pediatrics report
DESCRIPTION
umsf pediatrcs report 5th yosTRANSCRIPT
UNIVERSITATEA DE STAT DE MEDICINA SI FARMACIA
"NICOLAE TESTEMITANU"
DIN REPUBLICA MOLDOVA
Department of pediatrics
Clinical examination and Medical Report.
Represented by : Shahwan Husein.
Professor: Lilia Romanciuc.
Year of study: 2014/2015
Group : 1548
Passport data:

1- Full name : Braga Elena Nicolae
2- Age : 13 years
3- Date of birth : 25/09/1999
4- Sex : fmale
5- Occupation: Student.
6- Home address : R.Leova S.tomai.
7- Date and time of beginning of dieses : Last summer 2013.
8- Date and time of admitting to clinic : 26.11.2014, 9:30.
9- Diagnosis of directing institution : Cardiac Congenital Malformation.
10- Clinical diagnosis : juvenile rheumatoid polyarthritis.A ) the base one : juvenile rheumatoid polyarthritis.raynaud syndrome.Anemia grade 1.Mitral valve prolapsed.Mitral insufficiency grade 1.Amigdalitis.
11- Operation : no
Complains of the Patient :
1- Pain in the knee joints.

2- Dizziness.3- Fatigue, tired when walking / doing sport
History of present disease :
Patient felt weakness or in other words incapability to maintain / doing normal school sports while all other student have been doing that sport normal without have pain and fatique so she went to the family doctor and during the examination he addressed her to the hospital for further examination in order to diagnose this situation more deeply and to help her return to school and have fun and to function normally like other kids are doing and also to prevent further complication and she was hospital here in 26.11.2014.
History of patient life:
1- Short biographical data : The child was born in leova ,the child was born normally , the life condition in the family is satisfactory , there is no other childrens at the family.The condition of the family good and he having her own apartmentand the girlhave her own room he feel comfortable .
2- Sex anamnesis : female.3- Bad habits : -
alcohol: negativeSmoking: negativeParent smoking : negative Parents alcohol consumption : negative
4- Allergic anamnesis : No allergy5- Family anamnesis and hereditary : the parents of the patient are
Healthy and there is no history and congenital diseases. 6- Weight at birth : 3600gr7- Height at birth :50cm8- Infection diseases :
Tb: NO.Syphilis: NO.

AIDS: NO.9- Medical insurance: state insurance.
The patient physical development :
The patient height :136cm.The patient weight : 45kg.Age :15 years.
A)percentile method interpretation : Height in cm :
Age 3% 10% 25% 50% 75% 90% 97%
15 126,3 129,4 133,0 137,0 142,0 146,7 149,2
Weight in kg:
Age 3% 10% 25% 50% 75% 90% 97%
15 23,9 25,6 28,2 31,4 35,1 39,7 44,7
The patient Height : 136 cm contributed to the 25%-75% .The patient weight : 45kg contributed to the 90%-97%. Conclusion : medium development of the height, high development in
weight according to percentile method of the child physical development.
B) Body mass index : BMI formula : (weight in Kilogram \ (Height in meter x Height in meter)). BMI Categories :Underweight : <18.5. Normal weight : 18.5-24.9.Overweight :25-29.9.Obesity : greater than 30 .
BMI: 21

Conclusion the patient include n the normal weight category with 21 body mass index.
The present of the patient :

General condition : the general condition of the patient are excellent after receiving the treatment
Consciousness : clear
Position of the patient : active
Expression of the face : Normal
Constitution : astenic , now the weight – 45 kg. Height : 136cm.
Nails : rose color
Edema : no signs of edema during palpation of the back above pelvic and on parasternal area and on lower legs
Visible mucosa : no visible changes in the clolor (yellow – jaundice , white-edema )
Mouth : lips are symmetrical , Tongue is moist symmetrical freely moved smooth ,mucosa pink color no visible ulceration area
Fatty tissue : its on average development , its thickness is 1,5 cm above the Traube space
Lymphatic vessels : -Occipital nodes: are not enlarged and are not painful.-Auricular nodes: are not enlarged and are not painful.-Para auricular nodes: are not enlarged and are not painful.-Submandibular nodes: are not enlarged and not painful on palpation-Mental nodes: are not enlarged and are not painful.-Posterior Cervical nodes: are not enlarged and are not painful.-Anterior Cervical nodes:

are not enlarged and are not painful.-Supraclavicular nodes: are not enlarged and are not painful.-Auxiliary nodes: are not enlarged and are not painful.-Cubital nodes: are not enlarged and are not painful.-Inguinal nodes: are not enlarged and are not painful.-Popliteal nodes: are not enlarged and are not painful.-Maleollar nodes: are not enlarged and are not painful.
Head :
head proportion is about 1/8 of body mass , and it was not pain during pressing on the following painful points on the supraorbital and suporbital areas and maxillar sinuses and mastoid process . Normal proportion with the body there is no signs of Acromegaly ,microcephaly or hydrocephaly )
Neak :
there is no pathological deformity , normal proportion . There is no pathological pulsation of carotid artery and the Jugular veins are not dilated .
Muscle :
3 degree of development and muscle power is 5 the child can resist to gravity and resistance , there is no sings of atrophy or indurations of the muscles
Bone :
there is no signs of deformity , and it was painless on pressing

Joints : there is no signs of deformity , no edema and no swelling in the joints its painless on palpation and there is no crepitus , no sighs of inflammation
Respiratory system

Complains : no complains.
Breath sound : normal breathing sound.
Cough : no cough
Sputum : no sputum
Expectoration with blood : NO
Pain in the chest : chest pain in left side.
Inspection :
Noise : participation of the wings of nose in the respiratory tract , there is no signs of eruptions , normal transparent discharge from the nose
Voice : normal voice.
Chest : normostenic , sub and supraclavisular fossa are good expressed , symmetrical participation of both halfes of the chest in respiration , there is no retraction of intercostals , no diverticuloms .
Mix type of breathing , superficial breathing , respiratory frequency is 20 per minutes
Palpation : normal elastic chest , no pain during palpation on the painful points on the chest ( par vertebral points ) . vocal fremitus was normal on both sides of the chest .
Percussion:
Comparative percussion : (it was clear pulmonary sound – resonance )
The points and the mechanism of comparative percussion :
we will compare right and left side of the chest beginning with the supraclavicular fossa and then on the clavicle then the first intercostals space from medial clavicular line then second intercostals space , then we will ask the patient to put his both hands over the head and we will make comparative percussion in the axillary fossa and the on the fourth and fifth and sixth intercostals spaces . and then on the back of the patient we will

