perinatal mental health provision in the south east · page 4 introduction and background perinatal...
TRANSCRIPT

Authors: Dr Agnieszka Klimowicz and Beverley Lignum Email: [email protected]
Web: www.secscn.nhs.uk Date: 31st August 2016
Perinatal Mental Health Provision in the South East
Scoping Paper and Recommendations
Page 2
Table of Contents
INTRODUCTION AND BACKGROUND 4
PURPOSE 5
NATIONAL CONTEXT 6
NATIONAL PREVALENCE RATES 7
WHAT DOES ‘GOOD’ LOOK LIKE? 8
SPECIALIST COMMUNITY PERINATAL MENTAL HEALTH TEAMS (ENGLAND) 12
KENT, SURREY AND SUSSEX PREVALENCE 13
KENT AND MEDWAY PREVALENCE 13
SURREY PREVALENCE 13
SUSSEX PREVALENCE 14
KENT, SURREY AND SUSSEX BASELINE SERVICE PROVISION 15
SPECIALIST COMMUNITY PERINATAL MENTAL HEALTH TEAMS – KENT AND MEDWAY 15
SPECIALIST COMMUNITY PERINATAL MENTAL HEALTH TEAMS – SURREY 21
SPECIALIST COMMUNITY PERINATAL MENTAL HEALTH TEAMS – SUSSEX 26
MOTHER AND BABY UNITS 33
KEY ISSUES AND BARRIERS 35
OUTCOMES OF SCOPING WORK 35
PRIORITIES FOR CHANGE 36
SUMMARY AND RECOMMENDATIONS 37
SUMMARY 37
RECOMMENDATIONS 37
APPENDICES 39
APPENDIX 1 : RESOURCES FOR STANDARDS AND GUIDANCE 39
APPENDIX 2: ANTENATAL AND POSTNATAL MENTAL HEALTH NICE QUALITY STANDARD [QS115] FEBRUARY 2016: 40
APPENDIX 3: GLOSSARY OF PERINATAL MENTAL HEALTH CONDITIONS 41
REFERENCES 43

Page 3
Acknowledgements The authors would like to thank all the people – both providers and commissioners - in Kent, Surrey and Sussex who contributed information for the report and gave their valuable time to make comments and amendments. A special thank you to the women and their families, who shared their experiences of perinatal mental health problems and their experiences of care. We would also like to acknowledge the contribution of Laura Ansboro, Clinical Network Quality Improvement Lead, and Charlotte Clow, Clinical Network Manager. Beverley Lignum, South East Clinical Network Perinatal Mental Health Programme Lead Dr Agnieszka Klimowicz, South East Clinical Network Perinatal Mental Health Clinical Lead

Page 4
Introduction and Background
Perinatal mental health services are concerned with the Prevention, Detection and Management of mental
health problems that can occur during pregnancy and the post-partum year (RCPsych, 2015).
During the perinatal period all involved in the woman’s care should be aware of the following:
New onset of mental health problems,
Recurrence of mental health problems in women who have been well,
Women with existing mental health problems who want to become or become pregnant.
For several years there has been evidence and guidance from various sources stating the need for robust
services to support women and their families around perinatal mental health. The impacts on the mother,
child and family plus the economic cost from a lack of good quality care and specialist services are well
documented (NMHDU 2011, NSPCC, 2012, LSE and Centre for Mental Health, 2014, MBRRACE - UK,
2015, NHS IQ, 2015 ).
A number of national documents which include commissioning guidance, standards and recommendations
have been produced to support service improvement of perinatal mental health care from universal
services through to specialist perinatal mental health services. (Appendix 1)
The Five Year Forward View (NHS E, 2014) sets out a clear vision for bringing about change and service
improvement through innovation and integration. The report makes it clear that variations in care which
can be detrimental and devastating to individuals are unacceptable and that short term fixes are not the
answer. There needs to be sustainable strategies and plans that address the three fundamental gaps that
will influence equity across the system:-
The health and wellbeing gap
The care and quality gap
The funding and efficiency gap
The National Maternity Review (NHS E, 2016) and the Mental Health Taskforce Report (MHT, 2016) are a
result of the ambitions set out in the Five Year Forward View (2014). Both reports support the need for
improvement in perinatal mental health services through: addressing historical underfunding, developing
NICE concordant care and a drive towards an equality of response to mental and physical health.
On the 2nd July 2015 the Rt Hon Alistair Burt (Minister for Social and Community Care) (MMHA, 2015)
announced a contribution of £75m over 5 years to be allocated to perinatal mental health so that women
experiencing mental ill health during pregnancy and the first year after birth will have:
Better access to care.
Support and care from specialist community perinatal mental health teams.
Rapid access to mother and baby units close to home for those mothers who are seriously ill.
In response to the £15m per year allocation, NHS England commissioned the National Collaborating
Centre for Mental Health to support the programme and to establish a perinatal mental health expert group.
The aim of the group is to:
Advise on the use of the additional £75m investment.

Page 5
Produce model pathways to implement NICE concordant care and commissioning guidance to
support implementation of these.
Advise on the potential to introduce access and waiting times standards in part of the pathway. This includes work to understand the capacity and capability of current services to see how far need is met
and ensure that resources are targeted accordingly.
On the 11th January 2016, the Prime Minister as part of the Life Chances Strategy pledged a £290 million
investment by 2020/21, so that at least 30,000 more women each year will have access to evidence-based,
specialist mental health care during or after pregnancy (DoH, 2016). This builds on the initial investment
making a total investment from 2015/16 to 2020/21 of £365m.
Purpose
The South East Clinical Network provides support and advice in areas of healthcare challenge to improve
the quality and outcomes of patient care. We have been tasked with supporting commissioners and
providers in Kent, Surrey and Sussex to improve perinatal mental health services through whole system
integration and collaboration.
The aim of this document is to provide an overview of current national policy and guidance and the current
provision of perinatal mental health services in the South East.
This desktop exercise is the first step in bringing together the vast amounts of scoping work already carried
out nationally and across Kent, Surrey and Sussex which include:
A stock-take of perinatal mental health provision in England. Mother and baby units’ patient
mapping, NHS Benchmarking Network, September 2015.
Perinatal and infant mental health national seminar held by the Mental Health Foundation and
National Children’s Bureau, July 2015.
Feasibility study for the funding of a specialist perinatal mental health midwife. East Kent University
Hospital Trust, July 2015.
Perinatal mental health services survey – Clinical Commissioning Groups and Hospital Trusts
across Kent Surrey and Sussex, November 2015.
Perinatal mental health - gap analysis, Western Sussex University Hospital NHS Trust.
Service mapping and improvement event – Summary of outcomes – Kent and Medway Perinatal
Mental Health Clinical Network, November 2015.
Perinatal mental health services scoping paper - Crawley, Horsham and Mid Sussex Clinical
Commissioning Groups, August 2015.
Perinatal mental health needs assessment for Kent 2016 – Kent Public Health Observatory
Public Health and Maternity Services Review 2014.
Surrey and North East Hampshire perinatal mental health draft integrated pathway, April 2016.
The recommendations presented in this paper are a reflection of the needs analysis within the scoping
exercises, children and young people’s mental health local transformation plans, operating plans and also
take into account national guidance and standards.

Page 6
National Context
Guidance on implementing the five year forward view for mental health (NHSE, 2016) specifies that, by
2020/21, there will be increased access to specialist perinatal mental health support in all areas, in the
community or in-patient mother and baby units, allowing at least an additional 30,000 women each year to
receive evidence-based treatment, closer to home, when they need it. Total additional funding to support
delivery of this objective is £365 million over the period.
Plans are in place to develop metrics for 2016-17. Meanwhile, across the South East, all localities have
included perinatal mental health within their Local Transformation Plans for Children and Young People’s
Mental Health, against which delivery is being monitored.
Mild to moderate depressive illness/anxiety are common during pregnancy and the post-partum year and
women can deteriorate rapidly from these early after delivery. Childbirth is associated with psychiatric
morbidity and is known to increase the risk to a woman's mental health and to developing or exacerbating a
serious mental illness (MBRRACE – UK, 2015).
Studies found that the prevalence of antenatal depression ranged from 7.4% in the first trimester, 11.4% to
12.8% in the second trimester and 13.1% to 14.8% in the third. The prevalence of postnatal depression
varied from 7.4% to 11.0% in the first 3 months after childbirth, 7.8% to 12.8% in the 3rd to 6th months and
8.5% to 12.0% in the 6th to 9th months and approximately half of the affected individuals experience major
depression (LSE and Centre for Mental Health, 2014).
Despite it being well known that up to 20% of women will develop some mental health issue during the
perinatal period, services across the UK, England and the South East are disparate, poor and in some
cases non-existent (NMHDU, 2011, NSPCC, 2012).
Between 2011-2013 (UK), almost a quarter of maternal deaths between 6 weeks and one year after
pregnancy were related to mental health problems. It is stated that whilst deaths from direct causes are
decreasing, deaths from indirect causes, which include mental health problems are on the increase (LSE
and Centre for Mental Health, 2014).
The evidence suggests that in England:
Nearly half of perinatal depression and anxiety goes undetected.
There is failure to provide evidence based treatment for many of those identified with perinatal
anxiety and depression.
There is a lack of specialist perinatal mental health services for women with complex or severe
conditions.
There are a range of problems and severity of disorders associated with perinatal mental health. Table 1 (p
6) illustrates the national prevalence rates (JCPMH, 2012) and the estimated number of women affected by
perinatal mental illness each year. Understanding local prevalence rates is key to understanding future
service requirements but it should also be considered within the wider health and social care determinants.
Page 7
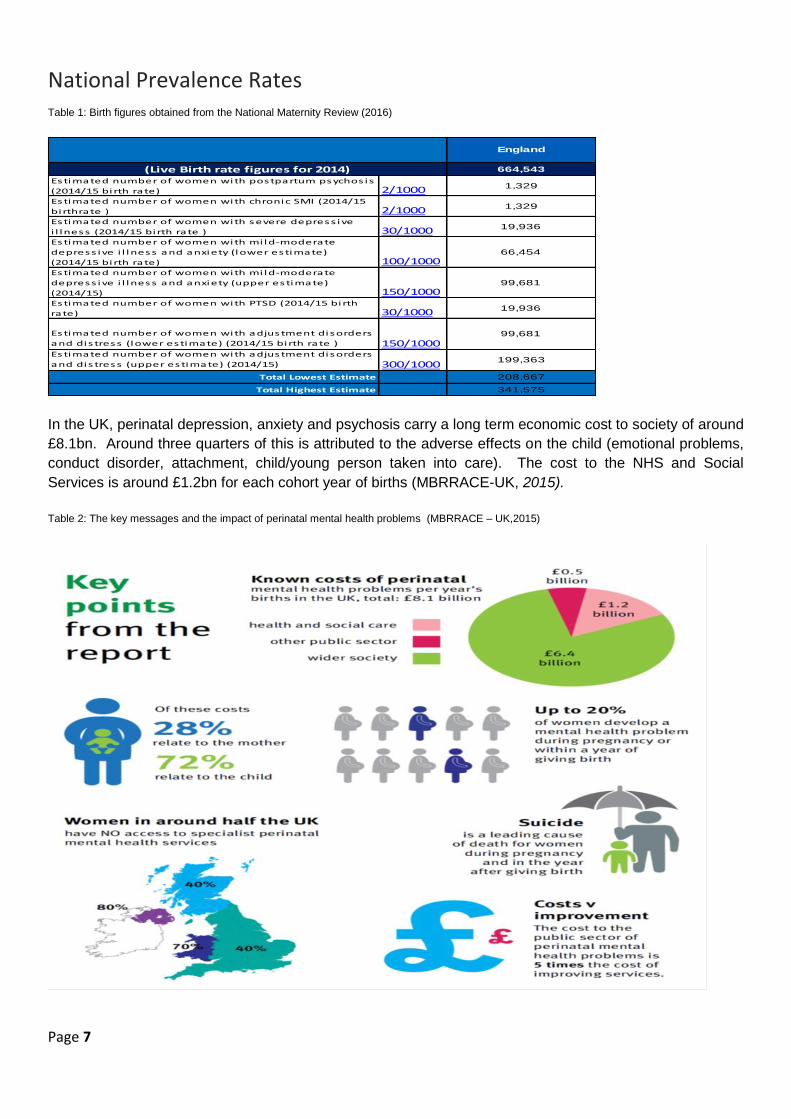
National Prevalence Rates Table 1: Birth figures obtained from the National Maternity Review (2016)
In the UK, perinatal depression, anxiety and psychosis carry a long term economic cost to society of around
£8.1bn. Around three quarters of this is attributed to the adverse effects on the child (emotional problems,
conduct disorder, attachment, child/young person taken into care). The cost to the NHS and Social
Services is around £1.2bn for each cohort year of births (MBRRACE-UK, 2015).
Table 2: The key messages and the impact of perinatal mental health problems (MBRRACE – UK,2015)
664,543
Estimated number of women with postpartum psychos is
(2014/15 birth rate) 2/1000 1,329
Estimated number of women with chronic SMI (2014/15
birthrate ) 2/1000 1,329
Estimated number of women with severe depress ive
i l lness (2014/15 birth rate ) 30/1000 19,936
Estimated number of women with mi ld-moderate
depress ive i l lness and anxiety (lower estimate)
(2014/15 birth rate) 100/100066,454
Estimated number of women with mi ld-moderate
depress ive i l lness and anxiety (upper estimate)
(2014/15) 150/100099,681
Estimated number of women with PTSD (2014/15 birth
rate) 30/1000 19,936
Estimated number of women with adjustment disorders
and dis tress (lower estimate) (2014/15 birth rate ) 150/100099,681
Estimated number of women with adjustment disorders
and dis tress (upper estimate) (2014/15) 300/1000199,363
Total Lowest Estimate 208,667
Total Highest Estimate 341,575
(Live Birth rate figures for 2014)
England

