peripheral nerve function – metabolic features, clinical - diva
TRANSCRIPT
Peripheral nerve function – metabolic features, clinical assessment, and heat shock protein 27 Kaveh Pourhamidi
Umeå University Umeå, Sweden Medical Dissertation 2013

Responsible publisher under Swedish law: the Dean of the Medical Faculty, This work is protected by the Swedish Copyright Legislation (Act 1960:729) © Kaveh Pourhamidi 2013 New series nr: 1589 ISBN: 978-91-7459-692-2 ISSN: 0346-6612 Electronic version available at http://umu.diva-portal.org/ Printed by: Print & Media, Umeå University Umeå, Sweden 2013

��������
To�my�parents�


5
Table of Contents
Diabetes Mellitus 11
Impaired glucose tolerance 12
Peripheral neuropathy – General considerations 12
Methods for assessing peripheral nerve function 17
Symptoms and signs of diabetic neuropathy 20
Diagnostic criteria for peripheral neuropathy in diabetes mellitus 23
IGT and peripheral neuropathy 23
Treatment of diabetic neuropathy 24
Pathogenesis of diabetic neuropathy 24
Heat shock protein 27 27
Study populations 30
Laboratory investigation 33
Heat shock protein 27 analyses 33
Clinical assessment 34
Statistical analyses 38
Paper I 39
Paper II 41
Paper III 44
Paper IV 44
Neuropathy in prediabetes or prediabetes in neuropathy? 46
Comparison of clinical tools and their use in detecting peripheral neuropathy 48
Insufficient neuroprotection in diabetes mellitus? 50
Limitations and strengths 53
Future perspectives 56

6
Abstract Peripheral neuropathy is a common complication among patients with diabetes mellitus, but whether peripheral neuropathy is present in individuals with impaired glucose tolerance (IGT) is debatable. In order to identify and diagnose peripheral neuropathy correctly, it is important to evaluate diagnostic tools that can be implemented in routine health care to assess both large and small nerve fibre function. There is currently limited knowledge about neuroprotective factors that could be useful for measuring peripheral nerve function in individuals at risk of developing neuropathy such as those with diabetes mellitus. Thus, studies are needed to investigate potential neuroprotective factors in relation to peripheral nerve function in humans. Objectives: The overall goal of this thesis was to study the metabolic features and clinical assessment of peripheral nerve function and the potential relationship between the neuroprotective factor heat shock protein 27 (HSP27) and peripheral nerve function. Methods: Thirty-nine participants with normal glucose tolerance (NGT) and 29 participants with IGT were recruited from the population-based Västerbotten Intervention Programme in 2003–2004. Patients with type 2 diabetes mellitus (T2DM, n = 51) were recruited from primary health care centres. NGT and IGT individuals underwent two separate oral glucose tolerance tests to verify their glucose status. The peripheral nerve function in the lower limb was assessed by nerve conduction studies, neuropathy disability scoring, quantitative sensory tests, and skin biopsies with subsequent quantification of intraepidermal nerve fibre density (IENFD). The concentrations of HSP27 in serum were determined in the NGT, IGT, and T2DM individuals. Patients with type 1 diabetes mellitus (T1DM) were recruited from the Diabetes Clinic, Skåne University Hospital in Malmö, Sweden (n = 27) in 1992 and were followed-up in 2005. Baseline and follow-up concentrations of HSP27 were determined in T1DM patients as well as in healthy non-diabetic controls (n = 397). The T1DM patients underwent nerve conduction studies and thermal and vibration perception threshold tests at baseline and at follow-up. Delta changes in HSP27 concentrations and small and large nerve fibre function were calculated. Results: There was no difference between IGT and NGT in sural nerve conduction, intraepidermal nerve fibre density, or thermal thresholds. The biothesiometer had a sensitivity of 82% and a specificity of 72% in identifying peripheral neuropathy with a cut-�������������� ����������medial malleolus. Adding the quantification of IENFD to the combination of the tuning fork and biothesiometer increased the diagnostic sensitivity from 81% to 95%, the negative predictive value from 87% to 94%, and the positive likelihood ratio from 1.8 to 1.9 when identifying small nerve fibre dysfunction. T2DM patients had lower HSP27 concentrations (mean HSP27 = 412 pg/mL, 95% CI 284–598 pg/mL) than NGT (mean HSP27 = 722 pg/mL, 95% CI 564–922 pg/mL) and IGT (mean HSP27 = 1010 pg/mL, 95%

7
CI 638–1300 pg/mL) individuals (p <0.05 for both comparisons). T1DM patients had lower HSP27 concentrations at baseline (mean HSP27 = 547 pg/mL, 95% CI 421–711 pg/mL) and at follow-up (mean HSP27 = 538 pg/mL, 95% CI 417–693 pg/mL) compared to healthy controls (mean HSP27 = 785 pg/mL, 95% CI 732–842 pg/mL), p <0.05 for both comparisons). High concentrations of HSP27 were associated with better large nerve fibre function (Odds ratio = 2.51, 95% CI 1.25–5.05, p <0.05). Deteriorating large nerve fibre function correlated with decreasing HSP27 concentrations over time in T1DM patients (r = 0.50, p = 0.01). Conclusions: Measures of large and small nerve fibre function in IGT individuals do not differ significantly from NGT individuals. The existence of peripheral neuropathy as a consequence of IGT is not likely, and extensive control of neuropathy in IGT individuals is not advocated by this thesis. The biothesiometer is a useful clinical tool to identify peripheral neuropathy in routine health care. Quantification of IENFD using skin biopsies in combination with methods measuring vibrotactile sense, such as the biothesiometer and the tuning fork, increase the diagnostic usefulness of identifying small nerve fibre dysfunction. High HSP27 concentrations are associated with better peripheral large nerve fibre function. Patients with diabetes mellitus have lower HSP27 concentrations than healthy non-diabetic controls, and deterioration of large nerve fibre function correlates with a decrease in HSP27 concentrations over time in T1DM. This could be indicative of insufficient neuroprotection in patients with diabetes mellitus.
8
Abbreviations
ANS autonomic nervous system
AUC area under the curve
BMI body mass index
CNS central nervous system
DSPN distal symmetric polyneuropathy
HSP27 heat shock protein 27
IENFD intraepidermal nerve fibre density
IFG impaired fasting glucose
IGT impaired glucose tolerance
IQR interquartile range
NCS nerve conduction study
NDR national diabetes registry
NDS neuropathy disability score
NGT normal glucose tolerance
OGTT oral glucose tolerance test
PNS peripheral nervous system
QST quantitative sensory testing
ROC receiver operating characteristic
T1DM type 1 diabetes mellitus
T2DM type 2 diabetes mellitus
VIP Västerbotten Intervention Programme
VPT vibration perception threshold
9
List of Papers
I.� No difference in small or large nerve fiber function
between individuals with normal glucose tolerance and impaired glucose tolerance. Pourhamidi K, Dahlin LB, Englund E, Rolandsson O. Diabetes Care 36:962-964, 2013
II.� Evaluation of clinical tools and their diagnostic use in distal symmetric polyneuropathy. Pourhamidi K, Dahlin LB, Englund E, Rolandsson O. Prim Care Diabetes. 2013. Ahead of print, doi:10.1016/j.pcd.2013.04.004
III.� Heat shock protein 27 is associated with better nerve
function and fewer signs of neuropathy. Pourhamidi K, Dahlin LB, Boman K, Rolandsson O. Diabetologia 54:3143-3149, 2011
IV.� Heat shock protein 27 concentrations are lower in patients
with type 1 diabetes mellitus than in healthy controls and correlates with large nerve fibre dysfunction. Pourhamidi K, Skärstrand H, Dahlin LB, Rolandsson O. (submitted)
Permission to reprint the published articles has been granted from the publishers.

10
Introduction Why study peripheral neuropathy and glucose metabolism? Increasing obesity, unhealthy diets, and sedentary lifestyles have led to a global population that is more prone to diabetes mellitus and its complications [1, 2]. Diabetic neuropathy is a common complication seen in routine health care and is the most common form of peripheral neuropathy in the developed world [3-6]. Diabetic neuropathy is, therefore, a major health problem with serious consequences for the patient and results in a significant financial burden on health care systems. This is especially true due to the current global epidemic of diabetes mellitus [1]. I became familiar with diabetes mellitus and neuropathy during my undergraduate studies in medicine, and at the midpoint of my studies I became involved in the projects that make up this thesis. Both my mother and father were diagnosed with type 2 diabetes mellitus. At the same time, my father was progressing in his diabetic neuropathy and he was suffering from disabling pain. I witnessed how his symptoms clearly affected his quality of life, and through my clinical work I have encountered many patients who are also struggling with the debilitating effects of diabetic neuropathy. These personal experiences were strong influences for my wanting to complete my thesis on the study of peripheral neuropathy. There is currently a debate as to whether peripheral neuropathy can occur before the onset of established diabetes mellitus, i.e. in the pre-diabetic stage, as in impaired glucose tolerance (IGT) [7-10]. Thus, it is important to study peripheral neuropathy in diabetes mellitus as well as in IGT because our increased knowledge about the pathogenesis of diabetic neuropathy has not been accompanied by successful treatments. Conventional clinical tools are not always sensitive or specific enough to identify small and large nerve fibre dysfunction, and nerve conduction studies, which are often considered the gold standard in the assessment of peripheral neuropathy, mainly detect large nerve fibre dysfunction and can overlook small nerve fibre dysfunction. Thus, I believe it is important to study and reassess current methods in order to measure large and small nerve fibre function objectively and reliably. Several randomized and controlled studies investigating enhanced glycaemic control and peripheral neuropathy have shown that enhanced glucose control prevents the development of peripheral neuropathy in type 1 diabetes mellitus [13, 14]. However, this effect on the development of neuropathy was more modest in type 2 diabetes mellitus [15-17]. Thus, factors other than hyperglycaemia might be important in the development of neuropathy, and neuroprotective molecules are good candidates for further investigation. Heat shock protein 27 (HSP27), a member of the small heat shock protein family, is a protein chaperone and an antioxidant that has been shown in animal studies to play an important role in cell motility and cytoprotection by acting as a filament stabilizer and by inhibiting apoptotic pathways [18-22]. Thus, HSP27 could perhaps play a significant role in relation to peripheral nerve function in humans.

11
Background Diabetes Mellitus Diabetes mellitus is a common disease in both the developed and the developing world, and it has been estimated that the number of individuals afflicted with diabetes mellitus globally has increased from 153 million in 1980 to 347 million in 2008 [1, 2]. This dramatic increase reflects the epidemic nature of this disease. Diabetes mellitus is a chronic disease that results when the pancreas fails to produce enough insulin (insulin deficiency) and/or when the body cannot efficiently use the insulin produced (insulin resistance). Because insulin is the hormone that regulates blood glucose concentrations, individuals with uncontrolled diabetes mellitus develop increased glucose concentrations (hyperglycaemia) over time. Hyperglycaemia can in turn damage many of the human body's systems, including the nervous system and cardiovascular system. Examples of chronic complications due to diabetes mellitus include nephropathy, retinopathy, neuropathy, and cardiovascular diseases such as stroke and coronary artery disease. Type 1 diabetes mellitus (T1DM) is a complex, polygenic disease in which autoimmune destruction of insulin-producing beta cells in the pancreas results in insulin deficiency [23]. Insulin deficiency leads to increased blood and urine glucose concentrations. Left untreated, T1DM is a serious and often fatal disease but it can be controlled with administration of exogenous insulin. Type 2 diabetes mellitus (T2DM) also involves both genetic and environmental factors and is characterized by high blood glucose levels due to both insulin resistance and insulin deficiency [23]. Obesity is a significant risk factor for the development of T2DM in people who are genetically predisposed to T2DM [24, 25]. Features of the metabolic syndrome, including fasting hyperglycaemia, hypertension, obesity, and high cholesterol, are frequently seen in T2DM [26, 27]. (See Appendix A for the diagnostic criteria set by the World Health Organization). Latent autoimmune diabetes in adults (LADA) refers to a slow-onset of T1DM in adults in which not all individuals are characteristically thin but are obese instead [28, 29]. This leads to these patients being misdiagnosed as having T2DM because of their weight and age. Other forms of diabetes are possible, such as gestational diabetes and monogenic diabetes, but these will not be discussed further in this thesis.
12
Impaired glucose tolerance The term prediabetes is sometimes used to describe conditions in which hyperglycaemia is present but the criteria for diabetes mellitus are not met. One of these conditions is called impaired glucose tolerance (IGT) and is characterized by a state of prolonged and abnormal rise in blood glucose concentrations after eating, although the rise is not as great as in T2DM. In this condition, fasting blood glucose concentrations remain normal. In another condition, called impaired fasting glycaemia (IFG), fasting blood glucose concentrations are elevated above normal but not enough to be defined as diabetes mellitus. Both IGT and IFG are associated with insulin resistance and secretion and with an increased risk of cardiovascular disease [30, 31]. IGT usually precedes T2DM, and individuals can remain in the IGT state for many years before progressing to overt T2DM [32]. These individuals can develop other metabolic risk factors over time and can also revert to normal glucose tolerance. (See Appendix A for diagnostic criteria set by the World Health Organization). Peripheral neuropathy – General considerations The human nervous system consists of the brain, spinal cord, and a network of neurons throughout the body. The nervous system is responsible for monitoring and coordinating organ functions and for sending, receiving, and interpreting information about changes in the external environment. This complex system of neural structures can be divided into two parts: the central nervous system (CNS) and the peripheral nervous system (PNS). The PNS is the subject of this thesis. The PNS consists of several cell types (anterior horn cells, dorsal root ganglion cells, autonomic ganglion cells, satellite cells, Schwann cells, and connective tissue) and structures (spinal nerves, nerves of the extremities, cranial nerves, and the cervical, brachial, and lumbosacral plexi). Together these cells and cellular structures provide the somatosensory and autonomic functions of the human body [33], and the PNS works as a two-way communication link between the CNS and the sensory, motor, and visceral end organs. Peripheral neuropathy includes a range of functional and pathologic disorders involving the PNS. The term polyneuropathy describes disorders resulting from diffuse lesions on the peripheral nerves and usually presents as sensory loss, pain, weakness, and autonomic dysfunction. Mononeuropathies specify disorders of a single nerve that are typically due to local trauma or compression or as an effect of diabetes mellitus. Mononeuropathy multiplex refers to focal involvement of two or more nerves usually as a result of a systemic disorder such as diabetes mellitus or vasculitis. The term neuritis usually refers to inflammatory disorders of nerves resulting from autoimmune reactions or from infection. When there is a disease or compression of the spinal nerve root, the term radiculopathy is sometimes used. The term axonopathy is used when there is axonal degeneration with preservation of neuron cell bodies. Loss of the whole neuron (cell body and axon) is referred to as a neuronopathy. Peripheral neuropathies can also result in alterations within the CNS, e.g. through involvement of dorsal root ganglion (DRG) cells and their central processes

13
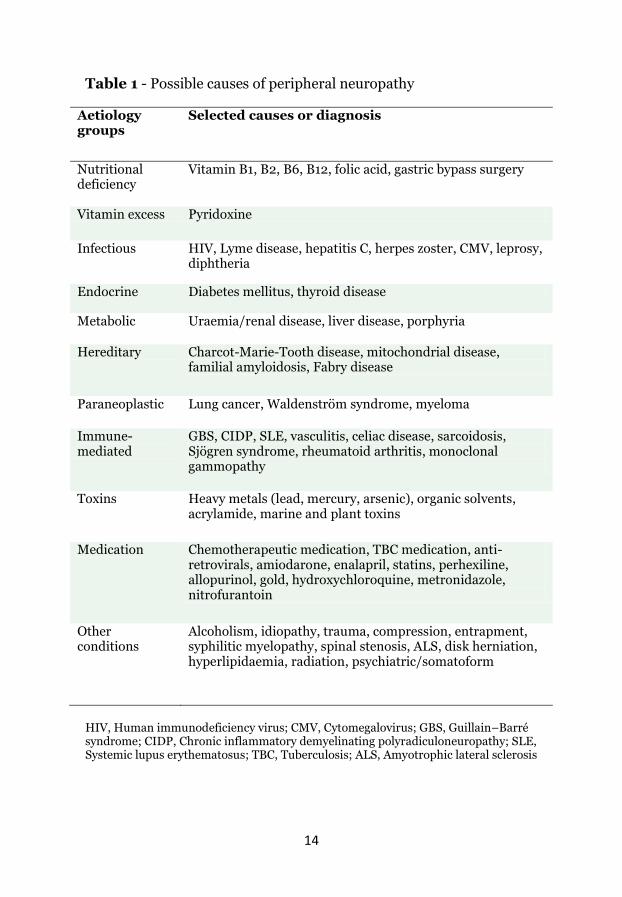
or through the involvement of the cell bodies and proximal axons of lower motor neurons within the spinal cord. Peripheral neuropathies can be classified as heritable or acquired forms [34] and Table 1 presents the possible causes of peripheral neuropathies. The most common form of the acquired neuropathies is generalized polyneuropathy, which will be described and discussed further in this thesis and is from here on referred to as peripheral neuropathy. The leading cause of peripheral neuropathy is diabetes mellitus (diabetic neuropathy) and is usually presented as a chronic and diffuse distal symmetric polyneuropathy (DSPN) with or without autonomic dysfunction [35]. Although diabetes mellitus, alcohol abuse, and vitamin B12 deficiency are common causes of polyneuropathy, one should try to search for other clues and exclude other aetiologies. The prevalence of peripheral neuropathy in diabetes mellitus is rather difficult to estimate because definitions of diabetic neuropathy have varied between studies. However, in general peripheral neuropathy has been reported to have a prevalence ranging from 20% to 50% in individuals with T1DM or T2DM with an average prevalence of 30% [36-41]. The prevalence of peripheral neuropathy increases with the duration of diabetes mellitus, and it is present in more than 50% of T2DM patients over 60 years of age [40]. In addition, peripheral neuropathy can be present in up to 21% of patients who have had diabetes mellitus for less than 5 years [40]. Furthermore, the prevalence of peripheral neuropathy varies from 10% within a year of diabetes mellitus diagnosis to 50% in patients who have had diabetes mellitus for 25 years or more [42-44]. As of 2010, the global prevalence of peripheral neuropathy associated with diabetes mellitus was almost 132 million people, or 2% of the world population [3]. Individuals with diabetes mellitus can also have more acute neuropathies as well as various forms of mononeuropathies, but these less frequent diabetic neuropathies will not be described further.
14
Table 1 - Possible causes of peripheral neuropathy
Aetiology groups
Selected causes or diagnosis
Nutritional deficiency
Vitamin B1, B2, B6, B12, folic acid, gastric bypass surgery
Vitamin excess Pyridoxine
Infectious HIV, Lyme disease, hepatitis C, herpes zoster, CMV, leprosy, diphtheria
Endocrine Diabetes mellitus, thyroid disease
Metabolic Uraemia/renal disease, liver disease, porphyria
Hereditary Charcot-Marie-Tooth disease, mitochondrial disease, familial amyloidosis, Fabry disease
Paraneoplastic Lung cancer, Waldenström syndrome, myeloma
Immune-mediated
GBS, CIDP, SLE, vasculitis, celiac disease, sarcoidosis, Sjögren syndrome, rheumatoid arthritis, monoclonal gammopathy
Toxins Heavy metals (lead, mercury, arsenic), organic solvents, acrylamide, marine and plant toxins
Medication Chemotherapeutic medication, TBC medication, anti-retrovirals, amiodarone, enalapril, statins, perhexiline, allopurinol, gold, hydroxychloroquine, metronidazole, nitrofurantoin
Other conditions
Alcoholism, idiopathy, trauma, compression, entrapment, syphilitic myelopathy, spinal stenosis, ALS, disk herniation, hyperlipidaemia, radiation, psychiatric/somatoform
HIV, Human immunodeficiency virus; CMV, Cytomegalovirus; GBS, Guillain–Barré syndrome; CIDP, Chronic inflammatory demyelinating polyradiculoneuropathy; SLE, Systemic lupus erythematosus; TBC, Tuberculosis; ALS, Amyotrophic lateral sclerosis

