perinatal outcomes in native chinese and chinese-american women
TRANSCRIPT

Perinatal outcomes in native Chinese andChinese-American womenppe_1185 202..209
Yinghui Liua, Jun Zhangc and Zhu Lib
aWomen’s and Children’s Health Center, Department of Obstetrics and Gynecology, the First Hospital of Peking University, bNational Center for
Maternal and Child Health, Peking University Health Science Center, Beijing, China, and cEunice Kennedy Shriver National Institute of Child
Health and Human Development, National Institutes of Health, Bethesda, MD, USA
Summary
Correspondence:Dr Jun Zhang, Division ofEpidemiology, Statistics andPrevention Research, EuniceKennedy Shriver NationalInstitute of Child Health andHuman Development,National Institutes of Health,Bethesda, MD 20892, USA.E-mail: [email protected]
Liu Y, Zhang J, Li Z. Perinatal outcomes in native Chinese and Chinese-Americanwomen. Paediatric and Perinatal Epidemiology 2011; 25: 202–209.
This study aimed to compare perinatal outcomes in native Chinese, foreign-born andUS-born Chinese-American women by analysing a cohort of 950 624 singleton preg-nancies in south-east China and 293 849 singleton births from the US live and stillbirthcertificates from 1995 to 2004. Only births at 28 weeks or later were included. Comparedwith US-born Chinese-American women, native Chinese and foreign-born Chinese-American women had substantially lower risks of having a small-for-gestational age(SGA) infant (adjusted relative risk [aRR] ranging from 0.46 to 0.66) or preterm birth(aRR ranging from 0.53 to 0.82). While having a White or Black father had a reducedrisk of SGA (aRR = 0.45 and 0.62, respectively), it has an increased risk for pretermbirth (aRR = 1.13 and 1.57, respectively). Infants with Chinese father and foreign-bornmother were heavier than those with Chinese father and US-born mothers. All findingswere statistically significant. Our findings demonstrated the protective role of foreign-born status on low birthweight and preterm delivery. The paternal contribution to fetalsize is substantial.
Keywords: pregnancy outcome, birthweight, preterm birth, stillbirth, migration.
Introduction
The China-born population in the US has increasedsubstantially in recent years. According to the 2000 USCensus, among the 31.1 million foreign-born popula-tion, China was the second largest source with 1.5million people, following Mexico with 9.2 millionpeople.1 From 2000 to 2007, the numbers of the China-born population in the US increased from 1.5 million to1.9 million, keeping China as the second largest originof immigrants in 2007.2
Numerous studies have demonstrated that foreign-born status is associated with perinatal outcome andthat the direction of this association varies across ethnicgroups. The improved pregnancy outcomes associatedwith foreign-born status have been demonstratedamong Mexican-Americans,3–7 Japanese-Americans,8
and African-Americans.9 For example, Singh et al.10
found that foreign-born status was associated with 7%
and 20% lower risks of low birthweight (LBW) andperinatal mortality, respectively, among 10 ethnicpopulations in the US when compared with theirUS-born counterparts. The incidence of LBW inMexican immigrants was found to be similar to non-Hispanic Whites but lower than that in many othercultural/ethnic groups, despite their social disadvan-tage and lack of prenatal care.3–5,7,10 However, notall studies found the same trend. Some studies inAsian-Indian-Americans showed that the infants offoreign-born women were lighter than their US-borncounterparts.11,12
Several studies have examined the effects of nativityon pregnancy outcomes among Chinese-Americanwomen and indicated the protective effects of foreign-born status on pregnancy outcomes.5,10,11,13,14 One studyfound that the foreign-born Chinese-Americanwomen had lower LBW rate than their US-born coun-terparts (3.9% vs. 5.4%).11 Another study reported a
202 doi: 10.1111/j.1365-3016.2010.01185.x
Paediatric and Perinatal Epidemiology, 25, 202–209. © 2011 Blackwell Publishing Ltd.

significantly lower infant mortality rate among infantsborn to China-born mothers residing in the US thanthat of their US-born counterparts (5.8 vs. 7.0 per thou-sand livebirths).10
However, studies that compared Chinese-Americanwith native Chinese women in perinatal outcomes arevery limited.13,15 One study compared the birthweightand LBW rate among US-born, China mainland-bornand Taiwan-born Chinese full-term infants, andreported a lower LBW rate among US-born infantsthan that among China mainland-born ones (LBW:1.9% vs. 2.3% for boys and 2.6% vs. 3.4% for girls).15
These studies were hospital-based, limiting their rep-resentativeness and generalisability. We used a largepopulation-based database to compare the differencein perinatal outcomes between native Chinese, foreign-born and US-born Chinese-American women.
