pcr vs. serology example mers how to interpret … · jan felix drexler souhaib aldabbagh sebastian...
TRANSCRIPT

Copyright: Marcel A. Müller
Dr. Marcel A. Müller
Institute of Virology
University of Bonn Medical Center Bonn, Germany
www.virology-bonn.de
January 20th, 2016
CONSISE Meeting Paris
PCR vs. Serology – example MERS
How to interpret results in
seroepidemiologic studies

Copyright: Marcel A. Müller
1. Reliable diagnostic tools available?
2. What kind of samples/ parameters should be
tested?
3. Optimal time points for testing?
Challenges in diagnostics

Copyright: Marcel A. Müller
Incre
ase
Vir
al
load
/ an
tib
od
yti
ter
Time post infection (days)
Incu
bati
on
tim
e
Virus
IgM
Antibody: IgG
10-143-10 180
Limit of
detection
Neutralizing IgG
(long time detection
and protection)
General virus infection
PCRSerology

Overview of MERS-CoV real-time PCR assays
Screening with upELimit: 3.4 RNA copies/reaction
Confirmation 1ALimit: 4.1 RNA copies/reaction
Amplification & Sequencing
Amplification & Sequencing
Features:
No cross-reactivity with clinical samples containing other respiratory viruses
No cross-reactivity with other hCoV isolates
Suitable for all known MERS-CoV isolates/sequences as of Dec 2015
Basis for development of commercial kits
Corman VM; Euro Surveill. 2012 Sep 27; Corman VM, Müller MA; Euro Surveill. 2012 Dec 6

Copyright: Marcel A. Müller
Incre
ase
Vir
al
load
/ an
tib
od
yti
ter
Time post infection (days)
Incu
bati
on
tim
e
Virus
IgM
Antibody: IgG
10-143-10 180
Limit of
detection
Neutralizing IgG
(long time detection
and protection)
Serology
PCRSerology

Copyright: Marcel A. Müller
Serodiagnostic assays
Recombinant IFA (rIFA)
Antigen: complete MERS Spike
Plaque Reduction Neutralization Test
Virus or Virus-like particle-based
ELISA
Antigens:
Recombinant S1 Spike Subdomain
Recombinant N protein
Inactivated virus
Virus immunofluorescence assay (vIFA)
Antigen: MERS-CoV

Copyright: Marcel A. Müller
Challenge: Vast diversity of coronaviruses
circulating in animals and human
Drexler et al., AVR 2014
MERS
SARS

Copyright: Marcel A. Müller
Human Coronaviruses
Name Genus Clinical picture
HCoV-229E Alpha
10% of all “Common Colds”
>90% of humans have IgG
HCoV-NL63 Alpha
HCoV-OC43 Beta
HCoV-HKU1 Beta
SARS-CoV Beta Severe acute respiratory syndrome
Diagnostic issue:
Cross-reactive antibodies in low serum dilutions

Copyright: Marcel A. Müller
Cross-reactivity CoV
Non-structural proteins (NSP)
CONSERVEDStructural proteins
VARIABLE
MERS-CoV
HCoV-OC43
HCoV-HKU1
HCoV-NL63

Copyright: Marcel A. Müller
Example: Non-specific reactivity in CoV
serodiagnostics (serum dilution 1:100)
Negative
serum
Cross-reactive
serum
MERS patient
serum
Fu
llv
iru
s
IFA

Copyright: Marcel A. Müller
Differential serology
Recombinant spike-based IFA (rIFA)
VeroB4 +
Spike encoding plasmid
24h
fix (4% PFA)
permeabilize (acetone/methanol; 1:1)
stain (heat-inactivated patient serum)
spotting,
drying
6h
229E NL63 OC43 HKU1 SARS MERS
Transfection

Copyright: Marcel A. Müller
Non-specific reactivity in CoV serodiagnostics
Negative
serum
Cross-reactive
serum
MERS patient
serum
Fu
llv
iru
s
IFA
Reco
mb
inan
t
IFA
Buchholz/Müller et al., Eurosurveillance 2013
rIFA more specific!

