perspectives on childhood obesity prevention ... · perspectives on childhood obesity prevention:...
TRANSCRIPT

Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
The Johns Hopkins Center for a Livable FutureBloomberg School of Public Health
615 N. Wolfe Street, E2150Baltimore, MD 21205-2179
www.jhsph.edu/clf410.502.7578
About the Johns Hopkins Center for a Livable FutureFounded in 1996, the Johns Hopkins Center for a Livable Future promotes research and communicates information about the complex interrelationships among diet, food production, the natural environment and human health. As an interdisciplinary center it serves as a resource to solve problems that threaten the health of the public and hinder our ability to sustain life for future generations.
About the Bloomberg School’s Department of Health, Behavior and Society The Department of Health, Behavior and Society was established in 2005 with a mission dedicated to research and training that advances scientific understanding of the impact on health of behavior and the societal context.
Document prepared by:
The Johns Hopkins Center for a Livable Future and The Department of Health, Behavior and Society
Melissa Gilkey
Acknowledgements:The authors would like to thank Robert S. Lawrence, Roni Neff, Sara Bleich, Shawn McKenzie, David Holt-grave, and Anne Palmer for their helpful review comments. Any errors contained in this document are the sole responsibility of the authors.
Winter 2007

�Winter 2007
Table of Contents
I. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2II. Background:DescribingtheBurdenofObesity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3III. Measurement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 • Develop intermediate measures to better evaluate prevention programs. . . . . . . . . . . . . . . . . . . . . . . 6 Spotlight: Leslie Lytle, PhD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8IV. TheSchoolEnvironment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 • Provide at least 30 minutes of moderate to vigorous physical activity. . . . . . . . . . . . . . . . . . . . . . . . . 9 • Encourage the consumption of healthy foods by increasing the number of healthy options and pricing them competitively. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 • Provide high-quality health education in areas such as nutrition and physical fitness. . . . . . . . . . . . . . . 10 Spotlight: Benjamin Caballero, MD, PhD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11V. TheBuiltEnvironmentandNeighborhoodFactors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 • Make communities more walk-able and bike-able. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 • Increase access to healthy foods.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 Spotlight: Penny Gordon-Larsen, PhD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13VI. Marketing,Industry,andPublicPolicy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 • Advocate for regulation of youth marketing. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 • Strengthen consumers’ ability to make informed food choices, access appropriate and accurate information, and take an active role in influencing food policy. . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 Spotlight: David Wallinga, MD. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15VII. TheEthnicityGapandCulturalContexts. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 • Engage local governments and community groups, particularly those most affected by obesity, in community and policy interventions.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 Spotlight: Shiriki Kumanyika, PhD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17VIII. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19AppendixI:ReportsReviewed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23AppendixII:KeyInformants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23

2 Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
I. Introduction
1 Because much of the research related to the issue of childhood obesity is school-based, this report considers both children and adolescents under the age of 18 with an emphasis on those of elementary- and middle-school age.
In less than a decade the issue of childhood obesity has become a leading public health concern in the U.S. In part, obesity’s new prominence is the result of its increas-ing prevalence. Data indicate the condition is widespread and ever-growing for Americans across many socio- demographic categories including children and adoles-cents1 (Wang & Beydoun, 2007). Obesity has often been described as a crisis of epidemic, and even pandemic, proportions (Kimm & Obarzanek, 2002), and is pro-jected to affect almost one in four American children by 2015 (Wang & Beydoun, 2007).
Obesity is complex and controversial. Despite extensive debate in scientific and lay communities, no single reason has been found to explain why obesity rates have risen so dramatically, nor has an agreement been reached as to how to reverse these trends. With most to lose in terms of years of life, children and adolescents are prominent in obesity discussions, which are particularly fraught in light of the fact that obesity-related behaviors such as eating and physical activity are inextricably linked to the broader cultural and social contexts of parenting, schooling, and policymaking. Increasingly, obesity is understood as a societal and environmental problem, rather than a purely individual or moral one, but researchers are still uncertain about which factors within the vast causal web are most important and changeable. Against this backdrop, interest in and funding for obesity-related research has increased in recent years, with the National Institutes of Health (NIH), for example, supporting over 270 child-specific obesity projects over the last five years (Huang & Horlick, 2007) and the Robert Wood Johnson Foundation award-ing over $40 million in obesity-related grants in 2006 alone (RWJF, 2007).