15
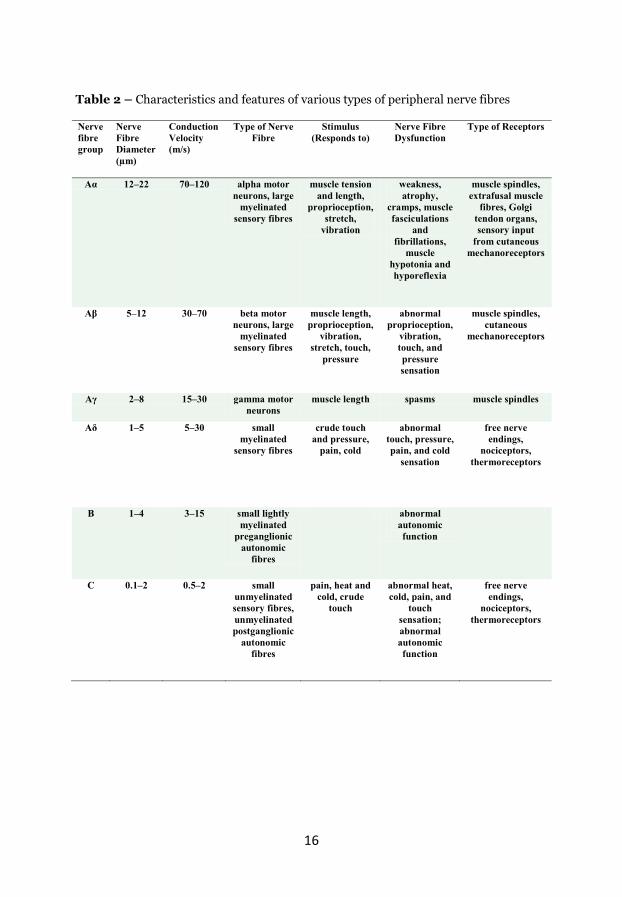
When studying peripheral neuropathy, it is important to have fundamental knowledge about the different nerve fibres that handle stimuli arising from the external and internal environments. In Table 2, the various types of nerve fibres and their corresponding receptors (group A, B, and C) are presented in more detail. There are primarily three systems of interest: 1) nerve fibres connecting sensory receptors on the body surface or deeper with the CNS, 2) nerve fibres linking the CNS and spinal cord to the skeletal muscles, and 3) nerve fibres that maintain and regulate autonomic and visceral functions. The varying architecture of these nerve fibres relates to their function of relaying information throughout the body [45]. This information is propagated with a conduction velocity ranging from less than 1 m/s to greater than 120 m/s. This varying conduction velocity can be partially explained by the degree of myelination of the nerve fibres. Greater myelination usually results in greater conduction velocity and vice versa. Traditionally, the nerve fibres of the PNS have been characterized as either unmyelinated or myelinated nerve fibres. Myelin is a membranous sheath consisting of lipids and proteins that wraps around the axons of nerve cells. In the CNS, this myelin sheath is produced by oligodendroglial cells whereas in the PNS it is produced by Schwann cells that support the neurons [33]. The main roles of the myelin sheath are to increase the velocity at which electrical nerve impulses propagate along the myelinated nerve fibre and to function as an insulator. In unmyelinated axons, which are also covered by the Schwann cell cytoplasm, the myelin sheath is absent. As the myelinated nerve fibres exit the CNS, they often become gradually less myelinated along their proximal to distal length and this phenomenon is not fully explained by the branching of nerve fibres. According to the Erlanger-Gasser classification system, nerve fibres can be categorized as A, B, or C based on their conduction velocities. The myelinated group A fibres are further sub-������������������������and ���[45]. Unmyelinated nerve fibres belong to group C, and these innervate pain and temperature receptors. All postganglionic autonomic nerve fibres are also considered to be unmyelinated and also belong to group C. Group B fibres are considered to be moderately myelinated – less than group A – and include mainly preganglionic autonomic nerve fibres. The term “free nerve endings” is sometimes used to denote the cutaneous endings ������������fibres.
16
Table 2 – Characteristics and features of various types of peripheral nerve fibres
Nerve fibre group
Nerve Fibre Diameter (μm)
Conduction Velocity (m/s)
Type of Nerve Fibre
Stimulus (Responds to)
Nerve Fibre Dysfunction
Type of Receptors
�� 12–22 70–120 alpha motor neurons, large
myelinated sensory fibres
muscle tension and length,
proprioception, stretch,
vibration
weakness, atrophy,
cramps, muscle fasciculations
and fibrillations,
muscle hypotonia and hyporeflexia
muscle spindles, extrafusal muscle
fibres, Golgi tendon organs, sensory input
from cutaneous mechanoreceptors
�� 5–12 30–70 beta motor neurons, large
myelinated sensory fibres
muscle length, proprioception,
vibration, stretch, touch,
pressure
abnormal proprioception,
vibration, touch, and pressure sensation
muscle spindles, cutaneous
mechanoreceptors
�� 2–8 15–30 gamma motor neurons
muscle length spasms muscle spindles
�� 1–5 5–30 small myelinated
sensory fibres
crude touch and pressure,
pain, cold
abnormal touch, pressure, pain, and cold
sensation
free nerve endings,
nociceptors, thermoreceptors
B 1–4 3–15 small lightly myelinated
preganglionic autonomic
fibres
abnormal autonomic function
C 0.1–2 0.5–2 small unmyelinated sensory fibres, unmyelinated postganglionic
autonomic fibres
pain, heat and cold, crude
touch
abnormal heat, cold, pain, and
touch sensation; abnormal autonomic function
free nerve endings,
nociceptors, thermoreceptors

17
Methods for assessing peripheral nerve function Quantitative Sensory Testing (QST) The term QST (quantitative sensory testing) usually refers to psychophysical methods or techniques in which specific sensory stimuli (temperature, vibration, pain) are delivered to various sites of the human body to trigger certain nerve fibre types and their nerve pathways. Generally, most QST methods are regarded as semi-objective meaning that only the stimuli can be measured and controlled accurately and the patient response to the stimuli are subjective: the patient reports both if and how often how they feel a given stimulus. QST methods are very patient-dependent, but, provided that the patient is alert, concentrating, and motivated, such methods are sensitive in detecting sensory nerve dysfunction [47, 50]. There is a range of devices that are included in the term QST. These include more simple semi-quantitative tools, such as the monofilament, the graduated tuning fork, and thermal rods and more complex handheld instrument such as the biothesiometer and vibrameter [46]. Even more sophisticated apparatus are available, usually found only in neurophysiological clinics and research laboratories, where most aspects of the QST are controlled, standardized, and predetermined. In more advanced QST methods, such as testing of temperature threshold, the stimuli can be delivered and applied either as methods of limits or as methods of levels [47]. A method of limits means that the stimulus intensity is increased by small steps until it reaches the limit of detection. This limit indicates the estimated sensory threshold. In methods of levels, an algorithm is used to apply stimuli with predefined intensities. An abnormal QST outcome only suggests sensory dysfunction in the sensory nerve pathway, and the actual pathological process can be anywhere from the receptor level to the brain cortex where the sensory experience is perceived. A range of peripheral nerve disorders can be assessed using QST techniques, and this lack of diagnostic specificity is often considered a shortcoming of QST. However, in patients with established or newly debuted peripheral nerve diseases, such as those with diabetic neuropathy or in cases of idiopathic neuropathy, QST techniques can be useful for assessing and monitoring their nerve function and disease progression [48]. Thus, QST provides evaluation of sensation, which has some clinical relevance, especially for the patient. Anthropometric factors, such as height, weight, age, and sex and the relative subjectivity of the methods can influence the results of QST [49]. The need for, and level of, standardization of the methods should be considered when interpreting and reproducing data, comparing data from different testing systems and apparatus, and when planning for follow-up studies [46, 47, 50-52].

18
Nerve conduction studies (NCS) The fact that external electrical stimulation can initiate a nerve impulse along peripheral nerve fibres is the basic principle behind nerve conduction studies (NCS) that can test the function of both sensory and motor nerves. Thus, NCS play a central role in the assessment of peripheral nerve diseases [57]. NCS are sometimes only part of a complete neurophysiological assessment that also includes a needle electromyogram that can differentiate between myopathic and neuropathic causes of diffuse muscle weakness and can distinguish between upper and lower motor neuron lesions. The basic components of NCS include assessment of motor and sensory nerve conduction velocities and amplitudes, distal latencies, and F-wave and H-reflex studies [57]. Standardized, reproducible, and properly conducted NCS can provide useful information regarding the localization and distribution of peripheral nerve dysfunction (mononeuropathy, mononeuropathy multiplex, or generalized polyneuropathy) and the presence and extent of sensory and motor deficits [58, 59]. Pathological changes in peripheral neuropathy due to diabetes mellitus are characterized by segmental demyelination, axonal degeneration, or a combination of the two [60, 61]. The amplitude reflects the number of conducting fibres and is reduced in conditions in which axons have been lost. The conduction velocity reflects the integrity of the myelin sheath that is important for impulse conduction, and the velocity is reduced when demyelination has occurred [57]. Conduction velocities can also be lowered due to extensive loss of large and fast conducting fibres. Thus, NCS can determine whether the peripheral nerve dysfunction is mainly due to axonal damage (axonal neuropathy) or if it involves the myelin (demyelinating neuropathy) or if it involves both. An important limitation is that NCS only assess large myelinated nerve fibres and overlook possible small nerve fibre dysfunction. Important physiological factors to take into consideration when performing NCS include limb temperature, height, age, proximal versus distal nerve segments, and anomalous innervation [62, 63]. Common non-physiological sources of errors often include technical difficulties with the stimulation systems and recording-related issues such as inaccurate surface measurements and electrode placement [62, 63]. Skin biopsies and intraepidermal nerve fibre density (IENFD) Several studies have demonstrated the implications and utility of immunohistochemical quantification of cutaneous nerves in the assessment of peripheral nerve disorders [64-67]. Using minimally invasive skin punch biopsies or skin blisters, one can study the most distal population of cutaneous nerves within the epidermis (C-fibres and ��-fibres) and can assess dermal innervation. Thus, intraepidermal nerve fibre quantification is useful for identifying the occurrence of sensory small nerve fibre changes. While standard NCS and many QST techniques and routine clinical tools predominantly assess large sensory and motor nerve fibres, the quantification of intraepidermal nerve fibres allows for assessment of early small nerve fibre dysfunction even prior to obvious symptoms and signs of neuropathy [68]. Although the application of skin biopsies and IENFD

19
quantification do not provide information about the aetiology of the neuropathy, a series of biopsies can be taken over time to monitor and follow disease progression and to observe possible regeneration from therapeutic interventions in both clinical practice and research settings. Interpretation of the results from a skin biopsy can be affected by variables such as anthropometric factors, biopsy artefacts, varying nerve counting protocols, biopsy section thickness, local trauma, and other diseases. Tests for autonomic neuropathy Due to the anatomical and physiological complexity of the autonomic nervous system (ANS), there are no simple tests that can easily and directly measure the function of the ANS and its end organs. This is in contrast to the readily available NCS and QST techniques for the assessment of somatosensory pathways. Autonomic neuropathy was not considered in this thesis, but there is a range of autonomic tests and methods that differ in sophistication and clinical usefulness [69]. These tests, only some of which will be briefly mentioned here, are usually based on indirect measurements of ANS end organ activity and function. With this in mind, it is important to understand that symptoms and signs that might be suggestive of autonomic dysfunction could be due to causes other than true neurogenic processes. Autonomic neuropathy testing includes neurophysiologic recording of secretory glands such as sweat gland function (sympathetic skin response), heart rate testing (heart rate variations upon deep breathing or Valsalva’s manoeuvre), testing of secretory gland output (lacrimal glands, salivary glands, or sweat glands), smooth muscle function (blood flow measurements and bladder and gut activity), and cardiovascular pressor response tests such as the tilt table test. Clinical scoring of neuropathy There are various scoring systems to quantitate the signs and symptoms of somatosensory disease and impairments. Scoring and evaluation of symptoms will not be focused on in this thesis. Instead, clinical signs are considered and described because signs are considered to be better predictors of peripheral neuropathy than symptoms [53]. Historically, the basic concept of scoring clinical neuropathic signs according to Dyck is to evaluate the overall severity of neuropathy by assessing sensation, muscle strength, and reflexes in a clinical setting [53]. Modified versions of Dyck’s original Neuropathy Disability Score (NDS; later renamed the Neuropathy Impairment Score (NIS)) have been developed and can be used to score the entire body or only specific areas such as the lower limb [55, 56]. The NDS grading usually considers modalities such as touch, vibration, pinprick, temperature, reflexes, muscle strength, and joint position (See Appendices B–D for the NDS protocol used in Papers II and III).

20
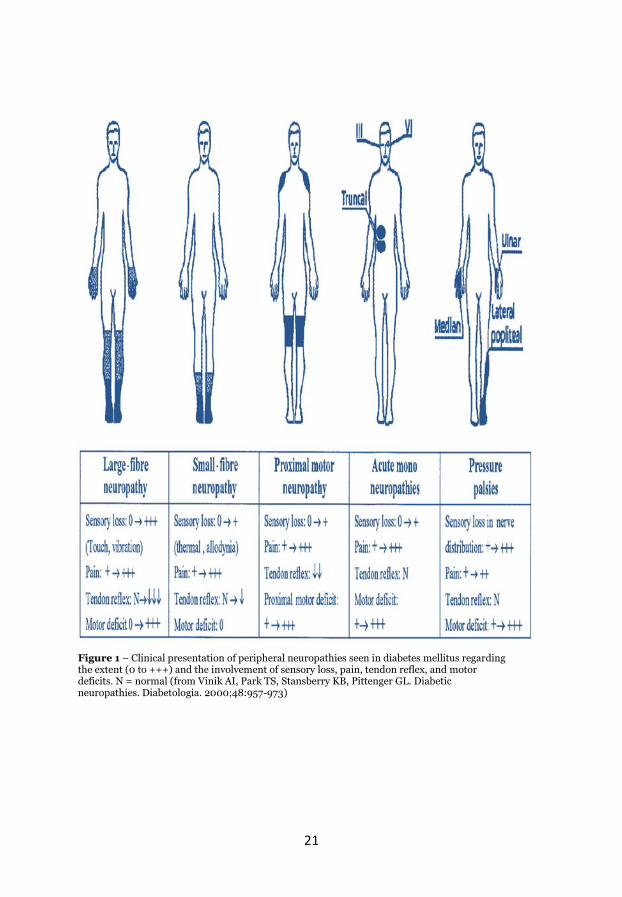
Symptoms and signs of diabetic neuropathy Common clinical patterns of peripheral neuropathies seen in diabetes mellitus are shown in Figure 1. Diabetic neuropathy can predominantly involve small or large diameter nerve fibres, but often affects both. The typical more common diabetic neuropathy also referred to as distal symmetric polyneuropathy (DSPN), is usually a combination of small and large nerve fibre dysfunction. Thus, the clinical manifestation of symptoms and signs of diabetic neuropathy depends on the topographic distribution, severity and functional selectivity. Examples of commonly encountered symptoms and signs of diabetic neuropathy are presented in Table 3. The clinical presentation often follows a sensory and motor length-dependent pattern usually starting in the lower extremities, but can involve upper extremities too as the neuropathy progress [70]. Some patients with diabetes have asymptomatic neuropathy [71, 72]. However, many patients can relate the onset of their symptoms to the presence and development of symmetrical paraesthesia and numbness of the feet, toes or sole [73, 74]. These symptoms can then advance further to proximal parts of the foot and ankle and. Patients can also describe sharp pain, lack of sensation and electric shocks [43, 75]. Some also develop increased sensitivity to pain (i.e. hyperalgesia) [76] and may also perceive painful sensation due to the stimulus that is normally not painful (i.e. allodynia) [77]. Motor symptoms are sometimes overlooked in clinical practice; especially since many patients with diabetes have subclinical neuropathy. Motor symptoms seen in clinical practice often include gait instability, tripping, cramps and weakness. In addition to greater risk of ulcerations and lower-extremity amputations, the quality of life of individuals with peripheral neuropathy is often affected, especially if pain symptoms are present.
21
Figure 1 – Clinical presentation of peripheral neuropathies seen in diabetes mellitus regarding the extent (0 to +++) and the involvement of sensory loss, pain, tendon reflex, and motor deficits. N = normal (from Vinik AI, Park TS, Stansberry KB, Pittenger GL. Diabetic neuropathies. Diabetologia. 2000;48:957-973)

22
Table 3 – Symptoms and signs of diabetic neuropathy
Common symptoms Common signs Autonomic symptoms and signs
Numbness, tingling sensation, and itching
Sensory loss to temperature, pinprick, and vibration
Dry mouth and eyes
Sharp pain, jabbing pain, and burning pain
Reduced or lost ankle reflex Difficulties adjusting to changes in light
“Electric shock” sensation and shooting pain
Toe extensor weakness Reduced or absent sweating
Gait imbalance and toe weakness Romberg sign Poor heat and cold tolerance
“Pins and needles” sensation Bowel and urinary incontinence
Typical late symptoms
Typical late signs
Erectile dysfunction
Proximal progression of sensory deficits
Further loss and proximal progression of temperature, pinprick, and vibration sensation and loss of proprioception
Lack of appropriate pulse rise
Worsening of neuropathic pain, myalgia, and cramps
Areflexia at ankle and knee level and foot drop
Abnormal blood pressure control
Worsening of gait and frequent tripping and falling
Impaired tandem and toe-and-heel walking and Charcot joints
Skin colour changes in hands and feet

23
Diagnostic criteria for peripheral neuropathy in diabetes mellitus The distal symmetric polyneuropathy (DSPN) that is commonly found in individuals with diabetes mellitus can be defined as the presence of symptoms and/or signs of peripheral nerve dysfunction after exclusion of other possible causes [53, 78]. It is important to realize that DSPN is mainly a clinical diagnosis and a thorough medical history, appropriate laboratory testing, and physical examination, including an accurate neurological examination, cannot be emphasized enough. With this in mind, the patients’ subjective description of their symptoms alone have relatively poor diagnostic value in predicting neuropathy and objective clinical signs are considered to be better predictors of neuropathy than symptoms [53]. However, recently published diagnostic criteria have proposed that a combination of signs and symptoms together with abnormal results in NCS provides an accurate diagnosis of DSPN [74]. DSPN can be defined according to published guidelines [16, 74, 78] and small nerve fibre measurements can be used when the results from NCS are normal. Basically, the presence of abnormal NCS and a sign(s) or symptom(s) of neuropathy confirms DSPN [16, 74, 78]. However, if valid criteria are not used then the results of these tests can be subject to bias by the investigating examiner or physician. Many individuals with predominantly small-fibre symptoms have normal electrophysiology and relatively normal neurological function. On the other hand, many individuals with DSPN have few if any symptoms but might present with many signs. Thus, one cannot define neuropathy purely on electrophysiology, particularly in a population where early clinical neuropathy could be associated with normal electrophysiology. In NCS, the nerve conduction velocity evaluates the condition of the best surviving large nerve fibres and the results might remain normal if even a few fibres are unaffected by a disease process. In other words, normal results from NCS could occur despite extensive nerve-fibre damage. However, decreasing amplitudes would be seen in such cases. Interpretation of NCS is highly context-specific, and thus correct clinical information will provide more useful results. IGT and peripheral neuropathy It has been debated whether peripheral neuropathy can develop in earlier stages of glucose dysmetabolism [7-10, 79], and IGT has frequently been identified in patients with idiopathic neuropathy [79-83]. Thus, a significant proportion of individuals with IGT might exhibit peripheral neuropathy [84-87]. However, whether neuropathy already exists in IGT or whether the IGT itself is the cause of neuropathy is debatable [7]. Still, IGT neuropathy has in general been considered to be milder compared to diabetic neuropathy. In one population-based study neuropathy was shown to be marginally increased in IGT than those with normal glucose tolerance but the measure of neuropathy was weighted toward large nerve fibres [85]. A recent large population-based study, however, showed no difference in measures of neuropathy between IGT and those with normal glucose tolerance (NGT) [88]. In that study, detailed measures of small nerve fibres were also not undertaken. Thus, in studies addressing the question of whether “IGT

