patrick webb, dean for academic affairs friedman school of nutrition tufts university boston des...
TRANSCRIPT

Patrick Webb, Dean for Academic Affairs
Friedman School of NutritionTufts University
Boston
Des Moines, Iowa October 13, 2005
Child Malnutrition – Child Malnutrition – TRENDS, SUCCESSES AND TRENDS, SUCCESSES AND
CHALLENGESCHALLENGES
United Nations System Standing Committeeon Nutrition

United Nations United Nations Standing Committee on Standing Committee on Nutrition (UN SCN)Nutrition (UN SCN)
“The SCN vision is a world where hunger and malnutrition are no longer impediments to human development.”
The mandate of SCN is to mobilize commitment to solve nutrition problems; to refine the direction, increase the scale and strengthen the coherence and impact of actions against malnutrition worldwide.

In 2005, c. 11 million children will die before age of 5—one every five seconds.
Many will die in conflicts or natural disasters
Most will die because already undernourished
But most child deaths occur outside emergencies
The main cause of death varies, but >50% willdie of factors linked directly to malnutrition.
The RealityThe Reality

0
5
10
15
20
25
30
35
neonataldeaths
diarrhea pneumonia malaria other AIDS Measles Unknown
% o
f ch
ild d
eath
s
proportion of deaths from being underweight
Under-nutrition is responsible for Under-nutrition is responsible for half of all Child Deathshalf of all Child Deaths
Source: Black, Morris, Bryce (2003) Lancet; 361: 2226-34
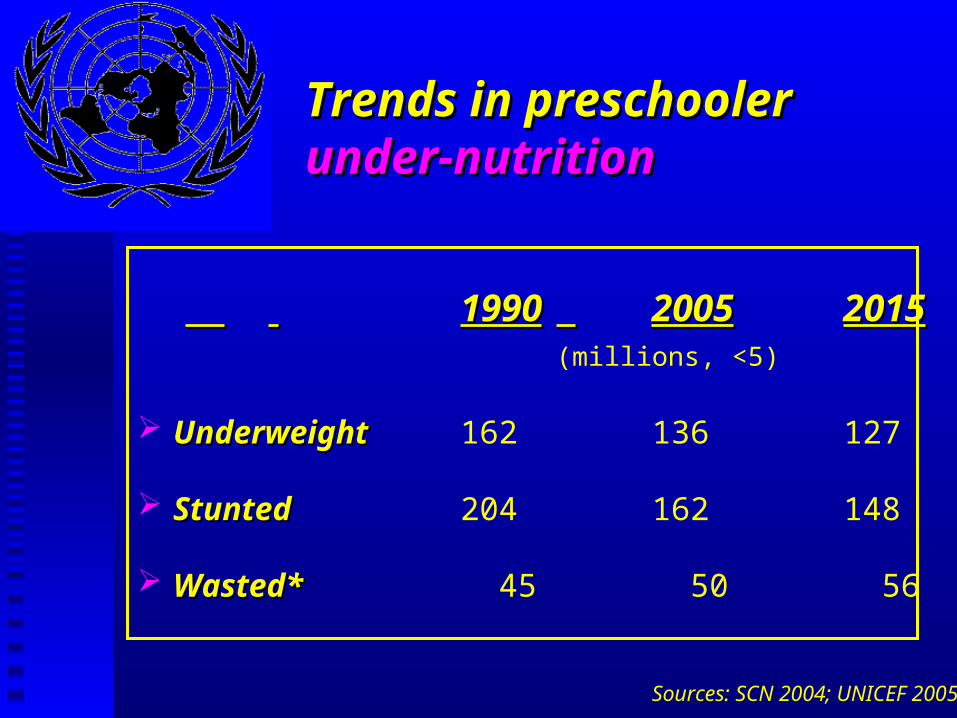
Trends in preschooler Trends in preschooler under-nutritionunder-nutrition
19901990 20052005 20152015(millions, <5)
UnderweightUnderweight 162 136 127
StuntedStunted 204 162 148
Wasted*Wasted* 45 50 56
Sources: SCN 2004; UNICEF 2005*

TrendsTrends
Wasting increasing in all regions of Africa
Most malnourished (<5) still in Asia, but locus of problem shifting to Africa
Obesity in some countries coexists at same level as undernutrition, and continues to grow…
But, principal challenge remains unfinished.

