payer perspectives on value-based contracting2014 life sciences industry forum payer perspectives on...
TRANSCRIPT

2014 Life Sciences Industry Forum
Payer Perspectives On
Value-based Contracting
Miles Snowden, MD, MPH, CEBS
Chief Medical Officer
1

2014 Life Sciences Industry Forum
Making the health system work better for everyone
A simple goal
2

2014 Life Sciences Industry Forum
60,000,000+ individuals
Statistics as of 6/30/13 except where noted; *as of 1/17/13
80,000 provider practices and other health care facilities
67,000 pharmacies*
5,000 hospitals
400 global life sciences organizations
300 health plans
150 state, federal and municipal agencies and departments
Optum serves
3

2014 Life Sciences Industry Forum
% Who Feel There are Significant Differences
in Quality of Care in Community
Majorities of physicians and, especially, hospital execs see significant differences in quality of care across the community.
Base: All Qualified Respondents: (Physicians n = 1,602, Consumers n = 3,400 / 3,398 / 3,397, Hospitals n = 400)
Q625/Q425/Q325 Are there, or are there not, significant differences in the quality of care provided by doctors and hospitals in your local area?
PHYSICIANS (A)
CONSUMERS (B)
HOSPITALS (C)
55%
37%
62%
4
2014 Life Sciences Industry Forum
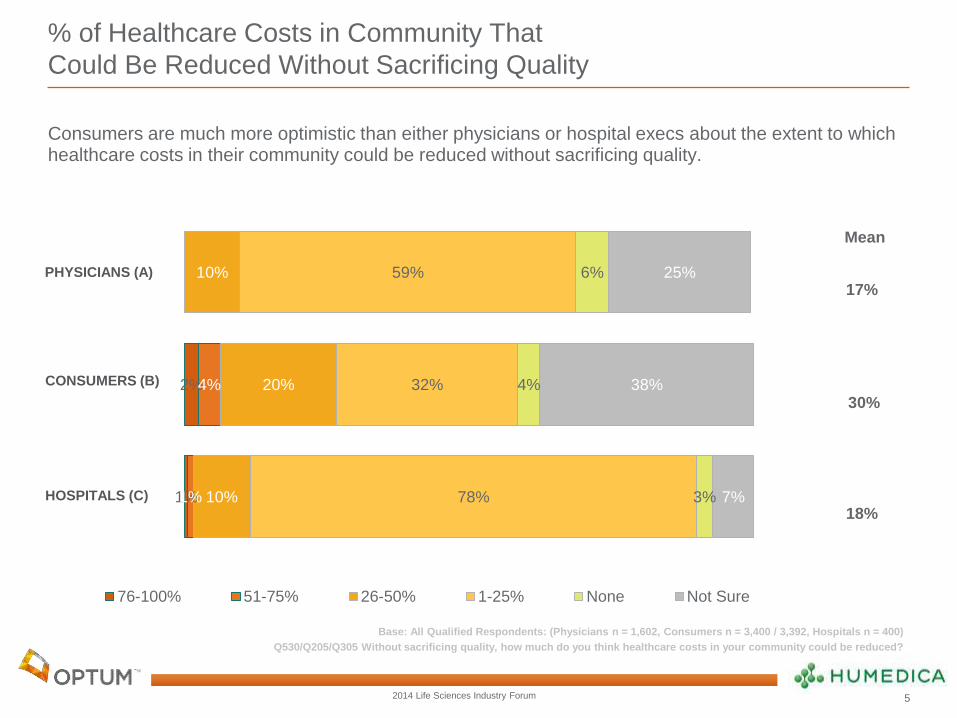
% of Healthcare Costs in Community That
Could Be Reduced Without Sacrificing Quality
Consumers are much more optimistic than either physicians or hospital execs about the extent to which healthcare costs in their community could be reduced without sacrificing quality.
Base: All Qualified Respondents: (Physicians n = 1,602, Consumers n = 3,400 / 3,392, Hospitals n = 400)
Q530/Q205/Q305 Without sacrificing quality, how much do you think healthcare costs in your community could be reduced?
2%
1%
4%
1%
10%
20%
10%
59%
32%
78%
6%
4%
3%
25%
38%
7%
76-100% 51-75% 26-50% 1-25% None Not Sure
PHYSICIANS (A)
CONSUMERS (B)
HOSPITALS (C)
17%
Mean
30%
18%
17%
Mean
30%
18%
5
2014 Life Sciences Industry Forum
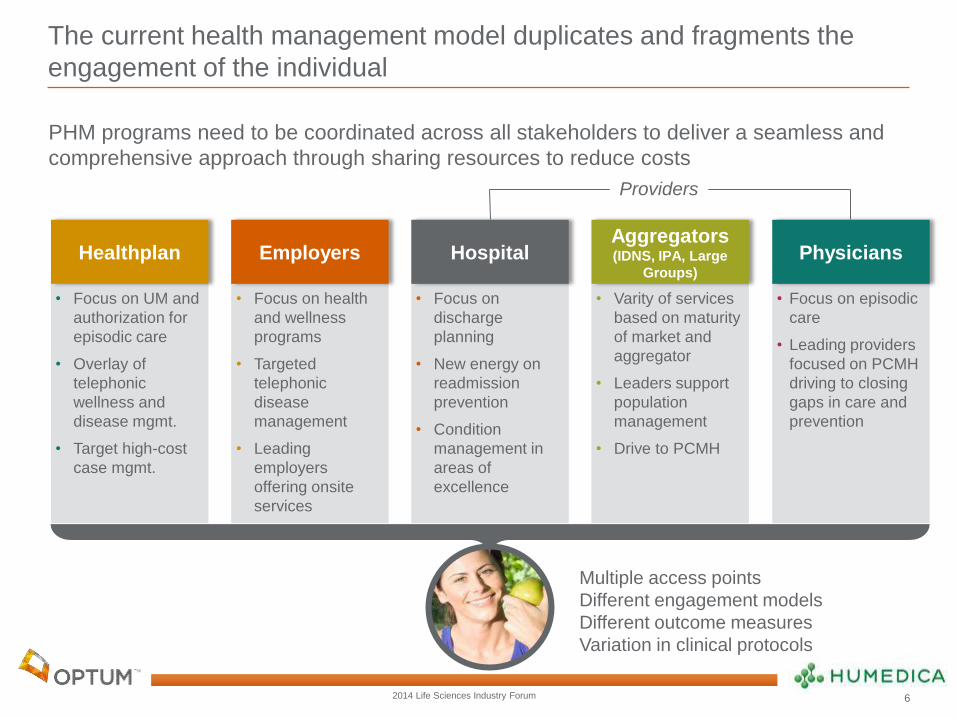
The current health management model duplicates and fragments the
engagement of the individual
• Focus on UM and
authorization for
episodic care
• Overlay of
telephonic
wellness and
disease mgmt.
