perioperative geriatrics. guidelines, limits and beyond
TRANSCRIPT

Camilla Wong MD FRCPC MHScOctober 29, 2016

#GeriUpdate16





A comprehensive geriatric assessment (CGA) is a multidimensional, interdisciplinary diagnostic process to determine the medical, psychological, and functional capabilities of a frail elderly person in order to develop a coordinated and integrated plan for treatment and long-term follow-up


Cochrane Database of Systematic Reviews 2011MDTea

CGA}geriatric assessment}
CGA}geriatric assessment}


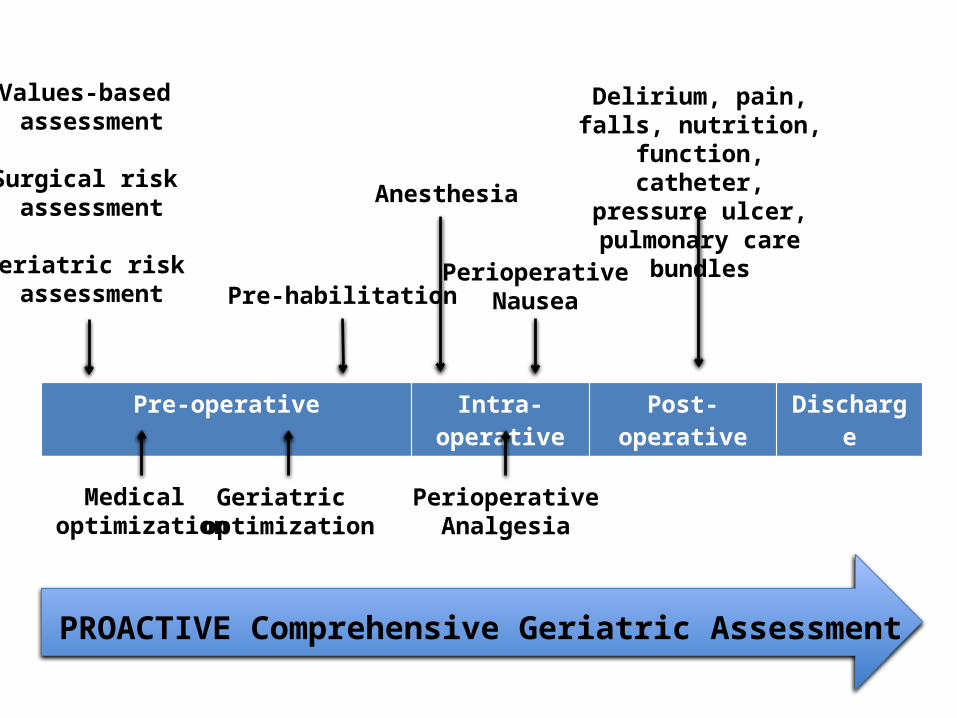
Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization
Pre-habilitation
Anesthesia
PerioperativeAnalgesia
PerioperativeNausea
Delirium, pain, falls, nutrition, function,
catheter, pressure ulcer, pulmonary care bundles
Care Transitions

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment

Determine goals and expectations.
Assess cognitive ability and capacity to understand anticipated surgery.
Screen for depression.
Identify and manage risk factors for delirium.
Screen for substance dependence.
Document functional status, mobility and falls.
Determine frailty.
Assess nutritional status and offer interventions.
Determine support system.
Order appropriate diagnostic tests.
Perform a preoperative cardiac evaluation.
Perform a preoperative pulmonary evaluation and implement optimization strategies.
Take a medication history and make any appropriate perioperative adjustments.
1
2
3
4
5
6
7
8
9
10
11
12
13J Am Coll Surg. 2012;215(4):453-66.
PRE-OP
a) “understand” the information that is relevant to making a decision about
the treatment, and b) “appreciate” the reasonably foreseeable consequences of a
decision or lack of decision.

PRE-OPERATIVE HARMONIZATION
1
VALUES BASED ASSESSMENT


JAMA. 2014;311(20):2110-2120.

