peripheral nerve imaging 2019 eposter 12.pdfnormal and abnormal appearance of nerves on both mri and...
TRANSCRIPT
Peripheral Nerve Imaging
DEPARTMENT OF RADIOLOGY AND IMAGING SCIENCES
A review of anatomy, imaging techniques, and selected pathologies
Ryan P. Joyce, MDPatrick H. Kobes, DORichard L. Leake, MD
Megan K. Mills, MD Sarah E. Stilwill, MD Hailey Allen, MD

Nothing to Disclose

Be familiar with the key anatomic landmarks and structures relevant to the most commonly imaged peripheral nerves
Understand the morphologic features of normal and abnormal peripheral nerves on MRI and US
Have developed a succinct and relevant differential diagnosis for abnormal findings
After review of this exhibit, the learner will:
Learning Objectives

MRI protocol considerations for peripheral neurography
Normal and abnormal appearance of nerves on both MRI and US
Practical tips for the sonographic evaluation of peripheral nerves
Anatomic review of commonly imaged nerves
Case-based review of pathology affecting peripheral nerves: • Entrapment/Compressive Neuropathy• Trauma• Tumor and Tumor-Like Conditions• Infectious and Inflammatory Pathology
Outline

MRI Protocol ConsiderationsAxial T1 Fat Suppressed (FS) Axial Proton Density (PD)
Used for assessment of: Nerve caliber and course Compressive bands or accessory muscles
Fascicular architecture Muscle atrophy/fatty infiltration Perineural fibrosis
Used for assessment of: Nerve caliber and course Compressive bands or accessory muscles
Fascicular architecture Muscle edema
Normal elbow with preserved perineural fat(arrow) about the ulnar nerve.
**
Coronal T1 imaging can also be useful in characterizing patterns of muscle atrophy.
Calf MRI (above and below) shows posterior and lateralcompartment fatty atrophy (asterisks) in a patient withCharcot-Marie-Tooth syndrome.
*
MRI of proximal calf in patient with Charcot-Marie-Tooth syndrome demonstrates enlarged fasciclesof the tibial nerve (arrow) and common peronealnerves (arrowhead).
Normal fascicular pattern and signal intensityassociated with the ulnar nerve (chevron) in thecubital tunnel.
Denervation edema involving the thenar musculature (arrowheads) in a patient withworsening weakness following a complicated carpel tunnel release.
Perineural fibrosis, seen as bands of hypointensetissue (arrowheads) around the median nerve(chevron) in a patient with worsening weaknessfollowing a complicated carpal tunnel release.
Sequence with highest signal-to-noise ratio

Coronal or Sagittal STIRUsed for assessment of: Denervation muscle edema; STIR is more sensitive than PD or T2 Denervated muscles should be downstream to the nerve injury
Post-Contrast Imaging
3D Nerve Imaging
Not necessary for routine nerve imaging
Can be added on in cases of tumor, infection, acute inflammation
Normal nerves demonstrate minimal or no enhancement in the setting of an intact blood-nerve barrier
Can demonstrate enhancement of denervated muscles
Excellent for assessment of: Nerve architecture, caliber,
fascicular pattern Nerve-selective and
maximum intensity projection techniques can be utilized
Can be acquired with variable weighting; fat suppressed T2 is the most common
Coronal STIR image of the thighs demonstratessubtle edema involving the muscles within theleft femoral nerve distribution (arrowheads) in apatient with a history of progressive weakness.
Homogeneously enhancing oval mass (arrow) alongthe course of the left common peroneal nerve,compatible with a peripheral nerve sheath tumor.
3D Coronal STIR SPACE image maximum intensity projection (MIP)image demonstratingnormal architecture of the lumbosacral plexus.
Sagittal STIR image of the elbow demonstratesnormal bulk and signal intensity of the muscles.
MRI Protocol Considerations

MRI Appearance of Peripheral NervesNormal Abnormal
On T1 weighted sequences, the median nerve (arrow) appears isointense to muscle with a peripheral hyperintense halo, representing the epineural fat (circle). High resolution MRI allows isointense nerve bundles to be distinguished within the hyperintense connective epi- and perineural tissue (arrowhead).
On fluid sensitive sequences (T2 FS, PD FS), the nerve demonstrates mild fluid signal. The fascicles(arrowheads) within the large nerve trunks exhibit a more pronounced hyperintensity secondary to the endoneural fluid.
On T1 weighted imaging, the left sciatic nerve (arrows) is markedly enlarged compared to the right in a patient with left sciatic mononeuropathy.
On T2 fat saturated imaging, the left sciatic nerve is markedly enlarged with fascicular edema (arrowhead) compared to the right (arrowhead).
On T1 fat saturated post gadolinium imaging, the left sciatic nerve is markedly enlarged with diffuse fascicular enhancement (arrowhead) compared to the right (arrowhead)which shows normal enhancement.
T1
Ax PD FS
T1
Ax PD FS
Ax T1 FS Post Gad

