patients with special needs wichita dental hygienists’ association january 10, 2008 barbara m....
TRANSCRIPT

Patients with Special Needs
Wichita Dental Hygienists’ AssociationJanuary 10, 2008
Barbara M. Gonzalez, RDH, MHS

Disabilities
Disability = one or more life skills is altered by physical or mental impairment
ADA = Americans with Disabilities ActPassed in 1990
Employment
Environment

Not your dentist’s ADA
The Americans with Disabilities Actenacted in 1990
Covers employment, public services, public accommodations, etc.
http://www.usdoj.gov/crt/ada/statute.html

What is a “Disability”?
Social PerceptionsThe Obvious
Wheelchair…
Spinal cord injury
Cerebral Palsy
Muscular Dystrophy– ALS (Lou Gehrig’s)

“You don’t look disabled…”
Social Perceptions?The Not-so-Obvious
Sensory Deficits– e.g. hearing impaired
Seizure disorders
Chronic managed – e.g. multiple sclerosis, lupus
Infectious diseases – e.g. HIV

The Dental Hygienists’ Role
Make good use of anecdotal notes
Meet basic patient needs, i.e.Modified oral hygiene techniques & aids
General Practice
Learn special techniques or skills, i.e.Sign language
Wheelchair transfersSpecialized Practice

PHYSICAL IMPAIRMENTS

Visual Impairment
Half of legally blind Americans are 60+
Legal Blindness Visual acuity of 20/200 or less with optimal correction
10% of legally blind Americans are school age children or younger
Etiology
TraumaIncidence is markedly decreased due to better workplace safety controls
Diseasei.e. macular degeneration, etc.
Structural / development defectsCataracts, etc.

Major Problems Encountered
Unsolicited and inappropriate assistance by strangers
Mistaking blindness for DEAFNESS
Addressing companions and not person
Verbalizing pity
Visually impaired usually independent and productive sans other disabilities

Barriers to Care
Accessing “yellow pages” to find dentist
Transportation
Release time from work
Negative attitudes about service dogs in office setting
Financial
Physical environment
Physical Environment
Loose rugs
Poor lightingLegal blindness vs. total blindness
Steps
Small print / written forms
Unwieldy doors
Sudden changes in surface texture
Assisting Your Patient
Verbal questioning to gain information
Schedule additional time
ASK for patient’s preferences
Oral Manifestations
Same as general peer population
Oral hygiene may be compromised
Poor OH may contribute to oral disease
Patient Management
Greet patient upon arrival
Describe office layout
Escort patient while describing changes, obstacles
Offer physical assistanceDo NOT take by hand!
Allow service dogs in operatory
Patient Management
Introduce patient to other staff members
Designate one as primary communicator
Minimize noise!
Identify sounds, smells, equipmentAllow them to touch
Inform patient upon approach to mouth

Patient Management
Inform the patient upon leaving and returning to operatory
OHI – use hand-over-hand technique
OHI – good verbal descriptions
OHI – use typodonts

Hearing Impairments
Can exist with no other disability
Often accompanies other disabilitiesCleft palate – 90%
Cerebral palsy – 20%
Down’s Syndrome – 70%

Oral Manifestations
Bruxism
Others as general population

Barriers to Care
Difficulty contacting officeTDD
Telecommunications device for the deaf

Patient Management
Allow interpreter into operatoryBUT, speak to the Patient!
Do not shout, unless directed to by patient
Maintain voice volume
Learn simple ASL / SEE signs
Patient Management
Write out information in advance of appointment
For children, use drawings or pictures
Use touch to communicate
Hearing aids often turned off
OHI – use disclosing, visual cues
Neuromuscular Disorders
Cerebral Palsy…
Muscular dystrophy
ALS
Neurological Disorders
Multiple Sclerosis

Cerebral Palsy
A static, non-progressive neuromuscular condition resulting from damage to brain, often peri-partum
Motor dysfunction, weakness, un-coordination, paralysis
May be accompanied by other diagnoses

Classifications of CP
Spastic – 50-75%S. diplegia, s. hemiplegia, s. quadriplegia
Athetoid dyskinetic – 15 – 25%
Ataxic – 10%
Hypotonic (Flaccid)- <10%
Mixed – 5-10%