PRE-OPERATIVE HARMONIZATION
1 2
VALUES BASED ASSESSMENT
SURGICAL RISK ASSESSMENT

http://riskcalculator.facs.org/RiskCalculator/

http://riskcalculator.facs.org/RiskCalculator/

http://riskcalculator.facs.org/RiskCalculator/

PRE-OPERATIVE HARMONIZATION
1 32
VALUES BASED ASSESSMENT
SURGICAL RISK ASSESSMENT
GERIATRIC RISK ASSESSMENT

Lancet. 2013;381(9868):752-62.

J Am Coll Surg. 2015 Dec;221(6):1083-92.

vs

P H E N OT Y P I C F R A I LT Y
J Gerontol A Biol Sci Med Sci 2001; 56:M146eM156.
ROBUST: 0-1
PRE-FRAIL: 2-3
FRAIL: 4-5
W E I G H T L O S Sunintentional > 10 pounds in prior year
W E A K N E S Sgrip strength in lower 20%
E X H A U S T I O Nself-report
S L O W N E S Sslowest 20% 15 feet walking time
L O W A C T I V I T Ylowest 20% kcals per week



Ann Surg 2013;258:582-588.

BMC Geriatrics (2016) 16:157

PRE-OPERATIVE HARMONIZATION
13
2VALUES BASED ASSESSMENT
SURGICAL RISK ASSESSMENT
GERIATRIC RISK ASSESSMENT

PRE-OPERATIVE HARMONIZATION
1 32
VALUES BASED ASSESSMENT
SURGICAL RISK ASSESSMENT
GERIATRIC RISK ASSESSMENT

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment


P R E O P E R A T I V E T E S T I N G
Preoperative diagnostic tests should be performed selectively. Normal laboratory values obtained up to 4 months before surgery can be used if no substantial interval chance in clinical status.
Routine sets of preoperative screening tests are NOT recommended.3 exceptions: hemoglobin, renal function, albumin.

P U L M O N A R Y
Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery. Ann Intern Med. 2006;144(8):575-80.
A N T I M I C R O B I A L
Clinical practice guidelines for antimicrobial prophylaxis in surgery. American Journal of Health-System Pharmacy 2013;70:195-283.
N U T R I T I O N
The European Society for Clinical Nutrition and Metabolism guidelines.http://www.espen.org/education/espen-guidelines
C A R D I O V A S C U L A R
2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. J Am Coll Cardiol. 2014;64(22):e77-e137.
T H R O M B O E M B O L I S M
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis. Chest 2012; 141(2S):e326S-e350S.
D I A B E T E S
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Can J Diabetes 2013;37(S1):S1-S212.

Cochrane Database Syst Rev. 2014;(3):CD002294.

Administer the CAGE Questionnaire.
If motivated, delay surgery for abstinence or detoxification.
If at risk, give perioperative prophylaxis for withdrawal syndromes.
In alcohol use disorder, give perioperative daily multivitamin and high-dose thiamine.
J Am Coll Surg. 2012;215(4):453-66.

J Am Coll Surg. 2016;222(5):930-47.
M E D I C AT I O N M A N A G E M E N T

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization

T E S T.
Perform an assessment such as the Mini-Cog.
If abnormal, then further evaluation.
D O C U M E N T.
Documentation of pre-operative cognitive
status helps to quantify postoperative cognitive dysfunction.
I N Q U I R E .
Ask informants about any cognitive decline.
J Am Coll Surg. 2012;215(4):453-66.
C O G N I T I V E I M P A R I M E N T

IDENTIFY POST-OP DELIRIUM RISKAge > 65, cognitive impairment, severe illness, hearing or vision impairment, presence of infection, inadequately controlled pain, depression, alcohol use, sleep deprivation or disturbance, renal insufficiency, anemia, hypoxia or hypercarbia, poor nutrition, dehydration, electrolyte abnormalities, poor functional status, limited mobility, use of psychotropic medications, risk of urinary retention of constipation, presence of urinary catheter, aortic procedures.
J Am Geriatr Soc. 2015;63(1):142-50.
Age Ageing. 2012;41(5):629-34.
NNT = 13

DELIRIUM PREVENTION
J Am Geriatr Soc. 2015;63(1):142-50.