Methods
The present analysis included singleton births born toChinese-American mothers who were born in (US-born) or outside (foreign-born) the US, and nativeChinese mothers in south-east China from 1995 to2004. Those foreign-born women included Chinesewomen who were born in China or elsewhere. We useddata from the 1995–2004 US Livebirth and Fetal Deathcertificates compiled by the National Center for HealthStatistics.16 Because maternal birthplace is not reportedin the nativity data after 2004, we were limited to usingdata prior to that year. Furthermore, since maternalbirthplace has never been reported on the fetal deathcertificate, we combined foreign-born and US-bornChinese-American women together when calculatingthe rate of stillbirth.
Data on native Chinese women were from thePerinatal Health Care Surveillance System (PHCSS),which was established by the National Center of Mater-nal and Infant Health (NCMIH) at Peking UniversityHealth Science Center as part of the evaluation of acommunity-based folic acid intervention programmeto prevent neural tube defects in China in 1993. Boththe folic acid intervention programme and the PHCSShave been described previously.17,18 The PHCSS covers27 cities and counties (6 in north China, 21 in south-east China) with a population of approximately 20million. Women were registered in the PHCSS whenthey came to local maternal and child health (MCH)facilities to obtain premarital examination, at the firstprenatal care visit or sought perinatal care services. The
registered women were followed up until the 42nd dayafter delivery. At registry and during the ensuing visit,local MCH staff collected information on maternaldemographic characteristics, reproductive history,health conditions, the conditions of the current preg-nancy, details of labour and the postpartum period.Staff at NCMIH were responsible for data cleaning,editing and correction. The process of data collectionand management has been described in detail else-where.18,19 No specific audit was conducted for PHCSSvalidation. But to ensure data quality for key variablessuch as stillbirth, birthweight and gestational age,several quality assurance and quality control measureswere used. They included using database software toperform logic and range checking, uniform training forthe staffs who were responsible for data collection,transfer and entry, monthly and annual report for thekey outcomes (e.g. stillbirth), regular check of theentered data, and assessment of newborn mortality.
Included were those women who delivered single-ton births in the 21 counties/cities in south-east China.Data from north China were excluded because com-plete population-based data were not available from2000 to 2004. Because the definition of a livebirth inChina is �28 weeks, we restricted our analysis to live-births or stillbirths �28 weeks for both Chinese and USdata. With the exclusion of 16 511 native Chinesewomen and 13 755 Chinese-American women, thefinal database contains a total of 1 222 437 women whogave singleton births with gestation 28 weeks or later.Based on maternal birth place, Chinese-Americanwomen were divided into three groups: foreign-born(n = 255 714), US-born (n = 27 231) and unknown(n = 1694). Because there were large differencesbetween the native rural and urban Chinese popula-tion, we separated native Chinese women into rural(n = 759 024) and urban (n = 176 914) groups.
Pregnancy outcomes included birthweight, LBW(<2500 g), gestational age at birth, preterm birth (<37weeks), small-for-gestational age (SGA) and stillbirth.Birthweight of infants was recorded in the medicalrecords or perinatal booklets within 1 h after birth. Forboth US and China births, gestational age at birth wascalculated based on the last menstrual period (LMP).The SGA was defined as birthweight at less than the10th percentile at a given gestational week according toa Chinese standard.20
Maternal characteristics included parity (primiparaand multipara), age (<22, 22–25, 26–29, 30–34, 35–54years), education (primary school or less, middle
Perinatal outcomes in Chinese women 203
Paediatric and Perinatal Epidemiology, 25, 202–209. © 2011 Blackwell Publishing Ltd.