begin from the suprascapular and then 2 times between the scapula and 2 times under the scapula .
Topographical percussion :
The points and the mechanism of topographical percussion :
First of all we will begin with the apex of the lung , in a healthy person the apex of lung is situated 2-3 cm above the clavicle . we will make percussion along the sternocleoidmastoid muscle of the neck its anteriorly and then we will go posteriorly and we will make the percusiion on the direction of the 7 cervical vertebra beginning from the shoulder and then we have to make the chronics field , it must be between 6-8 cm . we will find muscle trapeziums ad put our hand on it and then we will make percussion medially and laterally to it .and then we have to make the lower border of the lung , we will begin on the parasternal line putting our fingers on the second and third intercostals space and we will go tell the full dullness of the sound and the second line will be middle clavicle and then will be the anterior auxillary line and then posterior auxiliary line and then will be from the back the scapula line will begin from end of scapula in theses case will be found the lower border of the lung when we will connect all the points together . Then we will put our finger back on the patient on the last point that we found and the patient will inspire deeply and will keep the air in the chest and we will go down and then the patient will expire the air deeply and will keep the chest without air . Then we will go upper and then he will inspire . In these case we will found the motility of lower border of the lung . and after that we must make on the left scapula and at left 3 auxiliary lines , but we will not make at the anterior left part due to the presence of the heart .
Height of condition of apex of lung from front : 4 cm above the clavicle
Height of condition of apex of lung from behind : in the middle of the chronics field 3 cm laterally from the sterocleidmastoid muscle in the direction of 7 cervical vertebra
Lower border of the lungs according to classic lines

1-parathoracic : 10 cm
2-medioclavicular : 9 cm
3-anterior axillary : 9cm
4- middle axillary : 8 cm
5- posterior axillary : 8 cm

6-scapular : 6 cm
7-prevertebral : 10 cm
Mobility of the lower edge of the lung along the medioclavicular line : 2 cm
Auscultation
The points of vesicular breathing auscultation are :
Anteriorly – 5 pairs of points
1- Supraclavicular points 2- Subclavicular points ( first intercostals space ) under the previous point 3- Second intercostals space , under the previous point 4- Third intercostals space , at the margin of pectoral muscle 5- Fourth intercostals space , at the margin ofpectoral muschle under the
previous point
Laterally – 3 pairs of points
1- In the auxillary fossa 2- Under the previous point with one intercostals space 3- Under the previous point with one intercostals space
Posteriolly – 4 (5-6) pairs of points
1- Above the scapula2- In the interscapular space 3- In the interscapular space , under ther previous points 4- Under the scapulae
Mechanism for auscultation of vesicular breathing : here we will make exactly like the point we used in comparative persusion , we will begin with right apex and then left apex , then to the first intercostals space of the middle clavicular life on right side then on left one , then to the second intercostals space of the middle clavicular line on right and left side , after that we will go to the auxillary fossa on right side then on left side and then near the mamilon , laterally to the mamilon on right and then on left side , so together they will be 5 points , in each of these 5 points when we will put

the stethoscope we need to hear in inspiration and expiration .After that the patient will put his hand o this head and we will begin on the first 4 inercostal space on the middle axillary line down of the auxillary fossa on the right side and then on the left side. And then we will begin from the opposite side beginning from point on the clavicle on both sides and then 2 imes on 2 points between the scapular on both sides and then on one point on the inferior angle of the scapula and then one point a little down on right and then on left .
The character of breath : vesicular breath sound
Secondary respiratory sounds : no
Blood circulating system
Complains
Dizziness, weakness.

Pains in the heart : pain in the left side.
Edema : No signs of edema upon palpation of the parasternal area and on the back above the pelvic and on lower extremity
The difference between cardiac and renal edema:
1 – Cardiac edema – appear in the evening after physical effort and cold on palpation , dull , cyanotic , appear from lower to upper extremity , will never disappear with help of diuretics
2-renal edema – appear in the morning , warm on palpation , soft , pale , appear in the morning , appear from upper limb to lower limb , can disappear and without help of diuretics
Expectoration with blood : No
Fatigue : present.
Dizziness : present.
Palpitation : present.
Examination
The condition of the vessel of neck : normal pulsation of carotid artery , normal JVP
Inspection :
1- Apex beat : pulsation of the apex beat at the level of 4 intercostal space 1-1.5 cm laterally from left midclavicular line
2- Of peripheral vessels : carotid pulse –synchronous to the heart beat , Jugular pulsation – absent , Varicous veins of lower extremity – not present
Palpation :

1-location : pulsation of the apex beat at the level of 4 intercostal space 1-1.5 cm laterally from left midclavicular line
2- Surface : 1 cm
3- amplitude : high
4- resistance
Percussion :
Relative dullness
1- Right border : 4th intercostals space 1 cm laterally of R. adge 2- Left border : 4th intercostals space 1 – 1.5 cm from left midclavicular
line 3- Upper border : 3th intercostals space 1 cm to the left sterna
Absolute dullness
1- Right border : 3 intercostal space on left edge of sternum 2- Right border : 1-1.5 cm medially from the left border of relative
dullness 3- Upper border : 1 intercostals space down from of relative 4th
Auscultation :
Characteristics of the cardiac sounds :
-Sound 1:Spliting of the first sound
-better heard at the apex.
Sound 2:-heard at the base of the heart of same intensity upon the aortic and pulmonary valves.
Sound 3 : not heard.
Sound 4 : not heard.
Points of auscultation :

1- Mitral : at the apex , in the 4th left intercostals space 1-1,5 cm medially to midclavicular life
2- Tricuspid : at inferior edge of xiphoid 3- Pulmonary valve : at its anatomical projection at the 2th left intercostals
space 4- Aortic valve : at the 2th right intercostals space 5- Botkin - Erb point : left to sternum on 3th and 4th intercostals space ,
they are associated with coarctation of aortic valve .
Characteristic and murmurs :
1- Systolic ejection murmur that is attributed to the pulmonary valve ( these is due increase blood flow throght pulmonary valve )
2- Splitting if the second heart sound
Examination of vessels:
1-palpation of radial and femoral artery is coincide with the apex beat and its similar at both hands
3- examination of the veins , no sings of hyperemia or induration , absent of varicose dilatation
Blood pressure : 80/47 mmHg
Digestive System
Complains:
Pain in the abdomen : no pain was during palpation of the abdomen
Dyspeptic manifestation : no signs of vomiting , no sickness , no heartburn , no belch
Appetite :normal