• Target high-cost
case mgmt.
Healthplan
• Focus on health
and wellness
programs
• Targeted
telephonic
disease
management
• Leading
employers
offering onsite
services
Employers
• Focus on
discharge
planning
• New energy on
readmission
prevention
• Condition
management in
areas of
excellence
Hospital
• Varity of services
based on maturity
of market and
aggregator
• Leaders support
population
management
• Drive to PCMH
Aggregators (IDNS, IPA, Large
Groups)
• Focus on episodic
care
• Leading providers
focused on PCMH
driving to closing
gaps in care and
prevention
Physicians
Providers
Multiple access points
Different engagement models
Different outcome measures
Variation in clinical protocols
PHM programs need to be coordinated across all stakeholders to deliver a seamless and
comprehensive approach through sharing resources to reduce costs
6

2014 Life Sciences Industry Forum
We begin by understanding the market trends
Trends Implications
1. Need to focus on clinical and
operational improvement to achieve
value beyond market share
2. Market is defining new
reimbursement models focused on
population management
3. Market is defining new incentives
and penalties in physician
compensation models
4. New primary care models are
being deployed
5. New capabilities needed to
measure and deliver value-based
care
Continued focus on gaining market leverage with
payer community
Consolidation of
Provider
Community
System
Affordability
Consumers are faced with a health care affordability
crisis
Value-Based
Care Models
Aligned economic and practice incentives between
providers and payers
Population Care
Management
Focus on managing populations and individuals
across the system of care
Industry Defined
Performance
Measurements
New patient satisfaction, outcomes and quality
measurements are tied to reimbursement and