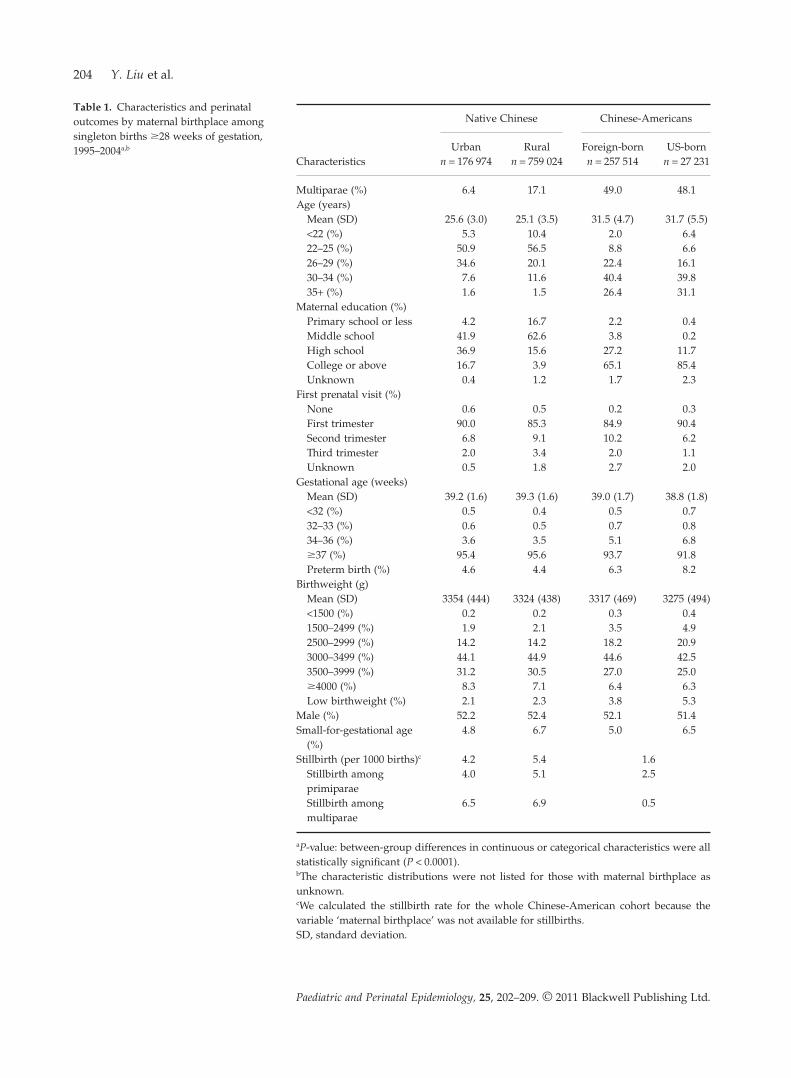
Table 1. Characteristics and perinataloutcomes by maternal birthplace amongsingleton births �28 weeks of gestation,1995–2004a,b
Characteristics
Native Chinese Chinese-Americans
Urban Rural Foreign-born US-bornn = 176 974 n = 759 024 n = 257 514 n = 27 231
Multiparae (%) 6.4 17.1 49.0 48.1Age (years)
Mean (SD) 25.6 (3.0) 25.1 (3.5) 31.5 (4.7) 31.7 (5.5)<22 (%) 5.3 10.4 2.0 6.422–25 (%) 50.9 56.5 8.8 6.626–29 (%) 34.6 20.1 22.4 16.130–34 (%) 7.6 11.6 40.4 39.835+ (%) 1.6 1.5 26.4 31.1
Maternal education (%)Primary school or less 4.2 16.7 2.2 0.4Middle school 41.9 62.6 3.8 0.2High school 36.9 15.6 27.2 11.7College or above 16.7 3.9 65.1 85.4Unknown 0.4 1.2 1.7 2.3
First prenatal visit (%)None 0.6 0.5 0.2 0.3First trimester 90.0 85.3 84.9 90.4Second trimester 6.8 9.1 10.2 6.2Third trimester 2.0 3.4 2.0 1.1Unknown 0.5 1.8 2.7 2.0
Gestational age (weeks)Mean (SD) 39.2 (1.6) 39.3 (1.6) 39.0 (1.7) 38.8 (1.8)<32 (%) 0.5 0.4 0.5 0.732–33 (%) 0.6 0.5 0.7 0.834–36 (%) 3.6 3.5 5.1 6.8�37 (%) 95.4 95.6 93.7 91.8Preterm birth (%) 4.6 4.4 6.3 8.2
Birthweight (g)Mean (SD) 3354 (444) 3324 (438) 3317 (469) 3275 (494)<1500 (%) 0.2 0.2 0.3 0.41500–2499 (%) 1.9 2.1 3.5 4.92500–2999 (%) 14.2 14.2 18.2 20.93000–3499 (%) 44.1 44.9 44.6 42.53500–3999 (%) 31.2 30.5 27.0 25.0�4000 (%) 8.3 7.1 6.4 6.3Low birthweight (%) 2.1 2.3 3.8 5.3
Male (%) 52.2 52.4 52.1 51.4Small-for-gestational age
(%)4.8 6.7 5.0 6.5
Stillbirth (per 1000 births)c 4.2 5.4 1.6Stillbirth amongprimiparae
4.0 5.1 2.5
Stillbirth amongmultiparae
6.5 6.9 0.5
aP-value: between-group differences in continuous or categorical characteristics were allstatistically significant (P < 0.0001).bThe characteristic distributions were not listed for those with maternal birthplace asunknown.cWe calculated the stillbirth rate for the whole Chinese-American cohort because thevariable ‘maternal birthplace’ was not available for stillbirths.SD, standard deviation.
204 Y. Liu et al.
Paediatric and Perinatal Epidemiology, 25, 202–209. © 2011 Blackwell Publishing Ltd.

