perioperative und paliative therapie des ... - gi-oncology.degi-oncology.de/download/2012/01-02...
TRANSCRIPT

GI Oncology 2012 8. Interdisziplinäres Update, 7. Juli 2012
Perioperative und paliative Therapie
des Ösophaguskarzinoms
- Standards und neue Studien -
Florian Lordick
Klinikum Braunschweig
Medizinische Klinik III (Hämatologie und Onkologie)
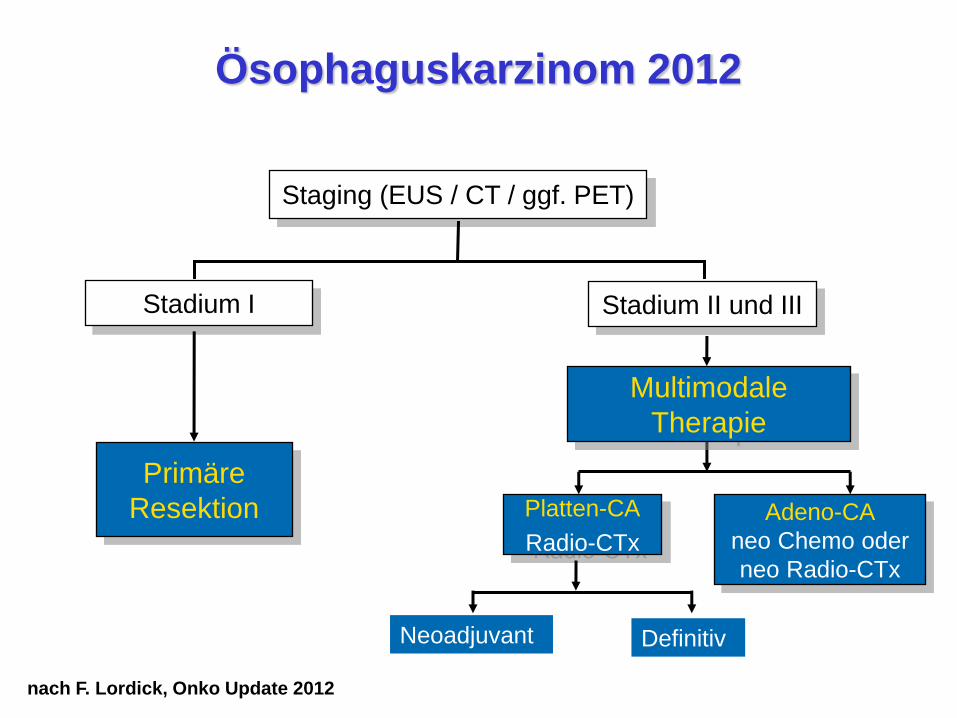
Staging (EUS / CT / ggf. PET)
Stadium I
Primäre
Resektion Adeno-CA
neo Chemo oder
neo Radio-CTx
Multimodale
Therapie
Platten-CA
Radio-CTx
Neoadjuvant Definitiv
nach F. Lordick, Onko Update 2012
Ösophaguskarzinom 2012
Stadium II und III

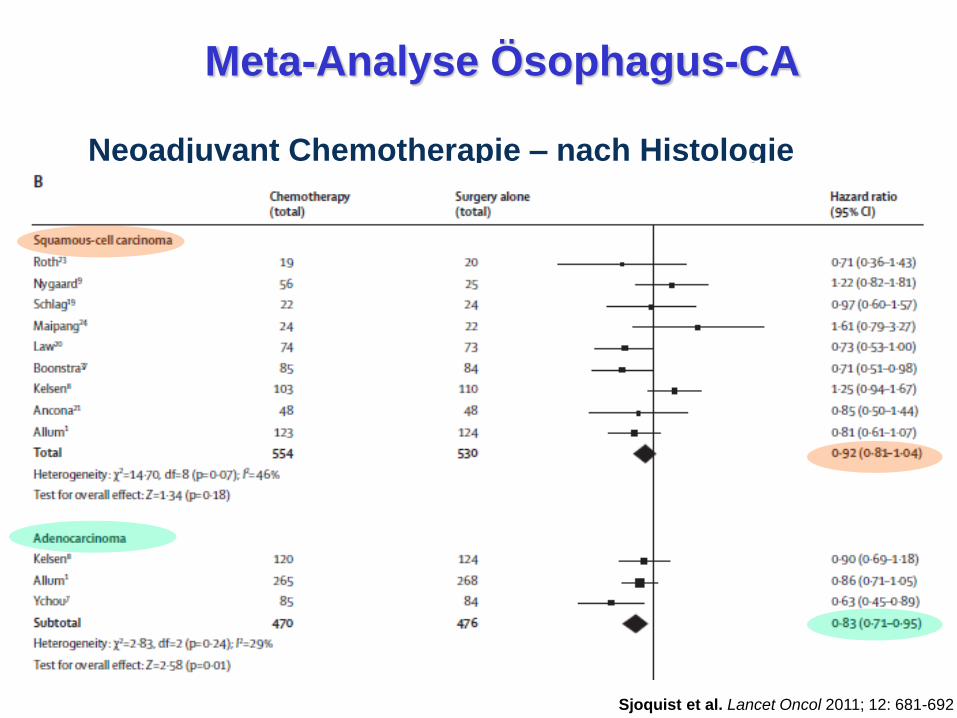
Meta-Analyse Ösophagus-CA
Sjoquist et al. Lancet Oncol 2011; 12: 681-692
Neoadjuvant Chemotherapie
Sjoquist et al. Lancet Oncol 2011; 12: 681-692
Neoadjuvant Chemotherapie – nach Histologie
Meta-Analyse Ösophagus-CA

Sjoquist et al. Lancet Oncol 2011; 12: 681-692
Neoadjuvant Radiochemotherapie
Meta-Analyse Ösophagus-CA

Sjoquist et al. Lancet Oncol 2011; 12: 681-692
Neoadjuvant Radiochemotherapie – nach Histologie
