paving the path to better health - home - rcpa annual ...... miller, k. (2013). care coordination...
TRANSCRIPT
© Copyright 2015 The Children’s Institute of Pittsburgh © Copyright 2015 The Children’s Institute of Pittsburgh
Paving the Path to Better Health
© Copyright 2015 The Children’s Institute of Pittsburgh
Presenters:
Angie Sarneso, LSW, CCM, MPM Director of Care Coordination
Jenny Randolph, RN, LCSW
Care Coordinator
Sarah Fallica, LSW, HSV Social Worker
© Copyright 2015 The Children’s Institute of Pittsburgh
Learning Objectives:
• Implement an effective non-medical home model for family-centered care
• Improve health and quality outcomes for medically complex children
• Empower and strengthen families as advocates for their children

© Copyright 2015 The Children’s Institute of Pittsburgh
Family-Centered Care assures the health and well-being of children and their families through a respectful family-professional partnership. It honors the strengths, cultures, traditions and expertise that everyone brings to this relationship. Family-Centered Care is the standard of practice which results in high quality services.
- National Center for Family-Centered Care
Family-Centered Care

© Copyright 2015 The Children’s Institute of Pittsburgh
Medical Home
The medical home is best described as a model or philosophy of primary care that is patient-centered, comprehensive, team-based, coordinated, accessible and focused on quality and safety.
-American Academy of Pediatrics
© Copyright 2015 The Children’s Institute of Pittsburgh
Care Coordination
Care Coordination is a process that links children and youth with special health care needs and their families with appropriate services and resources in a coordinated effort to achieve good health.
-American Academy of Pediatrics

© Copyright 2015 The Children’s Institute of Pittsburgh
PREVENTIVE HEALTH wellness support and preventive services for healthy patients
DISEASE MANAGEMENT patients with single (or non-complicated) chronic conditions
CASE MANAGEMENT patients with acute, time-limited medical needs
COMPLEX CARE
patients with multiple ongoing medical and
social concerns
Source: California Quality Collaborative
Addressing the Need
© Copyright 2015 The Children’s Institute of Pittsburgh
Medical Complexity
• Severe primary condition in one body system that is more likely to cause significant long lasting health impairment
OR
• Significant chronic condition in two or more body systems
OR
• Progressive or life limiting chronic conditions
OR
• Conditions requiring a dependency on technology
source: The 3M Clinical Risk Group®
© Copyright 2015 The Children’s Institute of Pittsburgh
The Children’s Institute’s Care Coordination Program
• Proof of concept initiative
• Part of a three year strategic plan
• Serving children with complex medical conditions, a subset of children with special healthcare needs
• Family-centered coordination service
© Copyright 2015 The Children’s Institute of Pittsburgh
Care Coordination Program at CI
• A team that includes primary care physicians, specialists, patients and families, care coordinators, health coaches and social workers
• Works with families to ensure that their medically complex children receive the services that they need in a timely manner

Criteria for Enrollment
• Including, but not limited to ABI, SCI and APM
• Medically complex
• 23 county region in western PA
• Child does not need to be receiving services at CI
• No cost to the family

Care Coordination Team • Completes a comprehensive medical and psychosocial
assessment
• Develops a family-centered plan of care including goals and expectations
• Maintains a partnership with PCP and medical providers
• Facilitates communication between home health providers and families
• Revises plan of care when indicated
Care Coordinator
• Conducts ongoing review of family’s medical, social, educational, legal and general needs and identified potential barriers
• Serves as a patient/family advocate
• Assists with the development of goals to decrease caregiver stress
• Promotes independence, empowerment and positive self care
Health Coach
• Reviews presenting psychosocial stressors and barriers
• Establishes a linkage to a wide range of community based social resources
• Coordinates care with community based social service providers to ensure effective service delivery
Social Worker

© Copyright 2015 The Children’s Institute of Pittsburgh
Care Coordination Process
• Intake Referral
• Assessment
• Goal Setting
• Care Planning
• Continuous Monitoring
and Family Coaching

