percussion auscultation - semmelweis.husemmelweis.hu/...en_iii_percussionauscultation... ·...
TRANSCRIPT
PERCUSSION
AUSCULTATION
Emese Mihaly MD, PhD Semmelweis University
2nd Department of Internal Medicine
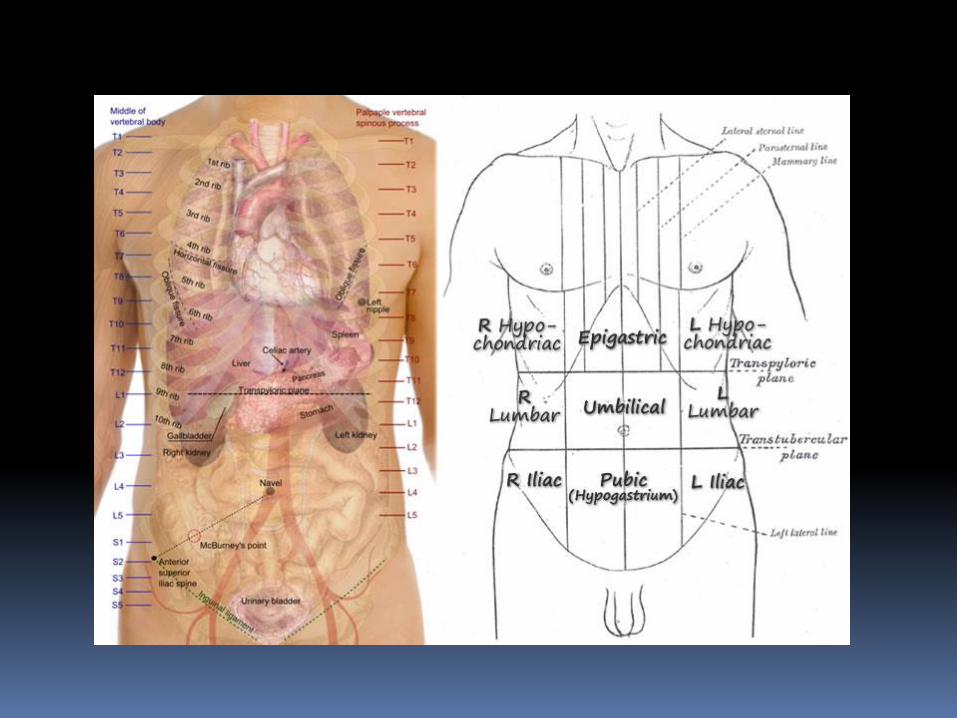
Palpation
Tenderness
Mass or swelling
Position of the trachea
Tactile fremitus
Chest expansion
Tenderness
Inflamed pleura
Injury of the chest
Intercostal muscular pain
Herpes Zoster
Rib fracture
Pleurosy

Mass/swelling
Tumor
Rubor
Calor
Functio laesa
Site/surface /consistency/size/mobility
Trachea position
Normally: on midline, may slightly deviate to
the right
Abnormal:
Deviation to the same side: lung collapse or
fibrosis
Diveation to the opposite side: PTX, pleural
effusion
No tracheal deviaton in lung consolidation
Tactile (Pectoral) Fremitus
Palpable vibrations transmitted
through the broncho-pulmonary tree
from the larynx to the chest wall
Ask the patient to say: 99/HUN33
