patient safety - northern lincolnshire and goole hospitals ... · patient had diarrhoea prior to...
TRANSCRIPT

NLG(16)047
DATE OF MEETING 26th
January 2016
REPORT FOR Trust Board of Directors – Public
REPORT FROM Infection Prevention & Control
CONTACT OFFICER Viv Duncanson / Maurice Madeo
SUBJECT C. difficile Action Plan
BACKGROUND DOCUMENT (IF ANY) N/A
REPORT PREVIOUSLY CONSIDERED BY & DATE(S) Infection Prevention & Control Committee , 18th
January 2016
EXECUTIVE COMMENT (INCLUDING KEY ISSUES OF NOTE OR, WHERE RELEVANT, CONCERN AND / OR NED CHALLENGE THAT THE BOARD NEED TO BE MADE AWARE OF)
N/A
HAVE THE STAFF SIDE BEEN CONSULTED ON THE PROPOSALS?
N/A
HAVE THE RELEVANT SERVICE USERS/CARERS BEEN CONSULTED ON THE PROPOSALS?
N/A
ARE THERE ANY FINANCIAL CONSEQUENCES ARISING FROM THE RECOMMENDATIONS?
N/A
IF YES, HAVE THESE BEEN AGREED WITH THE RELEVANT BUDGET HOLDER AND DIRECTOR OF FINANCE, AND HAVE ANY FUNDING ISSUES BEEN RESOLVED?
N/A
ARE THERE ANY LEGAL IMPLICATIONS ARISING FROM THIS PAPER THAT THE BOARD NEED TO BE MADE AWARE OF?
N/A
WHERE RELEVANT, HAS PROPER CONSIDERATION BEEN GIVEN TO THE NHS CONSTITUTION IN ANY DECISIONS OR ACTIONS PROPOSED?
N/A
WHERE RELEVANT, HAS PROPER CONSIDERATION BEEN GIVEN TO SUSTAINABILITY IMPLICATIONS (QUALITY & FINANCIAL) & CLIMATE CHANGE?
N/A
THE PROPOSAL OR ARRANGEMENTS OUTLINED IN THIS PAPER SUPPORT THE ACHIEVEMENT OF THE TRUST OBJECTIVE(S) AND COMPLIANCE WITH THE REGULATORY STANDARDS LISTED
N/A
ACTION REQUIRED BY THE BOARD For information
Page 2 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
TRUST Clostridium difficile RCA REVIEW ACTION PLAN 2015/16
Section 1 : Actions brought forward from Trust wide and Site specific C. difficile Action Plans 2014/ 2015 Section 2 : Actions brought forward from 2015/16 Site specific C. difficile Action Groups / CQUIN/ CEO
Challenge Section 3: Actions identified following DIPC RCA reviews
Author: Viv Duncanson