Copyright: Marcel A. Müller
DifferentialrIFAassaysinMERS-S1ELISAreactivesera vIFA ELISA(Ratio) ELISAResult rIFA
SubjectID MERS MERSS1 MERSS1 229E HKU1 MERS NL63 OC43 SARS
3 neg. 0,278 reactive 320 neg. neg. 320 320 neg.
44 neg. 0,561 reactive neg. 320 neg. 320 320 neg.
94 neg. 0,207 reactive 320 320 neg. 320 >1000 neg.
161 neg. 0,269 reactive 320 320 neg. neg. >1000 neg.
174 neg. 0,182 reactive 320 320 neg. neg. >1000 neg.
185 10 0,182 reactive >1000 320 neg. 320 >1000 neg.
207 neg. 0,200 reactive 320 320 neg. 320 >1000 neg.
211 neg. 0,748 reactive 320 320 neg. 320 320 neg.
217 neg. 0,424 reactive 320 320 neg. 320 320 neg.
225 neg. 0,211 reactive 320 320 neg. 320 >1000 neg.
229 neg. 0,278 reactive neg. 320 neg. 320 320 neg.
249 neg. 0,517 reactive 320 320 neg. neg. >1000 neg.
From Drosten, NEJM 2014 (supplementary data)
Non-specific sera show high titers against
other HCoVs

Copyright: Marcel A. Müller
Goldstandard: Plaque Reduction-Neutralisation-Test
(PRNT)
1:160
1:20
1:20 1:40 1:80
Serum
1:2 1:2 1:2
1:20 1:40 1:80 1:160
50 PFU
Y
Y
Y
Y
No Infection No plaques
Infection Plaques
Y
Y
Y
Y
Neutralized
Y
Y
Y
Y
Not neutralized
1h

Copyright: Marcel A. Müller
Screening
Stage 1
Stage 2
Established staged serological testing
algorithm for camels and humans
S1 ELISA
S1 ELISA rIFA full S
S1 ELISA rIFA full S PRNT
Drosten et al. 2014, NEJM & Müller et al. 2015, Lancet ID
Testing dilution ELISA, vIFA
1:100
Starting dilution PRNT:
1:10
Cutoff PRNT50: 1:20
ELISA and vIFA commercial
rIFA and PRNT: in-house
vIFA
Testing dilution rIFA:
1:40

Copyright: Marcel A. Müller
1. Reliable diagnostic tools available?
2. What kind of samples/ parameters should
be tested?
3. Optimal time points for testing?
Challenges in diagnostics

Copyright: Marcel A. Müller
PCR: Which samples?
Corman et al., CID 2015
BAL, Sputum optimal for MERS detection
Lower resp. tract Upper resp. tract
VIR
AL
LO
AD
(lo
g c
op
ies
per
ml)
NO
. S
AM
PL
ES
93% pos. 47.6% pos.
Mean:
5.0x106
Mean
2.0x104
Low viral loadHigh viral load

Copyright: Marcel A. Müller
Other body compartments?
14.6% pos.
2.4% pos.
30.6% pos.
1.6x104
1.3x102
2.5x103
Corman et al., CID 2015

Copyright: Marcel A. Müller
Antibodies: IgM or IgG?
IgM
IgG
Corman et al., CID 2015
N=37 MERS patients
IgM and IgG increase is comparable
IgM higher risk of cross-reactivity
IgM indicates recent infection

Copyright: Marcel A. Müller
1. Reliable diagnostic tools available?
2. What kind of samples should be tested?
3. Optimal time points for testing?
Challenges in diagnostics

Copyright: Marcel A. Müller
Time point for PCR testing
Corman et al., CID 2015
High viral loads up to 15 days post diagnosis
VIR
AL
LO
AD
(lo
g c
op
ies
per
ml)
NO
. S
AM
PL
ES
93% pos.
Mean:
5.0x106
High viral load

