pediatrics - 1 file download
TRANSCRIPT

Pediatrics ID 8820 APGAR SCORING
- 1st step once the baby is born - immediate newborn care involves - drying the infant, clearing the secretions from the mouth and nares, and providing warmth.
- APGAR scores - quick measure of neonates overall status and response to resuscitation. And usually done at 1 and 5 minutes. Follow up Apgar score at 5 minutes of life is helpful in assessing response to preliminary interventions.
- Normal APGAR score - 7-9 and requires no intervention. - Score < 7 - require further evaluation and resuscitation.
- Concerning aspects are irregular breathing and HR<100, hence pulse OX monitoring and PPV should be initiated according to the neonatal resuscitation algorithm. If the heart rate drops below 60, chest compressions should be performed.
- Maternal factors that increase the risk of resuscitation - Young maternal age - Hx of substance abuse - Hx of diabetes mellitus or HTN.
Note - Blue extremities and pink body is very common, benign, and can last for 1-2 days. In contrast, cyanosis of the face or central body should raise concern for hypoxia from respiratory or cardiac problems such as Congenital heart disease.
UW3 QID 6399 Caput Succedaneum versus cephalohematoma

Normal Milestones in 1st year of life
Normal milestones in 1- 5 years of life
Delayed Milestones UW 3 QID 5105 - DELAYED LANGUAGE DEVELOPMENT AT 2 Y/O AGE
- Delayed speech dev’t may indicates a hearing impairment. Thus, Hearing test is warranted as an initial evaluation, thus child should be referred for audiologic assessment.
- Other candidates that should be considered for hearing evaluation → children with a family hx of hereditary hearing loss, hx of meningitis, hx of recurrent or persistent otitis media with effusion > 3 months, documented intrauterine infections, craniofacial anomalies, and use of ototoxic meds (aminoglycoside)
UW 3 ID 6117 - SUSPECTED DEVELOPMENTAL DELAY - INITIAL EVALUATION
- Suspected language delay and mental retardation → initial evaluation - HnP - May provide important clues to the lead poisoning, microcephaly,
dysmorphic features - Sensory examination - including opthalmologic and audiometry testing, preferably
using brainstem evoked audiometry potential testing - Further evaluation may depend on the findings from HnP and sensory screening.
Q 4 ID 3721 Congenital Hypothyroidism Etiology Thyroid Dysgenesis - aplasia, hypoplasia, and ectopic gland(Most
common)- usually autosomal recessive pattern Clinical Manifestations
Majority of infants are asymptomatic Symptoms include lethargy, hoarse cry, poor feeding, constipation, jaundice, dry skin, large fontanelles
Diagnosis Increased TSH, decreased T4 levels Most infants are identified by newborn screening
Treatment Levothyroxine Q 21 ID 2423 - Neonatal Thyrotoxicosis Pathophysiology Transplacental passage of maternal Anti - TSH receptor antibodies
Abs bind to infants TSH receptors and cause excessive Thyroid hormone release
S/S Warm, moist skin Tachycardia Poor feeding, irritability and poor wt gain Low birth weight or preterm birth
Dx Maternal Anti -TSH receptor ABs >/= 500% normal Treatment Self Resolves within 3 months (Disappearance of maternal AB
Methimazole + Beta Blocker Neonates born to women with Anti-TSH receptor ABs > 5x the upper limit of normal are at greatest risk. ID 4890 - Jejunal Atresia - Bilious emesis, abdominal distension, and Abd Xray - tripple bubble sign and absence of gas anywhere in the colon, and maternal usage of vasocclusive meds or drugs such as

Cocaine or Tobacco - lead to atresia anywhere along the GI tract secondary to vascular accident in utero. - in contrast to Duodenal atresia, ileal and jejunal atresia are not associated with chromosomal abnormalities Treatment include - resuscitation, and stabilizing the pxt, followed by surgical correction. Q 31 ID 4787 Physiologic Leukorrhea - Know how to differentiate between pathologic and physiologic vaginal discharge. Pathologic Discharge Physiologic Discharge Hx of pruritus, burning, and malodorous vaginal discharge - edema, erythema, friability of vaginal mucosa, and green or curd like vaginal discharge
Copious vaginal discharge that is white or yellow in color, non malodorous, and occurs in the absence of other symptoms or findings of vaginal exam is physiologic Leukorrhea. RX - REASSURANCE.
Q 17 ID 4198 Complications of Shoulder Dystocia
Fractured Clavicle Clavicular crepitus/ bony irregularity Decreased moro reflex due to pain on Affected side Intact biceps and grasp reflexes
Fractured humerus Upper arm crepitus /bony irregularity Rest of the findins same as clavicular fracture
Erb-Duchenne Palsy(C5-C7) Decreased Moro and Biceps reflexes on affected side "Waiter's tip"
● extended elbow ● pronated forearm ● flexed wrist and fingers
Intact Grasp reflex
Klumpke Palsy (C8-T1/T2) "Claw Hand" ● Extended wrist ● hyperextended MCP joints ● Flexed IP joints ● Absent grasp reflex
Horner Syndrome (ptosis and miosis) Intact Moro and biceps reflex
Perinatal Asphyxia - usually results from compromised placental or pulmonary gas exchange- severe hypoxia --> poor perfusion and acidosis initially in peripheral tissues followed by the brain.
Variable presentation depending on duration of hypoxia Alt Mental status (e.g Irritability, lethargy), Respiratory or feeding difficulties, poor tone, seizure

Q30 ID 2572 FETAL HYDANTOIN SYNDROME Characteristics features - midfacial hypoplasia, microcephaly, cleft lip and palate, digital hypoplasia, hirsutism, and developmental delay. Most commonly associated meds - phenytoin and carbamezapine. Fetal Alcohol Syndrome -
- Classic Sign - Smooth philthrum - short palpebral fissures, thin vermillon border, midfacial hypoplasia, microcephaly, and
stunted growth. CNS damage include - hyperactivity, mental retardation, or learning disability.
Q 35 Id 3273 Congenital b/l rena agenesis Fetuses with b/l renal agenesis will not survive outside the uterus b/c of risk of severe pulmonary hypoplasia associated with renal agenesis. They will survive in utero b/c the placenta oxygenates the fetal blood and removes waste products from fetal circulation. In this case with preterm labor with rupture of membranes - spontaneous vaginal delivery should be allowed to proceed. Attempts to prolong pregnancy will not improve fetal mortality.
Q 37 ID 2575 Complications in DES daughters ● Clear cell adenocarcinoma of the vagina and cervix ● Structural anomalies of the reproductive tract (e.g. hooded cervix, T-shaped uterus, small
uterine cavity, vaginal septae, and vaginal adenosis) ● Pregnancy problems (e.g. ectopic pregnancy, pre-term delivery) ● infertility
Males Exposed in utero - are at risk of Cryptorchidism, microphallus, hypospadias, and testicular hypoplasia Congenital Muscular Torticollis id 4761 is the postural deformity of the neck Presentation - B/W age 1-6 months with neck mass and head tilt to one side with chin deviation to the other side. PE - neck with limited ROM, a palpable well circumscribed mass that does not transilluminate in the inferior portion of sternocleidomastoid muscle. RFs → intrauterine Positioning or crowding in the uterus e.g. Multiple gestation, breech positioning and oligohydramnios. Other conditions related to intrauterine positioning → DDH, metatarsus adductus, and clubfoot. Rx → 3P’s → Positioning (increased tummy time), Passive stretching, and Physical Therapy. Complication → Missed or delayed Dx can lead to craniofacial asymmetry - aka Positional Plagiocephaly i.e flattening of the head with ipsilateral anterior displacement of the ear and forehead. Limited ROM of the neck increases the risk of Positional Plagiocephaly. Cystic Hygromas → congenital malformation of lymphatic system and are commonly located in the posterior Triangle of the neck and have a high association with aneuploidy. Postnatal examination would reveal a fluctuant mass that would transilluminate.

Flexible versus Structural kyphosis ID 5541 - 5542 - UW3 - Flexible kyphosis →Physical examination shows a postural round back that is corrected by
voluntary hyperextension. - A common finding in adolescents, typically noticed by parents or teachers who observe
adolescents sitting or standing in a slouched position - On lateral radiographs, the angle of thoracic kyphosis is normal or slightly increased (normal
20-40 degree) - Rx→.easily correctable by voluntary effort and on prone-extension test.
Structural kyphosis aka Scheurmann disease - Not corrected with voluntary efforts. - A sharp angulation is commonly seen on forward bending (>40 degrees angle) - Mild to moderate kyphosis (<70-80 degree angle) → milwaukee brace and exercises to strengthen
the spine muscles - More severe cases → i.e. significant angulation, intractable pain and neurological abnormalities
→ treated surgically. Differentials:
1) Idiopathic scoliosis → characterized by lateral angulation of the spine that is observed on forward bending.
Q 3 ID 3688 Genetic disorders - miscellaneous systems Genetic Disorder
INHERITANCE MODE
GENE MUTATION
CHARACTERISTICS Complications
Marfan Syndrome
Autosomal Dominant
Fibrillin 1 gene Skeletal Fx- Joint hypermobility, skin hyperelasticity, long fingers(arachnodactyly - "thumb sign"), pectus excavatum, and Scoliosis/kyphosis Lens Dislocation (ectopia Lentis) and iridodonesis, and myopia (from elongation of the globe)
Aortic root dilatation - puts pxt at risk for thoracic aortic aneurysms- it requires close monitoring with Echo. 1st degree relatives should undergo genetic testing.
Homocystinuria
Autosomal Recessive
Cystathione synthase deficiency- enzyme involved in metabolism of methionine.
Pectus deformity, tall stature, and arachnodactyly, lens is dislocated downward,fair complexion and intellectual disability
Thromboembolic events
Ehler Danlos Syndrome
Collagen disorder
Scoliosis, joint laxity, and aortic dilation
ID 2439 Friedreich Ataxia (FA) Mode of inheritance Autosomal recessive - with extensive number of trinucleotide repeat
sequences → abnormality of a tocopherol transfer protein In families with one child affected , the subsequent risk of another child affected is 25% - genetic counselling is recommended for prenatal diagnosis for parents with one affected child.
CFx unsteady gait and weakness in the lower limbs wide based gait with constant shifting of position to maintain her balance decreased vibratory and position sense in the LE deformed feet with high plantar arches Cardiac arrythmia, CHF, contribute to a significant number of deaths
Diagnostic studies MRI - brain and spinal cord - atrophy of the cervical spinal cord and minimal cerebellar atrophy Nerve Conduction velocities are normal EKG - T-wave inversions in the inferior and lateral chest leads - myocarditis
prognosis very poor, pxts are wheelchair bound by age 25 and death occuring by 30-35 yrs of age
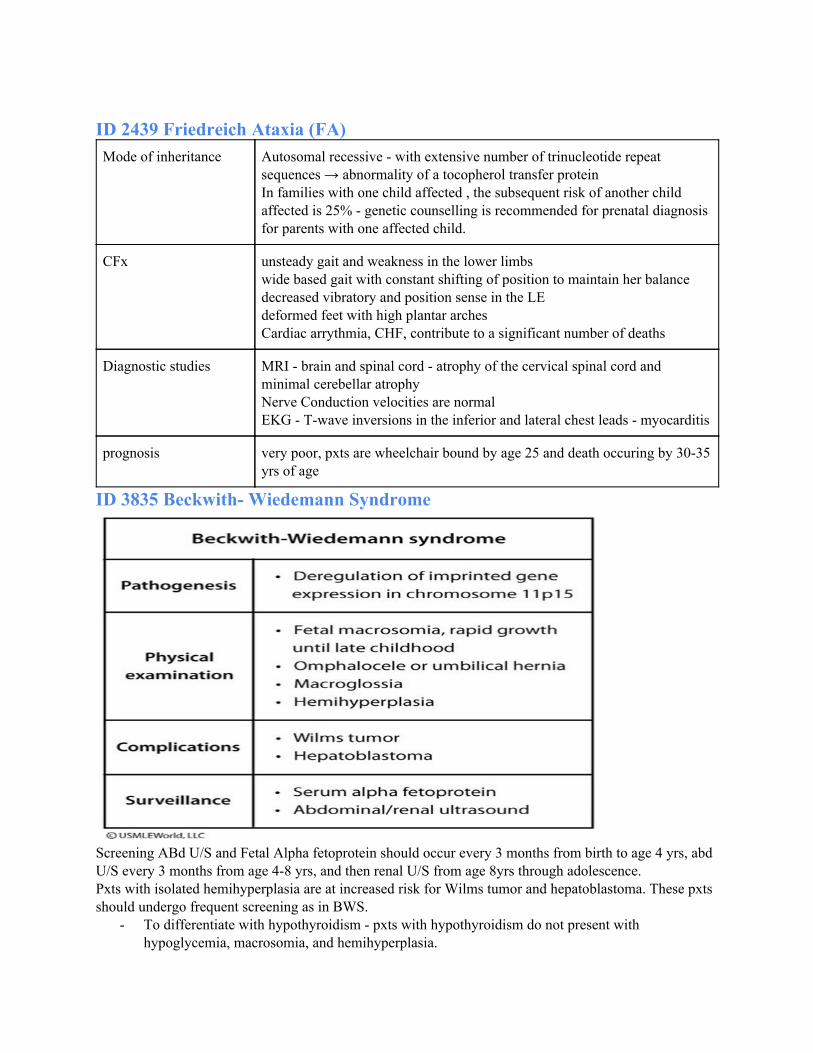
ID 3835 Beckwith- Wiedemann Syndrome
Screening ABd U/S and Fetal Alpha fetoprotein should occur every 3 months from birth to age 4 yrs, abd U/S every 3 months from age 4-8 yrs, and then renal U/S from age 8yrs through adolescence. Pxts with isolated hemihyperplasia are at increased risk for Wilms tumor and hepatoblastoma. These pxts should undergo frequent screening as in BWS.
- To differentiate with hypothyroidism - pxts with hypothyroidism do not present with hypoglycemia, macrosomia, and hemihyperplasia.