US Appearance of Peripheral NervesNormal Abnormal
Normal nerve fascicles are homogenouslyround and mildly hypoechoic on short axisimaging, with surrounding hyperechoicperineural fat.
Short axis US image of the ulnar nerve in the distal forearm (arrows) with anormal fascicular pattern and normal perineural fat. The normal mediannerve is partially included on this image (arrowhead).
Longitudinal US image of the tibial nerve in the popliteal fossa (arrowheads)demonstrates a normal fascicular pattern.
Short axis and longitudinal US images of an ulnar nerve, status post transposition due to severe ulnar neuropathy.
The fascicles are enlarged (arrows) and abnormally hypoechoic (arrowheads). Perineural fat in this case is preserved (chevrons).
Abnormal nerve fascicles are enlarged, can be heterogeneous in size, and are often more hypoechoic than normal nerves. Occasionally bands of hypointense perineural tissue, representing perineural fibrosis, can be seen.
Distal Humerus

Nerve Ultrasound: Practical Tips For most nerves, a high-frequency linear transducer will
provide the best image quality
Cine clips acquired in short axis are often better than static images for identifying and
characterizing small nerves
Optimize depth and focal zone settings for the nerve of interest
Long axis imaging is good for measuring segment length of abnormal nerves and for delineating the relationship of masses
and adjacent nerves.
Scanning the contralateral side for comparison can be useful for problem solving
Use short axis imaging for the evaluation of nerve caliber, fascicular pattern, and presence/absence of perineural fibrosis
Right Median NerveLeft Median Nerve
Tibial Nerve
Common Peroneal NerveCommon Peroneal Nerve

