pc giulianotti, md, facs robotic pancreatic surgery professor and chief division of general,...
TRANSCRIPT

PC Giulianotti, PC Giulianotti, MD, FACSMD, FACS
Robotic Pancreatic SurgeryRobotic Pancreatic Surgery
Professor and ChiefDivision of General, Minimally Invasive and Robotic Surgery
University of Illinois Medical Center at Chicago

Laparoscopic Pancreatic Surgery: Background
1994 Gagner M, Pomp A.Laparoscopic pylorus-preserving pancreatoduodenectomySurg Endosc 1994;8(5):408-10.
1994 Soper NJ et al.
Laparoscopic distal pancreatectomy in the porcine model
Surg Endosc 1994;8(1):57-60.
Robotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundLaparoscopic Pancreatic SurgeryLaparoscopic Pancreatic Surgery BackgroundsBackgrounds

Laparoscopic Pancreaticoduodenectomy: Background
Laparoscopic Whipple procedure is not only feasible but also safe, with low mortality and acceptable rates of complications.
146 procedures reported between 1994 and 2009
Morbidity: 16%Mortality: 1.3%Conversion Rate: 46% (12-100%)Fistula Rate: 7.5%
Laparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundLaparoscopic PancreaticoduodenectomyLaparoscopic PancreaticoduodenectomyBackgroundsBackgrounds
Laparoscopic Whipple procedure is not only feasible but also safe, with low mortality and acceptable rates of complications.
146 procedures reported between 1994 and 2009

Laparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundLaparoscopic PancreaticoduodenectomyLaparoscopic PancreaticoduodenectomyBackgroundsBackgrounds
Laparoscopic pancreaticoduodenectomy is feasible, safe, effective, and holds promise for providing advantages seen with minimally invasive approaches in other procedures.
54 totally laparoscopic procedures8 robot-assisted procedures
Morbidity: 41.9%Mortality: 1.6%Conversion Rate: 4.6%Fistula Rate: 17.7%
Laparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: background
Pancreas. 2009 Nov 12.Robotic and Laparoscopic Pancreaticoduodenectomy: A Hybrid Approach.Narula VK et al.
5 patientsLaparoscopic dissection
Robot-assisted reconstruction: pancreaticojejunostomy and choledocojejunostomy
Mean operative time: 420 minutes
Mean hospital stay: 9.6 days
At 6 months: all patients were disease-free.
Complex procedures such as PD can be accomplished with minimally invasive surgical techniques using robotic instrumentation.
Robotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyBackgroundsBackgrounds
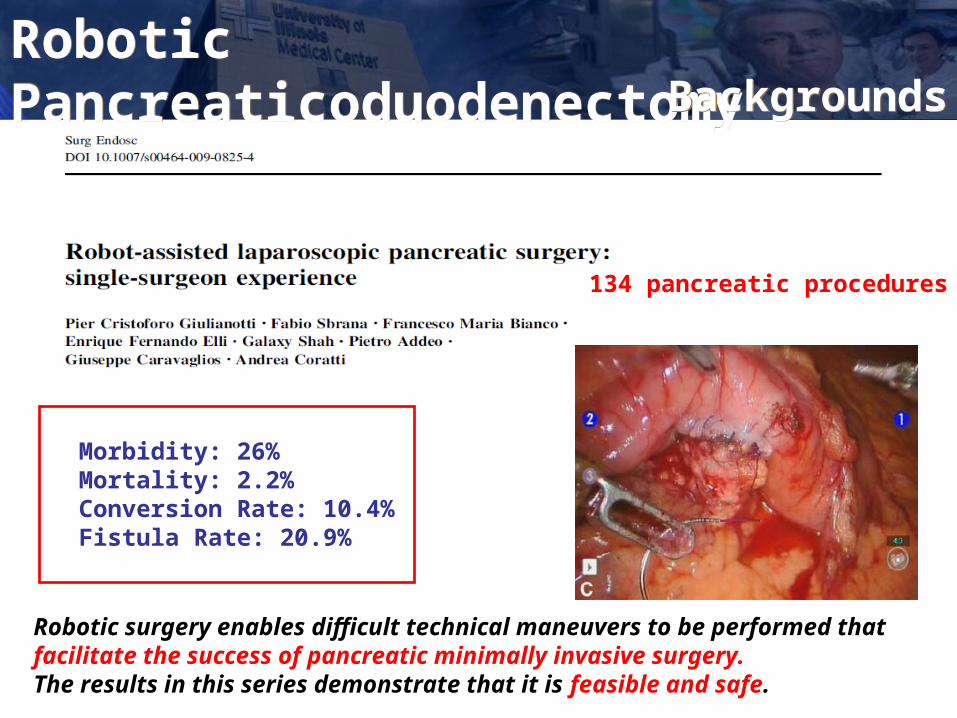
Robotic Pancreaticoduodenectomy
