,288 6,226,944£ 212,902 6,294,660£
2012/13 Outturn 2013/14 outturn 2014/15 Plan

Paper J East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
3
Table 2
The Year Three negotiation process took into consideration the following factors to agree a core contract value for 2014/15
underperformance in 13/14 against core activity to determine a reasonable base for 2014/15
increase in acuity/distance, hence more expensive mobility, Inflation Adjustment A fixed sum for professional escort activity.
The core activity was rebased to provide a more accurate reflection for core journeys. This also includes an assumption that the discharge booking and release efficiency work being done within UHL will reduce the number of aborted journeys. It was agreed the cost saving from reduction in activity would compensate Arriva for the increase in costs associated with the change in mobility acuity and distances. It was agreed to provide for a fixed sum of £161k for escorts only in contract, Arriva had previously tabled a charge of £0.5m for escorts. The Governing Body is asked to receive and approve the agreed contract price and activity for Year Three
C + C1
(Walkers)
WC1 ‐
Wheelchair
WC2 ‐
Wheelchair
A1 ‐
Ambulance
X1
A2 ‐
Ambulance X2
ST ‐
Stretcher N/P Total
Contracted Activity Year 3 121,591 11,386 3,775 875 35,655 7,271 505 181,058
Year 2 Activity (forecast June ‐ April) 100,079 16,274 7,433 6,290 28,307 11,028 512 169,924
Total Activity Variance (21,512) 4,888 3,658 5,415 (7,348) 3,757 7 (11,134)
Total Activity Variance (%) ‐18% 43% 97% 619% ‐21% 52% 1% ‐6%
Activity Variance 0‐20 Miles (24,154) 4,387 3,494 4,836 (8,202) 3,264 (33) (16,408)
Activity Variance 21‐51+ miles 2,642 501 164 580 854 493 40 5,274
Changes in Cost £ ‐£ 371,764 £ 152,449 £ 215,327 £ 117,015 ‐£ 261,891 £ 339,618 £ 1,123 £ 191,877

Paper J East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
4
Appendix Table 5 Break down by CCG
CCG Contract Value Abort Incentive
East 1,625,534.6£ 7,879£ West 1,898,965.4£ 9,205£ City 1,775,500.0£ 8,606£ Total LLR 5,300,000.0£ 25,690£


Blank Page

Paper K East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
1
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
Front Sheet
REPORT TITLE: Leicester, Leicestershire and Rutland Better Care Together Programme Update-September 2014
MEETING DATE: 9 September 2014
REPORT BY: Geoff Rowbotham Interim Programme Director Better Care Together
SPONSORED BY: Dave Briggs, Managing Director ELR CCG
PRESENTER: Geoff Rowbotham, Interim Programme Lead
PURPOSE OF THE REPORT: The purpose of this report is to update the Health and Well Being Board on progress since it received the draft Better Care Together 5 Year Strategic Plan.
RECOMMENDATIONS: The East Leicestershire and Rutland CCG Governing Body is requested to: Receive for information and note the progress made
REPORT SUPPORTS THE FOLLOWING STRATEGIC AIM(S) 2014 – 2015: Transform services and enhance quality of life for people with long-term conditions
Improve integration of local services between health and social care; and between acute and primary/community care.
Improve the quality of care – clinical effectiveness, safety and patient experience
Listening to our patients and public – acting on what patients and the public tell us.
Reduce inequalities in access to healthcare Living within our means using public money effectively
Implementing key enablers to support the strategic aims (e.g. constitutional and governance arrangements, communications and patient engagement).
EQUALITY ANALYSIS An Equality Analysis and due regard to the positive general duties of the Equality Act 2010 has not been undertaken in the development of this report as it is judged that it is not proportionate on the basis that it is an update on progress against a document that has been previously assessed

Paper K East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
2
RISK ANALYSIS AND LINK TO BOARD ASSURANCE FRAMEWORK: This report updates progress on a corporate risk identified within the Board Assurance Framework

Paper K East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
3
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
GOVERNING BODY MEETING
Report of Leicester, Leicestershire and Rutland Better Care Together Programme
Programme Update –September 2014
9th September 2014
1. Purpose of report
The purpose of this report is to the East Leicestershire and Rutland Clinical Commissioning Group on progress since it received the draft Better Care Together 5 Year Strategic Plan.
2. Policy Framework and Previous Decisions
The East Leicestershire and Rutland Clinical Commissioning Group received the Leicester, Leicestershire and Rutland draft Better Care Together 5 Year Strategic Plan in July 2014 and has provided written feedback for inclusion in the final document for approval at 2nd October 2014 Better Care Together Partnership Board.
Background The Better Care Together (BCT) Programme Board is responsible for the production of the 5 year strategic plan for the Leicester, Leicestershire and Rutland (LLR) health and social care system. The Programme Board includes local social care, health commissioners and providers, public and patient representatives. It is supported by a structure of clinical, patient, public, and political reference groups, and by enabling groups e.g. Estates, Workforce, Information Technology
The BCT Programme is taking a phased approach to the production of the 5 year strategic plan: development (to June 2014); discussion and review (June to September 2014); and, implementation and formal consultation where required (October onwards). A first draft of a 5 year strategic plan was submitted on behalf of the LLR unit of health and social care planning to NHS England (NHSE) on 4th April 2014. NHSE required LLR, as a ‘unit of planning’ to submit a further update of the 5 year strategic plan to NHS England on Friday 20th June 2014, that triangulates with local CCG, provider, Health and Well Being, Local Authority and Area Team plans. The BCT Board met this requirement and submitted a draft strategic plan on 20th June.
During July –August 2014 the BCT Programme has been focused on;-
i. LLR DRAFT 5 YEAR STRATEGIC PLAN- ‘DISCUSSION AND REVIEW’ PHASE
ii. LEADERSHIP AND GOVERNANCE OF THE BCT PROGRAMME

Paper K East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
4
iii. DEVELOPING, RESOURCING AND COMMENCING SERVICE RECONFIGURATION
Considerable progress has been made during the past 8 weeks resulting in the programme being on schedule despite the challenging timescales it has set itself. The purpose of the paper is to provide a high level update on progress since July 2014 to highlight for the Board the key programme priorities for the next 3 months. Proposals/Options
i. LLR DRAFT 5 YEAR PLAN- ‘DISCUSSION AND REVIEW’ PHASE July-September 2014 The draft plan was publicly launched across LLR by the NHS and Social Care Partnership through a number of media events on Thursday 26th June. Following the successful launch it has been circulated to Partner Boards, Cabinet/Executives, key stakeholder and public groups for comment as well as being made available on the Better Care Together web site. www.bettercareleicester.nhs.uk/information-library/better-care-together-plan-2014. Meetings have included:- Public, Patient, Voluntary and Community sector events Public and patient events have been held by Leicester, Leicestershire and Rutland Health watch committees and a summary of recommendations is being provided for inclusion in the refreshed draft 5 Year Strategic Plan being submitted to the BCT Partnership Board in October. Voluntary Action Leicester (VAL) have organised and supported a number of engagement events as part of an agreed ongoing engagement process at which the plan has been reviewed. Partner Organisation-NHS Leicester City, West Leicestershire and East Leicestershire and Rutland Clinical Commissioning Groups have formally reviewed the draft plan. Clinical review of the draft 5 Year Plan has been undertaken by the joint BCT Health and Social care Clinical Reference Group and externally by the East Midlands Clinical senate. Partner Organisations-Local Authority The Leicester, Leicestershire and Rutland Health and Well Being Boards and Local Authority cabinets and executive team have reviewed the plan. Heath and Overview and Scrutiny Committees have noted the plan. National Bodies-NHS The plan has been reviewed by NHS England, Trust Development Authority and the NHS Local Area. Key next Steps

Paper K East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
5
-The feedback to date has been positive, constructive and supportive of the approach outlined within the plan. This feedback is being incorporated in a refreshed LLR 5 Year Strategic plan that is going to the Better Care Together Board on the 2nd October for approval. - In addition to the 5 Year Plan the BCT Partnership Board, as recognised within OGC best practice, is developing 2 supporting key documents:
A Programme Initiation Document (PID). This document defines the BCT programme and sets out the basis on which it is to be initiated, governed and delivered- September completion.
The Strategic Outline Case (SOC). Provides the LLR system ‘wrapper’ for the individual LLR organisations business cases to ensure that the proposed preferred way forward represents value for money-October completion.
- Primary and Adult Social Care Strategic reviews have commenced led be partnership organisations to respond to the proposals within the 5 Year strategic plan. The outline proposals will be incorporated within the 5 Year strategic plan refresh, PID and SOC -Following this the key strategic documents will be circulated to partner organisations Boards, Health and Well Being Boards and Health Watch Committees for formal approval- November 2014.
- These proposals will be incorporated into the partner organisations operating plans 2015/16.
ii. LEADERSHIP AND GOVERNANCE OF THE BCT PROGRAMME
July- September 2014 The BCT Partnership Board carried out a review, which was supported by external consultants EY, to establish the appropriate leadership and governance of the BCT programme. The key revisions to the existing structure agreed by the BCT Partnership Board were as follows: Better Care Together Partnership Board -The recruitment of a permanent independent Chair- Appointee commences October 2014. -The appointment of Senior Responsible Officers to lead the programme-John Adler Chief Officer UHL and Toby Sanders MD West Leicestershire CCG appointed from August 2014. -Streamlining and refocus of the Partnership Board –Membership reduced by 20%, Non- Executive/Lay membership added and agreement to hold public meetings bi monthly from January 2015-Approved July 2014. -Establishment of a cross partnership BCT delivery group –Established August 2014

Paper K East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
6
External Assurance The benefits of embedding an ongoing external assurance process has been adopted by the LLR BCT Partnership Board to ensure we recognise good practice and are able to demonstrate good governance. -Clinical Assurance has been through the 2 reviews completed by the East Midlands Clinical Senate of the draft 5 Year Strategic Plan. A further review of the detailed clinical work stream proposals has been scheduled for February 2014. -National Assurance has been through the NHS England Planning and Delivering service changes for patients good practice guide December 2013. The initial ‘strategic sense check’ of the 5 Year Plan and programme was completed in August 2014 and a letter of approval with recommendations has been received. Key next steps -An independent OGC external gateway best practice review is being undertaken to assess the BCT programme governance- Nov 2014. -A further NHS England review will be carried out with a particular focus on approving the formal readiness and process for any areas requiring formal consultation post May 2015- Spring 2014. -The establishment of a small permanent BCT cross partnership programme management office to develop and support across the LLR partner organisations an integrated implementation and governance process and report system performance-January 2015. iii. DEVELOPING, RESOURCING AND COMMENCING SERVICE
RECONFIGURATION August onwards
The 8 priority clinical work streams (Frail Older People, Long term Conditions, Mental Health, Urgent Care, Planned Care, Learning Disabilities, Maternity& Neonates and Children’s services) and supporting enabling programmes (Workforce, IM&T, Estates & Facilities, Communication & Engagement) identified within the 5 Year draft strategic plan implementation plans have commenced development through a workbook process. To support this work:
A core team consisting of a Senior Reporting Officer, Workbook lead, Clinical lead (Primary & Acute) and Finance lead have been established from across the partnership organisations for each of the clinical work streams and enabling programmes.
These are being supported by nominated leads from Public and Patient Groups, Communication and Public Health representatives.
The Better Care Fund programmes are being aligned within the appropriate Better Care Together work streams.