Dysphagia : no
Heartburns : no
Vomiting : absent
Nausea : absent
Thirst : no
Loss of weight : no , weight at birth was 3,8kg and now is 6 kg
Bleeding : no signs of esophageal or gastrointestinal bleeding no signs of melena or vomiting of blood
Stool : Clear.
Examination of abdominal cavity :
Mouth cavity : normal smell , clear moist pink to red mucous membrane , there is no signs of septum deviation
Tonsils : are not enlarged
Tounge : pink to red , moist , without signs of ulceration or edema
Gum : pink to red , without presense of gray edging , no necrosis , absent of hyperemia
Teeth : normal development.
Examination of abdomen
Inspection :
Normal scaphoid shape of the abdomen , not distended
Symmetry : both sides are symmetrical , no protrusions are noticed
Scars are not found
Palpation :
Superficial palpation:
-Tenderness of abdomen: painless-Irritation of peritoneum: negative Blumberg’s symptom.-Abdominal muscles: not divaricating.-Hernia of linea Alba: not present .-Tumors: not present.
Deep palpation:
-Sigmoid part: painless and elastic.-Caecum: painless and elastic.-Terminal end of ileum: painless and elastic.

-Ascending colon: painless and elastic.-Descending colon: painless and elastic.-Transverse colon (2cm below stomach): painless and elastic .-Stomach: painless.
Auscultation : bowel sound are present
Persussion :
Tympanic sound
Ascitis is not present , dullness was not heard.
Liver and gallbladder :
Inspection :
No sings of Hepatomegaly , or right hypochondriac area enlargement
Percussion :
Normal liver dimensions : - Between 1st and 2nd points – 10 cm - Between 3rd and 4th points – 9cm - Between 3rd and 5th points – 8 cm.
Palpation of area of gallbladder : no signs of pain
De Mussy-Georgievsky, Ortner's, Obraztsov-Murphy, and Vasilenko's symptoms are Negative.1. Vasilenko`s symptom – sharp pain in the region of the gall bladder when it is tapped over at the height of inspiration.2. Obraztsov-Murphy symptom - sharp pain in the right hypochondrium when the examiner` hands press the gall bladder at the height of inspiration.3. Ortner`s symptom – pain during tapping over the right costal arch by the edge of the hand.4. The de Mussy-Georgievsky symptom – tenderness at the point of the phrenic nerve, between the heads of the sterno-cleidomastoid muscle.

Spleen
Inspection : no signs of diffuse or local protrusion
Percussion : no signs of splenomegaly
Technique of percussion :
NOTE: Percussion may indicate but does NOT confirm splenomegaly.
With patient supine, percuss inferior to lung resonance to map out gastric tympany (i.e. Traube’s Space).
o This area is variable; however, tympanic extending laterally makes splenomegaly less likely.
o Dullness may indicate splenomegaly, solid gastric content, or colon content.
Splenic Percussion Sign (Castell’s Sign): Percuss the most inferior interspace on the left anterior axillary line (Castell’s Point). This is usually tympanic. Ask pt to breath deeply.
o Remains tympanic on inspiration: Splenic Percussion Sign negative: splenomegaly less likely.
o Shift from tympanic to dullness: Splenic Percussion Sign positive: splenomegaly more likely.
Palpation : No signs of spleenmegaly
Technique of palpation :
Start in RLQ (so you don’t miss a giant spleen). Get your fingers set then ask patient to take a deep breath. Don’t
dip your fingers or do anything but wait. When patient expires, take up new position. Note lowest point of spleen below costal margin, texture of splenic
contour, and tenderness

If spleen is not felt, repeat with pt lying on right side. Gravity may bring spleen within reach.
o “LET THE SPLEEN PALPATE YOUR FINGERS AND NOT THE OTHER WAY AROUND. THERE IS NO GOLD, SO DON’T DIG!”
o Remember that the spleen can become very enlarged and fragile (e.g. in mononucleosis); overly aggressive palpation may cause injury.
Pancreas
Palpation : No signs of pain
Mechanism of pancreas palpation : the fist of the left hand is placed under the join . palpation is carried out the right hand when child exhaled
Urinary system
Complains :
Edemas: no isn’t present.
Pain: isn’t present in lumbar or pubic region.
Urination: frequent painless normal urination.
(No sings of polyuria,olyguria,anuria,isuria ,disuria or stranguria)
Urine quantity: 1400ml/24hours. Color: yellow
Inspection :
Swelling: no hyperemia in lumbar area.
Palpation :
The inferior pole of both kidneys were palpated
Mechanism of kidney palpation :
Mechanism of Palpation of the Left Kidney.

Move to the patient’s left side. Place your right hand behind the patient, just below and parallel to the 12th rib, with your fingertips just reaching the costovertebral angle. Lift, trying to displace the kidney anteriorly. Place your left hand gently in the left upper quadrant, lateral and parallel to the rectus muscle. Ask the patient to take a deep breath. At the peak of inspiration, press your left hand firmly and deeply into the left upper quadrant, just below the costal margin. Try to “capture” the kidney between your two hands. Ask the patient to breathe out and then to stop breathing briefly. Slowly release the pressure of your left hand, feeling at the same time for the kidney to slide back into its expiratory position. If the kidney is palpable, describe its size, contour, and any tenderness.
Alternatively, try to feel for the left kidney using a method similar to palpating the spleen. Standing at the patient’s right side, with your left hand, reach over and around the patient to lift up beneath the left kidney, and with your right hand, feel deep in the left upper quadrant. Ask the patient to take a deep breath, and feel for a mass. A normal left kidney is rarely palpable.
Mechanism of Palpation of the Right Kidney.
To capture the right kidney, return to the patient’s right side. Use your left hand to lift up from the back, and your right hand to feel deep in the right upper quadrant. Proceed as before.
A normal right kidney may be palpable, especially when the patient is thin and the abdominal muscles are relaxed. It may be slightly tender. The patient is usually aware of a capture and release. Occasionally, a right kidney is located more anteriorly and must be distinguished from the liver. The edge of the liver, if palpable, tends to be sharper and extend farther medially and laterally. It cannot be captured. The lower pole of the kidney is rounded.
Percussion :
Giordano symptom is negative.
Mechanism of Percussion Tenderness of the Kidneys.
If you find tenderness when examining the abdomen, also check each costovertebral angle. Pressure from your fingertips may be enough to elicit

