pediatric orthopedic diseases. categories congenital developmental neuromuscular metabolic acquired...
TRANSCRIPT

Pediatric Orthopedic Diseases
Categories• Congenital
• Developmental
• Neuromuscular
• Metabolic
• Acquired : inflammatory
infection
trauma
tumor
Mechanisms• Congenital.. Defect in the stage of
embryogenesis.
• Developmental.. Defect in the stage of
fetogenesis.
• Neuromuscular.. Upper or lower motor neuron
disease or different muscular pathologies.
• Metabolic .. Abnormality in different metabolic
lines in our bodies.

• Inflammatory..antigen antibody
reactions
• Infections.. Pyogenic spread
• Trauma.. Mechanical
forces….fractures
• Tumor..benign or malignant
General Problems
• Hip problems
• Angular deformities
• Foot problems
• Infections & Tumors
DDH• Predisposing factors - 5 F’s
• Female
• Family Hx. in 20 % of cases
• Frank breech birth
• First born
• Left side involvement
• Physical Exam
- Limited abduction of flexed hip( < 50-60%)
- Legs unequal in length
- Asymmetric fat folds in thigh
- Limp in the walking age child
- Trendelenburg sign: lurching toward affected
side

Clinical The artful approach is the secret of the exam
Ortolani test Limited Abduction
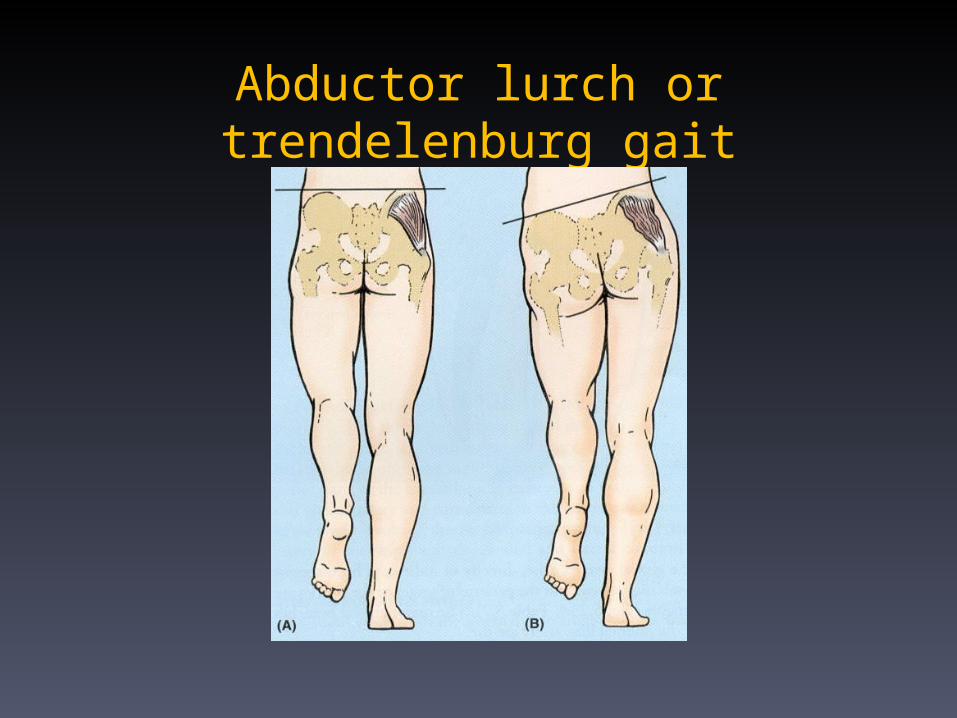
Abductor lurch or trendelenburg gait
• Diagnostic tests
• U/S in first few months to view
cartilage
• X-ray after 3 months