Child undernutrition increasing in Child undernutrition increasing in SSA and still high in South AsiaSSA and still high in South Asia
27 3034 37
4144
89 91 8881
7264
1980 1985 1990 1995 2000 2005
Sub-Saharan Africa Asia-South-central
Source: Based on estimates from de Onis and Blossner 2003
Millions <5 stunted


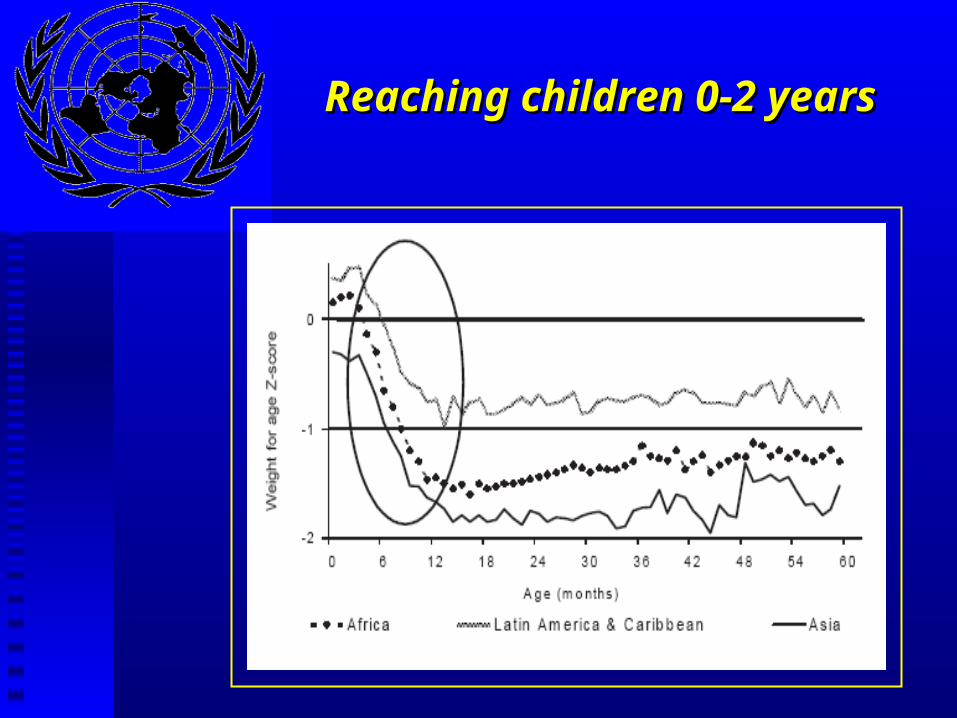
Reaching children 0-2 yearsReaching children 0-2 years

Factors linking Factors linking under-nutritionunder-nutritionwith obesity?with obesity?
In Utero nutritional ‘insults’ -- links with chronic disease, diabetes and obesity
Breastfeeding --“increasing body of evidence shows protective effect of breastfeeding against obesity” (Labbock 2005)
Stunting --“childhood stunting may be a risk factor indevelopment of obesity” (Popkin et al. 2003)
Micronutrient deficiencies -- high cholesterol foods linked with decliningfruit/veg., obesity in Mexico and US (Hawkes 2005)

Maternal Maternal obesity and low BMIobesity and low BMI
BMI <18.5 >30.0 (%)
Egypt 1 32Columbia 3 10Zimbabwe 5 7Armenia 5 7Ethiopia 26 0.2Bangladesh 45 0.7
Data >2000; SCN 2004)