school, high school, college or above, unknown), tri-mester to initiate the first prenatal visit (no prenatalcare, 1st, 2nd, 3rd trimester, unknown) and infant sex(male, female). To assess the effects of paternal race onbirthweight, infants were divided into seven groupsbased on paternal race/ethnicity and location: urbannative Chinese, rural native Chinese, Chinese-American, White, Black, other and unknown. The‘other’ group included Japanese, Korean, Vietnamese,American-Indian (including Aleuts and Eskimos),Hawaiian, Filipino, Asian-Indian, Samoan, Guama-nian, other Asian or Pacific Islander. The Chinese-American group was further divided into US- andforeign-born groups based on maternal birth place.
Statistical analysis
All data analyses were performed using SAS 9.1. Chi-square tests and analysis of variance were used to testbetween-group differences in categorical and continu-ous variables, respectively. We used log binomialmodels to examine whether paternal race and maternalnativity affect the risks of SGA and preterm delivery(PTD) after adjusting for maternal age, education, pre-natal visit and parity. To further quantify the paternalcontribution to fetal size, we restricted the study popu-lation to births at 39 and 40 weeks of gestation becausedeliveries at 39 and 40 weeks are more likely to benormal pregnancies. We used a multiple linear regres-sion model to adjust for other factors.
Results
Table 1 shows both demographic and perinatal charac-teristics by maternal birthplace. About half of theChinese-American women were multiparous whileonly 6.4% and 17.1% were multiparous among nativeurban and rural Chinese, respectively. The US-borngroup had the highest proportion of women aged 35years or more. The proportion of mothers havingcollege education or above was significantly higheramong Chinese-American groups than their nativeChinese counterparts. Most women had their initialprenatal visit during the first trimester, regardless oftheir birthplace. The boy-to-girl ratio was 1.09 for theurban Chinese group, 1.10 for the rural Chinese group,1.08 for the foreign-born group and 1.05 for theUS-born group, respectively.
Table 1 also presents pregnancy outcomes by mater-nal birthplace. Both LBW rate and PTD rate amongforeign-born groups were significantly lower thanUS-born groups, but higher than those among bothnative urban and rural Chinese groups. Infants born toUS-born Chinese mothers were the lightest among allgroups. The difference in PTD rate can be attributedmainly to the higher late preterm birth rate (34–36weeks) in the US population. The stillbirth rate amongall Chinese-Americans was significantly lower (1.6 per1000 livebirths) than those among rural (5.4 per 1000livebirths) and urban (4.2 per 1000 livebirths) nativeChinese groups. The same trend remained when sepa-rating by parity. The stillbirth rate was much lower
Table 2. Adjusted relative risks of small-for-gestational age and preterm birth according to father’s race and mother’s birthplace
Father’s race Mother’s birthplace
Small-for-gestational age Preterm birth
Prevalence (%) RR [95% CI]a Prevalence (%) RR [95% CI]a
Chinese-American US-born Chinese-American 7.8 1.00 Reference 6.9 1.00 ReferenceChinese-American Foreign-born Chinese-American 4.8 0.60 [0.56, 0.64] 4.6 0.60 [0.55, 0.65]Urban native Chinese Urban native Chinese 6.7 0.46 [0.42, 0.49] 4.4 0.53 [0.49, 0.58]Rural native Chinese Rural native Chinese 5.1 0.66 [0.61, 0.71] 6.0 0.82 [0.76, 0.89]White Chinese-American 3.7 0.45 [0.41, 0.49] 7.9 1.13 [1.03, 1.23]Black Chinese-American 5.8 0.62 [0.51, 0.76] 11.3 1.57 [1.32, 1.87]Other racesb Chinese-American 6.8 0.78 [0.72, 0.86] 7.6 1.07 [0.97, 1.18]Unknown race Chinese-American 6.3 0.58 [0.52, 0.64] 8.8 1.09 [0.98, 1.21]
aLog binomial model adjusting for maternal age, maternal education, parity and initial prenatal visit.bOther races include: Japanese, Korean, Vietnamese, American-Indian (including Aleuts and Eskimos), Hawaiian, Filipino, Asian-Indian,Samoan, Guamanian and other Asian or Pacific Islander.CI, confidence interval; RR, relative risk.
Perinatal outcomes in Chinese women 205
Paediatric and Perinatal Epidemiology, 25, 202–209. © 2011 Blackwell Publishing Ltd.
among multiparous group than in primiparousChinese-Americans, while the opposite was shown innative Chinese.
Table 2 shows that infants with a Chinese-Americanfather and US-born Chinese-American mother had thehighest risk of being SGA. Babies from native Chineseparents or White father and Chinese-American motherhad the lowest risk of SGA. The most instructivecase of ‘foreign-born’ advantage is presented by infantsfrom a Chinese-American father and a foreign-bornChinese-American mother. Compared with infantswith Chinese-American father and US-born Chinese-American mother, the former had a 40% reduction inrisk of being SGA. Such an advantage is particularlyobvious for preterm birth. Native Chinese women orforeign-born mothers all had a significantly reducedrisk of preterm birth, compared with US-born mothers.White and Black fathers were associated with anincreased risk of preterm birth, compared withChinese-American fathers (adjusted relative risk[aRR] = 1.13, 95% confidence interval [CI] 1.03, 1.23 forWhite father; aRR = 1.57, 95% CI 1.32, 1.87 for Blackfather).