tenderness; if not use fist percussion. Place the ball of one hand in the costovertebral angle and strike it with the ulnar surface of your fist. Use enough force to cause a perceptible but painless jar or thud
Urinary bladder size: No signs of increased size of urinary bladder
Mechanism of percussion of urinary bladder : Percuss from symphasis pubis ( urine filled gived dull sound )
Endocrine system
Complains : no thrist , no polyuria , no signs of itchy skin , no sighs of weight loss ,
Examination : no signs of weight loss – weitht at birth 3.8kg and now 6kg
No signs of acromegaly , no signs of moon shaped face , no sighs of hyper or hypopidmentation , normal distribution of fat under the skin lager ,
Palpation : normal size of thyroid gland ( a normal thyrod is estimated to be 10 grams with an upper limit of 20 grams or 2 to 4 teaspoons )
Inspection : no signs of thyroid gland enlargamet
Mechanism of Examination of the thyroid gland :
A normal thyroid is estimated to be 10 grams with an upper limit of 20 grams or 2 to 4 teaspoons.
Examination for goiter can increase the possibility of thyroid disease in patients with symptoms of hypo- or hyperthyroidism, in determining the choice of treatment in hyperthyroidism and monitoring the response to therapy directed at decreasing the size of the thyroid in cases of symptomatic goiter.
The examination consists of three portions:
Inspection, Palpation, and Synthesis of data from these techniques

In addition to palpating for size, also note the gland texture, mobility, tenderness and the presence of nodules.
Inspection
Inspection: Anterior Approach
1. The patient should be seated or standing in a comfortable position with the neck in a neutral or slightly extended position.
2. Cross-lighting increases shadows, improving the detection of masses.3. To enhance visualization of the thyroid, you can:
1. Extending the neck, which stretches overlying tissues2. Have the patient swallow a sip of water, watching for the upward
movement of the thyroid gland.
Inspection: Lateral Approach
1. After completing anterior inspection of the thyroid, observe the neck from the side.
2. Estimate the smooth, straight contour from the cricoid cartilage to the suprasternal notch.
3. Measure any prominence beyond this imagined contour, using a ruler placed in the area of prominence.
Palpation
Note: There is no data comparing palpation using the anterior approach to the posterior approach so examiners should use the approach that they find most comfortable.
Palpation: Anterior Approach
1. The patient is examined in the seated or standing position.2. Attempt to locate the thyroid isthmus by palpating between the cricoid
cartilage and the suprasternal notch.3. Use one hand to slightly retract the sternocleidomastoid muscle while
using the other to palpate the thyroid.4. Have the patient swallow a sip of water as you palpate, feeling for the
upward movement of the thyroid gland.

Palpation: Posterior Approach
1. The patient is examined in the seated or standing position.2. Standing behind the patient, attempt to locate the thyroid isthmus by
palpating between the cricoid cartilage and the suprasternal notch.3. Move your hands laterally to try to feel under the sternocleidomstoids
for the fullness of the thyroid.4. Have the patient swallow a sip of water as you palpate, feeling for the
upward movement of the thyroid gland.
Synthesis of data from these techniques
Using the data from anterior and lateral inspection and from palpation, categorize the gland as:
a. goiter ruled out [normal or small (1 to 2 times normal) with lateral prominence <2 mm ],
b. goiter ruled in [large (& 2 times normal) or lateral prominence >2 mm] or
c. inconclusive.
Nodules: Examination of the thyroid for nodularity
Thyroid nodules are common (prevalence 4%). Half of the thyroids glands examined by ultrasound or direct visualization (surgery or autopsy) have nodules. Physical examination detects approximately 10% of the nodules found by these methods. Nodules increase in frequency with age and are four times more likely in women than men. Less than 5% of all nodules are cancerous
Nerve psychic condition and sense organs
Consciousness : clear
Mood : Calm.
Sleeping : usually with superficial sleep
Headache : not present
Preliminary diagnosis:
the patient admitted to the hospital in 27\11\2014 complaining from pain in his chest, weakness, vision disturbances , dizziness. The mother mentioned that the last year in summer the same signs happened to him and he went to the doctor and the doctor give him magnesium(4,2x2times per day orally) to reduce the symptomatic signs.
The patient this year felt the same sings and symptoms in November this year (pain in his left part of his chest, dizziness, weakness, fatigue) .
In Objective signs : pale skin, abnormal heart rate, moderate intensity of murmur
Apex beat if felt in many intercostals spaces.

Plan of examination of patient
1- Biochemical exam.2- Blood analysis.3- Immunological test. 4- Urine.5- Echocardiography.6- Chest x-ray.7- Electrocardiography .8- Ultrasound of abdomen.
Results from performed laboratory and instrumental investigations
1- Biochemical exam :

Test result Normal values
Total protein 75 65-85g\L
Urea 1,7 2,5-6,5mmol\L
Creatinine 67 53,0-97,0umol\L
Total bilirubin 9,0 0,17mkmol\L
Glucose 5,3 3,89-5,83mmol\L
ALAT 11 <33U\L
ASAT 27 <32U\L
LDH 228
CK 89
CK-MB 45
Total Cholesterol 4,8 0-5,2mmol\L
B-Lipoprotein 51
Potassium 52
Sodium 140
Calcium 2.45
Iron 11,8