Paper K East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
7
A Communication and Engagement framework that recognises the need to tailor and differentiate our approach for key audiences and stakeholders i.e. Public and Patient engagement, Staff engagement and Partner Assurance through an ongoing engagement process is being developed jointly by the partner organisations Communication leads and the BCT Public and Patient Reference Group.
As part of this framework the Equality and Diversity leads have held a workshop to develop a shared approach to Equality, Diversity and Human rights.
This framework will build further on the ongoing need to ensure we continue to demonstrate assurance required against the four key tests for any major service change (ie strong public & patient support, patient choice, clinical evidence base and clinical commissioner support).
Key next Steps
-The review and approval of the clinical and enabling workbooks through the Clinical Reference Group and Better Care Partnership Board - October 2014.
-The resourcing and establishment of the approved implementation programmes - November 2014.
-The approval of the Communication and Engagement strategy framework to support the implementation and development of the formal engagement plan - October 2014.
-Following approval of the 5 Year Strategic Plan the process, programme and timescales to identify areas requiring formal consultation will be developed for approval and before any commencement planned for post May 2015.
Recommendation: The East Leicestershire and Rutland CCG Governing Body is requested to: Note the progress made over the past 12 weeks and the key next steps outlined

Paper K ELR CCG Governing Body
9 September 2014
1
LEICESTER, LEICSTERSHIRE and RUTLAND BETTER CARE TOGETHER
PROGRAMME UPDATE
September 2014
BACKGROUND
The Better Care Together (BCT) Programme Board is responsible for the production of the 5 year strategic plan for the Leicester, Leicestershire and Rutland (LLR) health and social care system. The Programme Board includes local social care, health commissioners and providers, public and patient representatives. It is supported by a structure of clinical, patient, public, and political reference groups, and by enabling groups e.g. Estates, Workforce, Information Technology.
The BCT Programme is taking a phased approach to the production of the 5 year strategic plan: development (to June 2014); discussion and review (June to September 2014); and, implementation and formal consultation where required (October onwards).
A first draft of a 5 year strategic plan was submitted on behalf of the LLR unit of health and social care planning to NHS England (NHSE) on 4th April 2014. NHSE required LLR, as a ‘unit of planning’ to submit a further update of the 5 year strategic plan to NHS England on Friday 20th June 2014, that triangulates with local CCG, provider, Health and Well Being, Local Authority and Area Team plans. The BCT Board met this requirement and submitted a draft strategic plan on 20th June.
During July –August 2014 the BCT programme has been focused on:-
i. LLR DRAFT 5 YEAR PLAN- ‘DISCUSSION AND REVIEW’ PHASE. ii. LEADERSHIP AND GOVERNANCE OF THE BCT PROGRAMME. iii. DEVELOPING, RESOURCING AND COMMENCING SERVICE
RECONFIGURATION.
Considerable progress has been made during the past 8 weeks resulting in the programme being on schedule despite the challenging timescales it has set itself. The purpose of the paper is to provide a high level update on progress during this time and to highlight the key programme priorities for the next 3 months.
i. LLR DRAFT 5 YEAR PLAN- ‘DISCUSSION AND REVIEW’ PHASE July-Sept 2014
The draft plan was publicly launched across LLR by the NHS and Social care partnership through a number of media events on Thursday 26th June. Following the

Paper K ELR CCG Governing Body
9 September 2014
2
successful launch it has been circulated to Partner Boards, Cabinet/Executives, key stakeholder and public groups for comment as well as being made available on the Better Care Together web site. www.bettercareleicester.nhs.uk/information-library/better-care-together-plan-2014.
Meetings have included:-
Public, Patient, Voluntary and Community sector events
Public and patient events have been held by Leicester, Leicestershire and Rutland Health watch committees and a summary of recommendations is being provided for inclusion in the refreshed draft 5 Year Strategic Plan being submitted to the BCT Partnership Board in October.
Voluntary Action Leicester (VAL) have organised and supported a number of engagement events as part of an agreed ongoing engagement process at which the plan has been reviewed.
Partner Organisation-NHS
Leicester City, West Leicestershire and East Leicestershire and Rutland Clinical Commissioning Groups have formally reviewed the draft plan.
Clinical review of the draft 5 Year Plan has been undertaken by the joint BCT Health and Social care Clinical Reference Group and externally by the East Midlands Clinical senate.
Partner Organisations-Local Authority
The Leicester, Leicestershire and Rutland Health and Well Being Boards and Local Authority cabinets and executive team have reviewed the plan. Heath and Overview and Scrutiny Committees have noted the plan.
National Bodies-NHS
The plan has been reviewed by NHS England, Trust Development Authority and the NHS Local Area.
Key next Steps
-The feedback to date has been positive, constructive and supportive of the approach outlined within the plan. This feedback is being incorporated in a refreshed LLR 5 Year Strategic plan that is going to the Better Care Together Board on the 2nd October for approval.

Paper K ELR CCG Governing Body
9 September 2014
3
- In addition to the 5 Year Plan the BCT Partnership Board as recognised within OGC best practice is developing 2 supporting key documents:
A Programme Initiation Document (PID). This document defines the BCT programme and sets out the basis on which it is to be initiated, governed and delivered- September completion.
The Strategic Outline Case (SOC). Provides the LLR system ‘wrapper’ for the individual LLR organisations business cases to ensure that the proposed preferred way forward represents value for money-October completion .
-Primary and Adult Social Care Strategic reviews have commenced to respond to the proposals within the 5 Year plan. The outline proposals will be incorporated within the 5 Year Plan refresh, PID and SOC - 1st Draft September.
-Following this the key strategic documents will be circulated to partner organisations Boards, Health and Well Being Boards and Health Watch Committees for formal approval- November 2014.
-Incorporated into the partner organisations operating plans 2015/16.
ii. LEADERSHIP AND GOVERNANCE OF THE BCT PROGRAMME July- Sept 2014
The BCT Partnership Board carried out a review which was supported by external consultants to establish the appropriate leadership and governance of the BCT programme. The key revisions to the existing structure agreed by the BCT Partnership Board were as follows:
Better Care Together Partnership Board
-The recruitment of a permanent independent Chair- Appointee commences October 2014.
-The appointment of Senior Responsible Officers to lead the programme-John Adler Chief Officer UHL and Toby Sanders MD West Leicestershire CCG appointed from August 2014.
-Streamlining and refocus of the Partnership Board –Membership reduced by 20%, Non- Executive/Lay membership added and agreement to hold public meetings bi monthly from January 2015-Approved July 2014.
-Establishment of a cross partnership BCT delivery group –Established August 2014

Paper K ELR CCG Governing Body
9 September 2014
4
External Assurance
The benefits of embedding an ongoing external assurance process has been adopted by the LLR BCT Partnership Board to ensure we recognise good practice and are able to demonstrate good governance.
Clinical Assurance has been through the 2 reviews completed by the East Midlands Clinical Senate of the draft 5 Year Plan. A further review of the detailed clinical work stream proposals has been scheduled for February 2014.
National Assurance has been through the NHS England Planning and Delivering service changes for patients good practice guide December 2013. The initial ‘strategic sense check’ of the 5 Year programme was completed in August and the plan approved.
Key next steps
An independent OGC external gateway best practice review is being undertaken to assess the BCT programme governance- Nov 2014.
A further NHS England review will be carried out with a particular focus on approving the formal readiness and process for any areas requiring formal consultation post May 2015- Spring 2014.
-The establishment of a small permanent BCT cross partnership programme management office to develop and support across the LLR partner organisations an integrated implementation and governance process and report system performance-January 2015.
iii. DEVELOPING, RESOURCING & COMMENCING SERVICE RECONFIGURATION Aug- onwards
The 8 priority clinical work streams (Frail Older People, Long term Conditions, Mental Health, Urgent Care, Planned Care, Learning Disabilities, Maternity& Neonates and Children’s services) and supporting enabling programmes ( Workforce, IM&T, Estates & Facilities, Communication & Engagement) identified within the 5 Year draft strategic plan implementation plans have commenced development through a workbook process. To support this work:
A core team consisting of a Senior Reporting Officer, Workbook lead, Clinical lead (Primary & Acute) and Finance lead have been established from across the partnership organisations for each of the clinical work streams and enabling programmes.