compensation models
7

2014 Life Sciences Industry Forum
There are many new partnership models occurring to engage
stakeholders in many different ways
Private Exchanges/Defined Contribution Direct to Employer
Three-Prong Partnership Traditional
8
Payer
Provider
Employer
Employer
Provider
Payer
Individual
Employer
Provider
Individual
Employer
Payer
Payer Provider
Ind
ivid
ua
l
Payer Provider
Exchange
8
2014 Life Sciences Industry Forum
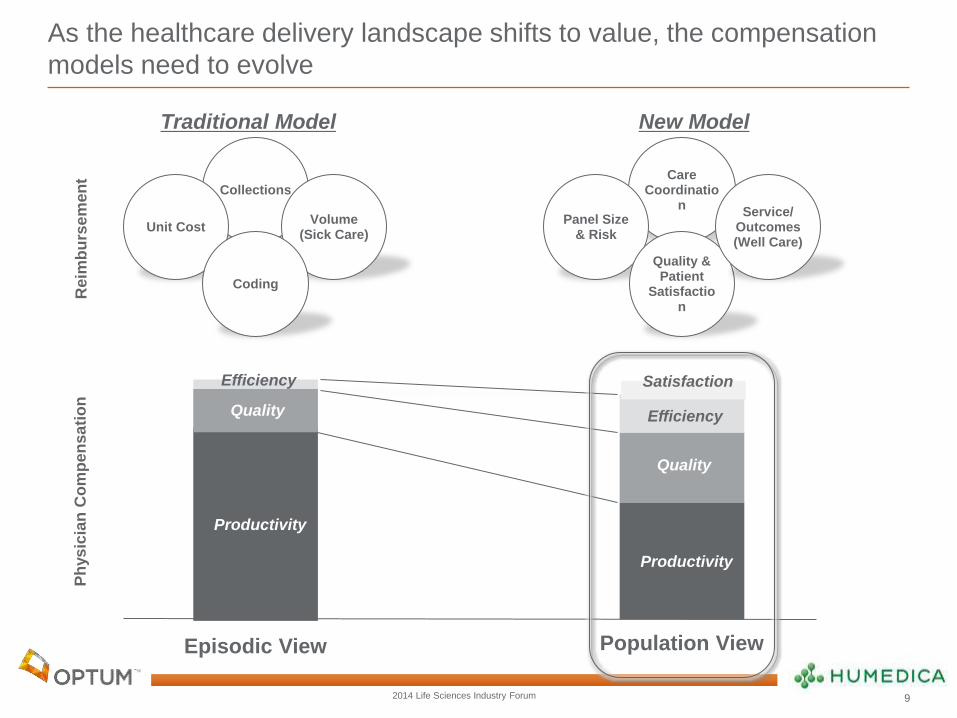
As the healthcare delivery landscape shifts to value, the compensation
models need to evolve
Collections Care
Coordination
Panel Size & Risk
Quality & Patient
Satisfaction
Service/ Outcomes (Well Care)
Productivity
Quality
Efficiency
Ph
ys
icia
n C
om
pe
nsa
tio
n
Unit Cost Volume
(Sick Care)
Coding
Reim
bu
rse
men
t
Traditional Model New Model
Population View
Productivity
Quality
Efficiency
Episodic View
9
Satisfaction
2014 Life Sciences Industry Forum
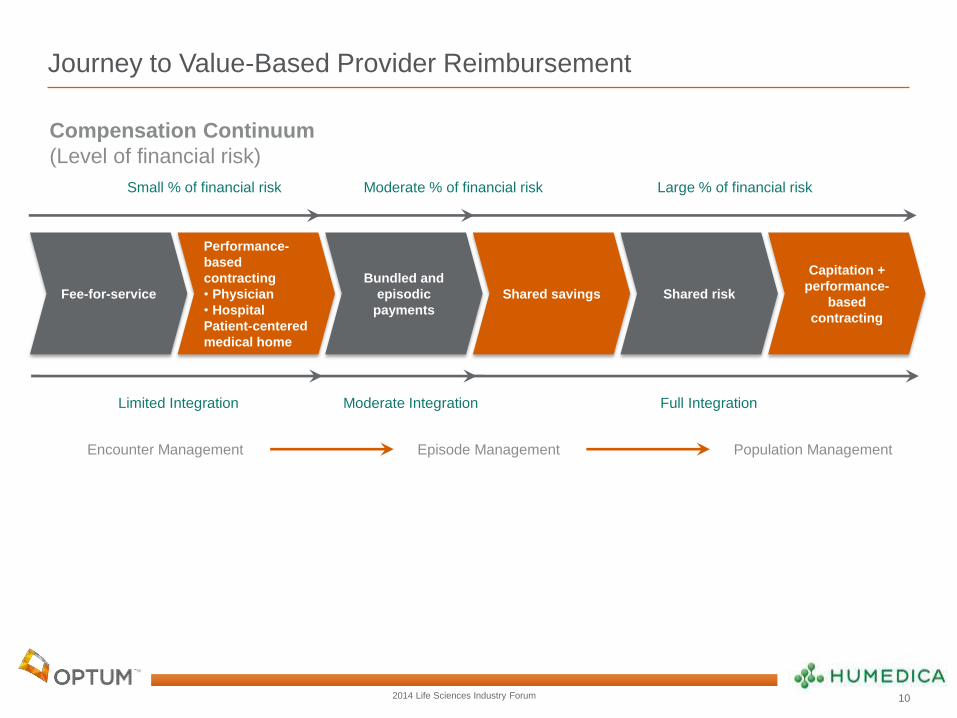
Journey to Value-Based Provider Reimbursement
Fee-for-service
Performance-
based
contracting
• Physician
• Hospital
Patient-centered
medical home
Bundled and
episodic
payments
Shared savings Shared risk
Capitation +
performance-
based
contracting
Episode Management Encounter Management Population Management
Moderate Integration Full Integration Limited Integration
Small % of financial risk Moderate % of financial risk Large % of financial risk
Compensation Continuum
(Level of financial risk)
10
2014 Life Sciences Industry Forum
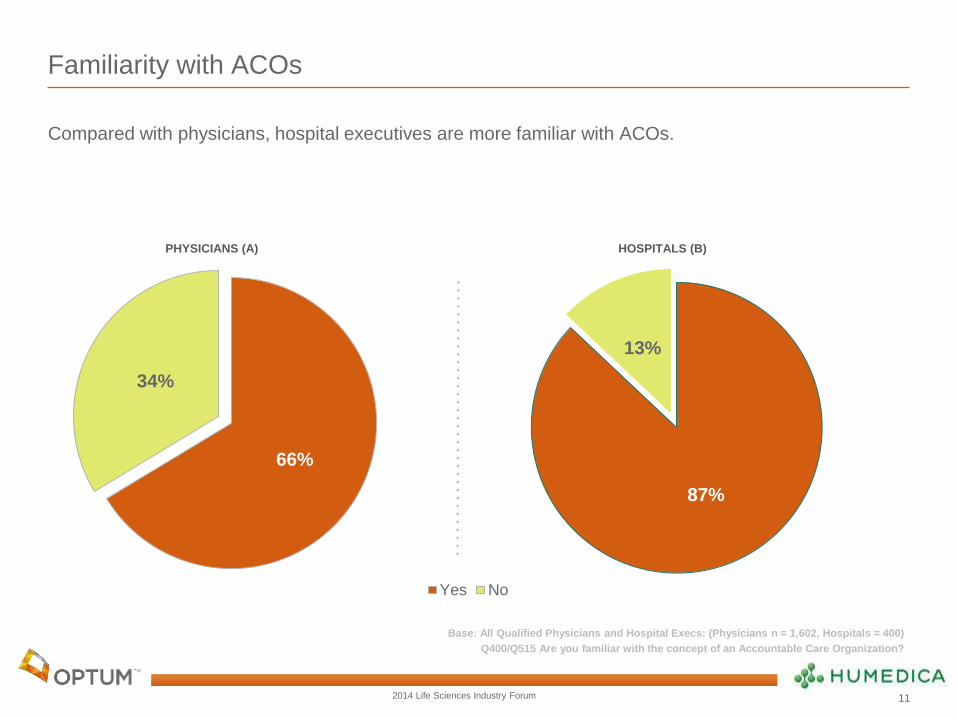
87%
13%
Familiarity with ACOs
Compared with physicians, hospital executives are more familiar with ACOs.
Base: All Qualified Physicians and Hospital Execs: (Physicians n = 1,602, Hospitals = 400)
Q400/Q515 Are you familiar with the concept of an Accountable Care Organization?