ID 2763 Sturge Weber Syndrome Clinical Features
● Include Focal or generalized seizures can start at any age ● mental retardation ● port wine stain or nevus flammeus along the territory of the trigeminal
nerve which represents a congenital unilateral cavernous hemangioma ● Other pertinent findings
○ hemianopia ○ hemiparesis ○ hemisensory disturbance ○ ipsilateral glaucoma
Diagnosis ● Mostly clinical diagnosis ● Skull X-ray - taken after age 2 yrs - gyriform intracranial calcifications that
resemble a tramline
Rx ● aimed at controlling seizures and reducing intraocular pressure ● Argon laser therapy is successful in removing skin lesions
ID 2441 Fragile X syndrome - Mode of inheritance - X- linked disoder - with expansion of CGG (Unstable) trinucleotides
repeats in the fragile mental retardation 1 gene (FMR1 gene) of the X chromosome(Located at Xq27.3) resulting in hyper-methylation of the gene and imapired transcription of the protein FMRP, which is most important to normal brain development. >200 repeats leads to silencing of the gene and an absence of the protein.
- It is much more common in males > females as they have only one X chromosome. - It is the MC’n inherited form of intellectual disability, and most pxts exhibit autistic
behavior ( e.g poor social and communication skills, repetitive or stereotypical behavior and limited interests)
- In Childhood - affected pxts often have delayed milestones(speech and motor delays), seizures(simple or complex partial seizures), macrocephaly, and hypotonia.
- Long head, prominent forehead(elongated face with protruding ears and prominent chin, and macroorchidism - these features usually appear later in adulthood.
- Other comorbid conditions are ADHD and anxiety. - Females pxts may have mild intellectual disability
Q 15 ID 2445 Neimann Pick Disease and Tay Sachs disease Diagnosis Neimann Pick Disease (TYPE A) Tay-Sachs Disease Pathology Sphingomyelinase deficiency
Foam cells with lipid laden macrophages.
Beta Hexosaminidase A deficiency
Epidemiology ● Autosomal recessive inheritance ● Ashkenazi jewish heritage
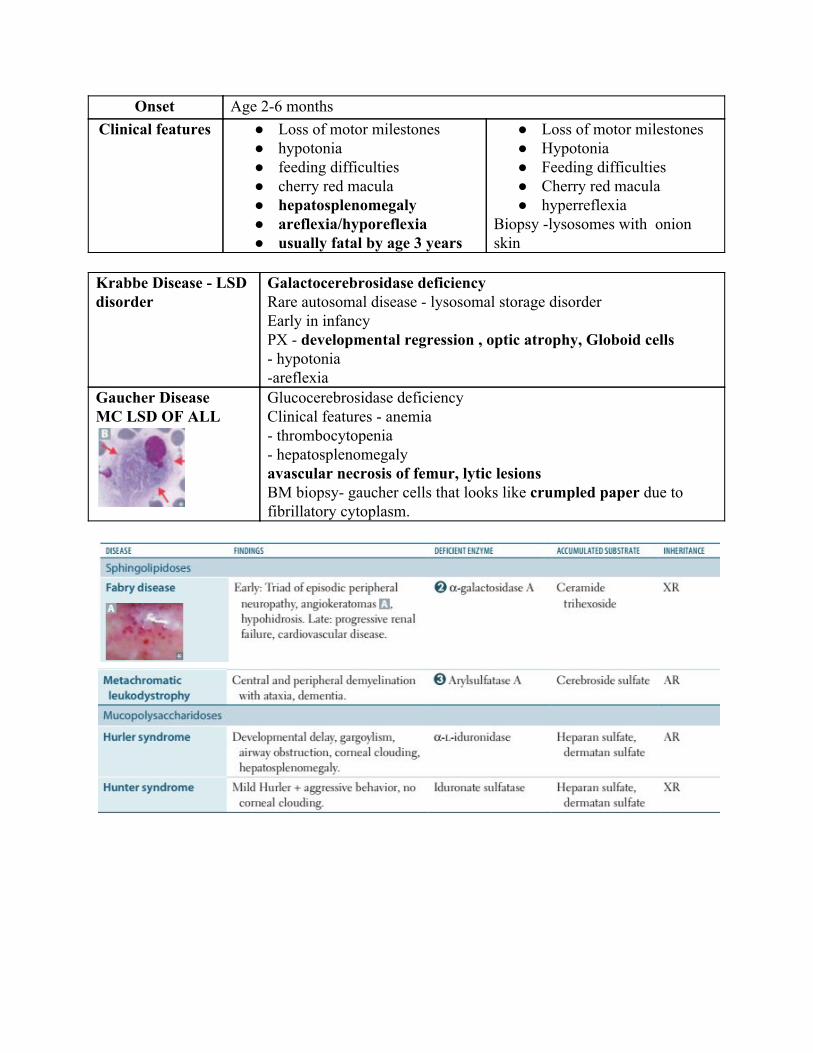
Onset Age 2-6 months Clinical features ● Loss of motor milestones
● hypotonia ● feeding difficulties ● cherry red macula ● hepatosplenomegaly ● areflexia/hyporeflexia ● usually fatal by age 3 years
● Loss of motor milestones ● Hypotonia ● Feeding difficulties ● Cherry red macula ● hyperreflexia
Biopsy -lysosomes with onion skin
Krabbe Disease - LSD disorder
Galactocerebrosidase deficiency Rare autosomal disease - lysosomal storage disorder Early in infancy PX - developmental regression , optic atrophy, Globoid cells - hypotonia -areflexia
Gaucher Disease MC LSD OF ALL
Glucocerebrosidase deficiency Clinical features - anemia - thrombocytopenia - hepatosplenomegaly avascular necrosis of femur, lytic lesions BM biopsy- gaucher cells that looks like crumpled paper due to fibrillatory cytoplasm.
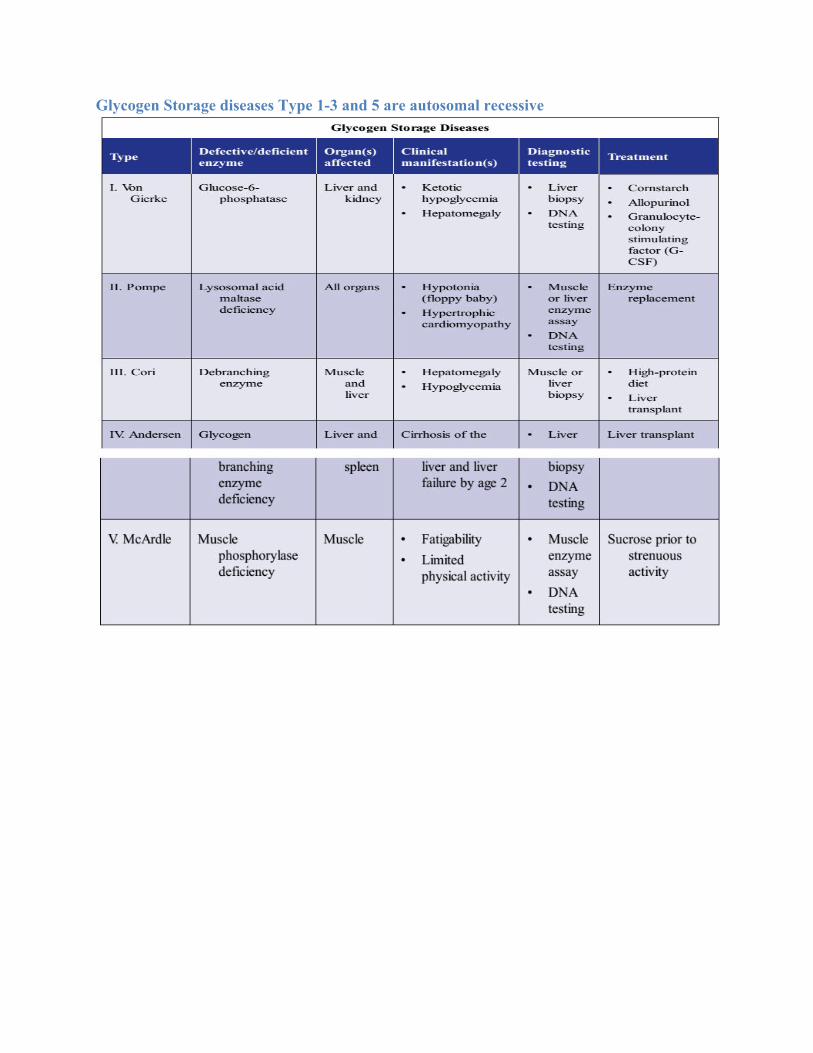
Glycogen Storage diseases Type 1-3 and 5 are autosomal recessive