Paper K ELR CCG Governing Body
9 September 2014
5
These are being supported by nominated leads from Public and Patient Groups, Communication and Public Health representatives.
The Better Care Fund programmes are being aligned within the appropriate Better Care Together work streams.
A Communication and Engagement framework that recognises the need to tailor and differentiate our approach for key audiences and stakeholders i.e. Public and Patient engagement, Staff engagement and Partner Assurance through an ongoing engagement process is being developed jointly by the partner organisations Communication leads and the BCT Public and Patient Reference Group.
As part of this framework the Equality and Diversity leads have held a workshop to develop a shared approach to Equality, Diversity and Human rights.
This framework will build further on the ongoing need to ensure we continue to demonstrate assurance required against the four key tests for any major service change (ie strong public & patient support, patient choice, clinical evidence base and clinical commissioner support).
Key next Steps
-The review and approval of the clinical and enabling workbooks through the Clinical Reference Group and Better Care Partnership Board- October 2014.
-The resourcing and establishment of the approved implementation programmes- November 2014.
-The approval of the Communication and Engagement strategy framework to support the implementation and development of the formal engagement plan - October 2014.
-Following approval of the 5 Year Strategic Plan the process, programme and timescales to identify areas requiring formal consultation will be developed for approval and before any commencement planned for post May 2015.
G.W.Rowbotham
Interim Programme Director
Better Care Together


Blank Page

Paper L ELR CCG Governing Body Meeting
9 September 2014
1
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
Front Sheet
REPORT TITLE: Better Care Fund Rutland and Leicestershire Resubmission
MEETING DATE: September 2014
REPORT BY: Yasmin Sidyot (Head of Strategy & Planning)
SPONSORED BY: Jane Chapman Chief Strategy & Planning Officer
PRESENTER: Jane Chapman Chief Strategy & Planning Officer
PURPOSE OF THE REPORT: Detailed guidance was published for the resubmission of BCF Plans on 25th July. Revised deadline date of 12noon 19th September has been set. The amount type and depth of analysis required for the resubmission have substantially changed. This report summarises the progress made to date with the re-draft of the Rutland BCF Plan and the Leicestershire BCF Plan outlining the process and key changes made to the plan.
RECOMMENDATIONS: The East Leicestershire and Rutland CCG Governing Body is requested to: RECEIVE the report FOR INFORMATION PROVIDE feedback on the metrics and trajectories proposed in support of finalising these at the Health & Wellbeing Board on 17th September NOTE the main risks to the BCF plan resubmission and assurance, and the associated mitigation described in the report which includes:
• The delivery of the 3.5% target for total emergency admissions (advice sought from NHS England to reduce this)
• The need to secure additional assurance from the acute provider trust prior to the resubmission (actions have been identified and prioritised)
• The content being proposed to strengthen the risk stratification and population segmentation section of the plan (advice taken from national BCF support webinars/workshops)
• The assurance process for BCF plans (desk top review taking place ahead of the submission)

Paper L ELR CCG Governing Body Meeting
9 September 2014
2
REPORT SUPPORTS THE FOLLOWING STRATEGIC AIM(S) 2014 – 2015: Transform services and enhance quality of life for people with long-term conditions
x Improve integration of local services between health and social care; and between acute and primary/community care.
x
Improve the quality of care – clinical effectiveness, safety and patient experience
Listening to our patients and public – acting on what patients and the public tell us.
Reduce inequalities in access to healthcare Living within our means using public money effectively
x
Implementing key enablers to support the strategic aims (e.g. constitutional and governance arrangements, communications and patient engagement).
EQUALITY ANALYSIS 1. An Equality Analysis and due regard to the positive general duties of the Equality Act 2010
has not been undertaken in the development of this report as it is judged that it is not proportionate on the basis that this report is an update on national changes being made to local plans.
RISK ANALYSIS AND LINK TO BOARD ASSURANCE FRAMEWORK: Questions to consider:
Does the report align to corporate risks identified in the Board Assurance Framework? Yes
Does the report support in mitigating the risk(s) identified? Yes Does the report highlight a new risk(s)? if so please quantify the risk using the 5 x 5 risk
matrix or discuss with the Corporate Affairs Team. No

Paper L ELR CCG Governing Body Meeting
9 September 2014
3
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
BETTER CARE FUND RESUBMISSION RUTLAND
September 2014 1. Introduction and Background 1.1 Detailed guidance was published for the resubmission of BCF Plans on 25th
July. A revised deadline date of 12noon 19th September has been set. The amount type and depth of analysis required for the resubmission have substantially changed.
1.2 This report summarises the progress made to date with the re-draft of the
Rutland BCF Plan outlining the process and key changes made to the plan.
2. Summary Update Points from the Rutland BCF Plan 2.1. There is a pay for performance requirement on the fund linked to achieving a
reduction in all non-elective (emergency) admissions. Each Health and Wellbeing Board must approve the local threshold for the reduction in non-elective admissions. However there is an expectation that this will need to equate to a 3.5% reduction from Q4 2014/15 to Q3 2015/16.
2.2. On 20th August further information was published on the flexibilities associated with this metric, which can apply in certain circumstances. A local target below 3.5% can be proposed with the agreement of the local health and wellbeing board, if there is a clear rationale for this.
2.3. Local analysis has been undertaken for Rutland with regard to the 3.5% (reduction of 103 non-elective admissions for Rutland) metric. The financial risk associated with this metric if not achieved for Rutland is £194,000. The Rutland Integration Executive on 4th September discussed whether this was a realistic and achievable target for Rutland. The reasons for this concern are due to the population size of Rutland is small and therefore the level of reduction although small creates greater risk of non-delivery due to external factors that could impact on non-elective admissions going up. This has been discussed with NHS England and it has been agreed that Rutland can set a lower reduction than 3.5%. a proposed revised target of 2% for Q4 2014/15 and 2.5% for 2015/16 is being worked up to include in the final submission for BCF submission. This reduces the financial risk for the CCG, Rutland CC and acute providers.
2.4. All BCF Schemes that currently sit in the plan have been assessed to determine their contribution to the non-elective admissions metric and the remaining 5 metrics in the plan. A greater level of detail about their potential

Paper L ELR CCG Governing Body Meeting
9 September 2014
4
impact, with mapping to the new benefits analysis for the resubmission, including expressing impact in terms of activity and finances by organisation have been developed.
2.5. The new BCF guidance also asks for greater detail on the approach to risk stratification and population segmentation in support of BCF plans to demonstrate case for change. While it is not expected that local areas can achieve the “gold standard” example given in the national webinar (which would be a 6-12 month piece of work entailing changes to Information Sharing Agreements), local areas have been recommended to do the following as a starting point: 2.5.1. Provide an initial analysis that is achievable within 2-3 weeks, (we
have requested this from the Greater East Midlands Commissioning Support Unit)
2.5.2. Set out an indicative action plan to achieve the longer term piece of work.
2.6. The Integration Executive agreed the use of 1 patient experience metric from the Adult Social Care survey where we have a good baseline to support the development of the metric. furthermore it was agreed that injuries due to falls would remain as the local metric.
2.7. Provider sign off by Acute trusts is essential for BCF submission, in particular the plans to meet the 3.5% total emergency admissions metric and the impact on the acute sector’s activity and income. Discussion with UHL and Peterborough Hospital has taken place through the Integration Executive which has identified where additional assurance is needed and a number of actions have been agreed to provide the additional information ahead of the resubmission.
2.8. Further guidance was issued on 2/9/14 about BCF risk sharing agreements and the current narrative within the BCF plan submission is being cross checked against this guidance.
2.9. A full refresh of the BCF Risk Analysis and BCF Programme Plan has been undertaken in support of the resubmission and these documents are currently with partners for comment ahead of the Health and Wellbeing Board meeting on 17th September.

Paper L ELR CCG Governing Body Meeting
9 September 2014
5
2.10. Payment will be made in May 2015 and will be CCGs will be requested to release this into the BCF. The payment is related to the level of performance, therefore if only 70% of the target is achieved; only 70% of the payment into the BCF will be made. Payments will then be made quarterly in arrears on the same basis. Any monies not paid into the fund due to lack of performance will be held by the CCG and spent by agreement to offset the activity incurred in the acute sector as a result of failing to avoid sufficient admissions.
3. Next Steps and Milestones 3.1. Drafts of the BCF submission materials for Template 1 and 2 are now
available. These have been shared with the Integration Executive and comments are being received from partners ahead of the Health and Wellbeing Board meeting on 17th September.
3.2. Significant work is still ongoing to finalise the documents in the remaining time
available before the resubmission, in particular: 3.2.1. Securing acute provider sign off 3.2.2. Finalising the risk sharing agreement 3.2.3. Taking into account additional BCF guidance as published 3.2.4. Developing and agreeing the revised non-elective admissions metric 3.2.5. Incorporating advice from the national support offer, including:
o The recommended risk stratification and population segmentation analysis
o Findings from a desk top review of the final draft of the plan against the assurance process criteria (to identify and address any remaining gaps and risks where possible)
4. Summary
4.1. The requirements for BCF resubmissions are substantial and the timescales are challenging.
4.2. There has been a significant amount of new information to assimilate from July 25 to date, all issued during peak holiday season.
4.3. The assurance process indicates that BCF plans in challenged health and care economies are likely to receive low ratings (e.g. approved with conditions).
4.4. The 3.5% metric presents a specific challenge to the Rutland plan however agreement from NHS England has been sought to revise the metric from 3.5% to 2 – 2.5%.

Paper L ELR CCG Governing Body Meeting
9 September 2014
6
4.5. A timeline for the remaining period was prepared, including the governance steps needed ahead of the resubmission
4.6. Actions have been prioritised to address acute provider concerns 4.7. A desk top review of the submission by an external supplier has been
commissioned from the national support offer.

Paper L East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
1
LEICESTERSHIRE BETTER CARE FUND
PROGRESS REPORT ON THE NATIONAL BCF RESUBMISSION
Overview of National Developments July/August 2014
1. A new set of detailed guidance for BCF plans was published on July 25th, 2014 which is to be applied to BCF resubmissions for each HWB area. The deadline for these resubmissions is 12.00 noon on September 19th 2014.
2. A summary paper for Leicestershire’s Health and Wellbeing Board, highlighting the key points of the guidance was issued on August 5th which highlighted that the amount, type and depth of analysis needed for each BCF resubmission have changed substantially. This has been due to requirements for more rigour in BCF plans nationally, in particular with reference to NHS acute sector impact.
3. There is now a new pay for performance scheme linked to a revised BCF metric
which equates to a reduction of 3.5% in total emergency admissions in 2015/16. 4. The baselines for all the metrics in the BCF guidance have been revised
using2013/14. This means all the metrics and trajectories in the BCF plan have had to be recalculated / revalidated.
5. The submission entails a much more extensive schedule of what needs to be
included in Template 1 has been issued. 6. Template 2 includes the detailed analysis for metrics, benefits realisation and
expenditure plans. The new technical guidance covers how this should be prepared linking to the pay periods for the pay for performance scheme.
7. The seven national conditions still apply to the resubmission as follows::
Protecting adult social care services How the NHS number will be adopted The arrangements for accountable leads professionals for care planning How care act requirements have been met (with reference to the total
allocation by LA) How information governance has been addressed for records sharing How a proportion of the funds will be commissioned from NHS providers
outside of hospital. Alignment to local primary care strategies including co-commissioning plans
with NHS England.
8. The publication of the new guidance raised a large number of questions and clarifications across the county. These have been handled through a number of routes over the past few weeks as follows:

Paper L East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
2
National Webinars with Q&A - scheduled via the BCF national web pages, available also as archived files.
Individual questions/regionally collated questions submitted to the national BCF team/central email address – leading to a FAQs section of the webpages.
E-bulletins issued from Andrew Ridley, national BCF lead. Additional materials and guidance published since July 25th (e.g. on 20/8/14
additional guidance on was published on the 3.5% metric and the circumstances in which flexibility might be agreed).
Check point returns from each HWB area – these are template forms that have to be submitted nationally which test the readiness for resubmission at 3 specific dates between 25th July and 19th September.
9. In recognition of the more onerous and complex process for BCF resubmissions, some additional (nationally procured) support was made available with effect from 26th August in each region. This has included: BCF Regional Workshops - in the East Midlands this took place on 1/9/14
and consisted of booked “surgery” sessions where individual BCF teams could bring their draft plans and raise specific concerns/queries. 4 people from the Leicestershire BCF team attended to raise specific questions related to metrics and benefits in annex 2, and the new expectations with respect to risk stratification data which had been covered in a national webinar.
A new BCF “How to Guide” was also published on 2/9/14 setting out guidance covered primarily in national webinars and workshops over.
Additional “hands on” support into individual HWB areas – this is being
coordinated by NHSE and a nationally procured supplier. Support is targeted on the basis of need highlighted at BCF check point 1. We have been allocated 2 days resource from the external consultants, which we will be using for a desk top review of Template 2 and a desk top review of our entire submission against the assurance process.
10. While the additional support is welcomed, feedback has been given that this
comes at a very late stage in the process raising some practical/logistical difficulties for local areas to make best use of this in sufficient time for the resubmission. There is also the need to factor in the lead time needed to secure approval of BCF resubmissions through various governance routes (including getting specific assurance from providers and approval of the overall plan by health and wellbeing boards), ahead of the 19th September.
Update on BCF Assurance Process 11. The assurance process is being led by North East London Commissioning
Support Unit. On 20th August details of this process were published showing the methodology and criteria for assessing BCF plans, aiming to give a consistent process across the country. See BCF web pages NHS England and LGA for the detail.

Paper L East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
3
12. This is an intensive process involving a technical desk top review, triangulation of
other evidence about the wider context of the financial and delivery challenges facing local health and care economies, plus it involves a telephone interview with representatives from each BCF plan/HWB Board area.
13. The outcome of the review will be that all BCF plans fall into one of four
categories below, which have specific definitions: 1. Approved 2. Approved with support 3. Approved with conditions 4. Not approved
14. The assessment for categorisation will be determined by:
The National Consistent Assurance Review of the quality of the plans The assurance checkpoints’ assessment of the risk to delivery due to the
local context facing each local health economy 15. We expect the assurance process to take place w/c 22/9/14 and w/c 29/9/14.
This will be followed by national moderation, with reporting up to ministerial level. Additional Guidance on the 3.5% metric 16. On 20th August further information was published on the flexibilities associated
with this metric, which can apply in certain circumstances. A local target below 3.5% can be proposed with the agreement of the local health and wellbeing board, if there is a clear rationale for this - e.g. if the historical performance of the local health and care economy has already taken the area into the top quartile of performance nationally, if there are problems with the local baseline information or other specific local challenges which mean the target is unachievable in the short term.
Adapting the Leicestershire BCF Plan to the New Guidance 17. Analysis has been undertaken on the local health and care economy position with
regard to the 3.5% metric. The financial risk associated with this metric, if we are not able to achieve it, is £2.84m for Leicestershire’s BCF Plan. A meeting is being held with NHS England in early September to review the implications of this metric.
18. During August, further impact assessment work through 2 workshop sessions took place to refine the Leicestershire BCF Plan. The first workshop focused on the BCF interventions that will contribute to the new emergency admissions metric. This session assessed there are currently 4 main schemes which will contribute to this metric and considered the proportion each are estimated to contribute. Individual trajectories were then developed based on the operational phasing and implementation in each case.

Paper L East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
4
19. These trajectories have been presented to the Integration Executive on September 1st and have also been shared with the Executive Teams of University Hospitals of Leicester and Leicestershire Partnership Trust. These are now in the process of being finalised.
20. At the second workshop we reviewed and discussed all other BCF schemes and
their contribution to the other metrics within the BCF plan, to test the assumptions about scale of delivery and phasing of the impact. Although the other metrics are not subject to pay for performance, a greater level of detail about their potential impact, with mapping to the new benefits analysis for the resubmission, including expressing impact in terms of activity and finances by organisation have been developed.
21. The above has been supported by a review of the BCF evidence base using local
and national sources of evidence, undertaken by Public Health.
22. Further work has been completed during July/August to assess the data quality and data capture for all BCF schemes. Recommendations have been made from this to the Integration Executive on 1st September, showing how the data for achieving the metrics should be strengthened - e.g. via clinical audit, statistical processes, formal evaluation, and the work already completed/in progress on the performance dashboards for the integration executive and step up/step down working group.
23. The new BCF guidance also asks for greater detail on the approach to risk
stratification and population segmentation in support of BCF plans to demonstrate case for change. While it is not expected that local areas can achieve the “gold standard” example given in the national webinar (which would be a 6-12 month piece of work entailing changes to Information Sharing Agreements), local areas have been recommended to do the following as a starting point:
Provide an initial analysis that is achievable within 2-3 weeks, (we have
requested this from the Greater East Midlands Commissioning Support Unit) Set out an indicative action plan to achieve the longer term piece of work.
24. The Integration Executive approved on 1st September, the proposed 3 patient
experience questions, and that injuries due to falls should remain as our local metric, while a further local metric on LOS is also being developed in conjunction with the LLR 5 year plan.
25. The BCF financial plan has now been re-profiled to accommodate the contingency needed for the 3.5% target, additional Care Act requirements, and the rephasing of BCF schemes per the impact assessment actions noted above.
26. Appendix 3 shows the revised BCF spending plan. There is a reconciliation tab
showing where key changes have been made since the April submission.

Paper L East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
5
27. Provider sign off by Acute Trusts is essential for BCF resubmission, in particular the plans to meet the 3.5% total emergency admissions metric and the impact on the acute sector’s activity and income. Discussion with UHL’s Executive Team has identified where additional assurance is needed and a number of actions have been agreed to provide the additional information ahead of the resubmission.
28. Further guidance was issued on 2/9/14 about BCF risk sharing agreements and
the current narrative within the BCF plan submission is being cross checked against this guidance.
29. A full refresh of the BCF Risk Analysis and BCF Programme Plan has been
undertaken in support of the resubmission and these documents are currently with partners for comment ahead of the Health and Wellbeing Board meeting on 16th September.
Next Steps and Milestones 30. Drafts of BCF submission materials for Template 1 and 2 are now available.
These have been shared with the Integration Executive and comments are being received from partners ahead of the Health and Wellbeing Board meeting on 16th September.
31. Significant additional work is still needed to finalise the documents in the remaining time available before the resubmission, in particular:
Securing acute provider sign off Finalising the risk sharing agreement wording Taking account of any additional BCF guidance which is published Incorporating advice from the national support offer, including
o The recommended risk stratification and population segmentation analysis
o Findings from a desk top review of the final draft of the plan against the assurance process criteria (to identify and address any remaining gaps and risks where possible).
Summary
The requirements for BCF resubmissions are substantial and the timescales are challenging.
There has been a significant amount of new information to assimilate from July 25 to date, all issued during peak holiday season.
The assurance process indicates that BCF plans in challenged health and care economies are likely to receive low ratings (e.g. approved with conditions).
The 3.5% metric presents a specific challenge to the Leicestershire plan however 4 schemes have been identified that will contribute to achieving this metric.
A timeline for the remaining period was prepared, including the governance steps needed ahead of the resubmission

Paper L East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
6
Actions have been prioritised to address acute provider concerns A desk top review of the submission by an external supplier has been
commissioned from the national support offer. Recommendations
The CCG Board is asked to receive the update on work in progress to finalise the submission.
The CCG Board is asked to provide feedback on the metrics and trajectories in Template 2 in support of finalising this for approval these at the health and wellbeing board meeting on 16th September.
The CCG Board is asked to provide feedback on the BCF spending plan in support of finalising this for approval at the health and wellbeing board meeting on 16th September.
The CCG Board is asked to note the main risks to the BCF plan resubmission and assurance, and the associated mitigation described in the report which includes:
o The delivery of the 3.5% target for total emergency admissions (advice being sought from NHS England)
o The need to secure additional assurance from the acute provider trust prior to the resubmission (actions have been identified and prioritised)
o The content being proposed to strengthen the risk stratification and population segmentation section of the plan (advice taken from national BCF support webinars/workshops)
o The assurance process for BCF plans (desk top review taking place ahead of the submission)
Cheryl Davenport Director of Health and Care Integration (joint appointment) September 3, 2014

Paper L East Leicestershire and Rutland CCG Governing Body meeting
9 September 2014
7
Appendix 4: BCF Resubmission Key Milestones
Date Milestone Notes 26th August
HWBB & Integration Exec Briefing 5.00 – 6.00pm Framland Cttee Room, LCC
26th August WLCCG Strategy and Planning group BCF update paper
2pm Woodgate Loughborough
26th August Confirmation of any additional national resources we can draw down locally in LLR
Currently Liaising with NHSE and suppliers about this.
28th August LCC Corporate Management Team – BCF update paper
9.30am – 11.00am – exact slot to be confirmed
1st September
BCF regional workshops
Kegworth or Loughborough – external suppliers procured nationally
Integration Executive Meeting Review of draft submission materials, with list of key decisions to approve
5.00 – 6.30pm Framland Ctte Room, LCC Papers to be circulated 28th August
2nd September
Better Care Together BCF update BCT Programme Offices St John’s House
2nd September UHL Exec Team BCF update paper/implications for providers, assurance on provider support
1pm – LRI - room location to be confirmed.
3rd September
NHS England/LLR CCG MDs Meeting ref 3.5% target
15.30 – 16.30 NHSE Grove Park: Fosse House
8th September EL&R CMT BCF update paper
9.30am Bridge Park Plaza
8th September
LPT Exec Team BCF update paper/implications for providers, assurance on provider support
1-4pm Evington Centre LGH (30min slot being confirmed)
9th September
ELR & WL CCG Board Meetings Draft BCF submission materials and key decisions for approval
2nd – 9th Recommended additional action: Desk top review of submission against assurance pack with feedback to H&WBB on 16th
Independent Opinion (can potentially be drawn down from the nationally procured BCF support offer)
16th September
Health & Wellbeing Board 2.00 – 4.00pm LCC Committee Suite – room TBC Papers to be circulated 9th September
19th September
BCF plan submission day – 12.00 deadline
w/c 22nd Sept and w/c 29th Sept
BCF plans undergo national assurance process.
Exact timings to be confirmed for the Leicestershire plan