Page 3 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward C6 DPOW
Date of specimen 29/09/2013
Date of DIPC review 18/11/2013
HAI
Deemed : Not preventable
15.01.01 Previously 14.01.05
Develop a process for formal removal of pen allergy entries when established there is no true allergy.
Andy Karvot End of Jan 2014 Deadline end of
April 2014 New deadline end
April 2015 New deadline Dec
2015
Formal process in place April 2015: NICE CG183 gap analysis done and analysed by AK and Jeremy Daws (JD) Trust Drug Allergy Protocol to be written by AK, decision on availability of appropriate lab tests to be discussed by JD with Prof. Sewell and Ian Barlow, AK to check that Trust documentation meets recording standards for drug allergy and adverse drug reactions as per CG183 and JD & Katheryn Helley to look into will to commission a locally available drug allergy testing service. Policy will include removal of pen allergy label when appropriate. AK to provide update to IPCC by October meeting. Nov 15: Ongoing. Kate Woodrow taking over NICE CG183 which is the management of drug allergies. This will be included as part of this review and this action will be taken over by Medicine and therapeutics committee
Section 1 : Actions brought forward from Trust wide and Site specific C. difficile action plans 2014/ 2015
TRUST Clostridium difficile RCA REVIEW ACTION PLAN 2015/16: as at 01/04/15
Page 4 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
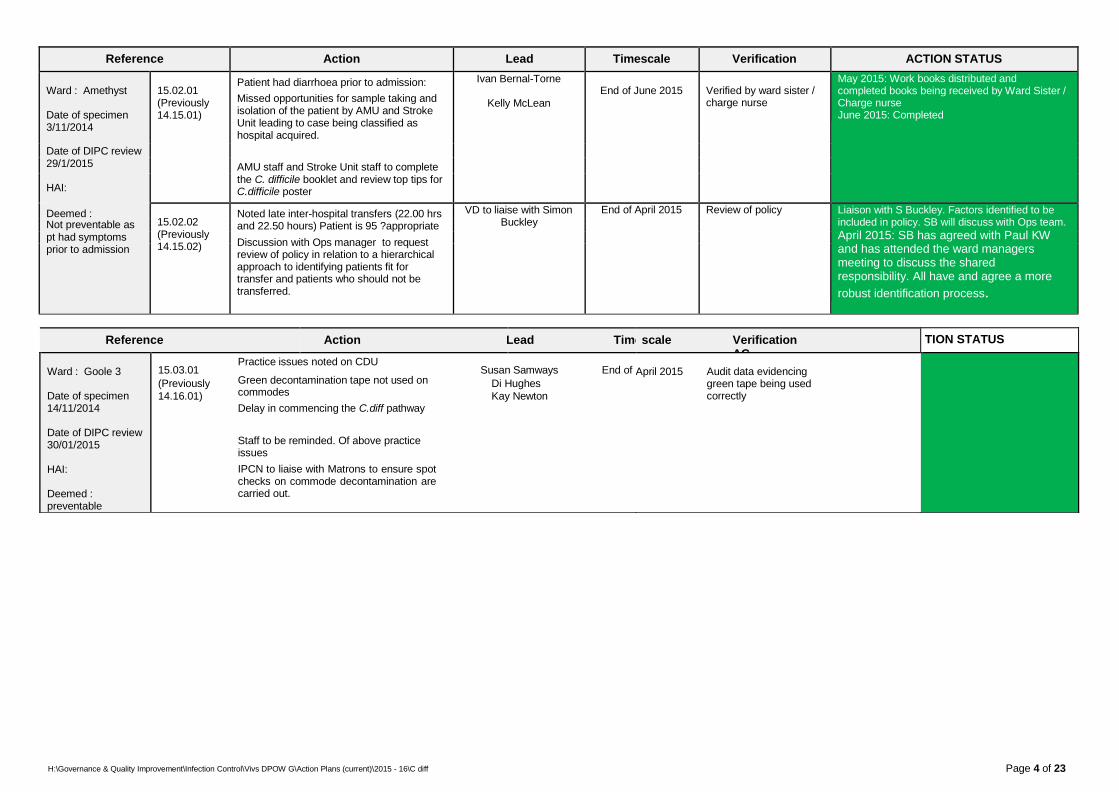
Ward : Amethyst
Date of specimen 3/11/2014
15.02.01 (Previously 14.15.01)
Patient had diarrhoea prior to admission:
Missed opportunities for sample taking and isolation of the patient by AMU and Stroke Unit leading to case being classified as hospital acquired.
Ivan Bernal-Torne
Kelly McLean
End of June 2015
Verified by ward sister / charge nurse
May 2015: Work books distributed and completed books being received by Ward Sister / Charge nurse June 2015: Completed
Date of DIPC review 29/1/2015 AMU staff and Stroke Unit staff to complete
HAI: the C. difficile booklet and review top tips for C.difficile poster
Deemed :
15.02.02 (Previously 14.15.02)
Noted late inter-hospital transfers (22.00 hrs and 22.50 hours) Patient is 95 ?appropriate
Discussion with Ops manager to request review of policy in relation to a hierarchical approach to identifying patients fit for transfer and patients who should not be transferred.
VD to liaise with Simon Buckley
End of April 2015 Review of policy Liaison with S Buckley. Factors identified to be included in policy. SB will discuss with Ops team.
April 2015: SB has agreed with Paul KW and has attended the ward managers meeting to discuss the shared responsibility. All have and agree a more
robust identification process.
Not preventable as pt had symptoms prior to admission
TION STATUS
Reference Action Lead Time scale Verification AC
Ward : Goole 3
Date of specimen 14/11/2014
Date of DIPC review 30/01/2015
HAI:
Deemed : preventable
Practice issues noted on CDU 15.03.01 Susan Samways End of
(Previously Green decontamination tape not used on Di Hughes
14.16.01) commodes Kay Newton Delay in commencing the C.diff pathway
Staff to be reminded. Of above practice issues
IPCN to liaise with Matrons to ensure spot checks on commode decontamination are carried out.
Completed April 2015 Audit data evidencing
green tape being used correctly
Page 5 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
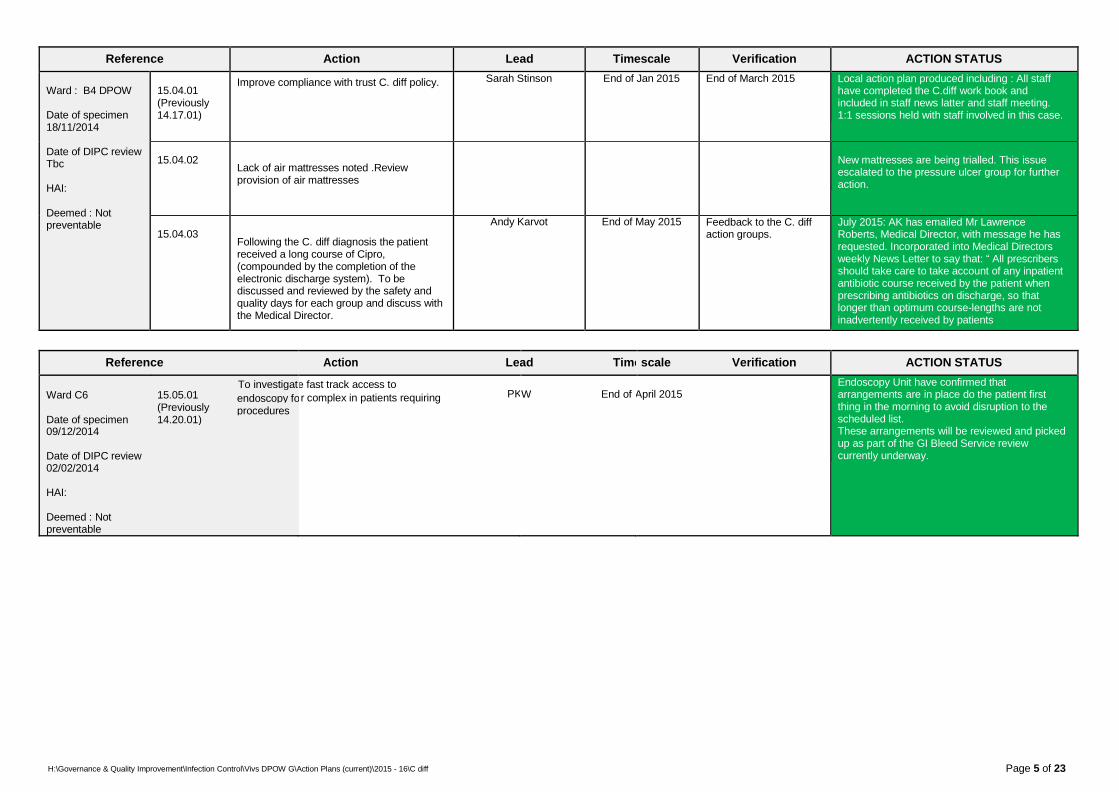
Ward : B4 DPOW
Date of specimen 18/11/2014
Date of DIPC review Tbc
HAI:
Deemed : Not preventable
15.04.01 (Previously 14.17.01)
Improve compliance with trust C. diff policy. Sarah Stinson End of Jan 2015 End of March 2015 Local action plan produced including : All staff have completed the C.diff work book and included in staff news latter and staff meeting. 1:1 sessions held with staff involved in this case.
15.04.02
Lack of air mattresses noted .Review provision of air mattresses
New mattresses are being trialled. This issue escalated to the pressure ulcer group for further action.
15.04.03
Following the C. diff diagnosis the patient received a long course of Cipro, (compounded by the completion of the electronic discharge system). To be discussed and reviewed by the safety and quality days for each group and discuss with the Medical Director.
Andy Karvot End of May 2015 Feedback to the C. diff action groups.
July 2015: AK has emailed Mr Lawrence Roberts, Medical Director, with message he has requested. Incorporated into Medical Directors weekly News Letter to say that: “ All prescribers should take care to take account of any inpatient antibiotic course received by the patient when prescribing antibiotics on discharge, so that longer than optimum course-lengths are not inadvertently received by patients
Reference Action Le ad Time scale Verification ACTION STATUS
To investigat Ward C6 15.05.01 endoscopy fo
(Previously procedures Date of specimen 14.20.01) 09/12/2014
Date of DIPC review 02/02/2014
HAI:
Deemed : Not preventable
e fast track access to
r complex in patients requiring PK
W End of
April 2015 Endoscopy Unit have confirmed that arrangements are in place do the patient first thing in the morning to avoid disruption to the scheduled list. These arrangements will be reviewed and picked up as part of the GI Bleed Service review currently underway.