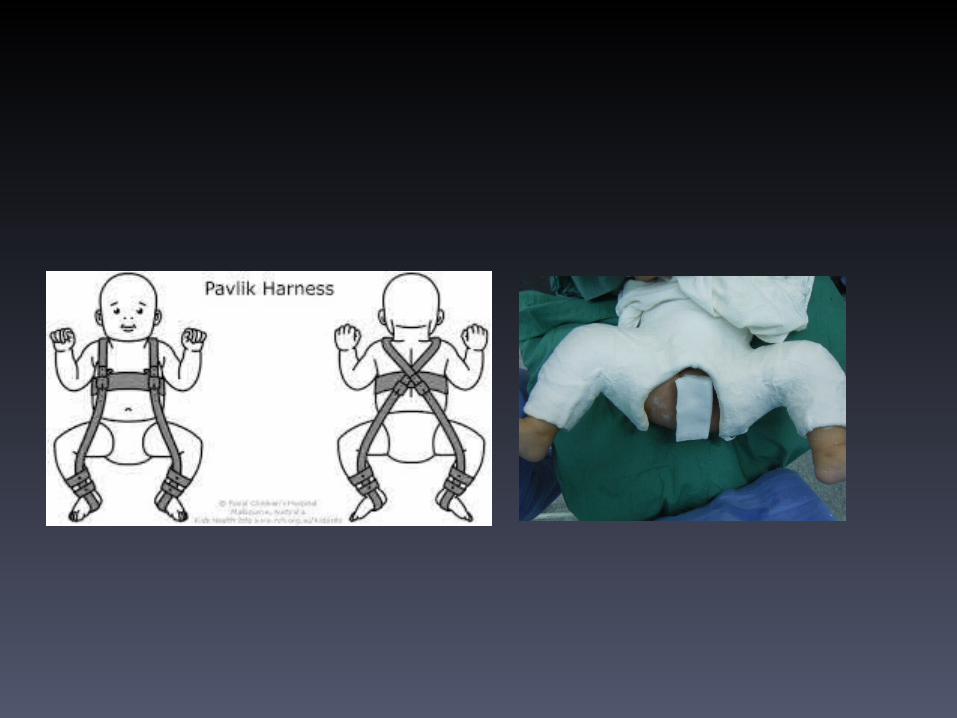
Treatment
• 0-6 months - Pavlik harness to maintain
abdution and flexion
• 6-18 months- reduction under GA, hip spica
cast for 2-3 months
• > 18 months- Open surgical reduction:
pelvic and/or femoral osteotomy
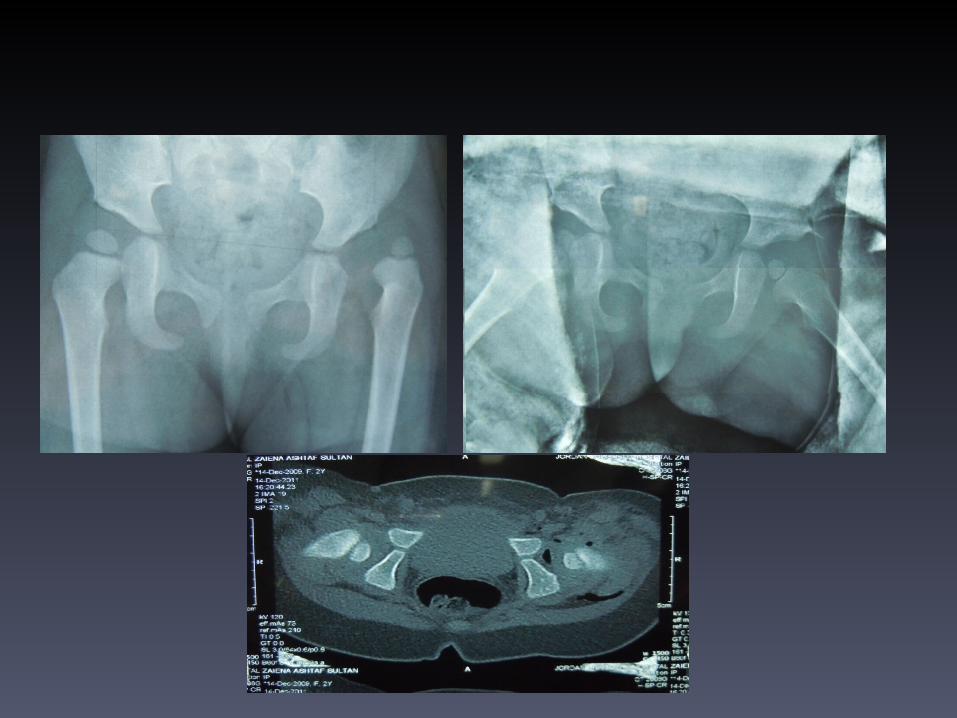