Anatomic Review of Commonly Imaged Nerves

The Radial Nerve
Common Extensor Muscle Group
RN Superficial Branch RN
Deep Branch RN
The radial nerve (RN) passes posterior to the mid humerus (HUM) at the level of the spiral
groove.
Ax T1 images of the right upper extremity, from proximal to distal, from the mid-humerus to the elbow joint
RNHUM
HUM
ULNULN
RAD
ULN
Superficial Branch RN
RAD
Triceps
Biceps
It then courses anteriorly within the lateral aspect of the
arm, deep to the common extensor muscles.
At the level of the radial head (RAD), the nerve splits into
superficial and deep branches. ULN = Ulna.
The deep branch of the RN continues as the Posterior Interosseous Nerve (PIN),
coursing between the superficial and deep fibers of the supinator muscle (SUP).
Posterior InterosseousNerve (PIN)
SUP
Origin Motor Function Sensory Function Associated Pathology
• Arises from the posterior cord of the brachial plexus
• Contributions from the C5, C6, C7, C8, and T1 nerve roots
• Triceps Brachii• Anconeus• Extensors of the hand/wrist
(mostly PIN)
• Dorsum of the upper arm • Dorsum of the forearm• Back of the thumb, index
finger, long finger, and ½ the ring finger
• Nerve injury associated with mid-shaft humerus fractures
• Posterior interosseous nerve (PIN) syndrome
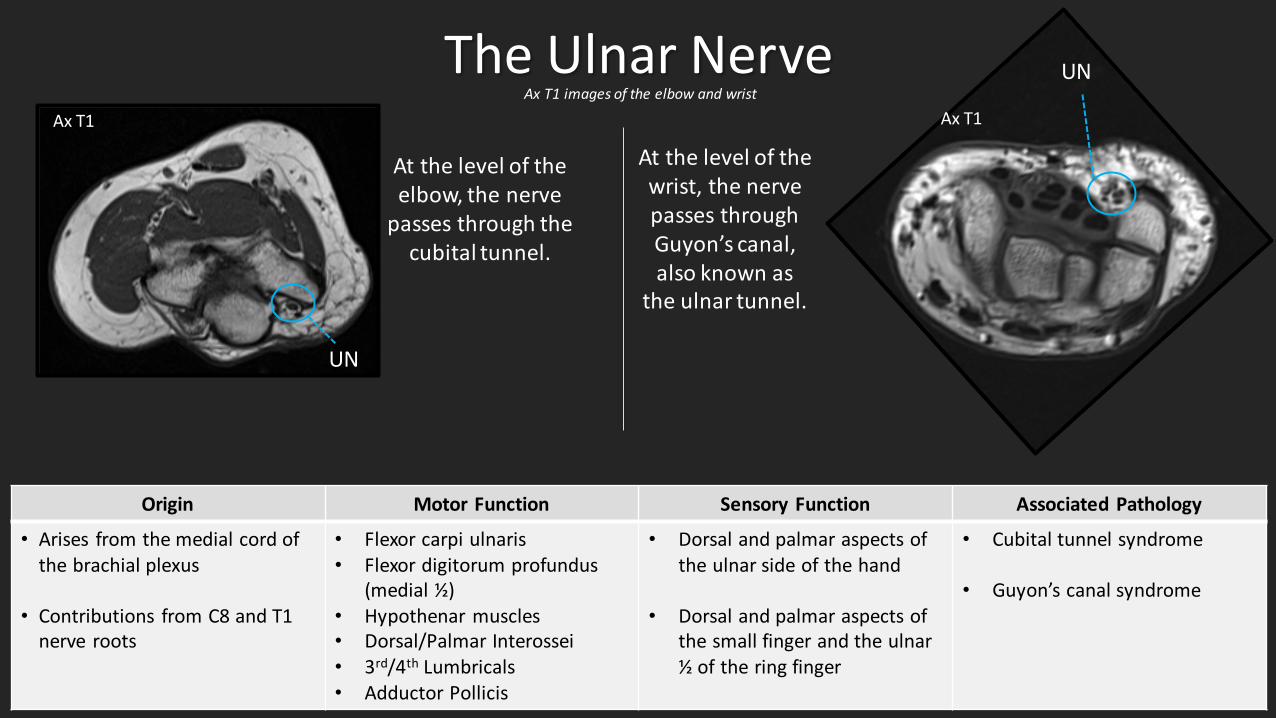
The Ulnar Nerve
Origin Motor Function Sensory Function Associated Pathology
• Arises from the medial cord of the brachial plexus
• Contributions from C8 and T1 nerve roots
• Flexor carpi ulnaris• Flexor digitorum profundus
(medial ½)• Hypothenar muscles• Dorsal/Palmar Interossei• 3rd/4th Lumbricals• Adductor Pollicis
• Dorsal and palmar aspects of the ulnar side of the hand
• Dorsal and palmar aspects of the small finger and the ulnar ½ of the ring finger
• Cubital tunnel syndrome
• Guyon’s canal syndrome
UN
UN
At the level of the wrist, the nerve passes through Guyon’s canal, also known as
the ulnar tunnel.
At the level of the elbow, the nerve
passes through the cubital tunnel.
Ax T1 Ax T1Ax T1 images of the elbow and wrist

The Sciatic Nerve
A-C) The sciatic nerve (circles) courses inferolaterally from the pelvis through the gluteal region. It is easiest to identify at the greatersciatic foramen (white circles) and as it courses over the ischial tuberosity (asterisks). It continues inferiorly within the posteriorcompartment of the thigh.
A) C)
* *
B)
Origin Motor Function Sensory Function Associated Pathology
• Arises from the L4-S3 nerve roots
• Contains fibers from the anterior and posterior divisions of the lumbosacral plexus
• Biceps femoris• Semimembranosus• Semitendinosus• Adductor magnus• Indirect motor function to the
lower leg via the tibial and peroneal nerves
• No direct sensory function
• Indirect sensory function via the tibial and peroneal nerves
• Piriformis syndrome
• Stump neuroma in BKA/AKA
• Sciatica (typically related to compression or irritation at the nerve root level)
Ax T1 images of the pelvis and proximal thigh, from proximal to distal
ST
AM
BF
AM = Adductor magnus, ST = Semitendinosus, BF = Biceps Femoris

The Femoral Nerve
A) Proximal segment of the femoral nerve (arrowhead) and obturator nerve(arrow) within the pelvis. From here, the femoral nerve will course partlywithin and/or along the psoas muscle and is difficult to visualize for severalcentimeters.
*
A)
Origin Motor Function Sensory Function Associated Pathology
• Derived from the anterior rami of the L2-L4 nerve roots
• Pectineus• Iliacus• Sartorius• Quadriceps femoris
• Anteromedial thigh (via anterior cutaneous branches)
• Medial leg and foot (via saphenous n.)
• Compression at the femoral canal/inguinal ligament
• Trauma (saphenous vein stripping)
Ax T1 images of the pelvis and proximal thigh, from proximal to distal
B) The femoral nerve (arrowhead) is easiest to identifywithin the femoral canal (white circle) just distal to theinguinal ligament. From lateral to medial, one canidentify the femoral nerve (arrowhead), artery, vein,and lymphatics (white dashed outline) within the canal.
B)