Page 6 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward : 17 SGH
Date of specimen 11/02/2015
15.06.01 (Previously 14.25.01)
Mr Roberts to discuss cephalosporin prescribing with Primary Care, although this issue was not necessarily related to the C difficile case.
LR End of May 2015 Liaison with P. care
Medical Director now has access to the CCG medical newsletter where key messages will be
posted. Date of DIPC review 13/04/2015
HAI: 15.06.02
All staff on ward 17 have been made of the correct procedure to isolate patients directly when a faeces sample has been obtained and not to wait for the result.
Jo foster
End of April 2015
Signatures from staff once completed
Completed Deemed : Not preventable
15.06.03
All staff on ward have completed the ‘Infection Control’ workbook.
Jo Foster
End of April 2015
Verification by Ward Sister
Completed
15.06.04
Since the incident spot checks have been undertaken on the cleanliness of the commodes by the Chief Nurse, IPCN and Operational matron and no further problems identified.
Susan Samways End of March 2015 Audit data Completed

Page 7 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
NIL as at May 2015
CEO Challenge 24/11/2015
CEO 1
CEO 2
In view of rising number of cases a weekly CEO challenge meeting is taking place from August 2015
Convene a task and finish group to review antimicrobial issues as per the Hygiene Code requirements. Issues
Actions form first meeting :
Ensure antimicrobial steering group is fit for purpose . addressing all antimicrobial stewardship issues and keeping the Trust Board informed
Antimicrobial audits; specifically looking at clinical appropriateness for perceived indication, feedback to clinicians
Reporting of antimicrobial susceptibility data Address gaps in education
Continue with monthly meetings until issues resolved
CEO Weekly Action log October 2015: Meetings commenced in August Ongoing action log commenced to address issues as they arise 24/11/2015/. CEO meetings discontinued. Outstanding actions to be added to This action plan and IPCC.
KD / AK Feb 2016 First meeting of task and finish group held 27/11/2015. Meet monthly until issues resolved
CEO 3
Cleanliness reports to be added to IPCC agenda KD / Keith Fowler
Dec 2016 Standing agenda item added to IPCC
IPCC to become sub group of the Board for 6 months and review
KD Dec 2015 Commenced and ongoing first meeting held December
CEO 4
Section 2 : Actions brought forward from 2014/15 Site specific C. difficile Action Groups / CQUIN / Increased Incidence/ CEO Challenge