66%
34%
Yes No
HOSPITALS (B) PHYSICIANS (A)
11
2014 Life Sciences Industry Forum
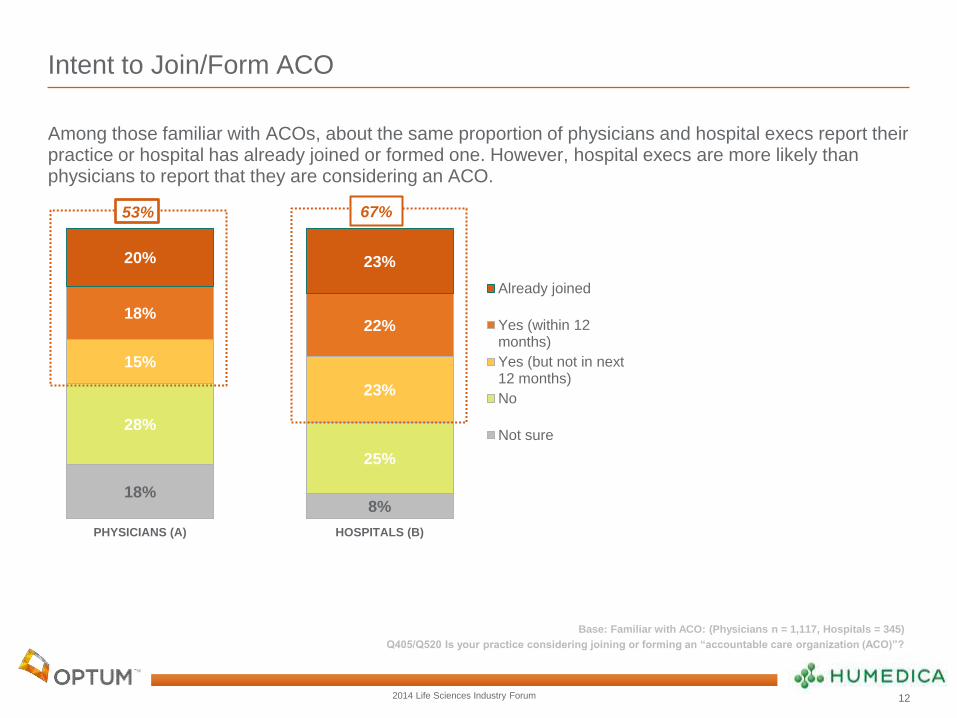
8% 18%
25%
28%
23%
15%
22% 18%
23% 20%
HOSPITALS (B)PHYSICIANS (A)
Already joined
Yes (within 12months)
Yes (but not in next12 months)
No
Not sure
Intent to Join/Form ACO
Among those familiar with ACOs, about the same proportion of physicians and hospital execs report their practice or hospital has already joined or formed one. However, hospital execs are more likely than physicians to report that they are considering an ACO.
Base: Familiar with ACO: (Physicians n = 1,117, Hospitals = 345)
Q405/Q520 Is your practice considering joining or forming an “accountable care organization (ACO)”?
A
53% 67%
12
2014 Life Sciences Industry Forum
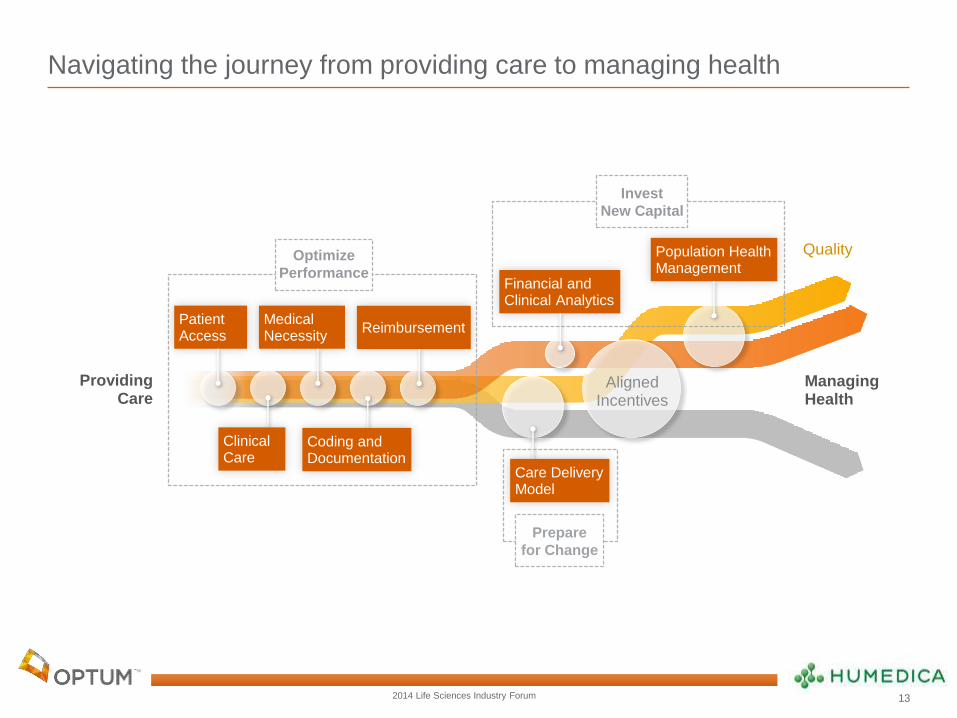
Navigating the journey from providing care to managing health
Quality
Patient Access
Medical Necessity
Reimbursement
Financial and Clinical Analytics
Population Health Management
Aligned Incentives
Providing Care
Clinical Care
Coding and Documentation
Care Delivery Model
Managing Health
Prepare
for Change
Optimize
Performance
Invest
New Capital
13
2014 Life Sciences Industry Forum
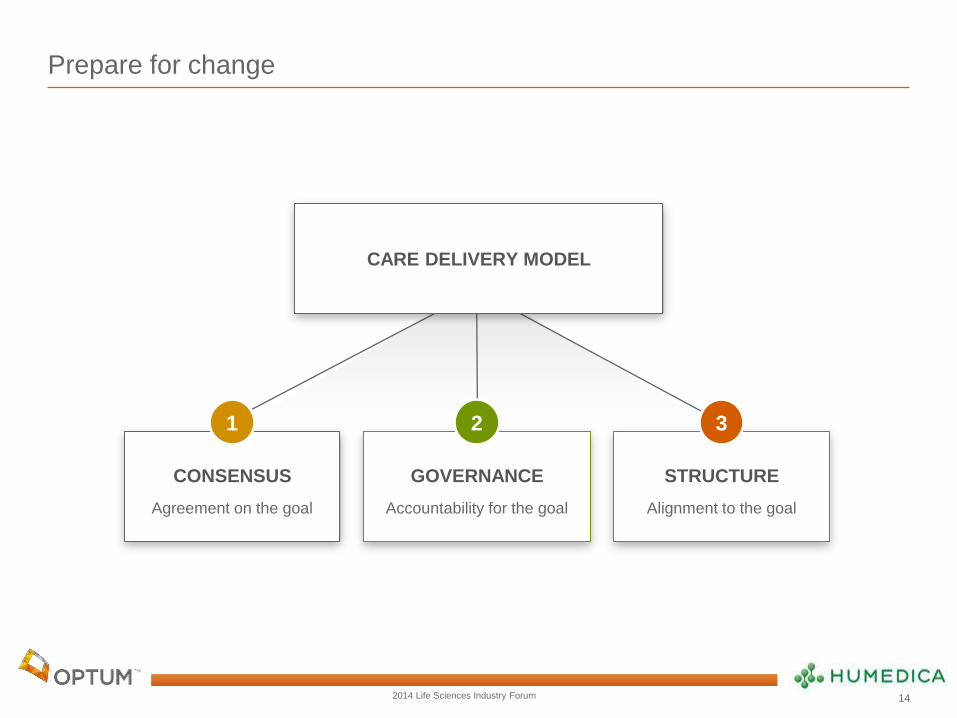
Prepare for change
CONSENSUS
Agreement on the goal
1
STRUCTURE
Alignment to the goal
3