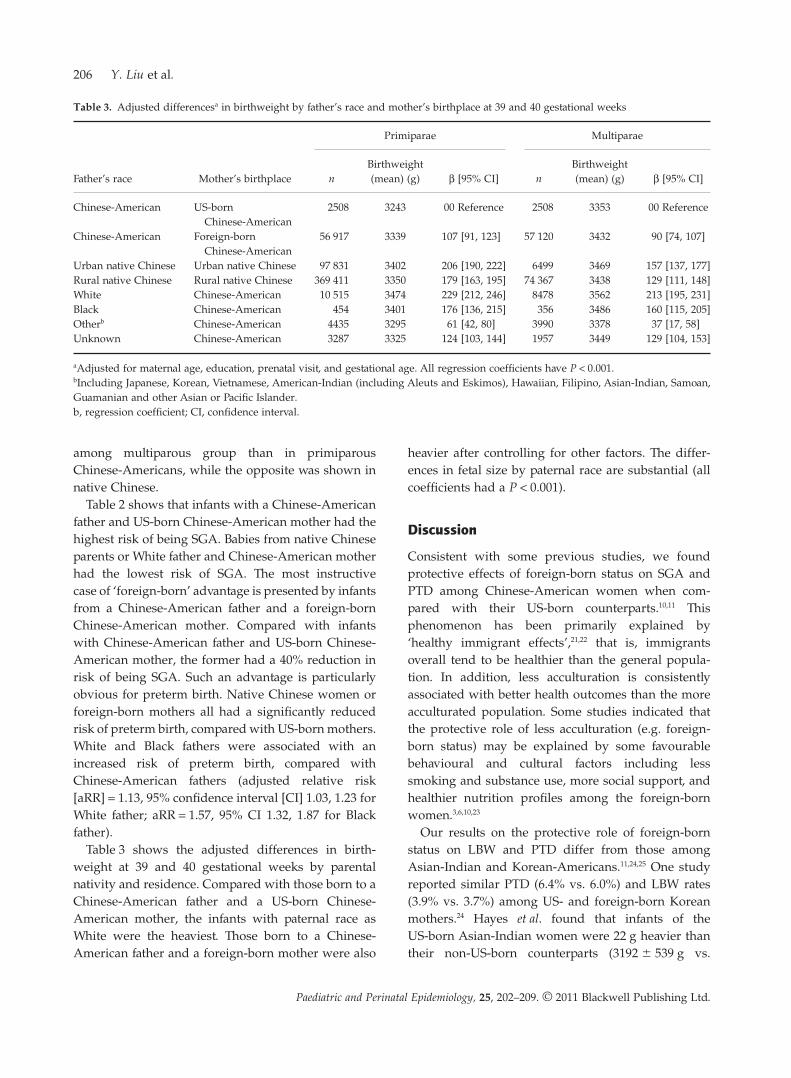
Table 3 shows the adjusted differences in birth-weight at 39 and 40 gestational weeks by parentalnativity and residence. Compared with those born to aChinese-American father and a US-born Chinese-American mother, the infants with paternal race asWhite were the heaviest. Those born to a Chinese-American father and a foreign-born mother were also
heavier after controlling for other factors. The differ-ences in fetal size by paternal race are substantial (allcoefficients had a P < 0.001).
Discussion
Consistent with some previous studies, we foundprotective effects of foreign-born status on SGA andPTD among Chinese-American women when com-pared with their US-born counterparts.10,11 Thisphenomenon has been primarily explained by‘healthy immigrant effects’,21,22 that is, immigrantsoverall tend to be healthier than the general popula-tion. In addition, less acculturation is consistentlyassociated with better health outcomes than the moreacculturated population. Some studies indicated thatthe protective role of less acculturation (e.g. foreign-born status) may be explained by some favourablebehavioural and cultural factors including lesssmoking and substance use, more social support, andhealthier nutrition profiles among the foreign-bornwomen.3,6,10,23
Our results on the protective role of foreign-bornstatus on LBW and PTD differ from those amongAsian-Indian and Korean-Americans.11,24,25 One studyreported similar PTD (6.4% vs. 6.0%) and LBW rates(3.9% vs. 3.7%) among US- and foreign-born Koreanmothers.24 Hayes et al. found that infants of theUS-born Asian-Indian women were 22 g heavier thantheir non-US-born counterparts (3192 � 539 g vs.
