perioperative heart transplant management and complications by dr. aliessa barnes, medical director...
TRANSCRIPT
Perioperative Heart Transplant Management and Complications
Aliessa Barnes MDDivision of CardiologyMedical Director of Heart Transplantation
Comprehensive EvaluationListingDonor selectionTransplantationPost operative careChronic management
Heart Transplant process
Outline
Risk AssessmentSurgical IssuesPost Operative ManagementComplications

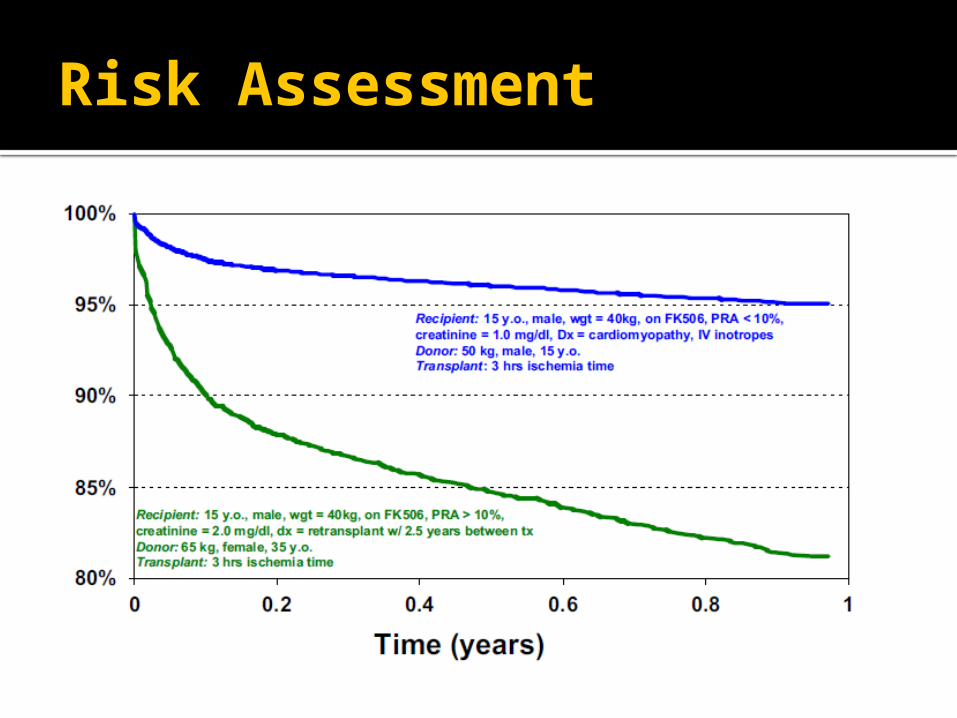
Risk Assessment
Primary Graft Failure (PGF) Severe dysfunction of the allograft
without any anatomic or immunologic cause▪ Need for multiple inotropes and/or
mechanical circulatory support in the first 24 hours
Varying rate based on definition▪ 1.4%-20% or more
Can be RV, LV or biventricular failure▪ RV most common

Risk Assessment- PGF
Most common cause of death (40%) in the first 30 days after transplant
18% of mortality in the first 12 months
30 day survival 1992-1997- 43% 1998-2004- 57%
Also decreases 1 year survival

Risk Assessment- PGF
Risk Factors Recipient
▪ High PVR▪ ECMO
Donor▪ Long Ischemic Times▪ Poor organ preservation▪ Reactive Oxygen Species

Risk Assessment
Other hypothesized factors▪ Female donors▪ Size mismatch▪ Marginal or Extended donors