Page 8
What does ‘good’ look like? Understanding the need and demand for services across the spectrum of perinatal mental health
problems along with robust care pathways, education and training are essential to ensure that women
receive the right care, at the right time by the right person.
It is crucial that services are made accessible and there is a whole system approach to caring for women
and their families with mental health problems. There needs to be learning for the future: through service
improvement and making maternity services safer; by using the findings and evidence of maternal deaths
to ensure that every woman receives coordinated care throughout her pregnancy and the post-partum year,
from all services that she may access.
Women and their families experiencing perinatal mental health problems can have their care managed in a
range of settings. These include:
Mother and baby units
Specialist community mental health teams
Adult mental health teams
Alcohol and drug misuse services
Intellectual disability services
CAMHS
Parent and infant mental health services
Maternity services
Clinical psychology
Social care
Children’s centres
GP’s, HV’s, extended primary care
Voluntary sectors
Delivering the vision of sustainable perinatal mental health services and a seamless integrated perinatal
mental health pathway needs to be designed through the principles of collaborative clinical leadership,
collaborative commissioning and service user expertise. New models of care, commissioning and
contracting need to reflect and be tailored to local population needs (RCP, 2015).
The funding that has been pledged to improve access to perinatal mental health care focuses on the
specialist end of service provision for women with more serious perinatal mental health problems. But it is
equally important to be improving the detection of women with mild to moderate mental health
problems and access to appropriate services to support their care.
Early support and intervention is critical in building the foundations of a baby’s emotional wellbeing,
bonding and attachment (1001 critical days, 2014). Working in partnership with universal services and
early years’ services are key to improving health and social care outcomes for children in the future.
The diagram below is a visualisation of the number of universal contacts during the antenatal, postnatal
and up to the child being one year old. There are up to 19 windows of opportunity during this time for the
detection and prevention of perinatal mental health problems that affect the family as a whole.

Page 9
Table 3: Antenatal and postnatal universal contacts
KEY
Midwife
GP
Months 0-3 Months 4-6 Months 7-9 Birth - 12months
Health Visitor
All
Antenatal and Postnatal Universal Contacts
Preconception TRIMESTER 1 TRIMESTER 2 TRIMESTER 3 Birth & Postnatal
First Contact
GP/Midwide
Booking appointment
8 -12+6wks
Dating Scan
11-15wks16 -17wks 19-21wks
25 wks
P/gravida
28 wks
Joint
31 wks
P/gravida 34 wks 38 wks36 wks 2,5,10 days 10-14 days 6-8 weeks 9-12 mnth3-4 mnth
First contact - refer to GP/Midwife
40 wks
P/gravida
South East Clinical Network – Perinatal Mental Health
Page 10
According to NICE guidance, perinatal mental health clinical networks should be set up covering
populations of patient flow of approximately 4 to 5 million (delivered population 50,000). A coordinating
board of healthcare professionals, commissioners, managers, and service users and carers should manage
them. The networks will be responsible for the development of strategic plans, service and pathway
redesign and assist in workforce development (NICE, 2014).
Each managed perinatal mental health network should:
Provide a specialist multidisciplinary perinatal mental health service in each locality, which provides
direct services, consultation and advice to maternity services, other mental health services and
community services; in areas of high morbidity these services may be provided by separate specialist
perinatal teams.
Provide access to specialist expert advice on the risks and benefits of psychotropic medication during
pregnancy and breastfeeding.
Have clear referral and management protocols for services across all levels of the existing stepped-care
frameworks for mental health problems, to ensure effective transfer of information and continuity of care.
Have integrated pathways of care for service users, with defined roles and competencies for all
professional groups involved.
Have links to a designated specialist inpatient services.
Networks should always include specialist addictions services (MBRRACE-UK, 2015).
Specialist multidisciplinary perinatal community services and inpatient psychiatric mother and baby
units should be available to support women with a mental health problem in pregnancy or the postnatal
period (Antenatal and Postnatal Mental Health NICE Quality Standard). They should be a member of the
CCQI Quality Network for Perinatal Mental Health Services (RCPsych, 2015). 'For specialist perinatal
mental health teams to achieve accreditation, they should consist of doctors (and that might be a consultant
psychiatrist without a junior doctor providing there is an increased number of sessions available), and
nurses, ideally however they also should include professionals as detailed in table 4 (pg 10). If the service
covers large geographical area, the number of community psychiatric nurses should be increased to take
the travelling time for home visits into account'.
Between 3 and 5% of the delivered population will require the services of a specialist community mental
health teams. These teams can serve a delivered population of between 6000 and 10 000 births per year.
Services for seriously mentally ill women need to be organised differently from adult mental health services
and need to respond to the maternity context, the timeframes of pregnancy, the differing thresholds and
response times to presenting problems, including problems with parent infant relationships. Services need
to relate to different health professionals, particularly to maternity services and children’s social services.
South East Clinical Network – Perinatal Mental Health
Page 11
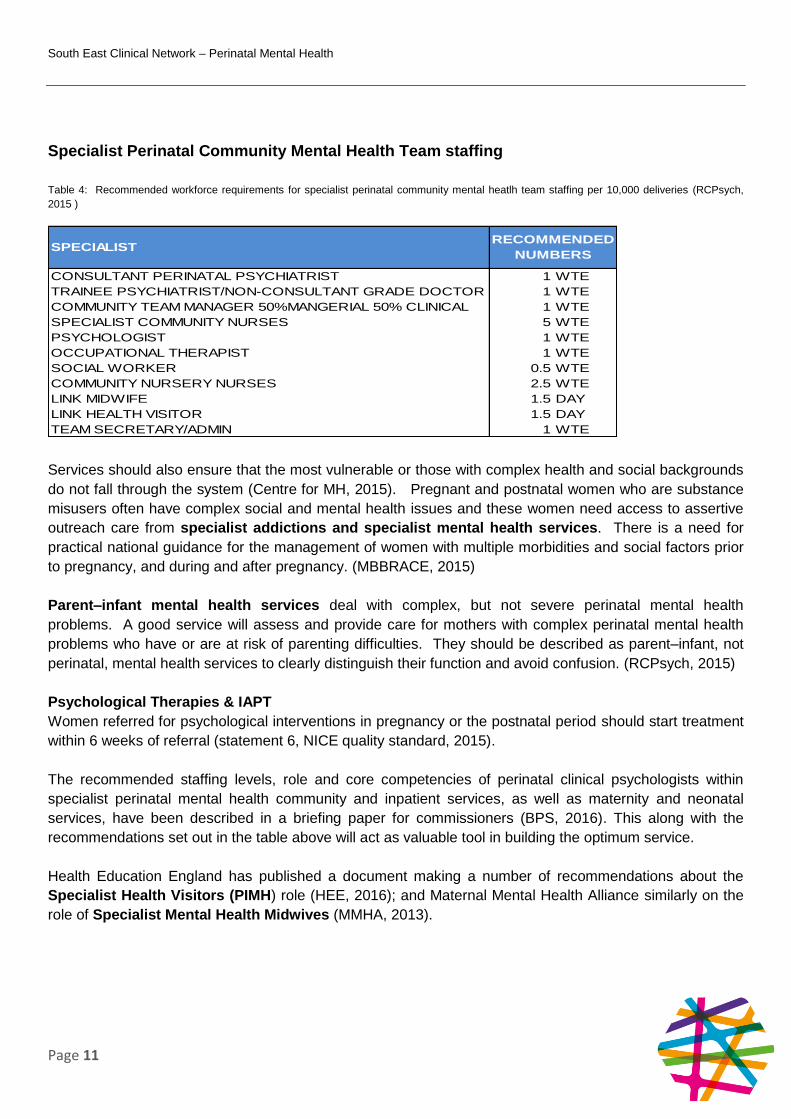
Specialist Perinatal Community Mental Health Team staffing
Table 4: Recommended workforce requirements for specialist perinatal community mental heatlh team staffing per 10,000 deliveries (RCPsych,
2015 )
Services should also ensure that the most vulnerable or those with complex health and social backgrounds
do not fall through the system (Centre for MH, 2015). Pregnant and postnatal women who are substance
misusers often have complex social and mental health issues and these women need access to assertive
outreach care from specialist addictions and specialist mental health services. There is a need for
practical national guidance for the management of women with multiple morbidities and social factors prior
to pregnancy, and during and after pregnancy. (MBBRACE, 2015)
Parent–infant mental health services deal with complex, but not severe perinatal mental health
problems. A good service will assess and provide care for mothers with complex perinatal mental health
problems who have or are at risk of parenting difficulties. They should be described as parent–infant, not
perinatal, mental health services to clearly distinguish their function and avoid confusion. (RCPsych, 2015)
Psychological Therapies & IAPT
Women referred for psychological interventions in pregnancy or the postnatal period should start treatment
within 6 weeks of referral (statement 6, NICE quality standard, 2015).
The recommended staffing levels, role and core competencies of perinatal clinical psychologists within
specialist perinatal mental health community and inpatient services, as well as maternity and neonatal
services, have been described in a briefing paper for commissioners (BPS, 2016). This along with the
recommendations set out in the table above will act as valuable tool in building the optimum service.
Health Education England has published a document making a number of recommendations about the
Specialist Health Visitors (PIMH) role (HEE, 2016); and Maternal Mental Health Alliance similarly on the
role of Specialist Mental Health Midwives (MMHA, 2013).
CONSULTANT PERINATAL PSYCHIATRIST 1 WTE
TRAINEE PSYCHIATRIST/NON-CONSULTANT GRADE DOCTOR 1 WTE
COMMUNITY TEAM MANAGER 50%MANGERIAL 50% CLINICAL 1 WTE
SPECIALIST COMMUNITY NURSES 5 WTE
PSYCHOLOGIST 1 WTE
OCCUPATIONAL THERAPIST 1 WTE
SOCIAL WORKER 0.5 WTE
COMMUNITY NURSERY NURSES 2.5 WTE
LINK MIDWIFE 1.5 DAY
LINK HEALTH VISITOR 1.5 DAY
TEAM SECRETARY/ADMIN 1 WTE
SPECIALISTRECOMMENDED
NUMBERS
South East Clinical Network – Perinatal Mental Health
Page 12
Specialist Community Perinatal Mental Health
Teams (England)
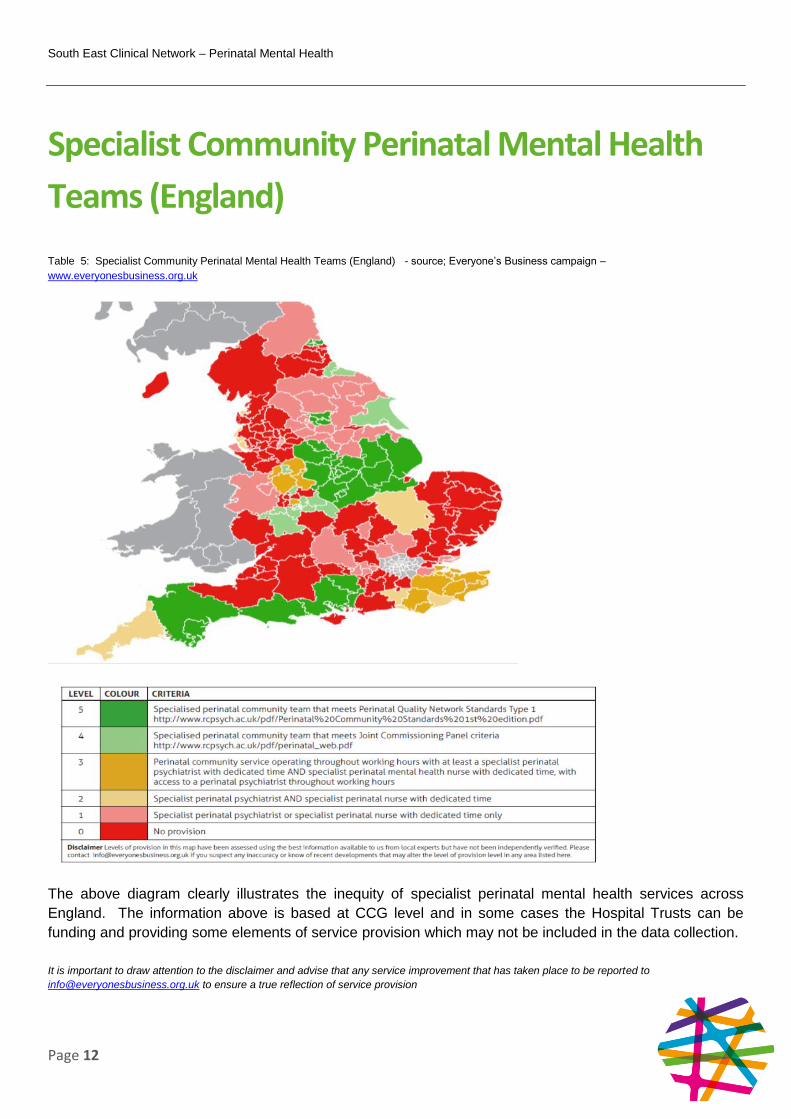
Table 5: Specialist Community Perinatal Mental Health Teams (England) - source; Everyone’s Business campaign –
www.everyonesbusiness.org.uk
The above diagram clearly illustrates the inequity of specialist perinatal mental health services across
England. The information above is based at CCG level and in some cases the Hospital Trusts can be
funding and providing some elements of service provision which may not be included in the data collection.
It is important to draw attention to the disclaimer and advise that any service improvement that has taken place to be reported to
[email protected] to ensure a true reflection of service provision