LEGG-CALVE-PERTHES DISEASE• AVN of proximal femoral epiphysis -
self limiting disease• Leads to abnormal growth of physis
followed by eventual remodeling of new bone
• Etiology unknown• More common in males 4:1 ratio
• History/Physical Exam
• Child 4-10 years
• Limping
• tenderness over anterior thigh
• Flexion contracture with decreased internal
rotation/abduction
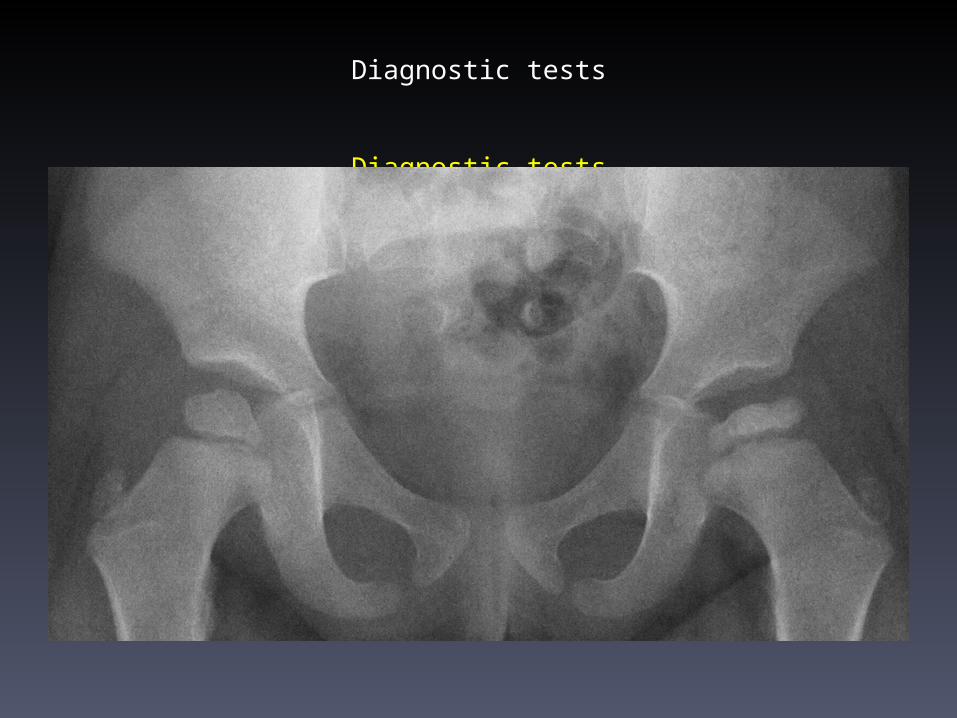
Diagnostic tests
Diagnostic tests

• Treatment : Aim CONTAINMENT
• Physiotherapy
• Brace in flexion/abduction x 2-3 years
• Femoral or pelvic osteotomy

SLIPPED CAPITAL FEMORAL EPIPHYSIS
• Epidemiology
- Occurs during maximal pubertal growth spurt
- Males: age 13 to 15- Females: age 11 to 13 - Most common adolescent hip disorder - Black race affected more often than white
race - Unilateral involvement in 90% of cases - Child is often overweight

SLIPPED CAPITAL FEMORAL EPIPHYSIS
Symptoms /Signs
-Hip pain or knee pain-Limp, decreased ROM-Hip held in abduction and external rotation - Markedly limited internal rotation


Management -Orthopedic Emergency!
Immediate
hospitalization
and operative
fixation
COMMON ANGULAR AND ROTATIONAL PEDIATRIC PROBLEMS
• Angular deformities of LL:-Bow legs.-Knock knees.
• Rotational deformities of LL:-In-toeing.-Ex-toeing.
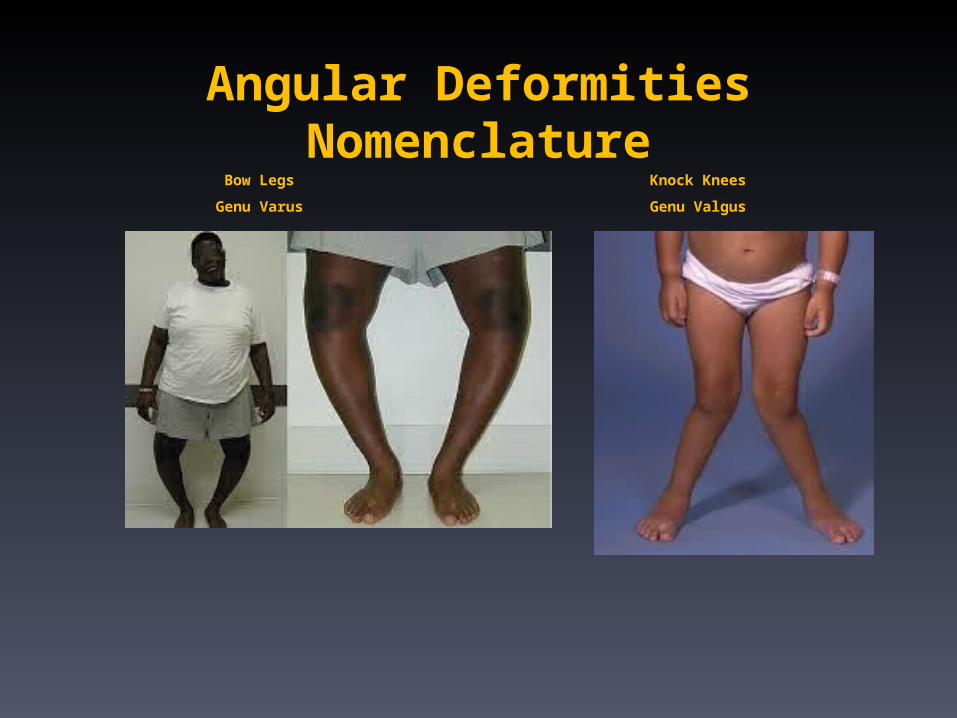
Angular DeformitiesNomenclature
Bow Legs
Genu Varus
Knock Knees
Genu Valgus
Angular DeformitiesEvaluation
Should differentiate between
physiologic and pathologicdeformities