In absence of an easy cure, obesity researchers from all backgrounds have stressed prevention. Biomedical scientists, for example, have sought to better understand metabolic mechanisms associated with childhood obe-
sity, while social scientists and prevention specialists have highlighted the importance of health behavior and educa-tion, lifestyle factors, psychosocial contexts, and the built environment, among other areas. Each focus has offered a particular perspective on obesity in children, and each has resulted in a different set of preliminary recommenda-tions and suggestions for continued work. Although most scientists agree that a multi-pronged, ecological approach is needed for effective prevention, the sheer number and diversity of recommendations make it challenging to select the best intervention for a particular situation. Nevertheless, given the stakes involved, public health researchers and practitioners must press forward with prevention efforts, following the Institute of Medicine’s dictate to act on the “best available evidence—as opposed to waiting for the best possible evidence” (2005, p. 3).
This report identifies areas of growing consensus regard-ing recommendations for childhood obesity prevention by leaders in the public health community. It was inspired by a 2006–2007 seminar series at the Johns Hopkins Bloomberg School of Public Health organized and sponsored jointly by the School’s Department of Health, Behavior and Society and the Center for a Livable Future. Based on interviews with experts featured in the seminar and prominent reports on childhood obesity (see Appen-dices I and II). This paper identifies promising areas of action in key social arenas: the school environment, the built environment, policymaking, and ethnic and cultural contexts. Recommendations related to issues of measure-ment are also discussed. In addition, leading researchers in obesity prevention are highlighted throughout the report in order to introduce various individual perspec-tives on the topic. By taking a look at childhood obesity prevention research and interventions to date, this report aims to help public health researchers and practitioners gain insight into its particular challenges and opportuni-ties for investigation and implementation.
�Winter 2007
II. Background: Describing the Burden of Childhood Obesity Prevalence
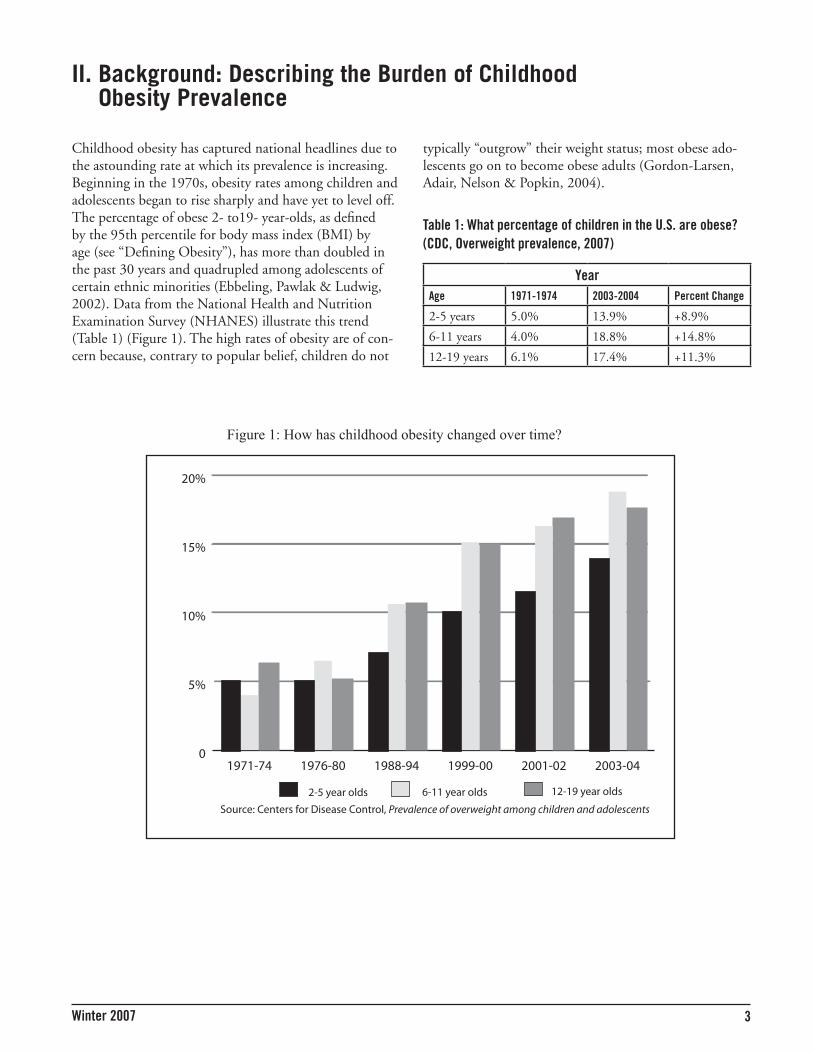
Childhood obesity has captured national headlines due to the astounding rate at which its prevalence is increasing. Beginning in the 1970s, obesity rates among children and adolescents began to rise sharply and have yet to level off. The percentage of obese 2- to19- year-olds, as defined by the 95th percentile for body mass index (BMI) by age (see “Defining Obesity”), has more than doubled in the past 30 years and quadrupled among adolescents of certain ethnic minorities (Ebbeling, Pawlak & Ludwig, 2002). Data from the National Health and Nutrition Examination Survey (NHANES) illustrate this trend (Table 1) (Figure 1). The high rates of obesity are of con-cern because, contrary to popular belief, children do not
YearAge �97�-�974 200�-2004 Percent Change
2-5 years 5.0% 13.9% +8.9%
6-11 years 4.0% 18.8% +14.8%
12-19 years 6.1% 17.4% +11.3%
typically “outgrow” their weight status; most obese ado-lescents go on to become obese adults (Gordon-Larsen, Adair, Nelson & Popkin, 2004).