Blank Page

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
1
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
Front Sheet
REPORT TITLE:
Strategy Planning and Commissioning Committee summary
MEETING DATE:
9 September 2014
REPORT BY:
Brandy Miller, Project Support Officer
SPONSORED BY:
Yasmin Sidyot, Head of Strategy and Planning
PRESENTER:
Andy Ker, Clinical Vice Chair
PURPOSE OF THE REPORT: This report aims to provide a summary of key areas of discussion and outcomes from the Strategy, Planning and Commissioning (SPC) Committee held on Tuesday19th August 2014. Approved minutes from the 15th July meeting are appended to the report for reference.
RECOMMENDATIONS: The East Leicestershire and Rutland CCG Governing Body is requested to: RECEIVE the report for information.
REPORT SUPPORTS THE FOLLOWING STRATEGIC AIM(S) 2014 – 2015: Transform services and enhance quality of life for people with long-term conditions
Improve integration of local services between health and social care; and between acute and primary/community care.
Improve the quality of care – clinical effectiveness, safety and patient experience
Listening to our patients and public – acting on what patients and the public tell us.
Reduce inequalities in access to healthcare Living within our means using public money effectively
Implementing key enablers to support the strategic aims (e.g. constitutional and governance arrangements, communications and patient engagement).
EQUALITY ANALYSIS An Equality Analysis and due regard to the positive general duties of the Equality Act 2010 has not been undertaken in respect of this report. The SPC Committee, through its review and approval of business cases, seeks assurances in respect of compliance with statutory requirements, including compliance with the Equality Act. The equality analysis can be found within each business case.
RISK ANALYSIS AND LINK TO BOARD ASSURANCE FRAMEWORK: The SPC Committee has the remit to seek assurance in respect of the risk management of projects through review of risks and issues logs included in business cases and monthly Quality, Innovation, Productivity and Prevention (QIPP) Project Dashboard Report. Links to Board Assurance Framework Reference:

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
2
BAF2: Patients and the public may not be able to influence CCG decisions within all stages of the commissioning cycle through consultation and engagement. BAF 9: Inability to deliver against the QIPP agenda resulting in failure to transform services.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
3
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
Summary Report Strategy, Planning and Commissioning Committee Summary and outcome of meetings The Strategy, Planning and Commissioning (SPC) Committee meeting was held on the 19th August 2014 and the following provides a summary of the key areas of discussion during this meeting:
1. July 2014 Highlight Report - Review To Determine The Optimum Number Of Community Inpatient Beds To Be Commissioned By The CCG
Ms Sue Bishop, Interim Strategy and Planning Manager, presented the report which was received and provides an introduction to the Project and outlines progress made during July 2014. Ms Bishop drew attention to the following strategic risks:
a. Availability of data to inform capacity and financial planning models needed to support the project
b. Resources available to immediately commence work on the subsequent business case
A number of queries were raised and discussed. Ms Bishop advised that her work was following a four stage process:
c. Stage 1 involved assessing current capacity and models of care with the final Stage 4 detailing where we want to be and what capacity will be needed to meet demographic demands in future.
d. The two steps in the middle are made up of (Stage 2) the quantified impact of things we have started, particularly in relation to use of Better Care Fund this year and the new health and social care services to try and reduce demand for inpatient stays, and (Stage 3) those other developments that will need to be put into place to bridge the final gap to Stage 4. Ms Bishop highlighted a risk in relation to the quantified impact of these middle stages as many of the developments were still being put into place and therefore it is difficult to understand the impact on this year and how to maximise them. Ms Bishop informed the Committee that more detailed quantified analysis would need to be contained within the full business case when that is produced.
Miss Rogers highlighted the importance of having early conversations with HealthWatch representatives as part of the CCG’s engagement work. Ms Bishop agreed this would be helpful and asked Ms Rogers to invite her to her next meeting with HealthWatch.
2. Community Services Strategy update Mrs Wendy Pearson, presented the report which provides an update on development of the Community Services Strategy to date, next steps and timescales for completion.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
4
Mrs Pearson highlighted key points as: e. The SPCC received a proposed framework for production of the Community Services
Strategy at the May SPCC, the focus has since been reviewed following issue of the LLR 5-year BCT Directional Plan. It was agreed that the focus will be on the frail, elderly and those with co-morbidities.
f. A literature review and review of the evidence regarding case of need has been undertaken which re-enforces the importance of frail and elderly in terms of step up and step down for community services.
g. The first draft of the strategy has been produced with the intention of outlining what the evidence and policy tells us, in order to aid discussions that will inform the next stage of development. As such, it is a high level directional strategy informed by published literature.
Next steps were highlighted as: h. The draft will be considered by commissioning colleagues and wider stakeholders. i. The plan will go to the Quality and Clinical Governance Committee on 2 September
2014 j. Governing Body to receive and comment on 9 September 2014.
The report was received acknowledging the timescales and resource commitments required to complete the draft framework strategy, along with opportunities for contributing to the strategy.
3. Commissioning Intentions Process Update
Mrs Charlotte Richardson presented the report which outlines the timeline to deliver the commissioning intentions for 2015/16. Mrs Richardson drew attention to key areas of work:
a. A review of current work programmes and developments will be underway until October 2014 in line with emerging guidance
b. There will be consultation with member practices and other key stakeholders c. The Commissioning Intentions will be published between January – March 2015
A number of queries were raised and discussed.
d. Mrs Sidyot explained the commissioning intentions originally spanned over two years in line with the Two Year Operational Plan. However, due to the subsequent revisions to the BCF Plan and the LLR BCT 5 Year strategy provides an opportunity to refresh the Two Year Operational Plan and an opportunity to revisit the commissioning intentions.
e. Mrs Sidyot drew attention to the LLR QIPP meeting which was held on Friday 22 August 2014 where the CCG would be pushed for their commissioning intentions.
f. In regards to communications and engagement for the commissioning intentions the process is to use as many existing events and forums.
g. Dr Briggs noted a decommissioning intentions session needed to be booked in.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
5
4. Business Case Cardiovascular Disease (CVD)
Mrs Charlotte Richardson presented the report which provides an update on the CVD developments for ELR CCG in 2014/15. Mrs Richardson drew attention to the 5 developments as follows:
Development 1 – Atrial Fibrillation in Screening and Management – Primary Care.
Development 2 - Heart Failure Virtual Advisory Service – UHL Development 3 - One Stop Rapid Access Clinic – UHL Development 4 - Review of HF Nurse Role – CHS Development 5 – Heart Failure Rehabilitation
A number of queries were raised and discussed.
Mrs Chapman queried whether there any outcomes to demonstrate the benefits available. Mrs Richardson advised there was an evaluation completed in regards to the training, however as the virtual review and rapid access clinic only started recently and there was no information available yet. Mrs Richardson agreed to check for any initial data.
Dr Briggs queried where the target of AF prevalence was recorded. Mr Barratt explained this was recorded in the primary care dashboard and there had been an increase in prevalence recording.
Dr Briggs raised concern over the statistic which states 32% of patients within the CCG are not on appropriate anticoagulation and felt this needs rapid change and asked to see progress and this and asked for information from practices on what they are doing around this by December. Mrs Richardson confirmed this information was built into the training course so which was due to end in October so there would be information that could be obtained from that.
Dr Ker queried why Choose and Book advice was not being utilised for the virtual Advisory Service as the CCG was potentially paying for something that could already be available. Mrs Richardson explained this related to a different cohort of patients however would query this.
The Committee received the report acknowledging the timescales and approved resource commitments required to complete the programme.
5. GP Support and Investment Plan Dashboard June 2014
Mr Jamie Barrett presented the report which provides an update on the GP Support and Investment Plan and associated indices. Mr Barrett highlighted key points to note as:
a. Out of ELR’s 34 GP practices 3 data submissions are still outstanding for May or June (These outstanding submissions are being chased hence reported amber position).
b. There has been a general positive trend with an increase in Palliative Care Registers, Care plans, After Death Audits, Death in place of choice, COPD registers and Atrial Fibrillation Registers.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
6
c. Prescribing is showing as a £50k underspend at M2 (May) d. The dashboard has been changed in respect of comments received previously from
the committee.
A number of queries were raised in relation to the data and discussed. Dr Ker suggested including locality baselines. Dr Briggs noted that the report was positive, especially in relation to the number of people who have died in their place of choice which had risen 57%
6. Draft Dashboard Step up and step down for community services
Mrs Wendy Pearson presented the dashboard which is the first draft dashboard for frail older people and co-morbidities. Ms Pearson noted:
a. The dashboard started off by taking all the things around step up and putting them into separate boxes and making sure there are clear KPIs which can be tracked.
b. This will now include Step down (community re-ablement step down) c. Risks and mitigations are up to date d. Further work is required to get KPI’s and activity populated. e. This is still work in progress.
A number of queries were raised and discussed.
f. Mrs Sidyot highlighted an issue in terms of validation of the data feed coming from LPT and obtaining the dashboard from them. A contract query has been issued contract in terms of getting an agreement on contract activity. The CCG has been given assurances that data should be coming through from next month.
g. Mrs Sidyot added that another element that starts from 1st September 2014 is the integrated crisis response (night nursing and assessment service). There have been some KPI’s agreed and this is in the process of being signed off.
h. Dr Ker queried what engagement was being undertaken with the GPs in relation to the night nursing service. Mrs Sidyot advised information has been sent to locality leads and formed part of the locality agenda for next month. This also applied to OOH via CNCS and EMAS.
The dashboard was received.
7. NHS 111/ DHU
Dr Briggs presented the report which provides details an options appraisal for the NHS 111 and Urgent Care Services. Dr Briggs provided a brief update on the background noting there are currently negotiations ongoing in relation to changing the price of the NHS 111 service. This has resulted in a contract variation which means the service has to go out to re-procurement. Dr Briggs requested the group to consider key elements around the following:
a. The scope of the procurement exercise in terms of what should be included Dr Briggs highlighted a view from Mr Mick Connell who was keen to see a clear way that joint community services were fully integrated fully.
b. Whether the CCG want to keep a NHS 111 service with a call centre with a clinical service, or whether they would prefer to incorporate it into Out of Hours.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
7
c. Whether the CCG wants to commission this as a group of counties or as four individual counties.
Dr Briggs highlighted the key risks as:
d. Currently they interface with 111 and OOH could be improved. However there is some synergy.
e. Separating the services could have a significant financial impact in terms of duplicating phone systems
f. Trying to maintain two separate Directory of Services could be challenging. A number of queries were raised and discussed. Dr Briggs requested the group to think about the points raised and provide comments electronically before the Commissioning Collaborative.
8. QIPP Project
Mrs Yasmin Sidyot presented the report which provides August 2014 project updates presented in the 2014-2015 ELR CCG QIPP dashboard including the QIPP activity dashboard developed by GEM. Mrs Sidyot drew attention to:
a. CHC Update: A process to review of all fast tracks has been implemented, and a financial model has been developed to demonstrate current cost and savings due to changes being made in relation to current live cases of fast tracks, and all new referrals in to fast track. Since changes have been made to the referral process in fast track there has been a significant drop in the number of referrals. The fast track finance report provides details of the work carried out to date. Projected savings for fast track element are around £1.1 million By the end of the financial year. The CHC referrals and processes are being reviewed and financial modelling is being scoped to explore further potential savings that can be made 2014/15. The current gap remains at £1.9 million. By the end of next week should be an updated position.
b. Activity: The QIPP activity dashboard as produced by GEM provides the actual activity against planned that has been transacted into the acute contracts for the 5 QIPP programmes:
c. Currently 4 of the 5 QIPP programmes reported on the dashboard are on plan which are
‐ COPD non - elective, emergency admission ‐ CVD - non elective, emergency and elective, daycase admissions ‐ First and follow up outpatient attendance, treatment specialty in
diabetic medicine QIPP Scheme is hitting amber and Mrs Richardson is picking this up.
‐ Urgent & Emergency Care at UHL provider
d. There has been a 7% increase in activity in month 3 compared to month 2 for Emergency Admission Avoidance QIPP scheme. An activity query notice has been sent to UHL as issues with coding and counting have been cited for the increase in emergency admissions. The significant increase in emergency