Angular Deformities Evaluation
physiologic
• Symmetrical
• Mild – moderate
• Progressive
• Generalized
• Expected for age
pathologic
• Asymmetrical
• Severe
• Progressive
• Localised
• Not expected for age

Symmertrical Deformities
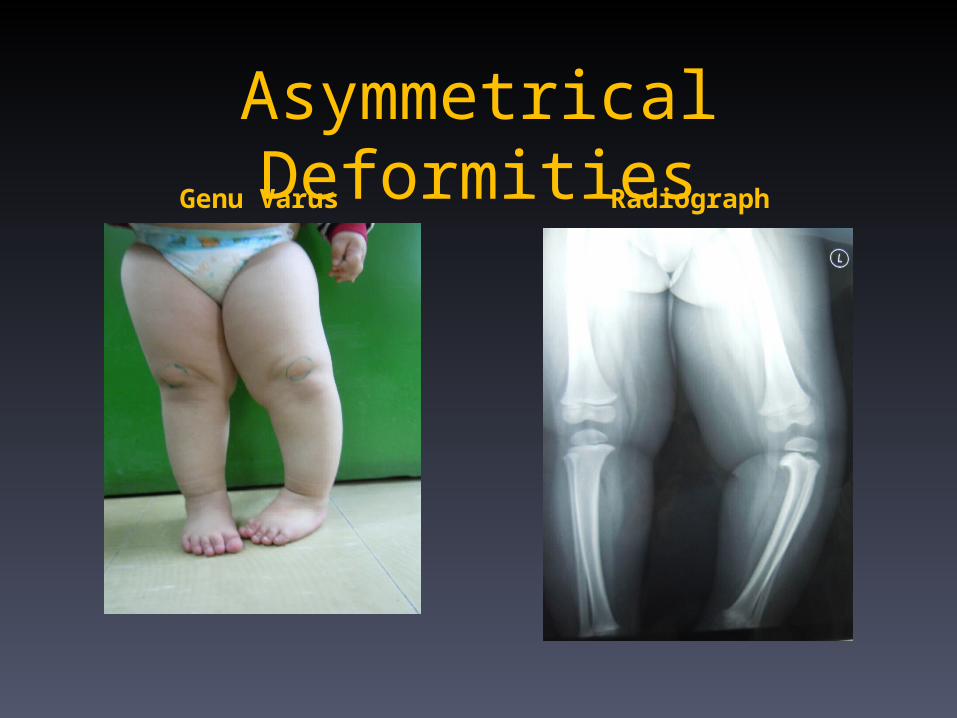
Asymmetrical DeformitiesGenu Varus Radiograph

Angular Deformities CausesPhysiologic
Normal for age
May be
exaggerated ??? :
a.Overwieght
b.Early walking
Pathologic
Rickets
Endocrinopathy
Metabolic diseases
Physeal plate injury :
a.Trauma
b. Infection
c. Tumor
Idiopathic
Evaluation• Investigations / Radiological
X-ray when severe or pathological
• Standing AP film
– long film ( hips to ankles ) with patellae directed
forwards
• Look for diseases :
– Rickets / Tibia vara (Blount’s) / Epiphyseal injury..
– Measure angles.