Page 8 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS Reference
CEO Challenge 24/11/2015
CEO 5
Determine a process with CSU / CCG’s for requests for removal of cases due to “NO LAPSE IN PRACTICE”
WB / VD Jan 2016 Meeting with CCG’s. Flow chart produced and agreed. Lapse in care reviewed by Quality committee
CEO 6
Upgrade C floor showers Jug Johal Feb 2016
CEO 7
Renew ward 24 flooring Jug Johal
Feb 2016 Completed
CEO 8
Consider the implementation of HPV decontamination
Maurice Madeo
March 2016

Page 9 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Tim escale Verification ACTION STATUS
15.07.01 Ward: 24 SGH Marion
Lessons learned: Highlight the issue to Date of specimen the ward Sister re 24-48 hours of no 05/04/2015 antibiotic given during the i/V oral
switch and review the reason why. Date of DIPC review Feedback to all ward 24 staff
03/07/2015
CAI : NLA G issues
Deemed: Awaiting CCG DIPC review
End of August 2015 Hewis and Andy Karvot
Completed. Liaison with the Ward sister who has fed back to ward 24 staff
Reference Action Lead Timescale Verification ACTION STATUS
Ward C6 DPOW 15.08.01 Discuss ?inappropriate transfer of patient
from C6 to a bay in B4
Andrea Webster- Cockrill/
End of July 2015
Review of appropriateness of
Discussed with Simon Buckley. Case reviewed and discussed with site managers
Date of specimen Simon Buckley patient transfer 04/04/2015
Date of DIPC review 15.08.02 Poor documentation of stool chart
Ward staff undergoing the C.difficile work book
Jo Jones / Sarah Stinson
End of August 2015 Completion of work book Completed
2/07/2015
HAI:
Deemed : 15.08.03 Discuss 1:1 with Consultant Dr Sarwar re
antibiotic prescription. Tazocin Px concurrently with Flucloxicillin and Amoxil
Andy Karvot
End of August 2015 Verification by AK that discussion held
AK has liaised with Dr Sarwar who has agreed to review the case.
Preventable
15.08.04 To include on the pilot ward round check lists a reassurance that there are not multiple live prescription sheets.
Lawrence Roberts
Immediate
Inclusion on Px sheet Requested to be included on the ward round check lists
Section 3: Actions identified from RCA reviews

Page 10 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: 28 SGH
Date of specimen 18/04/2015
Date of DIPC review 28/05/2015
HAI:
Deemed : Possibly preventable
15.09.01 Consultant Antimicrobial Pharmacist will discuss this case on a 1:1 basis with the relevant pharmacists / technicians regarding the history of the antimicrobial prescriptions and the review that was undertaken of this case.
Andy Karvot 1:1 Discussion end of August 2015
AK has spoken with ward pharmacist who had reviewed prescription, who had thought that antibiotic chosen was appropriate, despite long course. Discussed intervention with prescribers if repeat courses and longer than usual. Training complete.
15.09.02 Andy Karvot to formulate a programme to work / provide supervision to ward pharmacists regarding antimicrobial review
Andy Karvot Commence immediately
complete by end of March 2016
Programme drawn up: AK to perform 1:1 training with at least 1 pharmacist per site per month October 2015. Training ongoing; scheduled to complete by March 2016.
15.09.03 Andy Karvot is currently working on the new prescription sheet that will include antimicrobial stop dates
Andy Karvot End of August 2015 New date Dec 2015
Final format agreed / ratified by Medicines and Therapeutics Committee. October 2015: Printing tender proof revealed some required modifications. Will be printed in- house by NLAG Reprographics. AK to agree final changes with Philip Johnstone. November 2015. Completed
15.09.04 Relevant ward staff to undergo C.diff training / undertake the C.diff booklet
Michelle Long End of Aug 2015 Completed
15.09.05 Broken soap dispensers to be replaced on ward 28
Susan Samways End of Aug 2015 New date Nov 2015
Requested dispensers from Ecolab. Sept 2015: No dispensers available from Ecolab. Have been put on order as urgent. October Dispensers received
15.09.06 Lawrence Roberts to discuss with Dr Ahmed the requirements of this case with regards Duty of Candour.
Lawrence Roberts End of Aug 2015 Completed
15.09.07 Death certificate:. Mr Roberts identified that more work is required on raising awareness of completion of death certificates correctly
Lawrence Roberts 1:1 discussion with Dr Hanna end of
Aug 2015
Mr Roberts has sent out a Medical Directors bulletin with instructions on filling out death certificates . In addition the subject has been put on the HCC agenda for discussion ref centralising deathe certificates.
15.09.08 As C.diff was reported as 1c on the death certificate – Viv Duncanson will discuss with Wendy Booth to ascertain if this case should be escalated as an SUI
Viv Duncanson Immediate Liaised with colleagues currently who are working out the process
Escalation flo chart produced in conjunction with Wendy Booth