Table �: What percentage of children in the U.S. are obese? (CDC, Overweight prevalence, 2007)
0
5%
10%
15%
20%
12-19 year olds6-11 year olds2-5 year olds
2003-042001-021999-001988-941976-801971-74
Source: Centers for Disease Control, Prevalence of overweight among children and adolescents
Figure 1: How has childhood obesity changed over time?

4 Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
Defining Obesity
Debates surrounding childhood obesity extend even to its definition. In adult popula-tions, body mass index (BMI), as calculated by weight in kilograms divided by the square of height in meters, is the most common measure of the condition. A BMI of 18.5 to 24.9 is considered healthy, while a score of 25 to 29.9 is classified as overweight, 30 to 34.9 is obese, and 35 and above is morbidly obese.
In children and adolescents, BMI scores are not interpreted alone, but are considered in terms of percentiles by age and sex in order to better account for growth patterns. Some public health authorities define childhood obesity as a score at or above the 95th percentile for BMI by age, while overweight is used to describe the 85th to 95th percentiles. However, others, including the Centers for Disease Control and Prevention (CDC), prefer not to use the term obese in regard to children in order to acknowledge the shortcomings of BMI as a pediatric measure; these practitioners describe children at and above the 95th percentile as overweight, and those between the 85th and 95th percentiles as at risk for overweight (CDC, Defining Overweight and Obesity, 2007). This report uses the former classifications of obese and overweight with a more extensive discussion of BMI and its limitations provided in subsequent sections.
Health EffectsIllness. Childhood obesity was once framed primarily in terms of its long-term consequences. In particular, researchers emphasized that the condition was associ-ated with increased risk of cardiovascular disease, type II diabetes, and some cancers later in life. Today, however, experts know that childhood obesity has more immediate effects as well:
• TypeIIdiabetes, once virtually unknown in children, now accounts for up to 45 percent of all new pediatric diabetes cases and is more often found in obese youth (Fagot-Campagna, Pettitt, Engelgau, Burrows, Geiss, Valdez, et al., 2000). Estimating the prevalence of type II diabetes in children is difficult given low levels of surveillance and variations across sub-populations. However, using adult-specific data, the first estimates of lifetime risk for diabetes were recently calculated to suggest that the disease will eventually affect 33 percent of boys and 39 percent of girls among children born in 2000 if current trends continue (Narayan, Boyle, Thompson, Sorensen & Williamson, 2003).
• Adolescents and younger children suffer psychologi-calandsocialeffects related to obesity. Obese teens are more likely to have poor self-image and low body satisfaction (Strauss & Pollack, 2003) and experience weight-related teasing. This teasing has been linked to symptoms of depression, including thoughts of suicide, for male and female adolescents in varying degrees across ethnic groups (Eisenberg, Neumark-Sztainer, & Story, 2003).
• Obesity in youth is also associated with asthma, sleepapnea, and highbloodpressure (CDC, Consequences, 2007).