Risk Assessment
Risk Assessment
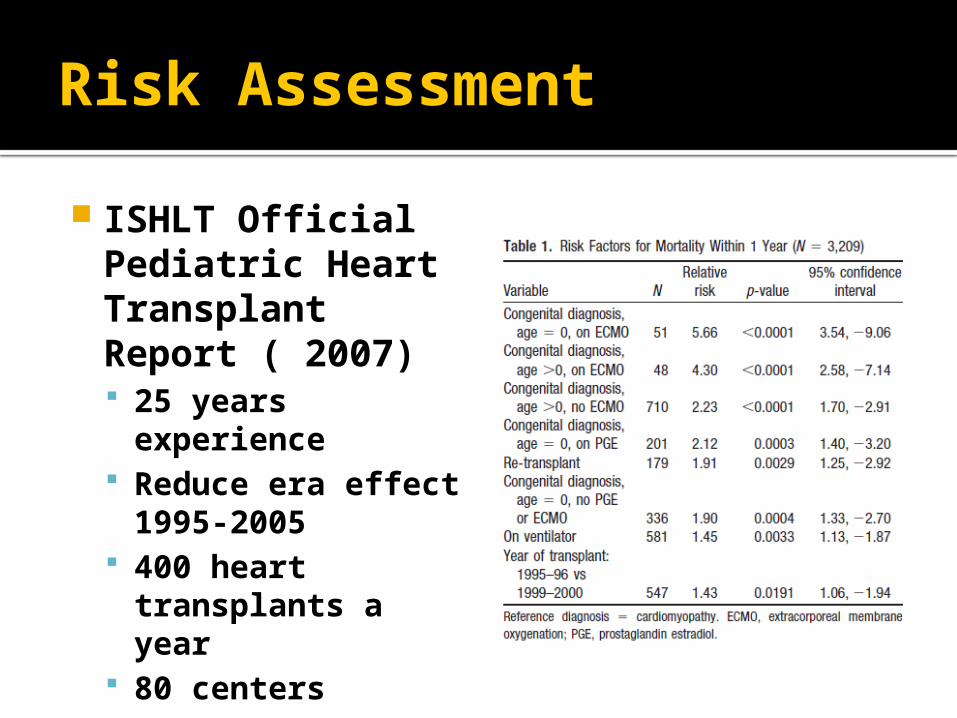
ISHLT Official Pediatric Heart Transplant Report ( 2007) 25 years
experience Reduce era effect
1995-2005 400 heart
transplants a year 80 centers

Risk Assessment
Risk Assessment

Risk Assessment
Risk Assessment
VAD versus ECMO Review since 2002 Toronto, Canada VAD available since 2004 36 patients (21 ECMO; 12 VAD) Waitlist mortality 38% on ECMO
decreased to 13% with VAD Survival post transplant to hospital
discharge better in VAD 92% versus ECMO 80%

Historical Surgical Appproach
1960 Lower and Shumway
Leaves large atrial cavities
Abnormal geometry lead to increased TR
Sinus node dysfunction from surgical trauma
Scar =AFib/Flutter
Bi-atrial anastomosis

Current Surgical Approach
Bi-caval anastomosis
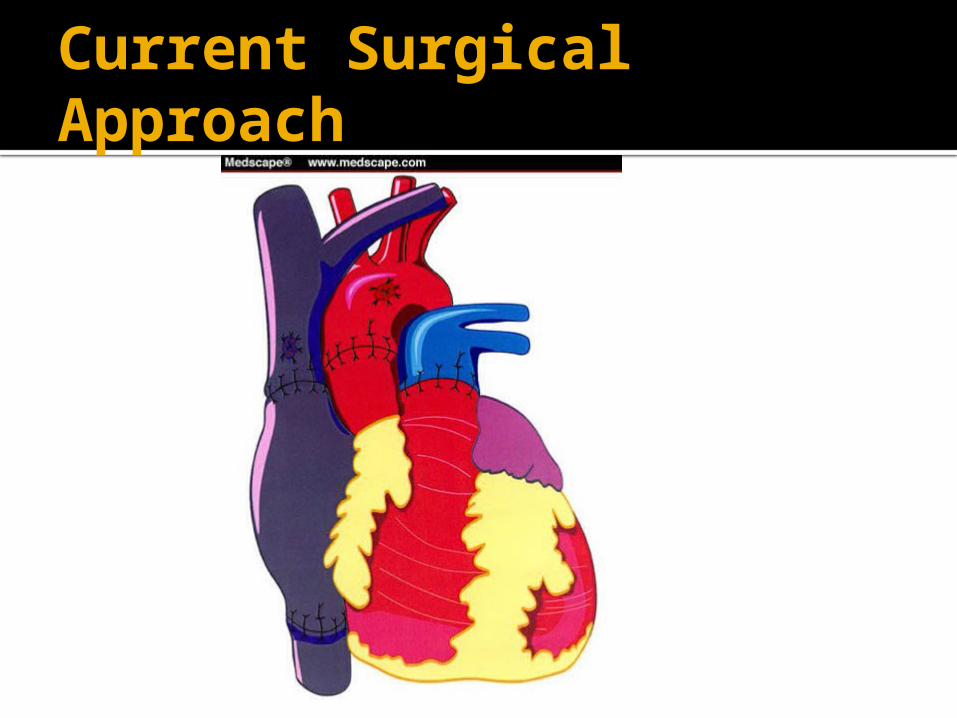
Current Surgical Approach