Care delivery model
GOVERNANCE
Accountability for the goal
2
CARE DELIVERY MODEL
14
2014 Life Sciences Industry Forum
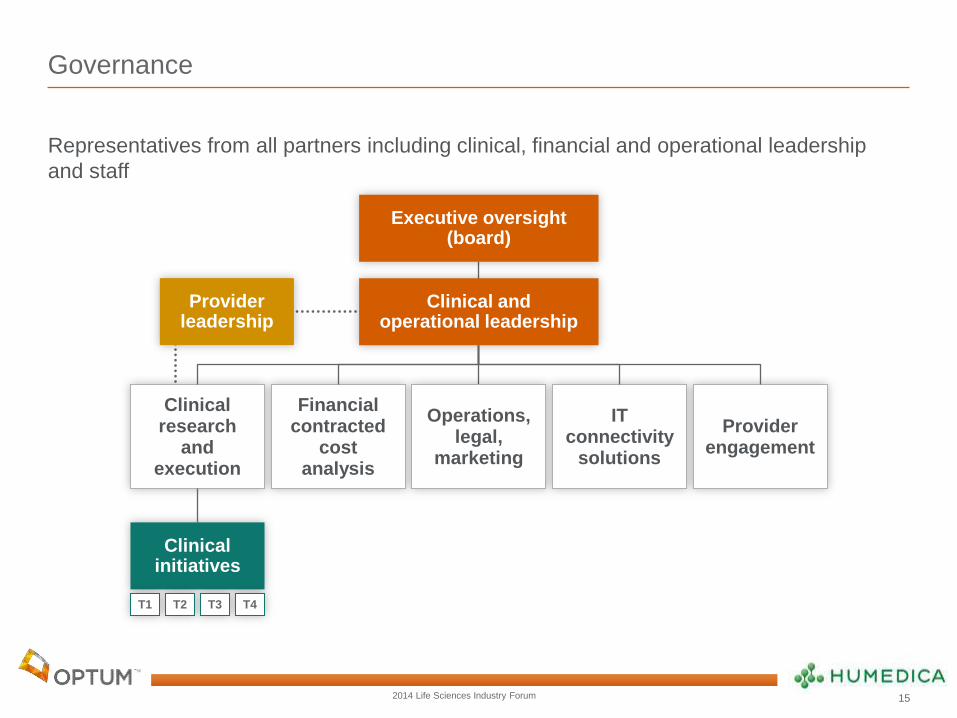
Governance
Representatives from all partners including clinical, financial and operational leadership
and staff
Executive oversight (board)
Clinical and operational leadership
Provider leadership
Clinical initiatives
Clinical research
and execution
IT connectivity
solutions
Operations, legal,
marketing
Financial contracted
cost analysis
Provider engagement
T1 T2 T3 T4
15
2014 Life Sciences Industry Forum 16
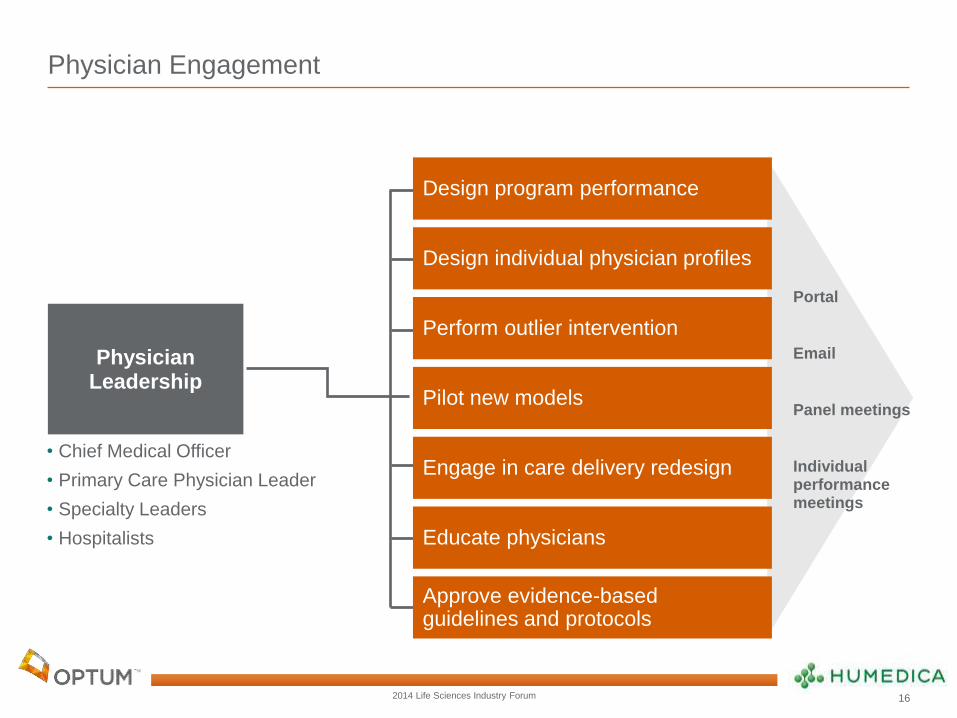
Physician Engagement
Portal
Panel meetings
Individual performance meetings
Design program performance
Design individual physician profiles
Perform outlier intervention
Pilot new models
Engage in care delivery redesign
Educate physicians
Approve evidence-based guidelines and protocols
Physician Leadership
• Chief Medical Officer
• Primary Care Physician Leader
• Specialty Leaders
• Hospitalists

2014 Life Sciences Industry Forum
Key opportunities in population health management
2012 medical claims cost distribution among 5.5 million commercial members using
Optum for Population Health Management services
Population medical costs are largely from treatment of chronic conditions in the
ambulatory setting.