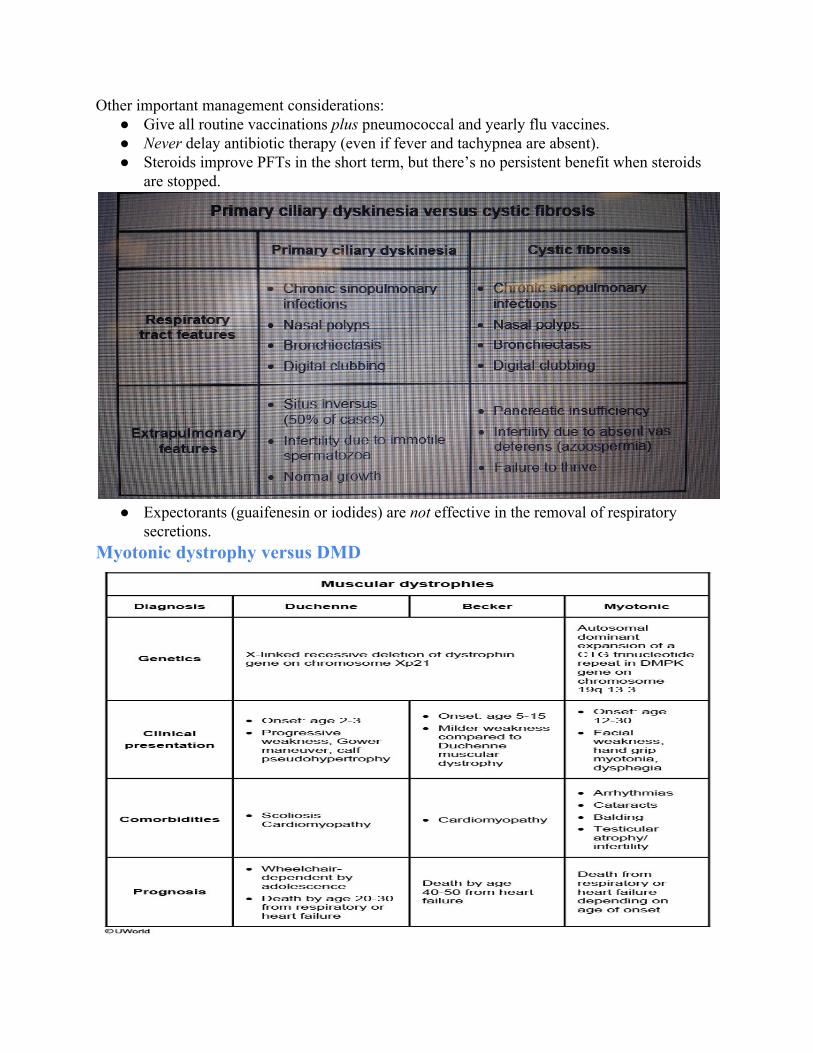
ID 8952 - CYSTIC FIBROSIS - LIFELONG COMPLICATION IS INFERTILITY IN MALES, subfertility in females (abnormally thick cervical mucus, amenorrhea)
for GI add Biliary cirrhosis. > 95% of males with CF will develop infertility due to congenital B/L absence of the vas deferens. The accumulation of inspissated mucus in fetal genital tract and obstructs the development of vas deferens. If the testes are descended as in this pxt, spermatogenesis should be normal. H/e, sperm cannot be ejaculated resulting in transparent or no semen production (Obstructive
Azoospermia). H/E, Women with CF - are usually subfertile and malnourished from pubertal delay and amenorrhea. In addition, viscous cervical mucus can obstruct sperm entry. Other associated condition is allergic bronchopulmonary aspergillosis.

Diagnostic tests :
- Best initial and most specific test: 2 elevated sweat chloride concentrations (> 60 mEq/L) obtained on separate days.
- Genetic testing is highly accurate but does not detect all chromosome-7 mutations. It is done to detect carrier status and for prenatal diagnosis.
- Newborn screening: Determine immunoreactive trypsinogen in blood spots and then confirm with sweat or DNA testing.
- Chest x-ray is useful in monitoring course of disease and acute exacerbations. - Pulmonary function testing is not done until age 5 or 6 to evaluate disease progression
(obstructive → restrictive). Findings on diagnostic tests: Arterial blood gas may show hypoxemia and, in advanced disease, a respiratory acidosis. PFTs show mixed obstructive and restrictive patterns; decrease in FVC and total lung capacity; and decreased diffusing capacity for carbon monoxide. Treatment of Cystic Fibrosis Supportive care consists of aerosol treatment, albuterol/saline, chest physical therapy with postural drainage, and pancrelipase (aids digestion in patients with pancreatic dysfunction). Ivacaftor (VX-770) is the first approved cystic fibrosis (CF) therapy that restores the function of a mutant CF protein. It is recommended for all patients age 6 and older who carry at least one copy of the G551D mutation. It has been shown to decrease sweat chloride levels, improve FEV1, decrease pulmonary symptoms and exacerbations, and improve weight gain The following treatment has been shown to improve survival:
● Ibuprofen reduces inflammatory lung response, slows patient’s decline ● Azithromycin slows rate of decline in FEV1 in patients < 13 years ● Antibiotics during exacerbations delay progression of lung disease
Antibiotics to treat CF: ● Mild disease: Give macrolide, trimethoprim-sulfamethoxazole (TMP-SMX), or
ciprofloxacin. ● Documented infection with Pseudomonas or S. aureus: Treat aggressively with
piperacillin plus tobramycin or ceftazidime. ● Resistant pathogens: Use inhaled tobramycin.
Other important management considerations: ● Give all routine vaccinations plus pneumococcal and yearly flu vaccines. ● Never delay antibiotic therapy (even if fever and tachypnea are absent). ● Steroids improve PFTs in the short term, but there’s no persistent benefit when steroids
are stopped.
● Expectorants (guaifenesin or iodides) are not effective in the removal of respiratory secretions.
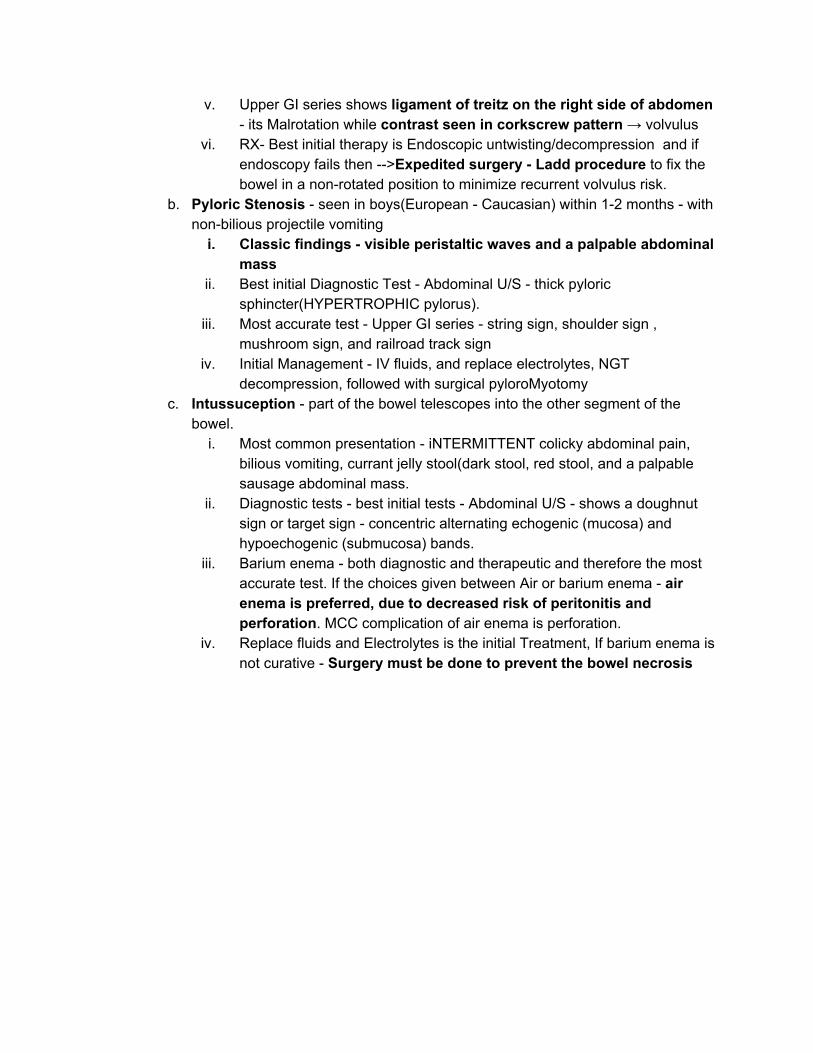
Myotonic dystrophy versus DMD

The first step in evaluation of muscle weakness involves measuring serum creatine phosphokinase (CPK). This enzyme is involved in muscle storage and transfer and is released into the blood with any muscle inflammation or damage. Serum CPK levels are markedly elevated (10-20 times normal) by age 2 and then decrease with advancing disease as the muscle is replaced by fat and fibrosis. Genetic testing showing deletion of one or more exons of DMD gene confirms the diagnosis. Congenital Infections Q 34 ID 3266 German Measles (Rubella) - 3 days measles
Clinical Presentation
Congenital Disease ● Sensorineural Hearing Loss ● Intellectual disability ● Cardiac Anomalies ● Cataracts, Glaucoma
Children ● Low grade fever, no koplik spots in rubella ● Conjunctivitis, coryza, cervical LAN(Posterior suboccipital or
auricular LAN), Forschheimer spots ● Cephalocaudal spread of blanching, erythematous maculopapular
rash Adolescents/Adults
● Same as Children +Arthralgias/arthritis Diagnosis Polymerase Chain Reaction
Acute and Convalescent serology for Anti- Rubella IgM and IgG Prevention Live Attenuated Rubella Vaccine Treatment Supportive care
Rubella can be contagious for 3 wks, during the incubation period prior to symptomatic manifestation. After a prodrome of fever, tender LAN, malaise and erythematous maculopapular rash erupts on the face and generalizes to the trunk and extremities within 24 hours. Rash spares the palm and sole. In contrast to children and med, adolescent girls and adult women usually have polyarthralgias and/or arthritis. Although most problems resolve in a few days(3 days), joint problems can last upto a month. Postinfectious encephalitis is a rare complication that can occur within a week of the exanthem. ID 2782 - Whereas Measles (Rubeola) -- Dark red rash
- Spares Palms and soles, hi fever, cephalocaudal, posterior cervical LAN - shawl distribution, spreads over time - gradually. Rash appears darker than the Rubella
- Transmission - via AIRBORNE - Pxts with known or suspected measles should be isolated and placed on airborne
precautions (negative pressure room, N95 facemask for health care personnel) - Supportive care includes - antipyretics and hydration as no specific antiviral therapy is
available. MC’n complication is pneumonia. - Prevention/recommended vaccines → 2 doses at age 1 and 4. For planned international
travel , an additional dose b/w age 6 and 11 months is also recommended. The pxt in

the vignette has not received MMR and likely acquired the disease duration international travel.
Roseola(Exanthem Subitum, sixth disease (HHV-6, MC in age <2y/o)
3-5days of VERY HI FEVER(104 F, this period is high risk of febrile seizures) followed by the maculopapular rash appears which spreads from neck and trunk to face and extremities.
Nonspecific manifestations are → palatal petechia, pharyngeal erythema, fussiness or rhinorrhea. Scarlet fever - spares palms and soles - caused by streptococcus pyogenes - presents with fever, blanching sandpaper like erythematous rash. RMSF - non pruritic macular rash begins on the distal extremities including palms and soles and spreads centripedally. Id 2768 Varicella Infection (Herpes Zoster) also Airborne Generally self limiting infxn that does not require antiviral therapy. In rare cases, Varicella can cause cerebellar ataxia or pneumonia. Superimposed aggressive Group A streptococcal can also develop and should be treated with antibacterial therapy. The Incidence of Varicella is declining due to vaccination. H/E, breakthrough infection is possible and occurs most frequently in children who have received only a single dose of VZV vaccine. Breakthrough varicella is generally mild with lower fever and fewer vesicles. UW3 ID 5540 VZV indications and contraindications → Contraindications
- Anaphylaxis to neomycin, gelatin - Pregnancy - Immunodeficient state
- Congenital immunodeficiency - LT immunosuppression - Hematologic or solid tumors - Severe HIV infection
→ Indications