Surgical Adaptations
Tunnel of Left SVC to Right atrium
Reconstruction of Hepatic Veins entered left atrium

Surgical Adaptations
Reconstruction of Systemic and Pulmonary veins in situs
inversus

Post Operative Note
Things to note Special surgical adaptations Ischemic time Bypass Time Blood Products required Post op TEE

Physiology – At Harvest
Harvesting site Function CAD Contusion
Procurement Fluid shifts harm RV
Myocardial Preservation Ischemic strategy
Hypothermia Pharmacologic arrest

Physiology –During Ischemia
No Oxygen to the muscle cells Decreased ATP use Can used stored Glycogen to make
ATP ATP too low= irreversible myofiber
contracture Ion homeostasis
Preservation Na-K pump reduced but still a
gradient Na H Ca-Ca lead to myofiber
damage

Physiology
Preservation Fluid Cold K to chemically arrest the heart Mg to protect from Ca Impermeants to stop cellular
swelling Free radical scavengers
HemodynamicsRhythmVentilationBleedingRejection/Immunosuppression Infection Prophylaxis
Post-op Care

Hemodynamics
Goals Inotropic support of the LV and RV Chronotropic support Decrease PVR Decrease SVR
Hemodynamics
Best Drug Isoproterenol
▪ Increases contractility and HR▪ Decrease PVR and SVR▪ Titrate HR
Milrinone▪ Increased contractility▪ Vasodilatory

Hemodynamics
Best Drug RV protection Avoid acidosis Hyperventilate 100% O2 Milrinone iNo Sildenafil Bosentan Prostacyclin if needed ECMO if needed
Function Hypoxic/Ischemic damage
( Troponin/ Lactate) Systolic function recovery rapid Diastolic function may persist for
weeks “Slump”-12 hours back off 2-5 days
Hemodynamics

Tools Exam CVP/RA line Arterial Blood Pressure Pacing wires
Hemodynamics

Elevated CVP (goal 8-12), with decrease CO Right heart failure ( pulmonary HTN,
massive blood transfusion, anatomic issue)
Decreased HCT without increase in the output of the tubes Cardiac tamponade
Troubleshoot
Factors Parasympathetic denervation Surgical trauma Catecholamines
Typical Sinus RBBB (14%-60%)
Possible Sinus node trauma-Bradycardia (2 weeks)-
18%-27% Recovers in 1-3 days CO= SV X HR
Rhythm- Physiology

Target Infant 140-150 bpm Teenager 100-120 bpm
Use Isoproternol or pacing if no response.
Pacing AAI ( preferred) or DDI Check the underline rhythm every
shift if the patient is paced. ECG upon arrival if not paced.
Rhythm

Ventilation
Similar principalsEarly extubationTracheobronchomalaciaPersistent atelectasis

Bleeding
Previous Cardiac SurgeriesCheck coagulation disorder pre-
opSame post bypass principalsBlood products= sensitization
One donor platlets Irradiated, Leukoreduced, Single
donor- PRBC FFP from pool of donors