Table 3. Adjusted differencesa in birthweight by father’s race and mother’s birthplace at 39 and 40 gestational weeks
Father’s race Mother’s birthplace
Primiparae Multiparae
nBirthweight(mean) (g) b [95% CI] n
Birthweight(mean) (g) b [95% CI]
Chinese-American US-bornChinese-American
2508 3243 00 Reference 2508 3353 00 Reference
Chinese-American Foreign-bornChinese-American
56 917 3339 107 [91, 123] 57 120 3432 90 [74, 107]
Urban native Chinese Urban native Chinese 97 831 3402 206 [190, 222] 6499 3469 157 [137, 177]Rural native Chinese Rural native Chinese 369 411 3350 179 [163, 195] 74 367 3438 129 [111, 148]White Chinese-American 10 515 3474 229 [212, 246] 8478 3562 213 [195, 231]Black Chinese-American 454 3401 176 [136, 215] 356 3486 160 [115, 205]Otherb Chinese-American 4435 3295 61 [42, 80] 3990 3378 37 [17, 58]Unknown Chinese-American 3287 3325 124 [103, 144] 1957 3449 129 [104, 153]
aAdjusted for maternal age, education, prenatal visit, and gestational age. All regression coefficients have P < 0.001.bIncluding Japanese, Korean, Vietnamese, American-Indian (including Aleuts and Eskimos), Hawaiian, Filipino, Asian-Indian, Samoan,Guamanian and other Asian or Pacific Islander.b, regression coefficient; CI, confidence interval.
206 Y. Liu et al.
Paediatric and Perinatal Epidemiology, 25, 202–209. © 2011 Blackwell Publishing Ltd.

3170 � 151 g, P < 0.05).11 The inconsistency suggeststhat there might be heterogeneous pathways in theinfluence of maternal nativity on LBW and PTD amongthe Asian-American women.
The substantially lower rate of preterm birth innative Chinese women than in the Chinese-Americanwomen may be explained by two factors. First, becauseof the one-child family policy, native Chinese womentend to pay more attention to the occurrence of men-struation and remember their LMP better than otherrace/ethnic groups. Studies have demonstrated thatmore accurate LMP or using early ultrasound dating toestimate gestational age reduces the rate of pretermbirth.26 Since we used LMP-based gestational age inboth Chinese and US data, the difference in pretermbirth rate may therefore be in part attributable to moreaccurate LMP in native Chinese women. Second, therate of late preterm birth (34–36 weeks of gestation) hasbeen steadily increasing in the US in the past decade .27
This has not happened in China. Indeed, the differencein the rate of late preterm birth was the largest con-tributor to the overall difference in the rate of pretermbirth (Table 1).
The stillbirth rate among native Chinese multiparouswomen was higher than that among primiparouswomen both in urban and rural areas (6.5 vs. 4.0 per1000 livebirths in urban areas, 6.9 vs. 5.1 per 1000 live-births in rural areas). This is consistent with previousstudies in native Chinese,28,29 but contrary to observa-tions in industrialised countries. This discrepancybetween China and the US may be explained by theone-child family planning policy in China. Accordingto the policy, only those who have had a previousstillbirth, infant death, or serious birth defects are per-mitted to have a second child. Those women with ahistory of stillbirth or serious birth defects are likely tohave a higher risk of delivering a stillbirth. Anotherpossible explanation is that when compared withprimiparae, the multiparae had a more disadvantagedsocial status. We found that they had less educationand fewer prenatal visits than the primiparae (resultsnot shown). Further research is warranted to elucidatethis phenomenon.
Our study also found that there were significantdifferences in birthweight of infants born to differentinter-racial groups, suggesting an effect of paternalrace on birthweight. For example, the infants with aWhite father were the heaviest; those with a Chinesefather and a foreign-born Chinese mother wereheavier than those with a Chinese father and a
US-born mother. This is consistent with previousstudies.30–33 One US study reported that Asian Whitecouples had larger babies than both Asian parents(3360 g and 3210 g, respectively, P < 0.001).32 Somestudies suggested that approximately 7% and 15% ofthe variability in fetal growth could be explained bythe father’s and mother’s characteristics, respec-tively.34 One study in France reported that the risk ofhaving a SGA offspring was 4.7 times greater formothers and 3.5 times greater for fathers who wereSGA at birth, when compared with their average forgestational age counterparts.35 Neonatal weight andheight have also been reported to be correlated sig-nificantly with paternal height and weight (P = 0.01).36
Genetic effects of paternal race on fetal growth haveyet to be fully elucidated.