IF SCREEN IS POSITIVE, THEN FURTHER EVALUATION IS RECOMMENDED.
In the past 12 months, have you ever had a time when you felt sad, blue, depressed, or down for most of the time for at least 2 weeks?
In the past 12 months, have you ever had a time, lasting at least 2 weeks, when you didn’t care about the things that you usually cared about or when you didn’t enjoy the things that you usually enjoyed?
J Am Coll Surg. 2012;215(4):453-66.

Management of ADLs and IADLS
History of falls
Vision, hearing, swallowing
Gait and balance assessment
P E R F O R M A N C E S TAT U SDEFICITS SHOULD PROMPT PROACTIVE DISCHARGE PLANNING
AND REFERRALS TO ALLIED HEALTH
J Am Coll Surg. 2012;215(4):453-66.

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization

increase functional capacity in anticipation of an upcoming stress

d e c r e a s e s p n e u m o n i aRR 0.45, 95% CI 0.24-0.83
d e c r e a s e s l e n g t h o f s t ay3.21 days, p=0.01
Cochrane Database of Systematic Reviews 2012 (11): CD010118.

Surg Endosc. 2013;27(4):1072-82.
PREHABIL ITAT IONA 1-month trimodal program improves post-op functional recovery.

Anesthesiology 2011;114:495-511.
Fasting from intake of clear liquids at least 2 hours before elective procedures requiring general anesthesia, regional anesthesia, or sedation/analgesia is recommended.
Fasting from intake of a light meal 6 hours of more before elective procedures requiring general anesthesia, regional anesthesia, or sedation/analgesia is recommended.
Anesthesiology 2011;114:495-511.

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization
Pre-habilitation

J Am Coll Surg. 2016;222(5):930-47.

J Am Geriatr Soc. 2015;63(1):142-50.

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization
Pre-habilitation
Anesthesia

J Am Coll Surg. 2016;222(5):930-47.

J Am Coll Surg. 2016;222(5):930-47.

J Am Coll Surg. 2016;222(5):930-47.

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization
Pre-habilitation
Anesthesia
PerioperativeAnalgesia

NauseaIn general, AVOID using:
corticosteroids scopolamine metoclopramide
promethazinedimenhydrinate
prochlorperazine
U S E 5 - H T 3 R E C E P T O R A N T A G O N I S T S
J Am Coll Surg. 2016;222(5):930-47.

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization
Pre-habilitation
Anesthesia
PerioperativeAnalgesia
PerioperativeNausea

Delirium prevention strategies
Multimodal, individualized acute pain control
Minimize pulmonary complications
Fall risk reduction
Maintain adequate nutrition
Urinary tract infection prevention
Prevent functional decline
Reduce pressure ulcers
1
2
3
4
5
6
7
J Am Coll Surg. 2012;215(4):453-66.
POST-OP
8
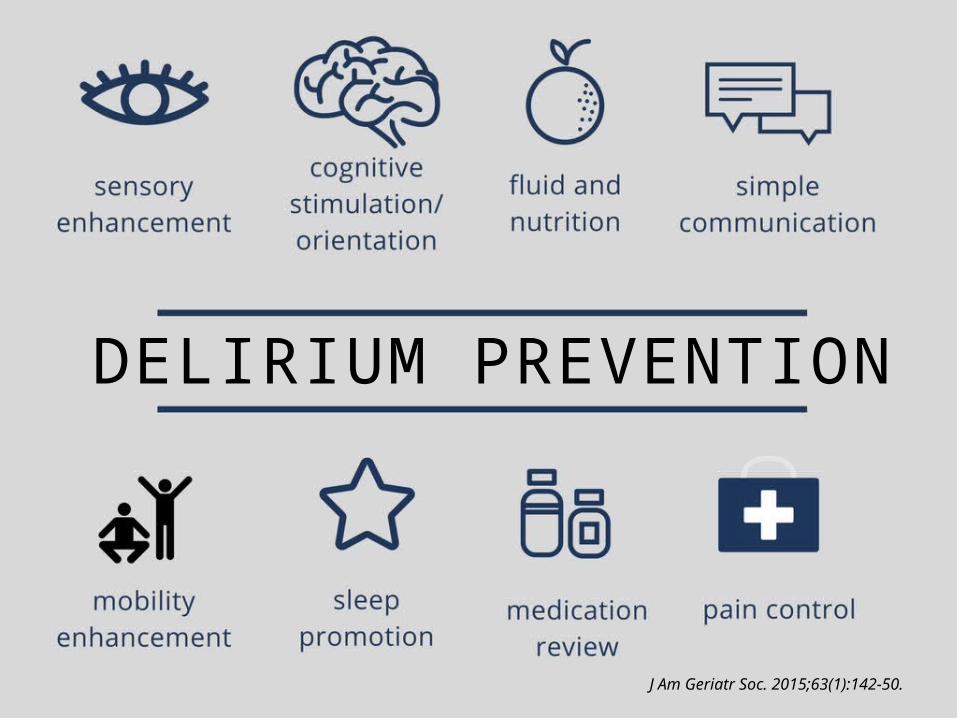
DELIRIUM PREVENTION
J Am Geriatr Soc. 2015;63(1):142-50.