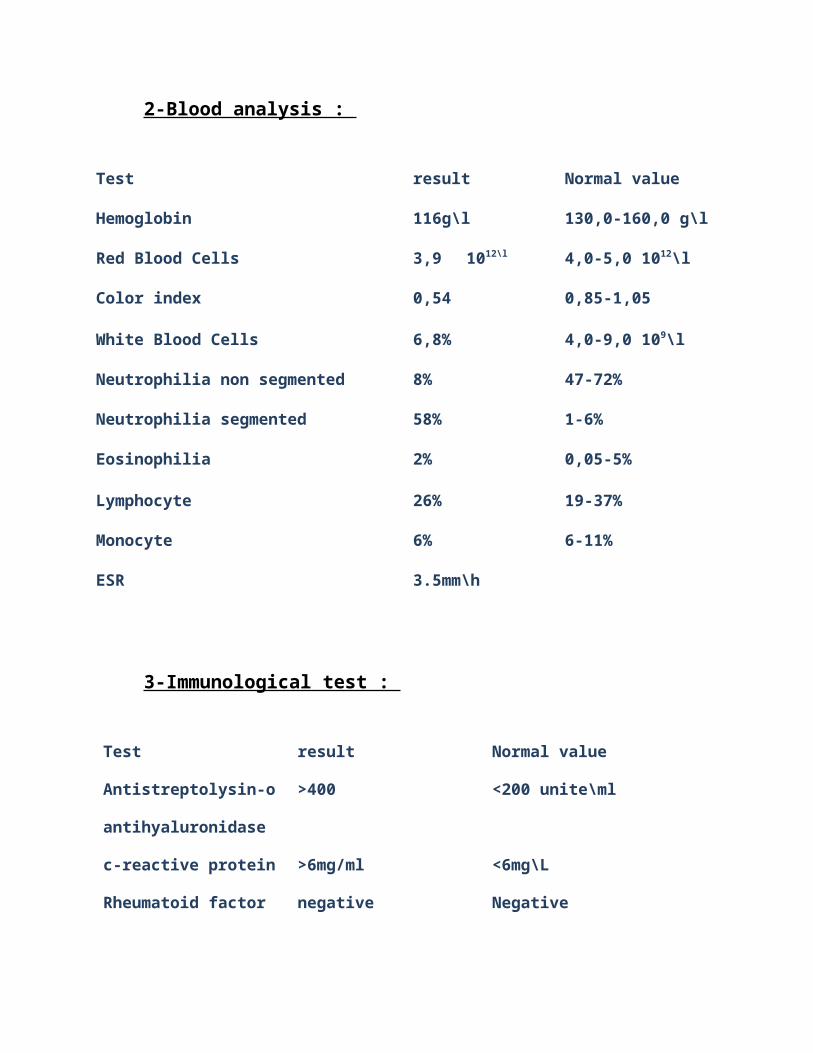
2-Blood analysis :
Test result Normal value
Hemoglobin 116g\l 130,0-160,0 g\l
Red Blood Cells 3,9 1012\l 4,0-5,0 1012\l
Color index 0,54 0,85-1,05
White Blood Cells 6,8% 4,0-9,0 109\l
Neutrophilia non segmented 8% 47-72%
Neutrophilia segmented 58% 1-6%
Eosinophilia 2% 0,05-5%
Lymphocyte 26% 19-37%
Monocyte 6% 6-11%
ESR 3.5mm\h
3-Immunological test :
Test result Normal value
Antistreptolysin-o >400 <200 unite\ml
antihyaluronidase
c-reactive protein >6mg/ml <6mg\L
Rheumatoid factor negative Negative

4- Urine analysis :
Test Result Normal value
Quantity 50 10-500ml
Color Yellow Yellow
Transparency transparent Transparent
Relative density 1020 1000-1030
Reaction acid Acid
Epithelial Moderate c\moderate-c\small
Leucocytes _ 0-3 c\v
Glucose _ 0-0 c\v
Proteins negative negative
Bacteria _ negative
Salts _ negative
Erythrocye _ negative
5- Echocardiography
Ascending aorta 20 20-40mm
Descending aorta 20-36mm Pulmonary artery 11-28mm
Right atrium 23 19-40mm Left atrium 18*21 20-40mm
PAVD 2-5mm VtD VS 79 53-15ml
VD 14 7-28mm VtS VS 26 23-76ml
SIV 6-11mm FS VS 37 26%

DtD VS 42 35-36mm FE VS 67 50%
DtS VS 23 25-40mm VB
6- Chest x-ray :The heart is enlarged. Cardiac silhouette is enlarged due to each and other cavities. Right atrial dilation is depicted by bulging of superior portion of the right inferior arch. Left atrial dilation is depicted by the bulging of the inferior portion of the left middle arch. Hypertrophy and dilation of the ventricules are depicted by rounded left inferior arch. Pulmonary arteries are dialted and pulmonary vascularisation is increased. The increase in the peripheral transparency of the lung fields suggests pulmonary vascular obstruction.
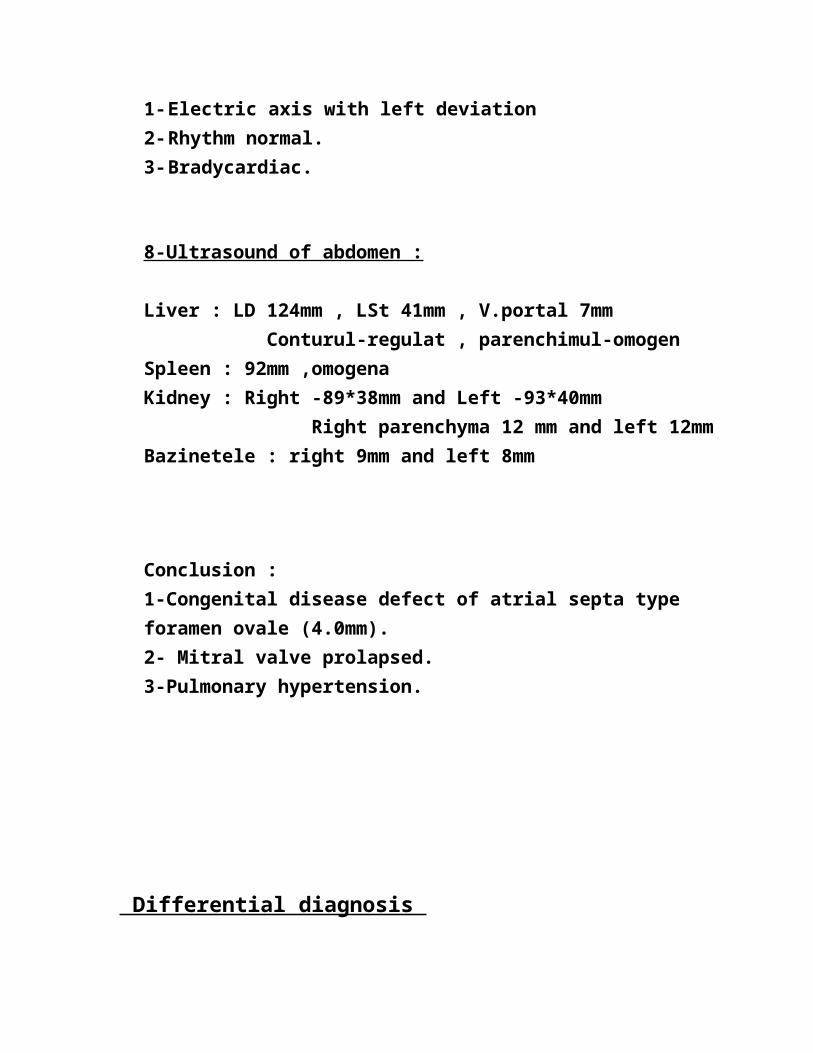
7--Electrocardiography :
1- Electric axis with left deviation 2- Rhythm normal. 3- Bradycardiac.
8-Ultrasound of abdomen :
Liver : LD 124mm , LSt 41mm , V.portal 7mm Conturul-regulat , parenchimul-omogenSpleen : 92mm ,omogena Kidney : Right -89*38mm and Left -93*40mm Right parenchyma 12 mm and left 12mmBazinetele : right 9mm and left 8mm
Conclusion : 1-Congenital disease defect of atrial septa type foramen ovale (4.0mm).2- Mitral valve prolapsed.3-Pulmonary hypertension.
Differential diagnosis
Condition Differentiating signs and symptoms
Differnating Test
Partial anomalous pulmonary venous drainage
Signs and symptoms similar to atrial septal defect
Atrial septum intact with dilated right heart structures: identified by echocardiography in children, and MRI or CT in adults.
Ventricular septal defect Small ventricular septal defects (VSDs) are associated with a holosystolic murmur and normal first and second heart sounds. With a larger shunt volume (ratio of pulmonary to systemic blood flow, Qp:Qs, >2), a mid-diastolic mitral valve flow murmur may be heard in addition to a holosystolic mid-
VSD identified by Doppler echocardiography.