Meta-Analyse Ösophagus-CA
CROSS Studie (Niederlande)
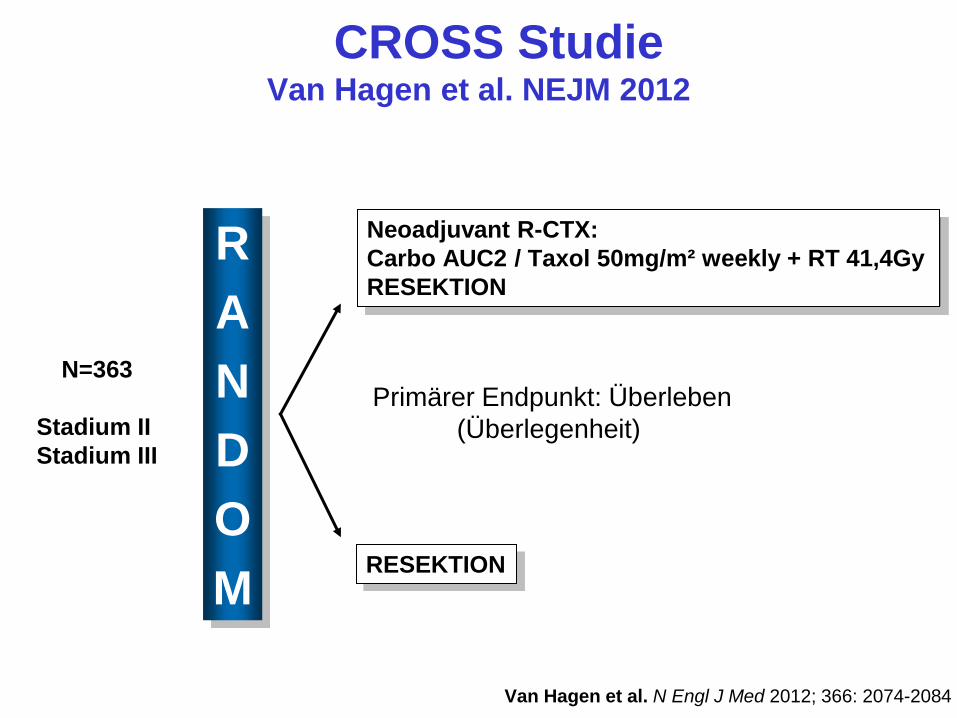
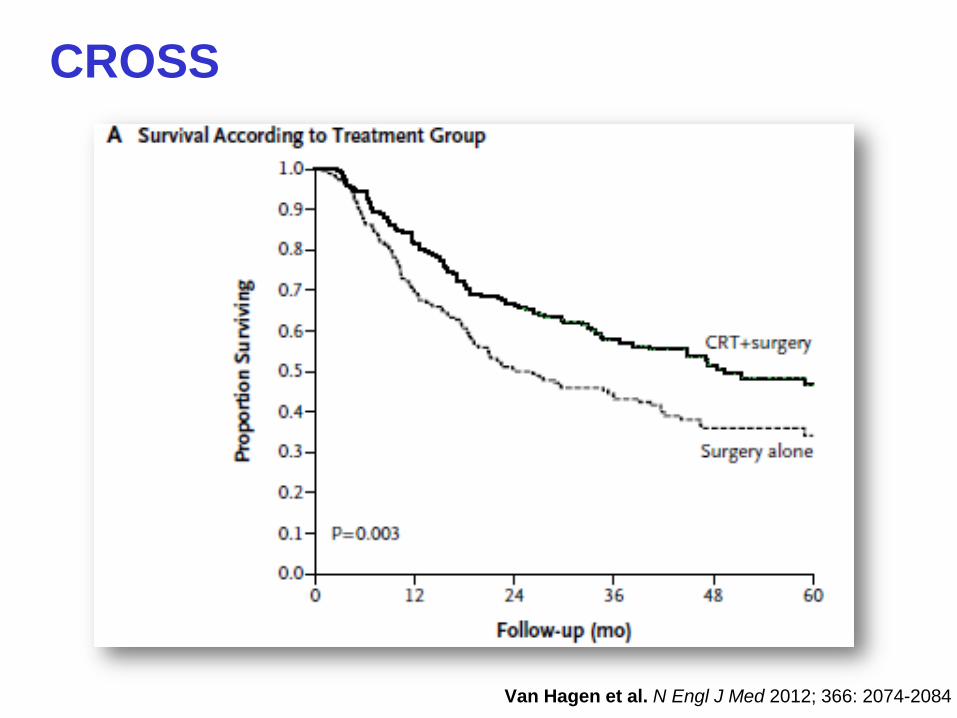
CROSS Studie Van Hagen et al. NEJM 2012
Van Hagen et al. N Engl J Med 2012; 366: 2074-2084
R
A
N
D
O
M
Primärer Endpunkt: Überleben
(Überlegenheit)
N=363
Stadium II
Stadium III
Neoadjuvant R-CTX:
Carbo AUC2 / Taxol 50mg/m² weekly + RT 41,4Gy
RESEKTION
RESEKTION

CROSS
Patientencharakteristika
RCTX + Chirurgie Chirurgie allein
Alter (median) 60 J. 60 J.
Geschlecht (männlich) 75% 81%
Histologie
Adeno-CA
Plattenepithel-CA
75%
23%
75%
23%
T Kategorie
cT2
cT3
15%
84%
19%
78%
N Kategorie
cN0
c N1
33%
65%
31%
64%

CROSS
Van Hagen et al. N Engl J Med 2012; 366: 2074-2084
RCTX + Chirurgie Chirurgie
allein
Klinik-Letalität 4% 4%
R0 Resektion 92% 69%
pCR Rate 29%
Medianes
Überleben
49,4 Mon 24 Mon HR 0,657
p = 0,003
5-Jahres-
Überleben
47% 34%
Ergebnisse
CROSS
Van Hagen et al. N Engl J Med 2012; 366: 2074-2084

CROSS
Van Hagen et al. N Engl J Med 2012; 366: 2074-2084
SCC: Plattenepithel-CA; AC: Adeno-CA
Was lernen wir aus CROSS?