Both the Chinese and US data were population-based registries. The PHCSS covers >95% of thewomen in the surveillance area. Some validationstudies have indicated that information in populationregistry data (parity, maternal age, race, education andbirthweight) tend to be more reliable.37,38 But ourstudy still has several limitations. First, the nativeChinese cohort was collected in 21 cities/counties insouth-east China, which may limit its generalisabilityand representativeness. On the other hand, theChinese-American cohort was from the US nationaldata. One could argue that Chinese-Americans arestill a diverse group. Earlier Chinese immigrants tothe US were probably more likely to come fromsouthern China while newer Chinese immigrantstend to be from broad areas in mainland China. Theforeign-born and US-born Chinese-Americans mightnot be totally compatible. Second, US-born Chinese-Americans have benefitted from better nutrition,environment and health care for one or more genera-tions, which should contribute to better fetal growth.Meanwhile, birthweight is affected by many factors,some of which counterbalance with each other. Thus,the differences observed in our study may reflectboth genetic and environmental effects. Finally, south-east China is economically more developed than therest of the country. Thus, perinatal outcomes reportedin this study may not be representative of the wholecountry.
In conclusion, our study has demonstrated thatthe protective effects of foreign-born status on bothSGA and PTD delivery exist in Chinese women,and that the paternal contribution to fetal size issubstantial.
Perinatal outcomes in Chinese women 207
Paediatric and Perinatal Epidemiology, 25, 202–209. © 2011 Blackwell Publishing Ltd.
Acknowledgement
J Zhang is supported by the Intramural Program ofEunice Kennedy Shriver National Institute of ChildHealth and Human Development, National Institutesof Health.
References
1 Schmidley AD. Profile of the Foreign-Born Population in theUnited States: 2000. US Census Bureau, Current PopulationReports, Series P23-206; 2001.
2 Elizabeth MG. Race and Hispanic Origin of theForeign-Born Population in the United States: 2007. USCensus Bureau, American Community Survey Reports,ACS-11; 2010:1–16.
3 Page RL. Positive pregnancy outcomes in Mexicanimmigrants: what can we learn? Journal of Obstetric,Gynecologic, and Neonatal Nursing 2004; 33:783–790.
4 Callister LC, Birkhead A. Acculturation and perinataloutcomes in Mexican immigrant childbearing women: anintegrative review. Journal of Perinatal and Neonatal Nursing2002; 16:22–38.
5 Cervantes A, Keith L, Wyshak G. Adverse birth outcomesamong native-born and immigrant women: replicatingnational evidence regarding Mexicans at the local level.Maternal and Child Health Journal 1999; 3:99–109.
6 Jones ME, Bond ML. Predictors of birth outcome amongHispanic immigrant women. Journal of Nursing Care Quality1999; 14:56–62.
7 Zambrana RE, Scrimshaw SC, Collins N, Dunkel-Schetter C.Prenatal health behaviors and psychosocial risk factors inpregnant women of Mexican origin: the role ofacculturation. American Journal of Public Health 1997;87:1022–1026.
8 Alexander GR, Mor JM, Kogan MD, Leland NL, Kieffer E.Pregnancy outcomes of US-born and foreign-born JapaneseAmericans. American Journal of Public Health 1996;86:820–824.
9 David RJ, Collins JW Jr. Differing birth weight amonginfants of US-born blacks, African-born blacks, and US-bornwhites. New England Journal of Medicine 1997; 337:1209–1214.
10 Singh GK, Yu SM. Adverse pregnancy outcomes:differences between US- and foreign-born women in majorUS racial and ethnic groups. American Journal of PublicHealth 1996; 86:837–843.
11 Hayes DK, Lukacs SL, Schoendorf KC. Heterogeneitywithin Asian subgroups: a comparison of birthweightbetween infants of US and non-US born Asian Indian andChinese mothers. Maternal and Child Health Journal 2008;12:549–556.
12 Madan A, Palaniappan L, Urizar G, Wang Y, Fortmann SP,Gould JB. Sociocultural factors that affect pregnancyoutcomes in two dissimilar immigrant groups in the UnitedStates. Journal of Pediatrics 2006; 148:341–346.
13 Wen SW, Kramer MS, Usher RH. Comparison of birthweight distributions between Chinese and Caucasianinfants. American Journal of Epidemiology 1995; 141:1177–1187.
14 Li Q, Keith LG, Kirby RS. Perinatal outcomes amongforeign-born and US-Born Chinese Americans, 1995–2000.Journal of Immigrant and Minority Health 2008; 12:282–289.
15 Yip R, Li Z, Chong WH. Race and birth weight: the Chineseexample. Pediatrics 1991; 87:688–693.
16 Martin JA, Hamilton BE, Sutton PD, Ventura SJ, MenackerF, Kirmeyer S. Births: final data for 2004. National VitalStatistics Reports 2006; 55:1–101.
17 Berry RJ, Li Z, Erickson JD, Li S, Moore CA, Wang H, et al.Prevention of neural-tube defects with folic acid in China.China-US Collaborative Project for Neural Tube DefectPrevention. New England Journal of Medicine 1999;341:1485–1490.