Palpate and compare symmetrical
areas
For presence or absence of simmetry
of TF
Tactile (Pectoral) Fremitus
TF Increased: lung consolidation
lung fibrosis
TF Decreased or missing:
Hydrothorax
Pleural thickening
PTX
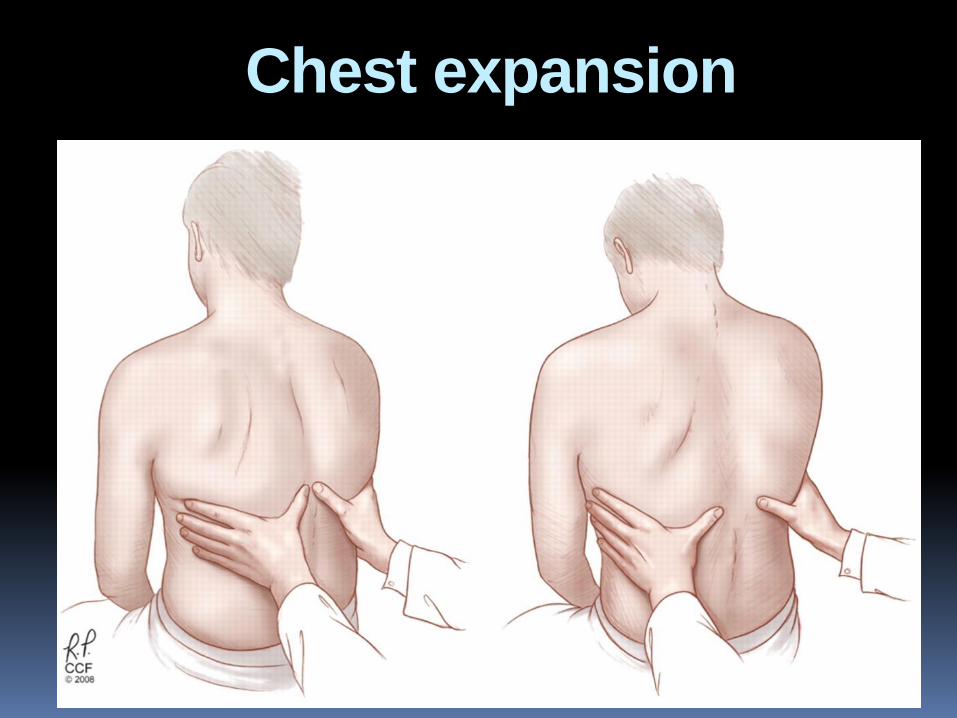
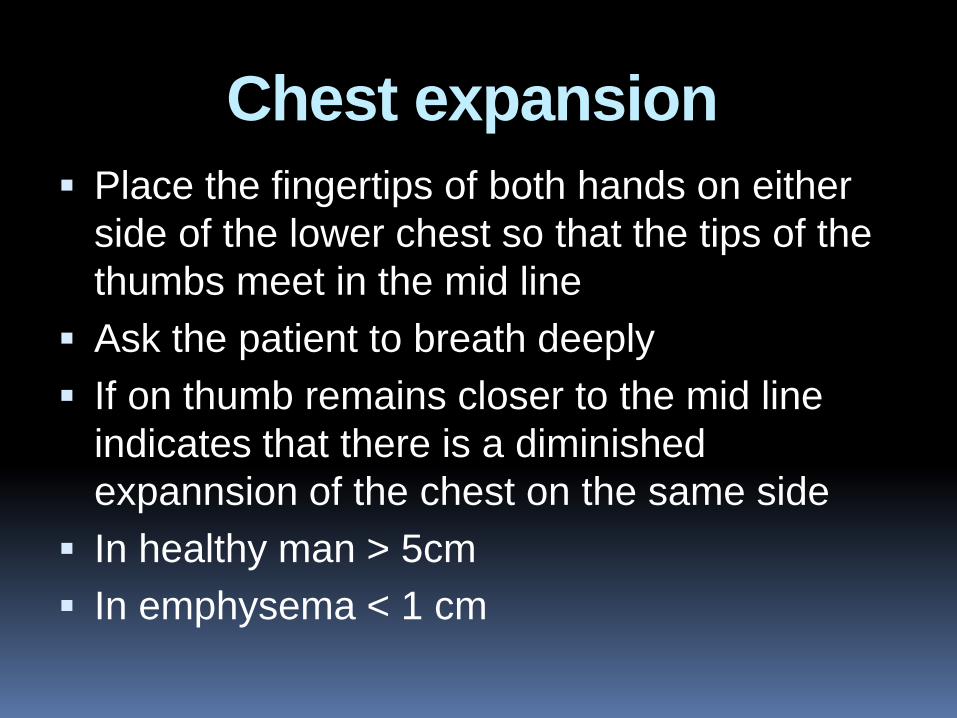
Chest expansion
Chest expansion
Place the fingertips of both hands on either
side of the lower chest so that the tips of the
thumbs meet in the mid line
Ask the patient to breath deeply
If on thumb remains closer to the mid line
indicates that there is a diminished
expannsion of the chest on the same side
In healthy man > 5cm
In emphysema < 1 cm
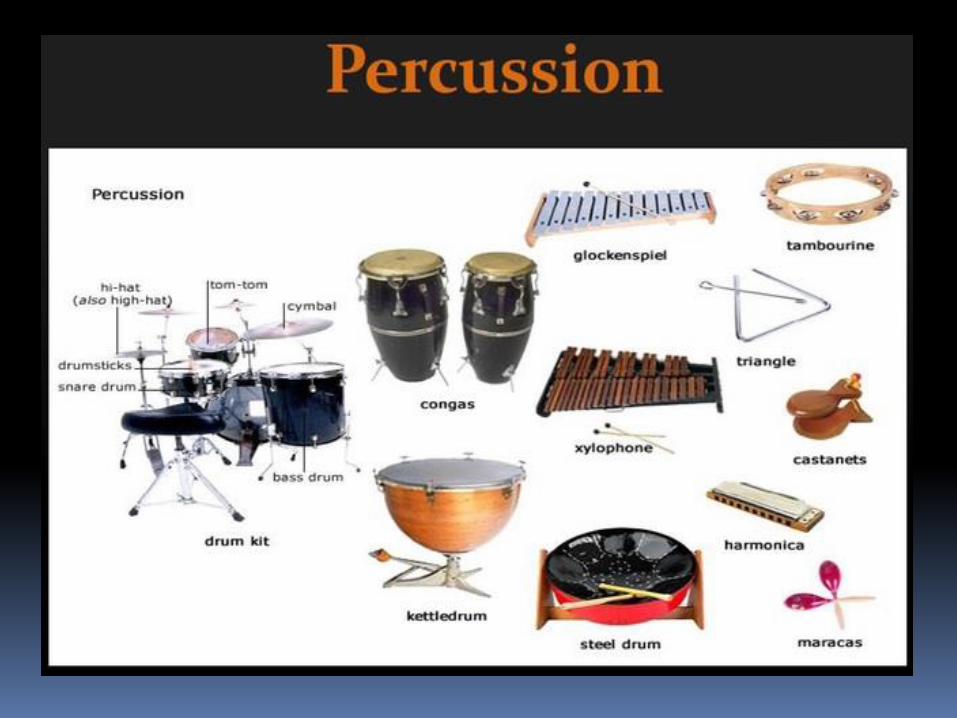
Percussion
First used by Avicenna, Ibn Sina,
(980-1030)
One of the greatest intellects of
Islam’s Golden Age
Best known for his contributions to
medicine
His works, after being translated
into Latin became deeply influential
in Medieval and renaissance
Europe.