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
8
admissions has also been an issue for the other 2 CCGs, hence the reason why coding, counting and data validity is being queried with UHL. Once these issues have been resolved this will give us a truer picture of emergency admissions. No response has yet been received however the team continue to chase.
A number of queries were raised and discussed.
Mr Martin acknowledged that the Emergency Admission Avoidance target was a risk. Mrs Sidyot explained the target was calculated looking at a baseline (3%), which was acknowledged as ambitious at the time. However, this was because it needed to be in line with additional requirements as set out in the operational plan. Mr Martin requested clarification on what the CCG needed to do in order to recover the position. Mrs Sidyot explained that when changes are made by the CCG, other changes are made in response. Mrs Sidyot referenced anecdotal evidence which demonstrates changes in behaviour are as a direct response to change in pathways.
9. QIPP Challenge
Mrs Yasmin Sidyot presented the report which provides an update on the identified areas of work for the QIPP challenge.
a. Mrs Sidyot explained that there was work underway in relation to each of the actions to quantify savings in terms of reductions and what isn’t going to enable us to have any impact and rule that out.
b. Dr Briggs highlighted the importance of colleagues coming forward with ideas within the next four weeks otherwise the disinvestments for next year will be bigger.
c. Mrs Sidyot explained she would still value input on things such as MRET highlighting it was better to know earlier so a decision can be made.
10. AOB
None
11. The approved minutes of the 17th June 2014 meeting is in Appendix 1.
RECOMMENDATIONS The East Leicestershire and Rutland Clinical Commissioning Group Governing Body is requested to: RECEIVE the report.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
9
APPENDIX 1
EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP Minutes of the Strategy, Planning and Commissioning Committee Meeting held on Tuesday 15th July 2014 at 09.30am at ELR CCG HQ, Boardroom, Unit 2 – 3
Bridge Business Park, 674 Melton Road, Thurmaston, Leicester, LE4 8BL Present: Dr Andy Ker (Chair) Clinical Vice Chair designate Mrs Jane Chapman Chief Strategy and Planning Officer Mr Graham Martin CCG Chair Mr Warwick Kendrick Independent Lay Member Mr Dave Briggs Managing Director Mrs Karen English Chief Finance Officer Mr Tim Sacks Chief Operating Officer Mrs Carmel O’Brien Chief Nurse and Quality Officer Dr Richard Hurwood GP Locality Lead, Melton, Rutland and Harborough Dr Hilary Fox GP Locality Lead, Melton, Rutland and Harborough Dr Nick Glover GP, Blaby and Lutterworth Locality Lead Dr Graham Johnson GP, Blaby and Lutterworth Locality Lead Dr Tabitha Randell Secondary Care Clinician Mr Julian Mallinson Consultant in Public Health Dr Tim Daniel Consultant in Public Health Ms Emma Rogers Head of Communications Ms Yasmin Sidyot Head of Strategy and Planning Ms Claire Saul Head of Strategic Commissioning Mr Robin Wintle Interim Associate Director of Contracts and Provider
Performance In Attendance: Ms Samantha Woodhead Project and Programme Accountant Mrs Brandy Miller Project Support Officer Mrs Poonam Beeharry Corporate Affairs Officer (minutes)
ITEM DISCUSSION LEAD RESPONSIBLE
SP/14/92 Apologies for Absence: Dr Ker confirmed a change to the order of items on the agenda, noting that the Draft Five Year Strategic Plan 2014/15 to 2018/19 Update would be discussed before the QIPP Project Dashboard Report 2014/15 which will lead onto the QIPP challenge. No formal apologies were noted. Dr Ker formally welcomed back Dr Tim Daniels and introduced Dr Hilary Fox, GP Locality Lead, Melton, Rutland and

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
10
ITEM DISCUSSION LEAD RESPONSIBLE
Harborough.
SP/14/93 Declarations of Interest All GP members declared an interest in any items relating to primary care where a potential conflict may arise.
SP/14/94 Minutes of the Meeting Held on Tuesday 17 June 2014. The minutes of the meeting held on Tuesday 17 June 2014 (Paper A) were accepted as an accurate record for the meeting. Updates against actions from the minutes were provided as follows: Page 3 – Draft Five Year Strategic Plan – Ms Emma Rogers confirmed an update on the communications plan would be provided as part of agenda item SP/14/97. It was noted a number of Primary Care dashboard actions needed to be taken forward to the next meeting as the dashboard was not on the agenda this month. Page 8 – Better Care Funds plan: Following discussion of technology at the last meeting, Dr Ker advised he had spoken with the IT lead for Better Care Together and they had confirmed they were not looking at either telehealth or telecare. Mr Sacks added that he was in the process of working on an IM&T strategy for the organisation with GEM and this will be cross checked against the Better Care Together work. It was RESOLVED to:
APPROVE the minutes.
Mr Tim Sacks
SP/14/95 Matters Arising: Update on Actions from the Meeting held on Tuesday 20 May 2014. The action log (Paper B) was received and some actions noted as complete. Updates against outstanding actions were noted as follows:
SP/14/75: Project Dashboard Report 2013/14 and 2014/15 - Mrs Yasmin Sidyot confirmed this would be discussed during the meeting under agenda item SP/14/96.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
11
ITEM DISCUSSION LEAD RESPONSIBLE
SP/14/74 – Draft Framework for the community services strategy- It was noted this paper was circulated for virtual approval.
SP/14/73 – The draft Winter Plan and Master
Escalation Plan - Mrs Sidyot advised this had been deferred to the August meeting. Dr Briggs provided a brief verbal update advising members comments from the Governing Body had been fed into the meeting and the Chief Operating Officers had written the comments into the strategy confirming the Governing Body’s actions around this had been fulfilled.
SP/14/62 – Coordinated Community Health Services
Specification - Mrs Claire Saul advised this action was still on-going.
The following actions were noted as complete:
SP/14/70: Draft Primary Care Operational Dashboard SP//14/69:Two Year Operational Plan SP/14/49: Care Home Pharmacist Report
Dr Briggs suggested having a date column inserted in the action log this would enable more focus to be given the outstanding actions. It was RESOLVED to:
RECEIVE the action log.
Ms Brandy Miller/ Mrs Poonam Beeharry
SP/14/97 Draft Five Year Strategic Plan 2014/15 to 2018/19 Update Mrs Jane Chapman provided a verbal update on the 5 year Strategic Plan noting:
The initial direction of the plan has been submitted and Mr Geoff Rowbatham, Interim Programme Director for Better Care Together, attended the July Governing Body meeting to advise of the next steps.
Whilst the directional plan has been submitted there will be further on going work from July – September 2014, during which time there will be significant engagement.
The team are now focusing on resourcing delivery of the plan which includes the function of the Project Management Office (PMO), detailing the

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
12
ITEM DISCUSSION LEAD RESPONSIBLE
responsibilities of all the organisations involved and looking at information and accountability flows with the aim of producing a framework to deliver the high level plans.
Years 1 and 2 of the plan focus on CIP and QIPP with years 3 – 5 focusing on the transformational delivery of the plans.
Mrs Claire Saul provided further information from the BCT strategy & delivery workshop meeting attended on Thursday 10th July 2014 for strategy leads which looked at the resource, delivery and implementation of plans. Mrs Saul highlighted key areas of discussion as:
It was proposed (subject to governance cycles) the PMO should retain a lead role and within each workstream of the delivery framework there should be a ‘triumvirate’ encompassing a person from the Programme Management Office and a manger who supports delivery of driving the plans forward.
Discussion of the meeting focused on the skills those people needed to have and the interaction between the PMO and people on the ground.
Ms Emma Rogers, Head of Communications provided a verbal update on the communication plan. Ms Rogers highlighted key updates as:
The public announcement was made at the end of June. This did not have the negative impact that was anticipated.
There has been some interest from MP’s, broadly offering support but also challenging to get the community aspects of the plans right.
Critical letters from the public – these were currently being reviewed and responded to.
In terms of engagement, Ms Rogers highlighted key updates as:
The Communications and Engagement group will be meeting on 16 July 2014. The group has undertaken a mapping exercise to review existing activities which will be shared in tomorrow’s meeting. This is to ensure resource is used appropriately.
To maximise the use of resource there are plans to maximise the use of existing events as much as possible. The Better Care Together Communications lead will be pulling together a plan which will then be shared.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
13
ITEM DISCUSSION LEAD RESPONSIBLE
Healthwatch have been supportive and are looking to hold their own public events, which will be supported by the CCG but run by Healthwatch. Leicester and Leicestershire Healthwatch are still considering whether to have a joint or separate event.
Mr Martin suggested using the CCG’s Annual General Meeting (AGM) as part of the plans. Ms Rogers confirmed this had already been picked up. It was RESOLVED to:
RECEIVE the verbal update
SP/14/98 Better Care Funds Plan (BCF) Ms Yasmin Sidyot presented the report (Paper D) which provides an update on the Better Care Fund Plans 2014/15 -15/16 for Leicestershire and Rutland. Mrs Sidyot drew attention to key updates as follows:
BCF plans will need to resubmitted. A letter from the Department of Health and Local Government has been released which details they are expecting plans to be re-submitted by the end of summer, but no exact date has been given.
Guidance is clear that metrics and pay for performance
will be going ahead, however the details are still being finalised.
There has been a request to review the level of ambition
around reducing emergency admission metrics. A minimum reduction of at least 3.5% has been requested. Current plans are set around 2% and work is currently underway on what this change will mean and how this will tie in with the 5 year strategy and CCG operational plans, which was submitted in April.
The letter also talked about reducing emergency
admissions and not avoidable emergency admissions. It was thought this might be a typing error, however clarity has been sought.
Dr Nick Glover acknowledged clarity had been requested in terms of admissions and highlighted the importance of