18 Zhang J, Liu Y, Meikle S, Zheng J, Sun W, Li Z. Cesareandelivery on maternal request in southeast China. Obstetricsand Gynecology 2008; 111:1077–1082.
19 Liu Y, Liu J, Ye R, Ren A, Li S, Li Z. Association ofeducation and the occurrence of low birthweight in ruralsouthern China during the early and late 1990s. AmerianJournal of Public Health 2008; 98:687–691.
20 The study group of urban neonatal growth in China.The growth and development study among the newbornsin 15 cities in China. Zhonghua Er Ke Za Zhi 1988;26:206–209.
21 Flores G, Brotanek J. The healthy immigrant effect: a greaterunderstanding might help us improve the health of allchildren. Archives of Pediatrics and Adolescent Medicine 2005;159:295–297.
22 Ray JG, Vermeulen MJ, Schull MJ, Singh G, Shah R,Redelmeier DA. Results of the recent immigrant pregnancyand perinatal long-term evaluation study (RIPPLES).Canadian Medical Association Journal 2007; 176:1419–1426.
23 Dixon LB, Sundquist J, Winkleby M. Differences in energy,nutrient, and food intakes in a US sample ofMexican-American women and men: findings from theThird National Health and Nutrition Examination Survey,1988–1994. American Journal of Epidemiology 2000;152:548–557.
24 Qin C, Gould JB. Maternal nativity status and birthoutcomes in Asian Immigrants. Journal of Immigrant andMinority Health 2010; 12:798–805.
25 Gould JB, Madan A, Qin C, Chavez G. Perinatal outcomesin two dissimilar immigrant populations in the UnitedStates: a dual epidemiologic paradox. Pediatrics 2003;111:e676–e682.
26 Dietz PM, England LJ, Callaghan WM, Pearl M, Wier ML,Kharrazi M. A comparison of LMP-based andultrasound-based estimates of gestational age using linkedCalifornia livebirth and prenatal screening records.Paediatric and Perinatal Epidemiology 2007; 21 (Suppl 2):62–71.
27 Martin JA, Kirmeyer S, Osterman M, Shepherd RA. Born abit too early: recent trends in late preterm births. NationalCenter for Health Statistics Data Brief 2009; 24:1–8.
28 Wu Z, Viisainen K, Wang Y, Hemminki E. Perinatalmortality in rural China: retrospective cohort study. BritishMedical Journal 2003; 327:1319.
29 Zhang Q, Ananth CV, Rhoads GG, Li Z. The impact ofmaternal anemia on perinatal mortality: a population-based,
208 Y. Liu et al.
Paediatric and Perinatal Epidemiology, 25, 202–209. © 2011 Blackwell Publishing Ltd.

prospective cohort study in China. Annals of Epidemiology2009; 19:793–799.
30 Patel D, Patel U, Piotrowski ZH, Nelson M. Maternal andpaternal risk factors and birth outcomes among Asian andPacific Islanders in Illinois. Asian American and PacificIslander Journal of Health 1995; 3:42–51.
31 Parker JD, Schoendorf KC. Influence of paternalcharacteristics on the risk of low birth weight. AmericanJournal of Epidemiology 1992; 136:399–407.
32 Nystrom MJ, Caughey AB, Lyell DJ, Druzin ML, El-SayedYY. Perinatal outcomes among Asian-white interracialcouples. American Journal of Obstetrics and Gynecology 2008;199:385.e1–385.e5.
33 Ma S. Paternal race/ethnicity and birth outcomes. AmericanJournal of Public Health 2008; 98:2285–2292.
34 Hennessy E, Alberman E. Intergenerational influencesaffecting birth outcome. I. Birthweight for gestational
age in the children of the 1958 British birth cohort.Paediatric and Perinatal Epidemiology 1998;12 (Suppl 1):45–60.
35 Jaquet D, Swaminathan S, Alexander GR, Czernichow P,Collin D, Salihu HM, et al. Significant paternal contributionto the risk of small for gestational age. British Journal ofObstetrics and Gynaecology 2005; 112:153–159.
36 Miletic T, Stoini E, Mikulandra F, Tadin I, Roje D, Milic N.Effect of parental anthropometric parameters on neonatalbirth weight and birth length. Collegium Antropologicum2007; 31:993–997.
37 Reichman NE, Hade EM. Validation of birth certificate data.A study of women in New Jersey’s HealthStart program.Annals of Epidemiology 2001; 11:186–193.
38 Roohan PJ, Josberger RE, Acar J, Dabir P, Feder HM,Gagliano PJ. Validation of birth certificate data in New YorkState. Journal of Community Health 2003; 28:335–346.
Perinatal outcomes in Chinese women 209
Paediatric and Perinatal Epidemiology, 25, 202–209. © 2011 Blackwell Publishing Ltd.