Page 11 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: Stroke Unit 15.10.01 Request that the Stroke Group review the
Jon Wood
End of October 2015
Feedback from Stroke
Tabled at Stroke Group case with regards the interval between
DPOW admission and definitive diagnosis to Group via Jon Wood
determine whether there was undue delay Date of specimen in obtaining an MRI based diagnosis 31/05/2015
All other actions have been completed:
Date of DIPC review 15.10.02
Actions have been taken regarding the mis- labelling if the specimen to prevent reoccurrence. Requires reporting on to the datix database
Jane Stocks
Completed 27/08/15
HAI
Deemed: Not
15.10.03 Education re isolation and stool specimen taking has been completed with all members of staff
Andrea Webster-Cockrill Completed
preventable

Page 12 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: C1K DPOW 15.11.01 Infection Control to be added on to the Ops
Jon Wood
End of Sept 2015
Completed communication template
Date of specimen 15.11.02
Ensure newly appointed Deputy Site Managers to have time scheduled with an IPCN
Simon Buckley/ Ali Wickham
End of November 2015
X1 Deputy site manager has had 1:1 with IPCN 18/06/2015
Date of DIPC review 27/08/15
HAI 15.11.03
Death certification: Medical director to follow up the case with the specific doctor
Lawrence Roberts
End of sept 2015
Completed. MD’s bulleting sent out instructing on correct way of completing death certificates
Deemed: Not preventable
15.11.04 Cleaning of mattresses: there are still some areas where local cleaning of mattresses is taking place. Business case to be reviewed and to raise issue at CEO meeting
Tara Filby End of Sept 2015 Raised at CEO meetings.
Tara Filby has ensured that mattresses are not cleaned at ward level and the facility for sending mattress to an external facility is available
15.11.05
Lab report sensitivity. PC to check that amoxicillin release is always released when Co-amox is released
Peter Cowling
End of Sept 2015
Review by PC revealed that there is no function within the rules that detects whether or not an antibiotic has been released or suppressed.

Page 13 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
15.12.1 AK to be asked to lead a revisit of the Ward: DPOW B6
Date of specimen 15/06/2015
Date of DIPC review 16/6/2015
HAI
Deemed: Not preventable
orthopaedic prophylaxis issue/ antimicrobial policy involving the Orthopaedic consultants, Consultant Microbiologist, and Acute Kidney injury Consultant. LR / AK
End of Nov 2015 Review of policy October 2015: Raised at CEO’s weekly Clostridium difficile Challenge Group by AK. Dr. Cowling felt that issue too complex to make a decision at that group. Mr. Roberts will retain on “to do” list and will raise when Royal Orthopaedic Society guidance is updated. Nov 2015: Ongoing Further discussion at Pathlinks antimicrobials group meeting 17/11/2015 Meetings scheduled to meet with Ortho Clinical Lead to agree way forward Dec 2015: Meeting cancelled to be rescheduled
15.12.2 Penicillin allergy remains an issue. Noted that it appears on the Trust action plan as an ongoing issue. Medical Director aware
AK See 15.01.01 Review / Update to protocol
October 2015: AK to provide update to Infection Prevention and Control Committee in Nov 2015.
Changes to policy ratified.
15.12.3 Review actions for GDH positive patients Lawrence Roberts/
IPCT
End of September
2015
Review / Update to protocol
October 2015: Flo w chart and actions drafted by IPCT To be ratified at Oct IPCC.
Ratified by Oct IPCC
15.12.4 Review/ assess whether cefuroxime should
be the second line choice for gynae / obs patients
AK/ Microbiologists End of September 2015
New date: end November 2015
Review / Update to protocol
November 2015: To be considered at Path Links Antimicrobials Guidance Committee meeting. Has been agreed that cefuroxime is correct as second line choice for gynae / obs patients

Page 14 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: SGH 24 15.13.01
Continue to monitor commode cleanliness by completing spot checks
Quality matrons and IPCN’s
Immediate and on- going
Implemented and ongoing
Date of specimen 19/06/2015
Date of DIPC review 15.13.02
Improved decision making re antibiotic choice (Tazocin) and improved documentation in support of choices made.
AK and PC
Dec 2015 Decision making on when to use piperacillin /
tazobactam incorporated into the Trust’s Antibiotic Formulary and Prescribing Advice for Adult Patients. Improved documentation in support of choices made. New adult treatment sheet with dedicated antibiotics prescribing sections, released 16/11/2015
6/8/15
HAI
Deemed: Possibly preventable
TION STATUS
Ward: 3 DGH
Date of specimen 07/05/2015
Date of DIPC review 03/07/2015
HAI
Deemed: Not preventable
Reference
15.14.01
Action Lead Timescale
Ward staff to be reminded that in addition to ward urinalysis, specimens of urine should be taken and sent to the Lab when urine is cloudy / signs of infection
MH and Ward Sister ward 17 at SGH
Immediate
Verification
Confirmation of communication
ACTION STATUS
Completed
Reference Action Lead Timescale Verification AC
Ward: B4 DPOW
Date of specimen 14/07/2015
Date of DIPC review 20/07/2015
HAI
Deemed: Not preventable
15.15.01 Nil actions identified N/
To be sent for consideration of taking of total cases as no lapse in practice
A N/A N/A
Completed