24
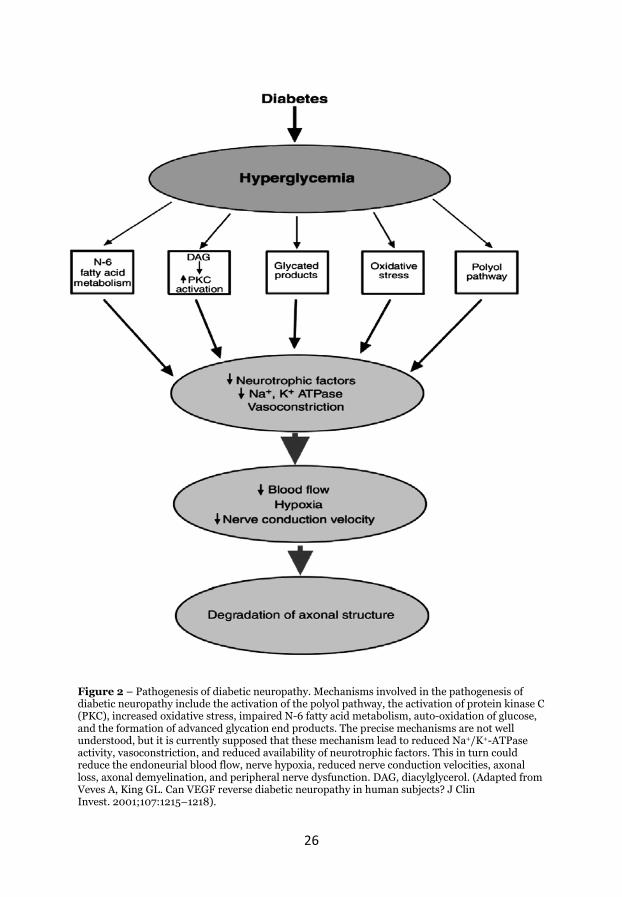
neuropathy” truly exists, objective measures of nerve dysfunction have frequently been crude and focused on large nerve fibres while ignoring small nerve fibre function. Treatment of diabetic neuropathy Several clinical trials involving aldose reductase inhibitors, nerve growth factor (NGF), and protein kinase C-���!"�-�# inhibitors have all failed to successfully alter the course of diabetic neuropathy suggesting that these compounds are not likely to be of clinical use in treating peripheral neuropathy associated with diabetes mellitus. Currently, the only treatments available to individuals with established diabetic neuropathy include glycaemic control and pain management. The positive effect of strict glucose control on peripheral neuropathy is well recognized although there are indications that this effect is considerably smaller in patients with T2DM [15-17] compared to those with T1DM [13, 14]. This is an important aspect for future development of disease-modifying therapies because many individuals with T2DM continue to develop peripheral neuropathy despite acceptable glucose control. Thus, development of therapies that focus on modifiable risk factors other than hyperglycaemia, such as dyslipidaemia, obesity, and hypertension, might be of value in light of the fact that T2DM is a growing disease and is affecting younger populations. There are various guidelines regarding the treatment of the pain component of peripheral neuropathy [89-92], but in general the recommended first line medications are pregabalin, gabapentin, tricyclic antidepressants, duloxetine, and venlafaxine. These are only measures intended to alleviate symptoms and improve quality of life. Titration to a tolerated maximum dose, switching to another first-line agent, or combination therapy are common approaches before considering second-line medications such as opioid analgesics and tramadol. It is important to evaluate effectiveness over time, possible comorbidities, side effects, and addiction potential when planning for what is often long-term use. Pathogenesis of diabetic neuropathy Multiple mechanisms and pathways have been implicated and identified in the pathogenesis of peripheral neuropathy associated with diabetes mellitus, i.e. diabetic neuropathy [11]. These include activation of the polyol pathway, the activation of PKC-�����$reased oxidative stress, impaired fatty acid metabolism, formation of advanced glycation end products (AGEs), and reduced availability of growth factors such as vascular endothelial growth factor (VEGF) and NGF [12]. In Figure 2, the main pathogenic pathways are outlined. Many of these mechanisms are based on animal studies and studies on cultured cells, but this section will mention mechanisms that have been reported from human studies.
Hyperglycaemia has long been regarded to be the main factor leading to a cascade of various mechanisms and pathways that result in nerve tissue damage [93]. However, it cannot be excluded that repeated hypoglycaemic episodes can also contribute to peripheral nerve dysfunction [94-96].

25
The polyol pathway leads to increased intracellular and extracellular sorbitol concentrations and increased concentrations of reactive oxygen species along with decreased concentrations of nitric oxide and glutathione, and this has been suggested to result in cell damage [97-102]. Another mechanism induced in diabetic neuropathy is the glycation process in which proteins, nucleotides, and lipids are glycated and form AGEs. These are thought to damage nerves and their micro-vessels [103-106]. Increased oxidative stress has also been implicated in the pathogenesis of human diabetic neuropathy [107, 108], and studies have shown regression of symptoms and signs after experimental treatment with antioxidants such as �-lipoic acid [109-113]. However, clinical trials involving aldose reductase inhibitors, NGF, and PKC-� inhibitors have all failed to successfully alter the course of diabetic neuropathy. Vascular disease is also involved in the pathogenesis of neuropathy in at-risk individuals such as those with diabetes mellitus [114-116], and metabolic perturbations, such as obesity and dyslipidaemia, appear to be important in the pathogenesis of human diabetic neuropathy [117-121]. It might be possible that defective neuroprotective pathways or reduced levels of neuroprotective factors could explain the progression of peripheral nerve dysfunction in diabetes mellitus. If this is true, then increasing neuroprotective factors in patients with diabetes mellitus might inhibit the development of peripheral neuropathy.
26
Figure 2 – Pathogenesis of diabetic neuropathy. Mechanisms involved in the pathogenesis of diabetic neuropathy include the activation of the polyol pathway, the activation of protein kinase C (PKC), increased oxidative stress, impaired N-6 fatty acid metabolism, auto-oxidation of glucose, and the formation of advanced glycation end products. The precise mechanisms are not well understood, but it is currently supposed that these mechanism lead to reduced Na+/K+-ATPase activity, vasoconstriction, and reduced availability of neurotrophic factors. This in turn could reduce the endoneurial blood flow, nerve hypoxia, reduced nerve conduction velocities, axonal loss, axonal demyelination, and peripheral nerve dysfunction. DAG, diacylglycerol. (Adapted from Veves A, King GL. Can VEGF reverse diabetic neuropathy in human subjects? J Clin Invest. 2001;107:1215–1218).

27
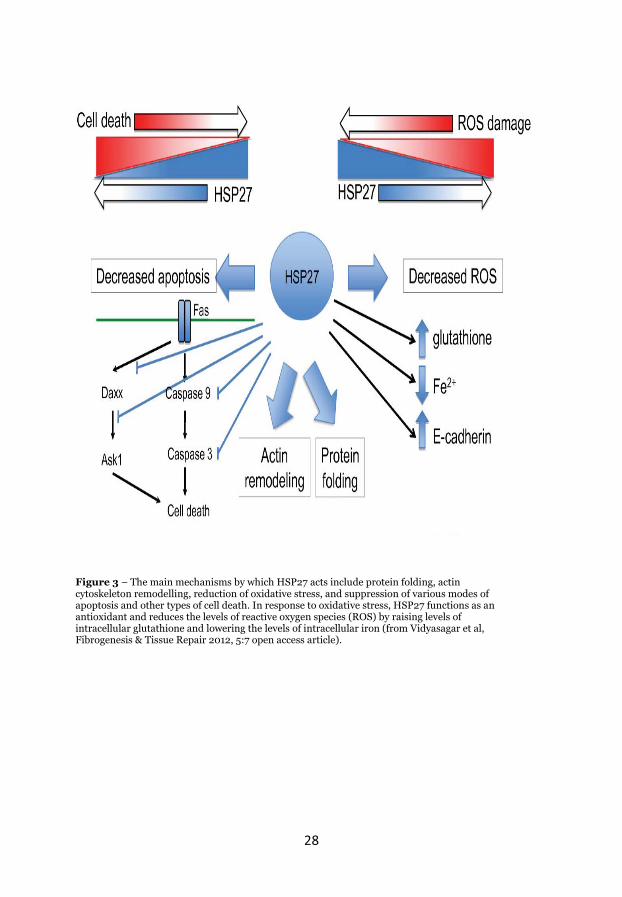
Heat shock protein 27 The heat shock protein family is associated with a range of functions that promote cell survival during times of cellular stress [18-22]. Heat shock protein 27 (HSP27 or HSPB1) appears to be generally cytoprotective by promoting cell survival through the stabilization of the actin filament cytoskeleton, the inhibition of apoptotic processes, the reduction of oxidative stress, and by functioning as a chaperone (Figure 3) [18, 122-124]. Induction of HSP27 has been observed in Schwann cells and in regenerating axons after nerve injury [125] as well as in the sensory neurons of the DRG [21, 126] in animal studies. HSP27 is constitutively produced in sensory and motor neurons as well as in the surrounding satellite cells [19, 20, 22, 127, 128]. It has been shown in animal models that experimental up-regulation of HSP27 is related to neuronal protection [129, 130] and that HSP27 is up-regulated after induction of acute nerve injuries [22, 131]. Studies in animal models have shown that overexpression of HSP27 results in protection from a range of sensory abnormalities [20] and upregulation of HSP27 has been related to neuronal protection [129]. Constitutive HSP27 overexpression in mice has been ��������������$���&��&���-cells) and to attenuate the effects of streptozotocin-induced diabetes mellitus [132]. In addition, mutations of the HSPB1 gene have been linked to hereditary neuropathies including variants of Charcot-Marie-Tooth disease [133, 134]. In humans, high concentration of serum HSP27 have been associated with peripheral neuropathy in patients with T1DM and this has been proposed to be a potential circulating marker for diabetic neuropathy [135]. However, the relationship between nerve function and circulating levels of HSP27 has not been studied in NGT individuals or in individuals with T2DM or IGT. In summary, peripheral neuropathy is a common complication observed among patients with diabetes mellitus. Whether peripheral neuropathy is evident in individuals with IGT is debatable and should be studied further. It is also important to better understand large and small nerve fibre function in order to identify and diagnose peripheral neuropathy. Thus, evaluation of diagnostic tools is needed along with investigations into the association between peripheral nerve function and HSP27 in humans.
28
Figure 3 – The main mechanisms by which HSP27 acts include protein folding, actin cytoskeleton remodelling, reduction of oxidative stress, and suppression of various modes of apoptosis and other types of cell death. In response to oxidative stress, HSP27 functions as an antioxidant and reduces the levels of reactive oxygen species (ROS) by raising levels of intracellular glutathione and lowering the levels of intracellular iron (from Vidyasagar et al, Fibrogenesis & Tissue Repair 2012, 5:7 open access article).
29
Aims Overall aim The overall aim of this thesis is to study the metabolic features and clinical assessment of peripheral nerve function and the relationship between HSP27 and peripheral nerve function. Specific aims:
�� To assess small and large nerve fibre function in NGT, IGT, and T2DM individuals.
�� To compare the diagnostic usefulness of the tuning fork, monofilament, biothesiometer, and quantification of IENFD in identifying small and large nerve fibre dysfunction in individuals with varying glucose metabolism.
�� To investigate the association between peripheral nerve function and
signs of neuropathy and HSP27 in individuals with different glycaemic statuses.
�� To study whether HSP27 concentrations differ between individuals with and without T1DM and to evaluate the relationship between the progression of peripheral nerve dysfunction and HSP27 concentrations.
30
Methods Study populations Västerbotten Intervention Programme Participants were recruited from the population-based Västerbotten Intervention Programme (VIP) [136]. In the VIP, all persons who turn 40, 50, or 60 years of age in Västerbotten County, Sweden, are invited to a health examination with the aim of reducing morbidity and mortality from cardiovascular diseases and diabetes mellitus. Individuals in the VIP who are identified with diabetes mellitus are invited to participate in a diabetes register (DiabNorth) [137]. NGT and IGT individuals from the VIP The study population for Papers I–III consists of NGT and IGT individuals from Skellefteå (a city in Västerbotten County in northern Sweden with a population of ~70 000 persons in 2003–2004) who were consecutively recruited in 2004 from the VIP. When the recruitment began, there were 508 and 74 possible NGT and IGT individuals from the VIP, respectively, living within Skellefteå. About 50 invitations were sent out simultaneously during each round of recruitment and the order of invitations was based on the patient’s participation date in the VIP that year. The postal invitations continued until the desired group size (n = 30) was met. Those who did not answer the first invitation were reminded once. T2DM individuals from primary health care centres Invitations were sent to primary health care centres within Skellefteå in order to recruit T2DM patients. About 600 individuals had T2DM in the Skellefteå region during the recruiting year 2003–2004. The diabetes nurse in each primary health care centre asked their T2DM patients at their yearly diabetes control appointments whether they wanted to participate in the neuropathy study. Oral glucose tolerance test for verification of glycaemic status The NGT and IGT individuals underwent two standardized oral glucose tolerance tests (OGTTs) after overnight fasting to verify their glucose status. The two tests were performed with about a week between tests and both OGTT results had to be within the cut-off values for fasting plasma glucose (fPG) and 2-hour plasma glucose (2hPG) according to the 1999 World Health Organization recommendations in order to be further included in the study. For NGT individuals, these cut-offs were fPG <7.0 mmol/L and 2hPG <8.9 mmol/L and for IGT individuals these cut-offs were fPG <7.0 mmol/L and ��!>�@ X�mmol/L and <12.2 mmol/L. In total, 129 individuals were included from which four withdrew, three were excluded due to nutritional deficiencies in vitamin B12, and three were excluded due to sciatica or stroke. This left 39 NGT, 29 IGT, and 51 T2DM individuals for the cross-sectional descriptive studies in Papers I–III.

31
Individuals with T1DM from the Diabetes Clinic in Malmö Paper IV is based on patients with T1DM who were treated in the Diabetes Clinic, Skåne University Hospital, Malmö, Sweden, and received their diagnosis between the ages of 15 and 25 years. In 1984–1985, 110 patients were registered at the clinic and all of them were asked to participate in a neuropathy study. Fifty-eight out of the 110 (53%) patients agreed to participate [138-141]. The patients were later asked to participate in a neuropathy study in 1992 with follow-up in 2005 (See Figure 4 for flow chart). In this thesis, clinical data and blood samples (n = 27) were obtained from 1992 (baseline) and from 2005 (follow-up).

32
Figure 4 – Flow chart of study population in Paper IV.

33
Laboratory investigation Papers I–III Blood samples were analysed for chronic alcoholism (gamma glutamyl transferase and carbohydrate deficient transferrin), thyroid disease (thyroid stimulation hormone and thyroid hormones T4 and T3), kidney and liver function (creatinine, albumin, ASAT, ALAT, ALP, and bilirubin), lipid status (LDL, HDL, total cholesterol, and triglycerides), electrolytes (sodium and potassium), and complete blood counts to rule out other possible causes of neuropathy, but we found no such cases. Paper IV Measurements were taken both at baseline and follow-up to exclude other causes of neuropathy. Blood samples were taken and analysed for renal, liver, and thyroid function, cholesterol levels, haemoglobin, cobalamine, folic acid, homocysteine, and lipids. In addition, a history of alcohol consumption was obtained. Besides one individual with severe vitamin B12 deficiency, no other causes of peripheral neuropathy were found. HbA1c concentrations were measured at baseline and follow-up. For HSP27 analysis, blood samples were obtained from 397 healthy blood donors from Malmö in 2004 who had no known cases of diabetes mellitus or cardiovascular disease. Heat shock protein 27 analyses Papers III and IV In both Papers III and IV, the Calbiochem® HSP27 ELISA Kit was used for the quantitative colorimetric determination of human HSP27 in serum (Calbiochem, San Diego, CA). A mouse anti-human HSP27 monoclonal antibody was pre-coated on the wells of a 96-well plate and served as the capturing antibody. HSP27 standard dilutions and samples were incubated in the pre-coated wells together with a rabbit polyclonal detection antibody specific for human HSP27. After the washing step, a goat anti-rabbit IgG horseradish peroxidase conjugate was added that bound to the polyclonal human HSP27 antibody. This was followed by the addition of substrate. The absorbance was read at 450 nm and HSP27 concentrations were determined by comparing the absorbance of samples with the values obtained from the standard curve. To determine the final amount of HSP27 in each sample, the concentrations derived from the standard curve were multiplied by a factor of 2 (to account for the dilution obtained by mixing equal volumes of standard/sample and 1× HSP27 detection antibody) and then multiplied by the initial dilution factor (×10). It must be noted that the HSP27 concentrations presented in Paper III were not multiplied by a factor 2 as was done in Paper IV. In Paper III, the inter- and intra-assay coefficients of variation were 10.4% and 10.6%, respectively. In Paper IV, the inter- and intra-assay coefficients of variation were 9.5% and 7%, respectively, for the healthy controls and 15% and 10%, respectively, for the T1DM patients.

34
Clinical assessment In Papers I–III, the participants’ height, weight, and blood pressure were measured, their BMI was calculated (kg/m2), and their medical histories and medications were scrutinized. In Paper IV, the duration of diabetes mellitus and the year of diagnosis were obtained and blood pressure, weight, and height were measured at baseline and at follow-up. In addition, any histories of renal disease, cardiovascular disease, medication, or smoking were recorded at baseline and follow-up. Nerve conduction studies In Papers I-III, an experienced neurophysiologist, who was blinded to the group identity of the participants, performed standardized motor and sensory NCS. The measurements were performed in the peroneal, tibial, and sural nerves of the right leg and the median and ulnar nerves of the right arm. In this thesis, only nerve attributes for the lower extremities were considered, including the motor conduction velocity, amplitude, and latency of the tibial and peroneal nerves, the sensory conduction velocity, amplitude, and latency of the sural nerve, and F-wave studies of the tibial and peroneal nerves. In Paper I, the conduction velocity of the peroneal nerve and conduction velocity and amplitude of the sural nerve were considered. In Paper II, the definition of neuropathy was based on NCS and clinical signs of neuropathy or, in cases where NCS were normal and there were clinical signs of neuropathy, on thermal thresholds as a measure of small nerve fibre function [53, 74, 78]. The neurophysiologist who performed the NCS considered and assessed the nerve attributes representative of neurophysiological abnormality in peripheral neuropathy and determined whether the participants had abnormal results from NCS or not (Paper II). In Paper III, a Z-score for each nerve measurement was calculated using the formula (Z-score = (individual value of participant Y mean value of control group (NGT individuals)) / (SD of mean value for the NGT group)). A composite Z-score for the leg, reflecting the nerve function in the leg, was calculated as ((Z-score conduction velocity peroneal nerve + Z-score conduction velocity sural nerve + Z-score amplitude sural nerve) / 3). The limb temperature was monitored prior to and during the recordings using a skin surface probe, and the limb temperature was maintained above 31 °C. In Paper IV, similar standardized NCS were performed and included the conduction velocity of the peroneal and sural nerves and the amplitude of the sural nerve in the right leg. Quantitative sensory testing In Paper II, the vibration perception threshold (VPT) was tested with a hand-held biothesiometer (Bio-Medical Instrument Co, ROVA Company Inc, Newbury, OH). The rubber tractor of the biothesiometer was balanced perpendicular to each test site with a constant and steady pressure while the individual was in a supine position on their back. The voltage was slowly increased at a rate of 1 V/s. When the individual indicated that a vibration was felt, the voltage at which this occurred was recorded as the VPT. Prior to the recordings, all individuals were familiarized with the biothesiometer and the rubber tractor was applied to the dorsal aspect of the hand as a reference

35
and for practice readings. The VPT was measured bilaterally at the prominent part of the medial malleolus and at the distal dorsal bony surface of both great toes. In Paper II, results from the right medial malleolus were used. Three rounds of VPT measurements were taken at each site and mean values were given. Thermal sensory testings were performed with the method of limits using Thermotest® equipment (Somedic AB, Hörby, Sweden). Thermal stimulations were applied bilaterally to the dorsum of both feet one at a time. By using the method of limits [47, 50, 51], the individuals were told to respond when they felt a noticeable thermal sensation (heat or cold). The starting temperature was 32 °C for both the heat and cold sensation measurements. The rate of temperature change was 1 °C/s and 10 stimulations were applied for each thermal sensation. The results were given as mean values ± 2 SD and the standard laboratory cut-off values (adjusted for age and sex) of 40.6 °C for heat and 26.7 °C for cold perceptions were used for delimiting pathological findings. Individuals with bilaterally abnormal values were considered to have a pathological outcome of the sensory testing. The limb temperature was kept above 31 °C. In Paper IV, a standardised method of determining VPT according to Goldberg and Lindblom [116] was performed with a Goldberg-Lindblom type vibrameter on the left great toe. Warm and cold perception thresholds were measured on the lateral side of the left foot using the Thermotest® equipment [143]. Clinical sensory test In Paper II, vibration perception was also tested with a 128 Hz tuning fork applied bilaterally to the medial malleolus. Absent or reduced perception on either malleoli was recorded (a normal reading was when the individual could distinguish between vibrating and not vibrating). The pressure/touch sensation was examined with a 10 gram monofilament (Gertab AB, Stockholm, Sweden) at three standard points – the plantar surface of the distal hallux and the 1st and 5th metatarsal heads – bilaterally on the sole of the foot [144]. Absence of sensation at one or more sites on either foot was recorded. A modified version [55, 56] of Dyck’s original NDS was used to evaluate signs of neuropathy (Papers II and III). Sensory perception, muscle strength, and reflexes in both arms and legs were evaluated by the NDS to quantify and grade the severity of neuropathy in the subjects. NDS data from the lower extremities were used in this thesis. Sensory perception (NDS-A) was tested by stimulating modalities of light touch (cotton wool), vibration (tuning fork), pinprick (needle), and temperature (cold metal item). The assessments were made on the dorsal aspect of the great toe, anterior foot, pretibial and medial malleoli, and the knee. Patellar and ankle reflexes (NDS-B) were evaluated together with muscle strength at the great toe, foot, and knee level (NDS-C). For NDS-A and NDS-B, normal findings were scored as 0, reduced reflexes or sensation as 1, and absent reflexes or sensation as 2. For NDS-C, normal findings were scored as 0, reduced muscle strength as 1, considerable reduction as 2, and paralysis as 3. NDS-A, NDS-B, and NDS-C were added together to give a composite NDS of the lower extremities (See Appendix B–D for the NDS-A-B-C protocol in Swedish).