Copyright: Marcel A. Müller
3-6 years
Incre
ase
Vir
al
load
/ an
tib
od
yti
ter
Time post infection (days)
Incu
bati
on
tim
e
Virus
105 180
Limit of
detection
Summary: MERS-CoV infection and
diagnostics
PCRSerology
PCR: up to day 15 post diagnosis high viral loads
(>10e6 copies per ml) approx. 25 days post infection
20 90

Copyright: Marcel A. Müller
3-6 years
Incre
ase
Vir
al
load
/ an
tib
od
yti
ter
Time post infection (days)
Incu
bati
on
tim
e
IgM
IgG
105 180
Limit of
detection
Neutralizing IgG
Summary: MERS-CoV infection and
diagnostics
PCRSerology
Reinfection
possible?
Serology: IgM, IgG increase simultaneously approx 9
days post onset of symptoms
20 90

Copyright: Marcel A. Müller
Application & Interpretation
1. Identification of the source of infection
2. Clinical/ Outbreak investigations
3. Cross-sectional studies
4. Case-contact studies

Copyright: Marcel A. Müller
1. Source: Livestock screening
MERS-CoV antibodies in dromedaries
Reusken/Haagmans/Müller et al. Lancet ID, 2013
Mohamed Abdiwahab/AFP/Getty Images
SE
RO
LO
GY

Copyright: Marcel A. Müller
Young camels as source of infection
Wernery et al. EID 2015
SerumantibodyELISA
RNA detection RT-PCR (%)
Virus isolation
Adults, >4 yrs 298/310 (96.1) 0/250 (0) 0/12 (0)
Subadults, 2–4 yrs 328/340 (96.5) 10/344 (2.9) 1/14 (7.1)
Calves, <1 yr 92/108 (85.2) 24/68 (35.3) 6/44 (13.6)
Young camels < 1 year virus-positive!
SE
RO
LO
GY
+P
CR

Copyright: Marcel A. Müller
Long-term and widespread circulation of
MERS-CoV in dromedaries
1983/84 Sudan/Somalia
Müller et al. EID 2014
1992-96Saudi Arabia
Alagaili et al.mBio 2014
2009/10Saudi Arabia
Alagaili et al.mBio 2014
1997Egypt
Müller et al.EID 2014
2003UAE
Meyer et al. EID 2014
2013UAE/Oman/
Egypt/ Jordan
Meyer et al. EID 2014Reusken TLID 2013Chu et al. EID 2013Reusken et al.Euro Surv 2013Perera et al.Euro Surv 2013
1992Kenya
Corman et al EID 2014
2010/11Ethiopia/ Nigeria
Reusken et al.EID 2014
2009Tunisia
Reusken et al.EID 2014
Red=Africa
Black=Arabian Peninsula
SE
RO
LO
GY
+P
CR

Copyright: Marcel A. Müller
MERS-CoV originates from Africa
Nigeria
Egypt
Arabian
Peninsula
Korea
First human isolate
Egypt
PC
R

Copyright: Marcel A. Müller
2. Outbreak: Jeddah April 2014
PCR diagnostic laboratory artifact? NO CONTAMINATION
Increase of zoonotic transmission?
Mutant Virus?
Drosten et al. 2014, CID
2014
PC
R

Copyright: Marcel A. Müller
Monophyly of Jeddah outbreak viruses
Jed
dah
Single introduction of virus in Jeddah outbreak
7 full-length genomes
Jeddah viruses monophyletic
Drosten et al. 2014, CID
PC
R

Copyright: Marcel A. Müller
Diagnostic laboratory artifact? NO CONTAMINATION
Increase of zoonotic transmission? NO
Mutant Virus?
Drosten et al. 2014, CID
2014
PC
R

Copyright: Marcel A. MüllerDrosten, Muth, Corman, Hussain et al., CID 2014
No hints toward
changes in shedding
from patients
No relevant / unique
changes in spike
ALIGNMENT OF SEQUENCES
PC
R