Page 15 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference
Action
Lead
Timescale
Verification
ACTION STATUS
Ward: B4 DPOW 15.16. 01 Full generic MDT required to review the Dr Khan / Kev Taylor End of sept 2015
Best interest meeting held by Dr Naqvi’s team ongoing plan and care for this patient – Dr (C6) Khan / Kev Taylor 4/11/2014
Date of specimen
20/07/2015 15.16.02
Review of patients penicillin allergy status
AK
End of Dec 2015 Completed. Decided patient was not pen allergic
Date of DIPC review
21/09/215 15.16.03
Relook at bed management process with regards to why the patient was out – lied.
PKW
End of Nov 2015 Policy checked: considered robust. Recirculated
to all ward managers
HAI
Deemed: possibly
15.16.04
Review / Feedback documentation issues to medical and nursing staff –
PKW / LR
End of Dec 2015
Completed via medical directors newsletter
preventable
15.16.05
MRSA screening. New policy on a page has been implemented and staff made aware.
JJ
Immediate
Completed
15.16.06
Recognised that there are a number of new staff : IPCN to work on the ward alongside staff to support and train in IPC techniques and policies (specifically MRSA, isolation and C. difficile)
AWC
Commence 1/10 and ongoing for 3
months Review Jan 2016
Completed
15.16.07
Revisit hand over process / process for escalation out of hours (Medical and nursing)
LR & PKW
End of Nov 2015
Completed Conversation has been held with the Groups > Rota has been updated
15.16.08
For patients who are difficult to cannulate, ensure staff are aware of the vascular nurse role Nick Harrison / Maggie Parker
PKW
End of sept 2015
Completed. Included in staff magazine. Extra sessions delivered by IPCN
15.06.09
Ensure staff aware of correct procedure for sending specimen for catheterised patient : Kev Taylor
Kev Taylor
End of Oct 2015
Kirsty Dent Ward Manager has conveyed the message to all C6 staff on an informal basis and will discuss at the ward training day that has been arranged for October
Page 16 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
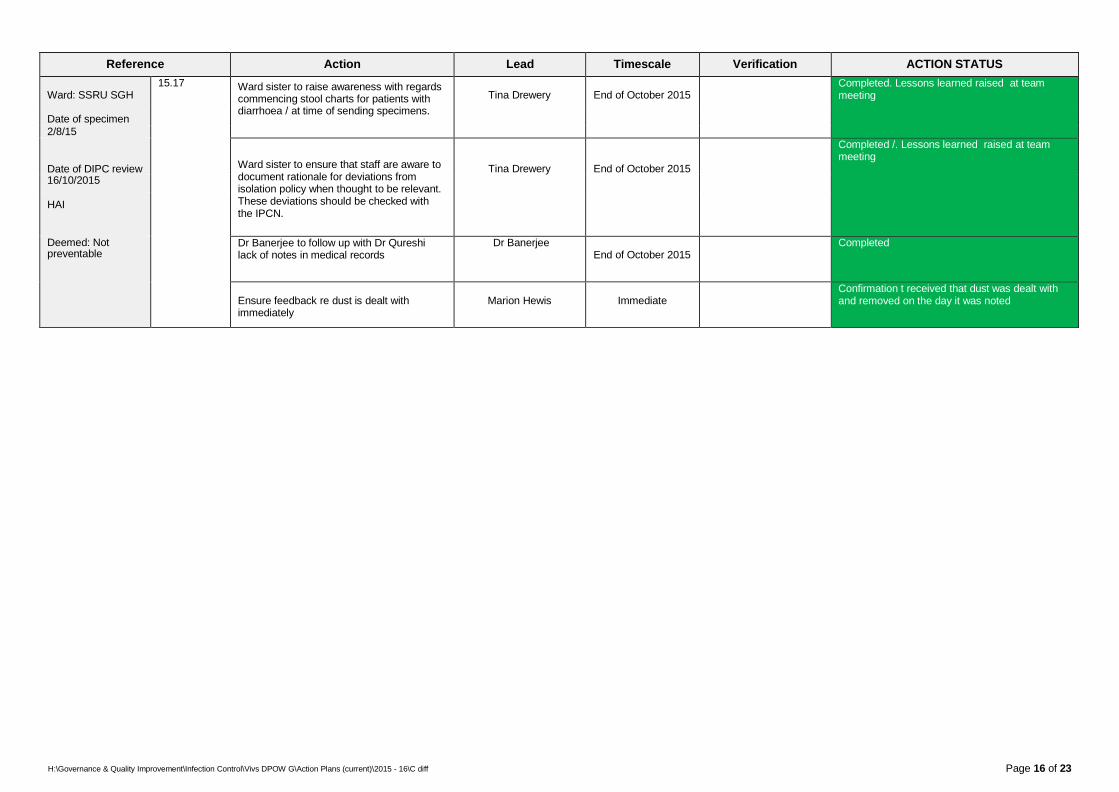
Ward: SSRU SGH 15.17 Ward sister to raise awareness with regards
commencing stool charts for patients with
Tina Drewery
End of October 2015 Completed. Lessons learned raised at team
meeting
Date of specimen diarrhoea / at time of sending specimens.
2/8/15
Date of DIPC review
Ward sister to ensure that staff are aware to document rationale for deviations from isolation policy when thought to be relevant. These deviations should be checked with the IPCN.
Tina Drewery
End of October 2015
Completed /. Lessons learned raised at team meeting
16/10/2015
HAI
Deemed: Not Dr Banerjee to follow up with Dr Qureshi lack of notes in medical records
Dr Banerjee
End of October 2015 Completed
preventable
Ensure feedback re dust is dealt with immediately
Marion Hewis
Immediate Confirmation t received that dust was dealt with
and removed on the day it was noted