Therapie in Zentren führt zu guten Ergebnissen
Carboplatin / Paclitaxel + RTX 41,4 Gy
ist ein gut toleriertes Therapieschema
Neoadjuvante R-CTx ist wirksam
Heidelberg fragt nach…
Email an: [email protected]
6. Juli 2012, 12:32
Hallo Florian,
Ist CROSS jetzt der neue Standard bei Ösophagus-CA?
Wie ist Deine Meinung?
Gruss, J.
Lieber Jürgen,
Plattenepithel-CA: ja.
Adeno-CA: ein Standard: ja! Der einzige Standard: nein!
Gruss, Florian
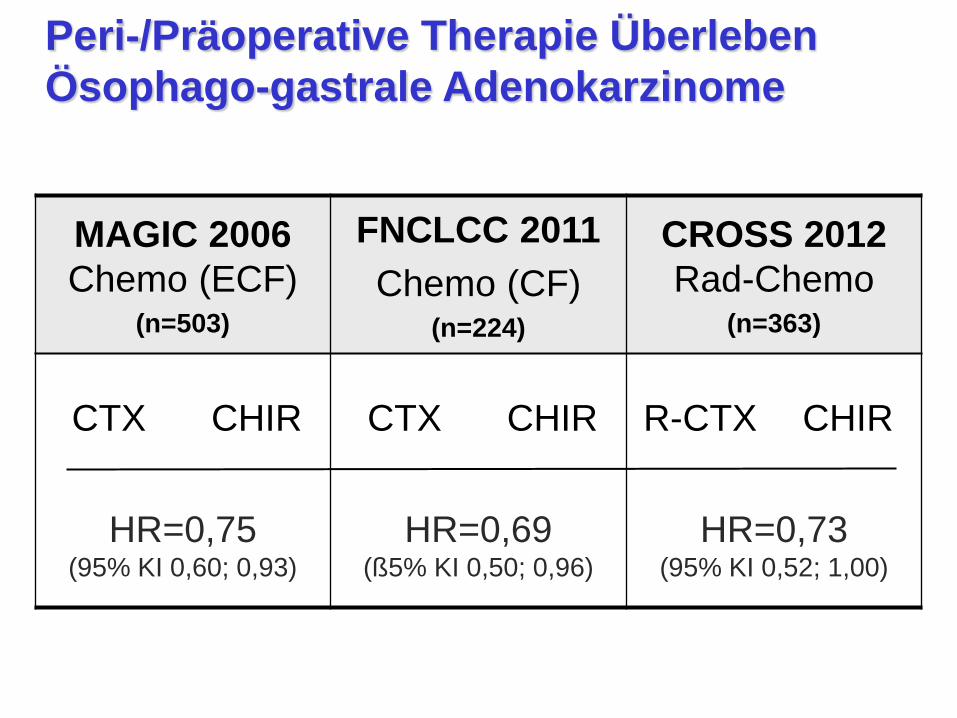
Peri-/Präoperative Therapie Überleben
Ösophago-gastrale Adenokarzinome
MAGIC 2006
Chemo (ECF) (n=503)
FNCLCC 2011
Chemo (CF) (n=224)
CROSS 2012
Rad-Chemo (n=363)
CTX CHIR CTX CHIR R-CTX CHIR
HR=0,75 (95% KI 0,60; 0,93)
HR=0,69 (ß5% KI 0,50; 0,96)
HR=0,73 (95% KI 0,52; 1,00)

Sjoquist et al. Lancet Oncol 2011; 12: 681-692
Neoadjuvant Radiochemotherapie vs. Chemotherapie
Meta-Analyse Ösophagus-CA
Sjoquist et al. Lancet Oncol 2011; 12: 681-692
Meta-Analyse Ösophagus-CA
neo Radiochemotherapie vs. Chemotherapie
“A clear advantage of neoadjuvant chemoradiotherapy over
neoadjuvant chemotherapy has not been established.”