South East Clinical Network – Perinatal Mental Health
Page 13
Kent, Surrey and Sussex Prevalence This information below is based on the National Prevalence Rates. The National Child Health and
Maternity Network have published locality needs assessments on Perinatal Mental Health which can be
found using the following link: Mental health in pregnancy, the postnatal period and babies and toddlers:
needs assessment report. However the latest data available is 2013/14. In order to provide localities with
a more recent picture, the rates below are based on the CCG birth rate for 2014/15, (obtained from the
Quality Observatory – sourced from HES). At the time of writing this report we became aware of possible
discrepancies between CCG data and maternity data about the number of deliveries. It is anticipated that
Local Perinatal Mental Health Networks will consider those discrepancies.
Kent and Medway Prevalence Table 6: Kent and Medway prevalence based on birth rate figures for 2014/15
Surrey Prevalence Table 7: Surrey prevalence based on birth rate figures for 2014/15 (excludes North East Hampshire and Farnham)
1430 1730 1919 1532 5243 3192 1277 3606
Estimated number of women with postpartum
psychosis 2/10003 3 4 3 10 6 3 7
Estimated number of women with chronic SMI 2/1000
3 3 4 3 10 6 3 7
Estimated number of women with severe
depressive illness 30/100043 52 58 46 157 96 38 108
Estimated number of women with mild-moderate
depressive illness and anxiety (lower estimate) 100/1000143 173 192 153 524 319 128 361
Estimated number of women with mild-moderate
depressive illness and anxiety (upper estimate) 150/1000215 260 288 230 786 479 192 541
Estimated number of women with PTSD 30/1000
43 52 58 46 157 96 38 108
Estimated number of women with adjustment
disorders and distress (lower estimate) 150/1000215 260 288 230 786 479 192 541
Estimated number of women with adjustment
disorders and distress (upper estimate) 300/1000429 519 576 460 1573 958 383 1082
Total Lowest Estimate 449 543 603 481 1646 1002 401 1132
Total Highest Estimate 735 889 986 787 2695 1641 656 1853
Medway
(Birth rate figures for 2014/15)
Ashford Canterbury NHS South
Kent CoastThanet West Kent DGS Swale
2090 4312 2082 2892 923
Estimated number of women with postpartum
psychosis 2/10004 9 4 6 2
Estimated number of women with chronic SMI
2/10004 9 4 6 2
Estimated number of women with severe
depressive illness 30/100063 129 62 87 28
Estimated number of women with mild-moderate
depressive illness and anxiety (lower estimate) 100/1000209 431 208 289 92
Estimated number of women with mild-moderate
depressive illness and anxiety (upper estimate) 150/1000314 647 312 434 138
Estimated number of women with PTSD
30/100063 129 62 87 28
Estimated number of women with adjustment
disorders and distress (lower estimate) 150/1000314 647 312 434 138
Estimated number of women with adjustment
disorders and distress (upper estimate) 300/1000627 1294 625 868 277
Total Lowest Estimate 656 1354 654 908 290
Total Highest Estimate 1074 2216 1070 1486 474
Surrey
Heath
(Birth rate figures for 2014/15)
East Surrey North West
Surrey
Guildford
and
Waverley
Surrey
Downs

South East Clinical Network – Perinatal Mental Health
Page 14
Sussex Prevalence Table 8: Sussex prevalence based on birth rate figures for 2014/15
One of the current major barriers to understanding the number of women that have a perinatal mental
health problem and the severity of that problem is current data collection or the lack of it.
A midwife within East Kent University Hospital Foundation Trust completed a scoping project on perinatal
mental health in maternity and reported that it was difficult to compare the national prevalence rates due to
issues surrounding the recording, inputting and extrapolating information about a woman’s mental health
during the perinatal period. The categorisation output differs from the tables above making it difficult to
obtain a true reflection of the severity of a woman’s mental health during the perinatal period.
Further work should be carried out to establish if any other Trusts across the South East are experiencing
the same issues around data collection and whether figures are comparable with national rates.
The National Mental Health Network has developed a data collection catalogue to provide a list of
indicators and datasets pertinent to the scope of perinatal mental health intelligence. The purpose is to
ascertain the availability of all data available at a national scale and at sub-national geographies i.e. at
CCG, local authority, GP practice or provider level and to provide an indication of gaps within the available
data. The data catalogue has gone out for consultation and the outcomes are still awaited.
There is a varied commissioning and provider landscape for perinatal mental health services across the
South East. Clinical Commissioning Groups commission: primary care, maternity services and secondary
mental health services. Local authorities are responsible for: early years, health promotion and prevention
for the 0-5 years through the Healthy Child Programme, health visiting and the Family Nurse Partnership.
NHS England is responsible for the specialised commissioning of mother and baby units.
3094 4426 1730 2221 1699 1648 1424
Estimated number of women with postpartum
psychosis 2/10006 9 3 4 3 3 3
Estimated number of women with chronic SMI
2/10006 9 3 4 3 3 3
Estimated number of women with severe
depressive illness 30/100093 133 52 67 51 49 43
Estimated number of women with mild-moderate
depressive illness and anxiety (lower estimate) 100/1000309 443 173 222 170 165 142
Estimated number of women with mild-moderate
depressive illness and anxiety (upper estimate) 150/1000464 664 260 333 255 247 214
Estimated number of women with PTSD
30/100093 133 52 67 51 49 43
Estimated number of women with adjustment
disorders and distress (lower estimate) 150/1000464 664 260 333 255 247 214
Estimated number of women with adjustment
disorders and distress (upper estimate) 300/1000928 1328 519 666 510 494 427
Total Lowest Estimate 972 1390 543 697 533 517 447
Total Highest Estimate 1590 2275 889 1142 873 847 732
E'Bourne,
Hailsham
and
Seaford
Hastings
and Rother
High Weald,
Lewes and
Haven
Horsham
and Mid
Sussex
(Birth rate figures for 2014/15)
Brighton &
Hove
Coastal
WesternCrawley

South East Clinical Network – Perinatal Mental Health
Page 15
Kent, Surrey and Sussex Baseline Service
Provision
The National Perinatal Mental Health Programme is focused on achieving the provision of specialist
perinatal mental health teams which will be accredited members of the CCQI Quality Network for Perinatal
Mental Health Services (RCPsych, 2015). Therefore it is recommended that the chapter is read in
conjunction with the RCPsych Service Standards: Second Edition Perinatal Community Mental Health
Services (2014).
Specialist Community Perinatal Mental Health Teams – Kent and
Medway
The service provision in Kent and Medway falls into the ‘basic level’ of service provision and falls short of
national standards. Seven out of eight CCGs currently fall under level 3 and 1 CCG falls under level 1.
Table 9: Specialist community perinatal mental health teams provision in Kent and Medway according to www.everyonesbusiness.org.uk
Level Description Clinical Commissioning
Group
1 Specialist perinatal psychiatrist or specialist
perinatal nurse with dedicated time only
Dartford, Gravesham
and Swanley
3 Perinatal community service operating throughout working hours with at least a specialist perinatal psychiatrist with dedicated time and specialist perinatal mental health nurse with dedicated time, with access to a perinatal psychiatrist throughout working hours
Ashford, Canterbury
South Kent Coast
Thanet
West Kent
Swale
Medway
South East Clinical Network – Perinatal Mental Health
Page 16
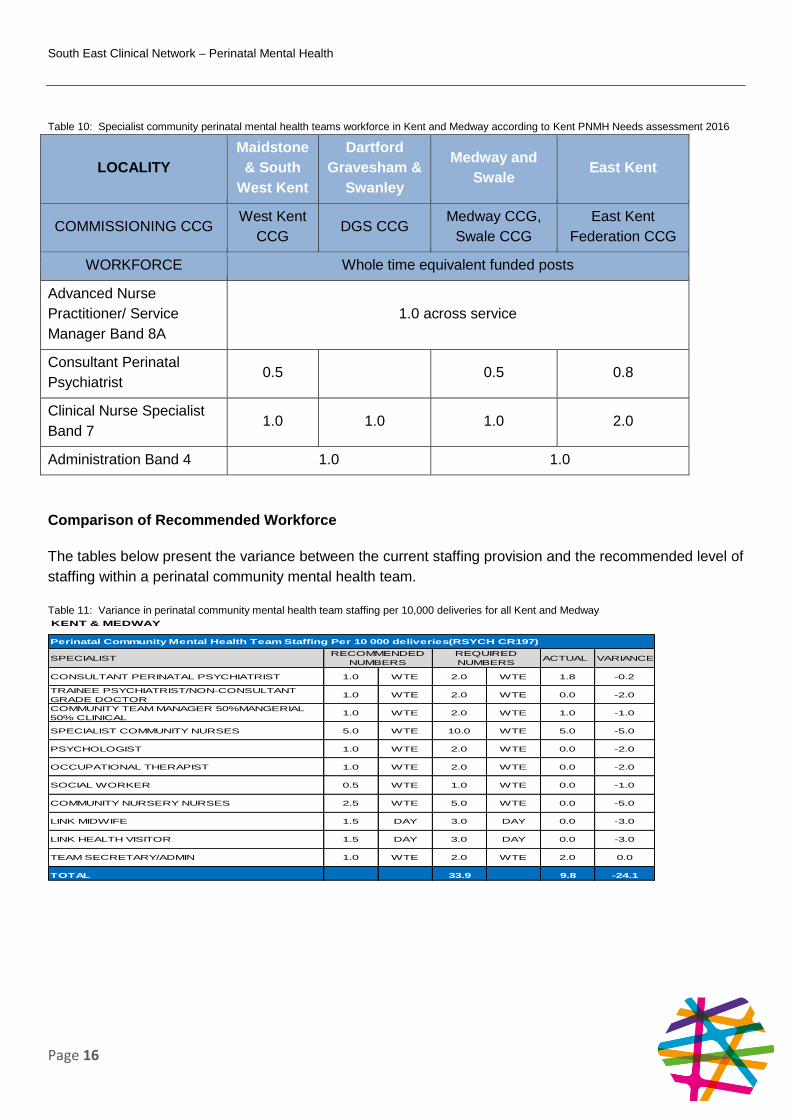
Table 10: Specialist community perinatal mental health teams workforce in Kent and Medway according to Kent PNMH Needs assessment 2016
LOCALITY
Maidstone
& South
West Kent
Dartford
Gravesham &
Swanley
Medway and
Swale East Kent
COMMISSIONING CCG West Kent
CCG DGS CCG
Medway CCG,
Swale CCG
East Kent
Federation CCG
WORKFORCE Whole time equivalent funded posts
Advanced Nurse
Practitioner/ Service
Manager Band 8A
1.0 across service
Consultant Perinatal
Psychiatrist 0.5 0.5 0.8
Clinical Nurse Specialist
Band 7 1.0 1.0 1.0 2.0
Administration Band 4 1.0 1.0
Comparison of Recommended Workforce
The tables below present the variance between the current staffing provision and the recommended level of
staffing within a perinatal community mental health team.
Table 11: Variance in perinatal community mental health team staffing per 10,000 deliveries for all Kent and Medway
KENT & MEDWAY
ACTUAL VARIANCE
1.0 WTE 2.0 WTE 1.8 -0.2
1.0 WTE 2.0 WTE 0.0 -2.0
1.0 WTE 2.0 WTE 1.0 -1.0
SPECIALIST COMMUNITY NURSES 5.0 WTE 10.0 WTE 5.0 -5.0
1.0 WTE 2.0 WTE 0.0 -2.0
1.0 WTE 2.0 WTE 0.0 -2.0
0.5 WTE 1.0 WTE 0.0 -1.0
2.5 WTE 5.0 WTE 0.0 -5.0
1.5 DAY 3.0 DAY 0.0 -3.0
1.5 DAY 3.0 DAY 0.0 -3.0
1.0 WTE 2.0 WTE 2.0 0.0
33.9 9.8 -24.1
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
SPECIALIST
CONSULTANT PERINATAL PSYCHIATRIST
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL
PSYCHOLOGIST
OCCUPATIONAL THERAPIST
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
TOTAL
SOCIAL WORKER
COMMUNITY NURSERY NURSES
LINK MIDWIFE
LINK HEALTH VISITOR
TEAM SECRETARY/ADMIN