Micronutrient Initiative (2005)Micronutrient Initiative (2005)
(Discounted present value).
Micronutrient Initiative 2005
Important gains in vitamin A Important gains in vitamin A and iodine; but…and iodine; but…

Successes Successes (…yes there are many!)
1. Protocols and Products1. Protocols and Products: Saving lives in crises
2. Technology and Targeting2. Technology and Targeting: Delivering the goods
3. Knowledge and Know-How3. Knowledge and Know-How: Nutrition as a right(legislation in India, Brazil); Entitlements;
Nutrition Education
4. Synergies not Silos4. Synergies not Silos: UN/SCN; MDG Hunger Task Force; joint agency programming; WFPrize


1.1. Protocols and Products Protocols and Products
in Emergency Reliefin Emergency Relief
Despite rise in number and scale of disasters, excess mortality in crises has been falling. Reported non-violent deaths in major emergencies fell by 40% 1993 and 2003 compared with previous decade.
Humanitarian agencies are doing better at saving lives through more timely responses, improved mobilization of resources, and better management of both the symptoms and causes of malnutrition.


Niacin 10 mg*
Biotin 0.1 mg
Potassium 1173 mg*
Magnesium 73 mg*
Iron 0.35 mg max
Zinc 20 mg*
Copper 3 mg*
Selenium 47 μg*
Iodine 76 μg*
Sodium 170 mg max

2. Technology and Targeting2. Technology and Targeting


Mobile milling and Mobile milling and fortification unitfortification unit (Nangweshi refugee camp, Zambia)

3. Knowledge and Know-how3. Knowledge and Know-how
Awareness that nutrition is everyone’s responsibility (Gambia example)
Knowledge about rights, entitlements
Nutrition education (breastfeeding; riding out shocks)


“[Poorest] households with nutrition knowledge… allocate 20% more of their food budget to micronutrient-rich foods than do households lacking nutrition knowledge.”
Block (2004) Maternal Nutrition Knowledge and Demand for Micronutrient-Rich Foods, JDS.
Based on work by HKI, UNICEF, Gov Indonesia
Nutrition knowledgeNutrition knowledge..

4. Synergies not Silos:4. Synergies not Silos:Optimum packages for nutritionOptimum packages for nutrition
“Although increased incomes are essential, it has been shown that countries implementing direct nutritioninterventions have been more successful in
reducing malnutrition.
Approaches that should be supported include;promotion of breastfeeding, supplementary feeding, immunization, treatment of diarrhoea, supplementssuch as iron, folic acid, iodised salt, food
supplementation and micronutrient-rich foods.”
OECD/WHO. 2003. Poverty and Health. DAC Guidelines. Paris.
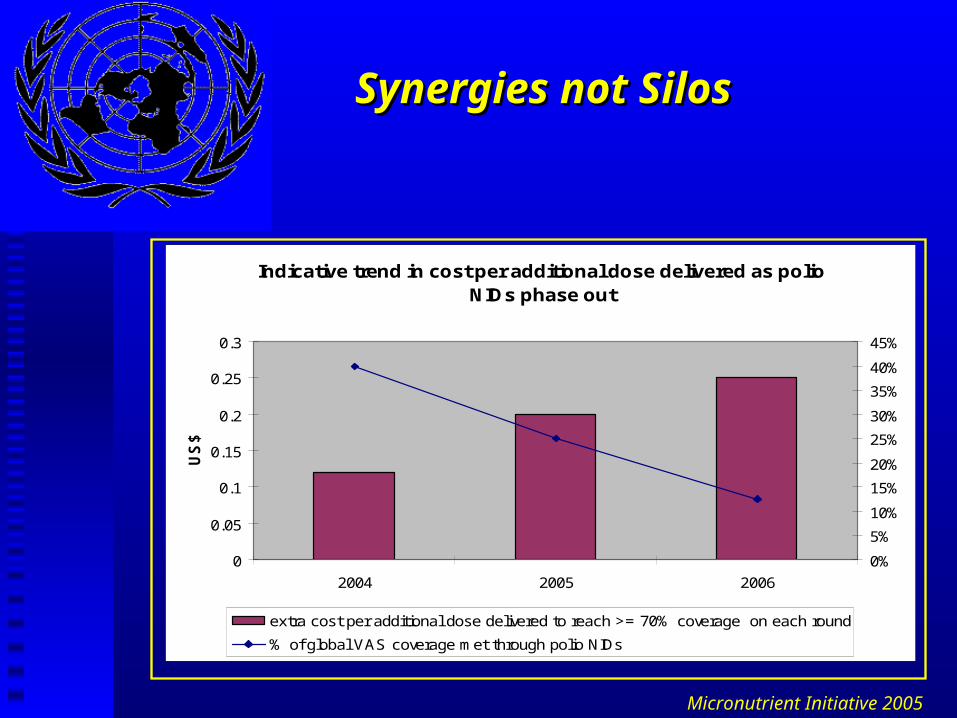
Synergies not SilosSynergies not Silos
Indicative trend in cost per additional dose delivered as polio NIDs phase out
0
0.05
0.1
0.15
0.2
0.25
0.3
2004 2005 2006
US
$
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
extra cost per additional dose delivered to reach >= 70% coverage on each round
% of global VAS coverage met through polio NIDs
Micronutrient Initiative 2005