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
14
ITEM DISCUSSION LEAD RESPONSIBLE
obtaining this, especially around percentage reductions for admissions. Specifically in relation to whether the percentage reduction is a true percentage reduction or whether it’s of a whole. Dr Glover also noted from a patient safety organisational perspective that it may be useful to reference the local position on the CCG’s use of emergency admissions as the professional body the governs doctors have made some strong comments about how close to a safe level of activity primary care are asked to get. Dr Richard Hurwood also highlighted a reduction in admissions of paediatrics was also a major category and commented that with all the work around the frail and elderly, paediatrics must not be lost. It was RESOLVED to:
RECEIVE the update report for information and comment
SP/14/96 QIPP Project Dashboard Report 2014/15
Mrs Yasmin Sidyot presented the report (papers C1,C2 and C3) which provides QIPP dashboard updates for against programmes of work. Mrs Sidyot noted:
Updates have been received on all programmes of work except the CHC programme. However it was noted this will form part of the discussion on QIPP challenges and work is underway to review the management of fast track referrals via a task and finish group.
The activity dashboard produced by GEM (paper C3) has been populated with April and May’s actual activity against planned that has been transacted into the acute contracts for the 5 QIPP programmes. This has only been done for UHL at this time as data for other providers is still currently being validated. However this will be available for the August report.
4 of the 5 QIPP programmes reported are on plan. These are, COPD, CVD, diabetes and urgent and emergency attendances.
The Emergency admission avoidance programme is over performing against planned activity. Further work is required to review elements critical to deliver the QIPP which includes the Integrated Crisis Response. The contract variation has reached the point of sign off in the hope this can start as soon as possible. Work is underway with Leicestershire Partnership Trust (LPT)

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
15
ITEM DISCUSSION LEAD RESPONSIBLE
looking at extending the current hours of the night nursing service and the current intermediate care service to enable delivery of the nursing crisis response element. Implementation of the coordinated health services model is underway, however a few issues have been raised in relation to the service specification. As a result contract queries have been raised with LPT in terms of activity as there was not enough information, a response has been received, however there are still further areas to clarify. Ms Pearson is trying to arrange a meeting to address this in order get this established and implemented.
Dr Graham Johnson raised concern in relation to the Emergency Admission Avoidance Non-elective admissions activity which showed over performance against planned activity. Mrs Sidyot advised the purpose of the paper was to inform discussion. Dr Nick Glover explained that most GP initiated admissions will go through ED as there are no longer any direct access beds It was clarified this activity had been taken out and therefore the graph could be interpreted as reflecting the admitting culture of ED. Dr Johnson queried what number from last year, the planned figures for the Emergency admission avoidance QIPP were based. Mrs Sidyot explained the plan from last year was drilled down to specifics HRGS with high admission, for this specific QIPP, admissions for patients aged 65 and over across a number of specialities were examined, this highlighted the areas with the number of highest admissions leading to where the biggest impact could be made. Those specific HRG codes were picked out and a subsequent plan put together around the activity. Dr Johnson queried what percentage reduction was applied to last year’s figures in the HRG’s as the reduction seemed unrealistic Mrs Sidyot explained, each HRG had a different reduction, but may have been 5% at the most, confirming it was not a large amount due to taking into account last year’s actuals and MRET.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
16
ITEM DISCUSSION LEAD RESPONSIBLE
Mr Warwick Kendrick queried whether it was feasible to work out what the financial impact would be if this QIPP continued to be red throughout the year. It was confirmed this data was already available. Dr Graham Johnson noted the post rag status for scheme number one on paper C2 should be red, not yellow. Dr Johnson also queried where the actual saving figure of £272k had come from given the activity levels. Ms Samantha Woodhead advised this figure was based on the plan explaining that as this was the first data to come through, there had not yet been an opportunity to confirm and challenge that figure. Mrs English clarified that the graph was only looking at one part of the scheme from scheme number one. Dr Ker requested the narrative from paper C2 correlated with the chart in paper C3. Mrs Sidyot confirmed this being worked on It was RESOLVED to:
RECEIVE the update and COMMENT on the project
Mrs Yasmin Sidyot
SP/14/99 QIPP challenge Dr Briggs opened the discussion by explaining urgent action is required to try and achieve the financial plans as currently the organisation was at risk of not achieving them. Key challenges were noted as:
QIPP plans were not delivering to the size and scale to close to close the financial gap
Continuing Healthcare (CHC) – the rate of growth is unsustainable with a much bigger overspend then anticipated
Urgent Care – Is central to the process as this effects all other areas.
Dr Nick Glover queried what the consequences would be if the organisation failed to close the deficit.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
17
ITEM DISCUSSION LEAD RESPONSIBLE
Dr Briggs advised the organisation would be tested, from finance and officer level to the leadership of the board. Dr Glover advised the system was not working explaining, to get a patient out of hospital (who perhaps should not have been there in the first place), CHC funding is put in place because of the pressing need for this patient to come out of hospital. This highlighted a financial spiral. Dr Glover suggested the focus should be on how we have a high conversion rate. Dr Briggs added that admission avoidance and the acute trusts also played a part. Readmission Rates: Dr Graham Johnson commented that data seemed to suggest that there is a high readmission rate. Suggesting that there are not positive or robust diagnoses being carried out by UHL, leading to questions about whether the quality of the discharge is as good as it could be. Dr Hilary Fox suggested utilising the SPA and Integrated Crisis response team as a downward step for acute trusts as well as an upward step for GPs. Therefore the discharge could be managed by the crisis response team who then refer for CHC if necessary after the period of reablement as opposed to whilst they are in hospital. Mrs Sidyot confirmed referrals from ED to ICRS were going up every month which suggested it was being utilised. However there could be some work in investigating changes once the night nurse element is introduced. Dr Johnson suggested it would be helpful to know the readmission rates from that service too. Dr Ker queried children admission rates. Dr Randell explained Ms Samantha Little, Children's and Maternity Commissioning manager, was looking at a piece of work regarding short stay admissions as there had been a large increase of children going through ED and staying for less than 24 hours, however Dr Randell had not heard back on that piece of work . Dr Randell highlighted Dr Hurwood’s emphasis on the need to reduce paediatric referrals as there are year on year increases. Dr Randell described a pilot in Nottingham where consultants were taking all of the calls and this resulted a 30% reduction in referrals which realised an immediate saving on the

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
18
ITEM DISCUSSION LEAD RESPONSIBLE
health economy, this also highlighted that Junior Doctors were admitting more than senior doctors. Dr Glover stated that if UHL were going to be asked to provide that type of service, Primary Care needed to ensure if was mirroring that and suggested through localities, the idea of peer review of prospective admissions could be refreshed. Dr Glover expanded noting there was big potential around this situation as junior doctors don’t have a health economy view. It also demonstrates to secondary care colleagues a commitment from Primary Care. Dr Johnson highlighted an example of where limited specialities at UHL had choose and book advise which had reduced referrals. Dr Glover added that in order to peer review to work, there needs to be suitable alternatives and as such, advice should be through choose and book. Mr Graham Martin queried whether the intention was to resolve the gap or find other schemes. Dr Richard Hurwood advised that if the plan was to reduce ED attendance, every GP and F2 needs to be aware of the new system and the best way to deliver that would be through Protected Learning Time (PLT). Dr Nick Glover queried if asking UHL to reduce their type 1 admissions (currently at 29%) to the national average (26%) would be a useful chunk of QIPP. Dr Briggs advised it would be, but challenged the group to think about the process to get there in asking them to carry out peer reviews. Dr Nick Glover highlighted the example of safety checklists used by airlines and suggested something similar was needed, such as an admission checklist. Dr Ker added that each tick on the checklist would need to be challenged by the clinician (peer) reviewing the admission. Mr Julian Mallinson drew attention to the GEM insight document which recommends peer review as a solution and the sense of being observed resulted in 25% reduction in referrals. Mr Sacks added that peer review had been happening in