South East Clinical Network – Perinatal Mental Health
Page 17
Table 12: Variance in perinatal community mental health team staffing per 10,000 deliveries in East Kent
Table 13: Variance in perinatal community mental health team staffing per 10,000 deliveries in West Kent
Table 14: Variance in perinatal community mental health team staffing per 10,000 deliveries in Dartford, Gravesham and Swanley
EAST KENT
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.7 WTE 0.8 0.1
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.7 WTE 0.0 -0.7
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.7 WTE 0.3 -0.4
SPECIALIST COMMUNITY NURSES 5.0 WTE 3.3 WTE 2.0 -1.3
PSYCHOLOGIST 1.0 WTE 0.7 WTE 0.0 -0.7
OCCUPATIONAL THERAPIST 1.0 WTE 0.7 WTE 0.0 -0.7
SOCIAL WORKER 0.5 WTE 0.3 WTE 0.0 -0.3
COMMUNITY NURSERY NURSES 2.5 WTE 1.7 WTE 0.0 -1.7
LINK MIDWIFE 1.5 DAY 1.0 DAY 0.0 -1.0
LINK HEALTH VISITOR 1.5 DAY 1.0 DAY 0.0 -1.0
TEAM SECRETARY/ADMIN 1.0 WTE 0.7 WTE 0.5 -0.2
TOTAL 11.2 3.6 -7.7
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
WEST KENT
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.5 WTE 0.5 0.0
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.5 WTE 0.0 -0.5
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.5 WTE 0.3 -0.3
SPECIALIST COMMUNITY NURSES 5.0 WTE 2.6 WTE 1.0 -1.6
PSYCHOLOGIST 1.0 WTE 0.5 WTE 0.0 -0.5
OCCUPATIONAL THERAPIST 1.0 WTE 0.5 WTE 0.0 -0.5
SOCIAL WORKER 0.5 WTE 0.3 WTE 0.0 -0.3
COMMUNITY NURSERY NURSES 2.5 WTE 1.3 WTE 0.0 -1.3
LINK MIDWIFE 1.5 DAY 0.8 DAY 0.0 -0.8
LINK HEALTH VISITOR 1.5 DAY 0.8 DAY 0.0 -0.8
TEAM SECRETARY/ADMIN 1.0 WTE 0.5 WTE 0.5 0.0
TOTAL 8.9 2.3 -6.7
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
DARTFORD, GRAVESHAM & SWANLEY
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.3 WTE 0.0 -0.3
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.3 WTE 0.0 -0.3
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.3 WTE 0.3 -0.1
SPECIALIST COMMUNITY NURSES 5.0 WTE 1.6 WTE 1.0 -0.6
PSYCHOLOGIST 1.0 WTE 0.3 WTE 0.0 -0.3
OCCUPATIONAL THERAPIST 1.0 WTE 0.3 WTE 0.0 -0.3
SOCIAL WORKER 0.5 WTE 0.2 WTE 0.0 -0.2
COMMUNITY NURSERY NURSES 2.5 WTE 0.8 WTE 0.0 -0.8
LINK MIDWIFE 1.5 DAY 0.5 DAY 0.0 -0.5
LINK HEALTH VISITOR 1.5 DAY 0.5 DAY 0.0 -0.5
TEAM SECRETARY/ADMIN 1.0 WTE 0.3 WTE 0.5 0.2
TOTAL 5.4 1.8 -3.7
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
South East Clinical Network – Perinatal Mental Health
Page 18
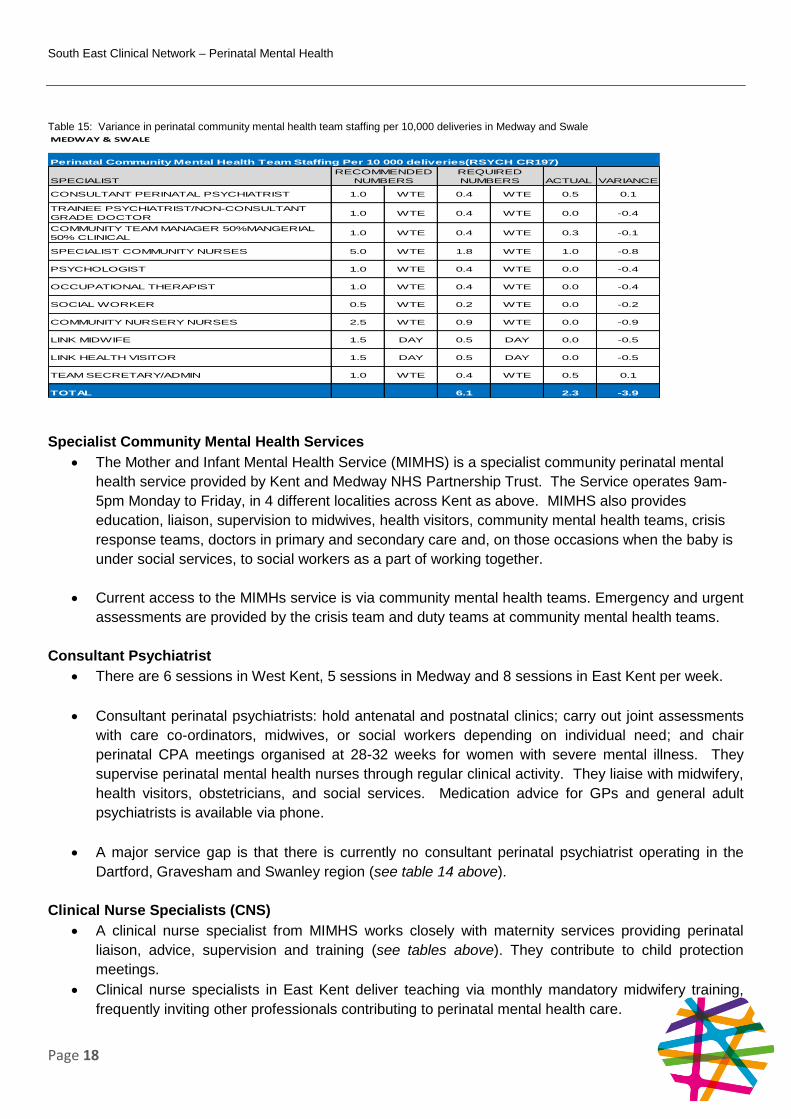
Table 15: Variance in perinatal community mental health team staffing per 10,000 deliveries in Medway and Swale
Specialist Community Mental Health Services
The Mother and Infant Mental Health Service (MIMHS) is a specialist community perinatal mental
health service provided by Kent and Medway NHS Partnership Trust. The Service operates 9am-
5pm Monday to Friday, in 4 different localities across Kent as above. MIMHS also provides
education, liaison, supervision to midwives, health visitors, community mental health teams, crisis
response teams, doctors in primary and secondary care and, on those occasions when the baby is
under social services, to social workers as a part of working together.
Current access to the MIMHs service is via community mental health teams. Emergency and urgent
assessments are provided by the crisis team and duty teams at community mental health teams.
Consultant Psychiatrist
There are 6 sessions in West Kent, 5 sessions in Medway and 8 sessions in East Kent per week.
Consultant perinatal psychiatrists: hold antenatal and postnatal clinics; carry out joint assessments
with care co-ordinators, midwives, or social workers depending on individual need; and chair
perinatal CPA meetings organised at 28-32 weeks for women with severe mental illness. They
supervise perinatal mental health nurses through regular clinical activity. They liaise with midwifery,
health visitors, obstetricians, and social services. Medication advice for GPs and general adult
psychiatrists is available via phone.
A major service gap is that there is currently no consultant perinatal psychiatrist operating in the
Dartford, Gravesham and Swanley region (see table 14 above).
Clinical Nurse Specialists (CNS)
A clinical nurse specialist from MIMHS works closely with maternity services providing perinatal
liaison, advice, supervision and training (see tables above). They contribute to child protection
meetings.
Clinical nurse specialists in East Kent deliver teaching via monthly mandatory midwifery training,
frequently inviting other professionals contributing to perinatal mental health care.
MEDWAY & SWALE
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.4 WTE 0.5 0.1
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.4 WTE 0.0 -0.4
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.4 WTE 0.3 -0.1
SPECIALIST COMMUNITY NURSES 5.0 WTE 1.8 WTE 1.0 -0.8
PSYCHOLOGIST 1.0 WTE 0.4 WTE 0.0 -0.4
OCCUPATIONAL THERAPIST 1.0 WTE 0.4 WTE 0.0 -0.4
SOCIAL WORKER 0.5 WTE 0.2 WTE 0.0 -0.2
COMMUNITY NURSERY NURSES 2.5 WTE 0.9 WTE 0.0 -0.9
LINK MIDWIFE 1.5 DAY 0.5 DAY 0.0 -0.5
LINK HEALTH VISITOR 1.5 DAY 0.5 DAY 0.0 -0.5
TEAM SECRETARY/ADMIN 1.0 WTE 0.4 WTE 0.5 0.1
TOTAL 6.1 2.3 -3.9
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS

South East Clinical Network – Perinatal Mental Health
Page 19
Junior Doctor
There are one to two sessions of a foundation trainee in West Kent, and periodically a higher
trainee session (special interest session) is available.
In Medway and East Kent there is no junior doctor.
Psychologist
There is no psychologist or parent and infant mental health service within Kent and Medway.
Link Midwife
There is a specialist mental health midwife at Darenth Valley Hospital – WTE not known at this
point.
There is a specialist perinatal mental health midwife at Medway Hospital.
A business case has been drafted to commission a specialist perinatal mental health midwife within
East Kent Hospitals University NHS Foundation Trust. The outcome of this is not known at this
point.
Link Health Visitors*
Perinatal mental health lead health visitors are now in all localities of Kent and Medway, employed
by Kent Community Hospital Trust, providing support and training as and when required. All health
visitors are trained in the early detection and intervention of perinatal mental health problems. This
is not a mental health dedicated workforce but perinatal mental health is an element of the role.
In Kent there is a developed pathway that links to key policy drivers: High Impact Area 2, Maternal
Mental Health - Healthy Child Programme - National HV Core Service Specification.
Medway Community Health Care Trust employs 1 WTE specialist health visitor for maternal and
infant mental health.
*Link midwife and Link Health visitors will not be included in the workforce table above until confirmed they will be a dedicated workforce.
Team Secretary Admin
There are 2 WTE secretaries working within the MIMHS service. (see tables above).
Service Lead
There is a managerial role which is full time (see tables above).
Other Services/Stakeholders
Maternal Bereavement Services
There is access to bereavement counselling within East Kent Hospitals University NHS Foundation
Trust. The workforce for this is not known at this point.
South East Clinical Network – Perinatal Mental Health
Page 20
In West Kent support for women/families is offered via midwifery services/GP/health visiting
services and dependent on whether the baby is born alive i.e. admitted to local/tertiary neonatal
intensive care unit as bereavement support is offered via these services in tandem with universal
services input.
Medway Foundation Trust has a 0.6WTE bereavement specialist midwife, with 20 hrs dedicated
admin support at band 2.
Access to bereavement services within Dartford, Gravesham and Swanley is not known at this
point.
Obstetrician
There is an Obsterician with a special interest in perinatal mental health at Pembury Hospital
There is an Obsterician with a special interest in perinatal mental health in Darenth Valley Hospital.
There is an Obsterician with a special interest in perinatal mental health at Medway Hospital.
IAPT
IAPT services offer psychological therapies for common mild to moderate mental health problems,
including perinatal mental illness. Access to services is either through self-referral, GP referral or
referral by a health care professional.
Thinkaction offer guided self-help through: cognitive behavioural therapy; feel well, live well
programme; and counselling. Pregnant women and fathers are prioritised when referred.
Thinkaction also provides a young person’s service.
Insight talking therapies is a free and confidential service, commissioned by the NHS, and is available to anyone aged 18+ and living in Kent and Medway.
The East Kent IAPT Providers are: South Kent Coast CCG: Insight, Thinkaction, University Medical Centre, Dover Counselling Centre Thanet CCG: Insight, Thinkaction, University Medical Centre, Dover Counselling Centre Canterbury and Coastal CCG: Insight, Thinkaction, University Medical Centre, Psicon Ashford CCG: Insight, Thinkaction, University Medical Centre, Faversham Counselling Service
Voluntary Groups
Voluntary groups and peer support groups for perinatal mental health can be a valuable resource
for patients, but these services have not been systematically mapped across Kent and Medway.
With groups that have been set up independently, it is important these service providers receive
training to ensure that safe advice is provided.
Based on the outcomes of the scoping work carried out across Kent and Medway it appears there is
a correlation with the criteria levels indicated in the Everyone’s Business mapping.