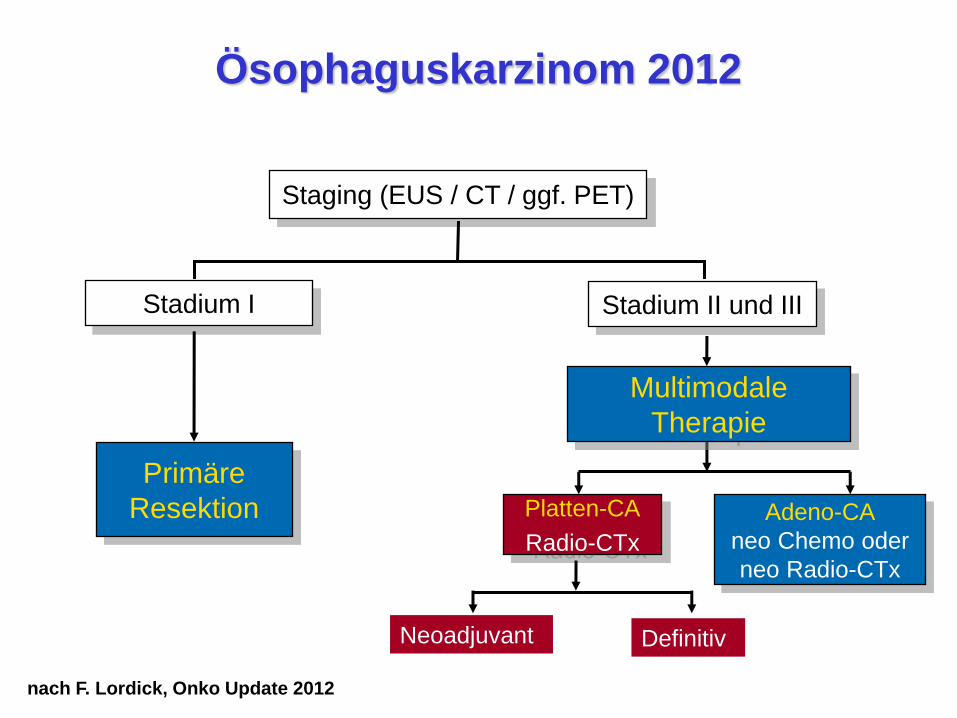
Staging (EUS / CT / ggf. PET)
Stadium I
Primäre
Resektion Adeno-CA
neo Chemo oder
neo Radio-CTx
Multimodale
Therapie
Platten-CA
Radio-CTx
Neoadjuvant Definitiv
nach F. Lordick, Onko Update 2012
Ösophaguskarzinom 2012
Stadium II und III
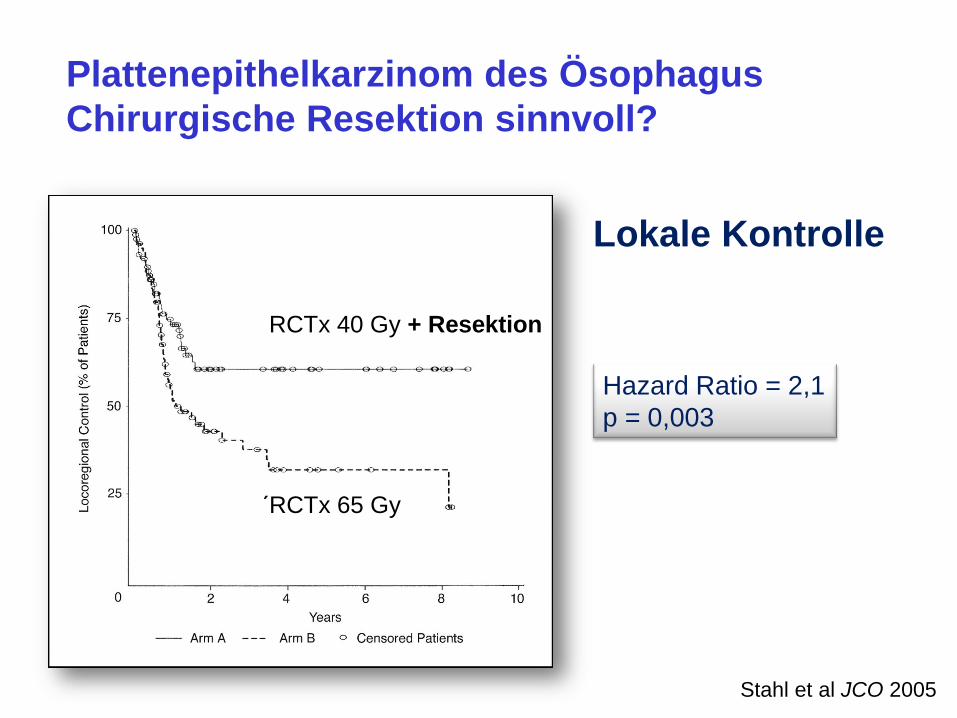
Plattenepithelkarzinom des Ösophagus
Chirurgische Resektion sinnvoll?
Stahl et al JCO 2005
Hazard Ratio = 2,1
p = 0,003
Lokale Kontrolle
RCTx 40 Gy + Resektion
´RCTx 65 Gy
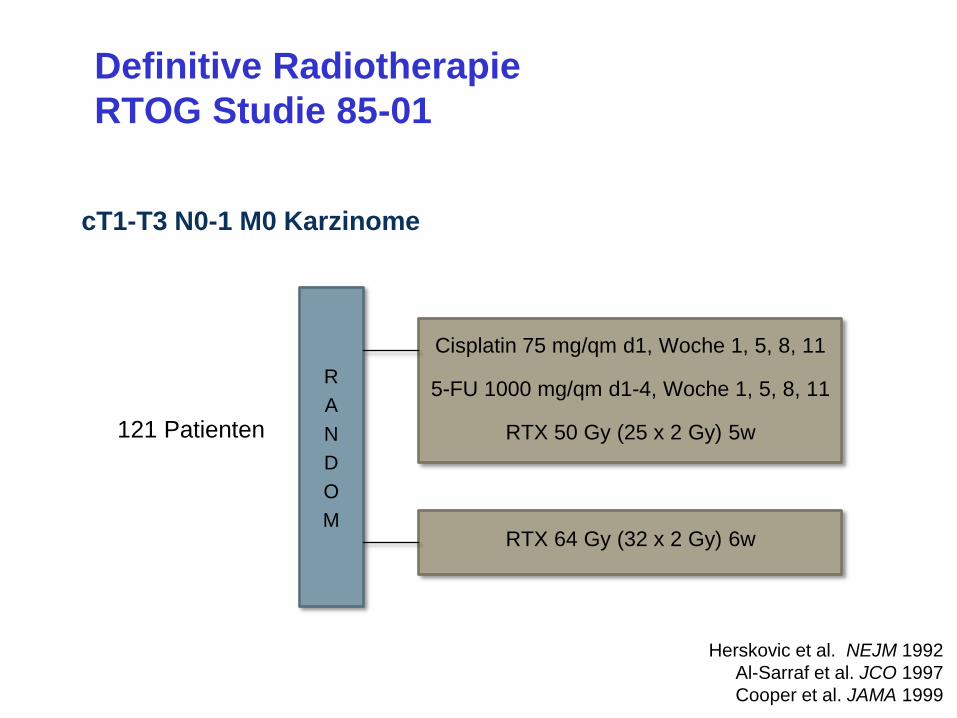
Definitive Radiotherapie
RTOG Studie 85-01
cT1-T3 N0-1 M0 Karzinome
121 Patienten
R
A
N
D
O
M
Cisplatin 75 mg/qm d1, Woche 1, 5, 8, 11
5-FU 1000 mg/qm d1-4, Woche 1, 5, 8, 11
RTX 50 Gy (25 x 2 Gy) 5w
RTX 64 Gy (32 x 2 Gy) 6w