Robotic surgery enables difficult technical maneuvers to be performed that facilitate the success of pancreatic minimally invasive surgery. The results in this series demonstrate that it is feasible and safe.
134 pancreatic procedures
Morbidity: 26%Mortality: 2.2%Conversion Rate: 10.4%Fistula Rate: 20.9%
Laparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyBackgroundsBackgrounds
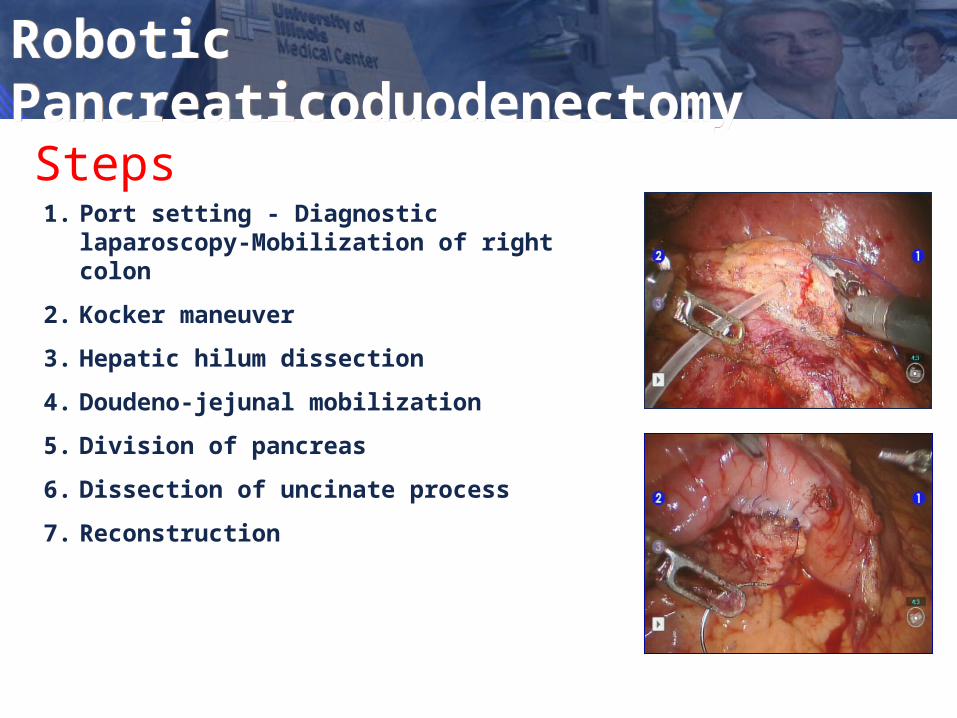
1. Port setting - Diagnostic laparoscopy-Mobilization of right colon
2. Kocker maneuver
3. Hepatic hilum dissection
4. Doudeno-jejunal mobilization
5. Division of pancreas
6. Dissection of uncinate process
7. Reconstruction
Steps
Robotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy
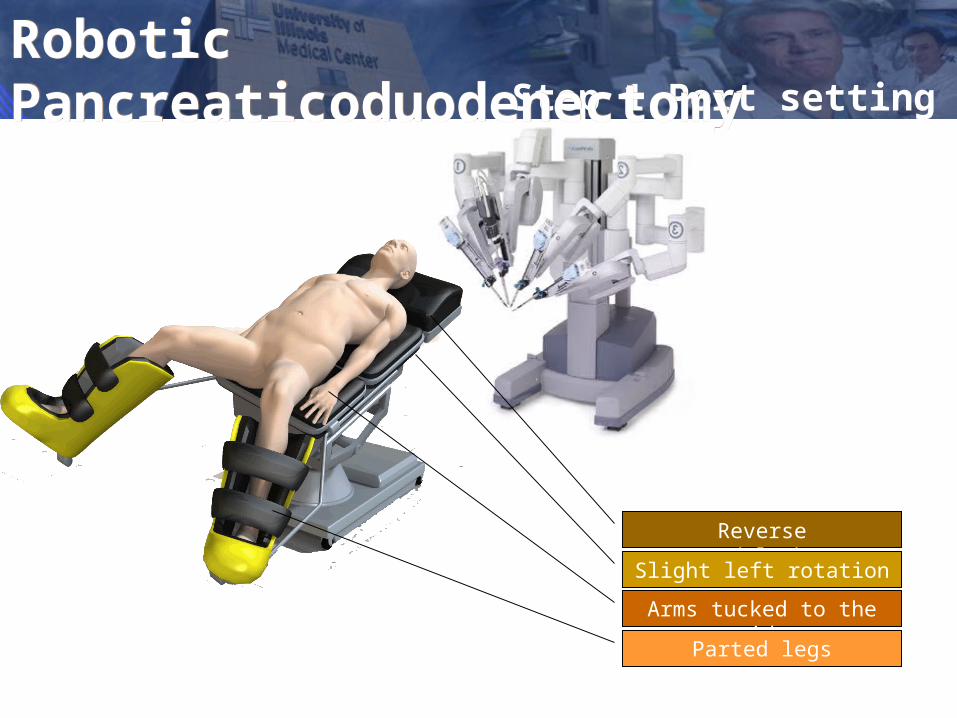
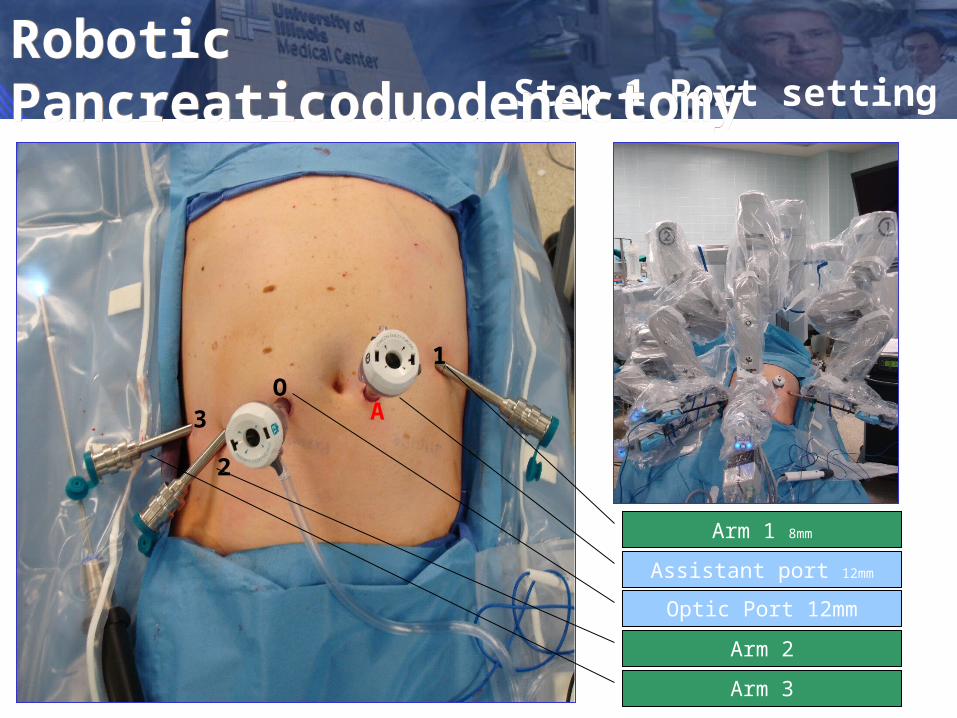
Step 1 Port setting
Reverse trendelemburg
Slight left rotation
Arms tucked to the side
Parted legs
Robotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy
A
2
3O
1
Step 1 Port setting
Arm 1 8mm
Assistant port 12mm
Optic Port 12mm
Arm 2
Arm 3
Robotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy

Step 2 Kocher Maneuver
Robotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy

Step 3 Hepatic HilumRobotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy
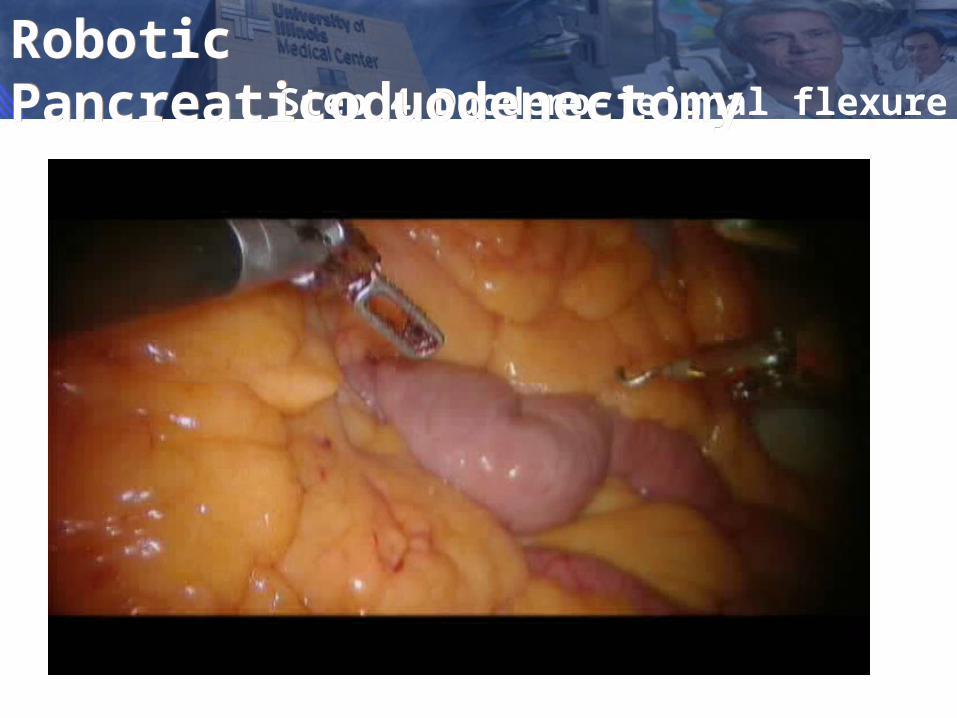
Step 4 Duodeno-jejunal flexure
Robotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy
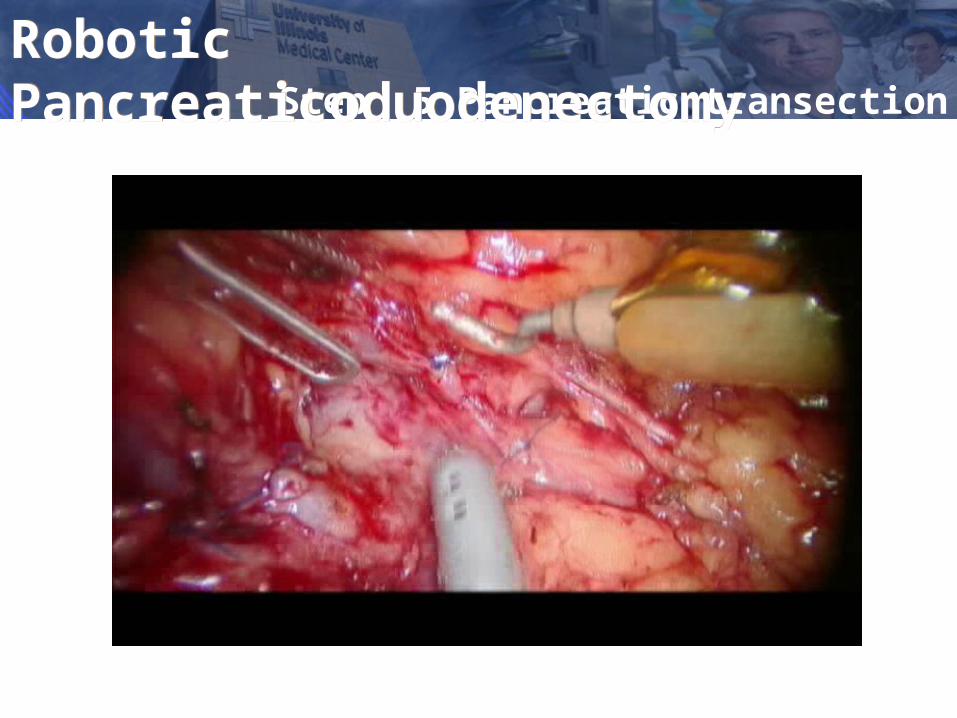
Step 5 Pancreatic transection
Robotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy

Robotic Pancreaticoduodenectomy
Uncinate Process Dissection
• The increasing retraction capabilities (IVth arm) combined with the stability of the system makes easier the exposure of the SMV and SMA
• Microsuturing makes easier and safer the control of bleeding.
• The stability of the system allows a better and selective delivery of energy (Harmonic)
Robotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyStep 6 Uncinate process
Robotic Pancreaticoduodenectomy
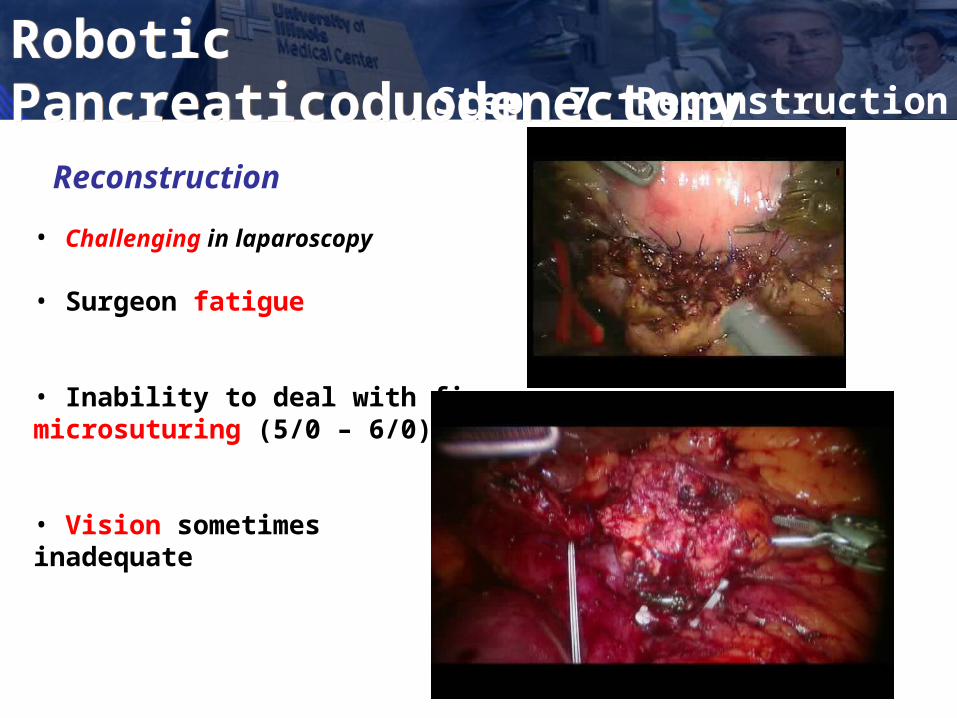
Reconstruction
• Challenging in laparoscopy • Surgeon fatigue
• Inability to deal with fine microsuturing (5/0 – 6/0)
• Vision sometimes inadequate
Robotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyStep 7 Reconstruction
Reconstruction: hepatico-jejunostomy
Robotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyStep 7 Reconstruction
Robotic Pancreaticoduodenectomy
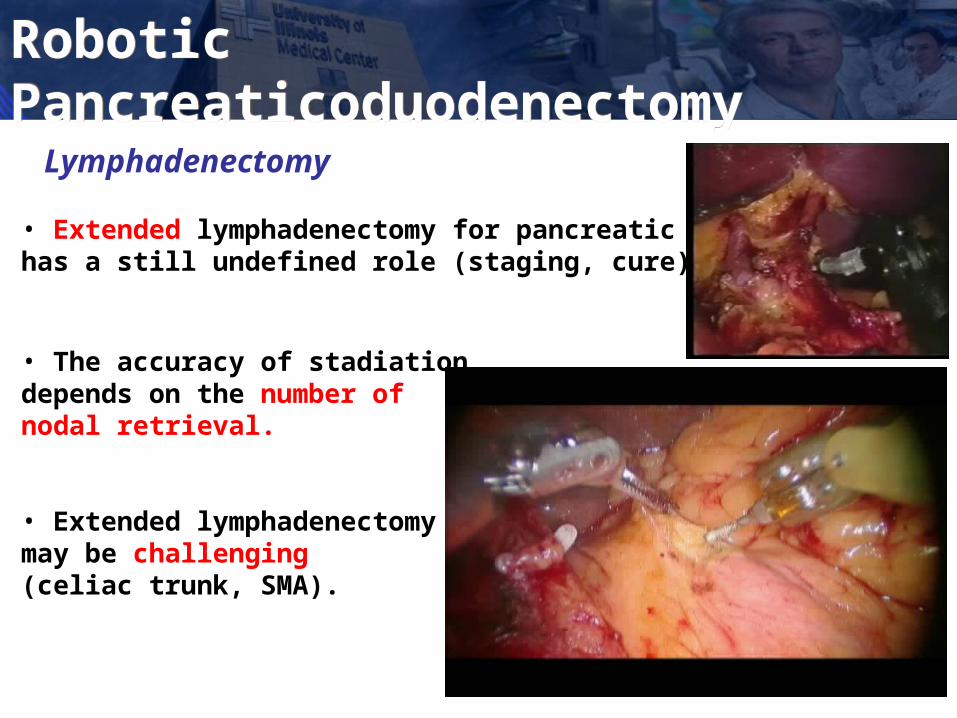
Lymphadenectomy
• Extended lymphadenectomy for pancreatic cancerhas a still undefined role (staging, cure).
• The accuracy of stadiation depends on the number of nodal retrieval.
• Extended lymphadenectomy may be challenging (celiac trunk, SMA).
Robotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy

Celiac trunk Lymphadenectomy
Robotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy
Lymphadenectomy: results
Nodes harvested: Average 19 (range: 12 - 27)
Gagner and Palermo
Systematic review of published laparoscopic pancreaticoduodenectomy
146 cases since 1994
Mean number of lymph nodes in the pathology was 19 (13–26).
Gagner et al. J Hepatobiliary Pancreat Surg 2009;16:726-30.
Robotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy
Robotic Pancreaticoduodenectomy
Personal Experience
87 Robotic Pancreaticoduodenectomies
PARAMETERS of US Series (49 patients)
Conversion rate: 4.1%Mean op. time: 444 minutes (range: 240-720)Transfusion: Postoperative: 22.2%Morbidity: 32.7% Mortality: 4.1% Fistula rate: 16.3%Mean Blood Loss: 387 mlLength of Stay: 13 days
Robotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic PancreaticoduodenectomyRobotic Pancreaticoduodenectomy
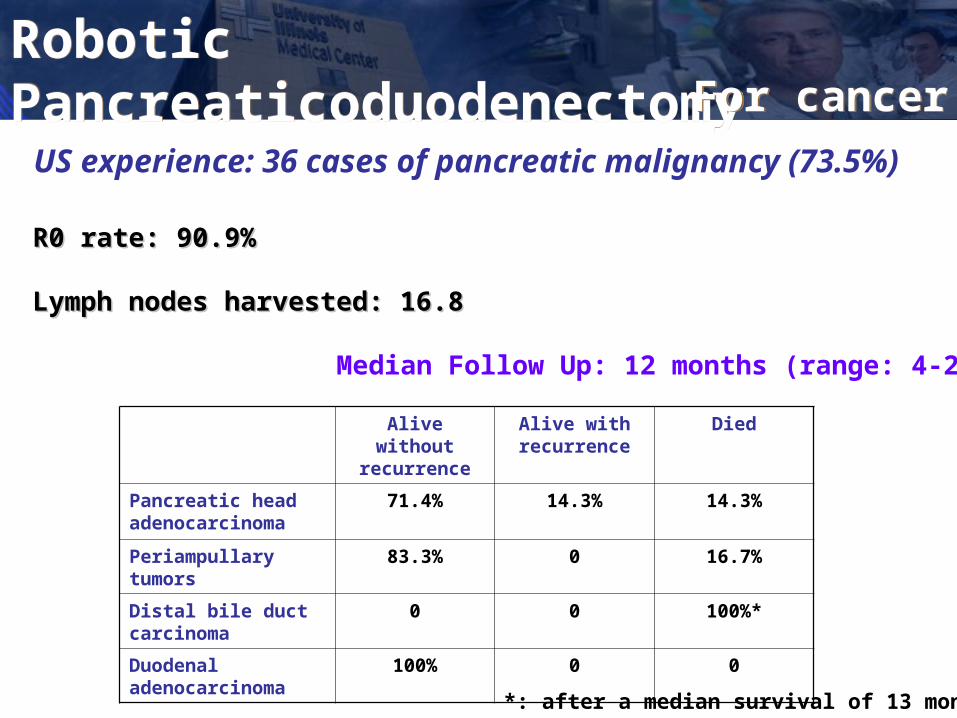
US experience: 36 cases of pancreatic malignancy (73.5%)
Median Follow Up: 12 months (range: 4-24)
Alive without recurrence
Alive with recurrence
Died
Pancreatic head adenocarcinoma
71.4% 14.3% 14.3%
Periampullary tumors 83.3% 0 16.7%
Distal bile duct carcinoma
0 0 100%*
Duodenal adenocarcinoma
100% 0 0
*: after a median survival of 13 months
R0 rate: 90.9%R0 rate: 90.9%
Lymph nodes harvested: 16.8 Lymph nodes harvested: 16.8
Robotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyFor cancerFor cancer