Types of Rejection
Hyperacute- minutes to hours Cellular “Acute” (T cell)-attacks the
muscle 80% in first year
Humoral/Vascular “Chronic” (B cell)- antibodies attack the blood vessles creating narrowings

Immunologic Mechanisms of Rejection
Allorecognition
Activation of Antigen
Presenting Cell (APC)
APC recognized by T cell
TCR and costimulatory
signals are activated
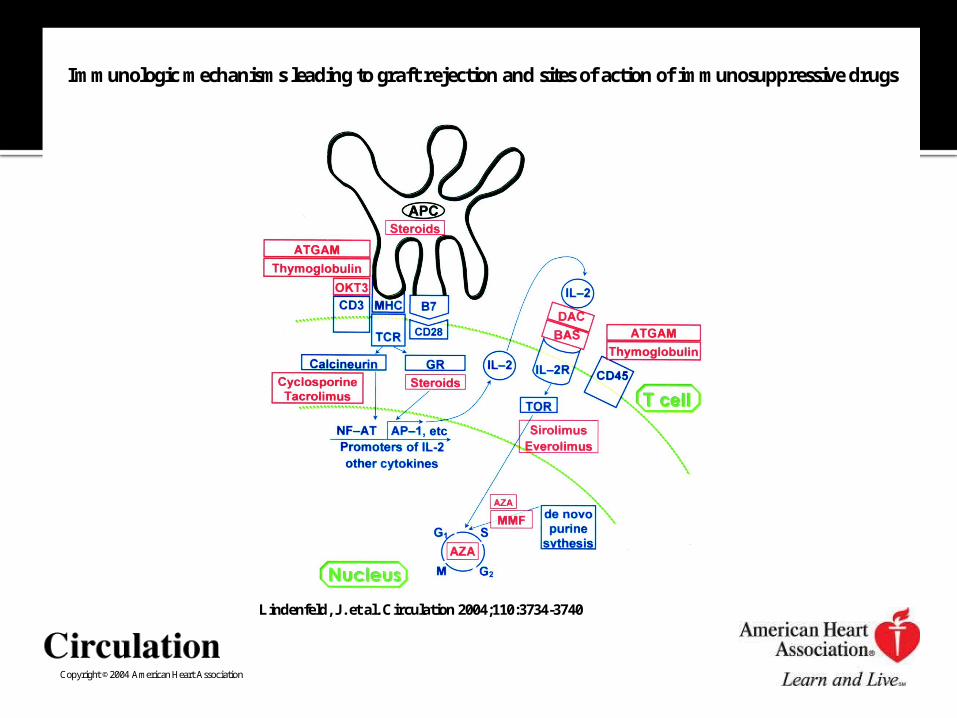
Copyright ©2004 American Heart Association
Lindenfeld, J . et al. Circulation 2004;110:3734-3740
Immunologic mechanisms leading to graft rejection and sites of action of immunosuppressive drugs

Types of Therapy
Induction Administration of a brief course of
high-dose immunosuppression in the preoperative and perioperative time period
Maintenance Less intense long term treatment
Rejection Additional therapy initiated due to
evidence of rejection

Anti-lymphocyte Polyclonal
ATGAM (horses)▪ Urticaria, serum
sickness, leukopenia, thrombocytopenia
ThymoglobulinO (rabbits)
Antibodies to surface receptors (CD3/CD45) cause apoptosis
Follow CD3 levels (5%-10% baseline/<50/ml)
SE both: fever, chills, rash
CMV!!!!! Need prophylaxis
Copyright ©2004 American Heart Association
Lindenfeld, J . et al. Circulation 2004;110:3734-3740
Immunologic mechanisms leading to graft rejection and sites of action of immunosuppressive drugs