orientation strategies vision and hearing aids sleep environment
family participation uncluttered hallways multimodal pain control
remove urinary catheters and other tethers
W H AT I S G O O D F O R D E L I R I U M ,
I S G O O D F O R FA L L S , I S G O O D
F O R F U N C T I O N A L D EC L I N E .
wound care: minimize pressure, friction,
humidity, shear force
avoid potentially inappropriate medications
resume diet early and provide dentures, if needed
chest physiotherapy and incentive spirometry
early, multidisciplinary involvement
nutritional supplement, if needed
early mobilization, using walking aids if needed scheduled toileting aspiration precautions
Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization
Pre-habilitation
Anesthesia
PerioperativeAnalgesia
PerioperativeNausea
Delirium, pain, falls, nutrition, function,
catheter, pressure ulcer, pulmonary care bundles

CO M M O N C O M P O N E N T S O F T R A N S I T I O N C A R E M O D E L S• Coordinated care with primary care physician• Engagement of patient, family, and/or caregiver• Patient-centered medical record • Post-discharge follow up plan• Medication management• Knowledge of important signs and symptoms
J Am Coll Surg. 2012;215(4):453-66.

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization
Pre-habilitation
Anesthesia
PerioperativeAnalgesia
PerioperativeNausea
Delirium, pain, falls, nutrition, function,
catheter, pressure ulcer, pulmonary care bundles
Care Transitions

Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization
Pre-habilitation
Anesthesia
PerioperativeAnalgesia
PerioperativeNausea
Delirium, pain, falls, nutrition, function,
catheter, pressure ulcer, pulmonary care bundles
Care Transitions
Palliative Care
Family Doctor
Geriatrics
Surgery
Internist
Pain Service
Anesthesia
PT
RDPharmacy
Nursing
SW
OTSLP


ENHANCEDRECOVERYPROGRAMS
“ T H E I M M E D I AT E C H A L L E N G E T O I M P R O V I N G T H E Q U A L I T Y O F S U R G I C A L C A R E I S N O T D I S C O V E R I N G N E W K N O W L E D G E , B U T R AT H E R H O W T O I N T E G R AT E W H AT W E A L R E A D Y K N O W I N T O P R A C T I C E .”
17 systematic reviews and 12 additional showed Enhanced Recovery After Surgery (ERAS) programs may reduce hospital stays by 0.5–3.5 days compared with conventional care.
BMJ. 2005; 330(7505): 1401–1402.BMJ Open 2014;4:e005015.

13%16%13%4.5 days
less delirium
less pneumonia
less catheters
less days in hospital
Age and Ageing 2007; 36:190–196



Pre-operative Intra-operative Post-operative Discharge
PROACTIVE Comprehensive Geriatric Assessment
Values-based assessment
Surgical risk assessment
Geriatric risk assessment
Medical optimization
Geriatric optimization
Pre-habilitation
Anesthesia
PerioperativeAnalgesia
PerioperativeNausea
Delirium, pain, falls, nutrition, function,
catheter, pressure ulcer, pulmonary care bundles
Care Transitions