Death. From a longer term perspective, the increase in cardiovascular disease and diabetes associated with obesity also has serious consequences in terms of increased mor-tality. Among adults, approximately 300,000 deaths are associated with the condition each year (CDC, Conse-quences, 2007), and these numbers are likely to increase as today’s children grow older. In fact, some researchers project that because of the rise in type II diabetes, today’s population of children may be the first generation in over a century to experience lowerlifeexpectancy than their parents (Fontaine, Redden, Wang, Westfall & Allison, 2003).
Economic costs. In addition to illness and early death, the burden of obesity is often conveyed in financial terms. For example, in the general population obesity-related health care costs are estimated to have totaled over $117 billion in 2000 (U.S. Department of Health & Human Services, 2007). Because obesity is associated with increased absenteeism from work and school, the condi-tion is associated with lost productivity as well (Nord, Andrews, & Carlson, 2005).
At the same time, it must be recognized that weight is not always the ideal predictor of health. For example, some people who are heavy but physically active may be health-ier than others who are slim but sedentary (Romero-Cor-ral et al., 2006). Pressure to lose weight may backfire in
�Winter 2007
the ongoing epidemic of eating disorders and widespread unhealthy emotional relationships with food, especially among girls, and in our cultural obsession with body image and dieting (Schwartz & Brownell, 2007). These pressures can actually contribute to increasing obesity and mental health problems. Effective public health interven-tions to address obesity must steer a careful path to avoid worsening these negative outcomes (Bauer et al., 2006).
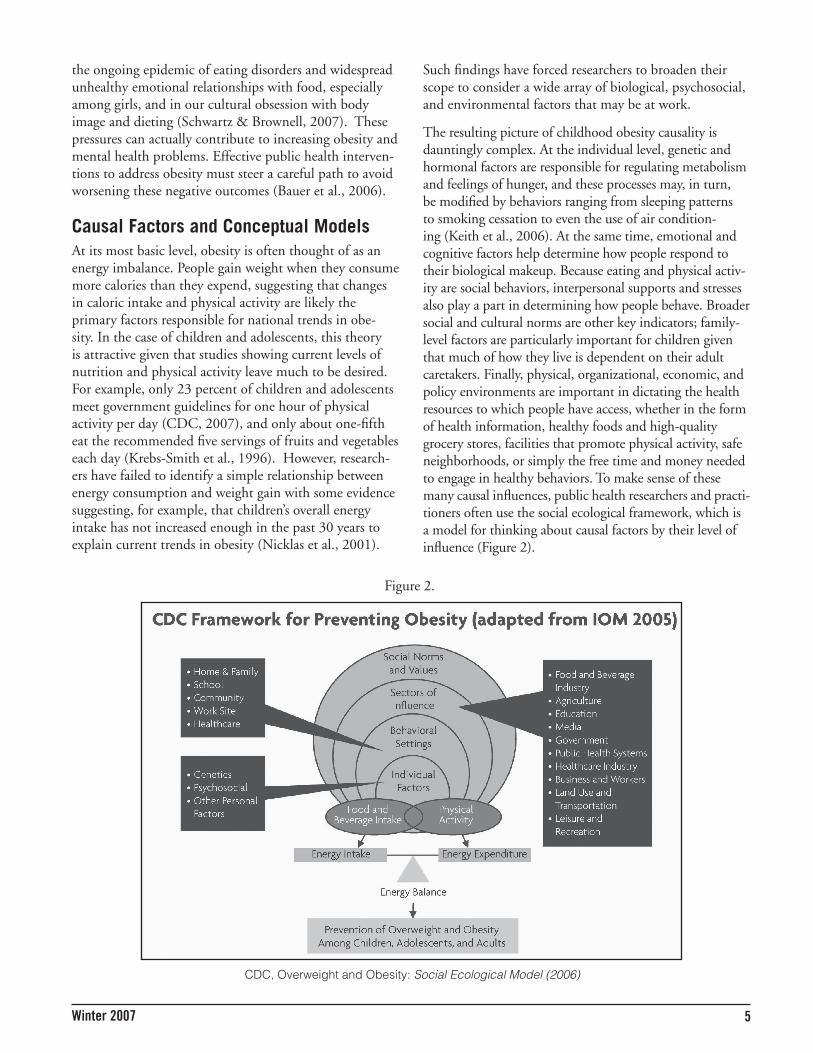
Causal Factors and Conceptual ModelsAt its most basic level, obesity is often thought of as an energy imbalance. People gain weight when they consume more calories than they expend, suggesting that changes in caloric intake and physical activity are likely the primary factors responsible for national trends in obe-sity. In the case of children and adolescents, this theory is attractive given that studies showing current levels of nutrition and physical activity leave much to be desired. For example, only 23 percent of children and adolescents meet government guidelines for one hour of physical activity per day (CDC, 2007), and only about one-fifth eat the recommended five servings of fruits and vegetables each day (Krebs-Smith et al., 1996). However, research-ers have failed to identify a simple relationship between energy consumption and weight gain with some evidence suggesting, for example, that children’s overall energy intake has not increased enough in the past 30 years to explain current trends in obesity (Nicklas et al., 2001).