- Typically administered in 2 doses: one at age 12-15 and second dose at age 4-6 years. - VZV is recommended in all children w/out absolute contraindications. Administering
vaccine to the household contacts of transplant recipients is safe and recommended by IDSA. IDSA also recommends that pretransplant should receive VZV vaccine 4 weeks prior to transplantation.
- Household contacts who receive vaccine should be monitored for the development of VZV rash (<10% of children get the rash following vaccine) and is potentially contagious to immunocompromised individuals.
UW3 ID 5735 - VZV - dermatomal Rash (Herpes Zoster)
- Due to reactivation of VZV from the dorsal root ganglia of a sensory distribution following initial infection with (Varicella - chicken pox) during childhood or early adulthood.
- Risk of reactivation is greatest in those with - Advanced age

- Malignancy - Kidney or liver disease - Immunocompromised (e.g. chronic glucocorticoid use)
- Typical Rash - evolves from erythematous papules into grouped vesicles, and most rashes typically involve single dermatome but may extend immediately to adjacent dermatomes
- Thoracic and lumbar regions are most commonly affected. Dermatomal pain (burning, throbbing, stabbing or pruritic) occurs in majority of pxts and often precedes teh rash by days or weeks.
- Dx - based on clinical presentation alone - Rx → oral Valacylovir to reduce transmission risk, new lesion formation and possibly risk
of postherpetic neuralgia - Analgesics are typically req’d for acute neuritis.
UW3 ID 5736 Contact precautions for Localized versus Disseminated Herpes zoster Hospitalization is required for pxts with disseminated infection (i.e. infection or lesions outside of the primary or immediately adjacent dermatomes such as involving both R and L flank regions and should be treated with IV acyclovir while in the hospital.
- Localized infection → standard precautions and lesion covering until the lesions are crusted over
- Disseminated infection → standard precautions and contact and airborne precautions
● Club foot versus Metatarsus Adductus a.
● LCP disease - common in between age 5-7 - limping, - Rx - NSAIDs and rest and surgical fixation of both hips
● SCFE common in adolescence (10-16)and obese pxts -Leg is externally rotated with sitting, and decreased ROM and pain with internal rotation of the hip. Frog leg lateral X- ray(should be obtained of both hips to compare) will show posteriorly and inferiorly displaced femoral head surgical pinning and internal fixation is the management to avoid risk of Avascular necrosis of the hip.
● Septic Arthritis In Children id 2447

GASTROENTEROLOGY Failure to thrive - UW 3 Office 91q - 2 (ID 5587)
- Def’n - failure to gain weight in children younger than 2yrs old . Children categorized as FTT weigh less than the 5th percentile for their age; more severe cases involve a slowing of linear growth and head circumference as well.
- 3 causes of FTT - inadequate calorie intake, inadequate calories absorption, and increased calorie requirements.
- Organic causes of FTT - feeding problems, milk protein intolerance, inborn error of metabolism, infection, cystic fibrosis, gerd or RTA.
- Newborn infants need 110kcal/kg/day, while children upto 12 months need 100kcal/kg/day to grow at a normal pace.
- For a child (6 months old) - who is <5th percentile - best initial approach → dietary modification i.e. pediatrician should review proper formula preparation with the parents, as some parents of limited financial means will dilute the formula.
- Schedule next appointment for the next 4-6 wks to monitor weight gain, if weight is not gained appropriately then supplemental feeding by NGT is preferred via IV route.
Nutrition guidelines

Dehydration assessment
Acute Diarrhea in Children UW3 ID 5897 - Its of primary concern if the child is dehydrated. In that case mgmt will focus on:
- Rehydration, replacement of continuing losses and return of early feeding of solid food
- If child is not dehydrated, child can be given normal (age-appropriate) diet with complex carbs, fluids low in sugar, and limited fat and sugar intake
- Sugar → can increase the osmolality of the stool in intestinal lumen and fatty foods can delay the gastric emptying. Both are known to worsen diarrhea.
Bowel habits normal for age UW3 ID 5118 - Normal freq of passage of stools in the infant is around 6-8x daily. Approximately one
passage of stool per episode of breastfeeding. - On 4th wk of life → this pattern changes to one or 2 episodes daily or even less, such as
<3 episodes/week. - Untreatable or prolonged constipation should prompt the clinician to consider diagnosis
of Hirchsprung’s disease Q 14 # 2226 Chronic Constipation and Recurrent Cystitis in Children
Constipation In Children and their complications RFs Initiation of solid food and cow's milk
Dietary intake is higher in dairy products and low in fiber

Toilet training School entry
Clinical Presentation Straining with passage of hardening stools Crampy abd pain </= 2 defecations/wk
Complications Anal fissures Hemorrhoids Encopresis Enuresis/UTI s Vomitting
Treatment Increase Dietary Fiber Limit cow's milk intake to <24 oz Laxative - MgSO4 aka Milk of magnesia - MOA (causes osmotic retention of fluid in the gut lumen, can be titrated to produce non- liquid stool. Short term rescue therapy for severe constipation - Bisacodyl (increased peristalsis, abd cramping, diarrhea, and nausea) +/- Suppositries(e.g. Bisacodyl), enema(PO4 enema can relieve the impaction, but puts pxts at risk for electrolyte imbalances, usually reserved for bowel prep before GI procedures)
Chronic constipation can cause recurrent cystitis in toddlers. Impacted stool can cause rectal distension, which in turn compresses the bladder, prevents complete voiding, and leads to urinary stasis.
● Duodenal atresia - failure of programmed cell death leads to improper canalization of the duodenal lumen.
i. Presents during the 1st day of life with bilious vomiting with first feed ii. BNS - Abd X ray - double bubble sign iii. Initial step in mgmt - IVFs, NGT, and surgical duodenostomy
● Midgut Volvulus - presents within the 1st month of life (Without hx of abdominal surgery)
i. S/S abd distension, bilious emesis, and sometimes if present later in the course can present with bloody stools
ii. Complications - Bowel perforation, bloody stools, abdominal distension, and peritonitis . Signs of ischemia or systemic decompensation(i.e. shock) are an indication for emergency laparotomy.
iii. Clinically stable neonates with bilious emesis - initial steps are stop the feeds, NGT decompression, and IVFs.
iv. An xray is done to rule out pneumoperitoneum → indicate immediate need for surgery.
1. If there is no free air and the bowel gas pattern - not suggestive of duodenal atresia or distal obstruction (dilated loops of bowel) then an upper GI series (barium swallow) should be performed.
v. Upper GI series shows ligament of treitz on the right side of abdomen - its Malrotation while contrast seen in corkscrew pattern → volvulus
vi. RX- Best initial therapy is Endoscopic untwisting/decompression and if endoscopy fails then -->Expedited surgery - Ladd procedure to fix the bowel in a non-rotated position to minimize recurrent volvulus risk.
b. Pyloric Stenosis - seen in boys(European - Caucasian) within 1-2 months - with non-bilious projectile vomiting
i. Classic findings - visible peristaltic waves and a palpable abdominal mass
ii. Best initial Diagnostic Test - Abdominal U/S - thick pyloric sphincter(HYPERTROPHIC pylorus).
iii. Most accurate test - Upper GI series - string sign, shoulder sign , mushroom sign, and railroad track sign
iv. Initial Management - IV fluids, and replace electrolytes, NGT decompression, followed with surgical pyloroMyotomy
c. Intussuception - part of the bowel telescopes into the other segment of the bowel.
i. Most common presentation - iNTERMITTENT colicky abdominal pain, bilious vomiting, currant jelly stool(dark stool, red stool, and a palpable sausage abdominal mass.
ii. Diagnostic tests - best initial tests - Abdominal U/S - shows a doughnut sign or target sign - concentric alternating echogenic (mucosa) and hypoechogenic (submucosa) bands.
iii. Barium enema - both diagnostic and therapeutic and therefore the most accurate test. If the choices given between Air or barium enema - air enema is preferred, due to decreased risk of peritonitis and perforation. MCC complication of air enema is perforation.
iv. Replace fluids and Electrolytes is the initial Treatment, If barium enema is not curative - Surgery must be done to prevent the bowel necrosis
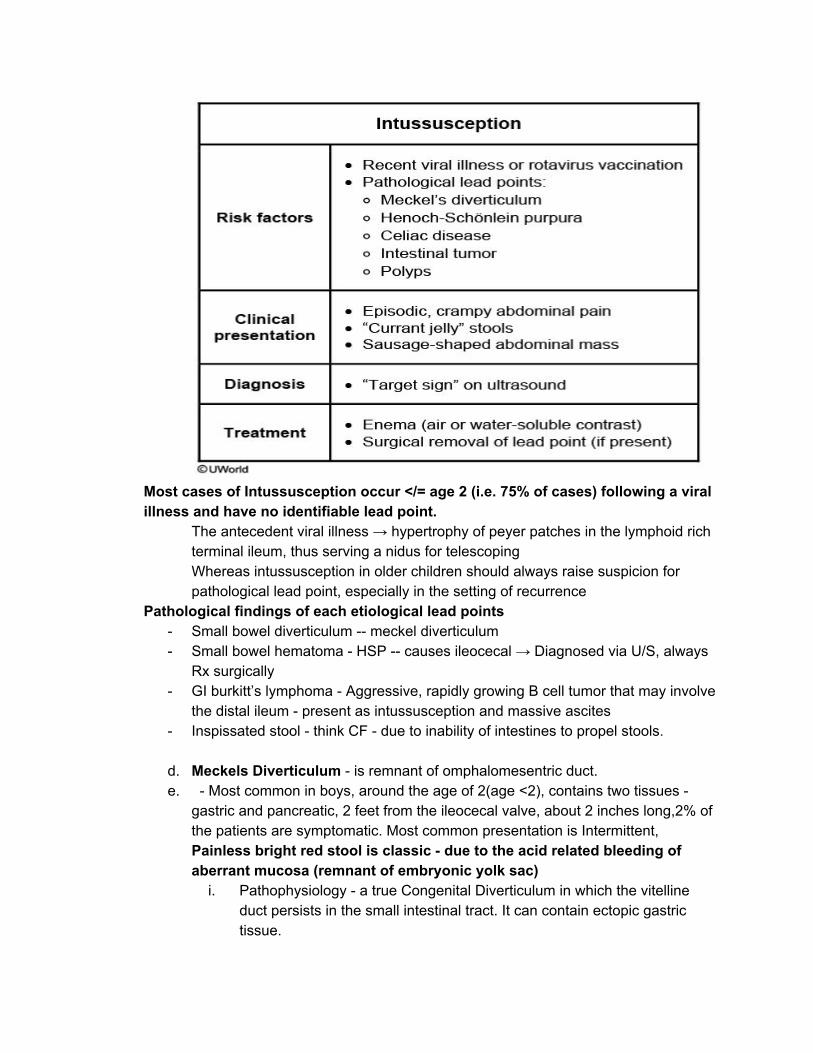
Most cases of Intussusception occur </= age 2 (i.e. 75% of cases) following a viral illness and have no identifiable lead point.
The antecedent viral illness → hypertrophy of peyer patches in the lymphoid rich terminal ileum, thus serving a nidus for telescoping Whereas intussusception in older children should always raise suspicion for pathological lead point, especially in the setting of recurrence
Pathological findings of each etiological lead points - Small bowel diverticulum -- meckel diverticulum - Small bowel hematoma - HSP -- causes ileocecal → Diagnosed via U/S, always
Rx surgically - GI burkitt’s lymphoma - Aggressive, rapidly growing B cell tumor that may involve
the distal ileum - present as intussusception and massive ascites - Inspissated stool - think CF - due to inability of intestines to propel stools.
d. Meckels Diverticulum - is remnant of omphalomesentric duct. e. - Most common in boys, around the age of 2(age <2), contains two tissues -
gastric and pancreatic, 2 feet from the ileocecal valve, about 2 inches long,2% of the patients are symptomatic. Most common presentation is Intermittent, Painless bright red stool is classic - due to the acid related bleeding of aberrant mucosa (remnant of embryonic yolk sac)
i. Pathophysiology - a true Congenital Diverticulum in which the vitelline duct persists in the small intestinal tract. It can contain ectopic gastric tissue.