Herskovic et al. NEJM 1992
Al-Sarraf et al. JCO 1997
Cooper et al. JAMA 1999
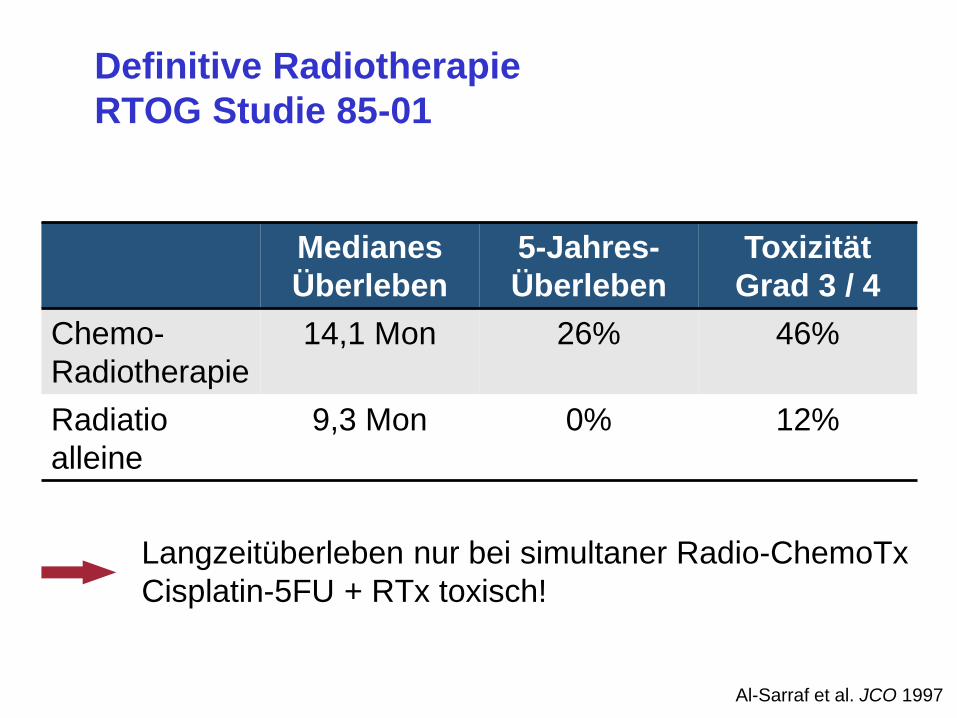
Al-Sarraf et al. JCO 1997
Langzeitüberleben nur bei simultaner Radio-ChemoTx
Cisplatin-5FU + RTx toxisch!
Medianes
Überleben
5-Jahres-
Überleben
Toxizität
Grad 3 / 4
Chemo-
Radiotherapie
14,1 Mon 26% 46%
Radiatio
alleine
9,3 Mon 0% 12%
Definitive Radiotherapie
RTOG Studie 85-01
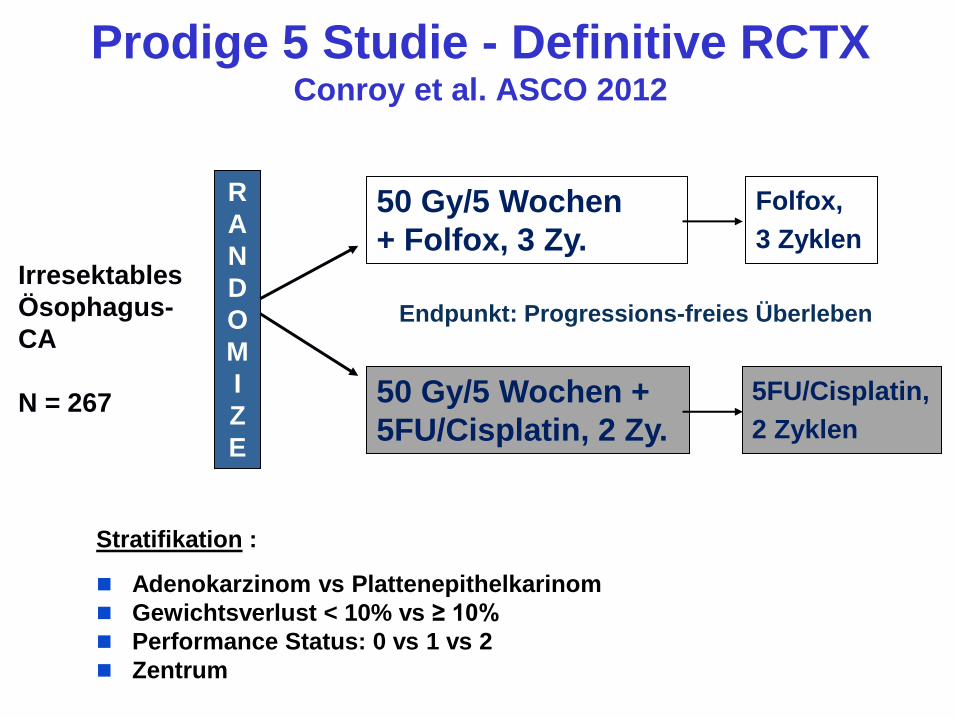
Prodige 5 Studie - Definitive RCTX Conroy et al. ASCO 2012
Stratifikation :
Adenokarzinom vs Plattenepithelkarinom
Gewichtsverlust < 10% vs ≥ 10%
Performance Status: 0 vs 1 vs 2
Zentrum
Irresektables
Ösophagus-
CA
N = 267
R
A
N
D
O
M
I
Z
E
50 Gy/5 Wochen
+ Folfox, 3 Zy.
50 Gy/5 Wochen +
5FU/Cisplatin, 2 Zy.