Limb Involvement Classifications
Monoplegic
Hemiplegic
Paraplegic
Diplegic
Quadriplegic
Triplegic

Oral Manifestations
BruxismMalocclusionClenchingFood retention / pouching
CariesPlaque control
PeriodontitisGingivitis
Patient Management
Schedule initial interview to acquaint with patient
Assess muscle / reflex patterns
Communication and comprehension
Medical conditions
Caregiver should participate

Patient Management
Speak to adult patient as an adult
Speak to a child patient as a child
Gear information to patient’s level of intelligence, not communication
Managing Reflex Patterns
Tonic labyrinthine reflexOccurs when head tilts backward
Asymmetric tonic neck reflexOccurs when head turns to side or away from midline
Gag reflex
Cough reflex
Bite reflex
Swallow reflex
Gag and Cough Reflex
If HypoactiveAt risk for aspiration
Use small bursts of water
Use frequent suction
If HyperactiveFlex patient’s head with chin to chest
Introducing items intraorally will probably induce reflex

Bite Reflex
Mouth prop may be helpful
Tie off!
Treat lingual as quickly as possible

Mouth Gag (molt)
Adjustable

Swallow Reflex
Swallow ReflexAvoid mouth props
Be patient!
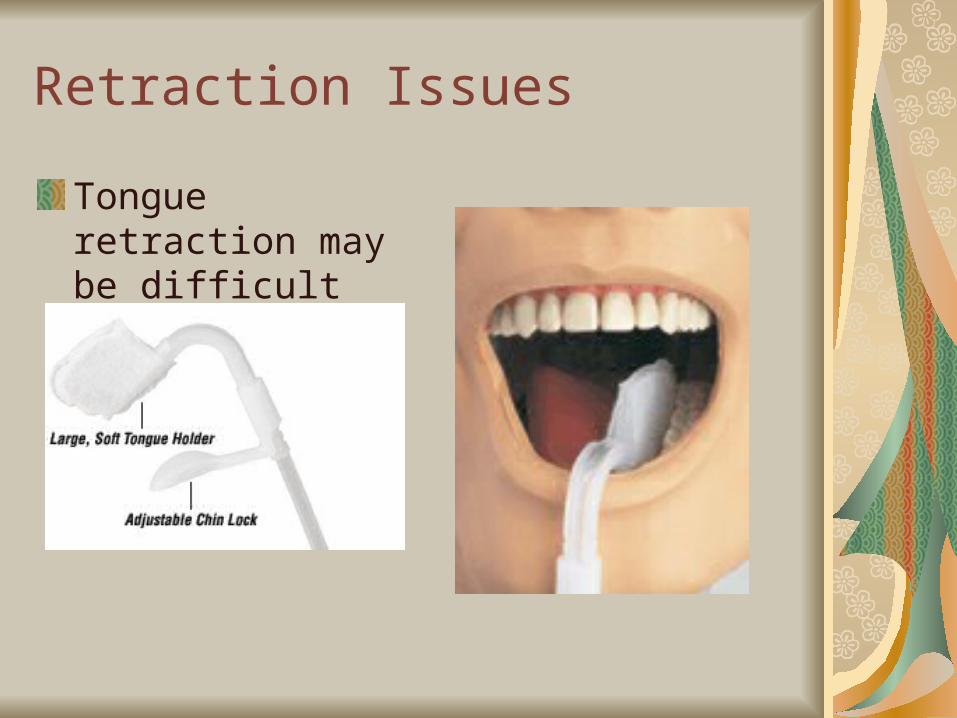
Retraction Issues
Tongue retraction may be difficult

Patient Management
Allow adequate time
Be aware that un-coordination (ataxic) becomes aggravated with time
Support patient with pillows, bean bags, restraints, as needed
Control tonic neck reflex by cradlingMay require second person
Sedation / Gen. Anesthesia
Oral Hygiene Needs
Food retention a big problem!Frequent toothbrushingLubrication of gingival tissuesNutritional analysis
Cariogenicity
Fluoride Frequent prophylaxesModified oral hygiene aids