Copyright: Marcel A. Müller
Nosocomial outbreak in Jeddah
Nosocomial infections starting at
King Fahd Hospital
Drosten et al. 2014, CID

Copyright: Marcel A. Müller
Tested >10,000 serum samples from all 13 provinces
3. Cross-sectional serosurvey in
Saudi Arabia
Müller et al. 2015, Lancet ID
SE
RO
LO
GY
AGE RANGE

Copyright: Marcel A. Müller
Screening 152 (1.5%)
Stage 1 17 (0.2%)
Stage 2 15 (0.2%)
Results cross-sectional study
S1 ELISA
S1 ELISA rIFA full S
S1 ELISA rIFA full S PRNT
Total N=10,009
Müller et al. 2015, Lancet ID
SE
RO
LO
GY

Copyright: Marcel A. Müller
Müller et al. 2015, Lancet ID
-15/10,009 (0.15%) in 6/13
provinces had MERS
antibodies (asymptomatic!)
-up to 23-fold increase in
camel-exposed individuals
Seroprevalence in Saudi Arabia
Copyright: Marcel A. Müller
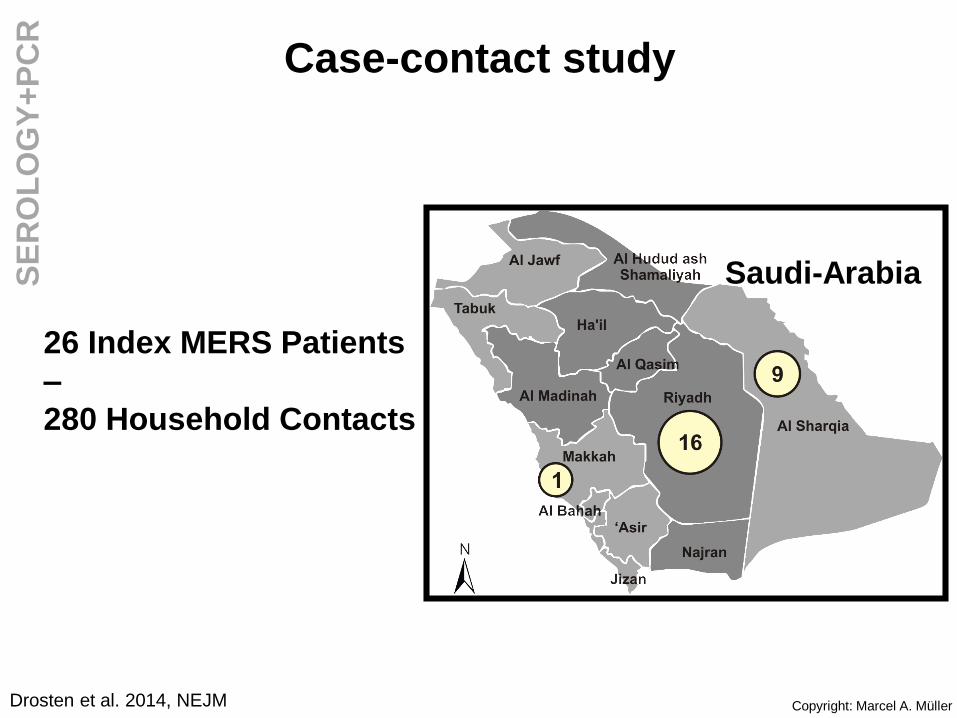
Saudi-Arabia
26 Index MERS Patients
–
280 Household Contacts
Drosten et al. 2014, NEJM
Case-contact studyS
ER
OL
OG
Y+
PC
R

Copyright: Marcel A. MüllerDrosten, New England Journal of Medicine 2014
26 MERS Patients
RT-PCR
7 positive
280 Contacts
Serology
5 positive
12 transmissions in
26 households, max 1 transmission per
householdR < 0.5