17

2014 Life Sciences Industry Forum
Invest new capital
With expert financial and clinical predictive analytics as your enabler, patient risk now
becomes an opportunity to manage health and drive down costs.
Financial & Clinical Analytics
To predict the future medical
experience of individual health
consumers and defined populations
Population Health Management
To identify, engage, and impact
every individual with a health need
within a defined population
18
2014 Life Sciences Industry Forum
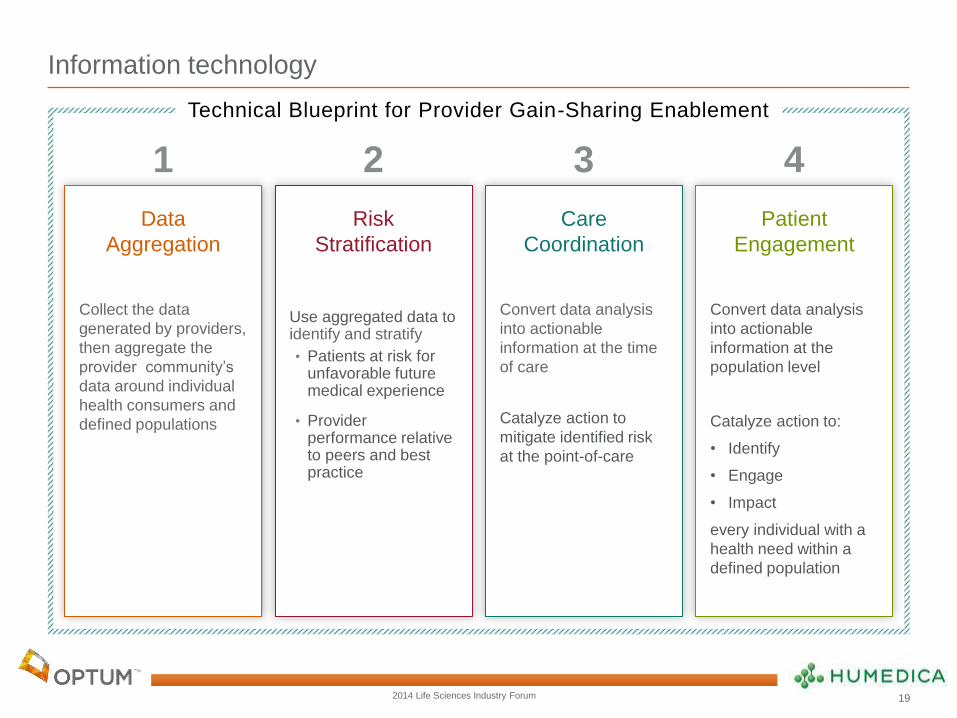
Information technology
Technical Blueprint for Provider Gain-Sharing Enablement
Data
Aggregation
Collect the data
generated by providers,
then aggregate the
provider community’s
data around individual
health consumers and
defined populations
Risk
Stratification
Use aggregated data to identify and stratify
• Patients at risk for unfavorable future medical experience
• Provider performance relative to peers and best practice
Care
Coordination
Convert data analysis