Angular Deformitieswhen to refer ?!!!!!!
• If Pathological
• Exaggerated physiological

TreatmentOsteotomy &
Fixation
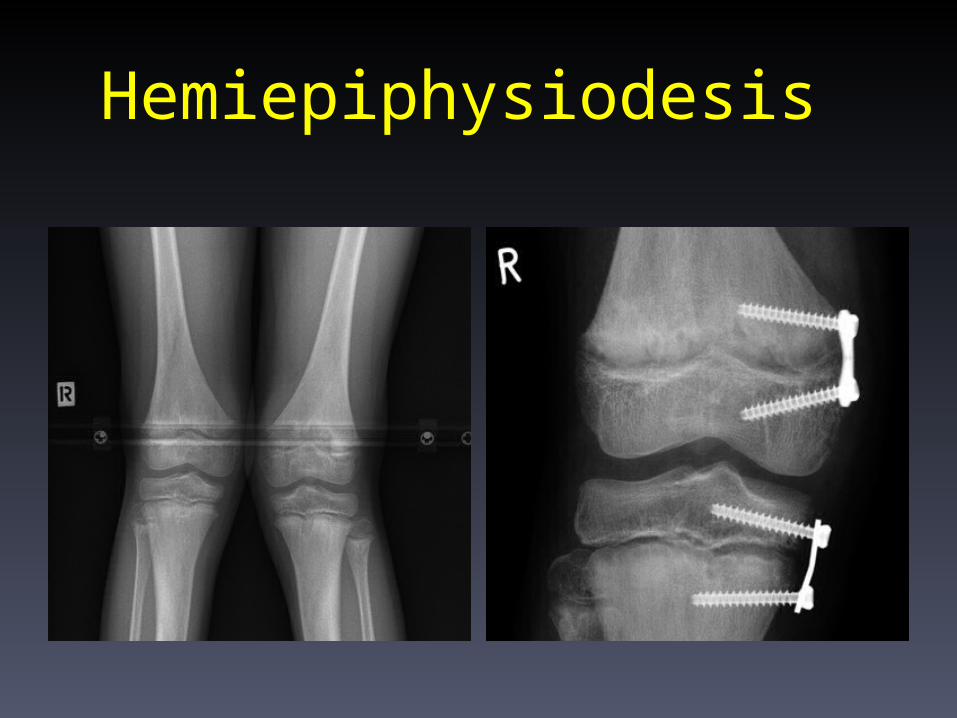
Hemiepiphysiodesis

Rotational Deformities
• INTOEING
Causes
• Metatarsus Adductus
• Tibial Torsion
• High femoral Anteversion

Metatarsus Adductus• A cause of intoeing in
the first year of life
• Rx :
stretching exercises
casting
surgery
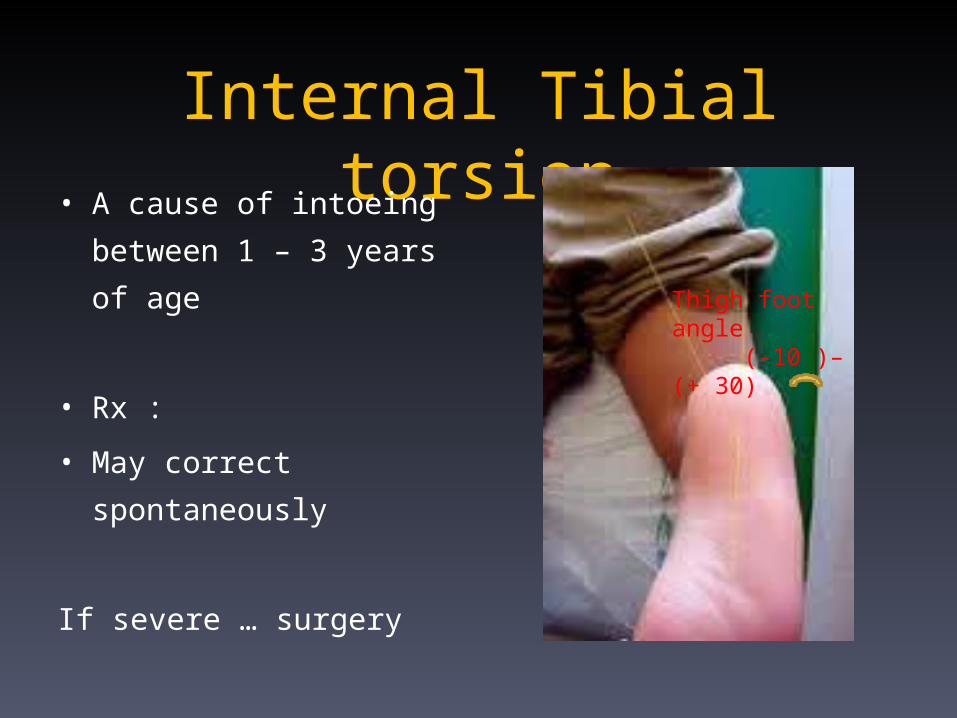
Internal Tibial torsion• A cause of intoeing
between 1 – 3 years of
age
• Rx :
• May correct
spontaneously
If severe … surgery
Thigh foot angle (-10 )– (+ 30)