Percussion Direct percussion:
to perform direct percussion, tap directly on
the patient's skin
tapping movement should originate from your
wrist, not your elbow
best for percussing the paranasal sinuses.
Indirect percussion
Two fingers: pleximeter and striking finger
Used for most parts on the body
Percussion
Method of tapping on a surface to determine
the underlying structure
To assess the condition of the thorax or
abdomen
Hyperextend the middle finger of one hand
and place firmly against the patient’s chest
(nonstriking finger, pleximeter)
With the tip of the opposite middle finger use
a quick flick of the wrist to strike the first
finger
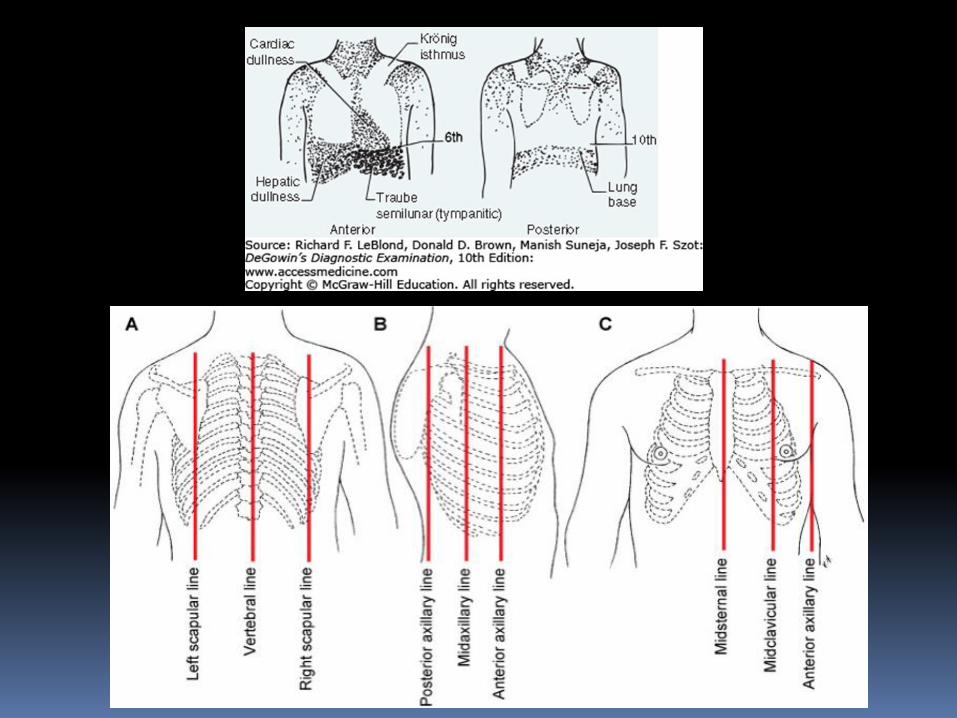
Percussion
Percussion
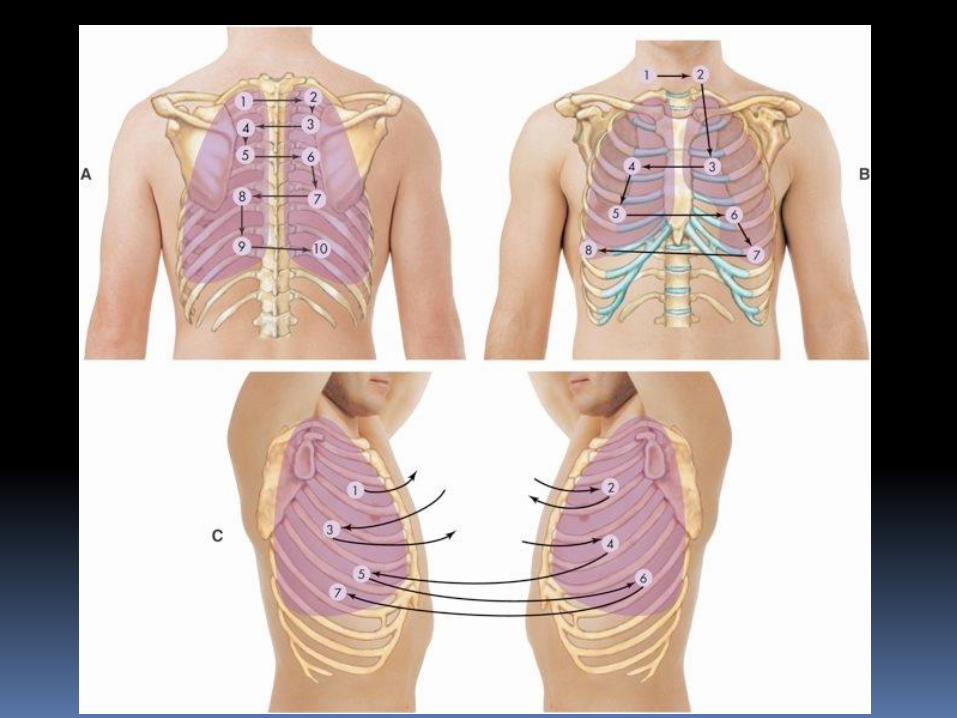
Percuss simmetrical areas of both sides
From upper to lower part
From left to the right
And from right to the left
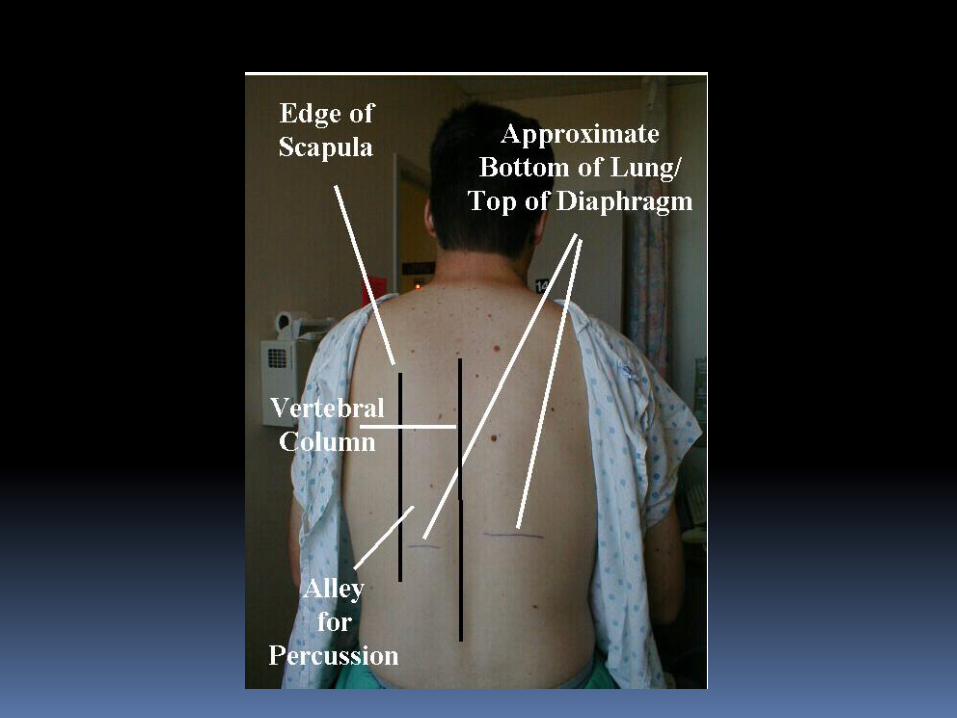
Find the level of diaphragmatic dullness on both sides
Percussion
There are four types of percussion sounds:
resonant, hyper-resonant, stony dull or dull.
Dull sound indicates the presence of a solid
mass under the surface, pleural effusion.
Resonant sound indicates hollow, air-
containing structures.