The Obturator Nerve
A-B) Proximal origin of the femoral nerve (arrowhead) and obturator nerve (arrow) within the pelvis. From here, theobturator nerve can be followed along the pelvic sidewall to the obturator canal (circle). C) Small branches (arrowheads) of the anterior and posterior
divisions of the obturator nerve are faintly seen within the fat planebetween adductor magnus, adductor brevis, and pectineus.
*
A) B) C)
Origin Motor Function Sensory Function Associated Pathology
• Arises from the anterior divisions of the L2-L4 nerve roots
• Adductor longus• Adductor brevis• Adductor magnus• Gracilis• Obturator externus
• Medial mid-thigh • Iatrogenic injury during abdominopelvic surgery
• Injury during childbirth• Entrapment within the canal
or obturator externus muscle
Ax T1 images of the pelvis and proximal thigh, from proximal to distal

A-B) As the sciatic nerve (dashed circle) travels down the posterior thigh compartment, itbifurcates as it enters the popliteal fossa into the tibial (arrow) and common peroneal(arrowhead) nerves. The tibial nerve then courses medially and deeper to travel inferiorlyin close proximity to the posterior tibia.
E) Tibial nerve seen posteriorto the tibia.
D) Tibial nerve interposed betweenpopliteus and the medial and lateralheads of gastrocnemius, partially seenon this image.
B)
D) E)
A)
C)
B)
The Tibial NerveAx T1 images of the distal thigh and proximal lower leg, from proximal to distal
Origin Motor Function Sensory Function Associated Pathology
• Arises from the sciatic nerve (L4-S3)
• Popliteus• Flexor hallicus longus• Flexor digitorum longus• Tibialis posterior• Plantaris• Soleus• Gastrocnemius
• Sole of the foot (via medial calcaneal branches, medial plantar nerve, and lateral plantar nerve)
• Posterolateral leg and lateral foot (via sural nerve)
• Tarsal tunnel syndrome
• Trauma
• Soleal sling syndrome

E) The common peroneal nervesplits into superficial and deepperoneal nerves (arrowheads)after wrapping around the fibularhead and neck.
D) Common peroneal nerve along theposterolateral aspect of the fibularhead (asterisk). Here, its superficialpositioning predisposes to injury,including direct trauma or stretchinjury secondary to fracture orposterolateral corner injury.
*
D) E)
*
The Peroneal NerveAx T1 images of the distal thigh and proximal lower leg, from proximal to distal
Origin Motor Function Sensory Function Associated Pathology
• Arises from the sciatic nerve (L4-S2)
• Short head of biceps femoris• Peroneus longus and brevis• Tibialis anterior• Extensor digitorum longus• Extensor hallicus longus• Several small intrinsic foot muscles
• Posterolateral leg and lateral foot (via sural nerve)
• Upper lateral leg (via lateral sural cutaneous nerve)
• Anterolateral leg and dorsum of foot (via superficial peroneal nerve)
• 1st intermetatarsal web space (via deep peroneal nerve)
• Fibular head fracture - direct trauma or stretch injury
A-C) As the sciatic nerve (dashed circle) travels down the posterior thigh compartment, itbifurcates as it enters the popliteal fossa into the tibial (arrow) and common peroneal(arrowhead) nerves. The common peroneal nerve then courses laterally along bicepsfemoris, around the lateral aspect of the fibular head (asterisk), and down theanterolateral compartment of the lower leg.
A) B)
*C)
Case Based Review
Entrapment/Compressive Neuropathy TraumaTumor and Tumor-Like Conditions Infectious and Inflammatory Pathology