frequency murmur.
Patent ductus arteriosus Associated with prematurity. Patent ductus arteriosus is also associated with bounding peripheral pulses due to wide pulse pressure. The left ventricular impulse may be prominent. The murmur associated with a patent ductus arteriosus is often described as a machinery-like continuous murmur. However, in some premature and newborn infants the murmur can be heard only in systole. A mid-diastolic mitral valve flow murmur may be heard.
PDA identified by Doppler echocardiography.
Pulmonary stenosis A click follows the first heart sound, which is best heard at the left upper sternal border.
The second heart sound may be normal, split, or single depending on the severity of the stenosis.
Pulmonary stenosis identified by Doppler echocardiography
Right bundle-branch block Can produce a widely split second heart sound similar to that
ECG shows right bundle-branch block.
Echocardiography
heard in patients with an ASD.
The characteristic ASD murmurs are absent.
shows no evidence of an ASD
Other congenital heart defects ASDs occur in the context of other congenital heart conditions, including transposition of the great arteries, pulmonary atresia, and Ebstein's anomaly.
Abnormal anatomy identified by Doppler echocardiography.
Clinical diagnosis :
1-Congenital disease defect of atrial septa type foramen ovale (4.0mm).2- Mitral valve prolapsed.3-Pulmonary hypertension.4-deregulation of cardiac rhythm.5- Sinus Bradycardiac. 6-insufficient of cardiac function grade 1 after NYHA.
Epycrisis :
1. First name: Bologan
2. Last name :Sergiu.
3. Date of birth:2\2\2004
4. Sex : boy
5. Date of hospitalization:27/11/14
6. Department of : cardiology
7. Occupation: student of 5th grade at middle school
8. Address: R.Glodeni.S.Zimbreni.
9. Diagnosis:

a)base one: Congenital Heart Disease.
b)accompanying disease:1- atrial septa type foramen ovale (4.0mm).2- Mitral valve prolapsed.3-Pulmonary hypertension.4-deregulation of cardiac rhythm.5- Sinus Bradycardiac.
6-insufficient of cardiac function grade 1 after NYHA
c)complication:
Specific complications of congenital heart defects depend on the type and severity of the
particular condition.
The following conditions can develop as complications of congenital heart defects:
Endocarditis (inflammation of heart tissue due to a bacterial infection) can develop any
time bacteria enter the bloodstream. Before dental procedures and minor surgeries,
children with certain congenital heart defects are advised to take preventative
antibiotics to avoid this complication.
Delayed growth, learning disabilities, developmental delays
Cyanosis, fainting, seizures (sudden death also can occur)
Mental retardation due to lack of oxygen to the brain at birth
Structural damage to the heart chambers and major blood vessels near the heart
Pulmonary hypertension (high blood pressure in the arteries of the lungs)
Congestive heart failure (CHF) is a condition in which the heart becomes unable to
pump an adequate amount of blood through the body. A person with congestive heart
failure becomes tired and short of breath easily.
Premature heart disease
Arrhythmia (irregular heart rate)
Stroke (brain attack)
10-methods of examination:

CBC: Erythrocytes3,9 ,non segmented neutrophils 8 , ESR 4, Leukocytes 6,8.
Biochemical Blood analysis: Urea 1,7 , ALAT 20 ,Total protein 75, ASAT 27 , Creatinine 67.
Immunoserologicaltest: Antistreptolysin-o>=400 , CRP (-), RF(-).
ECG: sinus bradycardic. EchoCG: Mitral valve prolapse 1st degree 5mm.
Treatment :
1- Captopril 6.25mg/2times per day ( its an angiotensin converting enzyme inhibitor used to treatment of hypertension and congestive heart failure )
2- Verosprion (Spironolactone ) 12.5mg/5 times day ( is used primarily as
a diuretic and antihypertensive, but may also be employed for the purpose of reducing elevated or unwanted androgen activity in the body. It acts predominantly as an antagonist of the mineral corticoid and androgen receptors, and in relation to its antimineralocorticoid effects, belongs to a class of pharmaceutical drugs known as potassium-sparing diuretics.)
3- tinctura valeriana 10 drops\2times per day orally.( use as a sedative, antiseptic,
anticonvulsant, migraine treatment and pain reliever, most basic science research has been directed at the interaction of valerian constituents with the GABA neurotransmitter receptor
system).
4- Vitamin E 30% 5 drops\2 times per day orally.( Vitamin E has many biological
functions, the antioxidant function being the most important and best known. Other functions include enzymatic activities, gene expression, and neurological function(s). The most important function of vitamin E has been suggested to be in cell signaling (and it may not have a significant
role in antioxidantmetabolism).
5- Magnesium 4,2mg\2 times per day orally.( Magnesium is the second most plentiful
cation of the intracellular fluids. It is essential for the activity of many enzyme systems and plays an important role with regard to neurochemical transmission and muscular excitability. Magnesium sulfate reduces striated muscle contractions and blocks peripheral neuromuscular transmission by reducing acetylcholine release at the myoneural junction. Additionally, Magnesium inhibits Ca2+ influx through dihydropyridine-sensitive, voltage-dependent channels.
This accounts for much of its relaxant action on vascular smooth muscle).
Recommendation:
Diet : Nr10 which includes rich potassium products such as bananas, sweet potatoes , tomatoes sauce, beans, soybeans , yogurt, milk, clams sea food , fish, prunes, carrot juice, orange juice.
Activity: Initially place patient in bed rest followed by a period of indoor activity before they are permitted to return to the school , do not allow full activity until the general state of patient returned to normal.