Institutional Synergies, not SilosInstitutional Synergies, not Silos
SCN is forum for identifying gaps in knowledge (science and practice), promote harmonized policies and approaches, share information, advocate.
Joint programming among agencies

Persistent Challenges Persistent Challenges
Reaching early pregnancy and 0-2 years Exclusive Breastfeeding Iron deficiency anemia Preventing obesity
Interventions at scale Resolving the worst cases—where capacity
is weakest and funding negligible Mutually reinforced actions needed
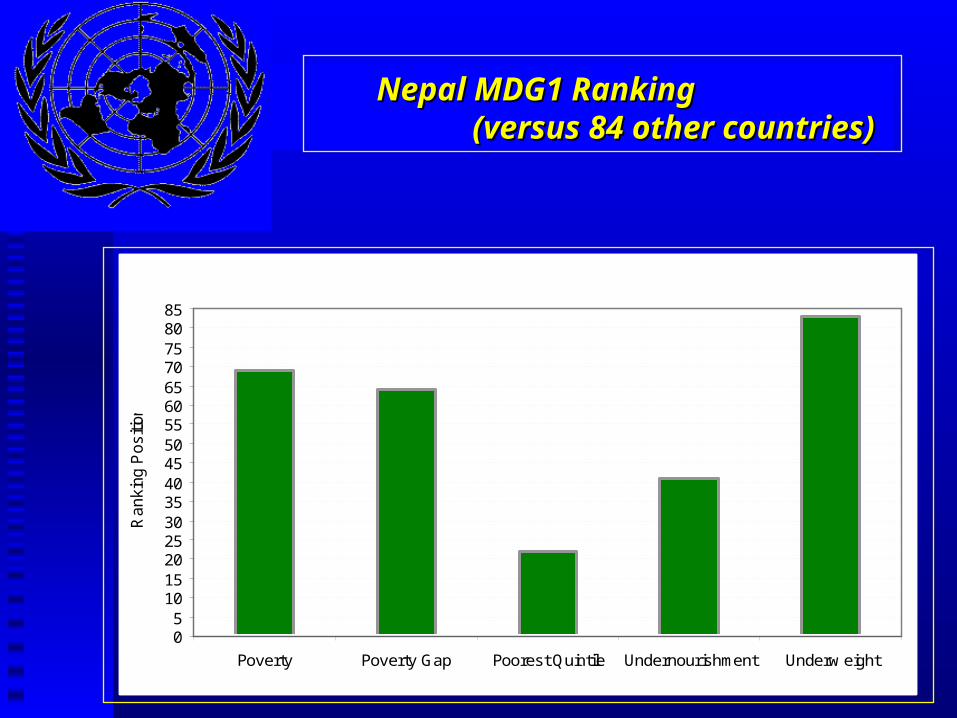
Prioritizing AssistanceNepal MDG1 Ranking Nepal MDG1 Ranking
(versus 84 other countries)(versus 84 other countries)
05
10152025303540455055606570758085
Poverty Poverty Gap Poorest Quintile Undernourishment Underw eight
Rankin
g P
ositi
on

