perinatal services in medi-cal managed care: strategies to better serve our members 11/5/14...
TRANSCRIPT

Perinatal services in Medi-Cal Managed Care: strategies to better serve our members
11/5/14 Perinatal Services Coordinator Annual Meeting
Maternal, Child and Adolescent Health (MCAH) Branch
California Department of Public Health
Sarah Royce, MD, MPH, Chief, Medical Policy Section
Medi-Cal Managed Care Division, DHCS

2
– Medi-Cal Managed Care Plans• Models• Requirements for obstetric care
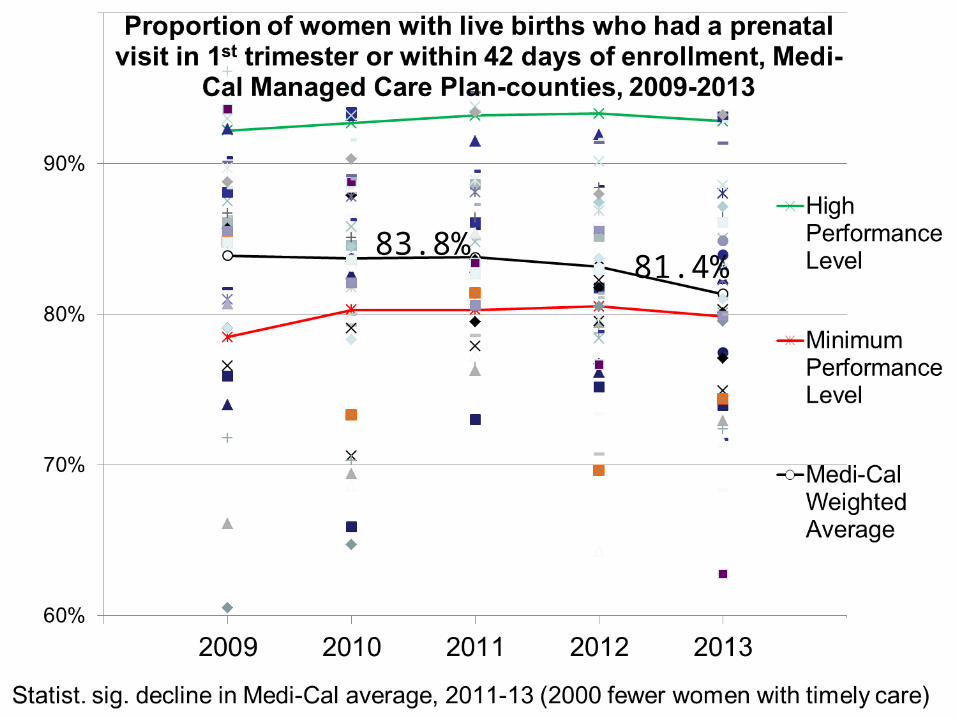
– How are Plans doing in assuring women have timely prenatal and postpartum care?
– What we need to do to close the performance gaps?
• Medi-Cal Managed Care Quality Strategy, 2014-5
Overview

3
• Commercial + local initiative 12 Plans in 14 counties
• Two commercial Plans– 3 Plans in 19 counties
• County organized health system (COHS)– Single Plan in each county– 6 Plans in 22 counties
• Geographic managed care– 6 commercial plans in
Sacramento and San Diego
• San Benito– Single commercial plan (only
county where enrollment optional)
Medi-Cal managed care models
http://www.dhcs.ca.gov/individuals/Pages/MMCDHealthPlanDir.aspx
Hatch marks show2013 expansion

4
• cover and ensure provision of all medically necessary services for pregnant women
• ensure that ACOG guidelines are used• implement a risk assessment tool that is
– comparable to ACOG, CPSP standards, including: medical, OB, nutritional, psychosocial, health education
– administered at initial prenatal visit, once each trimester, and at postpartum visit
• Develop individualized care plans• Follow up identified risks with
appropriate interventions
DHCS contracts require Plans to

5
• Apply provider credentialing standards to all prenatal care providers. Ensure they are – trained on standards of providing
comprehensive perinatal services per ACOG standards
– Demonstrate professional
competence• Execute an MOU (or subcontract)
for services provided by local
health department MCAH programs
DHCS contracts require Plans to:

6
• Plans review medical records of primary care providers (including obstetrics)– When OB joins network and every 3 years – Chart review tool– Results reported to DHCS every 6 months
• Two perinatal performance measures included in set that Plans report each year
– Validated by external quality review organization– DHCS contracts require Plans to perform at least as
well as the lowest 25% of Medicaid plans in the US (Minimum Performance Level, MPL)
Oversight of obstetric care

7
Prenatal and postpartum caremeasures• Healthy mother• Healthy birth, newborn
~82,000 women in Medi-Cal managed care denominator in 2013 because they:• had a live birth, and • enrolled continuously in same Plan from 43 days prior through 56 days after delivery
8
83.8%81.4%
9
Served in 2013
Left to do**
81% of women who gave birth had had timely prenatal care*
15,000 pregnant women without timely prenatal care
* no improvement compared to 2012** among 6 million members as of 12/2013
Our task at hand

10
Timely postpartum visit
• Preconception health• Family planning• Breastfeeding• Depression screening
• Follow-up of conditions Example: diabetes in 11.9% of women with live births in 2012*• Preconception diabetes in 3.9%• Gestational diabetes in 8%
*DHCS FPACT/UCSF analysis of encounter data in DHCS data warehouse (reported by Plans)

11
Statistically significant decline in Medi-Cal average, 2011-13 (4000 fewer women with timely postpartum care)
61.7%

12

13

14
• Disparities– Significantly lower proportion of Black mothers had timely
postpartum care than other race-ethnic groups– For ensuring timely postpartum visits among Black
mothers, the Plans with the best success had double the postpartum visit rates compared to the lowest performing Plans*
• For all women, Plans report it is difficult to:– Promptly identify women who recently gave birth, needed
for outreach efforts– Collect visit info from providers using global billing or
capitation*among Plan-counties with > 200 Black women who gave birth in 2012
Challenges in timely postpartum care
15
5% improvement in timely post partum care– Statewide Medi-Cal average– # Plan-counties > minimum performance level– Black women who gave birth
Re-visit statewide targets in light of:– Plan-specific commitments– Effort DHCS, Plans, partners
can mobilize– What is ambitious yet feasible
Preliminary targets: Medi-Cal Managed Care Quality Strategy, 2014-5

16
1. Speed up, intensify DHCS response – Rapid cycle quality improvement (QI)
2. QI Learning Collaborative
Postpartum subgroup – Understand, address causes of
low performance– Optimize provider education,
feedback, incentives– Optimize member engagement
3. Improve data quality and use
4. Enhance collaboration
DHCS interventions

17
Share resources, improve the community systems of care by:
• Providing Plans a cross walk of available MCAH programs so they can refer members
• Provide to Plans CDPH training opportunities and materials for managed care providers and mothers
• Promote partnerships between Plans and local MCH programs via MOUs or other mechanisms
Collaboration with CDPH/MCAH