Page 17 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: 24 SGH 15.18.01 Feedback given via News flash incident
process (ward communication)
Ward sister Sharon Roberts
End of Oct 2015 Documents used for news flash
Completed
Date of specimen
2/8/15 15.18.02
Ward hand over used to highlight the incident / lessons learned
Ward Sister Sharon Roberts
End of Oct 2015 Ward documents Completed
Date of DIPC review 10/11/2015
HAI 15.18.03 PC and TD to review the sample journey –
to identify where it went wrong?
Peter Cowling
End of Dec 2015
Report from PC Mark Cioni Lab manager has reviewed this . Issues identified at the lab end with regards processing the specimen have been corrected
Deemed: not 15.18.04 Communicate to teams that bed spaces / bays must undergo a terminal clean cleaned when potentially and infected patients are moved / transferred
Pete Bowker Tony Dawson
End of Nov 2015
Evidence of communication
Completed preventable
15.18.05
Review terminal cleaning process for the 3x cases on ward 24
Jayne Girdham
Immediate
Facilities records Unable to obtain full assurance that areas had been cleaned to due lack of records. Facilities now keep robust records that are sited on the intranet.
15.18.06
Escalate state of fabric of ward 24 to weekly CEO challenge meeting
Karen Dunderdale Jug Johal
Immediate Improvement in flooring KD has escalated concerns to Director of
Facilities. Ward 24 has been moved to the top of the work schedule.
15.18.07
VD to escalate to NMAF the issue of implementing isolation correctly e.g. cleaning and mop and bucket being available for isolation side rooms.
Viv Duncanson
Dec NMAF NMAF minutes Escalated to Tara Filby for December NMAF
meeting

Page 18 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: 6 Goole (28 SGH)
15.19.01 Consider review of trust antimicrobial policy to reflect age and previous antimicrobial history before giving high risk antimicrobials
PC and AK
End of Jan 2015 Updated policy Warnings on the policy have been clarified.
Document also covers ULH and so could not be amended as full agreement not reached
Date of specimen 4/8/15
Date of DIPC review 15.19.02 Ensure the orthopaedic case is subject to a DIPC review
VD
End of Nov 2015 Notes from meeting Review meeting held 17/11/2015 with Mr Bayne.
A DIPC review meeting is being held to review 4 / 5 SSI orthopaedic cases in December. It was agreed that ward 6 / ward 28 followed the antimicrobial policy (but did not take in to account the prolonged prescription of Cipro by the GP and the pervious orthopaedic admission (for a SS Joint infection) . Dr Cowling has asked that the current policy takes in to account the patients age
12/11/2015
HAI
Deemed: Not
preventable
Reference Action Lead Timescale Verification ACTION STATUS
Ward: 22 SGH 15.20.01 Failure to isolate / Failure to identify
appropriate outlier. Debrief ward staff using
Tony Dawson
End of Nov 2015 Staff meeting Completed
Date of specimen 21/09/2015
a lessons learned approach – action Tony Dawson
Date of DIPC review
15.20.02 Follow up transfer process to ensure that the vacated side room was cleaned when the patient was transferred out
Viv Duncanson
End of Nov 2016 Verification by checking Facilities terminal cleaning records
Facilities could not verify this, but now keep robust records for terminal cleans, which are available on the intranet.
30/10/2015
HAI
Deemed: Not
15.20.03
Request that Ops centre record where complex decisions are required in order that review / lessons learned / support can be given.
Graham Jaques / Simon Buckley
End of Nov 2015 All Ops staff reminded to document rationales
preventable
15.20.04 Mr Roberts to follow up absence of Clinician at DIPC review.
Mr Roberts
Immediate Completed

Page 19 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: 16 SGH 15.21.01 Reminder to ensure that microbiology
results are reviewed in a timely manner as
MR L Roberts
End of Dec 2015
Newsletter Completed via MD’s newsletter
Date of specimen 27/08/2015
per antimicrobial policy to be included in MD’s newsletter
Date of DIPC review 6/11/2015
15.21.02
IPCT to review use of a C. diff predictor / risk score is being used in any other trusts
Dr Cleeve and IPCT
End of Jan 2016 Search for predicator tools carried out and
reviewed. There are no tools in existence that can be transferred directly for use by NLAG. Suggest campaign on raising awareness re C.diff and infection risk factors. To be discussed at next FULL IPCT meeting
HAI
Deemed: possibly preventable