High Femoral Anteversion• After 3 years of age
Rx: spontaneous
improvment till 10
years of age
NO functional
impairment
Surgery not indicated

EXTOEING
• External tibial torsion
Doesnot correct
spontaneously
If severe …surgery

Foot Deformities

Calcaneovalgus
• Common condition
• Packeging disorder
• Benign
• ???LLD in the
future
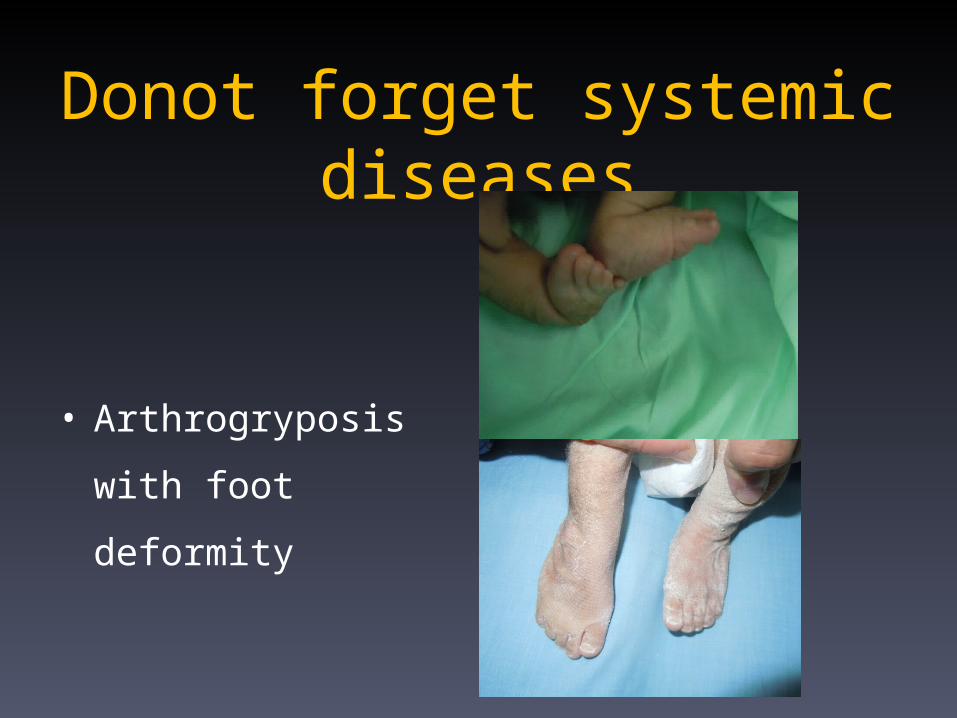
Donot forget systemic diseases
• Arthrogryposis
with foot deformity
SEPTIC ARTHRITIS
• Bacterial infection within a joint
• Serious medical emergency!
• Spread by direct extention , hematogenous(
most commonly), inoculation
• Organisms:- 0-6 months- S.aureus, E.Coli
- 6-36 months- S.aureus, H.influenza
- > 36 months- S.aureus, Streptococci

• History/Physical Exam- Severe pain
- Fever, chills
- Dehydration
- Lethargy
- Local redness, swelling, heat, tenderness
- Unable or unwilling to move joint - neonates get
pseudoparalysis
- Joint held in flexion

• Diagnostic tests
- Blood and throat cultures
- Joint aspirate for cultures
- CBC, WBC,
- Bone scan (for hip involvement only, to assess
for vascular compromise to femoral head)
SEPTIC ARTHRITIS
• Admit
• Rest the limb
• IV fluids for dehydration
• Analgesia
• Incision & Drainage
• IV antibiotics