36
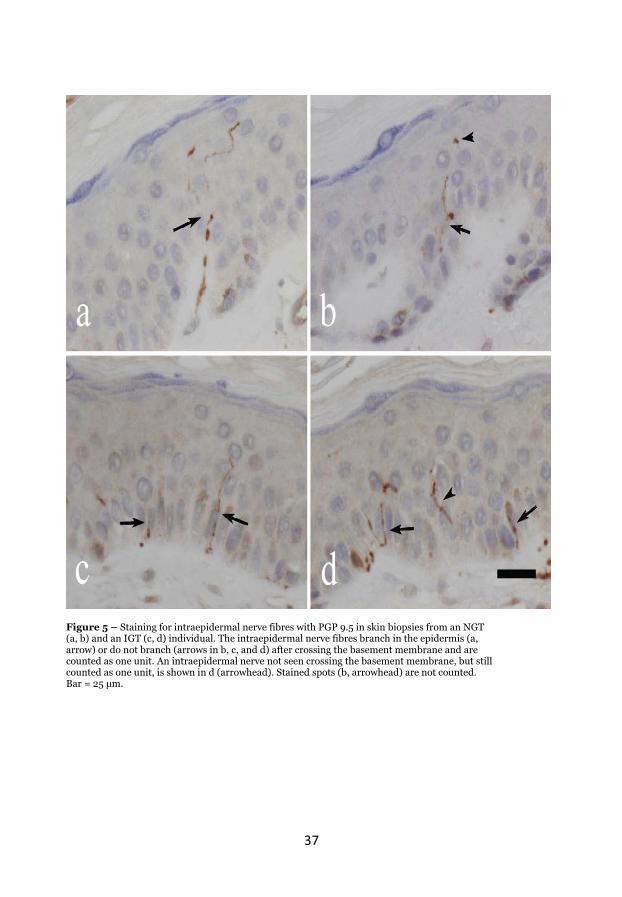
Skin biopsy and quantification of intraepidermal nerve fibre density Skin biopsies were performed, and published guidelines were considered [65]. During local anaesthesia, a punch skin biopsy was taken using a 3 mm disposable circular needle (Dermal Biopsy Punch; Miltex Inc., PA, USA). The site of the biopsy was at the lateral right leg approximately 10 cm proximal of the lateral malleolus. The procedure was well tolerated by the participants and without any complications. The biopsies were immediately fixed in 4% buffered formaldehyde solution at room temperature for 5 days, dehydrated, bi-partitioned with a central, parasagittal cut, and subsequently embedded in paraffin. Three sections, with a thickness of 5 μm and with a distance \�^��&$����&����_��`{, were obtained and mounted on positively charged glass slides for immunohistochemical staining. The sections were dewaxed, rehydrated, and microwave pre-treated in 10 mM citrate buffer to achieve antigen retrieval. Immunohistochemical staining was performed with the rabbit polyclonal antibody Protein Gen Product (PGP) 9.5 (Ultra Clone, Isle of Wright, England) at a 1:3000 dilution and an automated immunostainer (TechMate 500 Plus, Dako, Glostrup, Denmark). The histotechnical preparation and the subsequent microscopic assessment followed a protocol developed in 2004 [145] and later modified [146]. Two observers, both blinded to the identities of the participants, assessed all of the sections at the same time. One of the observers re-counted a random selection of 100 samples three months later and the intra-observer correlation (rs = 0.98) and the inter-observer correlation (rs = 0.84) were calculated. The biopsy length measurements and nerve fibre counting were performed manually using light microscopy (Olympus BX50; 40× magnification). Single intraepidermal nerve fibres visibly crossing the dermal-epidermal junction were counted, but subsequent secondary branching within the epidermis was not (Figure 5). In addition, well-defined isolated filamentous nerve fibres within the epidermis, but not clearly crossing the dermal-epidermal junction, were counted. Positively stained granular fragments within the epidermis were noted but were not counted. The method for quantification was slightly modified from a previous study on similar thin 5 μm sections [145, 146]. The IENFD was expressed as the number of fibres/mm of epidermal length, and the mean counts/mm in three sections were calculated.
37
Figure 5 – Staining for intraepidermal nerve fibres with PGP 9.5 in skin biopsies from an NGT (a, b) and an IGT (c, d) individual. The intraepidermal nerve fibres branch in the epidermis (a, arrow) or do not branch (arrows in b, c, and d) after crossing the basement membrane and are counted as one unit. An intraepidermal nerve not seen crossing the basement membrane, but still counted as one unit, is shown in d (arrowhead). Stained spots (b, arrowhead) are not counted. Bar = 25 `{
38
Statistical analyses In all papers, data are presented as numbers (n), proportions (%), or distribution as mean and standard deviation or median and interquartile range (IQR) if not stated otherwise. In Papers I-III, differences between groups were tested by ANOVA and subsequent Student’s t-test for normally distributed variables. For non-normally distributed variables, the Kruskal-Wallis test was applied with subsequent Mann-Whitney U-testing. Differences in proportions were tested using the Chi-square test and trends were tested with linear-by-linear associations. Pearson’s or Spearman’s correlation coefficient was used in bivariate correlation analysis between independent variables when appropriate. In Paper I, a 25% higher occurrence of peripheral neuropathy in IGT vs. NGT could be detected with a power of 80% (a priori) using the sample sizes that we chose. In Paper II, the dependent variable was the occurrence of neuropathy and receiver-operating characteristic (ROC) curves were produced where appropriate and the area under the curve (AUC) and optimal sensitivity and specificity were determined. In Paper III, for log-transformed variables (natural logarithm), differences between groups were tested with ANOVA and Dunnett’s post hoc analysis and are presented as geometric means (95% CI). In Paper III, initial univariate logistic regression analyses were performed. Multinomial logistic regression analyses were then used to determine the probabilities of the different possible outcomes of a categorically distributed dependent variable given a set of independent variables. Variables that were significantly associated (p <0.05) with the dependent variables in the univariate regression analyses were entered in a forward stepwise manner into the final multinomial logistic regression models. In Papers III and IV, HSP27 concentrations were non-normally distributed and presented as geometric means (95 % CI). In Paper IV, data that were normally distributed were tested for statistical significance using a paired samples t-test and data that were not normally distributed were tested using the Wilcoxon-paired signed rank test. Variables with non-normal distribution were also used after logarithmic transformation. In Paper IV, the dynamic change of HSP27 was given as delta-HSP27 (the baseline HSP27 measurement subtracted from the follow-up HSP27 measurement). Similarly, the delta value of the individual nerve fibre measures from the NCS and thermal and vibration threshold tests were calculated. The results from the nerve conduction studies and sensory threshold test in Paper IV were given as Z-scores, where laboratory reference data was used to standardise for sex, age and height of individual patients by calculating the Z-scores. A composite Z-score for large nerve fibre function was given as: (Z-score for sural conduction velocity + sural amplitude + peroneal conduction velocity)/3. Presence of abnormal nerve function was defined as values > 1.64 standard deviation (SD) below (conduction velocities and amplitude) or above (vibration and heat thresholds) the reference value. Statistical analyses were performed with IBM SPSS versions 18.0, 19.0, and 20.0 (SPSS Inc., Chicago, IL, USA). For further details, the reader is referred to the individual papers.

39
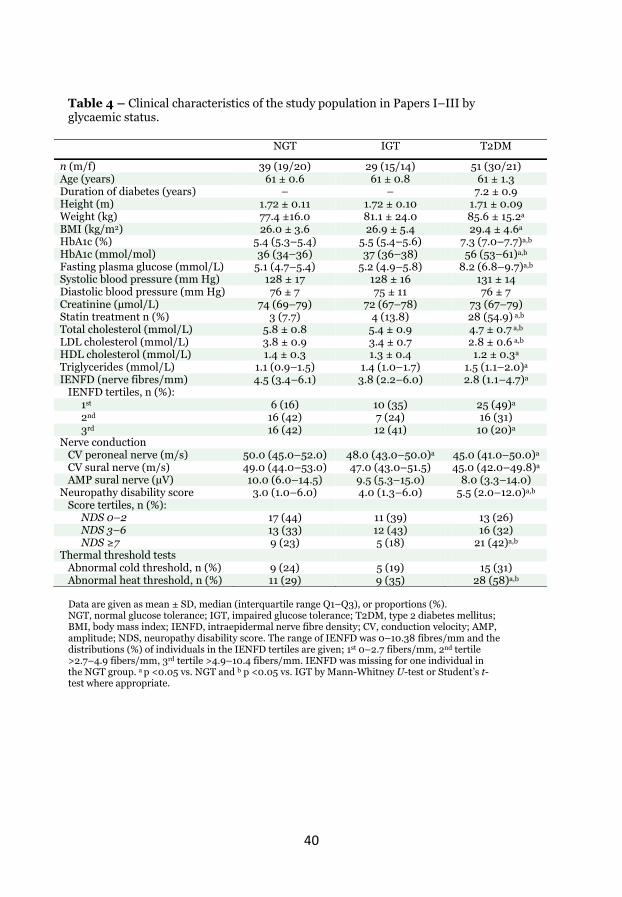
Results In this section, the main results from the individual papers are briefly presented in addition to results that were not included in the individual papers. Detailed data can be found in the individual papers. Paper I Peripheral nerve function in individuals with NGT, IGT, and T2DM Sural nerve conduction and amplitude did not differ between IGT and NGT individuals, but IGT individuals had lower conduction velocities of the peroneal nerve than those with NGT. The conduction velocities of the peroneal and sural nerve were lower in T2DM compared with NGT individuals but were still within normal reference values. There were no differences in temperature thresholds or IENFD between IGT and NGT individuals. The proportion of abnormal heat thresholds was significantly higher in individuals with T2DM than NGT and IGT. IENFD was significantly lower in T2DM patients compared with NGT individuals, and men had lower IENFD than women. Clinical characteristics of the NGT, IGT, and T2DM individuals are shown in Table 4. Additional results: Clinical neuropathy and IENFD A total of six individuals in the NGT group had abnormal results from NCS. Furthermore, there were a number of NGT individuals (n = 9, 23%) who had apparent signs of neuropathy (NDS >6) of which three also had abnormal results from NCS. Individuals (n = 18) with no signs of clinical neuropathy (NDS = 0 and normal results from NCS) were compared with a group of individuals (n = 13) with evident neuropathic affliction (NDS>6 and abnormal results from NCS). Individuals with no sign of neuropathy had significantly higher IENFD (median 5.67 fibres/mm, IQR 4.23–7.10 fibres/mm) than individuals with evident neuropathy (median 0.93 fibres/mm, IQR 0.00–2.63 fibres/mm, p = 0.001). Body weight was independently negatively associated with IENFD after adjustment for sex, height, glucose levels, HDL cholesterol, triglycerides, blood pressure, and &����������{����� = Y0.30, p = 0.017).
40
Table 4 – Clinical characteristics of the study population in Papers I–III by glycaemic status.
NGT IGT T2DM
n (m/f) 39 (19/20) 29 (15/14) 51 (30/21) Age (years) 61 ± 0.6 61 ± 0.8 61 ± 1.3 Duration of diabetes (years) – – 7.2 ± 0.9 Height (m) 1.72 ± 0.11 1.72 ± 0.10 1.71 ± 0.09 Weight (kg) 77.4 ±16.0 81.1 ± 24.0 85.6 ± 15.2a
BMI (kg/m2) 26.0 ± 3.6 26.9 ± 5.4 29.4 ± 4.6a HbA1c (%) 5.4 (5.3–5.4) 5.5 (5.4–5.6) 7.3 (7.0–7.7)a,b HbA1c (mmol/mol) 36 (34–36) 37 (36–38) 56 (53–61)a,b Fasting plasma glucose (mmol/L) 5.1 (4.7–5.4) 5.2 (4.9–5.8) 8.2 (6.8–9.7)a,b
Systolic blood pressure (mm Hg) 128 ± 17 128 ± 16 131 ± 14 Diastolic blood pressure (mm Hg) 76 ± 7 75 ± 11 76 ± 7 Creatinine (μmol/L) 74 (69–79) 72 (67–78) 73 (67–79) Statin treatment n (%) 3 (7.7) 4 (13.8) 28 (54.9) a,b Total cholesterol (mmol/L) 5.8 ± 0.8 5.4 ± 0.9 4.7 ± 0.7 a,b
LDL cholesterol (mmol/L) 3.8 ± 0.9 3.4 ± 0.7 2.8 ± 0.6 a,b
HDL cholesterol (mmol/L) 1.4 ± 0.3 1.3 ± 0.4 1.2 ± 0.3a
Triglycerides (mmol/L) 1.1 (0.9–1.5) 1.4 (1.0–1.7) 1.5 (1.1–2.0)a
IENFD (nerve fibres/mm) 4.5 (3.4–6.1) 3.8 (2.2–6.0) 2.8 (1.1–4.7)a
IENFD tertiles, n (%): 1st 6 (16) 10 (35) 25 (49)a
2nd 16 (42) 7 (24) 16 (31) 3rd 16 (42) 12 (41) 10 (20)a
Nerve conduction CV peroneal nerve (m/s) 50.0 (45.0–52.0) 48.0 (43.0–50.0)a 45.0 (41.0–50.0)a CV sural nerve (m/s) 49.0 (44.0–53.0) 47.0 (43.0–51.5) 45.0 (42.0–49.8)a AMP sural nerve (μV) 10.0 (6.0–14.5) 9.5 (5.3–15.0) 8.0 (3.3–14.0) Neuropathy disability score 3.0 (1.0–6.0) 4.0 (1.3–6.0) 5.5 (2.0–12.0)a,b Score tertiles, n (%): NDS 0–2 17 (44) 11 (39) 13 (26) NDS 3–6 13 (33) 12 (43) 16 (32) NDS 7 9 (23) 5 (18) 21 (42)a,b Thermal threshold tests Abnormal cold threshold, n (%) 9 (24) 5 (19) 15 (31) Abnormal heat threshold, n (%) 11 (29) 9 (35) 28 (58)a,b
Data are given as mean ± SD, median (interquartile range Q1–Q3), or proportions (%). NGT, normal glucose tolerance; IGT, impaired glucose tolerance; T2DM, type 2 diabetes mellitus; BMI, body mass index; IENFD, intraepidermal nerve fibre density; CV, conduction velocity; AMP, amplitude; NDS, neuropathy disability score. The range of IENFD was 0–10.38 fibres/mm and the distributions (%) of individuals in the IENFD tertiles are given; 1st 0–2.7 fibers/mm, 2nd tertile >2.7–4.9 fibers/mm, 3rd tertile >4.9–10.4 fibers/mm. IENFD was missing for one individual in the NGT group. a p <0.05 vs. NGT and b p <0.05 vs. IGT by Mann-Whitney U-test or Student’s t-test where appropriate.

41
Paper II Occurrence of peripheral neuropathy in NGT, IGT, and T2DM Twenty-two individuals (18%) were considered to have confirmed DSPN in the whole group, i.e. these individuals had abnormal NCS results and signs of neuropathy. Out of these 22 individuals, 17 had also abnormal thermal thresholds. In a subset of individuals, we observed 27 (23%) individuals with signs of small nerve fibre neuropathy (sDSPN), i.e. these individuals had normal results from the NCS but abnormal thermal thresholds together with signs of neuropathy. In individuals with NGT, the occurrence of DSPN and sDSPN was 16% and 13%, respectively. In the IGT group, the frequency of DSPN (12%) was lower compared to that of sDSPN (32%). Individuals with T2DM had an occurrence of 28% and 30% for DSPN and sDSPN, respectively. The prevalence of DSPN and sDSPN were not significantly different between NGT and IGT individuals (Table 5). � Table 5 – Prevalence of DSPN and sDSPN according to glycaemic status NGT
n = 39a IGT n = 29
T2DM n = 51
No DSPN/sDSPN, n (%) 27 (71) 14 (56) 20 (42)
sDSPN, n (%) 5 (13) 8 (32) 14 (30)
DSPN, n (%) 6 (16) 3 (12) 13 (28)
NGT, normal glucose tolerance; IGT, impaired glucose tolerance; T2DM, type 2 diabetes mellitus; DSPN, distal symmetric polyneuropathy; sDSPN, small nerve fibre predominate distal symmetric polyneuropathy. a Prevalence in NGT, IGT and T2DM are presented. One NGT, four IGT, and four T2DM individuals had a missing NDS or NCS/thermal threshold. Bold indicates significant difference from the other two groups.
42
Utility of methods for assessing DSPN The biothesiometer had a sensitivity of 82% and a specificity of 72% in identifying DSPN individuals (a cut-�������������� ����������{�����malleolus was determined via the ROC curve). The 128 Hz tuning fork was a relatively accurate method for identifying DSPN in terms of both sensitivity (77%) and specificity (67%). In individuals with confirmed DSPN, the ROC curve for the IENFD showed an almost equally high AUC as the biothesiometer with a sensitivity of 73% and specificity of 80% at an IENFD cut-off of �� X����\�&�{{ ���������of these methods overlapped in 12 out of 22 DSPN cases, and the combination of the tuning fork with the biothesiometer identified all but one of the DSPN cases. Adding quantification of IENFD to this combination did not increase the sensitivity of detecting DSPN. Utility of methods for assessing sDSPN For sDSPN, the tuning fork had a lower sensitivity (44%) but the same specificity (67%) when compared to identification of DSPN cases. For the biothesiometer, a cut-�������������� �����&����������&�&������������specificity of only 67% and 59%, respectively. For the skin biopsy method, an IENFD cut-��������� �X���\�&�{{�������&�&���������������������&�$���$����of 74%. These three methods overlapped in 7 out of 27 sDSPN cases. By adding quantification of IENFD to the combination of tuning fork and biothesiometer, the sensitivity of finding sDSPN increased from 81% to 93%. See Table 6 for further data regarding the usefulness of these methods. The monofilament The 10 g monofilament in combination with the other methods did not provide additional diagnostic usefulness in detecting peripheral neuropathy. The 10 g monofilament had a low sensitivity but a high specificity for detecting both DSPN and sDSPN. Two individuals with DSPN and one with sDSPN had abnormal monofilament outcomes. Two non-neuropathy individuals had abnormal monofilament outcomes.
43
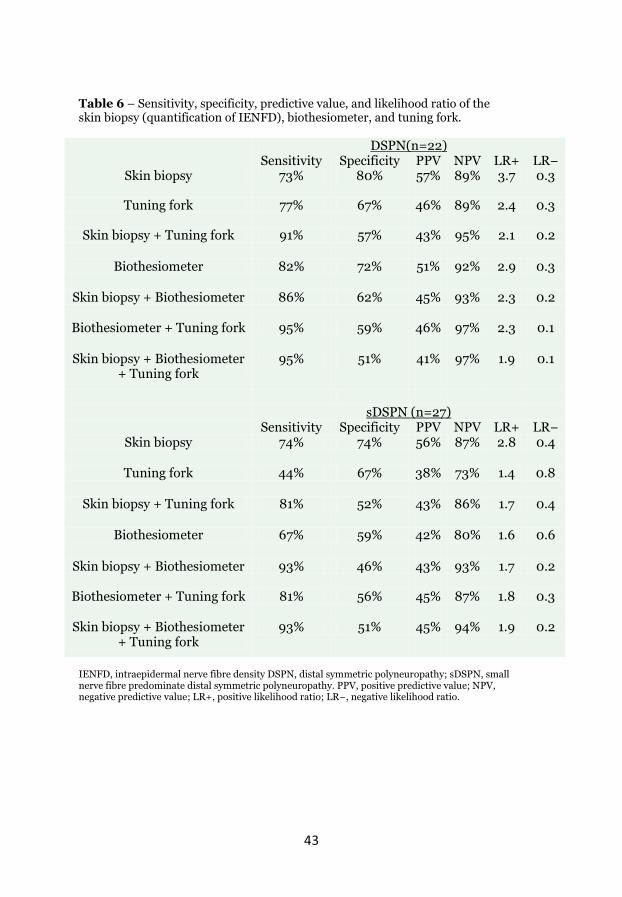
Table 6 – Sensitivity, specificity, predictive value, and likelihood ratio of the skin biopsy (quantification of IENFD), biothesiometer, and tuning fork.
DSPN(n=22) Sensitivity Specificity PPV NPV LR+ LRY
Skin biopsy 73% 80% 57% 89% 3.7 0.3
Tuning fork 77% 67% 46% 89% 2.4 0.3
Skin biopsy + Tuning fork 91% 57% 43% 95% 2.1 0.2
Biothesiometer 82% 72% 51% 92% 2.9 0.3
Skin biopsy + Biothesiometer 86% 62% 45% 93% 2.3 0.2
Biothesiometer + Tuning fork 95% 59% 46% 97% 2.3 0.1
Skin biopsy + Biothesiometer + Tuning fork
95% 51% 41% 97% 1.9 0.1
sDSPN (n=27) Sensitivity Specificity PPV NPV LR+ ��Y
Skin biopsy 74% 74% 56% 87% 2.8 0.4
Tuning fork 44% 67% 38% 73% 1.4 0.8
Skin biopsy + Tuning fork 81% 52% 43% 86% 1.7 0.4
Biothesiometer 67% 59% 42% 80% 1.6 0.6
Skin biopsy + Biothesiometer 93% 46% 43% 93% 1.7 0.2
Biothesiometer + Tuning fork 81% 56% 45% 87% 1.8 0.3
Skin biopsy + Biothesiometer + Tuning fork
93% 51% 45% 94% 1.9 0.2
IENFD, intraepidermal nerve fibre density DSPN, distal symmetric polyneuropathy; sDSPN, small nerve fibre predominate distal symmetric polyneuropathy. PPV, positive predictive value; NPV, negative predictive value; LR+, positive likelihood ratio; LRY, negative likelihood ratio.