Progress to meeting MDG 1: Progress to meeting MDG 1: Mauritania and PeruMauritania and Peru
Peru
-3
-2
-1
0
1Poverty
Poverty Gap
Poorest QuintileUndernourishment
Underw eight
Mauritania
0.0
0.5
1.0Poverty
Poverty Gap
Poorest QuintileUndernourishment
Underw eight

Target the process, not just the problemTarget the process, not just the problem:
Mainstreaming in development, PRSPs Challenge the ‘invisibility of malnutritionChallenge the ‘invisibility of malnutrition:
‘forgotten emergencies’, ‘hidden hunger’, Address all aspects (lifecycle) of malnutritionAddress all aspects (lifecycle) of malnutrition:
Wasting, stunting, micronutrients, obesity Protect investments against shocksProtect investments against shocks:
Multiple inputs, links with all MDGsLegislated empowerment (rights)Legislated empowerment (rights)::
Meeting demand requires funds for nutrition
ConclusionsConclusions

http://www.unsystem.org/scn/http://www.unsystem.org/scn/
Thank-youThank-you
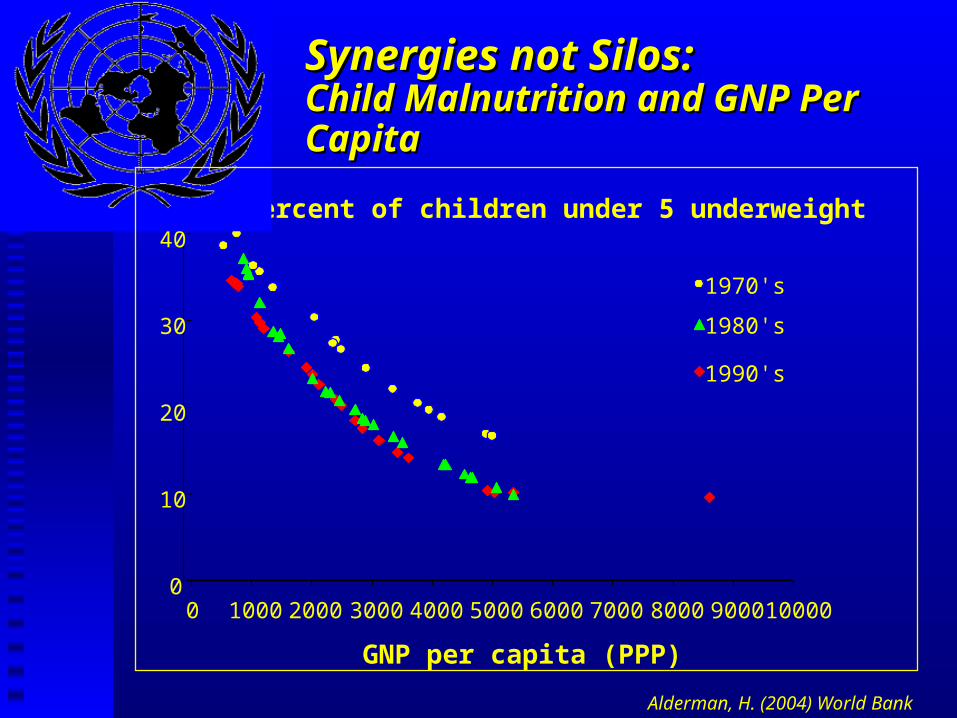
Synergies not Silos:Synergies not Silos:Child Malnutrition and GNP Per CapitaChild Malnutrition and GNP Per Capita
0
10
20
30
40
0 1000 2000 3000 4000 5000 6000 7000 8000 9000 10000
GNP per capita (PPP)
Percent of children under 5 underweight
1990's
1970's
1980's
Alderman, H. (2004) World Bank