Such findings have forced researchers to broaden their scope to consider a wide array of biological, psychosocial, and environmental factors that may be at work.
The resulting picture of childhood obesity causality is dauntingly complex. At the individual level, genetic and hormonal factors are responsible for regulating metabolism and feelings of hunger, and these processes may, in turn, be modified by behaviors ranging from sleeping patterns to smoking cessation to even the use of air condition-ing (Keith et al., 2006). At the same time, emotional and cognitive factors help determine how people respond to their biological makeup. Because eating and physical activ-ity are social behaviors, interpersonal supports and stresses also play a part in determining how people behave. Broader social and cultural norms are other key indicators; family-level factors are particularly important for children given that much of how they live is dependent on their adult caretakers. Finally, physical, organizational, economic, and policy environments are important in dictating the health resources to which people have access, whether in the form of health information, healthy foods and high-quality grocery stores, facilities that promote physical activity, safe neighborhoods, or simply the free time and money needed to engage in healthy behaviors. To make sense of these many causal influences, public health researchers and practi-tioners often use the social ecological framework, which is a model for thinking about causal factors by their level of influence (Figure 2).
Figure 2.
CDC, Overweight and Obesity: Social Ecological Model (2006)

� Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
The Role of Public Health Research
Although researchers have convincingly established the high prevalence and significance of childhood obesity, they have achieved much less success in intervening to stop or even slow its rate of increase. For this reason, a great deal of research is still needed to understand the mechanisms of childhood obesity and its prevention. The Institute of Medicine (IOM) recommended continued research along three lines: (1) behavioral research aimed at understanding the most important and changeable factors in obesity etiology; (2) evaluation of prevention efforts, especially in regard to policy; and (3) community-based research that explores the role of physical and social environments (2005, p. 17). In other words, researchers must refine their general ecological model to determine causal pathways of greatest importance.
To support these efforts, this report examines major threads in population approaches to childhood obesity prevention research to date. Areas examined include measurement, the school environment, the built envi-ronment, policy, and ethnicity and culture. The follow-ing discussion explores each area to identify research-informed recommendations for obesity prevention, provide an overview of the issue, and spotlight the work of leading researchers.
III. Measurement
Recommendation• Developanduseintermediatemeasurestobetter
assessthesuccessofobesitypreventionefforts.
A fundamental challenge for researchers and practitioners in obesity prevention is how to measure the effective-ness of prevention programs. Body mass index (BMI), calculated as weight in kilograms divided by the square of height in meters, is generally considered to be the “gold standard” of obesity assessment in adults. Because chil-dren are still growing, however, their BMI scores are not meaningful alone, but instead, are typically considered by age and sex using CDC growth charts (CDC, 2000 CDC Growth Charts, 2007). Children who fall above the 95th percentile for BMI are considered “obese” while those between the 85th and 95th percentile are termed “overweight.” For evaluation purposes, researchers may consider change in BMI scores or change in BMI catego-ries over time.