Hyper-resonant sound: emphysema
Tympanic sound if there is a pneumothorax
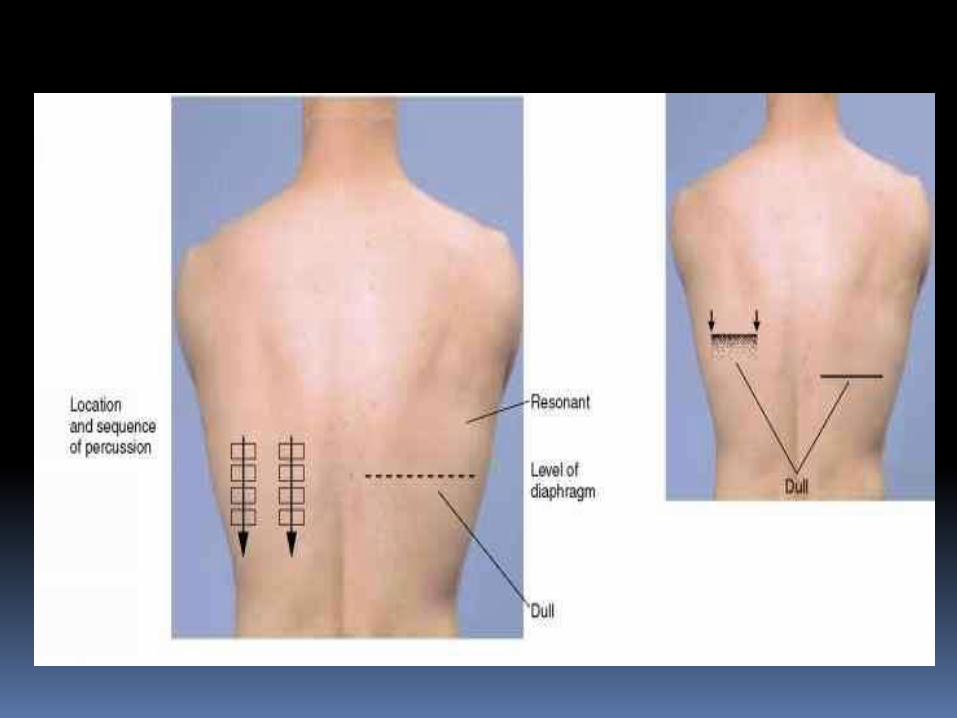
Diaphragmatic excursion
Percuss along the scapular line until the level of the diaphragmatic dullness
Ask the patient to inspire deeply and hold his breath
Proceed to percuss down from the marked point to determine the diaphragmatic excursion in deep inspiration
Repeat on the opposite side
Measure the distance between the upper-lower points on each side
Normally is 3-5 cm bilaterally (symmetrically)
Auscultation
Breath sounds
Added-adventitious- sound
Vocal resonance
Auscultation Normal breathing sound:
Over the lung tissue: vesicular-soft and low
pitched
Over the trachea: tracheal-loud, high pitched
Over the manubrium: bronchial- loud, high
pithced
Between the scapulae, and 1st-2nd interspace:
bronchovesicular-inter mediate intensity and
pitch
Air entry-Intensity
Normal
Decreased / absent:
Pleural effusion, PTX
Increased: Consolidation
Vocal resonance
Bronchophony: Ask patient to say 99 while auscultating the
chest wall
Normally the sound is muffled and indistinct
In pneumonia: normal speech is heard clearly
Vocal resonance
Egophony:
Ask the patient to say „ee” continuously
Ausculatate symmetrical areas
Mulffled EE sound should be head
If „ee” is heard as „ay” , change „E-A”
refers to consolidation
Vocal resonance
Whispered Pectoriloquy: Ask patient to whisper 99
Auscultate symmetrical areas
Whispered sound is normally heard faintly or
indistinctly
When louder and clearer whispered sound
are heard: whispreded pectoriloquy-refers to
consolidation
Added-adventitious sounds
Crackles/rales
Wheezes/ronchi
Pleural friction rub
Stridor
Added sounds Atypical-added, adventitious-sounds
Superimposed on breath sounds
Are not alterations in breath sounds
Patient should clear his or her secretion
Crepitation: short, discrete, interrupted crackling
sound at the end of inspiration
Fine crackles: soft, high pitched, brief 5-10
msec/fibrosing alveolitis, congestive heart failure
Course crackles: louder, lower in pitch, 20-30
msec-bronchiectasis
Added sounds Ronchi
Continuous sounds produced by the movements of air in the
presence of free fluid in the airway lumen
Wheezes
Often audible at the mouth as well at the chest wall
More prominent during expiration than inspiration
Oscillation of airway walls that occurs when there is airflow
limitation
Stridor: Interily or predominantly inspiratory
Louder in the neck
Due to larynx or trachea obstruction, demands immediate
attention (foreign body, epiglottitis, external obstruction)
Pleural friction rub
Creaking noise like to that emitted by
compression of new leather
Indicates inflammed pleural surfaces rubbing
against each other
Heard in both respiratory cicles (insp and exp)
Pleurisy from adjacent pneumonia, pulmonary
infaction or tbc
Confined to relatively small area of the chest
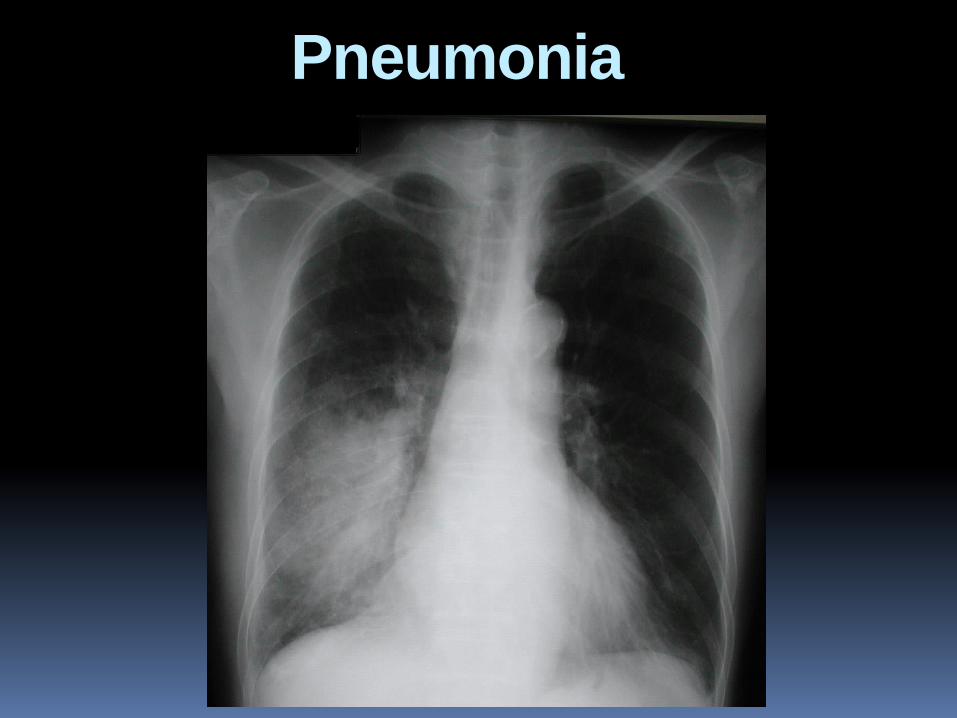
Pneumonia
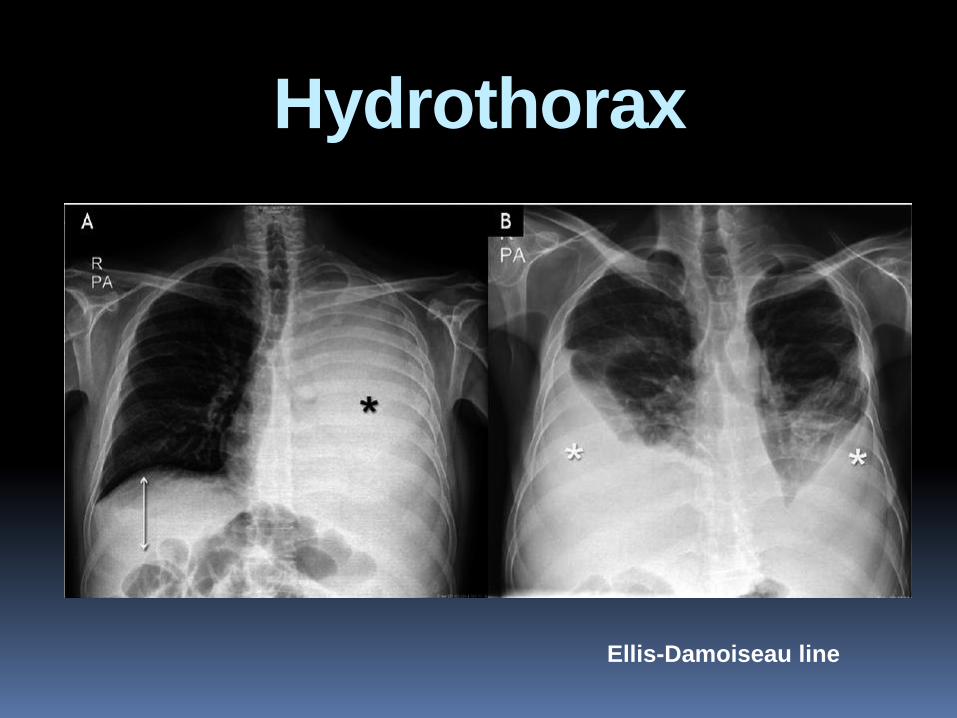
Hydrothorax
Ellis-Damoiseau line
Inspection
Careful inspection of the anterior chest may reveal the location of the apical impulse
Systolic retraction at the site of apical impulse indicates pericardial accretio (a form of adhesive pericarditis in which adhesions extend from the pericardium to the chest wall)
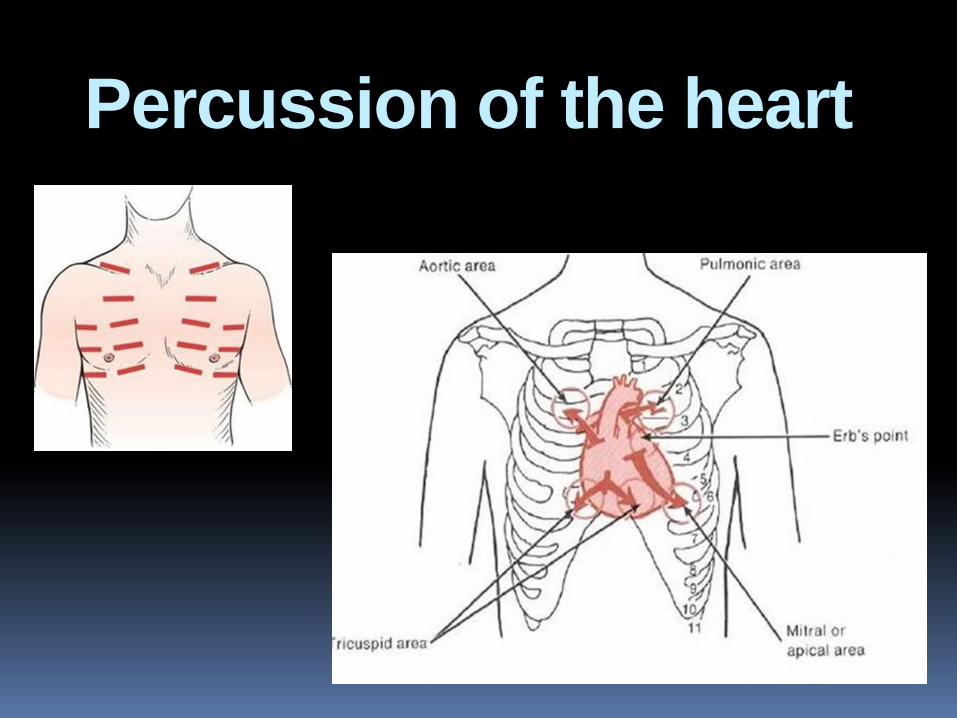
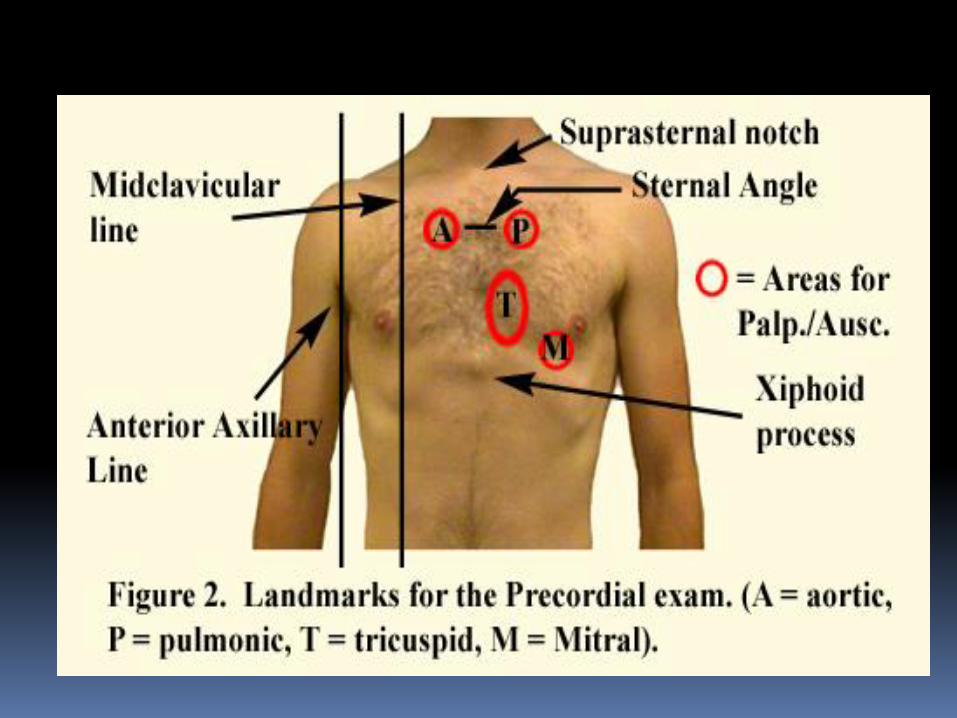
Percussion of the heart
Heart borders
1. Lower border: percussion the position of the diaphragma on the right side. 5-6th interspace in the midclavicular line.