Folfox,
3 Zyklen
5FU/Cisplatin,
2 Zyklen
Endpunkt: Progressions-freies Überleben

0.00
0.25
0.50
0.75
1.00
Pro
ba
bili
ty
134 106 76 48 33 18 6 5 3FOLFOX+RT133 105 74 43 25 19 10 3 05FU/CDDP+RT
Number at risk
0 6 12 18 24 30 36 42 48Months
5FU/CDDP+RT FOLFOX+RT
HR=0.94: 95%CI[0.68-1.29]
Med OS Folfox+RT:
20.2 mo. [14.7 – 25.6]
Med OS FU/CDDP+RT:
17.5 mo. [13.9 – 19.4]
Prodige 5: Überleben
Conroy et al ASCO 2012
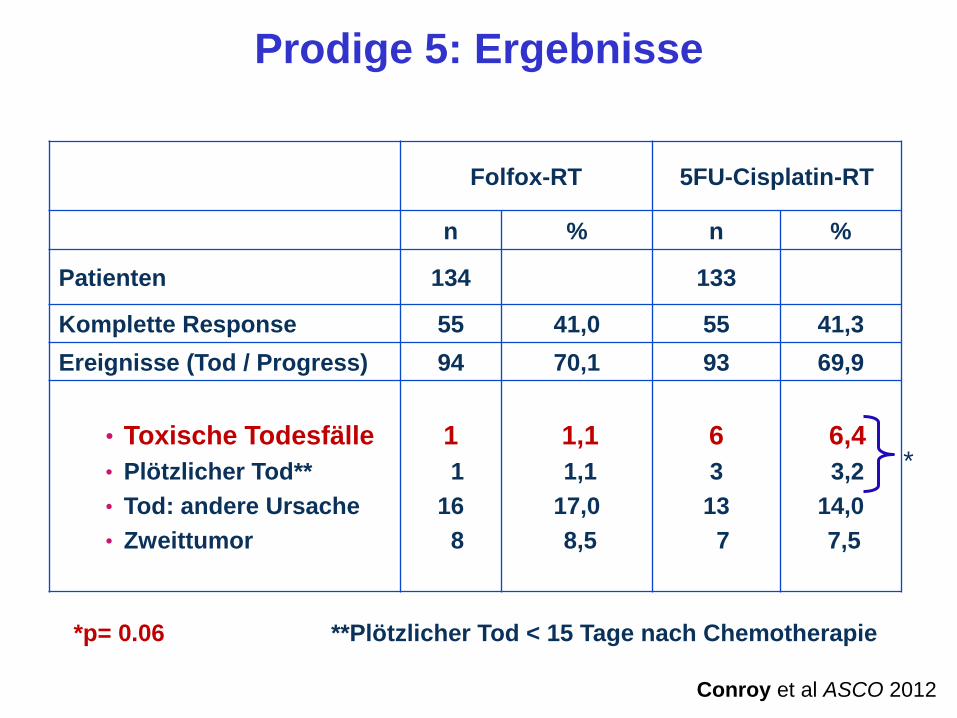
Prodige 5: Ergebnisse
Folfox-RT 5FU-Cisplatin-RT
n % n %
Patienten 134 133
Komplette Response 55 41,0 55 41,3
Ereignisse (Tod / Progress) 94 70,1 93 69,9
• Toxische Todesfälle
• Plötzlicher Tod**
• Tod: andere Ursache
• Zweittumor
1
1
16
8
1,1
1,1
17,0
8,5
6
3
13
7
6,4
3,2
14,0
7,5
*p= 0.06 **Plötzlicher Tod < 15 Tage nach Chemotherapie
*
Conroy et al ASCO 2012
Was lernen wir aus PRODIGE-5?
FOLFOX-RT ist wirksam und bietet mehr
Sicherheit als Cisplatin/5FU-RT
Empfehlenswert bei simultaner RCTx
des Ösophaguskarzinoms

Optimierungspotenzial