44
Paper III HSP27 in relation to peripheral nerve function and glucose metabolism In Paper III, individuals with better large nerve fibre function in the leg had significantly higher HSP27 concentrations than individuals with relatively worse nerve function. Similarly, individuals with few neuropathic signs had significantly higher HSP27 concentrations than individuals with many neuropathic signs (geometric mean HSP27 401 pg/ml, 95% CI 310–520 vs. 192 pg/ml, 95% CI 128–288) p = 0.007). Individuals with good nerve conduction in combination with few signs of neuropathy had significantly higher HSP27 concentrations than those with poorer nerve conduction and many neuropathic signs (geometric mean sHSP27 443 pg/ml, 95% CI 338–580 vs. 207 pg/ml, 95% CI 126–337, p = 0.048). HSP27 concentrations were significantly associated with better large nerve fibre function after adjustment for age, sex, height, and weight and were not attenuated by inclusion of HbA1c. Similarly, using tertiles of HSP27 as the dependent variable revealed that better large nerve fibre function was associated with high HSP27 concentrations after adjustment for statin medication, age, and sex and this association was not attenuated after adjustment for HbA1c (Odds ratio = 2.51, 95% CI 1.25–5.05, p <0.05). HSP27 concentrations in T2DM individuals were significantly lower than in those with IGT and NGT. Correlation analysis revealed that HSP27 concentrations were ���������$��������^�������������Y� ��#�������&�������$��������with composite Z-score in the leg (r = 0.23), amplitude of the sural nerve (r = 0.22), and conduction velocity of the peroneal nerve (r = 0.18) (p <0.05 for all results). However, HSP27 did not correlate with measures of small nerve fibre function such as heat and cold perception thresholds or IENFD. Paper IV HSP27 and peripheral nerve function in T1DM The healthy non-diabetic controls had higher HSP27 concentration (geometric mean = 785 pg/mL, 95% CI 732–842) than T1DM individuals (baseline: 547 pg/mL, 95% CI 421–711; follow-up: 538 pg/mL, 95% CI 417–693, p <0.05 for both comparisons). The conduction velocity of the peroneal nerve was significantly lower at follow-up (Z-score = Y3.28, IQR Y10.27 to Y2.02) than at baseline (Z-score = Y2.3, IQR Y4.1 to Y1.1, p <0.005). In addition, both vibration and heat perception thresholds deteriorated over time in the T1DM patients. The combined measure of sural and peroneal nerve function was worse at follow-up (composite Z-score = Y2.42, IQR Y4.32 to Y1.32) than at baseline (composite Z-score = Y1.79, IQR Y2.51 to Y1.00, p <0.005). Deteriorating large nerve fibre function correlated with a decrease in HSP27 concentrations over time in T1DM patients (r = 0.50, p = 0.01). Comparison of HSP27 concentrations Note that in Papers III and IV, HSP27 concentrations are presented as geometric means (95% CI). In addition, the HSP27 concentration in Paper III must be multiplied by a factor of 2 in order to be comparable to HSP27

45
concentrations in Paper IV (for more details see the Methods section in this thesis regarding HSP27 quantification). The geometric means for HSP27 concentrations were similar in non-diabetic controls in both Paper III and IV (geometric mean = 722 pg/mL, 95% CI 564–922 pg/mL in Paper III compared to 785 pg/mL, 95% CI 732–842 pg/mL in Paper IV). T2DM individuals in Paper III had lower HSP27 concentrations (geometric mean = 412 pg/mL, 95% CI 284–598 pg/mL) compared to T1DM patients in Paper IV (geometric mean = 547 pg/mL, 95% CI 421–711 (baseline) and 538 pg/mL, 95% CI 417–693 pg/mL (follow-up)).

46
General discussion This thesis has shown that measures of large and small nerve fibre function do not differ significantly between IGT and NGT individuals. The use of a biothesiometer in routine clinical practice appears to be a useful, sensitive and non-invasive method to identify peripheral nerve dysfunction. In addition, quantification of IENFD using skin biopsies in combination with methods measuring vibrotactile sense, such as the biothesiometer, increase the diagnostic usefulness of this method for identifying peripheral nerve dysfunction. Moreover, high concentrations of HSP27 are associated with better large nerve fibre function regardless of glycaemic status, and deteriorating large nerve fibre function in the lower extremities correlates with a decrease in HSP27 concentrations over time. Neuropathy in prediabetes or prediabetes in neuropathy? The possibility of neuropathy preceding the onset of diabetes mellitus was first addressed in the 1950s [147], and it is now well known that one of the most common causes of neuropathy globally is diabetes mellitus [3]. IGT, being a state of intermediate hyperglycaemia, usually precedes the onset of diabetes mellitus, and, therefore, it has been reasonable to investigate whether IGT can result in neuropathy as well. In this thesis, attempts were made to study a population-based cohort and to take measures of large and small nerve fibre function in order to address the question of whether the peripheral nerve function in IGT is considerably worse than individuals with NGT. A great number of studies have been published over the past years investigating the possible association between peripheral neuropathy and IGT [79, 80, 84-88, 121, 148-152]. Still, at the present time there remains considerable debate as to whether “IGT neuropathy” or prediabetic neuropathy truly exists [7, 8]. Various studies have shown that a great number of individuals with idiopathic neuropathy have IGT [79-83], and conversely a great number of those with IGT have neuropathy [84-87]. It has been suggested that small nerve fibres, those responsible for temperature and pain perception, are predominantly affected in IGT-associated neuropathy [79, 81, 117, 153], and this is supported by the present findings. However, one could question whether a retrospective study design might be less appropriate for ascribing IGT as a potential cause of neuropathy. One large study by Franklin et al. reported a higher frequency of neuropathy in IGT individuals compared to controls [84]. The definition and diagnosis of neuropathy in that study was based on physical examination, a focused history, and was validated by tests of vibrotactile thresholds in the legs and, therefore, only assessed large nerve fibres. However, the San Luis Valley study by Franklin et al. was a large, randomly assessed population-based epidemiological study [84]. Thus, even with the caveat that it was large nerve fibre weighted, the San Luis study found an increased prevalence of neuropathy in subjects with IGT using insensitive methods and, therefore, may have underestimated the true prevalence of neuropathy. Moreover, the

47
population-based study by Ziegler et al. assessed neuropathy in IGT and NGT individuals and showed it to be increased marginally in those with IGT [85], but, again, the measure of neuropathy was crude and weighted toward large nerve fibres. A recent large population-based study from Rochester by Dyck et al. [88] challenged these previous studies because it showed no difference in measures of neuropathy between IGT and NGT individuals. However, one of the flaws of that study was that detailed measures of small fibre neuropathy were not undertaken. Even though increased frequencies of neuropathy in IGT have been reported, two prospective studies could not find any support for an association with IGT in neuropathic patients [121, 151]. Another study reported that having IGT for at least 12–15 years was not associated with peripheral nerve dysfunction [149]. Thus, there are indications from the literature that cast doubt on the existence of peripheral neuropathy as a consequence of IGT. The findings in this thesis indicate that measures of large and small nerve fibre function do not differ between IGT and NGT individuals. Even though the peroneal nerve conduction velocity was significantly reduced in IGT compared to NGT individuals in Paper I, the sural nerve conduction, IENFD, and thermal thresholds showed no differences. In fact, the sural and peroneal nerve conductions were all within the normal range for the age group (Paper I). Thus the conclusion from the work in this thesis is that the existence of clinical neuropathy as a consequence of IGT per se seems unlikely and is not supported by this thesis. One can argue, of course, that there are limitations to the studies in this thesis, and these will be discussed later. Peripheral neuropathy has also been linked to dyslipidaemia and the metabolic syndrome [117-121], and this thesis showed that body weight was associated with reduced IENFD as a measure of small nerve fibre function. However, others have reported no correlation of weight with IENFD [64, 154]. Possible explanations for these diverging results might be the fact that the diabetes mellitus population in the previous study consisted of both T1DM and T2DM patients of different ages and with relatively short mean disease durations of around 4.5 years [154]. The well-defined population of NGT, IGT, and T2DM individuals in this thesis were all of the same age and with the mean duration of T2DM of 7.2 years. Increased body weight might lead to secondary changes, such as perturbations in circulating triglycerides and free fatty acids that in turn might have a negative impact on nerve fibres [118, 155, 156]. Obesity has been shown to directly result in neural pathology, perhaps through mechanisms involving structural and functional changes in the neural microvasculature [157, 158]. The proportion of the T2DM patients with BMI <25 kg/m2 in this thesis (10%) was less than in the Swedish NDR (20%), which represents the general diabetes mellitus population. In addition, one could speculate that overweight individuals, due to having a greater body volume, have a reduced IENFD because the nerve endings have

48
a larger surface area to cover. The clinical significance of this observation is unclear. This thesis suggests that the glycaemic status of IGT individuals per se does not cause peripheral neuropathy. Thus, there might be factors other than hyperglycaemia that are involved in the development of peripheral neuropathy. For example, the NGT and IGT individuals in this thesis had almost similar BMIs. Therefore, the association between IENFD and body weight might be important from a preventive point of view, and weight reduction in obese persons might reduce the incidence of neuropathy. In addition, increased body weight as an independent contributor to peripheral nerve dysfunction, as suggested by this thesis, might provide new approaches when developing disease-modifying treatments aiming to prevent and halt the development of diabetic neuropathy. Comparison of clinical tools and their use in detecting peripheral neuropathy Others have compared the tuning fork with a biothesiometer and concluded that the tuning fork alone was a reliable method of detecting neuropathy [159]. Moreover, VPT has been reported to be a sensitive measure of confirmed clinical neuropathy in T1DM [160]. However, nerve conduction abnormalities were included in the definition of neuropathy [160] and patients with small nerve fibre neuropathy might have been excluded. Moreover, it has been suggested that assessing vibrotactile perception with a biothesiometer is a sensitive method for screening individuals with neuropathy who are at risk of developing foot complications and that this method might even better than the 10 g monofilament [161]. Using the tuning fork for screening purposes proved to be a reliable method and was better than the 10 g monofilament [162] perhaps due to the fact that different anatomical sites were tested. The combination of the 10 g monofilament and 128 Hz tuning fork did not improve the sensitivity and specificity of identifying neuropathy defined by NCS [163], a finding that is confirmed by this thesis. In addition, it has been reported that the 2 g monofilament was better than the 10 g monofilament as a useful diagnostic test for DSPN [164], and a recent study on peripheral neuropathy in T2DM using von Frey’s hairs instead of the common 10 g monofilament showed that the sensitivity of von Frey’s hairs with respect to the occurrence of confirmed neuropathy (defined as clinical neuropathy and abnormal NCS) ranged from 38% to 85% and the &�$��$����ranged from 62% to 85% [165]. In another recent study, diabetes mellitus was found to be associated with an increased risk of peripheral neuropathy defined by monofilament insensitivity (one or more insensate sites of three sites tested per foot), but individuals with prediabetes showed only a slight increase in risk [144]. Others have reported that the prevalence o��{������{�����&�&������������peripheral neuropathy symptoms did not differ between NGT and IFG individuals [199]. One could argue that a graded Rydell-Sieffer tuning fork, which eliminates the observer’s perception of normal and abnormal by quantitating vibration and using age normalization, is a better alternative than a standard 128 Hz

49
tuning fork. Similarly, biothesiometry is a well-defined clinical tool that is most often used for the identification of the foot most at risk of ulceration as a consequence of neuropathy. This thesis showed that the use of a biothesiometer in routine clinical practice might be a sensitive method to identify and quantify large nerve fibre neuropathy in the lower extremities. In addition, quantification of IENFD in combination with methods measuring vibrotactile sense, such as the biothesiometer, increased the diagnostic sensitivity of detecting peripheral neuropathy prior to the large nerve fibre abnormalities that are detectable by NCS. Evaluation of vibrotactile sense can take a multi-frequency approach, and recent data indicate that frequencies lower than 128 Hz might be more sensitive for detecting large fibre neuropathy [166]. Interestingly, different frequencies correlated with the results from monofilament testing using a kit with 20 different monofilaments [166]. The 10 g monofilament assessment used in this thesis does not appear to be useful in identifying peripheral nerve dysfunction, and a range of monofilaments would perhaps have been more appropriate [166]. In clinical settings, such as primary health care centres, electrophysiological tests are not always available and routine methods (e.g. tuning fork, monofilament) do not detect small nerve fibre dysfunction. In such cases, a biothesiometer or even a multi-frequency tactilometer and skin biopsies would be useful alternatives. This thesis showed that quantification of IENFD in combination with measures of vibrotactile sense such as the biothesiometer and the 128 Hz tuning fork increased the diagnostic usefulness for identifying peripheral nerve dysfunction, in particular small nerve fibre neuropathy. However, the skin biopsy method is an invasive procedure and it would be challenging to introduce skin biopsies in routine clinical practice as a clinical tool. Quantifying IENFD could, however, be suitable in cases where one wants to correctly diagnose small nerve fibre neuropathy in situations where NCS are normal or when aiming to distinguish small nerve fibre symptoms such as pain. Based on the results of this thesis, the use the biothesiometer appears to provide sufficient diagnostic performance to identify clinical neuropathy in routine health care, especially when combined with routine clinical tool such as the 128 Hz tuning fork. An obvious question is why we should want to accurately detect diabetic neuropathy when there are no widespread disease-modifying treatments available. I believe that introducing methods that can quantify perceptible modalities such as vibrotactile sense could make the patient more conscious of its disease and disease complications. Increased awareness of peripheral neuropathy in diabetes mellitus patients could prevent and delay the associated risks of developing ulcers in the lower extremities and subsequent amputation. Methods that correctly identify nerve fibre pathology could perhaps also be used to monitor clinical symptoms and signs as well as the efficacy of future therapies aiming to reverse the progression of diabetic neuropathy.

50
Insufficient neuroprotection in diabetes mellitus? Studies on diabetic rats have shown that apoptosis of sensory ganglion cells is a noticeable feature in the pathogenesis of diabetic neuropathy [167-169]. Thus, insufficient downstream effects of HSP27 on apoptotic pathways might explain the growing evidence that it is not just axonal damage that is significant in diabetic neuropathy but also cell death of DRG neurons [11, 155]. As indicated in this thesis, HSP27 could serve as a measure of neuroprotection with regard to large nerve fibre function in humans, and the mechanisms involved in the regulation of HSP27 in humans could explain the development and progression of neuropathy in diabetes mellitus. Possible neuroprotective pathways could involve activating transcription factor 3 (ATF3), which is expressed in injured neurons. ATF3 has been shown to be involved in the induction of HSP27, which, through downstream signalling, inhibits apoptosis and induces nerve elongation [170]. Thus, the potential lack of HSP27 up-regulation in diabetes mellitus might hamper the anti-apoptotic downstream effects as well as contribute to a lack of nerve regeneration. The hyperglycaemia-induced polyol pathway, reduced nerve blood flow, decreased capillary density, and oxidative stress have been suggested as crucial pathogenic mechanisms in the development of diabetic neuropathy [99, 104, 126, 171-173]. Because HSP27 is also involved in opposing oxidative stress [122, 123, 181-183], it is possible that insufficient reduction of oxidative stress might contribute to the development of peripheral neuropathy in diabetes mellitus. There is a progressive loss of nerve fibres in peripheral nerves in human diabetic neuropathy that is accompanied by degeneration and loss of DRG neurons, i.e. a “dying-back” type of peripheral axonopathy that eventually involves the whole neuron [174-176]. It has been shown that apoptotic stress might be present in the DRG of chronically diabetic rats but this does not necessarily lead to apoptotic cell death [126]. However, following neural ischemia apoptotic suppression signalling fails if HSP27 is not present [180]. Furthermore, disturbed axonal transport and neural blood flow, features seen in diabetes mellitus [55, 103, 157, 174, 176-179], could add to a decreased neuroprotective function of HSP27. Individuals with T1DM and T2DM have lower concentrations of HSP27 than healthy individuals. The correlation between progression of large nerve fibre dysfunction and a relative decrease in serum HSP27 concentrations could be indicative of an association between peripheral nerve function and HSP27. This thesis also suggests that higher HSP27 concentrations are associated with better function of large nerve fibres and vice versa. Studies on animals have shown that overexpression of HSP27 results in protection from a range of sensory abnormalities [20], and up-regulation of HSP27 has been related to neuronal protection [129]. Thus, HSP27 might be important both as a neuroprotective factor [19, 20] and for neural regeneration [21, 22, 130, 170, 184]. It has also been shown that HSP27 is up-regulated after acute nerve injuries in animal models [22, 125, 131]. A decrease in serum HSP27 concentration over time for any reason could, perhaps, result in insufficient neuroprotection by HSP27. As the diabetes mellitus progresses, the chronic

51
metabolic stress remains along with subsequent damage to peripheral nerves in individuals with decreasing HSP27 regardless of whether the decrease in HSP27 is due to the diabetes mellitus per se. Thus, the low HSP27 concentration in diabetes mellitus could be an indication of inadequate neuroprotection by HSP27 in patients with diabetes mellitus. There is to my knowledge only one other clinical cross-sectional study on the relationship between HSP27 and diabetic neuropathy. That nested case-control study showed higher serum HSP27 concentrations in T1DM patients with neuropathy than in T1DM patients without neuropathy [135]. The NGT and IGT participants in this thesis had very minimal evidence of neuropathy. Even the T2DM patients had velocities in the peroneal and sural nerves of more than 45 m/s, which would be considered normal by most researchers. This might explain the differences from the study by Gruden et al. [135] with T1DM patients in which the severity of neuropathy was assessed relatively crudely based on symptoms, loss of ankle reflexes, and VPTs. The T1DM patients of Gruden et al. might, therefore, have significantly worse neuropathy than the T2DM patients in Paper III. It is clear that patients with diabetes mellitus in this thesis, as well as that of Gruden et al., all had lower HSP27 concentrations than the non-diabetic controls used in Papers III and IV, and this suggests an insufficient level of neuroprotection in diabetes mellitus (see Table 7 for HSP27 concentrations). HSP27 concentrations in T2DM patients were lower than in individuals with IGT, which in turn were higher than in individuals with NGT. The higher HSP27 concentrations seen in IGT individuals could reflect an initial and early up-regulation of HSP27 that would have a neuroprotective effect on peripheral nerves. This is in line with the early up-regulation of HSP27 that is seen after acute nerve injuries in animal models [22, 125, 131]. This could explain why IGT individuals did not differ significantly in their peripheral nerve function compared to NGT individuals. However, this up-regulation of HSP27 could be insufficient or could become exhausted when the patient proceeds to develop overt diabetes mellitus, and the low HSP27 concentrations could in turn explain why T2DM patients had poorer peripheral nerve function than NGT and IGT individuals. Thus, circulating HSP27 might be an important nerve survival factor in humans. Regardless of what causes a decrease in HSP27 concentrations, such a decrease signifies the relative vulnerability to peripheral nerve fibre damage in patients at risk of developing neuropathy such as those with diabetes mellitus. In order to understand this, future research should focus on studying the cellular expression of human HSP27 in peripheral nerves in response to metabolic stress.