Although BMI scores provide a quick and low-cost method for assessing childhood obesity, the measure is not without challenges. First, BMI scores do not directly measure fatness, and so may incorrectly assess children and adolescents who are heavy because of muscle mass (CDC, About BMI for children and teens, 2007). Second, BMI cutoff points are somewhat arbitrary in terms of health consequences, especially given that the effects of obesity on health seem to vary by ethnicity. For example, studies show that, compared to other groups, Asian Americans’ risk for diabetes increases at a lower BMI score; thus, more than one system of categorization may be needed (Razak et al., 2007). Third, adiposity rebound, which occurs when young children naturally lose weight for a brief period of time before continued weight gain, can complicate the tracking of BMI (Eisenmann et al., 2007). Finally, and perhaps most importantly, BMI mea-sures are very difficult to change, especially in the short term, because they are the result of many causal factors. As a result, the effectiveness of short-term interventions, or those that isolate a small number of factors, is difficult to assess using BMI. Other measures of body composi-tion, including skin-fold measurements, share many of BMI’s shortcomings.
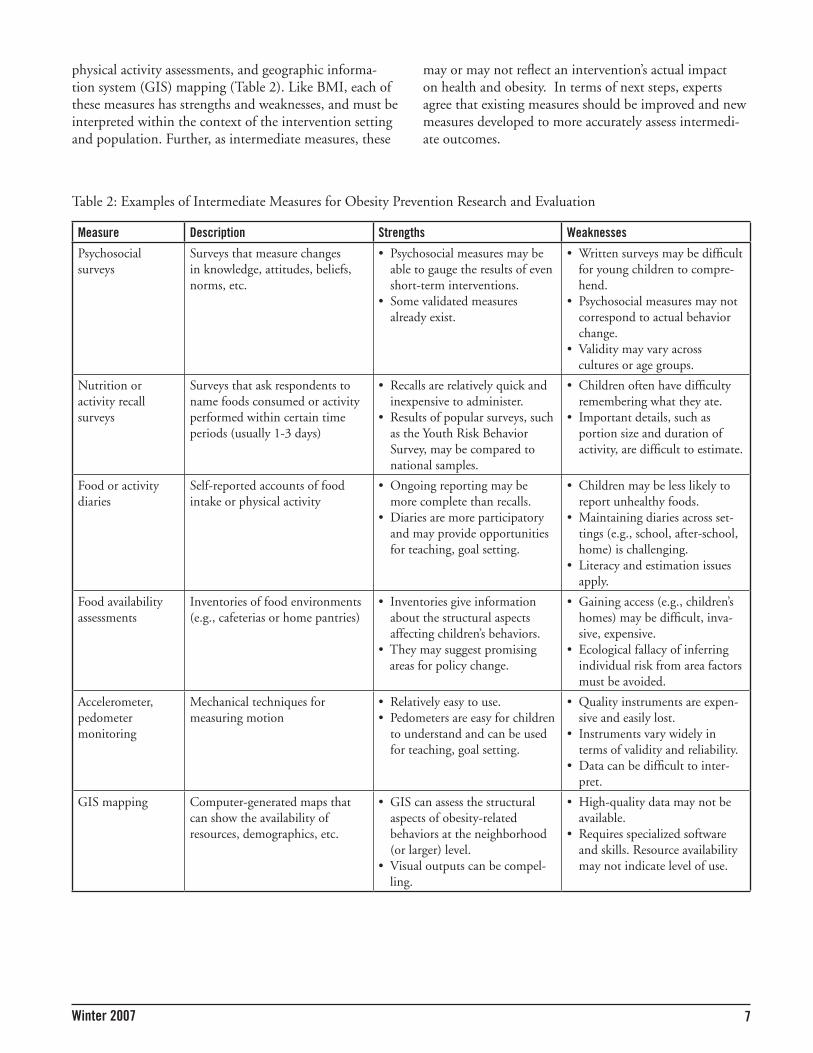
For these reasons, researchers and evaluators often use intermediate measures that assess individuals and/or phys-ical environment instead of, or in addition to, BMI. Tools of interest include psychosocial surveys, nutrition and
7Winter 2007
physical activity assessments, and geographic informa-tion system (GIS) mapping (Table 2). Like BMI, each of these measures has strengths and weaknesses, and must be interpreted within the context of the intervention setting and population. Further, as intermediate measures, these
may or may not reflect an intervention’s actual impact on health and obesity. In terms of next steps, experts agree that existing measures should be improved and new measures developed to more accurately assess intermedi-ate outcomes.
Measure Description Strengths Weaknesses
Psychosocial surveys
Surveys that measure changes in knowledge, attitudes, beliefs, norms, etc.
• Psychosocial measures may be able to gauge the results of even short-term interventions.
• Some validated measures already exist.
• Written surveys may be difficult for young children to compre-hend.