Medikamentöse Therapie
Ösophaguskarzinom
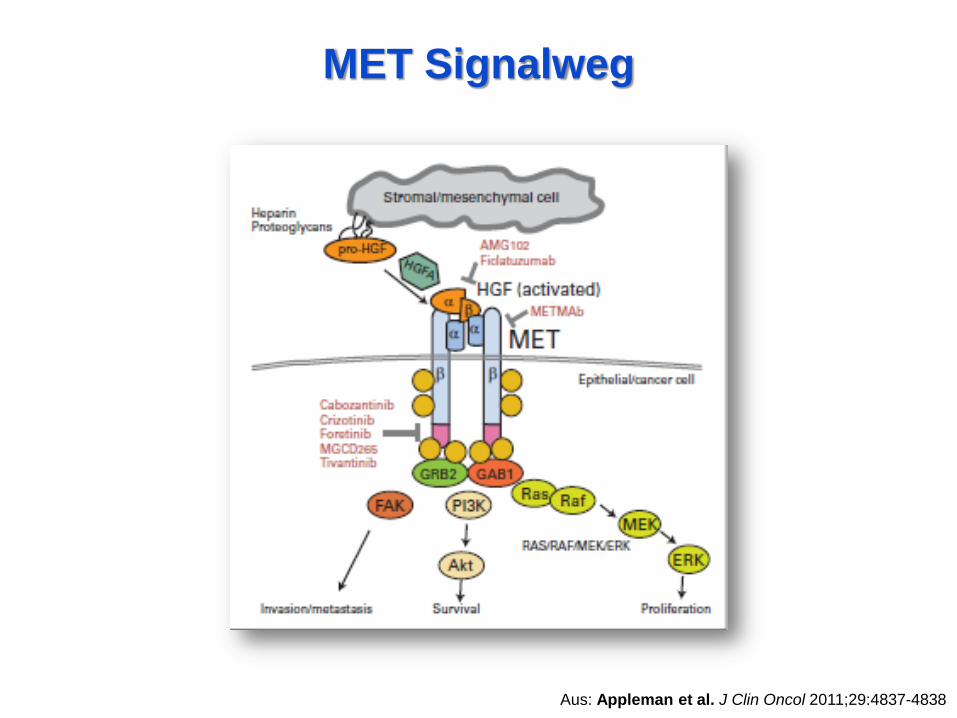
MET Signalweg
Aus: Appleman et al. J Clin Oncol 2011;29:4837-4838
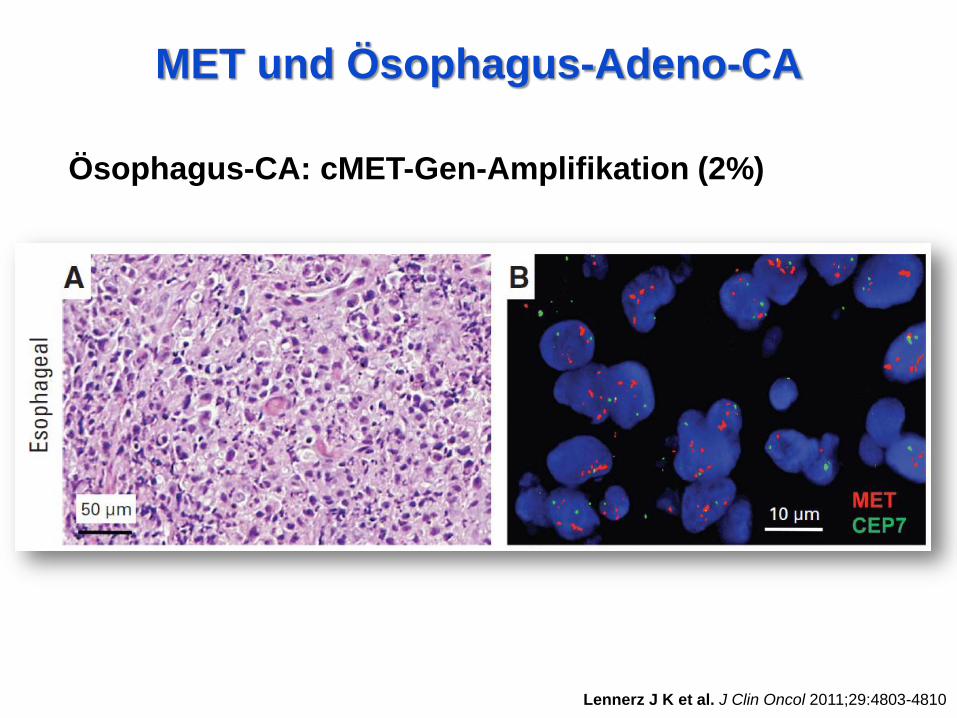
MET und Ösophagus-Adeno-CA
Lennerz J K et al. J Clin Oncol 2011;29:4803-4810
Ösophagus-CA: cMET-Gen-Amplifikation (2%)
Lennerz J K et al. J Clin Oncol 2011;29:4803-4810
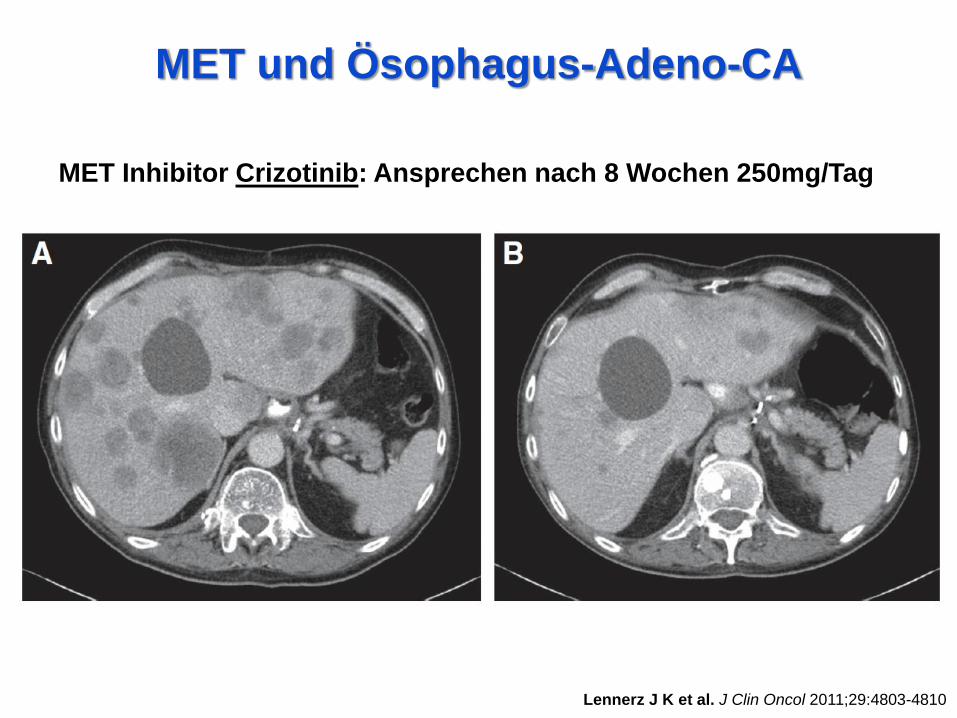
MET Inhibitor Crizotinib: Ansprechen nach 8 Wochen 250mg/Tag
MET und Ösophagus-Adeno-CA
EGFR Plattenepithelkarzinome
Lorenzen et al. Ann Oncol 2009; 20: 1667-1673
Weitgehend homogene EGFR-Expression
Kein Nachweis von k-RAS-Mutationen
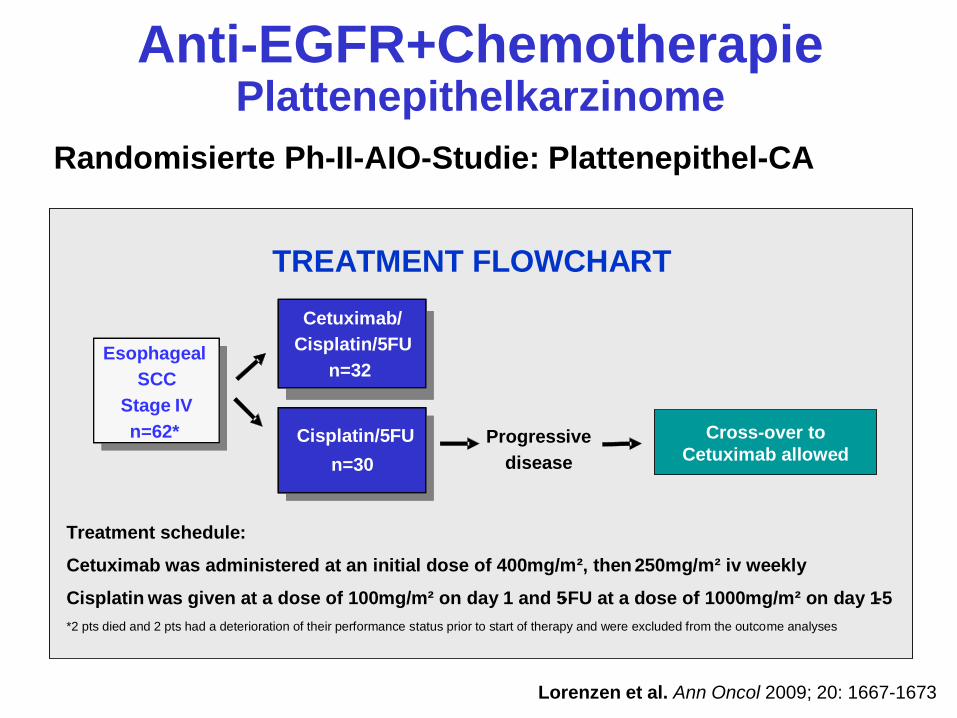
Anti-EGFR+Chemotherapie Plattenepithelkarzinome
Randomisierte Ph-II-AIO-Studie: Plattenepithel-CA
Lorenzen et al. Ann Oncol 2009; 20: 1667-1673
TREATMENT FLOWCHART
Esophageal
SCC
Stage IV
n= 62*
Esophageal
SCC
Stage IV
n=62*
Cisplatin/5FU
n= 30
Progressive
disease
Treatment schedule:
Cetuximab was administered at an initial dose of 400mg/m², then 250mg/m² iv weekly
Cisplatin was given at a dose of 100mg/m² on day 1 and 5-FU at a dose of 1000mg/m² on day 1-5
*2 pts died and 2 pts had a deterioration of their performance status prior to start of therapy and were excluded from the outcome analyses
Cetuximab/
Cisplatin/5FU
n=32
n=30
Cisplatin/5FU Cross-over to
Cetuximab allowed

AIO-Oesotux-Studie
Progressions-freies Überleben
Lorenzen et al. Ann Oncol 2009; 20: 1667-1673
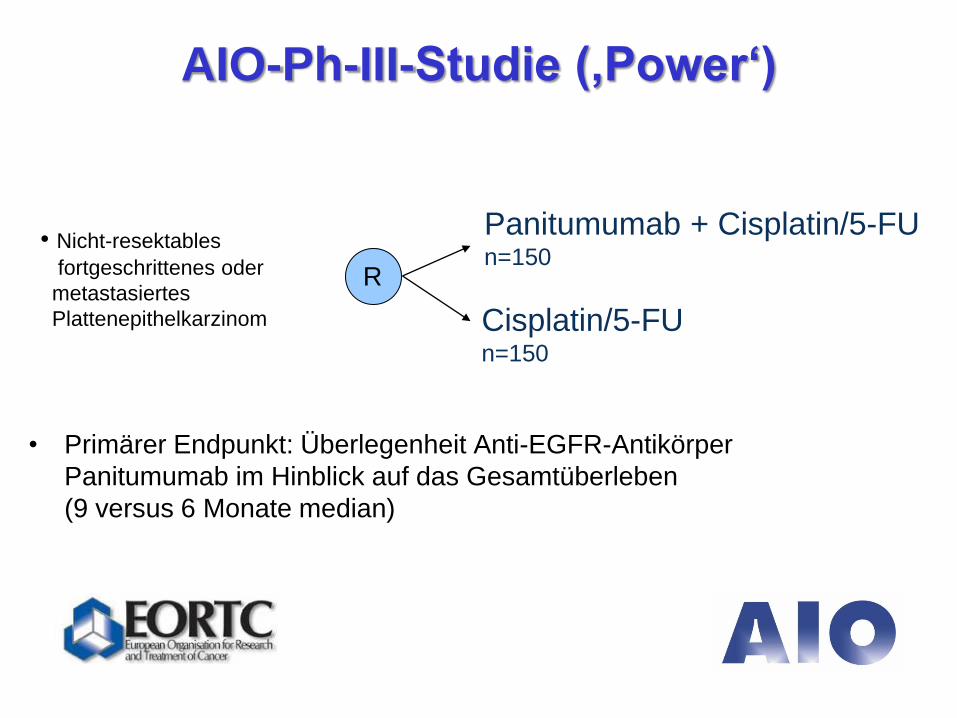
AIO-Ph-III-Studie (‚Power‘)
• Primärer Endpunkt: Überlegenheit Anti-EGFR-Antikörper
Panitumumab im Hinblick auf das Gesamtüberleben
(9 versus 6 Monate median)
Panitumumab + Cisplatin/5-FU n=150
Cisplatin/5-FU n=150
R
• Nicht-resektables
fortgeschrittenes oder
metastasiertes
Plattenepithelkarzinom

Medikamentöse Therapie
des Ösophaguskarzinom
Fortschritt in Sicht
EGFR (Platte) und MET (Adeno):
potenzielle neue Targets (Studien abwarten!)
HER2 (Adeno-CA): vergleichbar Magen-CA