52
Table 7 – Summary of HSP27 concentrations from Papers III and IV and from the study by Gruden et al.
Paper III Paper IV Gruden et alb
NGT IGT T2DM Healthy controls
T1DM baseline
T1DM follow-up
T1DM Cases
T1DM Controls
HSP27 pg/mLa
722 (564–922)
1010 (638–1300)
412 (284–598)
785 (732–842)
547 (421–711)
538 (417–693)
658 (286–1315)
568 (250–1136)
NGT, normal glucose tolerance; IGT, impaired glucose tolerance; T2DM, type 2 diabetes mellitus; T1DM, type 1 diabetes mellitus. a For NGT, IGT, T2DM, and T1DM at baseline and follow-up, the data are geometric means and 95% CI. b Data from Gruden et al are geometric means and 25th–75th percentiles and Cases (n =�363) were defined as T1DM patients with one or more complications of diabetes mellitus and Controls (n =�168) were defined as T1DM patients with no evidence of any complications [135].
In summary, this thesis has shown that the existence of peripheral neuropathy as a consequence of IGT is not likely, and extensive control of neuropathy in IGT individuals is not advocated by this thesis. This thesis has also shown that biothesiometry and quantification of IENFD with skin biopsies are useful methods when assessing peripheral nerve function in both clinical practice and research. The role of HSP27 in relation to peripheral nerve function has been better understood in this thesis, and this might be a reasonable starting point for future research aiming to find disease-modifying agents that can reverse or stop the progression of peripheral neuropathy. Overall, these insights contribute to a better understanding of the complex nature of peripheral neuropathy.

53
Limitations and strengths As with all research, there are a number of limitations in this thesis that must be addressed. One obvious limitation is the sample size in Papers I–III, and the relatively small group sizes might reduce the power to detect group differences. The main hypothesis was that IGT individuals have more evidence of peripheral nerve dysfunction than individuals with NGT suggesting that IGT by itself could be an adequate explanation for peripheral neuropathy. Our negative finding in this regard might be due to inadequate statistical power to detect a difference. Another explanation could be that individuals with NGT have other causes of neuropathy that have not been excluded in this thesis or they might have idiopathic neuropathy. The difference between IGT and NGT individuals in terms of peripheral nerve function, therefore, might not be significantly different. A possible type 1 error could lead to rejection of the null-hypothesis by concluding that there is a group difference when in reality there is no such difference; i.e. the incorrect rejection of a true null hypothesis. A conclusion based on such a type 1 error could misleadingly emphasize the existence of “IGT neuropathy”. Such a conclusion could lead to unnecessary attempts to control neuropathy in IGT patients and vice versa and to excessive health care costs and unnecessary worrying of patients. However, it is known that IGT individuals have risk factors related to cardiovascular disease as well as risk of progression to T2DM. Thus, a potential type 1 error-based conclusion would not necessarily result in risky mistreatment or over-diagnosis. A type 2 error would accept the null hypothesis by concluding that there are no differences in peripheral nerve dysfunction between IGT and NGT individuals (as suggested by Paper I) when in reality there is such a difference; i.e. a failure to reject a false null hypothesis. Such a conclusion could result in the possibility of failure and unawareness to assess and focus on neuropathy in IGT individuals, especially in those with subclinical neuropathy or with discrete signs and symptoms of neuropathy. In this thesis, tissue sections with a thickness of 5 μm were used instead of a thickness of 50 μm as used by others when quantifying IENFD [64, 65, 185]. The technique used in this thesis yields small numbers of fibres counted per section and the values might be more variable compared to thicker 50 μm sections. The present technique still allows for group comparisons between the NGT, IGT, and T2DM individuals in Papers I and II but it does limit comparisons to studies using thicker sections. In addition, the cross-sectional design of Papers I–III does not enable us to assess causal or temporal relationships. Another limitation is the risk of selection bias. In the Skellefteå cohort, the T2DM patients were invited by their diabetes nurses at their yearly check-ups and such an approach might result in a selection of relatively healthy T2DM participants. Several key metabolic variables from the Swedish national diabetes registry (NDR) data from 2004 and 2005 were compared with the T2DM patients in this thesis. The lipid profile of the T2DM patients

54
in this thesis was similar (in terms of HDL and LDL) or even better (in terms of total cholesterol and triglycerides) compared to that of the NDR. The percentage of T2DM patients with statin treatment was higher than in the NDR (55% vs. 41%). The proportion of T2DM patients in this thesis with \�������&&��&��_���@��{{����(41%) was higher than that of the NDR (30%), i.e. they had better blood pressures than the patients in the NDR. In addition, the proportion of individuals with HbA1c concentrations <6.5% or 47.4 mmol/mol in the T2DM population in this thesis was similar to that in the NDR (67% vs. 64%). For HbA1c concentrations <6.0 % or 42.1 mmol/mol, the same comparison was 59% vs. 47%, i.e. the T2DM patients in this thesis had better glycaemic control than the total cohort in the NDR. However, the proportion of the T2DM patients with BMI <25 kg/m2 was less than to that of the NDR (10% vs. 20%). Altogether, this analysis suggests that the T2DM patients in this thesis might represent a population that is relatively healthier than the overall Swedish T2DM population with respect to lipid profile, blood pressure, and glycaemic control. Furthermore, the T2DM individuals from the Skellefteå cohort were diagnosed clinically and some may have had latent autoimmune diabetes in adults and, therefore, possibly represented a rather heterogeneous group. Additional selection bias could have come from the fact that the NGT and IGT individuals were consecutively recruited from a population-based sample (the VIP), and one could argue that the NGT and IGT participants have not been randomly obtained. The prevalence of hypertension in the NGT and IGT participants recruited in this thesis was considerably lower than the total population of participants in the VIP who are 60 years old [186, 187], whereas the cholesterol and triglyceride concentrations were slightly higher for the NGT individuals mainly due to lower use of statins in this group. Thus, with respect to hypertension, the IGT and NGT participants in this thesis may represent a healthier population than in the VIP and, perhaps, the general population. In addition, IGT individuals in Västerbotten County are followed-up at primary health care clinics and many of them are treated for dyslipidaemia and hypertension. For example, the lipid status of the IGT individuals was better than the NGT individuals mainly due to the use of statin medication. Thus, one can argue that the IGT individuals were well treated and, therefore, did not differ in terms of peripheral nerve function from NGT individuals. HbA1c was low in IGT individuals and was almost identical to that in NGT individuals, and this was also the case with blood pressure. It is also possible that the Malmö cohort might represent a relatively healthy T1DM population because the majority of the participants in 1992 had been invited to a previous study and were familiar with participation in clinical studies concerning neuropathy. However, this would not necessarily make the population healthier but it might make the participants biased in how readily they “sense” the stimuli in the nerve function tests. Overall, the T1DM patients were well informed regarding their disease and the forthcoming follow-up examinations. In addition, all of the T1DM participants had been regularly treated at the diabetes clinic for many years prior to their invitation

55
to this study and thus a selection bias due to the recruitment of such patients could have occurred. In clinical research, the recruiting process of almost all studies results in a pool of participants who are interested in taking part in the research and are often well treated and healthier than the general population. However, when comparing the T1DM patients in this thesis at follow-up with that of T1DM patients from the NDR, the lipid profile, glycaemic control, and frequency of anti-hypertensive and statin treatment was almost identical. Thus, the T1DM individuals in this thesis are quite representative of the general T1DM population in Sweden. One of the strengths of this thesis is that the glycaemic status of NGT and IGT individuals was verified with two separate OGTTs. Another strength is that the NGT, IGT, and T2DM participants were of the same age. Thus, the Skellefteå cohort is a large and well-defined cohort. In addition, in both the Skellefteå and Malmö cohorts measures were taken to exclude other common causes of peripheral neuropathy in the population such as vitamin B12 deficiency and chronic alcoholism. Another unique strength is that HSP27 concentrations were for the first time measured prospectively in humans with T1DM and in a relatively large number of healthy controls. Finally, validated and reproducible methods assessing both large and small nerve fibre function were used both cross-sectionally and longitudinally.

56
Future perspectives Effective therapeutic agents aiming to reverse and halt the progression of diabetic neuropathy in humans are still needed. Currently, there are no successful therapeutic agents in use to target the metabolic dysfunctions that are thought to cause neuropathy in diabetes mellitus. The same is true for therapies for microvascular insufficiencies associated with diabetic neuropathy. In line with this, attempts to prevent neuropathy with neurotrophic factors, such as NGF, have failed [198]. The possibility to treat diabetic neuropathy with antioxidants has been the subject of several clinical trials. The most promising results from several studies have shown regression of symptoms and signs after experimental ����{���^�����-lipoic acid [109-113], and �-lipoic acid has been licenced for use in treating diabetes mellitus in some countries [108]. Therapy targeting several mechanisms simultaneously would perhaps be of interest because reversing or inhibiting only a single mechanism might not be sufficient to reverse peripheral nerve damage. The anti-apoptotic function of HSP27 along with its roles in neural differentiation and regeneration make HSP27 an interesting and potentially versatile factor when trying to simultaneously target several mechanisms to prevent and reverse peripheral neuropathy in diabetes mellitus. Thus, the neuroprotective role of HSP27 described in this thesis could be an important starting point for new disease-modifying therapies. Future studies should address the possibility of increasing and regulating HSP27 expression in patients with diabetes mellitus as a means of preventing the development of peripheral neuropathy. There is growing evidence that changes within the CNS develop concomitantly with peripheral neuropathy [188], and this reconsidering of the nature of diabetic neuropathy could open new directions for further research. This is important to emphasize because the progression of diabetic neuropathy is resistant to conventional medical treatment. Thus, the need to recognize the role of the CNS in the progression of peripheral neuropathy is important, and modulation of the CNS might provide new therapeutic approaches. Advanced neuroimaging techniques that measure both structure and function of the CNS and the PNS could also provide objective diagnostic measures of the entire nervous system [188, 189]. Recent advances in neuroimaging methods, such as magnetic resonance (MR) diffusion tensor imaging (DTI) and tractography, might lead to a better understanding of how diabetes mellitus affects the PNS and the CNS [188, 190-192]. Tractography is a technique that visually characterizes neural tracts using DTI and computer-based image analysis. The results from a tractography can then be presented as two- and three-dimensional images [193]. DTI is an MR imaging technique that can reveal pathologies that are not seen using conventional MR. DTI and tractography are currently only used in research, but these might have potential clinical uses as well. These methods could perhaps be used to better understand and visualize the progression of peripheral nerve dysfunction.

57
Other neuroimaging techniques including functional MR imaging, brain MR spectroscopy, and MR perfusion imaging have been used to image areas that generate or modulate pain in diabetic neuropathy as well as to study peripheral small fibres and their modulation at the spinal cord and the thalamus [73]. Development of these methods could perhaps lead to more effective pain treatments. The use of sonography has also emerged, and it has been proposed that peripheral nerves of patients with diabetic neuropathy are enlarged compared to controls [194, 195]. This might be indicative of a potential screening capability of sonography in diabetic neuropathy. Other possible assessments that are not yet clinically widespread and are still under development include morphological evaluation of nerve biopsies (often of the sural nerve) [56, 66] and corneal confocal microscopy. In corneal confocal microscopy, the small nerve fibres in the cornea are quantified noninvasively as a surrogate measure of peripheral nerve function [196, 197]. These emerging methods might also clarify how possible sex differences, age-related changes, and the fact that there could be individual variation in the number of neurons an individual is born with could contribute to the development of peripheral neuropathy.

58
Main conclusions �� Large nerve fibre function and measures of small nerve fibres do not
differ between IGT and NGT individuals.
�� The biothesiometer provides sufficient diagnostic performance to identify clinical neuropathy in routine health care. In addition, the use of skin biopsies with subsequent quantification of IENFD in combination with methods measuring vibrotactile sense increases the sensitivity of detecting small nerve fibre neuropathy.
�� High concentrations of HSP27 are associated with better large nerve
fibre function and few neuropathic signs. �� Individuals with T1DM and T2DM have lower HSP27 concentrations
than non-diabetic controls, and deteriorating large nerve fibre function is associated with a decrease in HSP27 concentrations over time in T1DM. This could be indicative of insufficient neuroprotection in patients with diabetes mellitus.

59
Acknowledgements This thesis could not have been completed without the work and help of many people who in one way or another contributed to the completion of this thesis. I want to thank all of them, including those not mentioned here by name. My deepest thanks to all of the study participants without whom this thesis would not have been possible. I would like to express my sincere gratitude to my supervisor Olov Rolandsson for his guidance, motivation, and support. Olov is not only an outstanding supervisor but also a researcher in its truest meaning. I could not imagine having a better mentor. I am also grateful to my co-supervisor Lars Dahlin for his encouragement, expertise and insightful comments on my work. I feel incredibly privileged that I had the opportunity to work with and learn from Olov and Lars. I want to thank Elisabet Englund, Kurt Boman, and Hanna Skjärstrand for their professional input and interesting discussions. I am also indebted to the late professor Göran Sundkvist who initiated the works of this thesis. I express my gratitude to Sigbritt Rasmark and Karin Eriksson for their involvement and practical contribution. I am also grateful to the National Research School in General Practice (Nationella forskarskolan i allmänmedicin). Last but not least, thanks to my mother and father for their love and support. The studies in this thesis were supported by grants from the Västerbotten County Council, Sweden, and Swedish Medical Research Council, Region Skåne, Lund University, Skåne University Hospital.
60
References [1] Danaei G, Finucane MM, Lu Y, et al. (2011) National, regional, and
global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2•7 million participants. Lancet 378: 31-40
[2] Wild S, Roglic G, Green A, Sicree R, King H (2004) Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 27: 1047-1053
[3] Vos T, Flaxman AD, Naghavi M, et al. (2012) Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2163-2196
[4] Cheng YJ, Gregg EW, Kahn HS, Williams DE, De Rekeneire N, Narayan KM (2006) Peripheral insensate neuropathy--a tall problem for US adults? Am J Epidemiol 164: 873-880
[5] Vinik AI, Kong X, Megerian JT, Gozani SN (2006) Diabetic nerve conduction abnormalities in the primary care setting. Diabetes Technol Ther 8: 654-662
[6] Vinik A, Ullal J, Parson HK, Casellini CM (2006) Diabetic neuropathies: clinical manifestations and current treatment options. Nat Clin Pract Endocrinol Metab 2: 269-281
[7] Papanas N, Ziegler D (2012) Prediabetic neuropathy: does it exist? Curr Diab Rep 12: 376-383
[8] Papanas N, Vinik AI, Ziegler D (2011) Neuropathy in prediabetes: does the clock start ticking early? Nat Rev Endocrinol 7: 682-690
[9] Smith A, Singleton J (2008) Impaired glucose tolerance and neuropathy. Neurologist 14: 23-29
[10] Singleton JR, Smith AG (2007) Neuropathy associated with prediabetes: what is new in 2007? Curr Diab Rep 7: 420-424
[11] Hinder LM, Vincent AM, Burant CF, Pennathur S, Feldman EL (2012) Bioenergetics in diabetic neuropathy: what we need to know. J Peripher Nerv Syst 17 Suppl 2: 10-14
[12] Zochodne DW (2007) Diabetes mellitus and the peripheral nervous system: manifestations and mechanisms. Muscle Nerve 36: 144-166
[13] (1993) The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med 329: 977-986
[14] Albers JW, Herman WH, Pop-Busui R, et al. (2010) Effect of prior intensive insulin treatment during the Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in type 1 diabetes during the Epidemiology of Diabetes Interventions and Complications (EDIC) Study. Diabetes Care 33: 1090-1096
[15] (1998) Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in