© Copyright 2015 The Children’s Institute of Pittsburgh
Process Evaluation
Precede - Proceed model
Subcommittee and weekly meetings
Gap identification
Measurement tools to evaluate care
coordination perspectives
© Copyright 2015 The Children’s Institute of Pittsburgh
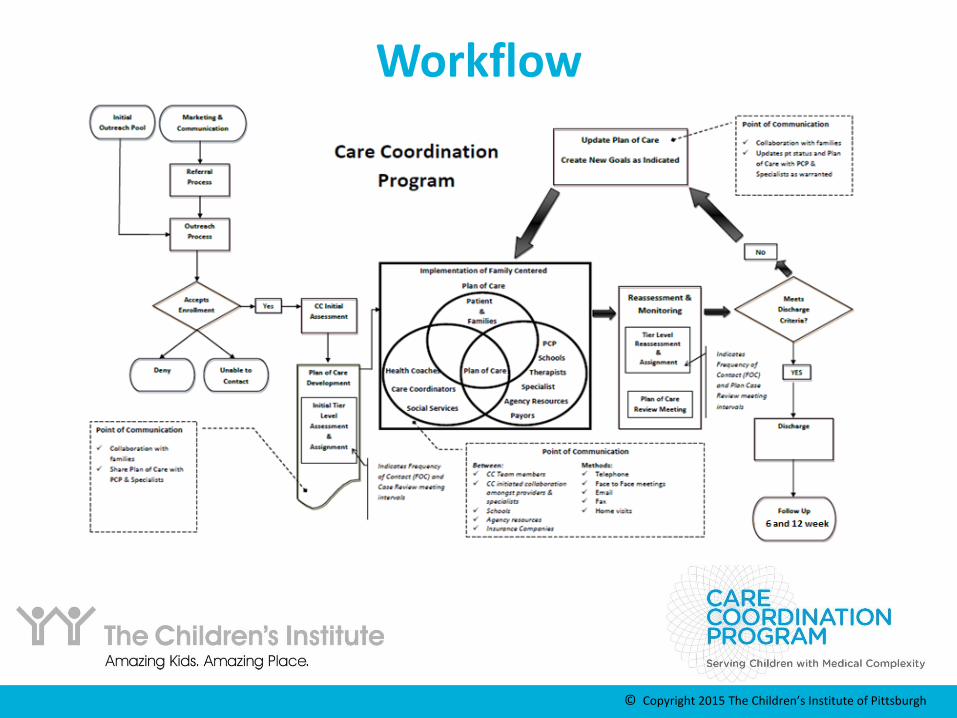
Workflow
© Copyright 2015 The Children’s Institute of Pittsburgh
Tier Risk Assessment
• Tool necessary to determine the medical and psychosocial acuity of our patients and their families.
• The level of intervention, specifically, the frequency of contact coincides with the number of identified risk factors.
• Both Medical and Psychosocial Risks are factors.
• Risks are reassessed by the team on an ongoing basis.
© Copyright 2015 The Children’s Institute of Pittsburgh
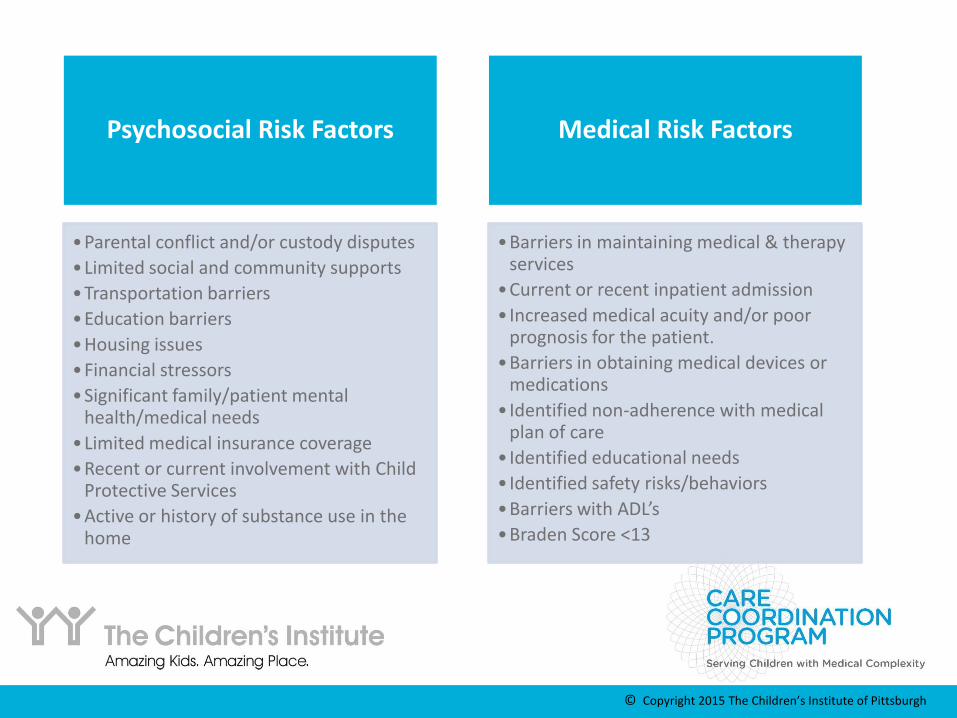
Medical Risk Factors
•Barriers in maintaining medical & therapy services
•Current or recent inpatient admission
• Increased medical acuity and/or poor prognosis for the patient.
•Barriers in obtaining medical devices or medications
• Identified non-adherence with medical plan of care
• Identified educational needs
• Identified safety risks/behaviors
•Barriers with ADL’s
•Braden Score <13