ii. Other findings - mass palpated in the middle left quadrant. iii. DIAGNOSTIC AND Treatment - Technetium 99 scan (Meckel Scan) and
surgical removal is the only curative therapy. f. Necrotizing Enterocolitis - premature infants, vomiting, fever, sometimes
bloody stools, and pain out of proportion and elevated lactic acid. i. Pathophysiology - bowel undergoes necrosis and bacteria invades the
intestinal wall. Mortality rate is as high as 30% ii. Diagnostic tests - Abd X-ray shows air in the bowel wall (“Pneumatosis
intestinalis”) but no free air in the peritoneum. iii. - Antibiotics - Gentamicin, Vancomycin, and metronidazole adjunct
with serial abdominal xrays iv. CT scan will reveal air in the portal vein, dilated bowel loops, and
pneumoperitoneum v. Frank or occult blood can be seen in stool vi. Mgmt - stop the feeds, IV fluids, NGT decompression if conservative
mgmt fails → then surgery is indicated to remove the affected bowel.
For Heme - Onc - see my weak topics Iron deficiency anemia
UW3 ID 6281 - Most rapid effect of iron supplementation
● To maximize absorption of iron supplementation, the doses should be given with juice in between meals.
● Those patients suffering from severe iron deficiency anemia should respond with an increased reticulocyte count within 72 hours. Children who improve with the iron

supplements should be continued on them for at least 2-3 months to replenish their iron stores.
● Hemoglobin and hematocrit are usually restored to normal levels within 2-3 months. Hemoglobin should rise at least 1 gm/dl within 2-3 weeks.
Cerebral Palsy - greatest RF is prematurity(<32 wks)- most appropriate diagnostic test MRI of the brain and most common type is spastic diplegia - hyperreflexia and hypertonia in LE
Had 1 question on nbme on this - Spinal Dysraphism spinal dysraphism is also called tethered cord. In children, symptoms may include:

Lesions, hairy patches, dimples, or fatty tumours on the lower back Foot and spinal deformities[2] Weakness in the legs[2] Change in or abnormal gait including awkwardness while running or wearing the tips or side of one shoe[2] Low back pain[2] Scoliosis[2] Urinary irregularities (incontinence or retention)[2] UW 3 ENT SS(9845) qid -5209 Cleft lip /Cleft Palate Isolated Cleft lip with or without cleft palate → a multifactorial disorder and the modes of inheritance can be AD, AR, and XLR Pxt in the vignettes has Van Der Woude Syndrome with variable expressivity b/z mother only has an upper lip pit with limited expression
- Associated with use of teratogenic agents (commonly alcohol) during pregnancy - Careful and thorough hx is required for Dx - Reconstruction of cleft lip is performed at generally 3 months of age -- RULE OF 10’S
s→ 10lbs weight, 10 wks of age, and 10 g of hemoglobin. RESP AND CARDIO CONGENITAL DISEASES Peds respiratory infections - croup/pertussis/bronchiolitis/epiglottitis (id 3288 - seal, dry, barky cough - media for croup (laryngotracheobronchitis) and steeple sign
● Croup - Laryngotracheobronchitis Most common between age 6 months to 6 yrs) a. - look for barking cough, inspiratory stridor, child will have more difficulty when
lying down and may show peripheral cyanosis and accessory muscle use- hypoxia on presentation , and viral prodrome(Parainfluenza),
b. CXR - subglottic edema also known as the “steeple sign” c. Management includes for mild cases - Humidified air +/- Dexamethasone d. and for severe cases → Dexamethasone + Racemic Epinephrine for stridor at
rest i.e. will have inspiratory and expiratory stridor. e. Prevention - frequent hand washing, decontamination of surfaces, and
ensure proper ventilation ● Epiglottitis - HiB, look for unvaccinated children, can occur in vaccinated children as well-
look for acute onset of high fever, dysphagia, muffled or hot potato voice, drooling, inspiratory stridor, refuses to lie flat, drooling in a tripod positioning, and hypoxia is imminent - mgmt include Intubation in the OR and give IV ceftriaxone and give Rifampin for prophylaxis to all the close contacts
● Laryngomalacia -Increased Laxity of supraglottic structures, begin between 4-8 months, and resolves by age 12-18 months
a. Diagnosis is made clinical, but can be confirmed with direct or flexible fiber optic Laryngoscopy will show supraglottic closure during inspiration and omega shaped epiglottis, chronic inspiratory stridor that begins in the neonatal period(1st few months of life) worsens when supine, exacerbated by
feeding or Upper respiratory illness; prone positioning improves; absence of URI signs.
b. Rx - Reassurance for most cases c. Most infants with laryngomalacia - will grow, feed, ventilate normally with
spontaneous resolution of stridor by age 18 months. H/E, majority of the pxts will have SX of GERD(vomiting, arching of the back with feeds, poor weight gain) and should be treated accordingly (e.g. upright positioning after feeds, acid reducers)
d. Supraglottoplasty for severe symptoms (e.g. poor weight gain, apnea, cyanosis, rapidly worsening stridor)
● Vascular Ring - Results from abnormal development of aortic arch, causing tracheal, bronchial or esophageal compression. Presents in infants AGE <1 MONTH, Biphasic stridor that improves with neck extension as it decreases the tracheal compression and more prominent during expiration
a. Diagnostic modalities - Barium swallow - can show indentations of esophagus, and the diagnosis can be confirmed with MRI with angiography
● Foreign Body Ingestion (8791) Management I. Sx - difficulty swallowing, feeding refusal, and vomiting II. Mgmt depends on the object’s material, location in the GIT, timing of ingestion,
and symptoms. A. Coin - Radio-opaque object seen on Xray, if a coin is visualized in the
esophagus and the pxt is symptomatic or the time of ingestion is unknown, the coin should be removed promptly via Flexible endoscopy .
1. If a coin is visualized in the esophagus and pxt is asymptomatic, the child can be observed for upto 24 hrs of ingestion, those that reach the stomach can be allowed to pass immediately.
2. If radiolucent object is suspected and not visualized on xr then NBS CT scan
B. Objects such as batteries, sharp objects, or multiple magnets - increase risk of perforation, obstruction, or ischemia and require preemptive removal. Id 2656
1. Immediate flex endoscopy is required 2. Dangerous Sx e.g. hematochezia, melena, and severe abd pain
are indications for surgical removal. III. Tracheobronchial foreign body aspiration - most common in toddlers - Most
common location is R mainstem bronchus 1. Sx - sudden onset stridor, wheeze, cough, or dyspnea. 2. Rigid bronchoscopy is the procedure of choice
B. Upper GI series with barium contrast is generally avoided because of risk of contrast aspiration and contrast can obscure the visualization on subsequent endoscopy.
NOTE - C AND D are chronic causes of inspiratory stridor. Croup and Foreign body aspiration are more acute causes of inspiratory stridor.

f) ID 4829 Chest X-ray and identifying thymus or Right atrium on XR. i)Thymus is normally visible on CXRs in children age < 3 yrs. Normally atrophies
and replaced by fat after puberty when it has completed production of T- lymphocytes. On frontal views - it is most commonly recognized as the “sail sign” - due to its triangular shape, scalloped border, and uniform density).
ii) it can shrink during times of stress or illness and rebound to a larger size after recovery(rebound hyperplasia).
iii) Its function in utero and during infancy and childhood for lymphocyte production and maturation.
iv)Its absence on Xray suggests - Thymic Hypoplasia or Aplasia (digeorge syndrome)
V)Adults with mediastinal opacities on Xray should undergo furthew work up for pathology. Residual thymic tissue can undergo malignant transformation into a thymoma, which can occur in pxts with myasthenia gravis. Lymphoma should also be on differential for an anterior mediastinal mass in children and adults.
Id 4826 - Postpericardiotomy syndrome
ID 2435 Diaphragmatic Hernia Diaphragmatic Paralysis from Phrenic nerve injury
- Two most common causes of Diaphragmatic paralysis in a newborn 1) birth injury or 2) cardiothoracic surgery.
- It is typically accompanied by the signs of brachial plexus injury such as Erb’s palsy. Endocrine
● Infants of Diabetic Mothers (IDM) - Most common complications - IDM regardless whether pregestational or gestational diabetes are at increased risk of
RDS, preterm delivery, and fetal macrosomia. Maternal hyperglycemia with resultant fetal hyperinsulinemia(anabolic growth) delays cellular maturation. Consequently immature pneumocytes in fetal lungs unable to produce surfactant resulting in RDS.
- IDM can also be at increased risk for small for gestational age newborns because LT or poorly controlled DM increases vascular resistance that affects the placenta and restrict the fetal growth.

- Poorly controlled DM during 1st trimester → risk for cardiac and CNS defects such as CHD, NTDs, Small Left colon syndrome, and Spontaneous abortion, or Limb defects such as Sacral agenesis.
i. Macrosomia - all organs are enlarged except brain. Polycythemia and hyperviscosity
ii. Small left colon syndrome - Constipation and abdominal distension - diagnosed by Barium enema and treated with small frequent feeds
iii. Cardiac -- asymmetric intraventricular septal defects→ decreased CO - diagnosed with EKG and Echo; and managed with beta blockers and IVFs. Most common association is Truncus Arteriosus or TGV is more common
iv. Renal Vein thrombosis - Flank pain, hematuria, and thrombocytopenia and possible bruit can be appreciated.
v. Lab findings and effects 1. Hypoglycemia - jittery and seizures 2. Hypocalcemia - tetany and lethargy and prolonged QT syndrome 3. Hypomagnesemia - hypocalcemia and decreased PTH 4. Hyperbilirubinemia - Scleral icterus and kernicterus.
vi. For pxts with type I diabetes with mutiple Intermediate Insulin regimens - esp high school students - reduce the dose of insulin by 10-15% especially on the days of playing sports
b. Neonatal polycythemia - id 4819 - differentiate from hyperinsulinism (look for DM mother+ RDS on Xray + big infant)
● Normal HCT → 45-65%. The hematocrit reaches its maximum value when the infant is approximately two hours of age. For this reason, it is important to recheck the hematocrit levels 12 to 24 hours after delivery if the hematocrit value is borderline high. The sample must be venous (not capillary) blood.
● Initial testing → capillary (heel or finger pinprick HCT level) - if HCT is > 65% → nbs → to get the venous HCT level via peripheral blood sample. Peripheral venous hematocrit is usually 5 - 15% HCT lower than HCT taken from a capillary sample. Source uw 3 (Inpxt) id - 6188.
● Genetic/metabolic disease: hypothyroidism or hyperthyroidism, genetic trisomy (13,18, 21)
● Common cause of neonatal polycythemia → delayed umbilical cord clamping → excess transfer of placental blood.
● Asymptomatic - MC’n Symptom, add hyperbilirubinemia ● Increased RBC mass causes hypoglycemia and hypocalcemia (due to increased
cellular uptake) ● Rx → IVFs hydration via feeding or parenteral fluids, Glucose, and partial
exchange transfusion (symptomatic pxts - blood is removed in exchange for normal saline to normalize the HCT). .
● In the given pxt - with hx of preeclampsia → infant developed polycythemia due to reduced placental flow and intrauterine growth restriction.