61
patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 352: 837-853
[16] Ismail-Beigi F, Craven T, Banerji MA, et al. (2010) Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: an analysis of the ACCORD randomised trial. Lancet 376: 419-430
[17] Duckworth W, Abraira C, Moritz T, et al. (2009) Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 360: 129-139
[18] Arrigo AP (2007) The cellular "networking" of mammalian Hsp27 and its functions in the control of protein folding, redox state and apoptosis. Adv Exp Med Biol 594: 14-26
[19] Benn S, Perrelet D, Kato A, et al. (2002) Hsp27 upregulation and phosphorylation is required for injured sensory and motor neuron survival. Neuron 36: 45-56
[20] Korngut L, Ma CH, Martinez JA, et al. (2012) Overexpression of human HSP27 protects sensory neurons from diabetes. Neurobiol Dis 47: 436-443
[21] Williams KL, Mearow KM (2011) Phosphorylation status of heat shock protein 27 influences neurite growth in adult dorsal root ganglion sensory neurons in vitro. J Neurosci Res 89: 1160-1172
[22] Ma CH, Omura T, Cobos EJ, et al. (2011) Accelerating axonal growth promotes motor recovery after peripheral nerve injury in mice. J Clin Invest 121: 4332-4347
[23] Mellitus ECotDaCoD (2003) Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 26 Suppl 1: S5-20
[24] Mokdad AH, Ford ES, Bowman BA, et al. (2003) Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 289: 76-79
[25] Bressler J, Kao WH, Pankow JS, Boerwinkle E (2010) Risk of type 2 diabetes and obesity is differentially associated with variation in FTO in whites and African-Americans in the ARIC study. PLoS One 5: e10521
[26] Bonora E, Targher G, Formentini G, et al. (2004) The Metabolic Syndrome is an independent predictor of cardiovascular disease in Type 2 diabetic subjects. Prospective data from the Verona Diabetes Complications Study. Diabet Med 21: 52-58
[27] Lorenzo C, Okoloise M, Williams K, Stern MP, Haffner SM, Study SAH (2003) The metabolic syndrome as predictor of type 2 diabetes: the San Antonio heart study. Diabetes Care 26: 3153-3159
[28] Beyan H, Ola T, David R, Leslie G (2006) Progression of autoimmune diabetes: slowly progressive insulin-dependent diabetes mellitus or latent autoimmune diabetes of adult. Ann N Y Acad Sci 1079: 81-89
[29] Carlsson S, Midthjell K, Tesfamarian MY, Grill V (2007) Age, overweight and physical inactivity increase the risk of latent autoimmune diabetes in adults: results from the Nord-Trøndelag health study. Diabetologia 50: 55-58
62
[30] Chakarova N, Tankova T, Atanassova I, Dakovska L (2009) Serum lipid and hsCRP levels in prediabetes - impaired fasting glucose (IFG) and impaired glucose tolerance (IGT). Diabetes Res Clin Pract
[31] Goldberg R, Temprosa M, Haffner S, et al. (2009) Effect of progression from impaired glucose tolerance to diabetes on cardiovascular risk factors and its amelioration by lifestyle and metformin intervention: the Diabetes Prevention Program randomized trial by the Diabetes Prevention Program Research Group. Diabetes Care 32: 726-732
[32] Meigs JB, Muller DC, Nathan DM, Blake DR, Andres R, Aging BLSo (2003) The natural history of progression from normal glucose tolerance to type 2 diabetes in the Baltimore Longitudinal Study of Aging. Diabetes 52: 1475-1484
[33] Smith BE (2006). Anatomy and histology of peripheral nerve. In: Handbook of Clinical Neurophysiology V, Peripheral Nerve Diseases, Volume editor: J. Kimura, Series Editors: Daube JR, Mauguière F, pp. 3-22. Elsevier, Amsterdam.
[34] Weimer L, Latov N (2010) General considerations. In: Merritt’s Neurology. Editors: Rowland P, Pedley T, pp. 813-815. Lippincott Williams & Wilkins, Philadelphia
[35] Boulton A, Vinik A, Arezzo J, et al. (2005) Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care 28: 956-962
[36] Pirart J (1977) [Diabetes mellitus and its degenerative complications: a prospective study of 4,400 patients observed between 1947 and 1973 (3rd and last part) (author's transl)]. Diabete Metab 3: 245-256
[37] Dyck PJ, Kratz KM, Karnes JL, et al. (1993) The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: the Rochester Diabetic Neuropathy Study. Neurology 43: 817-824
[38] Young M, Boulton A, MacLeod A, Williams D, Sonksen P (1993) A multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia 36: 150-154
[39] Tesfaye S, Stevens L, Stephenson J, et al. (1996) Prevalence of diabetic peripheral neuropathy and its relation to glycaemic control and potential risk factors: the EURODIAB IDDM Complications Study. Diabetologia 39: 1377-1384
[40] Young MJ, Boulton AJ, MacLeod AF, Williams DR, Sonksen PH (1993) A multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia 36: 150-154
[41] Cabezas-Cerrato J (1998) The prevalence of clinical diabetic polyneuropathy in Spain: a study in primary care and hospital clinic groups. Neuropathy Spanish Study Group of the Spanish Diabetes Society (SDS). Diabetologia 41: 1263-1269
[42] Pirart J (1977) [Diabetes mellitus and its degenerative complications: a prospective study of 4,400 patients observed between 1947 and 1973 (author's transl)]. Diabete Metab 3: 97-107
63
[43] Vinik AI, Holland MT, Le Beau JM, Liuzzi FJ, Stansberry KB, Colen LB (1992) Diabetic neuropathies. Diabetes Care 15: 1926-1975
[44] Sima AA (1994) Pathological definition and evaluation of diabetic neuropathy and clinical correlations. Can J Neurol Sci 21: S13-17
[45] Krarup C (2006) Physiologhy and function. In: Handbook of Clinical Neurophysiology V PND, Volume editor: J. Kimura, Series Editors: Daube JR, Mauguière F, pp. 23-61. Elsevier, Amsterdam.
[46] Chong PS, Cros DP (2004) Technology literature review: quantitative sensory testing. Muscle Nerve 29: 734-747
[47] Shy ME, Frohman EM, So YT, et al. (2003) Quantitative sensory testing: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 60: 898-904
[48] Coppini DV, Spruce MC, Thomas P, Masding MG (2006) Established diabetic neuropathy seems irreversible despite improvements in metabolic and vascular risk markers--a retrospective case-control study in a hospital patient cohort. Diabet Med 23: 1016-1020
[49] Lin YH, Hsieh SC, Chao CC, Chang YC, Hsieh ST (2005) Influence of aging on thermal and vibratory thresholds of quantitative sensory testing. J Peripher Nerv Syst 10: 269-281
[50] Heldestad V, Linder J, Sellersjö L, Nordh E (2010) Reproducibility and influence of test modality order on thermal perception and thermal pain thresholds in quantitative sensory testing. Clin Neurophysiol 121: 1878-1885
[51] Heldestad V, Nordh E (2007) Quantified sensory abnormalities in early genetically verified transthyretin amyloid polyneuropathy. Muscle Nerve 35: 189-195
[52] Valensi P, Attali JR, Gagant S (1993) Reproducibility of parameters for assessment of diabetic neuropathy. The French Group for Research and Study of Diabetic Neuropathy. Diabet Med 10: 933-939
[53] England J, Gronseth G, Franklin G, et al. (2005) Distal symmetric polyneuropathy: a definition for clinical research: report of the American Academy of Neurology, the American Association of Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Neurology 64: 199-207
[54] Dyck P (1988) Detection, characterization, and staging of polyneuropathy: assessed in diabetics. Muscle Nerve 11: 21-32
[55] Thrainsdottir S, Malik R, Dahlin L, et al. (2003) Endoneurial capillary abnormalities presage deterioration of glucose tolerance and accompany peripheral neuropathy in man. Diabetes 52: 2615-2622
[56] Thrainsdottir S, Malik RA, Rosén I, et al. (2009) Sural nerve biopsy may predict future nerve dysfunction. Acta Neurol Scand 120: 38-46
[57] Freeman TL JE, Freeman ED, et al. Nerve Conduction Studies (NCS) (2004) In: Cuccurullo S, editor. Physical Medicine and Rehabilitation Board Review. New York: Demos Medical Publishing. Available from: http://www.ncbi.nlm.nih.gov/books/NBK27199/
[58] Misra UK, Kalita J, Nair PP (2008) Diagnostic approach to peripheral neuropathy. Ann Indian Acad Neurol 11: 89-97
64
[59] Franssen H, van den Bergh PY (2006) Nerve conduction studies in polyneuropathy: practical physiology and patterns of abnormality. Acta Neurol Belg 106: 73-81
[60] Bagai K, Wilson JR, Khanna M, Song Y, Wang L, Fisher MA (2008) Electrophysiological patterns of diabetic polyneuropathy. Electromyogr Clin Neurophysiol 48: 139-145
[61] Valls-Canals J, Povedano M, Montero J, Pradas J (2002) Diabetic polyneuropathy. Axonal or demyelinating? Electromyogr Clin Neurophysiol 42: 3-6
[62] Koo YS, Cho CS, Kim BJ (2012) Pitfalls in using electrophysiological studies to diagnose neuromuscular disorders. J Clin Neurol 8: 1-14
[63] Gooch CL, Weimer LH (2007) The electrodiagnosis of neuropathy: basic principles and common pitfalls. Neurol Clin 25: 1-28
[64] Lauria G, Bakkers M, Schmitz C, et al. (2010) Intraepidermal nerve fiber density at the distal leg: a worldwide normative reference study. J Peripher Nerv Syst 15: 202-207
[65] Lauria G, Hsieh ST, Johansson O, et al. (2010) European Federation of Neurological Societies/Peripheral Nerve Society Guideline on the use of skin biopsy in the diagnosis of small fiber neuropathy. Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society. Eur J Neurol 17: 903-912, e944-909
[66] England J, Gronseth G, Franklin G, et al. (2009) Evaluation of distal symmetric polyneuropathy: The role of autonomic testing, nerve biopsy, and skin biopsy (an evidence-based review). Muscle Nerve 39: 106-115
[67] Nebuchennykh M, Løseth S, Lindal S, Mellgren S (2009) The value of skin biopsy with recording of intraepidermal nerve fiber density and quantitative sensory testing in the assessment of small fiber involvement in patients with different causes of polyneuropathy. J Neurol 256: 1067-1075
[68] Polydefkis M, Hauer P, Sheth S, Sirdofsky M, Griffin JW, McArthur JC (2004) The time course of epidermal nerve fibre regeneration: studies in normal controls and in people with diabetes, with and without neuropathy. Brain 127: 1606-1615
[69] Vinik A, Freeman R, Erbas T (2003) Diabetic autonomic neuropathy. Semin Neurol 23: 365-372
[70] Casellini CM, Vinik AI (2007) Clinical manifestations and current treatment options for diabetic neuropathies. Endocr Pract 13: 550-566
[71] Ragé M, Van Acker N, Knaapen MW, et al. (2011) Asymptomatic small fiber neuropathy in diabetes mellitus: investigations with intraepidermal nerve fiber density, quantitative sensory testing and laser-evoked potentials. J Neurol 258: 1852-1864
[72] Hendriksen PH, Oey PL, Wieneke GH, Bravenboer B, Banga JD (1992) Subclinical diabetic neuropathy: similarities between electrophysiological results of patients with type 1 (insulin-dependent) and type 2 (non-insulin-dependent) diabetes mellitus. Diabetologia 35: 690-695
65
[73] Tesfaye S, Selvarajah D (2012) Advances in the epidemiology, pathogenesis and management of diabetic peripheral neuropathy. Diabetes Metab Res Rev 28 Suppl 1: 8-14
[74] Dyck PJ, Albers JW, Andersen H, et al. (2011) Diabetic Polyneuropathies: Update on Research Definition, Diagnostic Criteria and Estimation of Severity. Diabetes Metab Res Rev
[75] Vinik A, Mitchell B (1988) Clinical aspects of diabetic neuropathies. Diabetes Metab Rev 4: 223-253
[76] Sorensen L, Molyneaux L, Yue DK (2006) The level of small nerve fiber dysfunction does not predict pain in diabetic Neuropathy: a study using quantitative sensory testing. Clin J Pain 22: 261-265
[77] Truini A, Biasiotta A, Di Stefano G, et al. (2013) Peripheral nociceptor sensitization mediates allodynia in patients with distal symmetric polyneuropathy. J Neurol 260: 761-766
[78] Tesfaye S, Boulton AJ, Dyck PJ, et al. (2010) Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 33: 2285-2293
[79] Sumner C, Sheth S, Griffin J, Cornblath D, Polydefkis M (2003) The spectrum of neuropathy in diabetes and impaired glucose tolerance. Neurology 60: 108-111
[80] Novella S, Inzucchi S, Goldstein J (2001) The frequency of undiagnosed diabetes and impaired glucose tolerance in patients with idiopathic sensory neuropathy. Muscle Nerve 24: 1229-1231
[81] Singleton J, Smith A, Bromberg M (2001) Increased prevalence of impaired glucose tolerance in patients with painful sensory neuropathy. Diabetes Care 24: 1448-1453
[82] Hoffman-Snyder C, Smith BE, Ross MA, Hernandez J, Bosch EP (2006) Value of the oral glucose tolerance test in the evaluation of chronic idiopathic axonal polyneuropathy. Arch Neurol 63: 1075-1079
[83] Singleton JR, Smith AG, Bromberg MB (2001) Painful sensory polyneuropathy associated with impaired glucose tolerance. Muscle Nerve 24: 1225-1228
[84] Franklin G, Kahn L, Baxter J, Marshall J, Hamman R (1990) Sensory neuropathy in non-insulin-dependent diabetes mellitus. The San Luis Valley Diabetes Study. Am J Epidemiol 131: 633-643
[85] Ziegler D, Rathmann W, Dickhaus T, Meisinger C, Mielck A, Group KS (2008) Prevalence of polyneuropathy in pre-diabetes and diabetes is associated with abdominal obesity and macroangiopathy: the MONICA/KORA Augsburg Surveys S2 and S3. Diabetes Care 31: 464-469
[86] Ziegler D, Rathmann W, Dickhaus T, Meisinger C, Mielck A, Group KS (2009) Neuropathic pain in diabetes, prediabetes and normal glucose tolerance: the MONICA/KORA Augsburg Surveys S2 and S3. Pain Med 10: 393-400
[87] Ziegler D, Rathmann W, Meisinger C, Dickhaus T, Mielck A, Group KS (2009) Prevalence and risk factors of neuropathic pain in survivors of myocardial infarction with pre-diabetes and diabetes. The KORA Myocardial Infarction Registry. Eur J Pain 13: 582-587
66
[88] Dyck PJ, Clark VM, Overland CJ, et al. (2012) Impaired glycemia and diabetic polyneuropathy: the OC IG Survey. Diabetes Care 35: 584-591
[89] Attal N, Cruccu G, Baron R, et al. (2010) EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur J Neurol 17: 1113-e1188
[90] Shenoy AM (2012) Guidelines in practice: treatment of painful diabetic neuropathy. Continuum (Minneap Minn) 18: 192-198
[91] Bril V, England J, Franklin GM, et al. (2011) Evidence-based guideline: Treatment of painful diabetic neuropathy: report of the American Academy of Neurology, the American Association of Neuromuscular and Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Neurology 76: 1758-1765
[92] Dworkin RH, O'Connor AB, Audette J, et al. (2010) Recommendations for the pharmacological management of neuropathic pain: an overview and literature update. Mayo Clin Proc 85: S3-14
[93] Negi G, Kumar A, Joshi RP, Sharma SS (2011) Oxidative stress and Nrf2 in the pathophysiology of diabetic neuropathy: old perspective with a new angle. Biochem Biophys Res Commun 408: 1-5
[94] Danta G (1973) Clinical features of peripheral neuropathy associated with hypoglycemia. Adv Metab Disord 2: Suppl 2:465-479
[95] Danta G (1969) Hypoglycemic peripheral neuropathy. Arch Neurol 21: 121-132
[96] Potter CG, Sharma AK, Farber MO, Peterson RG (1988) Hypoglycemic neuropathy in experimental diabetes. J Neurol Sci 88: 293-301
[97] Zochodne D (2007) Diabetes mellitus and the peripheral nervous system: manifestations and mechanisms. Muscle Nerve 36: 144-166
[98] Dyck PJ, Sherman WR, Hallcher LM, et al. (1980) Human diabetic endoneurial sorbitol, fructose, and myo-inositol related to sural nerve morphometry. Ann Neurol 8: 590-596
[99] Greene DA, Lattimer SA, Sima AA (1988) Are disturbances of sorbitol, phosphoinositide, and Na+-K+-ATPase regulation involved in pathogenesis of diabetic neuropathy? Diabetes 37: 688-693
[100] Mayhew JA, Gillon KR, Hawthorne JN (1983) Free and lipid inositol, sorbitol and sugars in sciatic nerve obtained post-mortem from diabetic patients and control subjects. Diabetologia 24: 13-15
[101] Hale PJ, Nattrass M, Silverman SH, et al. (1987) Peripheral nerve concentrations of glucose, fructose, sorbitol and myoinositol in diabetic and non-diabetic patients. Diabetologia 30: 464-467
[102] Dyck PJ, Zimmerman BR, Vilen TH, et al. (1988) Nerve glucose, fructose, sorbitol, myo-inositol, and fiber degeneration and regeneration in diabetic neuropathy. N Engl J Med 319: 542-548
[103] Wada R, Yagihashi S (2005) Role of advanced glycation end products and their receptors in development of diabetic neuropathy. Ann N Y Acad Sci 1043: 598-604
[104] Jack M, Wright D (2012) Role of advanced glycation endproducts and glyoxalase I in diabetic peripheral sensory neuropathy. Transl Res 159: 355-365
67
[105] ��&���������������"��������������������������$�������������������#�Advanced glycation endproducts in peripheral nerve in type 2 diabetes with neuropathy. Acta Diabetol 41: 158-166
[106] Bierhaus A, Haslbeck KM, Humpert PM, et al. (2004) Loss of pain perception in diabetes is dependent on a receptor of the immunoglobulin superfamily. J Clin Invest 114: 1741-1751
[107] Ziegler D, Sohr CG, Nourooz-Zadeh J (2004) Oxidative stress and antioxidant defense in relation to the severity of diabetic polyneuropathy and cardiovascular autonomic neuropathy. Diabetes Care 27: 2178-2183
[108] Ziegler D, Nowak H, Kempler P, Vargha P, Low PA (2004) Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a meta-analysis. Diabet Med 21: 114-121
[109] Ziegler D, Hanefeld M, Ruhnau KJ, et al. (1995) Treatment of symptomatic diabetic peripheral neuropathy with the anti-oxidant alpha-lipoic acid. A 3-week multicentre randomized controlled trial (ALADIN Study). Diabetologia 38: 1425-1433
[110] Ruhnau KJ, Meissner HP, Finn JR, et al. (1999) Effects of 3-week oral treatment with the antioxidant thioctic acid (alpha-lipoic acid) in symptomatic diabetic polyneuropathy. Diabet Med 16: 1040-1043