Patient education: timely evaluation of physical changes that decreases his physical state and or pathological changes which appears on his body.Timely permit medication and memorize each drug on which time exactly and for what pathology.
Outpatient car: -patient usually demonstrate significant improvement after initiation of anti inflammatory therapy; however , do not allow patients to resume full activities until all clinical symptoms and laboratory values have resumed to normal.-importance of prophylaxis against recurrent streptococcal pharyngitis ,patient should remain under antibiotic prophylaxis at least until the early third decade of life.-monitor patients routinely each month for the signs and symptoms of mitral valve prolapse and arrhythmia .-monthly perform laboratory tests such as CBC, Biochemical blood analysis ,Urine analysis.And imagistic such as Abdominal USG, ECG, Echo, X-Ray ,For chest or extremities if necessary, examination for monitoring the disease and the patient recovering.

Evaluation of disease:
Pain in chest and fatigue while running / doing sport , general weakness ,vision clear,
It start from the last year, after this event he took medication to relive the symptomatic signs ,this year in this period he came again with this symptoms.
Objective examination : normal skin mucosa , mucosa of pharynx
Normal.
Normal breathing in auscultation , Sinus bradycardia , abdomen normal without pain .
Para clinical examination : blood analyses normal , urine normal
PCR (-), rheumatoid factor (+) .
Diary of observing of the patient :
Date 28\11\2014 29\11\2014 30\11\2014
Temperature 36,7 36,5 36,4
RR 20 23 22
Auscultation of lung Vesicular sound, normal breathing
Vesicular sound, normal breathing
Vesicular sound, normal breathing
Pulse 64 63 62
BP 110\80 109\75 112\80
Auscultation of cardiac
Moderate intensity of systolic murmur by 2-3 degree.
Moderate intensity of systolic murmur by 2-3 degree.
Moderate intensity of systolic murmur by 2-3 degree.
Skin color Normal skin Normal skin Normal skin
Vomiting Neg Neg Neg

Prognosis :
In majority of the cases evolution is favourable. 50 – 60% of the cases close spontaneouslyand the rest reduces in the size of defect significantly. Stature is normal.VSD with left-to-right shunt (diameter more than 1 cm) and pulmonary arterial hypertension havethe following clinical manifestations:• Signs appear from the first day or week of life;• Dyspnea with tachypnea;• Cough;• Drawing of intercostals muscles;• Profuse transpiration;• Growth curve stationary or slow ascending;• Recurrent bronchopulmonary infections, short stature, pallor of skin;• Deformed thorax, bulge in the upper portion;• Frequently noted hepatomegaly;• Apex beat is down and pushed lateral• Systolic thrill on palpating the precordial region. Systolic murmur is followed byaccentuated second heart sound. VSD with pulmonary hypertension leads to low intensitysystolic murmur and marked second heart sound.X-ray findings:• Cardiomegaly (cardio-thoracic index 0,6 – 0,65); moderate enlargement of both left atrium andventricle.• Hilar and perihilar pulmonary vessels are dilated and pulmonary fields are accentuated.ECG:Increased volume in the left cavities. Overloading of right ventricle may lead to pulmonaryhypertension. Biventricular hypertrophy is found.

ECHO cardiography:Right ventricular dilatation and pulmonary artery dilatation may be found. Ventricular septal defect
can be seen
Juvenile Idiopathic Arthritis
Juvenile rheumatoid arthritis (JRA) is the most common chronic rheumatologic disease in children and is one of the most common chronic diseases of childhood. The etiology is unknown, and the genetic component is complex, making clear distinctions between the various subtypes difficult. A new nomenclature, juvenile idiopathic arthritis (JIA), is being increasingly used to provide better definition of subgroups.
Children exposed to antibiotics may be at greater risk for juvenile arthritis
In a nested case–control study of 153 children with juvenile arthritis and 1,530 matched controls, researchers found that exposure to antibiotics during childhood significantly increased the risk for developing JIA (adjusted odds ratio = 2.6) in a dose-dependent manner. Compared with those with no exposure, the odds ratio for developing JIA was 3.1 for children exposed to one or two courses of antibiotics, and for those exposed to three to five courses the odds ratio was 3.8.[1]
The association between antibiotic exposure and JIA was similar for different classes of antibiotics. No association was found between exposure to nonbacterial antimicrobial agents and JIA. Adjustment for the number and type of infections and age at antibiotic exposure did not change the associations significantly.[1]
Management
A team-based approach to the treatment of JIA can be helpful. Management may include 1 or all of the following areas:
Pharmacologic therapy with nonsteroidal anti-inflammatory drugs (NSAIDs), disease-modifying antirheumatic drugs (DMARDs), biologic agents, or intra-articular and oral corticosteroids
Psychosocial interventions Measures to enhance school performance (eg, academic counseling) Improved nutrition Physical therapy Occupational therapy
American College of Rheumatology (ACR) criteria for complete remission are as follows[2] :

No inflammatory joint pain No morning stiffness No fatigue No synovitis No progression of damage, as determined in sequential radiographic examinations No elevation of the ESR and CRP level
The ACR recommends treatment approaches to JIA on the basis of the following 5 treatment groups[3] :
A history of arthritis in 4 or fewer joints A history of arthritis in 5 or more joints Active sacroiliac arthritis Systemic arthritis without active arthritis Systemic arthritis with active arthritis
Within each group, choice of therapy is guided by the severity of disease activity and the presence or absence of features indicating a poor prognosis.
Advances in medical treatment have reduced the need for surgical intervention. Procedures that may be considered in specific circumstances include the following:
Synovectomy Osteotomy and arthrodesis Hip and knee replacement
See Treatment and Medication for more detail.
Image library
Sequelae of chronic anterior uveitis. Note the posterior synechiae (weblike attachments of the pupillary margin to the anterior lens capsule) of the right eye secondary to chronic anterior uveitis. This patient has a positive antinuclear antibodies (ANAs) and initially had a pauciarticular course of her arthritis. She now has polyarticular involvement but no active uveitis. Image courtesy of Carlos A. Gonzales, MD.