H:\Governance & Quality Imp
Page 20 of 23
Reference Action Lead Timescale Verification ACTION STATUS
Ward: C5 DPOW
Date of specimen 20/9/2015
Date of DIPC review 11/11/2015
HAI
Deemed:
15.22.01
Delay in isolation (7 days) Matron to try to identify members of staff who were involved in the case ‘interview’ them / consider a file note being recorded
Kevin Taylor
End of October 2015
Confirmation action completed from Matron
Difficulties in identifying individual staff members and so all staff included in the actions. One agency nurse involved in the case will not be employed by the Trust in the future
15.22.02
Poor documentation with nursing records regarding stools and classification: Stool chart commenced for every patient on ward C5, all staff to sign document on entry.
Kevin Taylor
Immediate
Confirmation form Matron
Implemented
15.22.03
Trust document needs updating to accommodate signature.
VD to liaise with Hazel Moore
End of October 2015
Document ratified at NMAF
Completed and ratified 6/11/2015
15.22.03 Education of staff by IPCN regarding recognising Bristol stool chart classification. and when to isolate. Ensure staff have pocket sized aid memoirs for stool specimen collection Ensure posters depicting Bristol stool chart are available Provide extra education
Kevin Taylor and Ward Sister
Jo Jones
End of January 2016
Immediate
Education commenced Credit card sized aid memoirs distributed to all staff Education completed
15.22.04 Investigate reasons and subsequent actions as to why the lab did not ring the ward with the result- PC/ Mark Cioni
Peter Cowling Mark Cioni
End of Nov 2015 Investigation conducted by Marc Cioni. . Phone log not completed by lab staff although member of staff said that they did ring the ward. The need to complete the phone log has been stressed at the lab meeting using this case as an example. Highlighting exactly what impact not phoning the result may have.
15.22.05
Investigate reason for Consultant Microbiologist not being available via telephone when Dr Menon called
Peter Cowling End of Nov 2015 This was period where there was sickness re Consultant Microbiologists leading to a temporary shortage of Consultants. Consultant busy on other calls. Now resolved
15.22.06
Review induction information given to agency staff by the Trust.
Wendy Booth
End of Nov 2015 IPCT have developed top tips for “transient “
staff. Sent to Wendy Booth
15.22.07
Review feasibility of staff ringing the lab to inform them when a C.diff test is require – IPCT
Peter Cowling / IPC
T
End of Dec 2015 This has been considered and has been deemed not possible due to the lab deciding whether or not to perform a C.diff test using a strict protocol, which takes in to account consistency, location , age. clinical details and previous specimen history. As long as the lab is provided with all relevant information a C.diff test will be performed.
15.22.08
rovement\Infection Con
Review the terms ‘frailty and old age’ (as recorded on the death certificate) to see if they are acceptable causes of death. - LR
trol\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Lawrence Roberts
End of Dec 2015 Med Director feedback: ‘Frailty’ can be used in
a death certificate and may be the only reason for death given if the patients is over 80 with certain restrictions. Med Director will communicate this to medical staff.

Page 21 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: AMU short stay
15.23.01
Review the catheter journey with regards catheter remaining in situ or removal– L
Linda Barker
End of Jan 2016 Catheter journey reviewed. Well documented in
the patients records the need for the catheter to remain in situ and further reviews.
Date of specimen Barker
17/11/2015
Date of DIPC review
15.23.02
Escalate the case for review to the End Of Life Mortality Review group
LR to Jeremy Dawes
End of Dec 2015 Completed
16/12/2015
HAI 15.23.03 Review process of paper referrals of
inpatients to Endoscopy
Simon Buckley End of Jan 2016
Deemed: Possibly preventable
15.23.05 Prescribers of the Cefalexin and Cefuroxime need to be identified and followed up.
Andy Karvot / Tony Vicca
End of January 2016
TION STATUS
Reference Action Lead Timescale Verification AC
Ward: 24 SGH
Date of specimen 24/11/2015
Date of DIPC review 6/1/2016
HAI
Deemed: possibly preventable
15.24.01 To identify rationale for Ceftriaxone as not
clear according to medical records although Dr Cow
appears to have been approved by covering microbiologist.
ling 14/01
/2016 ICC Discussed with Jnr Dr the rationale for agent and antimicrobial pharmacist. Clarification established. Prescribed as advised by on call Microbiologist (Boston) – considered as a lapse in care case

Page 22 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: Amethyst
Date of specimen 28/11/2015
Date of DIPC review
HAI
Deemed:
15.25.01
15.25.02
Reference Action Lead Timescale Verification ACTION STATUS
Ward: Amethyst
Date of specimen 23/12/2015
Date of DIPC review
HAI
Deemed:
15.26.01
15.26.02

Page 23 of 23 H:\Governance & Quality Improvement\Infection Control\Vivs DPOW G\Action Plans (current)\2015 - 16\C diff
Reference Action Lead Timescale Verification ACTION STATUS
Ward: Amethyst
Date of specimen 04/01/2016
Date of DIPC review
HAI
Deemed:
15.27.01
15.27.02
Reference Action Lead Timescale Verification ACTION STATUS
Ward: 24 SGH
Date of specimen 06/01/2016
Date of DIPC review
HAI
Deemed:
15.28.01
15.28.02