Copyright: Marcel A. Müller
Overview/ Summary
Study PCR Serology
1. Source -Identify virus and putative mutations-Phylogenetic analyses-Monitor acute infection in animals
-Largescale screening of livestock-Retrospective detection-Infection dynamics in livestock
2. Outbreak -Identify virus and mutations-Phylogenetic analyses-Monitor patients and contacts-Quarantine decision making-Prognostic value (e.g. viral load andoutcome of disease)
-Identify asymptomatic cases, contacts (e.g. HCW)-Retrospective control ofquarantine success-Prognostic value (antibody kineticsand outcome of disease)
3. Cross-sectionalserosurvey
Not applicable -Largescale screening of human sera for „background“ seroprevalence-Seasonality
4. Case-contact -Identify acutely infected contacts-Quarantine decision making-R0 value estimates
-Identify unrecognized(asymptomatic) contacts-R0 value estimates

Copyright: Marcel A. Müller
Open questions
R0<1
Young camels
as amplifiers
Hospital
outbreaks„Silent“
transmissions
MERS-CoV a common cold virus for
camels! Why?
Has camel MERS-CoV evolved towards
better transmissibility? Look at diversity of
camel-associated MERS-CoV in Africa, old
respiratory samples needed!
Influence of husbandry, farming?
Seasonality? Parturition differences
between African countries and Arabian
Peninsula!
Are there human cases in Africa? Lack of
testing, predispositions, co-morbidities?
MERS: Why 2012? Only on the Arabian Peninsula?

Copyright: Marcel A. Müller
Intervention?
Hygiene
In hospitals, ER
Avoid contact with (young)
camels
Vaccination
MVA-based vaccine:
Phase 1 clinical trial
planned
Proof of principle
vaccination in camels
showed protection
(Haagmans et al Science
2015)Source: CDC und REUTERS/Faisal Al Nasser

Copyright: Marcel A. Müller
Capacity building/ workshops
First WHO-MERS diagnostic workshop in Dubai in 2015 organized
by WHO-EMRO, University of Bonn, MOH Dubai, CVRL and
University of Hong Kong
Increase awareness, improve quality

Copyright: Marcel A. Müller
a n t i gone
Bonn:
Victor Corman
Doreen Muth
Isabella Eckerle
Jan Felix Drexler
Souhaib Aldabbagh
Sebastian Brünink
Acknowledgments
Funding: BMBF (SARS), DFG
Africa, DFG SPP1596, EU grants
ANTIGONE, EVA, EMPERIE,
COMPARE, PREPARE, ZAPI
ERASMUS Rotterdam, NL
Bart Haagmans
Ron Fouchier
Ab Osterhaus
V. Raj Stalin
Chantal Reusken
Marion Koopmans
EUROIMMUN AG Lübeck
Erik Lattwein
Kai Fechner
Katja Steinhagen
Global Centre for Mass
Gatherings Medicine (GCMGM),
Ministry of Health, Riyadh, KSA
Malak Al-Masri
Abdulhafeez Turkestani
Raafat F Alhakeem
Abdullah M Assiri
Ziad A. Memish
Utrecht University
Berend-Jan Bosch
Huihui Mou
ILRI, Kenya
Jörg Jores
Mario Younan
National Vet Institute, Sweden
Set Bornstein
CVRL, UAE
Ulrich Wernery
All volunteers and
assistants for sampling
Müller lab:
Benjamin Meyer
Andrea Sieberg
Daniel Ritz
Daniela Niemeyer
Jan Papies
Eva-Maria Klein
Robert Wollny
Tasnim Suliman
Stephan Kallies
Ute Winke
John Hopkins Aramco Healthcare,
Dhahran, KSA
Jaffar A. Al-Tawfiq
Saudi Center for Disease
Control, Riyadh, KSA
Ali M. Albarrak
University of Edinburgh, UK
Paul WikramaratnaKing Abdulaziz Medical City
&Advisor Royal court,
Riyadh, KSA
A A Alrabeeah
National Health Laboratory,
Riyadh, KSA
Ali M. Al-Shangiti
Head:
Christian Drosten