Compressive Neuropathy
MRI images of the right shoulder shows a nondisplaced posterior-superior labral tear(arrowhead) with a large paralabral cyst (arrows) extending along the medial glenoidand into the spinoglenoid notch (yellow arc) and the suprascapular notch (blue arc).There is denervation atrophy involving the infraspinatus muscle (chevrons) with normalsignal of the supraspinatus muscle, consistent with denervation related to compressionof the distal suprascapular nerve.
Axial PD FS
Spinoglenoid Notch Cyst: Suprascapular NerveSag T2 FS
Cor T2 FS
32-year old male with right shoulder pain.
Compressive Neuropathies in the Shoulder
Nerve Location of Compression
Causes Typical Muscle Denervation Pattern
Suprascapular
Suprascapular notch (proximal)
Spinoglenoid notch (distal)
• Para labral cyst• Fracture• Tumor• Hypertrophied or
anomalous spinoglenoidl igament or transverse scapular l igaments
Compression proximal to spinoglenoid notch:
supraspinatus + infraspinatus
Compression distal to spinoglenoid notch: infraspinatus only
Axil lary Quadrilateral space
• Fibrous band• Juxta-articular cyst • Fracture• Tumor
DeltoidTeres minor

Posterior Interosseous Nerve (PIN) Syndrome
Compressive Neuropathy
68-year old man with right elbow weakness, numbness and tingling after an altercation several months prior to presentation.
Axial PD FS Axial T1 Axial T1 FS Post
There is denervation edema of the supinator muscle (arrowheads), with associated fatty infiltration (chevrons) and mild post-contrastenhancement (arrows). There is focal enlargement and increased signal of the posterior interosseous nerve (arrow).
The deep branch of the radial nerve, also known as the
posterior interosseous nerve, courses between the two heads
of the supinator muscle
There are numerous described causes of compression of the PIN, although not all are appreciated by imaging:
• Leash of Henry: A fan-shaped network of branches of the radial artery • Arcade of Frohse: a fibrous band located between the heads of the supinator muscle• Distal edge of the supinator or edge of the extensor carpi radialis

Peroneal Neuropathy: Compressing Ganglion Cyst
Compressive Neuropathy
25-year old man with progressive right leg numbness and paresthesias along the proximal lateral lower leg and along the dorsum of the foot.
Axial PD FS Cor T2 FSCor T1
There is a multiloculated ganglion cyst located at the lateral margin of the fibular head (arrowheads). The common peroneal nerve(arrows) takes an elongated course around the cyst. The nerve itself is increased in caliber and increased in signal intensity, but itsnormal fascicular pattern is preserved. There is denervation edema of the peroneus longus muscle (asterisks). The cyst was surgicallyresected and the patient’s symptoms improved.
Sag T2 FS
*
**

Trauma
Traumatic Axonotmesis: Radial Nerve52-year old woman with right wrist extensor weakness and intermittent numbness in the distribution of the radial nerve, status post
ORIF for humeral diaphysis fracture incurred from a ground level fall.
Humerus radiograph demonstrates stabilization plate and screwsassociated with a comminuted humeral diaphysis fracture (chevrons).Diagnostic US reveals enlargement of the radial nerve (arrows) beginning atthe level of the spiral groove adjacent to the surgical plate (asterisk).Distally, the posterior interosseous nerve (arrowhead) is identified as itcourses between the deep and superficial heads of the supinator muscle(dashed lines). The nerve is markedly enlarged and has lost its normalfascicular pattern.
Short Axis US – Level of Spiral GrooveAP View of R Humerus
Short Axis US – Level of Proximal Radius*
Class Description MRI Findings Recovery Potential
I Nerve stretch injury (neurapraxia)
Normal nerve caliber but with abnormally increased T2 signal. Full
II Axonal injury (axonotmesis)with intact endoneurium
Nerve is enlarged and abnormally T2 hyperintense. Fascicular pattern preserved. Full
III Axonal injury (axonotmesis)with disrupted endoneurium
Enlarged, hyperintense nerve with enlarged or effaced fascicles. + Denervation changes.
SlowPartial
IVEndoneurium + perineurium disrupted; epineurium intact
(neuroma-in-continuity)
Focally enlarged nerve with disrupted fascicles. + Denervation changes. Poor
V Transected nerve (neurotmesis) Complete nerve discontinuity. Over time neuroma can develop. +Denervation changes. None
Sunderland Classification of Nerve Injuries*
*Chhabra Indian J Radiol Imaging 2014

