pediatric & adolescent gynecology fellow university of ...c.ymcdn.com/sites/ · pdf...
TRANSCRIPT

4/3/2015
1
Veronica I. Alaniz, MD, MPH Pediatric & Adolescent Gynecology Fellow
University of Michigan
Utility of Ultrasound and MRI in Patients with Disorders of Sex Development Undergoing Prophylactic Gonadectomy Veronica I. Alaniz, MD, MPH, Melina Dendrinos, MD, Noam Smorgick-Rosenbaum, MD, Elisabeth H. Quint, MD
Disclosures
l My co-authors and I have no relevant financial or non-financial relationships to disclose.
Disorders of Sex Development (DSD)
l Defined as atypical development of chromosomal, gonadal, or anatomic sex l 46 XX DSD l 46 XY DSD l Sex Chromosome DSD
l Estimated incidence is 1 in 4,500 births [1]

4/3/2015
2
Prophylactic Gonadectomy
l Indicated for patients with Y chromosome material at risk for developing Germ Cell Tumors (GCTs) [5-7] l Premalignant: Gonadoblastoma (GB), intratubular germ cell
neoplasia (ITGCN) l Malignant: Dysgerminoma, seminoma, and non-seminoma
l Risk of GCT varies by degree of virilization, location of gonads, and DSD diagnosis
Germ Cell Tumor Risk DSD Diagnosis Estimated Tumor Risk [7,9]
Denys Drash Syndrome 40%
46 XY Gonadal Dysgenesis 30%
45 X/46 XY DSD 15-40%
17 β hydroxysteroid dehydrogenase deficiency
17%
Partial androgen insensitivity syndrome
15%
Ovotesticular DSD 2.6%
Complete androgen insensitivity syndrome
0.8%
High Risk
Intermediate Risk
Low Risk
Pre Operative Evaluation
l No standard diagnostic guidelines for patients undergoing prophylactic gonadectomy
l Unless gonads are easily palpated, imaging is performed to: l Evaluate for the presence and type of
Mullerian structures l Locate gonads l Identify any features concerning for malignant
transformation

4/3/2015
3
Study Objectives
1. To evaluate ultrasonography (US) and magnetic resonance imaging (MRI) in identifying gonads in patients with Disorders of Sex Development (DSD) undergoing prophylactic gonadectomy
2. To assess the capacity of pre-operative imaging to detect pre-malignant and malignant transformation
Methods
l Retrospective case series at tertiary care academic center
l Chart review of patients with relevant ICD-9 codes seen between January 1998 and August 2014
l Inclusion criteria: l Karyotype showing 46 XY or 45 X/46 XY l Unilateral or bilateral prophylactic gonadectomy l Pre operative MRI and/or ultrasound
l Exclusion criteria: l Incomplete records
Methods
l Data was abstracted from demographic facesheets, outpatient clinic visits, radiology reports, operative reports, and pathology reports
l Proportions were compared with a chi-square test with a statistical significance set at 0.05
l Institutional IRB approval was obtained
4/3/2015
4
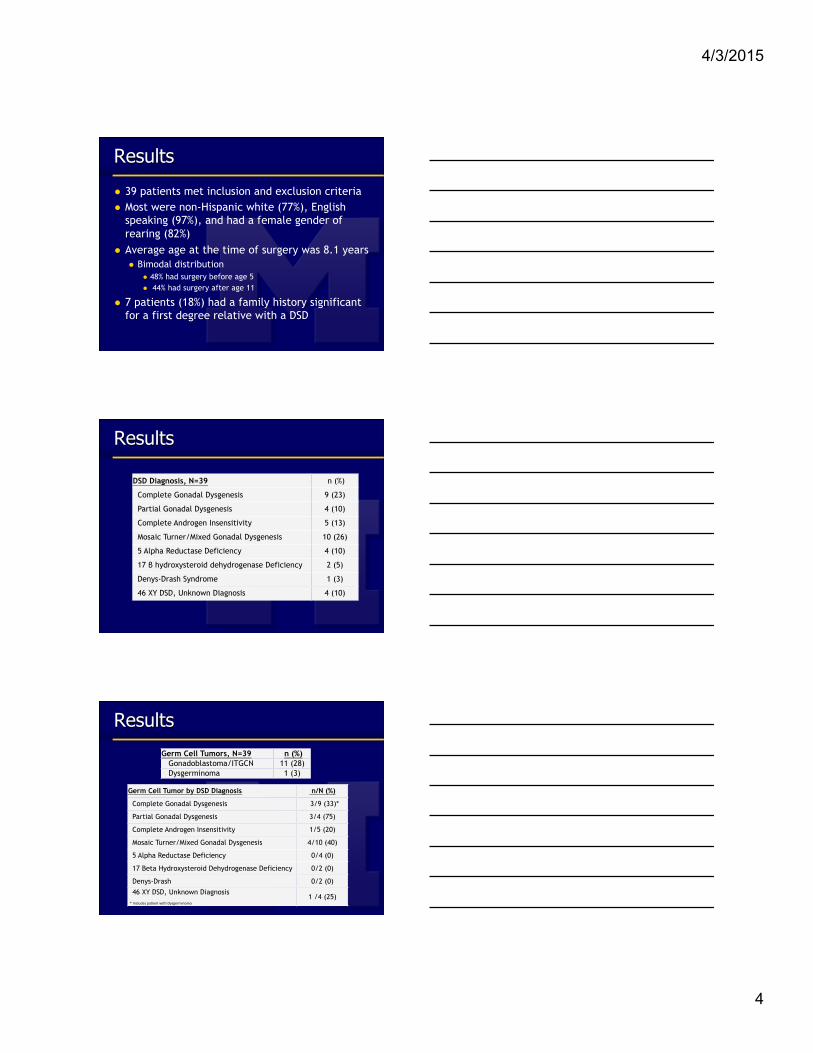
Results
l 39 patients met inclusion and exclusion criteria l Most were non-Hispanic white (77%), English
speaking (97%), and had a female gender of rearing (82%)
l Average age at the time of surgery was 8.1 years l Bimodal distribution
l 48% had surgery before age 5 l 44% had surgery after age 11
l 7 patients (18%) had a family history significant for a first degree relative with a DSD
Results
DSD Diagnosis, N=39 n (%)
Complete Gonadal Dysgenesis 9 (23)
Partial Gonadal Dysgenesis 4 (10)
Complete Androgen Insensitivity 5 (13)
Mosaic Turner/Mixed Gonadal Dysgenesis 10 (26)
5 Alpha Reductase Deficiency 4 (10)
17 β hydroxysteroid dehydrogenase Deficiency 2 (5)
Denys-Drash Syndrome 1 (3)
46 XY DSD, Unknown Diagnosis 4 (10)
Results
Germ Cell Tumors, N=39 n (%) Gonadoblastoma/ITGCN 11 (28) Dysgerminoma 1 (3)
Germ Cell Tumor by DSD Diagnosis n/N (%)
Complete Gonadal Dysgenesis 3/9 (33)*
Partial Gonadal Dysgenesis 3/4 (75)
Complete Androgen Insensitivity 1/5 (20)
Mosaic Turner/Mixed Gonadal Dysgenesis 4/10 (40)
5 Alpha Reductase Deficiency 0/4 (0)
17 Beta Hydroxysteroid Dehydrogenase Deficiency 0/2 (0)
Denys-Drash 0/2 (0) 46 XY DSD, Unknown Diagnosis * Includes pa-ent with Dysgerminoma
1 /4 (25)