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
19
ITEM DISCUSSION LEAD RESPONSIBLE
Primary Care for many years and suggested the peer review for secondary care should start at the admission stage. Dr Briggs noted a discharge checklist would be helpful too. Mrs Sidyot confirmed this was already in place however needed to be implemented. Dr Briggs highlighted a crucial element would be how the checklist was used. Dr Briggs summarised main actions points from the discussion so far as:
- Ensuring care plans are used across all sectors including EMAS, OOH, NHS 111 and out of county.
- The aim is for a reduction in number of admission or conversions from ED and to address that, there is scope to look at a peer review of each admission decision and using a checklist as part of the admission decision making process
- Children’s work – looking at some form of consultant input into the admission process, such as consultant triaging the phone calls not junior clinicians, and some form of consultant review of outpatient referrals.
- Choose and book advice needs to be more robust and detailed, and involve more specialities.
- Single point of access – to be used by clinicians in both admission avoidance and when discharging patients. E.g. Making sure ICRS is used, this would be a useful part of the admission checklist
Dr Briggs suggested it would be useful to have a similar process for Primary Care. Dr Fox noted that both ED and primary care were working under severe time pressures and suggested the use of SPA as it takes the decision away from them and moves the pressures to someone who knows what all the options are. Dr Briggs stated consultants and senior doctors need to be doing this work. Dr Glover highlighted PRISM does not contain any of the Choose and Book advice options. Mr Sacks explained a proposal about PRISM going to the Managing Directors meeting to ensure the system was kept up to date.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
20
ITEM DISCUSSION LEAD RESPONSIBLE
Dr Glover stressed the importance about the tone of peer reviews, and the emphasis needs to be on the process being supportive. Dr Briggs commented that admissions would be a useful place to start discussion with providers about how to make this work. Dr Johnson noted that as part of the peer review process, if a senior person was involved, they would also begin to learn about themes which would prove useful. Dr Ker queried how this would be address out of county. Dr Briggs suggested a sequenced approach and for Dr Ker and Dr Hurwood to begin having a conversation with the appropriate acute colleagues, such as Ben Teesdale and Ian Sturgess to talk through the detail of how it could work. Dr Hurwood highlighted the importance of discussions between GPs and consultants needing to have trust otherwise and be open to challenge. It was agreed Dr Glover would support Dr Ker and Dr Hurwood due to his experience in peer reviews. Dr Glover noted that there was also need to think about how the peer review message was going to be delivered to localities and feels it is best delivered through locality meetings. Dr Richard Hurwood felt it would be more appropriate delivered through PLT. Dr Ker suggested doing both. Dr Ker noted there was also a need to consider the Out of Hours doctors in terms of admission and how the peer review would work for them Dr Glover responded stating emphasis needs to be put on whether the patient has an advanced care plan. Dr Briggs described the next steps and the principals behind them as:
- Admissions can be negative for the patient, therefore an admission checklist/ peer review should take place before an admission happens, with either a primary care or secondary care colleague and PRISM.
- If in admission unit or ED, the same principles apply.
Dr Dave Briggs/ Dr Richard Hurwood/ Dr Andy Ker Dr Nick Glover

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
21
ITEM DISCUSSION LEAD RESPONSIBLE
- The same principles to be applied to discharge. It was agreed for Dr Johnson to work on the discharge work. Mr Martin queried why the ‘Choose Better’ campaign wasn’t being promoted more. Ms Rogers explained there would be substantial marketing of the service available in East Leicestershire and Rutland following the urgent care review. Dr Randell explained in relation to children’s health services, there was a booklet available that was being distributed by the health visitors on how to manage common childhood conditions. It was noted that this had West Leicestershire’s logo on despite being a three CCG initiative. Ms Sidyot agreed to follow that up. Ms Rogers confirmed she would investigate how the booklets were being distributed Care Plans: Dr Briggs noted the need to think about other groups of people who access patients such as EMAS and the challenge in making sure they are checking for a care plan. Dr Briggs suggested a similar process could be used and the care plan could feature on a checklist. IT solutions were discussed, and it was acknowledged a system was being developed for the long term, an interim solution (the checklist) was needed. Dr Briggs also suggested OOH phoning the Urgent Care Centre as a peer review and vice versa. Dr Johnson queried whether an acronym could be developed to help remember key points such as ‘CBA, Care plan Before Admission’ It was agreed Ms Rogers would look into this further. Falls Pathway: Ms Claire Saul provided some information about the falls pathway explaining. Key points to note are:
- There are a number of initiatives within the BCT
Dr Graham Johnson Ms Emma Rogers Ms Emma Rogers

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
22
ITEM DISCUSSION LEAD RESPONSIBLE
programme across all CCGs. There is an Urgent Care working group interested in falls which result in hospital admissions.
- In terms of the 5 year strategy, falls come under long term conditions which is under the frail older people workstream.
- A project brief is being put together to identify the activities and interventions that need to happen to reduce both admissions and to promote prevention. That particular piece of work will be going to the Urgent Care working group on Thursday to gain support for elements that need to be in place before winter, it takes an approach which integrates prevention and addressing falls across all providers.
Mr Mallinosn queried whether social care featured in the pathway, Ms Saul confirmed it did. CHC Mr Robin Wintle, Interim Associate Director of Contracts and Provider Performance, distributed a paper regarding the current position for CHC. Mr Wintle highlighted key issues as:
- Fast Track referrals are the root cause of the pressures and associated costs in CHC.
- Alternative pathways of care are not being considered adequately
- Leicestershire is an outlier against national statistics for fast tracks
Actions underway are: A task and finish group to look at the fast track process has been established and have put a number of actions in place to ensure that only appropriate fast track referrals are funded. These include:
- Peer review of the current processes - UHL and LPT have been asked to put additional checks
in place to ensure referrals are appropriate - Guidance will be provided to refers about packages of
care - The GEM CHC team will be provided with support to
confirm and challenge referrals coming through. Dr Nick Glover suggested a set of criteria be applied similar as happens in bariatric surgery. Dr Johnson queried whether fast tracks are challenged It was confirmed the decision was not challenged.

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
23
ITEM DISCUSSION LEAD RESPONSIBLE
Mr Wintle explained this is why the peer review is right, as there needs to be checking balance at next stage. There has been some discussion about a limit, such as 14 days, however this is not in line with national guidance. Dr Briggs stated there needs to be more focus and encouragement around rehabilitation and reablement and suggested a question which asked, as part of the fast track referral, whether there was any possibility of reablement or whether the patient would benefit from reablement, and if the answer is yes, they are not entitled to fast track and other alternatives would need to be offered. Dr Johnson suggested another question that could be asked is whether the patient is expected to die within three months and then ask for a reason why and also ask why they would not benefit from a reablement package. This then begins to build a more clinical picture and provides more information to provide other options. Dr Glover highlighted the importance as part of the peer review, to have realistic and constructive feedback. Mr Wintle added that there is a need for alternative pathways. Mr Graham Martin queried how long before we see results Mr Wintle explained following the implementation of peer reviews which start next week, the first thing expected to be seen is a reduction in the number if fast tracks. The next step is to identify patients already in the system to check whether they are still eligible. The intention by the end of the financial year is to see a minimum 10% reduction on current costs and maybe more. In addition, work is underway in trying to address the wider CHC cohort of patients and looking at reviews that have not been made, and looking at the frequency of review to ensure patients obtaining CHC are still eligible. Dr Glover queried whether there was information on the number of people awaiting fast tracks and where they were. Mrs Sidyot confirmed this was available and they were either in the hospital or community. Dr Glover queried whether this would impact on Delayed Transfers Of Care (DTOC). Dr Briggs confirmed it would not. Dr Fox commented that if the patients on fast track have a short

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
24
ITEM DISCUSSION LEAD RESPONSIBLE
prognosis, there should be other things in place such as DNR’s and advanced care plans so should be queried whether all these other things had been done prior to referral. It was agreed this could be added to a fast track confirm and challenge checklist Dr Briggs summarised the key points for the checklist as:
- Asking why they are they eligible - - Do they have an advanced care plan - A question that enables enough information to obtain a
proper accurate diagnosis - Asking for a rationale for why the patient is End of Life
(EoL), such as ‘what features makes this patient EoL’ Dr Johnson reiterated the importance of asking questions that required more than a yes/no answer. Mr Wintle highlighted that this was not just an acute issue as there were significant referral from community nurses too.. Dr Glover noted that by the end of the year, all care home patients should have a personalised care plan and within that, should evidence the clinical picture and determine whether the patient is CHC eligible. Dr Johnson queried who were completing the forms from nursing. Mrs Sidyot explained that previously, Band 5 and 6 nurses could directly refer, but now all referrals need to be checked by the Band 7 clinical case manager. Dr Johnson queried who would be supporting GEM with the confirm and challenge. Mr Wintle explained they were looking to bring in a third party, who does not have a conflict, to provide the peer review so GEM are not faced with the residual of having to criticise colleagues. Mrs English queried whether three was a budget limit on approvals. Mrs Sidyot confirmed it was £50k. Mrs Sidyot also advised that packages that have come through to the CCG have been challenged and as a result, care packages have been reduced. Mrs English asked if the threshold could be lowered. Mr Wintle agreed the threshold of cost approval could be

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
25
ITEM DISCUSSION LEAD RESPONSIBLE
lowered. Dr Briggs opened discussion to consider work around care homes and whether winter money could be used to bring services forward or pay someone else to do it, such as training, education etc. Mr Sacks advised it was not happening yet as the aim was on care planning, it will depend on the capacity of primary care. Dr Briggs explained that due to the pressures of primary care over the next two years, it may be worth considering buying in services for the next couple of years. Dr Hurwood commented that he didn’t think it would help as GPs offer support to care homes. Mr Sacks explained there is a piece of work around making sure the correct processes are in place regarding making sure contact is made with primary care before 999 and the local authority had funding for it another key element was shared training. Dr Briggs moved the discussion onto long term conditions and asked the group whether there was anything that could be done around heart failure. Mr Sacks confirmed this was in the GP support and Investment framework, Dr Briggs requested Mr Sacks meet with Mrs Sidyot and Ms Saul for potential opportunities and risks. Dr Glover stated that he felt primary care could not be reviewed this year, if so there is a risk, if the attention was diverted from care plans now, there would need to be a good reason for it. Dr Ker highlighted that UHL have withdrawn “Open access” to 24 hours ECG’s. i.e patients are having to see a consultant before a 24hr ECG is ordered. It was agreed Mrs Sidyot would follow this up. Dr Briggs highlighted an international example where patients who changed their setting of care, were reviewed by a community team regardless of whether it was specified. Due to the current risk around changes of care settings and the risk of admission, Dr Briggs asked the group to do some further work on this. – is this an action?
Mr Tim Sacks/ Ms Claire Saul/ Ms Yasmin Sidyot Ms Yasmin Sidyot

Paper M East Leicestershire and Rutland CCG Governing Body Meeting
9 September 2014
26
ITEM DISCUSSION LEAD RESPONSIBLE
Mrs English highlighted that as a result of the comparison done a number of areas were not captured in the QIPP schemes and therefore required further work, it was agreed Mrs English would liaise with Ms Saul and Mrs Sidyot to work through this. It was RESOLVED to:
DISCUSS the QIPP challenge .
SP/14/100
Update on the Current position with Paediatric Phlebotomy This item is to be received and commented on virtually
SP/14101 Procurement Report AQP (Phase 2) for cataracts Direct Referral and Helicobacter This item is to be received and commented on virtually
Any Other Business There were no items reported under Any Other Business
Date of next meeting The next meeting of the East Leicestershire and Rutland CCG Governing Body will be take place on Tuesday 19 August 2014 at ELR CCG, Unit 2 – 3 Bridge Business Park, 674 Melton Road, Thurmaston, Leicester, LE4 8BL