The proximal stump neuroma (dashed circle) demonstrates homogeneous
enhancement surrounding the distal nerve fascicles (arrowheads).
There is transection of the sciatic nerve with a2 cm gap (dashed line) between the torn ends(arrows) and a stump neuroma (arrowheads)at the proximal nerve end.
A stump neuroma is a disorganized proliferation of nerve fascicles after injury to a nerve whichforms at the proximal nerve ending as it attempts to regenerate. They are most commonlyencountered in amputees but, as in this case, can be seen after any nerve transection.
The distal stump (dashed circle) is shown. There is no enhancing stump neuroma at
the distal nerve end, supporting the philosophy that only the proximal nerve end attempts to regenerate after injury.
Trauma
Traumatic Neurotmesis with Neuroma: Sciatic Nerve50-year-old male with history of a horse riding accident one year prior, with total loss of sensation
and function of the left lower leg and foot.
Sag T2 Sag T2 Ax T1 FS Post Ax T1 FS Post

Both sciatic nerves are shown (dashed outline). Interval neuroma resection
and nerve reapproximation shown on the left. Note the T1 hypointense
granulation tissue (arrowhead) at the site of nerve repair.
Diffuse T2 hyperintense denervation edema (arrows) throughout the
partially imaged musculature of the proximal lower leg.
Minimal enhancement of the granulation tissue (arrowhead) surrounding the
repaired nerve ends. 3 consecutive axial images show the enhancing granulation
tissue surrounding the otherwise contiguous repaired sciatic nerve (dashed
circle). Several small nerve fascicles (punctate low signal foci) are seen bridging
the granulation tissue.
Trauma
Traumatic Neurotmesis with Neuroma: Sciatic NerveStatus post neuroma resection and repair.
Sag T2 Ax T1 FS Post
Ax T1 FS Post
Ax T1 FS Post
Cor T1 FS Post Ax T2 FS

Traumatic Neurotmesis: Peroneal Nerve24-year-old male struck by motor vehicle with knee pain and foot drop.
Marked enlargement and hyperintensity of the peroneal nerve (arrowheads) as it courses over the
lateral aspect of the fibular head (asterisk), where it is most vulnerable to direct impact and stretch injury in
the setting of trauma.
More proximally, at the level of the tibial plateau (asterisk) abnormal anterior course and redundancy of the transected peroneal nerve (dashed outline) is partially shown. The transected nerve stump is well seen
(arrowheads).
Peroneal nerve origin proximal to the transection demonstrates mild enlargement and
hyperintensity (arrowhead). Adjacent normal tibial nerve (arrow).
Ax PD FSCor T2 FS
*
Ax PD FS
Trauma
*

Images distal to the nerve transection demonstrate enlargement and hyperintensity of the peroneal nerve (arrowheads) anddenervation edema (arrows) within the tibialis anterior, extensor digitorum longus, and peroneus longus muscles innervated by theperoneal nerve.
Ax PD FS
Trauma
Traumatic Neurotmesis: Peroneal Nerve (Continued)24-year-old male struck by motor vehicle with knee pain and foot drop.
Ax PD FS

Peripheral Nerve Sheath Tumor (PNST)56-year old man presenting with pain and weakness of the left forearm and hand. The patient reports paresthesias in the thumb and
forefinger when carrying a grocery bag looped over his forearm.
Long Axis US B)
**
Imaging in the area of maximal tenderness demonstrates a well-circumscribed,
hypoechoic mass (asterisk) in the volar, radial aspect of the forearm among the flexor
compartment muscles. The fascicles of the median nerve (arrowheads) diverge around
the mass. There is a small triangle of fat (arrow) at the apex of the mass.
Cor T1
Ax T1 FS Post
Ax PD FS
MRI of the forearm confirms a well circumscribed mass (asterisks) arising from the center of the median nerve
(arrowheads). The mass is hyperintense to skeletal muscle on T1 weighted
imaging, homogeneously hyperintense on T2 weighted imaging, and enhances
homogenously.
*
*
*
The mass was surgically resected; pathology was consistent with a
schwannoma.
Tumor and Tumor-Like

Tumor and Tumor-Like
Malignant Peripheral Nerve Sheath Tumor (MPNST)22-year old man with a history of neurofibromatosis type I presents with a growing left elbow mass.
There is a fusiform mass arising from the ulnar nerve just above the elbow (asterisks). The mass is T2 hyperintense, but with central areas of central hypointensity (arrows). The mass enhances on post contrast images, but with peripheral areas of non-enhancement (chevrons). The
mass was resected; histology was consistent with a high-grade malignant nerve sheath tumor.
Additional small T2 hyperintense nodules along the course of the brachial plexus near the axilla, consistent
with small neurofibromas (arrowheads).
Sag T2 FS Ax PD FS Cor T1 FS Post
Ax T1 FS Post
*
*
* *
Imaging does not consistently differentiate between benign and malignant nerve sheath tumors. Features more characteristic of malignant tumors include:
Large tumor size Rapid growth in size or worsening pain
Infiltrative margins Larger lesions, history of NF1, and truncal
location all predict higher mortality Perilesional edema Central hypointensity on T2 weighting, which is
suggestive of central necrosis or hemorrhage
Peripheral rather than central enhancement