4/3/2015
5
Study Objective #1
l Evaluate ultrasonography and magnetic resonance imaging (MRI) in identifying gonads in patients with Disorders of Sex Development (DSD) undergoing prophylactic gonadectomy
Results
l 33 patients had pre operative ultrasound l 35 out of 65 gonads (54%) were identified
l 14 patients had pre operative MRI l 11 out of 27 gonads (41%) were identified
l *No significant difference between imaging modalities in identification of gonads (p=0.25)
Results
US US
MRI
MRI
0% 10% 20% 30% 40% 50% 60% 70% 80%
Dysgenetic Testes
Gonads Identified by Imaging Modality and Gonad Type
*
* indicates statistical significance

4/3/2015
6
Study Objective #2
l Assess the capacity of pre-operative imaging to detect pre-malignant and malignant transformation.
Results
l Pre-malignant lesions (gonadoblastoma and ITGCN) were diagnosed in 28% of patients l There were no distinguishing characteristics
documented on pre-operative imaging
l Dysgerminoma was diagnosed in one patient (2.5%) l Described as an ovary with “normal size and
echotexture” on both ultrasound and MRI
Streak Gonad vs Dysgerminoma
4/3/2015
7
Results
l No significant difference in pre-malignant gonadal tumors among those gonads that were visualized versus non-visualized on both ultrasound (17 % vs 23 %, p=0.57) and MRI (9% vs 25%, p=0.62)
Conclusions
l Both ultrasound and MRI were limited in identifying gonads l Ultrasound better at identifying dysgenetic gonads
l Pre-malignant lesions were not identified on either imaging modality
l The dysgerminoma was mistaken for a normal ovary in a patient expected to have streak gonads
Clinical Implications
l Ultrasound should be considered as the first line imaging modality in DSD patients undergoing prophylactic gonadectomy
l Because pre malignant lesions cannot be identified on imaging, surveillance of gonads in patients with DSD at low risk for GCT (such as CAIS) is controversial
4/3/2015
8
STRENGTHS AND LIMITATIONS
l Strengths l Thorough chart review l Adds to limited available data
l Weaknesses l Small heterogeneous patient group l Retrospective study
Special thanks to: Elisabeth Quint Emily Kobernik
Previous PAG fellows
Questions?
References l 1. Hughes, I.A., et al., Consensus statement on management of intersex disorders. J Pediatr Urol, 2006. 2(3): p.
148-62. l 2. Gomez-Lobo, V., Multidisciplinary care for individuals with disorders of sex development. Curr Opin Obstet
Gynecol, 2014. 26(5): p. 366-71. l 3. Moran, M.E. and K. Karkazis, Developing a multidisciplinary team for disorders of sex development: planning,
implementation, and operation tools for care providers. Adv Urol, 2012. 2012: p. 604135. l 4. Lee, P.A., A perspective on the approach to the intersex child born with genital ambiguity. J Pediatr Endocrinol
Metab, 2004. 17(2): p. 133-40. l 5. Ulbright, T.M. and R.H. Young, Gonadoblastoma and selected other aspects of gonadal pathology in young
patients with disorders of sex development. Semin Diagn Pathol, 2014. 31(5): p. 427-40. l 6. Pleskacova, J., et al., Tumor risk in disorders of sex development. Sex Dev, 2010. 4(4-5): p. 259-69. l 7. Cools, M., et al., Germ cell tumors in the intersex gonad: old paths, new directions, moving frontiers. Endocr Rev,
2006. 27(5): p. 468-84. l 8. Cools, M. and L.H. Looijenga, Tumor risk and clinical follow-up in patients with disorders of sex development.
Pediatr Endocrinol Rev, 2011. 9 Suppl 1: p. 519-24. l 9. Pleskacova, J., et al., Tumor risk in disorders of sex development. Sex Dev, 2010. 4(4-5): p. 259-69.