Etiology and Pathophysiology
The etiology and pathogenesis of JIA are not completely understood. Genetic susceptibility plays a major role, but there is significant overlap between loci associated with JIA and those associated with other autoimmune diseases.[7]
JIA is a genetically complex disorder in which multiple genes are important for disease onset and manifestations. The IL2RA/CD25 gene has been implicated as a JIA susceptibility locus, as has the VTCN1 gene.[8] Associations have been found between specific HLA alleles and clinical subtypes of JIA (eg, HLA-A(*)02:06 with susceptibility to JIA accompanied by uveitis, and HLA-DRB1(*)04:05 with polyarticular JIA, in a Japanese cohort).[9]
Humoral and cell-mediated immunity are involved in the pathogenesis of JIA. T lymphocytes have a central role, releasing proinflammatory cytokines (eg, tumor necrosis factor–alpha [TNF-α], interleukin [IL]-6, IL-1) and favoring a type-1 helper T-lymphocyte response. A disordered interaction between type 1 and type 2 T-helper cells has been postulated.
Studies of T-cell receptor expression confirm recruitment of T-lymphocytes specific for synovial nonself antigens. Evidence for abnormalities in the humoral immune system include the increased presence of autoantibodies (especially antinuclear antibodies), increased serum immunoglobulins, the presence of circulating immune complexes, and complement activation.
Chronic inflammation of synovium is characterized by B-lymphocyte infiltration and expansion. Macrophages and T-cell invasion are associated with the release of cytokines, which evoke synoviocyte proliferation. A study by Scola et al found synovium to contain messenger ribonucleic acid (mRNA) for vascular endothelial growth factor and angiopoietin 1, as well as for their receptors, suggesting that induction of angiogenesis by products of lymphocytic infiltration may be involved in persistence of disease.[10]
Some pediatric rheumatologists view systemic-onset JIA as an autoinflammatory disorder, such as familial Mediterranean fever (FMF) or cryopyrin-associated periodic fever syndromes, rather than a subtype of JIA. This theory is supported by work demonstrating similar expression patterns of a phagocytic protein (S100A12) in systemic-onset JIA and FMF, as well as the same marked responsiveness to IL-1 receptor antagonists.[11]
FMF is associated with mutations in the MEFV gene; these mutations are associated with activation of the IL-1b pathway, resulting in inflammation. A study by Ayaz et al found an increased frequency of MEFV mutations in Turkish children who were diagnosed with systemic JIA[12] ; this study has not been replicated in other populations.

Epidemiology
United States statistics
Approximately 300,000 children in the United States are estimated to have some type of arthritis. The incidence rate estimates for JIA range from 4-14 cases per 100,000 children annually; for JRA, the prevalence has ranged from 1.6 to 86.1 cases per 100,000.[13] These wide-ranging numbers are attributable to differing definitions and criteria for childhood arthritis; population differences, including environmental exposure and immunogenetic susceptibility; and difficulty in case ascertainment and lack of population based data.
International statistics
Worldwide, JIA appears to occur more frequently in certain populations (eg, indigenous peoples) from such disparate areas as British Columbia and Norway. A study in Sweden found the prevalence of JIA there to be similar to that in Minnesota, approximately 85 cases per 100,000 population, with an incidence of 11 cases per 100,000 population. A study from Germany found a prevalence rate of 20 cases per 100,000 population, with an incidence rate of 3.5 cases per 100,000 population.
Estimates from Norway include a prevalence rate of 148 cases per 100,000 population with an incidence rate of 22 cases per 100,000 population. The incidence of JIA in Japan has been reported to be low.
Disease-associated mortality for JIA is difficult to quantify, but it is estimated to be less than 1% in Europe and less than 0.5% in North America. Most deaths associated with JIA in Europe are related to amyloidosis, and most in the United States are related to infections.
The approximate frequencies of the various forms of JRA are as follows:
Oligoarticular - 30% Polyarticular RF negative - 20% Polyarticular RF positive – 5% Systemic-onset – 5% Psoriatic - 5% Enthesitis Related – 25% Undifferentiated – 10%
Sexual differences in frequency
Girls with an oligoarticular onset outnumber boys by a ratio of 3:1. In children with uveitis, the ratio of girls to boys is 5-6.6:1, and in children with polyarticular onset, girls outnumber boys by 2.8:1. In striking contrast, systemic-onset occurs with equal frequency in boys and girls. Boys outnumber girls with enthesitis-related arthritis.[14]
Age-related differences in frequency
Although JIA is defined as arthritis beginning before age 16 years, the age at onset is often much lower, with the highest frequency occurring in children aged 1-3 years.[15] This age distribution is most evident in girls with oligoarticular JIA and psoriatic arthritis.

Polyarticular RF-negative JIA has a biphasic peak of onset; the first is at a young age (1-4 y), similar to oligoarticular JIA, and the second peak is at age 6-12 years. RF-positive disease is more common in adolescents. Systemic-onset JIA is not characterized by a peak age of onset; it is spread across the childhood years. The usual age of onset of enthesitis-related arthritis is 10-12 years.[14]
Prognosis
Advances in treatment over the last 20 years—especially the introduction of early use of intra-articular steroids, methotrexate, and biologic medications—have dramatically improved the prognosis for children with arthritis. Almost all children with JIA lead productive lives. However, many patients, particularly those with polyarticular disease, may have problems with active disease throughout adulthood, with sustained remission attained in a minority of patients.
Early hip or wrist involvement, symmetrical disease, the presence of RF, and prolonged active systemic disease have been associated with poor long-term outcomes. Compared with adults with RF-positive rheumatoid arthritis, however, children are at less risk for rheumatoid lung involvement and vasculitis. The anti – cyclic citrullinated peptide antibodies (CCP) antibodies test may be more specific than the RF test, but it is not as well studied in children.
Children with systemic-onset disease tend to either respond completely to medical therapy or develop a severe polyarticular course that tends to be refractory to medical treatment, with disease persisting into adulthood.
Most children with oligoarticular disease demonstrate eventual permanent remission, although a small number progress to persisting polyarticular disease.
Concern has been raised that the use of biologics may increase cancer risk among patients with JIA; however, lack of data on the baseline risk of cancer in this population has made it difficult to determine whether the concern is justified. A review of a large cohort of patients from the Swedish registry found an increased risk of cancer in patients who had not been on biologic therapies and had been diagnosed with JIA in the last 20 years. However, this risk was not found if the analysis was extended to patients diagnosed between 1969 and 1987.[16, 17]
The results of this study were not statistically significant. Nevertheless, they may have implications for interpretation of cancer signals in patients with JIA, particularly those who are on ongoing therapy with biologic agents, such as TNF-alpha inhibitors.
Patient Education
Educating the patient, family, and school personnel (eg, classroom teachers, physical education teachers, nurses) about JIA and its presentation, treatment, and potential effects is continually necessary. Members of the pediatric rheumatology team in pediatric rheumatology clinics are the best educators about JIA. Another important source of information is the American Juvenile Arthritis Organization, a council of the Arthritis Foundation.

For patient education information, see the Arthritis Center, as well as Juvenile Rheumatoid Arthritis and Juvenile Rheumatoid Arthritis Treatment.
Note :
………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………….