Tumor and Tumor-Like
Lipofibromatous Hamartoma of Median Nerve
Ax T1 Ax PD FS
Marked enlargement of the median nerve fascicles (arrows)with increased T1 hyperintense fat (arrowheads) surrounding each individual fascicle is shown. This appearance has been
likened to a coaxial cable.
Proton density imaging better demonstrates that the apparent fascicular enlargement reflects intermediate
signal intensity fibrosis (arrow) surrounding each central low signal intensity nerve fascicle (arrowhead). Note the fat signal has been suppressed (asterisk). There is mass effect
as evidenced by volar bulging of the flexor retinaculum (chevrons) and dorsal displacement of the flexor tendons
within the carpal tunnel (dashed arc).
*
28-year-old female with 15-year history of a “bump” on her left wrist, with recent development of numbness and tingling involving the second and third digits.
A lipofibromatous hamartoma is a rare and slow growing benign fibro-fattytumor, characterized by proliferation of mature adipocytes within theepineurium and the perineurium of the peripheral nerves. The median nerve isthe most common site of involvement, typically leading to pain, numbness, andparesthesia within the median nerve distribution of the hand (carpal tunnelsyndrome).

Vascular Malformation
C)
DDx
**
MRI images demonstrate a large infiltrating mass in the forearm
(asterisks) involving both the volar and dorsal muscle compartments. There
are areas of interspersed fat (chevrons)and scattered hypointense phleboliths
(arrowheads). There is progressive enhancement between the axial post-contrast image, acquired early, and the
coronal image, acquired late. No associated flow voids are present.
8-year old boy presenting with a slowly growing, soft painless mass involving the left forearm.
Ax T1 Ax PD FS
Ax T1 FS Post
Cor T1 FS Post
The mass encases the superficial branch of the radial nerve (open arrow)and abuts the deep margin of the median nerve (arrow). Findings are mostcompatible with a venous malformation.
*
*
*
*Key MRI Features of Vascular Malformations• Transpatial lesions involving multiple muscle
compartments, can involve bone • Venous malformations: phleboliths and progressive
enhancement• Lymphatic malformations: fluid-fluid levels and
minimal septal/peripheral enhancement • Arteriovenous malformation: flow voids indicating
fast arterial flow with large draining veins • Combination lesions are common (i.e.
venolymphatic malformation). • Associated with syndromes: Klippel-Trenaunay,
Maffucci, Parkes-Weber, etc.
Tumor and Tumor-Like

Infectious Ulnar Neuritis
The transposed ulnar nerve (arrows)is markedly enlarged, abnormally STIR hyperintense, with a thick rind of abnormal enhancement, and is situated anteromedial to the cubital tunnel. It is located within a soft tissue abscess in the posteromedial arm (arrowheads). Adjacent susceptibility artifacts (asterisk) are related to prior fracture repair and nerve transposition.
78-year old male with elbow pain, swelling and paresthesias. History of remote elbow fracture fixation, underwent ulnar nerve transposition 5 months prior to presentation.
Ax T1
Infection/Inflammation
*
Ax T1 Post Sag STIR
Management of Perineural Infection• Conservative management with IV antibiotics • Incision/debridement of perineural abscess with stripping of the nerve itself may be indicated, as
was done in this case

49-year old female with right shoulder pain and progressive weakness.
Infection/Inflammation
Parsonage-Turner Syndrome: Idiopathic Brachial Neuritis
Sag T1 Sag T2 FS
Cor T2 FS
MRI images of the right shoulder show extensive edema in the deltoid(chevrons), supraspinatus (circle/oval) and infraspinatus (blue ovals) musculature.There is no corresponding atrophy on T1 weighted imaging.
Nerve Muscles Causes Treatment
Suprascapular (97%), axil lary and
subscapular nerves can also be involved
Most frequently supraspinatus and
infraspinatus (innervated by suprascapular
nerve) followed by deltoid (innervated
by axil lary nerve)
Uncertain. Viral and
autoimmune etiologies
postulated
Self Limiting. Weakness can last
for years though majority of
patients recover to normal function.