Psychosocial Risk Factors
•Parental conflict and/or custody disputes
•Limited social and community supports
•Transportation barriers
•Education barriers
•Housing issues
•Financial stressors
•Significant family/patient mental health/medical needs
•Limited medical insurance coverage
•Recent or current involvement with Child Protective Services
•Active or history of substance use in the home
© Copyright 2015 The Children’s Institute of Pittsburgh
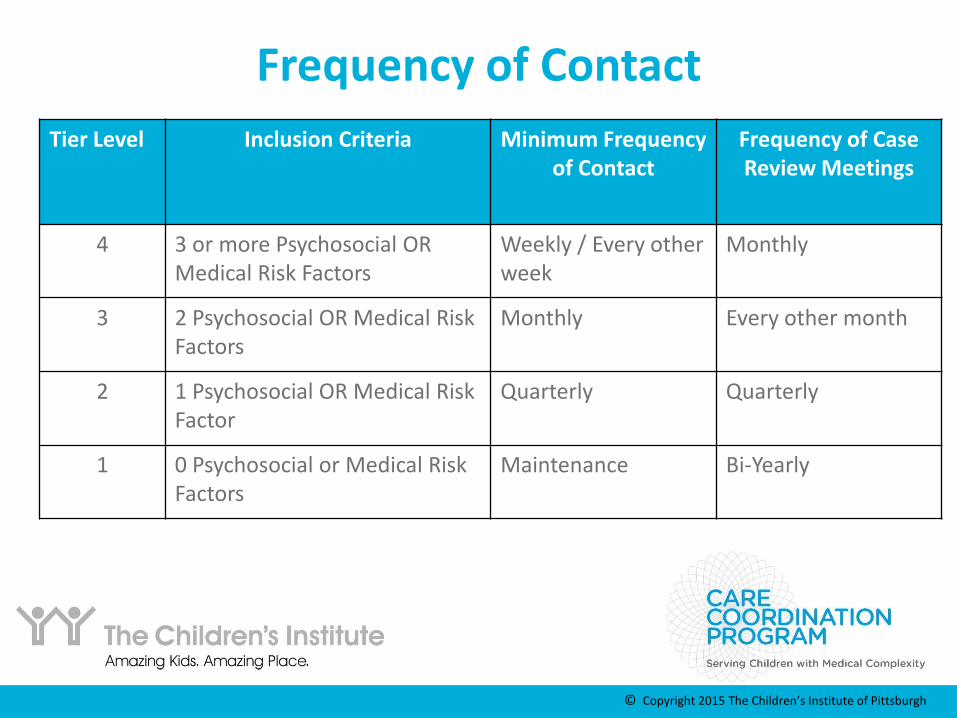
Frequency of Contact
Tier Level Inclusion Criteria Minimum Frequency of Contact
Frequency of Case Review Meetings
4 3 or more Psychosocial OR Medical Risk Factors
Weekly / Every other week
Monthly
3 2 Psychosocial OR Medical Risk Factors
Monthly Every other month
2 1 Psychosocial OR Medical Risk Factor
Quarterly Quarterly
1 0 Psychosocial or Medical Risk Factors
Maintenance Bi-Yearly
© Copyright 2015 The Children’s Institute of Pittsburgh
Measurement Tool
• Measures relevant data to monitor the provision of care including frequency and time.
• Measures: focus of encounter, care coordination activity, method of communication, tasks completed, and outcomes.
• Data is utilized to determine ongoing need for services