into actionable
information at the time
of care
Catalyze action to
mitigate identified risk
at the point-of-care
Patient
Engagement
Convert data analysis
into actionable
information at the
population level
Catalyze action to:
• Identify
• Engage
• Impact
every individual with a
health need within a
defined population
1 2 3 4
19
2014 Life Sciences Industry Forum
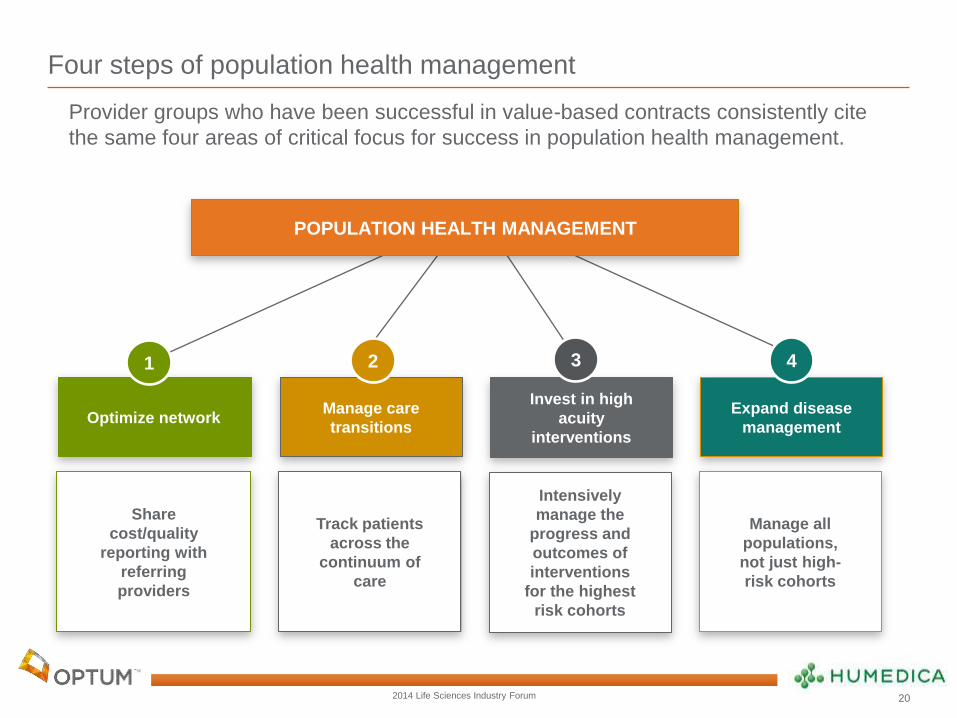
Four steps of population health management
Optimize network
Invest in high
acuity
interventions
Manage care
transitions
Expand disease
management
POPULATION HEALTH MANAGEMENT
1 2 3 4
Share
cost/quality
reporting with
referring
providers
Intensively
manage the
progress and
outcomes of
interventions
for the highest
risk cohorts
Track patients
across the
continuum of
care
Manage all
populations,
not just high-
risk cohorts
Provider groups who have been successful in value-based contracts consistently cite
the same four areas of critical focus for success in population health management.
20