Technically challenging high percentage of unecessary splenectomies
Associated with longer operative times
Greater potential for bleeding
Pryor A et al.Laparoscopic distal pancreatectomy with spleen preservation.Surg Endosc 2007;21:2326-30.
By a laparoscopic approach
Laparoscopic distal pancreatectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundDistal PancreatectomyDistal Pancreatectomy
BackgroundsBackgrounds

Robotic distal pancreatectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic Distal PancreatectomyRobotic Distal Pancreatectomy
BackgroundsBackgrounds
Robotic distal pancreatectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic Distal PancreatectomyRobotic Distal Pancreatectomy
BackgroundsBackgrounds
32 open vs. 28 laparoscopic vs. 17 robotic distal pancreatectomies
Similar cost
Shorter hospital stay for the robotic group
Higher rate of spleen preserving cases in the robotic group
Increased operative time for the robotic approach

Robotic distal pancreatectomy
Personal experience
55 robotic distal pancreatectomies
PARAMETERS (US)
Conv. rate: 3.4%Mean op. time: 281 min (140-510)Transfusion: 10%Morbidity: 17.2%, 2 fistulaMortality: NO MORTALITYBlood loss: 240 ml (10-1000)Length of stay: 7 days (3-19)
Robotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic Distal PancreatectomyRobotic Distal Pancreatectomy
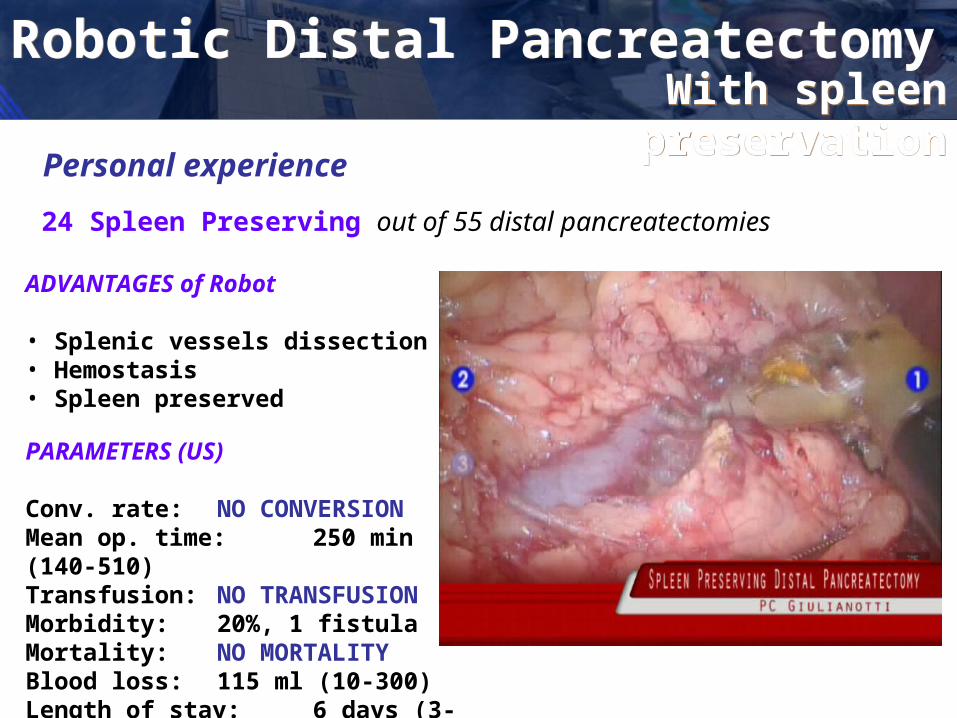
Robotic distal pancreatectomy with spleen preservation
Personal experience
24 Spleen Preserving out of 55 distal pancreatectomies
ADVANTAGES of Robot
• Splenic vessels dissection• Hemostasis• Spleen preserved
PARAMETERS (US)
Conv. rate: NO CONVERSIONMean op. time: 250 min (140-510)Transfusion: NO TRANSFUSIONMorbidity: 20%, 1 fistulaMortality: NO MORTALITYBlood loss: 115 ml (10-300)Length of stay: 6 days (3-13)
Robotic distal pancreatectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic Distal PancreatectomyRobotic Distal Pancreatectomy
With spleen preservationWith spleen
preservation
pancreatic malignancy (39.7%)
R0 rate: 87%R0 rate: 87%
Lymph nodes harvested: 16 Lymph nodes harvested: 16
Follow upFollow up
50% of patients are alive without recurrence at a mean FU of 51 months
33% are dead
Robotic distal pancreatectomy with spleen preservationRobotic distal pancreatectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic Distal PancreatectomyRobotic Distal Pancreatectomy
For cancerFor cancer
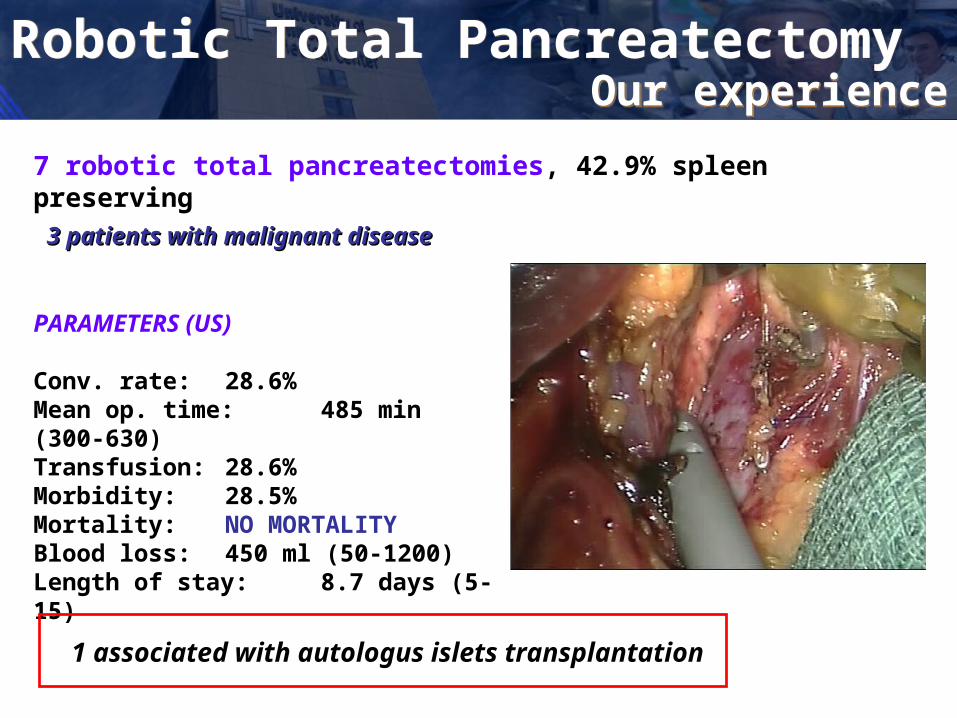
7 robotic total pancreatectomies, 42.9% spleen preserving
PARAMETERS (US)
Conv. rate: 28.6%Mean op. time: 485 min (300-630)Transfusion: 28.6% Morbidity: 28.5%Mortality: NO MORTALITYBlood loss: 450 ml (50-1200)Length of stay: 8.7 days (5-15)
1 associated with autologus islets transplantation
3 patients with malignant disease3 patients with malignant disease
Robotic distal pancreatectomy with spleen preservationRobotic distal pancreatectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyRobotic PancreaticoduodenectomyLaparoscopic Pancreaticoduodenectomy: BackgroundLaparoscopic Pancreatic Surgery: BackgroundRobotic Biliary Surgery: backgroundRobotic Liver Surgery: backgroundRobotic Total PancreatectomyRobotic Total Pancreatectomy
Our experienceOur experience