© Copyright 2015 The Children’s Institute of Pittsburgh
Discharge Criteria
• Patients that have reached the age of 22
• Patient/family remains at a Tier 1 for a period of six months
• Patient/family demonstrates the ability to manage care independently
• Patient/family declines further involvement
• Patient/family disengages intervention following the completion of the assessment and plan of care

© Copyright 2015 The Children’s Institute of Pittsburgh
Discharge Process • Care coordinator schedules a discharge review
meeting
• Discharge summary will be completed within 1 week of discharge review meeting
• Discharge letter and discharge summary mailed to patient/family, referral source, PCP and other child serving entities
© Copyright 2015 The Children’s Institute of Pittsburgh
Post Discharge Outreach
• Outreach to patient/family by the health coach at 6 weeks and 12 weeks post discharge
• The following information is gathered:
• Verification of receipt of discharge summary
• Current status of following medical recommendations and utilizing established resources
• Data collection

© Copyright 2015 The Children’s Institute of Pittsburgh
Outcomes
Achieve improved health
outcomes
Improve quality of life
Reduce overall healthcare costs
© Copyright 2015 The Children’s Institute of Pittsburgh
Research
Proof of concept
IRB
Research proposal

Gender
Number of
Participants
% of Total
Male 163 64%
Female 92 36%
Diagnosis
Total number of
participants
% of Total
ABI 44 17%
APM 19 7%
ASD 49 19%
CP 13 5%
Developmental