2014 Life Sciences Industry Forum
Actionable information begins with the right data
Analytics to predict future medical costs of individuals and populations are limited by the characteristics of the types of available data:
Claims data Clinical data
Socio-demographic
and Care
Management data
– insensitive
– non-specific
– untimely
+ always available
+ sensitive
+ specific
+ timely
– variably available (may be
incomplete or
unstructured
in EMR, or unavailable
from non-EMR users)
+ sensitive
– non-specific
+ timely
+ generally available
21
2014 Life Sciences Industry Forum
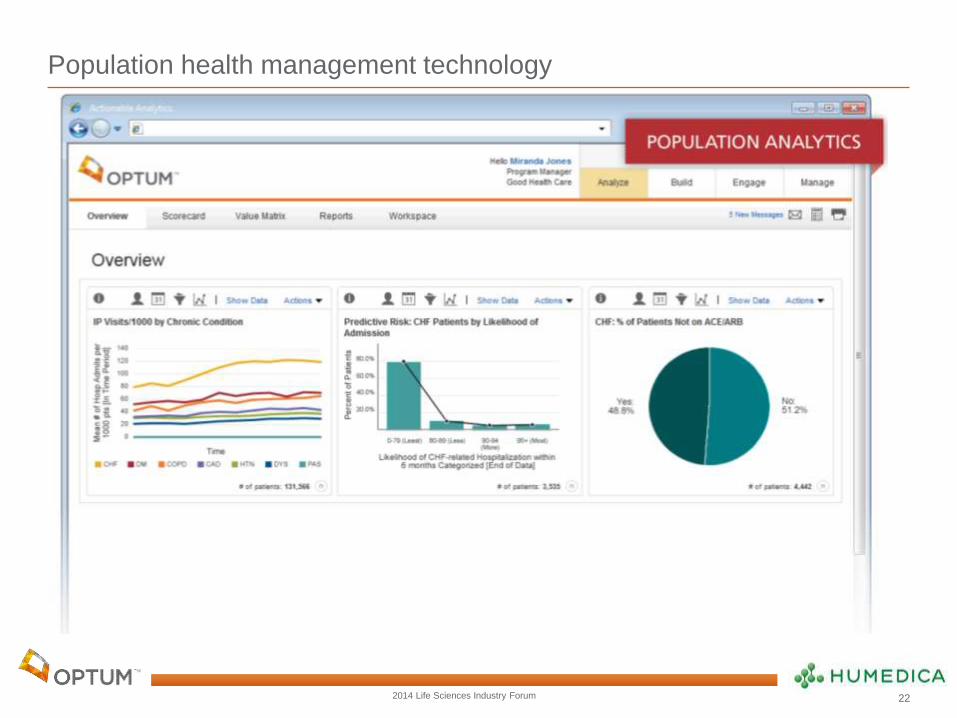
Population health management technology
22
2014 Life Sciences Industry Forum
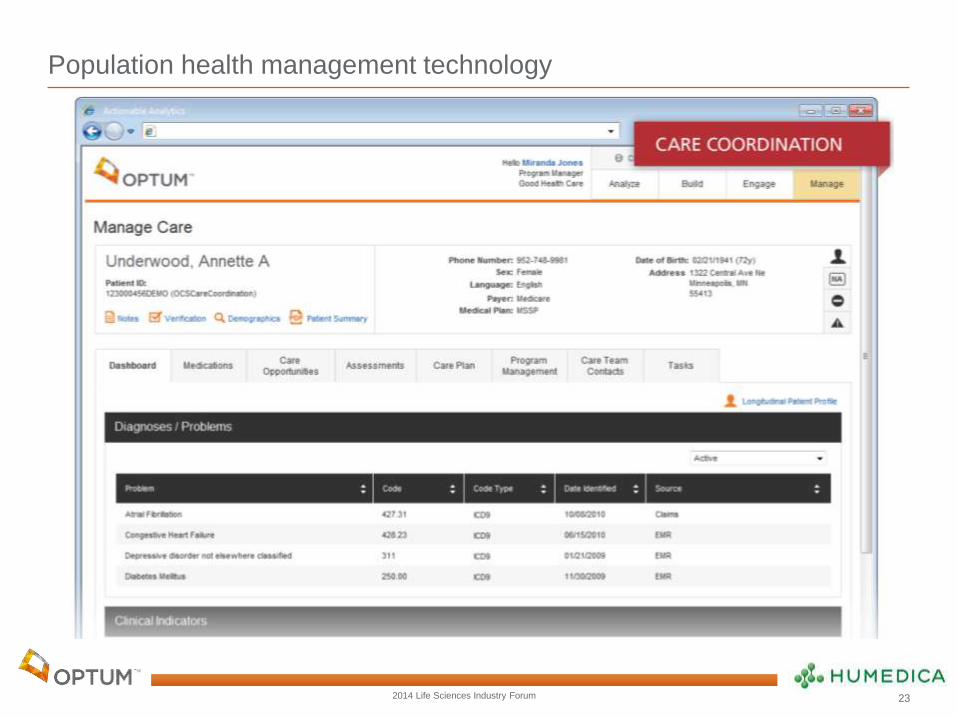
Population health management technology
23
2014 Life Sciences Industry Forum
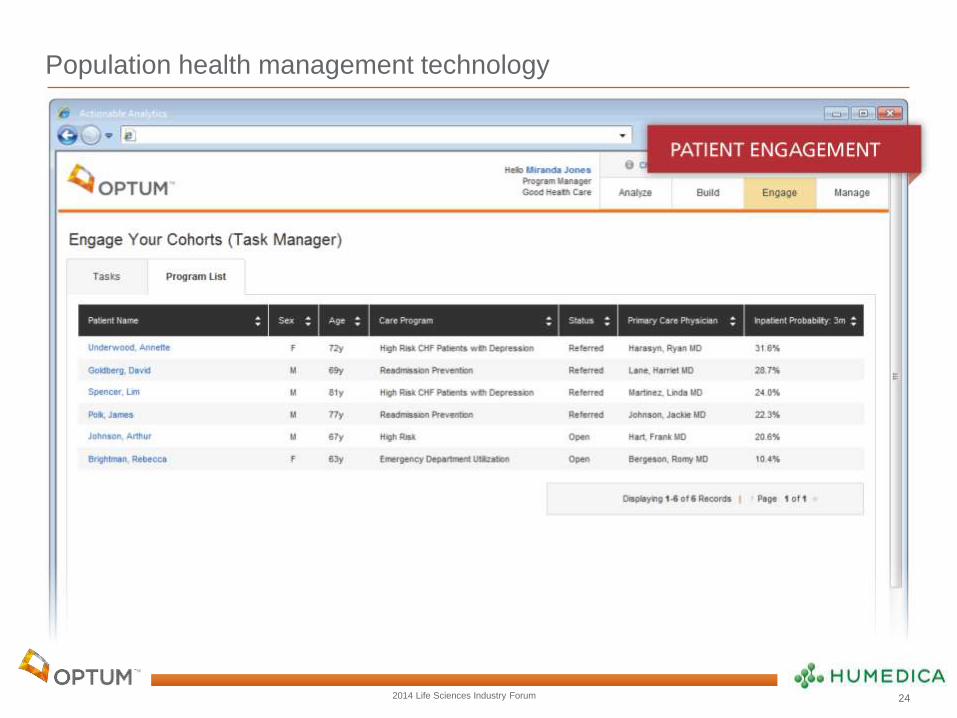
Population health management technology
24
2014 Life Sciences Industry Forum
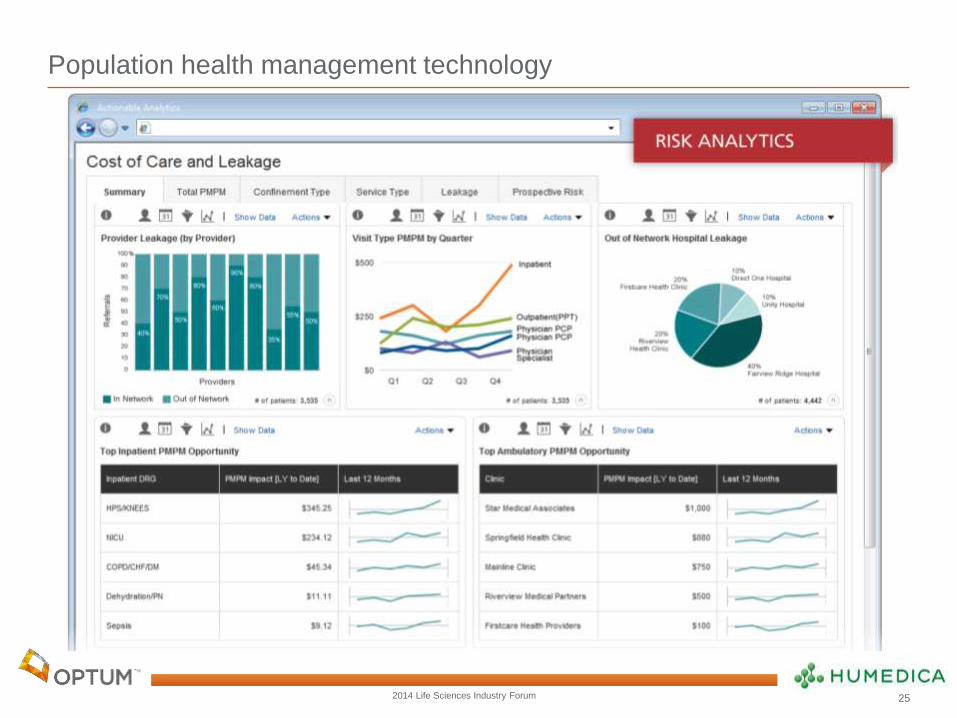
Population health management technology
25