South East Clinical Network – Perinatal Mental Health
Page 21
Specialist Community Perinatal Mental Health Teams – Surrey
The service provision in Surrey falls into the ‘no specialist service’ provision and all fall into level 0 and fall
short of national standards.
Table 16: Specialist community perinatal mental health teams provision in Surrey according to www.everyonesbusiness.org.uk
Level Description Clinical Commissioning
Group
0 No provision East Surrey
Guildford and Waverley
North West Surrey
Surrey Health
Surrey Downs
North East Hampshire
and Farnham
Comparison of Recommended Workforce
The tables below present the variance between the current staffing provision and the recommended level of
staffing within a perinatal community mental health team.
Table 17: Variance in perinatal community mental health team staffing per 10,000 deliveries for all Surrey
ALL SURREY
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 1.2 WTE
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 1.2 WTE
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 1.2 WTE
SPECIALIST COMMUNITY NURSES 5.0 WTE 6.1 WTE
PSYCHOLOGIST 1.0 WTE 1.2 WTE
OCCUPATIONAL THERAPIST 1.0 WTE 1.2 WTE
SOCIAL WORKER 0.5 WTE 0.6 WTE
COMMUNITY NURSERY NURSES 2.5 WTE 3.1 WTE
LINK MIDWIFE 1.5 DAY 1.8 DAY
LINK HEALTH VISITOR 1.5 DAY 1.8 DAY
TEAM SECRETARY/ADMIN 1 WTE 1.2 WTE
TOTAL 20.9
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)

South East Clinical Network – Perinatal Mental Health
Page 22
Table 18: Variance in perinatal community mental health team staffing per 10,000 deliveries in East Surrey
Table 19: Variance in perinatal community mental health team staffing per 10,000 deliveries in North West Surrey
Table 20: Variance in perinatal community mental health team staffing per 10,000 deliveries in Guildford and Waverley
EAST SURREY
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.2 WTE
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.2 WTE
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.2 WTE
SPECIALIST COMMUNITY NURSES 5.0 WTE 1.0 WTE
PSYCHOLOGIST 1.0 WTE 0.2 WTE
OCCUPATIONAL THERAPIST 1.0 WTE 0.2 WTE
SOCIAL WORKER 0.5 WTE 0.1 WTE
COMMUNITY NURSERY NURSES 2.5 WTE 0.5 WTE
LINK MIDWIFE 1.5 DAY 0.3 DAY
LINK HEALTH VISITOR 1.5 DAY 0.3 DAY
TEAM SECRETARY/ADMIN 1.0 WTE 0.2 WTE
TOTAL 3.6
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
NORTH WEST SURREY
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.4 WTE
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.4 WTE
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.4 WTE
SPECIALIST COMMUNITY NURSES 5.0 WTE 2.2 WTE
PSYCHOLOGIST 1.0 WTE 0.4 WTE
OCCUPATIONAL THERAPIST 1.0 WTE 0.4 WTE
SOCIAL WORKER 0.5 WTE 0.2 WTE
COMMUNITY NURSERY NURSES 2.5 WTE 1.1 WTE
LINK MIDWIFE 1.5 DAY 0.6 DAY
LINK HEALTH VISITOR 1.5 DAY 0.6 DAY
TEAM SECRETARY/ADMIN 1.0 WTE 0.4 WTE
TOTAL 7.3
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
GUILDFORD AND WAVERLEY
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.2 WTE
TRAINNE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.2 WTE
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.2 WTE
SPECIALIST COMMUNITY NURSES 5.0 WTE 1.0 WTE
PSYCHOLOGIST 1.0 WTE 0.2 WTE
OCCUPATIONAL THERAPIST 1.0 WTE 0.2 WTE
SOCIAL WORKER 0.5 WTE 0.1 WTE
COMMUNITY NURSERY NURSES 2.5 WTE 0.5 WTE
LINK MIDWIFE 1.5 DAY 0.3 DAY
LINK HEALTH VISITOR 1.5 DAY 0.3 DAY
TEAM SECRETARY/ADMIN 1.0 WTE 0.2 WTE
TOTAL 3.5
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS

South East Clinical Network – Perinatal Mental Health
Page 23
Table 21: Variance in perinatal community mental health team staffing per 10,000 deliveries in Surrey Downs
Table 22: Variance in perinatal community mental health team staffing per 10,000 deliveries in Surrey Heath
Specialist Community Mental Health Services
There is no local specialist perinatal mental health service commissioned in a dedicated way for
Surrey. The mainstream services do all work with women in the perinatal period and some roles
and pathways have been developed to respond as a priority such as IAPT services, a parent and
infant mental health service and recruitment of specialist mental health midwives in maternity
services.
Consultant Psychiatrist
There is no perinatal consultant psychiatrist in Surrey.
Clinical Nurse Specialist (CNS)
There is no perinatal clinical nurse specialist in Surrey.
Junior Doctor
There is no junior doctor supporting the clinical psychiatrist in Surrey.
SURREY DOWNS
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.3 WTE
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.3 WTE
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.3 WTE
SPECIALIST COMMUNITY NURSES 5.0 WTE 1.4 WTE
PSYCHOLOGIST 1.0 WTE 0.3 WTE
OCCUPATIONAL THERAPIST 1.0 WTE 0.3 WTE
SOCIAL WORKER 0.5 WTE 0.1 WTE
COMMUNITY NURSERY NURSES 2.5 WTE 0.7 WTE
LINK MIDWIFE 1.5 DAY 0.4 DAY
LINK HEALTH VISITOR 1.5 DAY 0.4 DAY
TEAM SECRETARY/ADMIN 1.0 WTE 0.3 WTE
TOTAL 4.9
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
SURREY HEATH
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.1 WTE
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.1 WTE
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.1 WTE
SPECIALIST COMMUNITY NURSES 5.0 WTE 0.5 WTE
PSYCHOLOGIST 1.0 WTE 0.1 WTE
OCCUPATIONAL THERAPIST 1.0 WTE 0.1 WTE
SOCIAL WORKER 0.5 WTE 0.0 WTE
COMMUNITY NURSERY NURSES 2.5 WTE 0.2 WTE
LINK MIDWIFE 1.5 DAY 0.1 DAY
LINK HEALTH VISITOR 1.5 DAY 0.1 DAY
TEAM SECRETARY/ADMIN 1.0 WTE 0.1 WTE
TOTAL 1.6
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS

South East Clinical Network – Perinatal Mental Health
Page 24
Psychologist
The workforce is not known at this point.
Occupational Therapist
There is no provision.
Social Worker
There is no provision.
Community Nursery Nurses
There is no provision.
Link Midwife*
There is 30 hours of a mental health liaison midwife’s time at Royal Surrey County Hospitals NHS
Foundation Trust.
There is 1 full time perinatal mental health specialist midwife (band 7) at Ashford and St Peters
Hospitals NHS Trust.
There is 1 wte specialist perinatal mental health midwife at Frimley NHS Foundation Trust.
Link Health Visitor*
There is no provision.
*Link midwife and link health visitors will not be included in the workforce table above until confirmed they will be a dedicated workforce
Other services/stakeholders
Maternal Bereavement Services
There is 1 x 30 hours bereavement midwife at the Royal Surrey County Hospitals NHS Foundation
Trust.
There is 1 full time bereavement/counselling midwife (band 7) and 1 full time support midwife (band
6) at Ashford and St Peters Hospitals NHS Trust.
On the Frimley site there are a team of 3 midwives who have one day a week to support bereaved
families.
There is no specific role on the Wexham site but they do have one midwife with a special interest.
Obstetrician
There is 1 consultant with specialist mental health interest (3 hours per week protected time) at the
Royal Surrey County Hospitals NHS Foundation Trust.

South East Clinical Network – Perinatal Mental Health
Page 25
There is 1 session per week from a consultant obstetrician with a specialist interest in perinatal
mental health. The clinic is run jointly by a specialist midwife at Ashford and St Peters Hospitals
NHS Trust.
Five hours (1 clinic every week) are available at Surrey and Sussex Health Care Trust.
There is 1 PA from an obstetrician with special interest at Frimley Park Hospital.
IAPT
IAPT services offer psychological therapies for common mild to moderate mental health problems,
including perinatal mental illness. Access to services is either through self-referral, GP referral or
referral by a health care professional.
Data about IAPT service provision is lacking.
Parent and Infant Mental Health Services
The Surrey Parent-Infant Mental Health Service (PIMHS) is a multi-agency service that provides a
tiered approach to working with vulnerable parents and their babies. CAMHS staff work closely with
specialist health visitors and the 0-19 public health nursing teams, now employed by Virgin, Central
Surrey Health and First Community Health. In total 4.1WTE are employed by this service
.
The PIMH service takes a strategic approach to promoting parent-infant mental health through
raising the awareness of its importance across agencies and professionals working with families in
Surrey. Training and workforce development is central in ensuring that practitioners are skilled at
identifying parent and infant relationships at risk. This supports appropriate referrals to the PIMH
service.
The service provides a tiered range of provision to meet the needs of infants and their families. This
includes targeted baby massage groups and individual intervention by specialist health visitors.
There is also access to specialist parent and infant psychotherapy for families with complex needs.
Voluntary Groups
Voluntary groups and peer support groups for perinatal mental health can be a valuable resource
for patients, but these services have not been systematically mapped across Surrey. With groups
that have been set up independently, it is important these service providers receive training to
ensure that safe advice is provided.
Based on the outcomes of the scoping work carried out across Surrey it appears there is a
correlation with the criteria levels indicated in the Everyone’s Business mapping.
South East Clinical Network – Perinatal Mental Health
Page 26
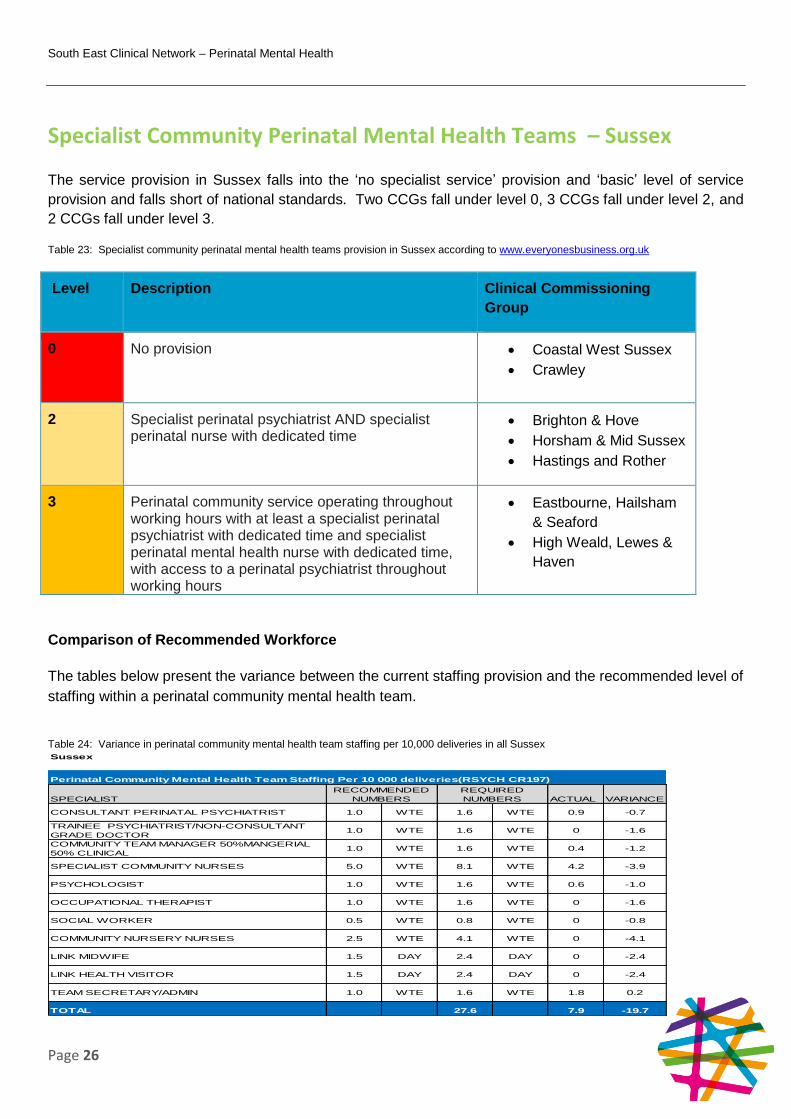
Specialist Community Perinatal Mental Health Teams – Sussex
The service provision in Sussex falls into the ‘no specialist service’ provision and ‘basic’ level of service
provision and falls short of national standards. Two CCGs fall under level 0, 3 CCGs fall under level 2, and
2 CCGs fall under level 3.
Table 23: Specialist community perinatal mental health teams provision in Sussex according to www.everyonesbusiness.org.uk
Level Description Clinical Commissioning
Group
0 No provision Coastal West Sussex
Crawley
2 Specialist perinatal psychiatrist AND specialist perinatal nurse with dedicated time
Brighton & Hove
Horsham & Mid Sussex
Hastings and Rother
3 Perinatal community service operating throughout working hours with at least a specialist perinatal psychiatrist with dedicated time and specialist perinatal mental health nurse with dedicated time, with access to a perinatal psychiatrist throughout working hours
Eastbourne, Hailsham
& Seaford
High Weald, Lewes &
Haven
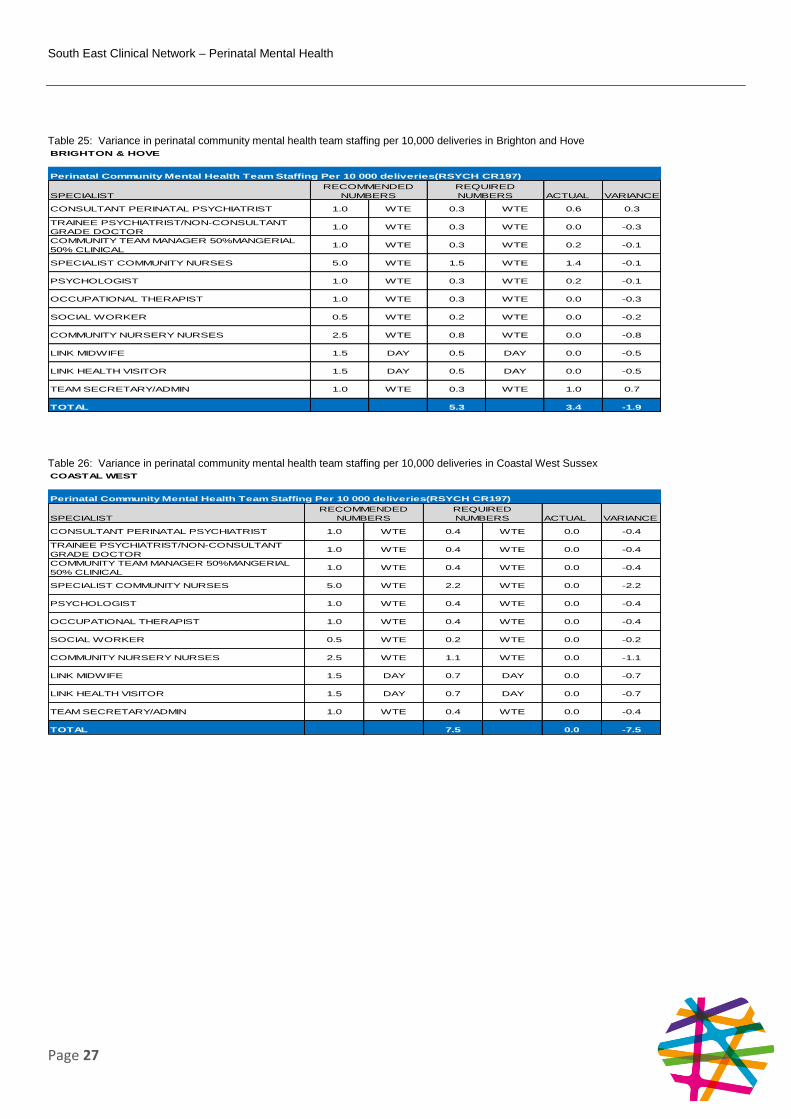
Comparison of Recommended Workforce
The tables below present the variance between the current staffing provision and the recommended level of
staffing within a perinatal community mental health team.
Table 24: Variance in perinatal community mental health team staffing per 10,000 deliveries in all Sussex
Sussex
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 1.6 WTE 0.9 -0.7
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 1.6 WTE 0 -1.6
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 1.6 WTE 0.4 -1.2
SPECIALIST COMMUNITY NURSES 5.0 WTE 8.1 WTE 4.2 -3.9
PSYCHOLOGIST 1.0 WTE 1.6 WTE 0.6 -1.0
OCCUPATIONAL THERAPIST 1.0 WTE 1.6 WTE 0 -1.6
SOCIAL WORKER 0.5 WTE 0.8 WTE 0 -0.8
COMMUNITY NURSERY NURSES 2.5 WTE 4.1 WTE 0 -4.1
LINK MIDWIFE 1.5 DAY 2.4 DAY 0 -2.4
LINK HEALTH VISITOR 1.5 DAY 2.4 DAY 0 -2.4
TEAM SECRETARY/ADMIN 1.0 WTE 1.6 WTE 1.8 0.2
TOTAL 27.6 7.9 -19.7
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
South East Clinical Network – Perinatal Mental Health
Page 27
Table 25: Variance in perinatal community mental health team staffing per 10,000 deliveries in Brighton and Hove
Table 26: Variance in perinatal community mental health team staffing per 10,000 deliveries in Coastal West Sussex
BRIGHTON & HOVE
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.3 WTE 0.6 0.3
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.3 WTE 0.0 -0.3
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.3 WTE 0.2 -0.1
SPECIALIST COMMUNITY NURSES 5.0 WTE 1.5 WTE 1.4 -0.1
PSYCHOLOGIST 1.0 WTE 0.3 WTE 0.2 -0.1
OCCUPATIONAL THERAPIST 1.0 WTE 0.3 WTE 0.0 -0.3
SOCIAL WORKER 0.5 WTE 0.2 WTE 0.0 -0.2
COMMUNITY NURSERY NURSES 2.5 WTE 0.8 WTE 0.0 -0.8
LINK MIDWIFE 1.5 DAY 0.5 DAY 0.0 -0.5
LINK HEALTH VISITOR 1.5 DAY 0.5 DAY 0.0 -0.5
TEAM SECRETARY/ADMIN 1.0 WTE 0.3 WTE 1.0 0.7
TOTAL 5.3 3.4 -1.9
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
COASTAL WEST
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.4 WTE 0.0 -0.4
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.4 WTE 0.0 -0.4
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.4 WTE 0.0 -0.4
SPECIALIST COMMUNITY NURSES 5.0 WTE 2.2 WTE 0.0 -2.2
PSYCHOLOGIST 1.0 WTE 0.4 WTE 0.0 -0.4
OCCUPATIONAL THERAPIST 1.0 WTE 0.4 WTE 0.0 -0.4
SOCIAL WORKER 0.5 WTE 0.2 WTE 0.0 -0.2
COMMUNITY NURSERY NURSES 2.5 WTE 1.1 WTE 0.0 -1.1
LINK MIDWIFE 1.5 DAY 0.7 DAY 0.0 -0.7
LINK HEALTH VISITOR 1.5 DAY 0.7 DAY 0.0 -0.7
TEAM SECRETARY/ADMIN 1.0 WTE 0.4 WTE 0.0 -0.4
TOTAL 7.5 0.0 -7.5
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS

South East Clinical Network – Perinatal Mental Health
Page 28
Table 27: Variance in perinatal community mental health team staffing per 10,000 deliveries in Crawley
Table 28: Variance in perinatal community mental health team staffing per 10,000 deliveries in Horsham and Mid-Sussex
Table 29: Variance in perinatal community mental health team staffing per 10,000 deliveries in Eastbourne, Hailsham and Seaford
CRAWLEY
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.2 WTE 0.0 -0.2
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.2 WTE 0.0 -0.2
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.2 WTE 0.0 -0.2
SPECIALIST COMMUNITY NURSES 5.0 WTE 0.9 WTE 0.0 -0.9
PSYCHOLOGIST 1.0 WTE 0.2 WTE 0.0 -0.2
OCCUPATIONAL THERAPIST 1.0 WTE 0.2 WTE 0.0 -0.2
SOCIAL WORKER 0.5 WTE 0.1 WTE 0.0 -0.1
COMMUNITY NURSERY NURSES 2.5 WTE 0.4 WTE 0.0 -0.4
LINK MIDWIFE 1.5 DAY 0.3 DAY 0.0 -0.3
LINK HEALTH VISITOR 1.5 DAY 0.3 DAY 0.0 -0.3
TEAM SECRETARY/ADMIN 1.0 WTE 0.2 WTE 0.0 -0.2
TOTAL 2.9 0.0 -2.9
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
HORSHAM & MID SUSSEX
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.2 WTE 0.1 -0.1
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.2 WTE 0.0 -0.2
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.2 WTE 0.0 -0.2
SPECIALIST COMMUNITY NURSES 5.0 WTE 1.1 WTE 0.0 -1.1
PSYCHOLOGIST 1.0 WTE 0.2 WTE 0.0 -0.2
OCCUPATIONAL THERAPIST 1.0 WTE 0.2 WTE 0.0 -0.2
SOCIAL WORKER 0.5 WTE 0.1 WTE 0.0 -0.1
COMMUNITY NURSERY NURSES 2.5 WTE 0.6 WTE 0.0 -0.6
LINK MIDWIFE 1.5 DAY 0.3 DAY 0.0 -0.3
LINK HEALTH VISITOR 1.5 DAY 0.3 DAY 0.0 -0.3
TEAM SECRETARY/ADMIN 1.0 WTE 0.2 WTE 0.0 -0.2
TOTAL 3.8 0.1 -3.7
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
EASTBOURNE, HAILSHAM & SEAFORD
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.2 WTE 0.1 -0.1
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.2 WTE 0.0 -0.2
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.2 WTE 0.1 -0.1
SPECIALIST COMMUNITY NURSES 5.0 WTE 0.8 WTE 1.0 0.2
PSYCHOLOGIST 1.0 WTE 0.2 WTE 0.0 -0.2
OCCUPATIONAL THERAPIST 1.0 WTE 0.2 WTE 0.0 -0.2
SOCIAL WORKER 0.5 WTE 0.1 WTE 0.0 -0.1
COMMUNITY NURSERY NURSES 2.5 WTE 0.4 WTE 0.0 -0.4
LINK MIDWIFE 1.5 DAY 0.3 DAY 0.0 -0.3
LINK HEALTH VISITOR 1.5 DAY 0.3 DAY 0.0 -0.3
TEAM SECRETARY/ADMIN 1.0 WTE 0.2 WTE 0.2 0.0
TOTAL 2.9 1.4 -1.5
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS

South East Clinical Network – Perinatal Mental Health
Page 29
Table 30: Variance in perinatal community mental health team staffing per 10,000 deliveries in Hastings and Rother
Table 31: Variance in perinatal community mental health team staffing per 10,000 deliveries in High Weald, Lewes and Havens
Specialist Community Mental Health Services
Brighton and Sussex University Hospital NHS Trust provides a specialist psychiatric consultant
service with mental health practitioners in the acute hospital including joint clinics with obstetricians
as well as a community clinic in a children’s centre and home visits. The whole service focuses on
needs for mothers with complex and severe mental health needs.
NHS Crawley CCG and NHS Horsham and Mid Sussex CCGs do not have any dedicated perinatal
MH services in the area although the current MH services offer a fast track for women with PMH
issues within services such as Time To Talk (IAPT service).
NHS Coastal West Sussex has no specialist service provision.
The 3 CCGs within East Sussex have recently commissioned an extended perinatal mental health service for East Sussex that is delivered by Sussex Partnership NHS Foundation Trust. Three extra consultant psychiatrist sessions have been commissioned but the post has not yet been appointed to.
HASTINGS & ROTHER
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.2 WTE 0.1 -0.1
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.2 WTE 0.0 -0.2
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.2 WTE 0.1 -0.1
SPECIALIST COMMUNITY NURSES 5.0 WTE 0.8 WTE 1.0 0.2
PSYCHOLOGIST 1.0 WTE 0.2 WTE 0.4 0.2
OCCUPATIONAL THERAPIST 1.0 WTE 0.2 WTE 0.0 -0.2
SOCIAL WORKER 0.5 WTE 0.1 WTE -0.1
COMMUNITY NURSERY NURSES 2.5 WTE 0.4 WTE 0.0 -0.4
LINK MIDWIFE 1.5 DAY 0.2 DAY 0.0 -0.2
LINK HEALTH VISITOR 1.5 DAY 0.2 DAY 0.0 -0.2
TEAM SECRETARY/ADMIN 1.0 WTE 0.2 WTE 0.4 0.2
TOTAL 2.8 2.0 -0.8
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS
HIGH WEALD, LEWES AND HAVEN
SPECIALIST ACTUAL VARIANCE
CONSULTANT PERINATAL PSYCHIATRIST 1.0 WTE 0.1 WTE 0.0 -0.1
TRAINEE PSYCHIATRIST/NON-CONSULTANT
GRADE DOCTOR1.0 WTE 0.1 WTE 0.0 -0.1
COMMUNITY TEAM MANAGER 50%MANGERIAL
50% CLINICAL1.0 WTE 0.1 WTE 0.0 -0.1
SPECIALIST COMMUNITY NURSES 5.0 WTE 0.7 WTE 0.8 0.1
PSYCHOLOGIST 1.0 WTE 0.1 WTE 0.0 -0.1
OCCUPATIONAL THERAPIST 1.0 WTE 0.1 WTE 0.0 -0.1
SOCIAL WORKER 0.5 WTE 0.1 WTE 0.0 -0.1
COMMUNITY NURSERY NURSES 2.5 WTE 0.4 WTE 0.0 -0.4
LINK MIDWIFE 1.5 DAY 0.2 DAY 0.0 -0.2
LINK HEALTH VISITOR 1.5 DAY 0.2 DAY 0.0 -0.2
TEAM SECRETARY/ADMIN 1.0 WTE 0.1 WTE 0.2 0.1
TOTAL 2.4 1.0 -1.4
Perinatal Community Mental Health Team Staffing Per 10 000 deliveries(RSYCH CR197)
RECOMMENDED
NUMBERS
REQUIRED
NUMBERS

South East Clinical Network – Perinatal Mental Health
Page 30
Consultant Psychiatrist
NHS Crawley CCG and NHS Horsham and Mid Sussex CCG (West Sussex) have a specialist
perinatal assessment clinic at Princess Royal Hospital (managed by the specialist perinatal mental
health team at SPFT) which runs for ½ a day a week for patients at risk of developing severe PMH
problems (however the clinic is only available for women booked to deliver, or who have delivered,
at Princess Royal Hospital) (see tables above)
NHS Brighton and Hove CCG has a part time (0.6 WTE) consultant who has joint clinics with the
obstetrician as well as community clinics. Brighton and Sussex University Hospitals NHS Trust has
a weekly fixed session (8 hours) in the out-of-hours acute liaison team.
The 3 East Sussex CCGs commission a consultant as per the tables above.
NHS Coastal West Sussex has no commissioned consultant.
Clinical nurse Specialist (CNS)
There is no provision.
Junior Doctor
There is no junior doctor supporting the specialist perinatal mental health teams in Sussex.
Psychologist
Brighton and Hove CCG has commissioned 1 day a week from a band 8 clinical psychologist,
specialising in parent-infant psychotherapy to work within the specialist perinatal mental health
team. No other specialist psychologist time is commissioned in Sussex. The specialist perinatal
mental health teams work closely with IAPT services.
Occupational Therapist
There is no provision.
Social Worker
There is no provision. The specialised perinatal mental health team works closely with local children
and families social services teams and health visitors.
Community Nursery Nurses
There is no provision.
Link Midwife*
Brighton and Sussex University Hospitals NHS Trust is developing a business case to provide a
cross site specialist midwife but this has not yet resulted in funding being agreed for such a post.
Hastings Conquest Hospital has appointed a specialist perinatal mental health midwife who works
closely with a consultant obstetrician who has a special interest in perinatal mental health.
Western Sussex Hospitals NHS Trust has a Senior Public Health midwife.
There is a 0.4WTE perinatal MH specialist midwife in East Sussex.