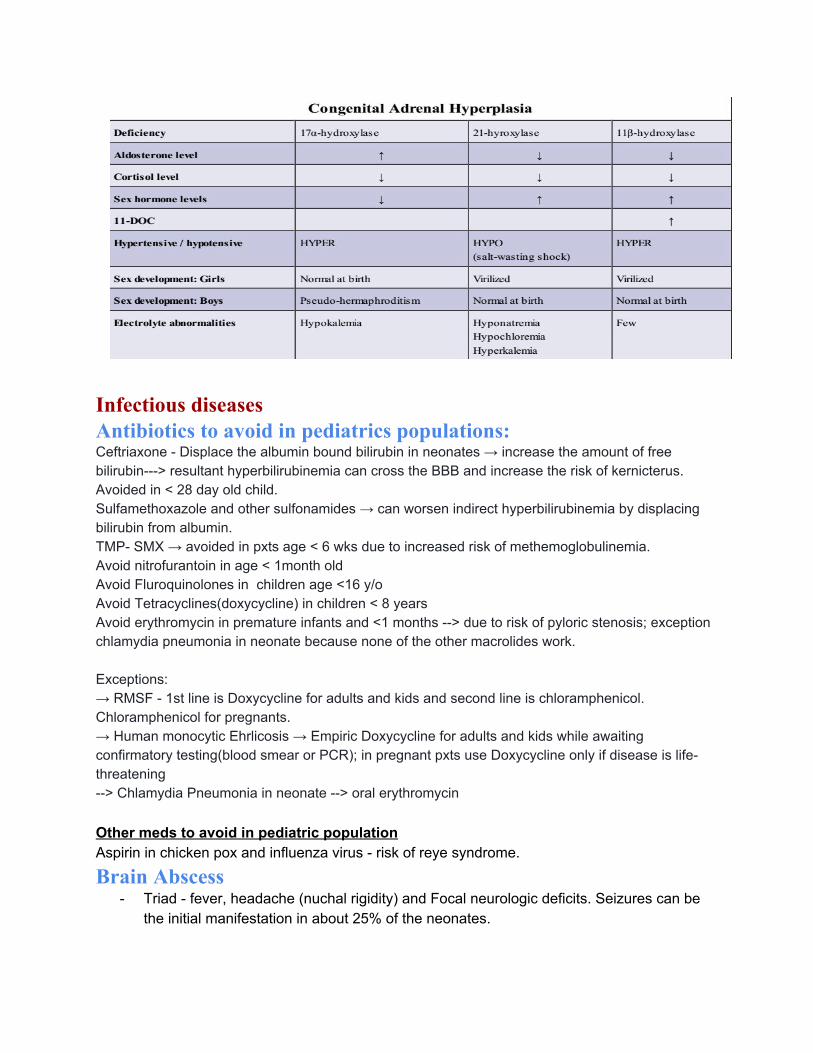
● CAH
a. Dx - Initial test - Elevated 17 OH progesterone and also low cortisol, hi ACTH, hi renin, and low aldosterone
b. Rx is IVFs and lifelong steroids such as Hydrocortisterone and Fludrocortisone if its salt wasting
c. In stress, both Hydro/Fludro- cortisterone doses should be increased d. Psychogenic counselling about gender identity and corrective surgery for females
Infectious diseases Antibiotics to avoid in pediatrics populations: Ceftriaxone - Displace the albumin bound bilirubin in neonates → increase the amount of free bilirubin---> resultant hyperbilirubinemia can cross the BBB and increase the risk of kernicterus. Avoided in < 28 day old child. Sulfamethoxazole and other sulfonamides → can worsen indirect hyperbilirubinemia by displacing bilirubin from albumin. TMP- SMX → avoided in pxts age < 6 wks due to increased risk of methemoglobulinemia. Avoid nitrofurantoin in age < 1month old Avoid Fluroquinolones in children age <16 y/o Avoid Tetracyclines(doxycycline) in children < 8 years Avoid erythromycin in premature infants and <1 months --> due to risk of pyloric stenosis; exception chlamydia pneumonia in neonate because none of the other macrolides work. Exceptions: → RMSF - 1st line is Doxycycline for adults and kids and second line is chloramphenicol. Chloramphenicol for pregnants. → Human monocytic Ehrlicosis → Empiric Doxycycline for adults and kids while awaiting confirmatory testing(blood smear or PCR); in pregnant pxts use Doxycycline only if disease is life- threatening --> Chlamydia Pneumonia in neonate --> oral erythromycin Other meds to avoid in pediatric population Aspirin in chicken pox and influenza virus - risk of reye syndrome. Brain Abscess
- Triad - fever, headache (nuchal rigidity) and Focal neurologic deficits. Seizures can be the initial manifestation in about 25% of the neonates.

i. Most common RFs are recurrent sinusitis(direct spread from sinuses to frontal sinus) and Congenital heart defects( Hematogenous spread).
ii. Once Suspected - brain imaging is necessary to confirm the diagnosis.
Meningitis ● Bacterial Meningitis id 3633
Causes of Meningitis in Children
< 3 months Group B strept (neonates < 28 days and infants age < 3months) Ecoli Listeria Monocytogenes HSV
3 months to 10 yrs
Streptococcus pneumoniae - 1st MC’n N. Meningitidis 2nd MC’n
>/= 11 yrs old N.Meningitidis
Bacterial Meningitis in Children age >1 month
MCC Organisms Streptococcus Pneumoniae - 1st MC’N Neisseria Menningitis is the 2nd MC’n
Clinical Features Fever Increased Intracranial pressure (e.g. Vomiting, altered mental status, and headache) Meningeal Irritation (e.g. Nuchal rigidity)
Work up Complete Blood count Blood cultures Lumbar Puncture for CSF analysis
Rx IV Vancomycin and Ceftriaxone (Contraindicated in neonates age </= 28 days due to increased risk of Kernickerus in infants with physiologic hyperbilirubinemia) OR Cefotaxime Dexamethasone for H aemophilus Influenzae type B meningitis as steroids can reduce the risk of sensorineural hearing loss
CSF analysis and adminstration of antibiotics are the priorities when meningitis is suspected. Herniation is extremely rare in infants as their fontanelles are open and can accommodate some brain swelling. Therefore, Head CT imaging should be reserved for pxts with :
- Comatose

- Have FNDs - Have a hx of neurosurgical procedure (VPS).
Viral Meningitis in Children ● Viral meningitis or encephalitis in the pediatric population in the United States is
usually related to enteroviruses or arboviruses. ● The common ones are Eastern equine encephalitis, Western equine encephalitis,
St. Louis encephalitis, Colorado tick fever, and California encephalitis. ● These infections are more frequent during summer, late spring, and early fall,
especially in the rural areas. ● HSV is the most common cause of viral meningitis in adults.
Most common complications of Meningitis - Hearing loss - Loss of cognitive function (loss of neurons in dentate gyrus of hippocampus) - Seizures - Mental retardation - Spasticity or paresis
Neonatal Conjunctivitis UW3 QID 4965
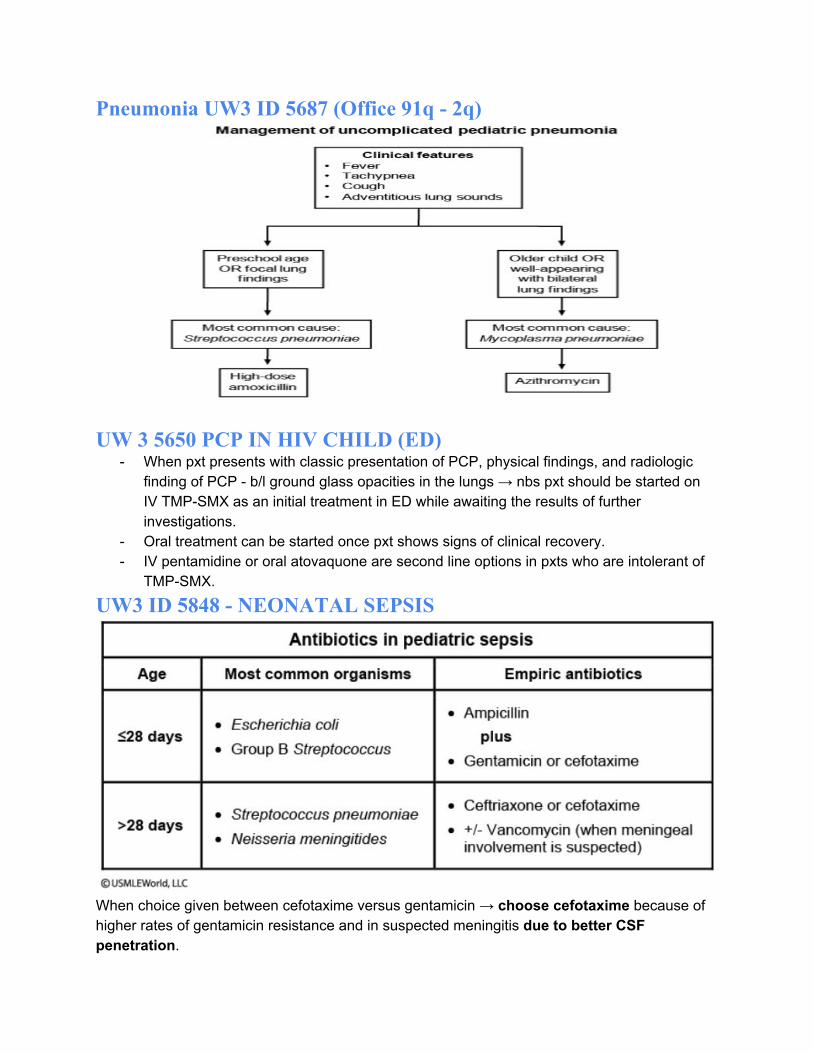
Pneumonia UW3 ID 5687 (Office 91q - 2q)
UW 3 5650 PCP IN HIV CHILD (ED) - When pxt presents with classic presentation of PCP, physical findings, and radiologic
finding of PCP - b/l ground glass opacities in the lungs → nbs pxt should be started on IV TMP-SMX as an initial treatment in ED while awaiting the results of further investigations.
- Oral treatment can be started once pxt shows signs of clinical recovery. - IV pentamidine or oral atovaquone are second line options in pxts who are intolerant of
TMP-SMX.
UW3 ID 5848 - NEONATAL SEPSIS
When choice given between cefotaxime versus gentamicin → choose cefotaxime because of higher rates of gentamicin resistance and in suspected meningitis due to better CSF penetration.