Conclusion The imaging evaluation of patients who present with
symptoms of peripheral nerve pathology is complex and requires a targeted, high quality, often multimodal investigation.
Knowledge of normal nerve anatomy and imaging characteristics, sites of common injury, and the expected MR and US manifestations of pathology are key to accurately protocoling, localizing, and characterizing nerve abnormalities.
A radiologist proficient in multimodal nerve imaging can prove invaluable for any practice or institution, and can significantly contribute to the optimal management of these complicated patients.

Kwee RM, Chhabra A, Wang KC, Marker DR, Carrino JA. Accuracy of MRI in diagnosing peripheral nerve disease: a systematic review ofthe l iterature. AJR Am J Roentgenol. 2014;203(6):1303-9. Epub 2014/11/22. doi: 10.2214/AJR.13.12403. PubMed PMID: 25415709.
Zhang H, Xiao B, Zou T. Cl inical application of magnetic resonance neurography in peripheral nerve disorders. Neurosci Bull. 2006;22(6):361-7. Epub 2007/08/11. PubMed PMID: 17690722.
Yanny, Sarah, Andoni P. Toms. MR Patterns of Denervation Around the Shoulder. American Journal Of Roentgenology, vol . 195, no. 2, 2010, pp. W157–W163.
Andreisek G, Cook DW, Burg D, Marincek B, Weishaupt D. Peripheral Neuropathies of the Median, Radial and Ulnar Nerves: MR Imaging Features. RadioGraphics 2006 26:5, 1267-1287
Wasa, Junji, et al. MRI Features in the Differentiation of Malignant Peripheral Nerve Sheath Tumors and Neurofibromas. AJR. American Journal of Roentgenology, vol . 194, no. 6, 2010, pp. 1568–74.
Carpenter EL, Bencardino JT. Focus on advanced magnetic resonance techniques in clinical practice: magnetic resonance neurography. Radiol Cl in North Am. 2015;53(3):513-29. Epub 2015/05/09. doi : 10.1016/j.rcl .2014.12.002. PubMed PMID: 25953287.
Chhabra A. Peripheral MR neurography: approach to interpretation. Neuroimaging Clin N Am. 2014;24(1):79-89. Epub 2013/11/12. doi: 10.1016/j.nic.2013.03.033. PubMed PMID: 24210314.
Konjengbam, M. and Elangbam, J. (2004), Radial nerve in the radial tunnel: Anatomic sites of entrapment neuropathy. Cl in. Anat., 17: 21-25. doi:10.1002/ca.10194
Kamath S, Venkatanarasimha N, Walsh MA, Hughes PM. MRI appearance of muscle denervation. Skeletal Radiol. 2008;37(5):397-404. Epub 2008/03/25. doi: 10.1007/s00256-007-0409-0. PubMed PMID: 18360752.
Ahlawat S, Chhabra A, Blakely J. Magnetic resonance neurography of peripheral nerve tumors and tumorlike conditions. Neuroimaging Clin N Am. 2014;24(1):171-92. Epub 2013/11/12. doi : 10.1016/j.nic.2013.03.035. PubMed PMID: 24210319.
Crush AB, Howe BM, Spinner RJ, Amrami KK, Hunt CH, Johnson GB, et al. Malignant involvement of the peripheral nervous system in patients with cancer: multimodality imaging and pathologic correlation. Radiographics. 2014;34(7):1987-2007. Epub 2014/11/11. doi: 10.1148/rg.347130129. PubMed PMID: 25384297.
Bal todano PA, Tong AJ, Chhabra A, Rosson GD. The role of magnetic resonance neurography in the postoperative management of peripheral nerve injuries. Neuroimaging Clin N Am. 2014;24(1):235-44. Epub 2013/11/12. doi: 10.1016/j.nic.2013.03.029. PubMed PMID: 24210322.
Chhabra A, Ahlawat S, Belzberg A, Andreseik G. Peripheral nerve injury grading simplified on MR neurography: As referenced to Seddon and Sunderland classifications. Indian J Radiol Imaging. 2014;24(3):217-24. Epub 2014/08/13. doi: 10.4103/0971-3026.137025. PubMed PMID: 25114384; PubMed Central PMCID: PMCPMC4126136.
Shekhani HN, Hanna T, Johnson JO. Lipofibromatous Hamartoma of the Median Nerve: A Case Report. J Radiol Case Rep. 2016;10(11):1-7. Published 2016 Nov 30. doi :10.3941/jrcr.v10i11.2787
References

We hope you enjoyed our exhibit. Please direct any questions or comments for
the authors to [email protected]
#SSRBONE19Poster12