South East Clinical Network – Perinatal Mental Health
Page 31
Link Health Visitor*
Brighton & Hove has a senior health visitor (HV) who leads on mental health within the HV team.
The health visiting service in Brighton and Hove is currently undergoing a re-procurement where
there are opportunities to address this gap.
There is a full time specialist health visitor in East Sussex, who manages the Afterthoughts Counselling service offering 10 counselling sessions to mothers during pregnancy or parents with a child under 5 or anyone with loss or trauma relating to pregnancy and birth. The health visitor also works with the perinatal mental health champion health visitors who run groups for mothers with mild to moderate postnatal depression, is responsible mental health education within the service and has a remit to review compliance with NICE guidance and writing/reviewing organisational policies relating to perinatal mental health.
*Link Midwife and Link Health Visitors will not be included in the workforce table above until confirmed they will be a dedicated workforce
Team Secretary Admin
Brighton and Hove has a full time team administrator.
East Sussex also has dedicated admin time.
Other services/stakeholders
Maternal Bereavement Services
Brighton and Sussex University Hospitals NHS Trust provides 15 hours a week.
Western Sussex Hospitals NHS Trust has a band 7 post on both hospital sites (SRH and WH).
NHS Crawley CCG and NHS Horsham and Mid Sussex CCG have no service.
The 3 CCGs within East Sussex have a partial service.
Obstetrician
Brighton and Sussex University Hospitals NHS Trust has a consultant obstetrician who works
alternate weeks for an antenatal clinic session (10 hours per month) who is also lead consultant for
women with perinatal mental health problems - this is flexible cover for inpatient care.
Surrey and Sussex Hospitals NHS Trust provides 1 clinic a week (5hrs).
Hastings Conquest Hospital has a consultant obstetrician with a special interest in maternal mental
health but who does not work with the perinatal mental health team specifically.
IAPT
IAPT services offer psychological therapies for common mild to moderate mental health problems,
including perinatal mental illness. Access to services is either through self-referral, GP referral or

South East Clinical Network – Perinatal Mental Health
Page 32
referral by a health care professional. Women are referred to IAPT’s services such as the Wellbeing
Service and Time to Talk.
Voluntary Groups
Voluntary groups and peer support groups for perinatal mental health can be a valuable resource
for patients, but these services have not been systematically mapped across Sussex. With groups
that have been set up independently, it is important these service providers receive training to
ensure that safe advice is provided.
Based on the outcomes of the perinatal mental health survey and the work carried out by Crawley,
Horsham and Mid Sussex CCG and Western Sussex Hospitals NHS Trust it appears that Crawley,
Horsham and Mid Sussex and Coastal West Sussex should all align to level 0 based on the criteria.
East Sussex has three CCG areas; the perinatal mental health provision is commissioned across them all.
For accuracy, the resource has been split across the CCG areas as there is an allocated nurse and
consultant for each area. There is 0.2 consultant time across East Sussex which has been added to their
actual areas (Hastings and Eastbourne), although women from the High Weald, Lewes and Havens CCG
do still get access to these medics. No women in east Sussex gets access to more than one session per
week of consultant time and part time specialist nurse cover.
West Sussex has 0 provision in all areas now that the 0.1wte perinatal mental health consultant clinic at
Princess Royal Haywards Heath clinic has stopped.
Based on the outcomes of the scoping work carried out across Sussex it appears that Brighton and
Hove CCG service provision should be aligned to criteria 3 and that Eastbourne, Hailsham &
Seaford and High Weald, Lewes & Haven should align to criteria 2.

South East Clinical Network – Perinatal Mental Health
Page 33
Mother and Baby Units
Table 32: Mother and baby units in the UK Source; Everyone’s Business campaign – www.everyonesbusiness.org.uk
The Clinical Reference Group for Perinatal Mental Health (NHSE, 2013) has stated that, based on the
prevalence of post-partum psychosis (2/1000 live births) and serious mental illness (2/1000 live births), an
estimated 2,750 women in England will need access to mother and baby units. It is reported that due to
capacity and demand issues and lack of service provision many women have to access general adult
mental health wards, which for women with serious mental health problems can have an adverse effect on
both her and her child in the future. Separation prevents early attachment, bonding and breastfeeding
(JCPMH, 2012).
There are 15 mother and baby units in England with 115 beds, with significant gaps in local provision. The
research carried out by the NHS Benchmarking Network (2015) found that some women have to travel
100km to access a unit. There is no designated mother and baby unit in the South East since the
Eastbourne T4 perinatal independent provider left the market due to a recurring under 30% occupancy on a
6 bed unit. The reasons for this under-occupancy appear to be complex and do not necessarily indicate a
lack of need.
The NHS Benchmarking research found that in 2014/15 women across the South East were admitted to
mother and baby units provided by Central and North West London NHS Foundation Trust, East London
NHS Foundation Trust, Hertfordshire Partnership University NHS Foundation Trust, South London and
Maudsley NHS Foundation Trust and the Southern Health NHS Foundation Trust. The latter two units are
where the majority of women in the South East were admitted.
Based on the Clinical Reference Group’s assumptions, the estimated number of women in Kent, Surrey
and Sussex potentially needing access to a mother and baby unit equates to around 194 women. It is also
suggested that the number of beds required will range from 0.25 -0.5/1000 live births dependent on the
South East Clinical Network – Perinatal Mental Health
Page 34
availability of specialist community perinatal mental health teams, meaning that the bed requirement for
Kent, Surrey and Sussex is between 12 and 24 beds per year. From 1st April 2014 to 4th February 2015
there were 19 admissions to Mother and Baby units from women across Kent and Sussex. There were no
admissions from women in Surrey.
The recommendation for mother and baby units is that specialist perinatal community mental health teams
form links with mother and baby units. It was reported in the perinatal mental health survey that referral
into mother and baby units is via current specialist perinatal mental health services/NHS England and that
access into to these units is dependent on availability.
As part of the research a snapshot in time (31/03/2015) was audited on the bed occupancy rate at mother
and baby units across England. The findings were as follows:
65%/62% (mean/median, excluding leave)
82%/85% (mean/median, including leave)
It is also reported that delayed transfers of care are very rare.
The optimum occupancy rate recommended by the Royal College of Psychiatrists is 85% for mental health
wards. This enables patients to take leave without losing their bed on the ward and avoids delays in
admission (RCPsych, 2011).
Based on the Clinical Reference Group’s assumptions, access being dependent on availability, travelling
distance and optimum occupancy rate, further work needs to take place to understand the bed
requirements and capacity throughout the year at individual unit level. There is an important need to
understand the total number of women admitted to a mother and baby unit along with the number of
women that had their needs met on an acute mental health ward or who had home treatment by a crisis
resolution and home treatment team or received their care on a maternity ward due to lack of availability or
choice not to travel.
Workforce and Training
Health Education England (HEE) has mandated post-registration training in perinatal mental health to
ensure that trained specialist mental health staff are available to support mothers in every birthing unit by
2017 (DoH, 2015b). They are also supporting the development of workforce capacity and capability in
specialist perinatal mental health services as part of the broader HEE mental health workforce strategy. To
date, HEE has established a national training and workforce steering group (with membership from all of
the Royal Colleges and including the Institute of Health Visiting and CPHVA) to support this work stream
and a partnership grant has been agreed between HEE, NHSE and RCPSYCH to establish a clinical
psychiatry bursary scheme in 2016 which will provide bursaries to train consultant psychiatrists as clinical
leads for the new perinatal mental health services.
Health Education Kent, Surrey and Sussex has commissioned 2 training programmes. The first is a series
of one day awareness workshops offered by the Institute of Health Visiting. They are offered to GPs,
practice nurses, obstetricians, midwives, neonatal nurses, mental health nurses, health visitors (who have
not already received iHV Perinatal Mental Health training) and other health professionals who work with
women, babies and children. The second is the Maudsley Simulation (part of South London and Maudsley
NHS Foundation Trust) perinatal mental health simulation training event which re-creates real-life clinical
situations in a safe environment which does not impact on patients. . It is a one-day inter-professional
South East Clinical Network – Perinatal Mental Health
Page 35
course suitable for a range of health care professionals, including all grades of psychiatrists and
obstetricians who are involved in the care of women with mental health problems, both during pregnancy or
following delivery.
The Royal College of General Practitioners has developed a perinatal mental health toolkit which includes a
range of resources that support primary care team members to deliver the best care to women with
perinatal mental health problems. The toolkit was launched on the 22nd July and can be found using the
following link Perinatal Mental Health Toolkit.
Key Issues and Barriers
Outcomes of scoping work
National Seminar
The findings of the perinatal and infant mental health national seminar held in July 2015 by the Mental
Health Foundation and National Children’s Bureau are as follows:
11 of the 12 Clinical Networks attended the seminar to understand the work that is being done
across the country.
It was found that there is varying work being undertaken which included mapping provision,
pathway development, workforce training and CQUINs.
It was found that there is lot of work going on that lacks coordination.
Some areas are further forward in developing networks than others.
There should be better integration and collaboration across stakeholders, which should include
CAMHS and IAPT services to deliver optimal maternal mental health and wellbeing for the mothers
and children.
There should be improved training with key competencies for perinatal mental health being a
tangible solution.
Data collection requires improvement.
The lack of a minimum data set can impede the true reflection of women with mental health
problems.
Prevention and early identification are key to the pathway.
South East
A significant amount of scoping work has already been undertaken across Kent, Surrey and Sussex. At
this point it is important to note that the perinatal mental health survey that was completed by clinical
commissioning groups and maternity providers had its limitations as it did not involve the wider provider
landscape such as primary care, the voluntary sector, local authorities or mental health trusts.

South East Clinical Network – Perinatal Mental Health
Page 36
According to the information to date there appears to be significant variation and gaps in service provision
across Kent, Surrey and Sussex. Identified below are the key themes that are creating barriers to closing
the gaps in service provision:-
Demand versus capacity within current service provision.
Lack of finance or staffing capacity within current resources.
Lack of funding to resource future developments.
Limited or no access to a perinatal psychiatrist.
Limited or no access to a specialist perinatal mental health midwife with dedicated time.
Inconsistent specialist support that adheres to national guidance.
Referral pathways and criteria for access to IAPT’s and specialist perinatal mental health services
unclear or unknown to some professionals.
Referrals to specialist service bounced back to the referrer as they do not meet the criteria.
Long waiting lists and in some cases limited access to service provision, in particular for mild to
moderate perinatal mental health problems.
Limitations of current documentation and data extrapolation to record the severity of perinatal
mental health problems.
Variation in voluntary sector provision and lack of information about what is available.
Delays in referral and early intervention.
Lack of confidence, skills and competencies in identifying and caring for women with perinatal
mental health problems.
The quantitative data in this report clearly demonstrates the inequity of access and service provision but
understanding is also required of the impact of these gaps and variation on other services and the impact
on women and their families.
Priorities for Change
Through the scoping work and within workshops, South East stakeholders identified key priorities that could
change and improve future perinatal mental health services:
Further exploration of data regarding women who report mental health issues at booking,
specifically in relation to geographical differences and severity of mental health problem.
Whole system workforce training for staff to improve communication, knowledge, confidence and
care planning for mental health in the perinatal period.
Improvement in documentation for collection of information, to improve care standards
Representation of all stakeholders to learn about local pathways and the role of different partners.
Improved communication and information sharing between services.
Improved information for families about the range of services available including the digital
technology.
Streamlining local processes across the system.
Commissioning of an ageless pathway to address the age gap.
A common assessment tool for use across all professionals.
Integrated service pathway agreed by all stakeholders identifying roles, responsibilities and
competencies.