UW 3 LOCAL ANESTHETICS USE IN CELLULITIS ID 4966 (ED) Cellulitis is characterized by its irregular and elevated borders, as well as increased local temperature, tenderness, and erythema. Local anesthetics are not effective for managing cellulitis pain because the acidic environment of the infection neutralizes the medication rendering it ineffective.If this patient's cellulitis progresses to abscess formation, a local anesthetic should be used to anesthetize the epidermis in order to drain the abscess. Test 29 ID 9849 Q 15 Oral Ulcers - Gingivostomatitis versus Hand foot mouth syndrome
Id 5765 - Group A streptococcus (Strept Pyogenes) - UWORLD STEP 3 91 Q1office
a. Streptococcal pharyngitis - uncommon in the children age < 3 years due fewer epithelial attachment sites in the throat
b. (IM or oral PCN can be started after +ve Rapid strept antigen test) which is highly specific.The goals of antibiotic treatment are to reduce symptom severity and duration, decrease spread to close contacts, prevent acute rheumatic fever and prevention of suppurative complications such as peritonsillar abscess, Cervical lymphadenitis)
c. Optimal duration of oral PCN is 10 days both to ensure full eradication of bacterial carriage and to prevent Rheumatic fever. If pxt is PCN allergic, alternative ABX is 5 day course of Azithromycin. Those who cannot tolerate oral meds, a single dose of IM PCN (bactericidal for upto a month) can be given.
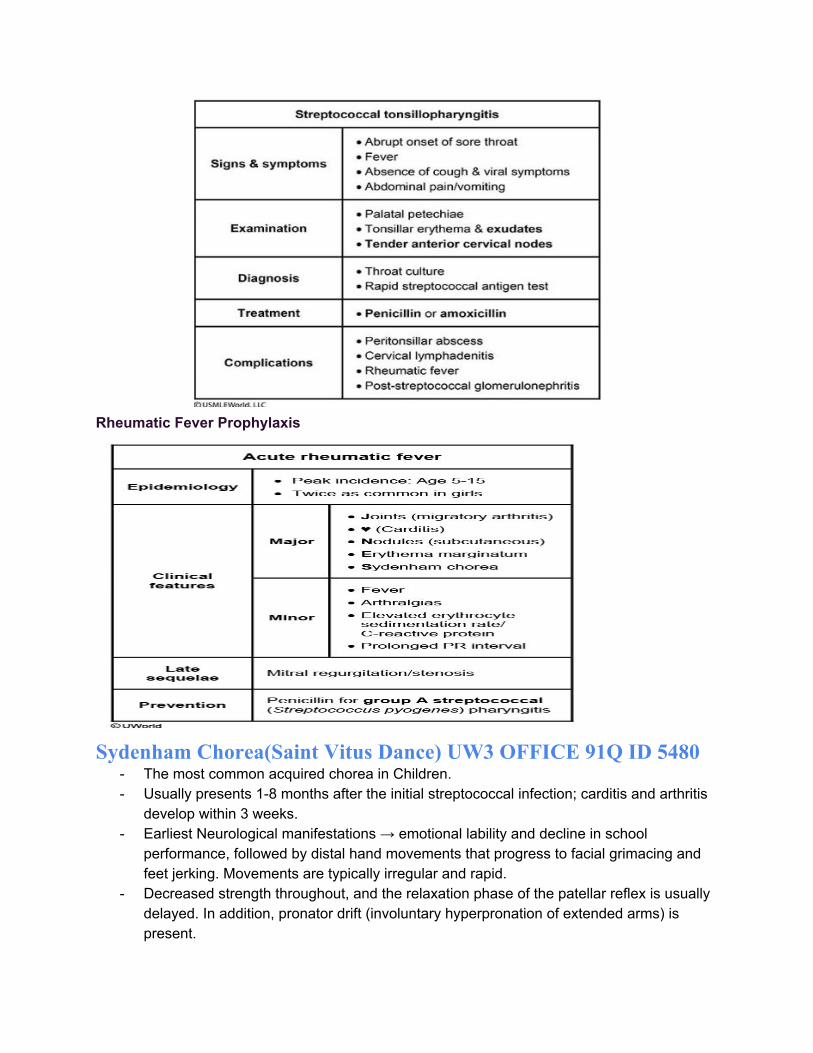
Rheumatic Fever Prophylaxis
Sydenham Chorea(Saint Vitus Dance) UW3 OFFICE 91Q ID 5480
- The most common acquired chorea in Children. - Usually presents 1-8 months after the initial streptococcal infection; carditis and arthritis
develop within 3 weeks. - Earliest Neurological manifestations → emotional lability and decline in school
performance, followed by distal hand movements that progress to facial grimacing and feet jerking. Movements are typically irregular and rapid.
- Decreased strength throughout, and the relaxation phase of the patellar reflex is usually delayed. In addition, pronator drift (involuntary hyperpronation of extended arms) is present.

- It is a clinical dx. - Rx → SC is the cardinal feature of rheumatic fever and affected pxts should receive long
acting IM PCN until adulthood for secondary prevention, even if there is no active pharyngitis.
- Rx of SC itself → primarily supportive with complete resolution of Sx within months. CSTs can reduce the duration of symptoms but are typically reserved for severe cases.
d. UW3 ID 12665 - 12668 Kawasaki Disease
Epidemiology : 90% age < 5 + increased incidence in East Asian ethnicity Diagnostic criteria : Fever >/= 5 days + 4 of the following findings:
- Conjunctivitis: B/L and nonexudative - Mucositis: injected/fissured lips or pharynx, “strawberry tongue” - Cervical LAN: >/= 1 LN > 1.5 cm in diameter - Rash: erythematous, polymorphous, generalized; perineal
erythema and desquamation; morbilliform (trunk and extremities) - Erythema and edema of hands/feet
Question: when to order the CRP, or ESR(elevated in KD) with daily follow-up scheduled to assess for new symptoms? Answer: when </= 3 diagnostic criteria are met in a child with >/= 5days of fever. Reasoning: KD can present a diagnostic challenge because viral illnesses can cause fever >/= 5 days and similar features (rash, conjunctivitis, or oropharyngeal erythema). Question: Which diagnostic criterion is least observed? Answer: Lymphadenopathy is observed least frequently.
Rx---> Aspirin + IVIG Question: What are the benefits of IVIG? Answer: It reduces inflammation when given with aspirin.although exact mechanism is unknown, the use of IVig greatly improves the morbidity and mortality and reduces the reisk of cardiac sequelae. Question: when is the risk of coronary aneurysms highest in kawasaki patient?

Answer: Failure to treat KD in a timely manner significantly increases the risk of coronary aneurysms, with substantial risk after the 10th day of illness. Thus, waiting for 3-4 days is inappropriate without making a definitive diagnosis or making an alternative diagnosis.
Complications: Coronary artery aneurysms and Myocardial Ischemia and infarctions Question: When to perform Echocardiogram? Answer: All children diagnosed with KD should have an echocardiogram performed at baseline. CA usually develop after the 10th day of fever and are often not evident during acute illness, some degree of coronary artery dilatation and myocardial dysfunction may be present at diagnosis. Question: Is there a need to repeat the echocardiograms? Answer: Even if the initial study is normal, aneurysms may later develop even in patients who receive appropriate treatment, follow up studies are indicated at 2 and 6 weeks after treatment. Question: Should the child receive the appropriate age vaccinations right after he/she being treated with IVIG? Answer: Pxt has been treated with IVIG which is composed of pooled ABs, the body’s normal immune response to live vaccines. Because of this, pxts should defer live vaccines for 11 months after receiving IVIG. Question: What is the prognosis of Kawasaki disease? Answer: The likelihood of relapse and recurrence after an episode of kawasaki disease is low (<2.5% recurrence during the 1st 3 years after treatment). If the pxt had coronary artery dilatation, coronary artery aneurysms, or myocardial dysfunction on his baseline echocardiogram, he would be at increased risk for future cardiac events and his participation in contact sports will be restricted.
e. Enterobius Vermicularis (pinworm) infection id 3791 - read in peds notes i. Mode of transmission - via contact with contaminated objects, bedding
or clothing or unwashed hands after scratching the perianal area ii. Female worms migrate distally to deposit eggs onto the perianal skin,
primarily at night. iii. Dx - made via tape test at night or early morning - where you will see
pinworms adhered to the tape under the microscopy. iv. Rx with Albendazole or pyrantel pamoate is recommended for the pxt
and the household to avoid reinfection. v. To differentiate with Lichen Sclerosus - LS can cause perianal and vulvar
pruritus as well as vaginal discharge or bleeding. PE may show hypopigmentation and ecchymoses of the affected area.
f. Id 4317 Cat Bites UW3 ID 5317 (ED)
Cat Bites
Microbiology ● Pasteurella Multocida

● Anaerobic bacteria
Mgmt ● Copious irrigation with saline and cleaning with providone -iodine solution
● Prophylactic amoxicillin and clavulante, another agent with good coverage for pasturella (TMP-SMX + CLINDAMYCIN);for severely ill pxts - use IV ampicillin - sulbactam. Pxt who are allergic to PCN use doxycycline.
● Tetanus booster as indicated ● Avoid Closure due to a high risk of infection,
unless there is a major cosmetic implication ● Bite wounds <24 hours old on the face without
clinical signs of infection can be closed. Antibiotic prophylaxis should be given for all wounds closed primarily.
● Intestinal parasitosis UW 3 ID 5083 - (Office 91 Q) a. Triad of chronic diarrhea, iron deficiency anemia and eosinophillia → suspect
intestinal helminthic infection b. Esp among pxts who recently emigrated from an endemic area, esp children. c. Reinfection is common even if treated with antihelminthic agent, due to poor or
inadequate hygeine measures may cause family members to be infected and subsequently puts the children at risk of reinfection. Thus, family members should be tested to determine if they are infected and appropriate therapy should be given to them as well.
d. IDA secondary to parasitosis will not resolve even after the treatment, thus iron replacement therapy should be initiated.
● Tick bites UW 3 ID 5078 Although ticks can transmit important infectious diseases (e.g., Lyme disease, RMSF, Ehrlichiosis), the only complication in most cases is local inflammation or local infection (if a

wound is produced). The transmission of Lyme disease takes place at least 36-48 hours after the tick has started suctioning the patient's blood.
● IV ABX indications a. Infants age < 2 months at high risk for urosepsis b. Pxts with vomiting who cant tolerate oral ABX, or fail Oral ABx, hemodynamically
unstable, or have a positive blood culture.
● Fanconi Anemia - ID 4438 - Cause of Aplastic anemia and fanconi anemia’s features. a. Fanconi anemia is the most common cause of aplastic anemia. It is autosomal
recessive or X-linked disorder. b. Most are diagnosed by age 16 yrs and have a predisposition for developing
cancer. Numerous genes, all believed to involve DNA repair. c. Dx is made by Chromosomal breaks on genetic analysis with the clinical
findings.
Location Clinical Manifestations of Fanconi Anemia
Bone Marrow Aplastic anemia and progressive bone marrow failure
Appearance Short stature, microcephaly, abnormal thumbs(slightly bent), and hypogonadism
Skin Hypopigmented/hyperpigmented areas, cafe au lait spots, and large freckles
Eyes/ears Strabismus, low set ears, and middle ear abnormalities (e.g. hemorrhage, incomplete development, chronic infections, deafness)- such as pounding sensation in ears
● Blackfan Diamond Anemia aka congenital hypoplastic anemia
a. Triphalengeal thumb, macrocytic anemia, low reticulocytes b. Majority of cases are sporadic, but can be dominant or recessive inheritance c. Pathology- intrinsic defect of the erythroid progenitor cells - which results in
increased apoptosis (programmed cell death) d. Average age being diagnosed being 3 months of age, usually presents with
pallor e. The macrocytic anemia is different from megaloblastic anemia - because its
neutrophils doesn’t contain - multiple nucleus f. Electrophoresis - elevated Fetal Hb levels g. Rx - steroids and for unresponsive pxts - transfusion therapy is indicated.
● Milk Protein enterocolitis - usually present age 2-8 weeks

● Pneumothorax - secondary to cough id 3457 - Severe coughing paroxysms → subcutaneous emphysema, where air leaks from the
chest wall into the subcutaneous tissues due to high intraalveolar pressure provoked by the cough.
- By a similar process, pneumothorax can occur, therefore in such patients - those with apparent subQ emphysema secondary to severe coughing paroxysms, CXR → must be obtained to rule out pneumothorax.
ID 2680 Breath Holding spells versus Generalized Seizures - Breath holding spells commonly occur in children age 6months to 2yrs, and present with either
cyanosis following an emotional trigger such as crying or breath holding in forced expiration or pallor following an upsetting event or minor injury. Pxts typically recover without any postictal period.
- Pallid episode lasts < 1 minute with subsequent confusion and sleepiness for few minutes. - Some children experience recurrent episodes that usually stop by age 5, others develop vasovagal
syncope later in life. - BHS - are commonly associated with iron deficiency anemia - so with Dx of IDA -- give iron
supplementation. - Parents should be reassured that these episodes are harmless and children will have normal
development.