Spinal Cord Injury
Location of injury determines extent
70% < 40 years of age
Overwhelmingly male
50% auto or motorcycle accidents
18% sporting accidents
20+ % occupational
Remaining GSW, falls, etc.
Other Considerations
Grieving ProcessShock
Denial
Reaction
Mobilization
Coping
Other Considerations
Anger
Depression
Withdrawal

Oral Manifestations
Depends on degree of injuryLower limb involvement only
Upper limb involvement
Depends on nature of injuryFractured teeth
Broken jaw / facial bones
Attritionmouthstick

Patient Management
Inspect office and operatories for barriers
Parking availabilityAccessible entranceDoorway widths (32 “+)Flooring materials Hallway width (36”+)Turnaround space (60”+)Restroom access

Patient Management
Operatory AccessibilityWheelchair transfer access
Follow the patient’s lead
Use the brakes
Have adequate physical support
Check urinary catheters during and after

Oral Hygiene Needs
Extremely important
Mouth and teeth often substitute for arms and hands
Modified aids
Engage caregiver

Mental Disabilities
Mental Illness
Mental Retardation

Mental Illness
“an illness with psychological or behavioral manifestations and/or impairment in functioning due to social, psycholgic, genetic, physical/chemical, or biologic disturbance. The disorder is no limited to relations between the person and society. The illness is characterized by symptoms and/or impariment in functioning.”
Mental Retardation
“A significant subaverage general intellectual functioning which originates during the developmental period and is associated with impairment in adaptive behavior”

Adaptations
Mental illness requires adaptations in both physical and emotional realms
Mental retardation requires adaptations in both physical and educational realms

Mental Illness
Affects one-sixth of Americans at some point in their lifetime
Chronic major depression affects 3-5% of total population

Mental Illness
For womenPhobias
Depression
For MenChemical dependence
Phobias
2-5% of populationAnxiety disorders

Patient Management
Consistency
Regularity
Reliability
Important for patients still working on stabilization

Patient Management
Dietary analysisSugar addiction
Pain controlAnxiety issues
Informed consent
Compliance
Patient Management
Drug interactions
Oral complications
What are side effects of meds?Xerostomia often with psych meds
Mental Retardation
Mild – 89% IQ 50-55 to 70 – “Educable”
Moderate – 6%IQ 35-40 to 50-55 – “Trainable”
Severe – 3.5%IQ 20-25 to 35-40
Profound – 1.5%IQ below 20 or 25

Etiology
Acquired – 9%Physical disorders of childhood
Environmental / chemical influences
Inherited – 13%i.e. Down’s
Perinatal problems i.e. FAS
Unknown – 75%

Oral Manifestations
Thick lips
Tooth anomalies
Periodontal conditions
Oral habits
Dental caries

Personalization of Care
Nutritional counseling
Simplified OH techniques
Repetitive follow-up
“An aggressive approach to preventive care, not an aggressive approach to the patient….”

Patient Management
Tailor to patient skills and comprehension
Sedation and/or general anesthesia may be required
NEVER “HOM”(hand over mouth)
Oral Hygiene Needs
Prevention and SimplificationBetter to prevent than treat
Have patient demonstrate and repeat!
KISS
Engage caregivers
Treat the Patient!Talk to the patient, not about the patient

HOME CARE HELPS

Daily Oral Hygiene
Manual toothbrushes can be easily modified
For self
For care-giver

Specialized Toothbrushes
Collis Curve Brush 1-800-298-4818

Specialized Brushes
www.colliscurve.com

Specialized Brushes
The Surround1-800-722-7375
www.specializedcare.com

Specialized Brushes
DexTBrush1-800-352-9669www.prevdentspec.com

Conclusion
Preparation
Respect
Recognize Limitations
Patients
Your own!

Resourceshttps://ice.iqsolutions.com/nohic/poc/publication/general.aspx
(This resource has great tips!)
LinguaFix
1-800-328-3899
www.zirc.com

Resources
Collis Curve Brush1-800-298-4818www.colliscurve.com
The Surround1-800-722-7375www.specializedcare.com
DexTBrush 1-800-352-9669www.prevdentspec.com