Personal experience
3 robotic middle pancreatectomies
No ConversionNo intra-operative transfusionNo morbidityNo mortality
Mean operative time: 245 minutes (240-255)
Pathology: 3 Cystadenomas
Giulianotti PC et al. J Laparoendosc Adv Surg Techn. In press
Robotic Middle PancreatectomyRobotic Middle Pancreatectomy
Vascular resection
Buchs NC et al. World J Gastroenterol 2010;16:818-31.
• One of the most important challenge in pancreatic surgery
• Surgical exploration remains the gold standard
• A recent review of the literature:
If an arterial invasion still remains a relative contra-indication, a venous invasion should not be considered as a contra-indication
A venous resection and reconstruction is feasible and reliable
But what about a minimally invasive vascular resection?
Robotic pancreatic surgeryRobotic pancreatic surgeryExtending the
limitsExtending the
limits
A technical challenge
A technical challenge
Robotic vascular resectionRobotic vascular resection
Our experienceOur experience in robotic vascular resection associated with pancreatic resection:
2 modified Appleby operations2 modified Appleby operations (splenopancreatectomy associated with celiac axis resection)
2 portal vein resections associated with pancreaticoduodenectomy2 portal vein resections associated with pancreaticoduodenectomy
1 portal vein resection associated with distal splenopancreatectomy1 portal vein resection associated with distal splenopancreatectomy
1 portal vein resection associated with a total pancreatectomy1 portal vein resection associated with a total pancreatectomy
Median age 60 years
Performed between May 2007 and December 2010

No Conversion
Mean operating time: 392 minutes (range: 310-460)
Mean Blood loss: 200 ml (range: 150-300)
No transfusion
No mortality
One reoperation for duodenal ulcer perforation
Hospital stay: 9.5 days
At a median FU of 6 months (range: 3-20): 4 patients alive and
disease-free
Robotic vascular resectionRobotic vascular resection A technical
challengeA technical
challenge
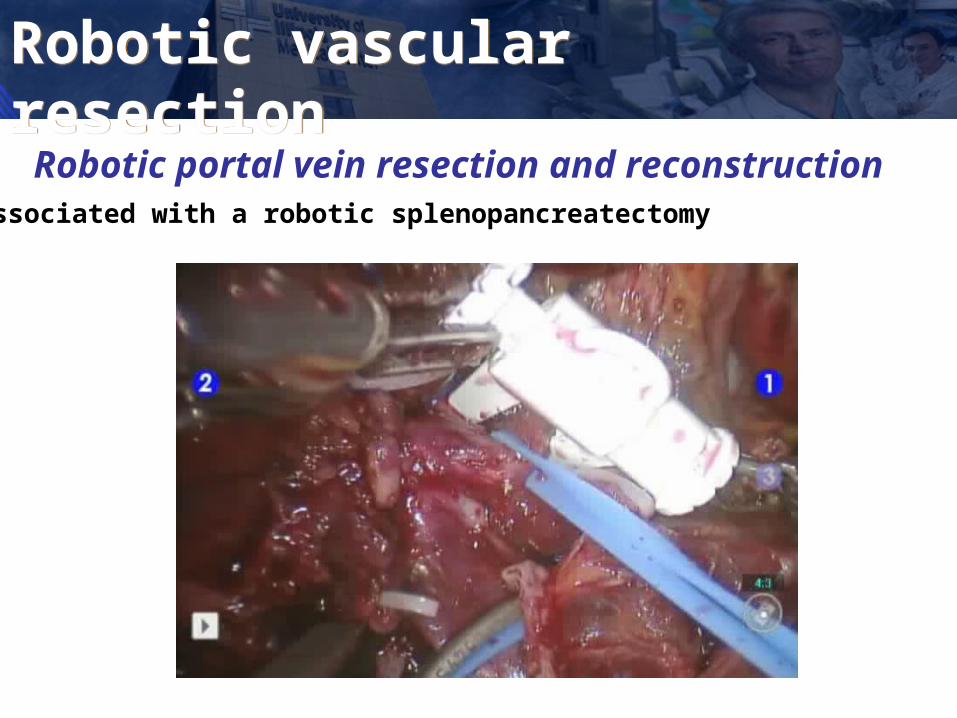
Robotic portal vein resection and reconstruction Associated with a robotic splenopancreatectomy
Robotic vascular resectionRobotic vascular resection

CONCLUSIONS
ROBOTIC TECHNOLOGY ALLOWS:
• Easiness dissection of the uncinate process
• High quality of tissue manipulation
• Safe reconstructive phase
• Easier microdissection and spleen preservation
Robotic pancreatic surgeryRobotic pancreatic surgery
CONCLUSIONS
• Minimally invasive pancreatic surgery still remains a big challenge.
• Robotic assistance overcome the limits of laparoscopy and is associated with lower blood losses and transfusion rate.
• Morbidity seems acceptable and lower than laparoscopy.
• Further randomized trials and longer follow up will be necessary to validate these results.
Robotic pancreatic surgeryRobotic pancreatic surgery

The Robotic Training LabThe Robotic Training LabThe Bruno and Tony Pasquinelli
Lab
Procedures performed at Procedures performed at UIC and offered for training UIC and offered for training include:include:• Splenectomy• Total gastrectomy• Lung lobectomy• Colorectal surgery• Thyroidectomy
• Adrenalectomy• Esophagectomy• Major hepatectomies• CBD Procedures• Whipple

The Robotic Training LabThe Robotic Training LabThe Bruno and Tony Pasquinelli
Lab
SimulationSimulation
Case observationCase observation
Hands onHands on