Returns on investments Returns on investments in food fortificationin food fortification
In Kenya, Mexico and Indonesia:
fortification increased workforce productivity by 7 to 42 times the cost of the programs
In The Philippines:
rise in productivity 6 to 21 times cost of program
Micronutrient Initiative (2005)

1.8
1.8
1.9
2.3
2.4
2.8
4.1
6.3
9.5
vitamin A deficiency
low fruit and veg intake
zinc deficiency
High BMI
iron deficiency
high cholesterol
tobacco
unsafe sex
infant and maternal underweight
Infant and Maternal Under-Nutrition Infant and Maternal Under-Nutrition
is Leading Cause of Diseaseis Leading Cause of Disease
Ezzati et. al. 2002
% Burden of Global Disease from

Trends in underweight <5sTrends in underweight <5s

1998 2002 2004
Stunting 62% 42% 38%
Wasting 16% 9% 7%
Source: UNICEF/WFP/DPRK (children 6-72m)
North Korea:North Korea:Repeat National SurveysRepeat National Surveys

ReversingReversingOn trackOn trackMadagascarLesothoZambiaEl SalvadorUzbekistanLaosBoliviaNigerMongolia
MauritaniaTunisiaChileAzerbaijanMalaysiaKenyaChinaThailandBrazil
Progress to date Progress to date in reaching MDG1 targetsin reaching MDG1 targets

MDG1 Goal: MDG1 Goal: Eradicate Extreme Poverty and HungerEradicate Extreme Poverty and Hunger
MDG1 Targets: By 2015 (vz 1990)
1. Halve % people with income <US$1/day
2. Halve % people suffering from Hunger

“Reducing malnutrition is central toreducing poverty. As long as malnutritionpersists, development goals for the
coming decade will not be reached.”
World Bank (2003)
Combating Malnutrition: Time to Act

Bangladesh 2005Bangladesh 2005

Thank-youThank-you

Aceh, January 2005Aceh, January 2005



Severe Wasting (<-2 S.D. wfh)Severe Wasting (<-2 S.D. wfh)
India 3, 500,000Pakistan 706,000*Ethiopia 140,000?Cambodia 84,500*Niger 76,500?Mali 51,600Nepal 36,900Ghana 29,800Laos 26,000
UNICEF (2005; 2005b)

10 years to 2005 saw every sub-region of Africa increase number of wasted under-5s.
Largest number of wasted children not in Africa: 78% of world’s 6 million wasted children live in India, Pakistan and Bangladesh.
Thus, wasting is not simple bi-product of conflict or famine—it reflects failure of long-term
processes, not their sudden and dramatic collapse.
Wasting is a concern Wasting is a concern beyond emergenciesbeyond emergencies

“The quantity of thermal energy required to raise one gram of water by 1°C (i.e. 15°C to 16°C ), at sea level.“
In other words….food is fuel.
What is a calorie?What is a calorie?

Child malnutrition and death
Household Food Insecurity
Inadequate Child and Maternal Care
Lack Health Care, Sanitation,
Manifestation
Immediate Causes
Social, Economic, Environmental Constraints
Childhood Sickness,Growth Impairment
UnderlyingCauses
Adapted from UNICEF
Inadequate DietaryIntake