2. Right border: does not exceed the right border of the sternum.
3. Upper border: 3d interspace parasternally on the left side
4. Left border: 7-9 cm from the midline
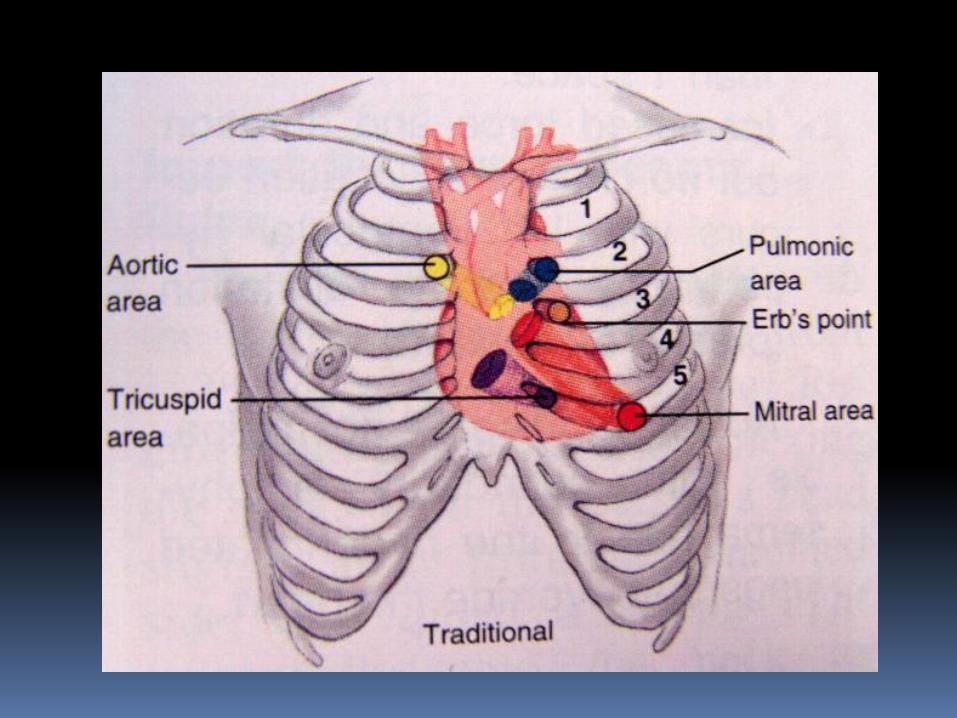
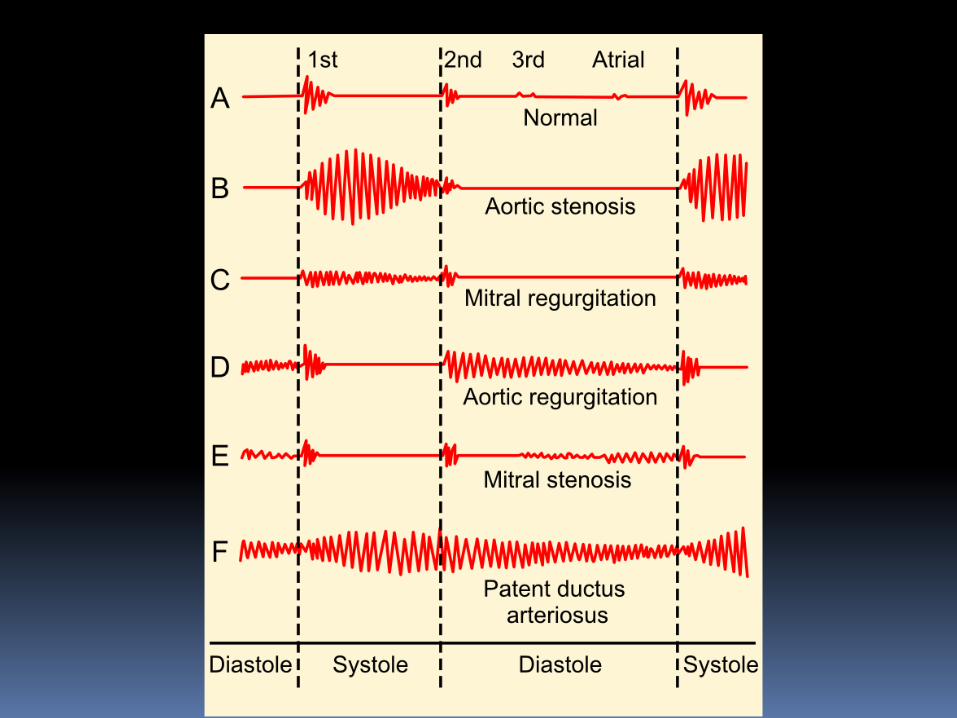
Heart sounds
Closure of the mitral and tricuspid valve
produces the first heart sound (S1).
Aortic and pulmonary valve closure
produces the second heart sound (S2).
Normally, the mitral valve closes just prior
to the tricuspid valve. Thus, M1 is audible
before T1 (a difference that is often not
detectable). If this difference is more
prominent=Split S1.

Thank You!