Anti-Cytokine Receptor Antibodies
Bind to IL2 R Basiliximab
( Simulect) SE:
Infection Malignancy
Copyright ©2004 American Heart Association
Lindenfeld, J . et al. Circulation 2004;110:3734-3740
Immunologic mechanisms leading to graft rejection and sites of action of immunosuppressive drugs
Steroids
Diffuse freely across cell membrane and bind to receptors
Affect number, distribution and response of T and B cells
SE: hypertension, emotional lability, cosmetic changes, hyperlipidemia, salt and water retention, diabetes, osteopenia, growth retardation
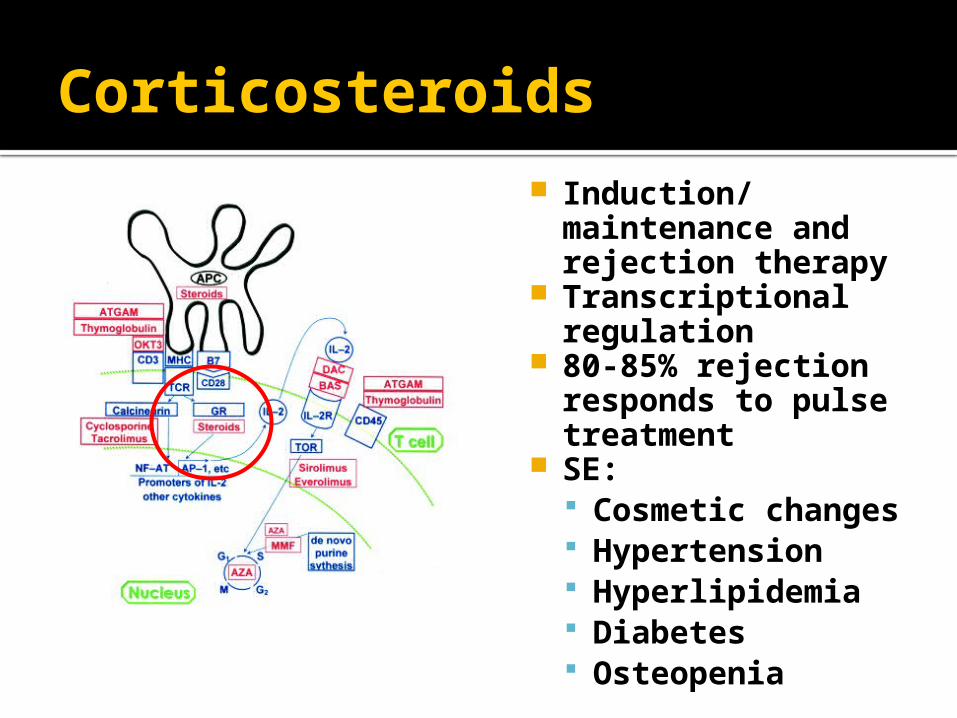
Corticosteroids Induction/
maintenance and rejection therapy
Transcriptional regulation
80-85% rejection responds to pulse treatment
SE: Cosmetic changes Hypertension Hyperlipidemia Diabetes Osteopenia

Antiproliferative Agents Mycophenolate
(MMF) (Cellcept) Maintenance
Therapy Inhibits DNA
synthesis and Tcell/B cell proliferation
Side Effects:▪ Nausea▪ Vomiting▪ Diarrhea

Calcineurin Inhibitors
Tacrolimus (FK506/Prograf) Maintenance
therapy Block IL-2
transcription Stimulates TGF- b
production Side Effect:
▪ Similar to CSA but hyperglycemia/diabetes, and neurologic toxicity are more common

Immunosuppression3 categories of outcomes Desired immunosuppressive effects
Adverse effects of immunodeficiency▪ Infection ▪ Malignancy
Nonimmune Toxicities▪ Diabetes▪ Hypertension▪ Renal insufficiency
Infection
Invasive lines and drains out ASAP Post-op antibiotic coverage with
First generation cephalosporin Vancomycin if MRSA
Prophylaxis CMV prophylaxis:▪ Ganciclovir
PCP prophylaxis:▪ Bactrim DS
Candida Prophylaxis:▪ Nystatin

Thank you Any Questions?