South East Clinical Network – Perinatal Mental Health
Page 37
Access to specialist clinical advice.
Services to focus on universal, targeted and specialist provision.
Summary and Recommendations
Summary
Good perinatal mental health is integral to both emotional and physical wellbeing, and the development of
the infant, child and young person. To provide equitable access and high quality perinatal mental health
services we need to fully understand the inequities along with the wider determinants of health and social
care within local populations.
The level of service provision required and the numerous access points clearly demonstrates how essential
partnership working and collaboration are to make service improvements through a whole system
approach. Across the South East there is a drive to develop an integrated pathway alongside the delivery
of education and training to staff within all organisations that come into contact with the woman and her
family during the perinatal period. Service improvement cannot be carried out in isolation and any agreed
model of perinatal mental health care can only be as good as the commitment of all involved.
There has been a significant amount of work carried out, not only nationally but also across the South East
footprint. Based on the findings there is still much work to be done to deliver services based on national
guidance and standards. This work along with the inclusion of local plans signifies the commitment to
improve and develop services that meet the needs of women and their families and it should be used as
the building blocks to bridging the gaps.
Partnership working and collaboration from all stakeholders, not forgetting the important contribution from
the voluntary sector and service user engagement, are key to service improvement.
Delivering the vision of sustainable perinatal mental health services and a seamless integrated perinatal
mental health pathway needs to be achieved through the principles of collaborative clinical leadership,
collaborative commissioning and service user expertise. New models of care, commissioning and
contracting need to reflect and be tailored to meet the needs of the local population (RCP, 2015).
Recommendations
The National Perinatal Mental Health Programme recommends the establishment of perinatal mental health
clinical networks (PMH CNs) as the vehicle for delivering transformed services, and this aligns also with the
NICE guidance. The South East Clinical Network has supported the development of three locality Perinatal
Mental Health Networks: Kent and Medway, Surrey and Sussex, which will be brought together as required
into a pan South East perinatal mental health network. It is not yet fully understood whether these
footprints will need in future to align with the strategic transformation planning (STP) footprints.

South East Clinical Network – Perinatal Mental Health
Page 38
It is recommended that this scoping paper is approved and signed off by each perinatal mental health
clinical network in the South East as an accurate baseline of current service provision.
It is further recommended that the South East and locality perinatal mental health clinical networks are
used as the vehicle for maintaining a strategic overview of the gaps and needs within each locality in order
to support the delivery of the 5 year transformation programme. It is suggested that each clinical network
takes on:
Development of a perinatal mental health integrated care pathway that has defined roles,
responsibilities and competencies to ensure the effective transfer of information and continuity of
care. This will be a high level pathway that should be adapted to meet the needs of the local
demographics.
Partnership working with Health Education England and Health Education Kent, Surrey and Sussex
to support the development of workforce strategies and training programmes.
Engagement and collaboration across the system to enable economies of scale and economies of
scope.
Development of a culture of shared learning through lessons learnt, peer review, and stakeholder
events.
These networks are voluntary collaborations that include commissioners, providers, the third sector and
patient representatives. They do not replace the existing formal decision making responsibilities and
governance arrangements of CCGs..
Further data analysis is required to quantify the number of women diagnosed with a perinatal mental Illness
against national prevalence rates and referrals into each service area to gain a full understanding of where
women are having their needs met. There needs to be an agreed process for collecting data until national
datasets are developed and implemented to undertake this function.
Future service improvement should also align to recommendations and programmes of work as advised by
NHS England’s Mental Health Strategy and the National Maternity Review.

South East Clinical Network – Perinatal Mental Health
Page 39
Appendices
Appendix 1
Resources for Standards and Guidance
The following guidance, standards and recommendations support the development and service
improvement for all those involved in Perinatal Mental Health.
JCPMH (2013) Ten key messages for commissioners – Joint commissioning Panel for Perinatal Mental
Health http://www.jcpmh.info/resource/guidance-perinatal-mental-health-services/
RCPSYCH (2015) CR197. Perinatal mental health services: Recommendations for the provision of services
for childbearing women http://www.rcpsych.ac.uk/usefulresources/publications/collegereports/cr/cr197
Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance Antenatal and
postnatal mental health: clinical management and service guidance | Guidance and guidelines | NICE
NHSIQ (2015) Improving Access to Perinatal Mental Health Services in England - A review - NHS
Improving Quality www.nhsiq.nhs.uk/media/2696378/nhsiq_perinatal_mental_health
RCPsych,The Quality Network for Perinatal Mental Health Services CCQI (2014): Service Standards:
Second Edition Perinatal Community Mental Health Services: http://everyonesbusiness.org.uk/wp-
content/uploads/2015/04/Perinatal-Community-Standards-2nd-edition.pdf
HEE (2016) Specialist Health Visitors in Perinatal & Infant Mental Health: What they do and why they
matter:https://www.hee.nhs.uk/sites/default/files/documents/Specialist%20Health%20Visitors%20in%20Per
inatal%20and%20Mental%20Health%20FINAL%20low%20res.pdf
BPS (2016) Briefing Paper No. 8 Update, February 2016 Perinatal Service Provision: The role of Perinatal Clinical Psychology: https://www.bps.org.uk/system/files/user-files/Division%20of%20Clinical%20Psychology/public/rep108_perinatal_service_provision.pdf MMHA (2013): Specialist Mental Health Midwives: What they do and why they matter: http://www.baspcan.org.uk/files/MMHA%20SMHMs%20Report.pdf
The Early Years High Impact Area 2 – Perinatal Mental Health
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/413129/2902452_Early_Year
s_Impact_2_V0_1W.pdf

South East Clinical Network – Perinatal Mental Health
Page 40
Appendix 2
Antenatal and postnatal mental health NICE quality standard [QS115]
February 2016:
Statement 1. Women of childbearing potential are not prescribed valproate to treat a mental health problem. Statement 2. Women of childbearing potential with a severe mental health problem are given information at their annual review about how their mental health problem and its treatment might affect them or their baby if they become pregnant. Statement 3. Pregnant women with a previous severe mental health problem or any current mental health problem are given information at their booking appointment about how their mental health problem and its treatment might affect them or their baby. Statement 4. Women are asked about their emotional wellbeing at each routine antenatal and postnatal contact. Statement 5. Women with a suspected mental health problem in pregnancy or the postnatal period receive
a comprehensive mental health assessment.
Statement 6. Women referred for psychological interventions in pregnancy or the postnatal period start
treatment within 6 weeks of referral.
Statement 7 (developmental). Specialist multidisciplinary perinatal community services and inpatient psychiatric mother and baby units are available to support women with a mental health problem in pregnancy or the postnatal period.

South East Clinical Network – Perinatal Mental Health
Page 41
Appendix 3
Glossary of Perinatal Mental Health Conditions
Adjustment disorders
Adjustment Disorder is a state of mixed emotions such as depression and anxiety which occurs as a
reaction to major life events or when having to face major life changes such as illness or relationship
breakdown
Mild-moderate depression and anxiety
The main symptoms of depression are losing pleasure in things that were once enjoyable and losing
interest in other people and usual activities. A person with depression may also commonly experience
some of the following: feeling tearful, irritable or tired most of the time, changes in appetite, and problems
with sleep, concentration and memory. People with depression typically have lots of negative thoughts and
feelings of guilt and worthlessness. Sometimes people with depression harm themselves, have thoughts
about suicide, or may even attempt suicide.
Mild depression is when a person has a small number of symptoms that have a limited effect on their daily
life. Moderate depression is when a person has more symptoms that can make their daily life much more
difficult than usual.
Mild anxiety is experienced as feelings of being overwhelmed by responsibilities and unable to cope.
People with depression may have feelings of anxiety as well.
Postpartum psychosis
Postpartum psychosis (or puerperal psychosis) is a severe episode of mental illness which begins suddenly
in the days or weeks after having a baby. Symptoms vary and can change rapidly. They can include high
mood (mania), depression, confusion, hallucinations and delusions.
Post-traumatic stress disorder
Postnatal Post Traumatic Stress Disorder (PTSD) is experienced as nightmares, flashbacks, anger, and
difficulty concentrating and sleeping. It may be a pre-existing condition or be triggered by a traumatic
labour.
Serious mental illness (severe mental illness)
Serious mental illness includes diagnoses which involve psychosis. The most common disorders which are
associated with psychotic symptoms are schizophrenia, bipolar disorder and psychotic depression.
Psychosis is used to describe symptoms or experiences that happen together. Each person will have
different symptoms, but the common feature is that they do not experience reality like most people. A
person with psychosis may have: hallucinations, delusions, muddled thinking, lack of insight

South East Clinical Network – Perinatal Mental Health
Page 42
Severe depressive illness
Severe depression is when a person has many symptoms that can make their daily life extremely difficult.
Sometimes a person with severe depression may have hallucinations and delusions (psychotic symptoms).

South East Clinical Network – Perinatal Mental Health
Page 43
References BPS (2016) Briefing Paper No. 8 Update, February 2016 Perinatal Service Provision: The role of Perinatal
Clinical Psychology:
https://www.bps.org.uk/system/files/userfiles/Division%20of%20Clinical%20Psychology/public/rep108_peri
natal_service_provision.pdf
Centre for Mental Health, (2015) Falling through the gaps: perinatal mental health and general practice for
mental health
DoH, 2013 A mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015
Department of Health Department of Health
DoH, 2014 A mandate from the Government to the NHS Commissioning Board: April 2014 to March 2015
Department of Health Department of Health
DoH, 2015a A mandate from the Government to the NHS Commissioning Board: April 2016 to March 2017
Department of Health Department of Health
DoH, 2015b Delivering high quality,effective, compassionate care: Developing the right people with the right
skills and the right values : A mandate from the Government to Health Education England: April 2015 to
March 2016
DOH (2016) Prime Ministers speech on life chances – Part of the Education of disadvantaged children,
Support for families and Mental health service reform Department of Health
HEE (2016) Specialist Health Visitors in Perinatal & Infant Mental Health: What they do and why they
matter:https://www.hee.nhs.uk/sites/default/files/documents/Specialist%20Health%20Visitors%20in%20Per
inatal%20and%20Mental%20Health%20FINAL%20low%20res.pdf
JCPMH (2012) Guidance for Commissioners of Perinatal Mental Health Services: Volume 2 Practical
Mental Health Commissioning Joint Commissioning Panel for Mental Health
LSE and Centre for Mental Health (2014) The costs of perinatal mental health problems Centre for Mental
Health and London School of Economics, 2014 http://www.centreformentalhealth.org.uk/costs-of-perinatal-
mh-problems
MBRRACE - UK(2015) Saving Lives, Improving Mothers’ Care Surveillance of maternal deaths in the UK
2011-13 and lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into
Maternal Deaths and Morbidity 2009-13 Reports | MBRRACE-UK
https://www.npeu.ox.ac.uk/downloads/files/mbrrace-uk/reports/MBRRACE-
UK%20Maternal%20Report%202015.pdf
MHTF (2016) The Five Year Forward View for Mental Health: A report from the Independent Mental Health
Taskforce to the NHS in England The Mental Health Task Force
South East Clinical Network – Perinatal Mental Health
Page 44
Maternal Mental Health Everyone’s business e bulletin issue 4 Special edition 2015/2016
www.everyonesbusiness.org.uk
MMHA (2013): Specialist Mental Health Midwives: What they do and why they matter: http://www.baspcan.org.uk/files/MMHA%20SMHMs%20Report.pdf NHSE (2013) C06 NHS Standard Contract for Specialised Perinatal Mental Health Services (Inpatient Mother and Baby Units linked to Outreach Teams) NHS England NICE (2014) Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance National
Institute for Health and Care Excellence
NICE (2016) Antenatal and postnatal mental health NICE quality standard [QS115] National Institute for
Health and Care Excellence
NHS E (2014) Five Year Forward View NHS England
NHS E (2016) National Maternity Review: Better Births, Improving outcomes for maternity services in
England NHS England
NHSIQ (2015) Improving Access to Perinatal Mental Health Services in England - A review - NHS
Improving Quality www.nhsiq.nhs.uk/media/2696378/nhsiq_perinatal_mental_health
NMHDU (2011) NATIONAL PERINATAL MENTAL HEALTH PROJECT REPORT - Perinatal Mental Health
of Black and Minority Ethnic Women: A Review of Current Provision in England, Scotland and Wales
National Mental Health Development Unit
NSPCC. (2012) Prevention in mind : All Babies Count: Spotlight on Perinatal Mental Health – NSPCC
RCP (2015) Putting the pieces together. Removing the barriers to excellent patient care London Royal
College of Physicians
RCPsych (2011) Do the right thing. How to judge a good ward. Ten Standards for Adult inpatient mental healthcare Royal college of Psychiatrists London RCPsych (2015) CR 197 Perinatal Mental Health Service – Recommendations for the provision of services
for child bearing women – College Report The Royal College of Psychiatrists www.rcpsych.ac.uk
Wave Trust (2014) The 1001 Critical Days: The importance of the conception to Age 2 year period A Cross
Party Manifesto