Delays 15 6%
Functional Feeding 26 10%
Genetic Disorder 33 13%
Neurological 9 4%
Obesity 6 3%
SCI 9 4%
Other 31 12%
Age
Summary
Number of
Participants
% of Total
<5 76 30%
5 to 9 76 30%
10 to 15 71 28%
16+ 32 12%
Insurance
Number of
Participants
% of total
Aetna 8 2%
Blue Cross 21 8%
Gateway 52 20%
Highmark 18 7%
UHC 12 5%
UHC Community 12 5%
UPMC 12 5%
UPMC for You 83 33%
Other 24 10%
Unknown 13 5%
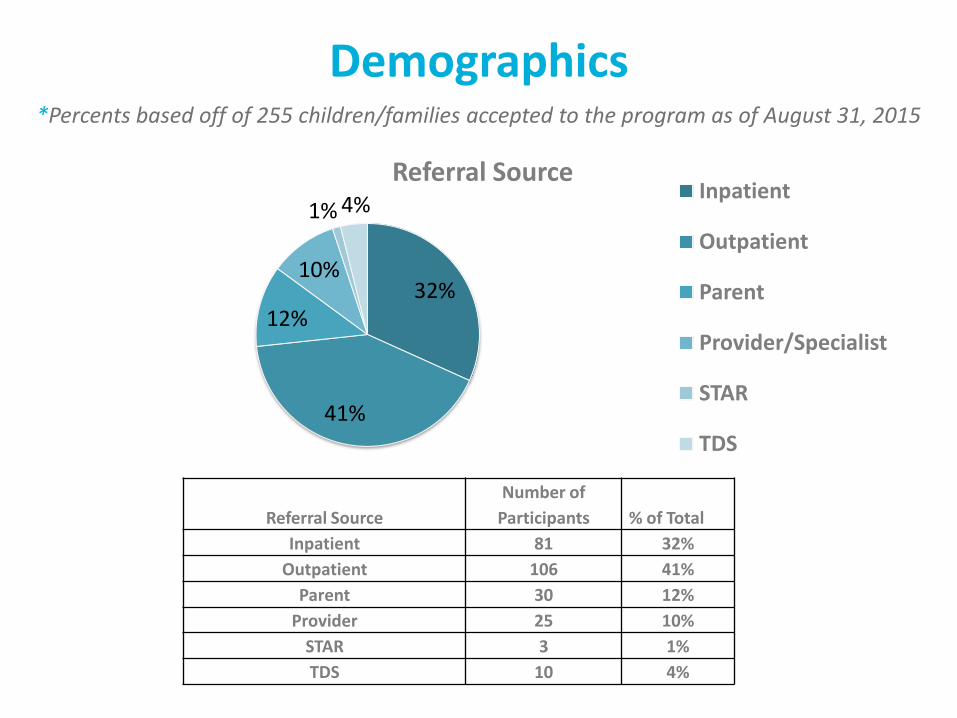
*Percents based off of 255 children/families accepted to the program as of August 31, 2015
Demographics
32%
41%
12%
10%
1% 4%
Referral Source Inpatient
Outpatient
Parent
Provider/Specialist
STAR
TDS
Referral Source
Number of
Participants
% of Total
Inpatient 81 32%
Outpatient 106 41%
Parent 30 12%
Provider 25 10%
STAR 3 1%
TDS 10 4%
Demographics *Percents based off of 255 children/families accepted to the program as of August 31, 2015
© Copyright 2015 The Children’s Institute of Pittsburgh
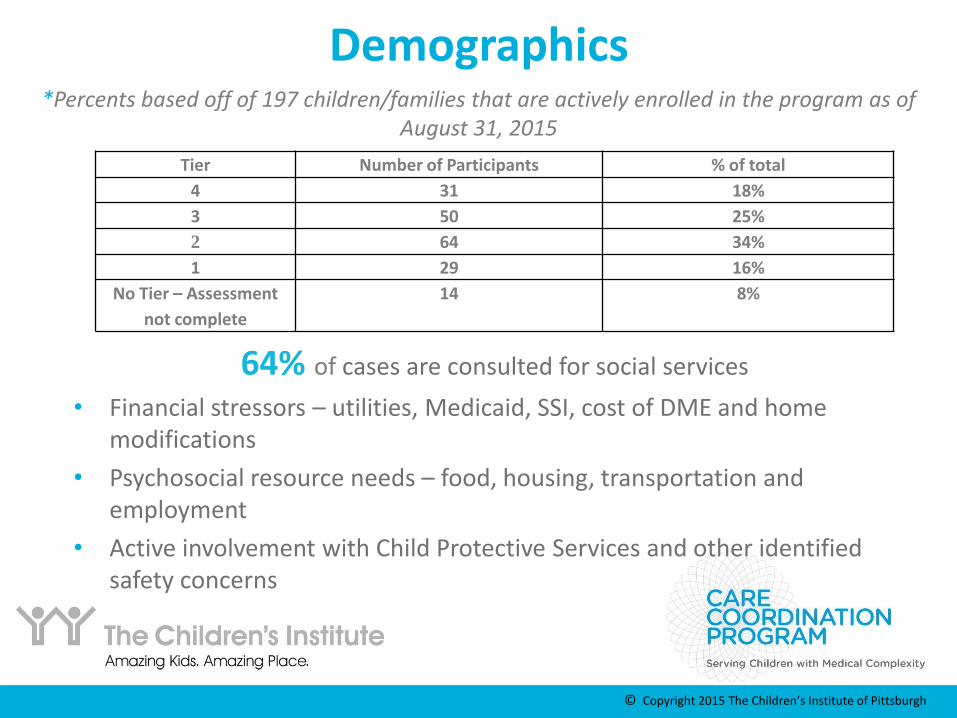
Tier Number of Participants % of total
4 31 18%
3 50 25%
2 64 34%
1 29 16%
No Tier – Assessment
not complete
14 8%
Demographics *Percents based off of 197 children/families that are actively enrolled in the program as of
August 31, 2015
64% of cases are consulted for social services
• Financial stressors – utilities, Medicaid, SSI, cost of DME and home modifications
• Psychosocial resource needs – food, housing, transportation and employment
• Active involvement with Child Protective Services and other identified safety concerns