Regurgitation and Vomiting Differentials in Peds
For Physiologic GERD - Rx - parents should be reassured and should be advised to give small freq feeds, hold the infant upright for 20-30 minutes after feeds, and place the infant prone when awake. Activities that increase intraabdominal pressure (e.g. fastening diaper too tight, bringing the knee to the stomach) should be avoided. Regurgitation usually improves around 6 months (when the infant can sit unsupported) and resolves by age 1 year. 11) Chronic Granulomatous Disease - 4495 ID with note. 12) Spondylolisthesis - ID 4064 - slipped disc syndrome - Chronic back pain + palpable step off at lumbosacral area (commonly L5 OVER S1) and neurological findings leads to the diagnosis. 13) CROUP (Laryngotracheobronchitis) Management Id 2424 14) Neonatal Polycythemia - ID 4819 16) Cryptorchidism - complications even after orchiopexy ID 8956 - Subfertility.
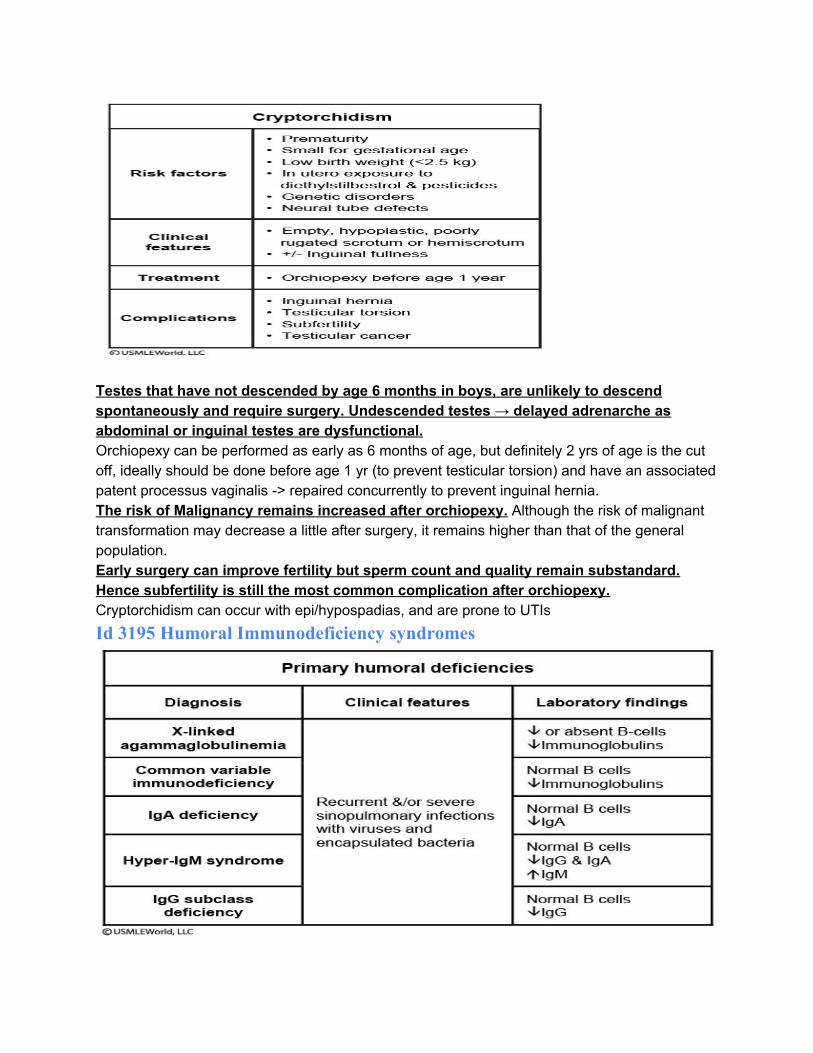
Testes that have not descended by age 6 months in boys, are unlikely to descend spontaneously and require surgery. Undescended testes → delayed adrenarche as abdominal or inguinal testes are dysfunctional. Orchiopexy can be performed as early as 6 months of age, but definitely 2 yrs of age is the cut off, ideally should be done before age 1 yr (to prevent testicular torsion) and have an associated patent processus vaginalis -> repaired concurrently to prevent inguinal hernia. The risk of Malignancy remains increased after orchiopexy. Although the risk of malignant transformation may decrease a little after surgery, it remains higher than that of the general population. Early surgery can improve fertility but sperm count and quality remain substandard. Hence subfertility is still the most common complication after orchiopexy. Cryptorchidism can occur with epi/hypospadias, and are prone to UTIs Id 3195 Humoral Immunodeficiency syndromes

ID 12519 Common Variable Immunodeficiency - Impaired B- cell differentiation and hypogammaglobulinemia - Most common primary immunodeficiency in adults, and characterized mainly by
increased susceptibility to bacterial infections - Most cases are sporadic and family hx is usually absent. Diagnosed by age 20-45 yr/old - Diagnosed via quantitative immunologic testing - Increased risk for NHL (non hodgkin lymphoma) - Markedly reduced or absent immune response to vaccination
Neuro Peds ID 4439 Common causes of Stroke in pediatric population
Sickle cell disease Prethrombotic diseases Congenital heart diseases Bacterial meningitis Focal cerebral arteriopathy Vasculitis Head trauma - intentional and unintentional
PSYCH PEDS
1) Grief and Bereavement in children a) 9 yr old boy and 5 yo girl brought to the physician by their mother. Ever since the
family’s dog was hit by a car and died 2 wks ago, the boy has been sad and cries frequently. Asks to sleep in his parents bed, which he hasnt done so in many years. In contrast his sister is cheerful and act as though nothing has happened . She is excited about her upcoming birthday party and plans to set a place for the
dog at the table. Their developmental and growth milestones are normal. Which of the following is the best approach in this situation?
i) Reassure the mother that both are normal age appropriate behavior/rxns. ii) Bereavement in children can present in many different ways, depending
on the childs age. iii) Responses depends on number of factors - type of death, relationship to
the deceased, personality or temperament of the child, pre-existing RFs such as prior mental illness, quality of family support, and concurrent life stressors.
iv) Preschool children usually react to the loss of a loved person or pet with disbelief and may think that death is temporary or reversible. Example such as 5 yo girl in this scenario acting as though the dog is still alive and her magical thinking that it can appear are not pathological.
v) Older children (>7 yrs) in contrast are aware that death is final. They may react with sadness, crying, self-blame, guilty, loss of concentration, anger, nightmares, regression to earlier behaviors, social isolation, and school problems such as avoidance or academic difficulty.
vi) Mgmt - Support from the child’s parents including encouragement to express feelings at the child’s own pace and reassurance that the child is not to blame, is usually sufficient to help the child through the bereavement period. If signs of mood disturbance or academic, or social impairment persists and do not improve, psychology referral should be pursued at that time.
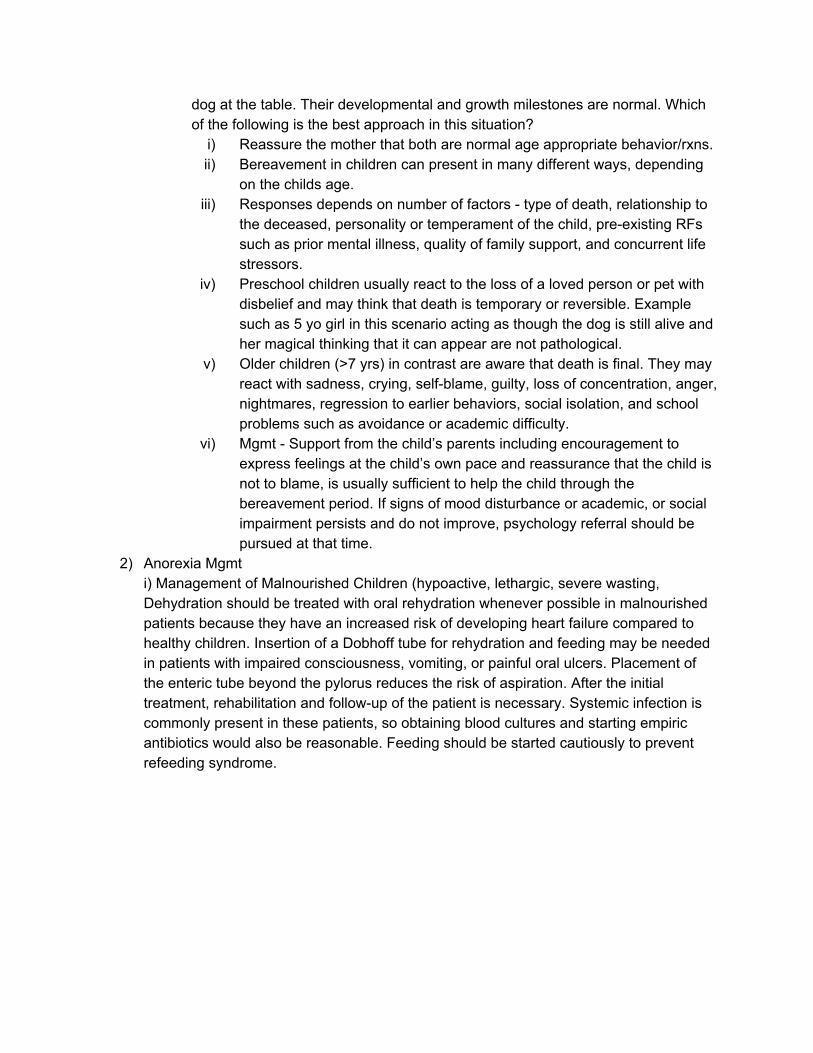
2) Anorexia Mgmt i) Management of Malnourished Children (hypoactive, lethargic, severe wasting, Dehydration should be treated with oral rehydration whenever possible in malnourished patients because they have an increased risk of developing heart failure compared to healthy children. Insertion of a Dobhoff tube for rehydration and feeding may be needed in patients with impaired consciousness, vomiting, or painful oral ulcers. Placement of the enteric tube beyond the pylorus reduces the risk of aspiration. After the initial treatment, rehabilitation and follow-up of the patient is necessary. Systemic infection is commonly present in these patients, so obtaining blood cultures and starting empiric antibiotics would also be reasonable. Feeding should be started cautiously to prevent refeeding syndrome.
3)Autism disorder
a) More common in boys, autism is a disorder characterized by a restricted range of interests and dramatic abnormalities in communication and social interaction. The condition always presents within the first 30 months of life and is often linked with mental retardation with intelligence quotients typically ranging from 35 to 50. Common findings include an absence of protodeclarative pointing, excessive or absent responses to environmental stimuli, speech abnormalities, and strange and solitary play. Often, most disturbing to parents is the child's indifference to social interaction with others and unwillingness to establish interpersonal relationships.
b) Artistic ability and concentration are often strong suits for autistic individuals.
4) ADHD - UW 3 QID 5468 METHYLPHENIDATE TOXICITY - Most common side effect is loss of appetite, followed by sleep disturbance. Other side
effects include palpitations, tachycardia, and elevated blood pressure. Dilated pupils and dry mouth are typical.
- LT use → decrease in height and weight when compared to peers, particularly in younger children.
- Also, Methylphenidate use → associated with increased probability of drug abuse problems in adulthood.
- Toxicity manifestations to differentiate from regular side effects are: - Nervousness, euphoria, nausea, vomiting, dizziness, agitation, aggressiveness,
tachycardia, increased BP and mydriasis. - Mgmt → depending on the circumstances. Toxicologic evaluation and also
methylphenidate cannot be stopped abruptly due to high prevalence of psychological dependence, its dosage must be slowly tapered.

Emergency Medicine
UW3 QID 5468 - Choking Mgmt - Children with partial or complete obstruction should be kept NPO as this may result in
further airway compromise. - For partial obstruction after allowing spontaneous coughing, children should still be
taken to the hospital. - For unconscious pxt → start CPR with compressions, before performing (rescue
breaths), open the mouth and inspect for any foreign bodies that may have dislodged.