[111] Reljanovic M, Reichel G, Rett K, et al. (1999) Treatment of diabetic polyneuropathy with the antioxidant thioctic acid (alpha-lipoic acid): a two year multicenter randomized double-blind placebo-controlled trial (ALADIN II). Alpha Lipoic Acid in Diabetic Neuropathy. Free Radic Res 31: 171-179
[112] Ziegler D, Hanefeld M, Ruhnau KJ, et al. (1999) Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a 7-month multicenter randomized controlled trial (ALADIN III Study). ALADIN III Study Group. Alpha-Lipoic Acid in Diabetic Neuropathy. Diabetes Care 22: 1296-1301
[113] Ametov AS, Barinov A, Dyck PJ, et al. (2003) The sensory symptoms of diabetic polyneuropathy are improved with alpha-lipoic acid: the SYDNEY trial. Diabetes Care 26: 770-776
[114] Young MJ, Veves A, Walker MG, Boulton AJ (1992) Correlations between nerve function and tissue oxygenation in diabetic patients: further clues to the aetiology of diabetic neuropathy? Diabetologia 35: 1146-1150
[115] Malik RA, Tomlinson DR (2002) Angiotensin-converting enzyme inhibitors: are there credible mechanisms for beneficial effects in diabetic neuropathy? Int Rev Neurobiol 50: 415-430
[116] Akbari CM, Gibbons GW, Habershaw GM, LoGerfo FW, Veves A (1997) The effect of arterial reconstruction on the natural history of diabetic neuropathy. Arch Surg 132: 148-152
[117] Smith A, Russell J, Feldman E, et al. (2006) Lifestyle intervention for pre-diabetic neuropathy. Diabetes Care 29: 1294-1299
[118] Vincent AM, Hayes JM, McLean LL, Vivekanandan-Giri A, Pennathur S, Feldman EL (2009) Dyslipidemia-induced neuropathy in mice: the role of oxLDL/LOX-1. Diabetes 58: 2376-2385
68
[119] Smith A, Rose K, Singleton J (2008) Idiopathic neuropathy patients are at high risk for metabolic syndrome. J Neurol Sci 273: 25-28
[120] Pittenger GL, Mehrabyan A, Simmons K, et al. (2005) Small fiber neuropathy is associated with the metabolic syndrome. Metab Syndr Relat Disord 3: 113-121
[121] Hughes RA, Umapathi T, Gray IA, et al. (2004) A controlled investigation of the cause of chronic idiopathic axonal polyneuropathy. Brain 127: 1723-1730
[122] Bauersachs J, Widder J (2010) Reductive stress: linking heat shock protein 27, glutathione, and cardiomyopathy? Hypertension 55: 1299-1300
[123] Brerro-Saby C, Delliaux S, Steinberg J, Boussuges A, Gole Y, Jammes Y (2010) Combination of two oxidant stressors suppresses the oxidative stress and enhances the heat shock protein 27 response in healthy humans. Metabolism 59: 879-886
[124] Rogalla T, Ehrnsperger M, Preville X, et al. (1999) Regulation of Hsp27 oligomerization, chaperone function, and protective activity against oxidative stress/tumor necrosis factor alpha by phosphorylation. J Biol Chem 274: 18947-18956
[125] Hirata K, He J, Hirakawa Y, Liu W, Wang S, Kawabuchi M (2003) HSP27 is markedly induced in Schwann cell columns and associated regenerating axons. Glia 42: 1-11
[126] Kamiya H, Zhangm W, Sima AA (2005) Apoptotic stress is counterbalanced by survival elements preventing programmed cell death of dorsal root ganglions in subacute type 1 diabetic BB/Wor rats. Diabetes 54: 3288-3295
[127] Yamamoto M, Fan L, Wakayama T, Amano O, Iseki S (2001) Constitutive expression of the 27-kDa heat-shock protein in neurons and satellite cells in the peripheral nervous system of the rat. Anat Rec 262: 213-220
[128] Lewis S, Mannion R, White F, et al. (1999) A role for HSP27 in sensory neuron survival. J Neurosci 19: 8945-8953
[129] Dodge M, Wang J, Guy C, Rankin S, Rahimtula M, Mearow K (2006) Stress-induced heat shock protein 27 expression and its role in dorsal root ganglion neuronal survival. Brain Res 1068: 34-48
[130] Williams K, Rahimtula M, Mearow K (2006) Heat shock protein 27 is involved in neurite extension and branching of dorsal root ganglion neurons in vitro. J Neurosci Res 84: 716-723
[131] Sharp P, Krishnan M, Pullar O, Navarrete R, Wells D, de Belleroche J (2006) Heat shock protein 27 rescues motor neurons following nerve injury and preserves muscle function. Exp Neurol 198: 511-518
[132] Dai T, Patel-Chamberlin M, Natarajan R, et al. (2009) Heat shock protein 27 overexpression mitigates cytokine-induced islet apoptosis and streptozotocin-induced diabetes. Endocrinology 150: 3031-3039
[133] Evgrafov O, Mersiyanova I, Irobi J, et al. (2004) Mutant small heat-shock protein 27 causes axonal Charcot-Marie-Tooth disease and distal hereditary motor neuropathy. Nat Genet 36: 602-606
[134] Houlden H, Laura M, Wavrant-De Vrièze F, Blake J, Wood N, Reilly MM (2008) Mutations in the HSP27 (HSPB1) gene cause dominant,
69
recessive, and sporadic distal HMN/CMT type 2. Neurology 71: 1660-1668
[135] Gruden G, Bruno G, Chaturvedi N, et al. (2008) Serum heat shock protein 27 and diabetes complications in the EURODIAB prospective complications study: a novel circulating marker for diabetic neuropathy. Diabetes 57: 1966-1970
[136] Norberg M, Wall S, Boman K, Weinehall L (2010) The Västerbotten Intervention Programme: background, design and implications. Glob Health Action 3
[137] Rolandsson O, Norberg M, Nyström L, et al. (2012) How to diagnose and classify diabetes in primary health care: lessons learned from the Diabetes Register in Northern Sweden (DiabNorth). Scand J Prim Health Care 30: 81-87
[138] Bergstrom B, Lilja B, Osterlin S, Sundkvist G (1987) Autonomic neuropathy in type I diabetes: influence of duration and other diabetic complications. Acta Med Scand 222: 147-154
[139] Nilsson H, Bergstrom B, Lilja B, Juul-Moller S, Carlsson J, Sundkvist G (1995) Prospective study of autonomic nerve function in type 1 and type 2 diabetic patients: 24 hour heart rate variation and plasma motilin levels disturbed in parasympathetic neuropathy. Diabet Med 12: 1015-1021
[140] Dahlin LB, Granberg V, Rolandsson O, Rosén I, Dahlin E, Sundkvist G (2011) Disturbed vibrotactile sense in finger pulps in patients with Type 1 diabetes--correlations with glycaemic level, clinical examination and electrophysiology. Diabet Med 28: 1045-1052
[141] Forsén A, Kangro M, Sterner G, et al. (2004) A 14-year prospective study of autonomic nerve function in Type 1 diabetic patients: association with nephropathy. Diabet Med 21: 852-858
[142] Goldberg JM, Lindblom U (1979) Standardised method of determining vibratory perception thresholds for diagnosis and screening in neurological investigation. J Neurol Neurosurg Psychiatry 42: 793-803
[143] Sundkvist G, Lilja B, Nilsson H, Nilsson JA, Rosén I (1997) Peripheral nerve dysfunction is reflected by loss of ankle reflexes but not by autonomic neuropathy in diabetic patients. Muscle Nerve 20: 740-743
[144] Katon JG, Reiber GE, Nelson KM (2012) Peripheral Neuropathy Defined by Monofilament Insensitivity and Diabetes Status: NHANES 1999-2004. Diabetes Care
[145] Thrainsdottir S. (2009) Peripheral polyneuropathy in type 2 diabetes mellitus and impaired glucose tolerance. Correlations between morphology n, and clinical findings. Doctoral Dissertations series 2009:67 ISBN 978-91-86253-55-4.
[146] Thomsen NO, Englund E, Thrainsdottir S, Rosén I, Dahlin LB (2009) Intraepidermal nerve fibre density at wrist level in diabetic and non-diabetic patients. Diabet Med 26: 1120-1126
[147] Ellenberg M (1958) Diabetic neuropathy presenting as the initial clinical manifestation of diabetes. Ann Intern Med 49: 620-631
[148] Isak B, Oflazoglu B, Tanridag T, Yitmen I, Us O (2008) Evaluation of peripheral and autonomic neuropathy among patients with newly
70
diagnosed impaired glucose tolerance. Diabetes Metab Res Rev 24: 563-569
[149] Eriksson K, Nilsson H, Lindgärde F, et al. (1994) Diabetes mellitus but not impaired glucose tolerance is associated with dysfunction in peripheral nerves. Diabet Med 11: 279-285
[150] Barr EL, Wong TY, Tapp RJ, et al. (2006) Is peripheral neuropathy associated with retinopathy and albuminuria in individuals with impaired glucose metabolism? The 1999-2000 AusDiab. Diabetes Care 29: 1114-1116
[151] Nebuchennykh M, Løseth S, Jorde R, Mellgren SI (2008) Idiopathic polyneuropathy and impaired glucose metabolism in a Norwegian patient series. Eur J Neurol 15: 810-816
[152] Sahin S, Karsidag S, Ayalp S, Sengul A, Us O, Karsidag K (2009) Determination of nerve conduction abnormalities in patients with impaired glucose tolerance. Neurol Sci 30: 281-289
[153] Green AQ, Krishnan S, Finucane FM, Rayman G (2010) Altered C-fiber function as an indicator of early peripheral neuropathy in individuals with impaired glucose tolerance. Diabetes Care 33: 174-176
[154] Umapathi T, Tan WL, Tan NC, Chan YH (2006) Determinants of epidermal nerve fiber density in normal individuals. Muscle Nerve 33: 742-746
[155] Vincent AM, Hinder LM, Pop-Busui R, Feldman EL (2009) Hyperlipidemia: a new therapeutic target for diabetic neuropathy. J Peripher Nerv Syst 14: 257-267
[156] Wiggin T, Sullivan K, Pop-Busui R, Amato A, Sima A, Feldman E (2009) Elevated triglycerides correlate with progression of diabetic neuropathy. Diabetes 58: 1634-1640
[157] Nowicki M, Kosacka J, Serke H, Blüher M, Spanel-Borowski K (2011) Altered sciatic nerve fiber morphology and endoneural microvessels in mouse models relevant for obesity, peripheral diabetic polyneuropathy, and the metabolic syndrome. J Neurosci Res
[158] Davidson EP, Coppey LJ, Calcutt NA, Oltman CL, Yorek MA (2010) Diet-induced obesity in Sprague-Dawley rats causes microvascular and neural dysfunction. Diabetes Metab Res Rev 26: 306-318
[159] Kästenbauer T, Sauseng S, Brath H, Abrahamian H, Irsigler K (2004) The value of the Rydel-Seiffer tuning fork as a predictor of diabetic polyneuropathy compared with a neurothesiometer. Diabet Med 21: 563-567
[160] Martin CL, Waberski BH, Pop-Busui R, et al. (2010) Vibration perception threshold as a measure of distal symmetrical peripheral neuropathy in type 1 diabetes: results from the DCCT/EDIC study. Diabetes Care 33: 2635-2641
[161] Gin H, Rigalleau V, Baillet L, Rabemanantsoa C (2002) Comparison between monofilament, tuning fork and vibration perception tests for screening patients at risk of foot complication. Diabetes Metab 28: 457-461
[162] Meijer JW, Smit AJ, Lefrandt JD, van der Hoeven JH, Hoogenberg K, Links TP (2005) Back to basics in diagnosing diabetic polyneuropathy with the tuning fork! Diabetes Care 28: 2201-2205
71
[163] Perkins BA, Olaleye D, Zinman B, Bril V (2001) Simple screening tests for peripheral neuropathy in the diabetes clinic. Diabetes Care 24: 250-256
[164] Kamei N, Yamane K, Nakanishi S, et al. (2005) Effectiveness of Semmes-Weinstein monofilament examination for diabetic peripheral neuropathy screening. J Diabetes Complications 19: 47-53
[165] ��������������{���>�������������_�#���&������������&�$���$�������von Frey's hairs for the diagnosis of peripheral neuropathy in patients with type 2 diabetes mellitus. J Diabetes Complications 26: 319-322
[166] Nelander J, Speidel T, Björkman A, Dahlin LB (2012) Vibration thresholds are increased at low frequencies in the sole of the foot in diabetes-a novel multi-frequency approach. Diabet Med 29: e449-456
[167] Schmeichel AM, Schmelzer JD, Low PA (2003) Oxidative injury and apoptosis of dorsal root ganglion neurons in chronic experimental diabetic neuropathy. Diabetes 52: 165-171
[168] Srinivasan S, Stevens M, Wiley JW (2000) Diabetic peripheral neuropathy: evidence for apoptosis and associated mitochondrial dysfunction. Diabetes 49: 1932-1938
[169] Vincent AM, Brownlee M, Russell JW (2002) Oxidative stress and programmed cell death in diabetic neuropathy. Ann N Y Acad Sci 959: 368-383
[170] Nakagomi S, Suzuki Y, Namikawa K, Kiryu-Seo S, Kiyama H (2003) Expression of the activating transcription factor 3 prevents c-Jun N-terminal kinase-induced neuronal death by promoting heat shock protein 27 expression and Akt activation. J Neurosci 23: 5187-5196
[171] Sima AA (2003) New insights into the metabolic and molecular basis for diabetic neuropathy. Cell Mol Life Sci 60: 2445-2464
[172] Sundkvist G, Dahlin L, Nilsson H, et al. (2000) Sorbitol and myo-inositol levels and morphology of sural nerve in relation to peripheral nerve function and clinical neuropathy in men with diabetic, impaired, and normal glucose tolerance. Diabet Med 17: 259-268
[173] Kim H, Kim JJ, Yoon YS (2012) Emerging therapy for diabetic neuropathy: cell therapy targeting vessels and nerves. Endocr Metab Immune Disord Drug Targets 12: 168-178
[174] Scott JN, Clark AW, Zochodne DW (1999) Neurofilament and tubulin gene expression in progressive experimental diabetes: failure of synthesis and export by sensory neurons. Brain 122 ( Pt 11): 2109-2118
[175] Sima AA, Nathaniel V, Bril V, McEwen TA, Greene DA (1988) Histopathological heterogeneity of neuropathy in insulin-dependent and non-insulin-dependent diabetes, and demonstration of axo-glial dysjunction in human diabetic neuropathy. J Clin Invest 81: 349-364
[176] Sima AA, Bouchier M, Christensen H (1983) Axonal atrophy in sensory nerves of the diabetic BB-Wistar rat: a possible early correlate of human diabetic neuropathy. Ann Neurol 13: 264-272
[177] Cellek S (2004) Point of NO return for nitrergic nerves in diabetes: a new insight into diabetic complications. Curr Pharm Des 10: 3683-3695
72
[178] Cameron NE, Eaton SE, Cotter MA, Tesfaye S (2001) Vascular factors and metabolic interactions in the pathogenesis of diabetic neuropathy. Diabetologia 44: 1973-1988
[179] Nagamatsu M, Nickander KK, Schmelzer JD, et al. (1995) Lipoic acid improves nerve blood flow, reduces oxidative stress, and improves distal nerve conduction in experimental diabetic neuropathy. Diabetes Care 18: 1160-1167
[180] Stetler RA, Gao Y, Zhang L, et al. (2012) Phosphorylation of HSP27 by protein kinase D is essential for mediating neuroprotection against ischemic neuronal injury. J Neurosci 32: 2667-2682
[181] Yu A, Fuchshofer R, Birke M, Kampik A, Bloemendal H, Welge-Lüssen U (2008) Oxidative stress and TGF-beta2 increase heat shock protein 27 expression in human optic nerve head astrocytes. Invest Ophthalmol Vis Sci 49: 5403-5411
[182] Whitlock N, Lindsey K, Agarwal N, Crosson C, Ma J (2005) Heat shock protein 27 delays Ca2+-induced cell death in a caspase-dependent and -independent manner in rat retinal ganglion cells. Invest Ophthalmol Vis Sci 46: 1085-1091
[183] Huot J, Houle F, Marceau F, Landry J (1997) Oxidative stress-induced actin reorganization mediated by the p38 mitogen-activated protein kinase/heat shock protein 27 pathway in vascular endothelial cells. Circ Res 80: 383-392
[184] Read D, Gorman A (2009) Heat shock protein 27 in neuronal survival and neurite outgrowth. Biochem Biophys Res Commun 382: 6-8
[185] Devigili G, Tugnoli V, Penza P, et al. (2008) The diagnostic criteria for small fibre neuropathy: from symptoms to neuropathology. Brain 131: 1912-1925
[186] Ng N, Carlberg B, Weinehall L, Norberg M (2012) Trends of blood pressure levels and management in Västerbotten County, Sweden, during 1990-2010. Glob Health Action 5
[187] Ng N, Johnson O, Lindahl B, Norberg M (2012) A reversal of decreasing trends in population cholesterol levels in Västerbotten County, Sweden. Glob Health Action 5
[188] Selvarajah D, Wilkinson ID, Davies J, Gandhi R, Tesfaye S (2011) Central nervous system involvement in diabetic neuropathy. Curr Diab Rep 11: 310-322
[189] Wilkinson ID, Selvarajah D, Greig M, et al. (2013) Magnetic resonance imaging of the central nervous system in diabetic neuropathy. Curr Diab Rep 13: 509-516
[190] Scott LV, Tesfaye S (2001) Measurement of somatic neuropathy for clinical practice and clinical trials. Curr Diab Rep 1: 208-215
[191] Manor B, Newton E, Abduljalil A, Novak V (2012) The relationship between brain volume and walking outcomes in older adults with and without diabetic peripheral neuropathy. Diabetes Care 35: 1907-1912
[192] Franc DT, Kodl CT, Mueller BA, Muetzel RL, Lim KO, Seaquist ER (2011) High connectivity between reduced cortical thickness and disrupted white matter tracts in long-standing type 1 diabetes. Diabetes 60: 315-319
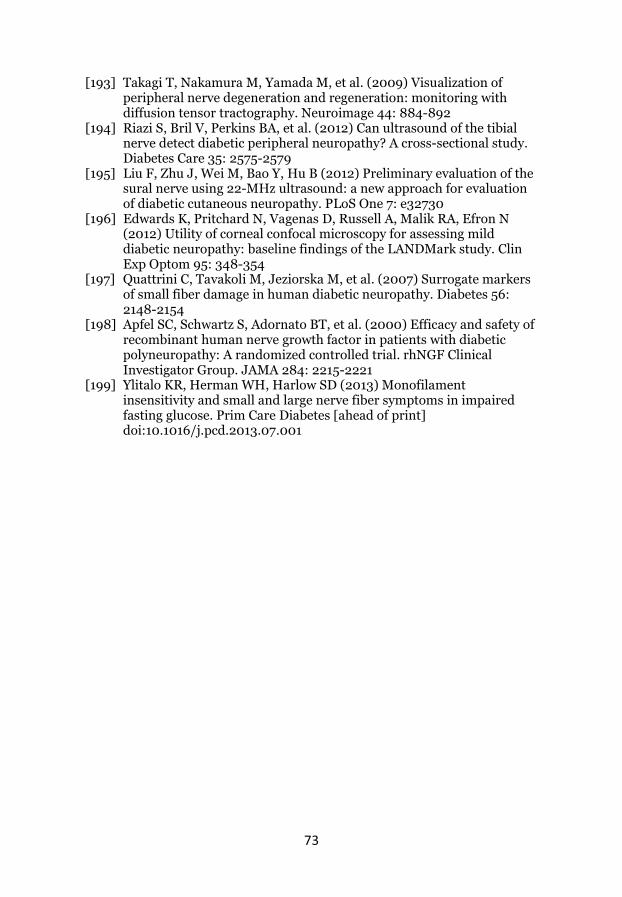
73
[193] Takagi T, Nakamura M, Yamada M, et al. (2009) Visualization of peripheral nerve degeneration and regeneration: monitoring with diffusion tensor tractography. Neuroimage 44: 884-892
[194] Riazi S, Bril V, Perkins BA, et al. (2012) Can ultrasound of the tibial nerve detect diabetic peripheral neuropathy? A cross-sectional study. Diabetes Care 35: 2575-2579
[195] Liu F, Zhu J, Wei M, Bao Y, Hu B (2012) Preliminary evaluation of the sural nerve using 22-MHz ultrasound: a new approach for evaluation of diabetic cutaneous neuropathy. PLoS One 7: e32730
[196] Edwards K, Pritchard N, Vagenas D, Russell A, Malik RA, Efron N (2012) Utility of corneal confocal microscopy for assessing mild diabetic neuropathy: baseline findings of the LANDMark study. Clin Exp Optom 95: 348-354
[197] Quattrini C, Tavakoli M, Jeziorska M, et al. (2007) Surrogate markers of small fiber damage in human diabetic neuropathy. Diabetes 56: 2148-2154
[198] Apfel SC, Schwartz S, Adornato BT, et al. (2000) Efficacy and safety of recombinant human nerve growth factor in patients with diabetic polyneuropathy: A randomized controlled trial. rhNGF Clinical Investigator Group. JAMA 284: 2215-2221
[199] Ylitalo KR, Herman WH, Harlow SD (2013) Monofilament insensitivity and small and large nerve fiber symptoms in impaired fasting glucose. Prim Care Diabetes [ahead of print] doi:10.1016/j.pcd.2013.07.001
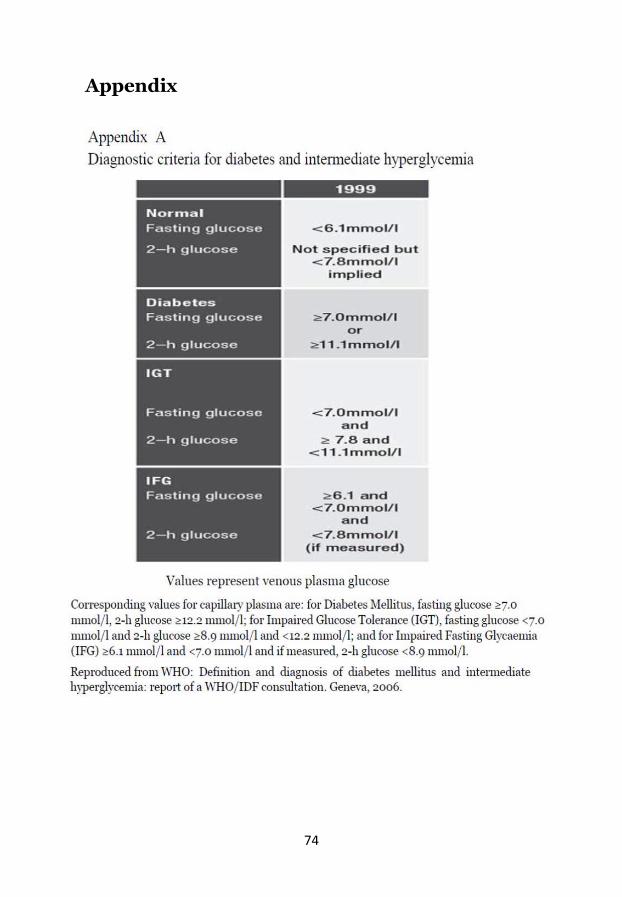
74
Appendix
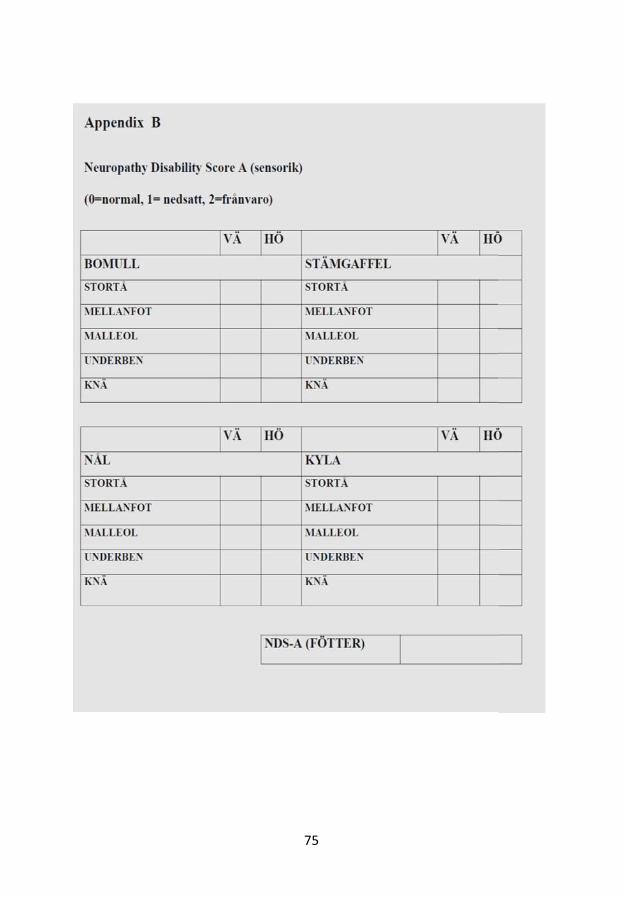
75
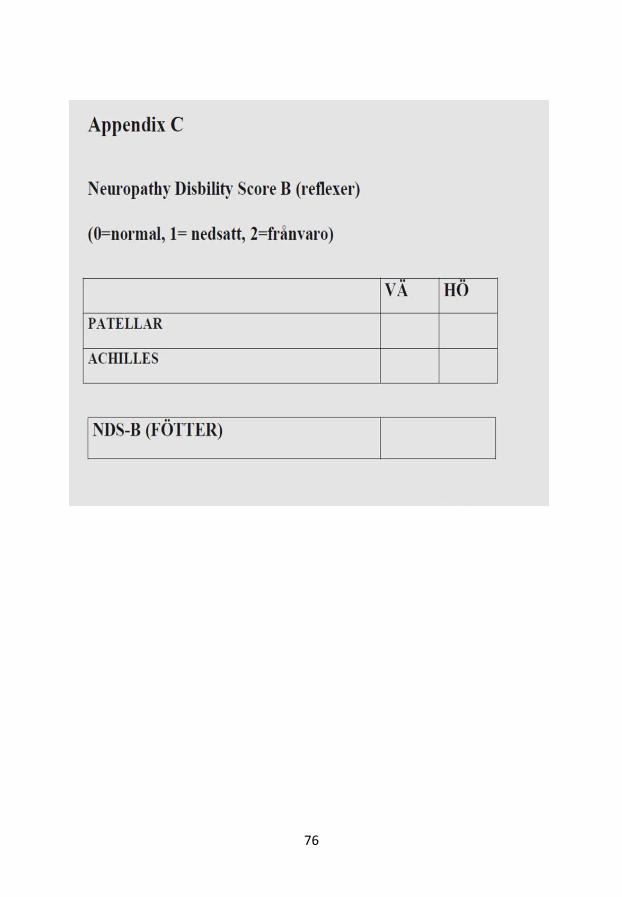
76
77