© Copyright 2015 The Children’s Institute of Pittsburgh
Program Sustainability
• Grant funded at no cost to families and will continue to be no cost to families
• Build referral base through physician and hospital partnerships
• Seek additional grant funding and program promotion
• Negotiate contracts with insurers to establish a per member per month (PMPM)
• NCQA accreditation

© Copyright 2015 The Children’s Institute of Pittsburgh
Thank you!
For more information, please visit: http://www.amazingkids.org
© Copyright 2015 The Children’s Institute of Pittsburgh
Literature Review
Antonelli, R., Stille, C., & Antonelli, D. (2008). Care Coordination for Children and Youth with Special Health Care Needs: A Descriptive, Multisite Study of Activities, Personnel Costs, and Outcomes. Pediatrics, 122(1), e209-e216. DOI:10.1542/peds.2007-2254
Antonelli, R., McAllister, J., & Popp, J. (2009). Making are Coordination a Critical Component of the Pediatric Health System: A Multidisciplinary Framework. Retrieved from www.commonwealthfund.org
Care Coordination in the Medical Home: Integrating Health and Related Systems of Care for Children with Special Health Care Needs (2005). Pediatrics, 116: 1238-1243. Retrieved from http://pediatrics.aappublications.org/content/116/5/1238.full.html
Committee on Children With Disabilities (1999). Care Coordination: Integrating Health and Related Systems of Care for Children With Special Health Care Needs. Pediatrics, 104: 978-891. Retrieved from http://pediatrics.aappublications.org/content/104/4/978.full.html
Craig, C., Eby, D., & Whittington, J. (2011). Care Coordination Model: Better Care at Lower Costs for People with Multiple Health and Social Needs. IHI Innovation Series white paper, 1-25. Cambridge, Massachusetts: Institute for Healthcare Improvement; 2011. Retrieved from www.ihi.org
Feldman, Heidi M. (2013). Redesigning Health Care for Children with Disabilities: Strengthening Inclusion, Contribution, and Health. Baltimore, MD: Paul H. Brookes Publishing Co.
© Copyright 2015 The Children’s Institute of Pittsburgh
Literature Review
“Health Care Utilization by Children”, Jacqueline Kuesner, Madeleine McDowell, Dave Jackson, Donna Shelton, Children’s Hospital Association, November 2013. McAllister, J., Presler, E., & Cooley, C. (2007). Medical Home Practice-Based Care Coordination. Center for Medical Home Improvement. Retrieved from United States Maternal and Child Health Bureau, Integrated Services for CSHCN, HRSA. McDonald, K.M., Schultz, E., Albin, L., Pineda, N., Lonhart, J., Sundaram, V., Smith-Spangler, C., Brustrom, J., Malcolm, E. (2010). Care Coordination Measures Atlas. Agency for Healthcare Research and Quality. AHRQ Publication No. 11-0023-EF. Retrieved from http://archive.ahrq.gov/professionals/systems/long-term-care/resources/coordination/atlas/index.html Miller, K. (2013). Care Coordination Impacts on Access to Care for Children with Special Health Care Needs Enrolled in Medicaid and CHIP. Maternal Child Health Journal, 18: 864-872. DOI:10.1007/s10995-013-1312-z
Minnesota Statutes.(2014). Care Coordination Tier Assignment Tool: Health Care Home Initiative, Version 1.0-1.2. Retrieved from http://www.health.state.mn.us/healthreform/homes/payment/HCHComplexityTierTool_March2010.pdf Wise, PH, Huffman, LC, & Brat, G. A Critical Analysis of Care Coordination Strategies for Children With Special Health Care Needs. Technical Review No. 14. (Prepared by the Stanford University—UCSF Evidence-based Practice Center under Contract No. 290-02-0017). AHRQ Publication No. 07-0054. Rockville, MD: Agency for Healthcare Research and Quality. June 2007. Wood, D. & Goldhagen, J. (2013). Promoting Child Health Equity: Family-Centered Care Coordination Is Just One Piece of the Puzzle. Pediatrics, 131: 336-337. DOI: 10.1542/peds.2012-3248