• Psychosocial measures may not correspond to actual behavior change.
• Validity may vary across cultures or age groups.
Nutrition or activity recall surveys
Surveys that ask respondents to name foods consumed or activity performed within certain time periods (usually 1-3 days)
• Recalls are relatively quick and inexpensive to administer.
• Results of popular surveys, such as the Youth Risk Behavior Survey, may be compared to national samples.
• Children often have difficulty remembering what they ate.
• Important details, such as portion size and duration of activity, are difficult to estimate.
Food or activity diaries
Self-reported accounts of food intake or physical activity
• Ongoing reporting may be more complete than recalls.
• Diaries are more participatory and may provide opportunities for teaching, goal setting.
• Children may be less likely to report unhealthy foods.
• Maintaining diaries across set-tings (e.g., school, after-school, home) is challenging.
• Literacy and estimation issues apply.
Food availability assessments
Inventories of food environments (e.g., cafeterias or home pantries)
• Inventories give information about the structural aspects affecting children’s behaviors.
• They may suggest promising areas for policy change.
• Gaining access (e.g., children’s homes) may be difficult, inva-sive, expensive.
• Ecological fallacy of inferring individual risk from area factors must be avoided.
Accelerometer, pedometer monitoring
Mechanical techniques for measuring motion
• Relatively easy to use.• Pedometers are easy for children
to understand and can be used for teaching, goal setting.
• Quality instruments are expen-sive and easily lost.
• Instruments vary widely in terms of validity and reliability.
• Data can be difficult to inter-pret.
GIS mapping Computer-generated maps that can show the availability of resources, demographics, etc.
• GIS can assess the structural aspects of obesity-related behaviors at the neighborhood (or larger) level.
• Visual outputs can be compel-ling.
• High-quality data may not be available.
• Requires specialized software and skills. Resource availability may not indicate level of use.
Table 2: Examples of Intermediate Measures for Obesity Prevention Research and Evaluation

� Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
SPOTLIGHT
Leslie Lytle, PhDLeslie Lytle, a professor at the University of Minnesota, has helped design and conduct a number of large-scale research projects related to health promo-tion and obesity prevention for youth, including the TEENS (Teens Eating for Energy and Nutrition at Schools) and TAAG (Trial for Activity for Adolescent Girls) studies which focused on adolescent girls. TEENS, com-
pleted in 2000, was an intervention study conducted in 16 middle schools. After the first year of a two-year program of classroom curricula, schoolwide events, and family activities, TEENS succeeded in increasing fruit and vegetable intake and decreasing fat intake in students (Birnbaum et al., 2002). By the end of the second year of intervention, though, those student-level effects were no longer seen (Lytle et al., 2004). School-level effects were still evident, however, with more healthful choices on the a la carte lines available for and purchased by students (Lytle et al., 2006). By contrast, TAAG, a randomized controlled trial of 36 middle schools, focused on increas-ing physical activity in middle school-age girls; results of this study are forthcoming. Both studies are ecological in nature, seeking to impact not only individual knowledge and attitudes but also food environments in the home and school (Elder et al., 2006).
Along with her colleagues, Lytle has developed and employed a wide array of measures in her work. TEENS assessment tools, for example, included students’ 24-hour dietary recall, parent surveys assessing food availability in the home, and school surveys tracking changes in food served at school (Lytle et al., 2004). Other measures used by Lytle include accelerometer data and three-day physical activity recalls, body composition assessments, as well as home food inventories, media inventories, school policy tracking, and even GIS analysis of food and activ-ity availability at the neighborhood level. By expanding her focus beyond BMI, Lytle’s work has demonstrated researchers’ success in some of the intermediary steps in obesity prevention and has shown that environmental fac-tors can be positively impacted.
In discussing next steps for obesity prevention research, Lytle emphasizes the need to identify the most “potent and mutable” factors. In her opinion, scientists need to take a step back from large, multi-center trials to do smaller scale research in which researchers can play a more active role in ensuring the fidelity of their inter-ventions. Although the result may have limited external validity, Lytle feels researchers need to better understand the most important factors in preventing obesity, and focus on smaller efficacy trials testing innovative inter-vention approaches. “When you work on a multi-center project, you must create an intervention that will work across a wide range of communities. Often, the most creative and innovative approaches need to be abandoned because they may not be feasible to test in all communi-ties or research sites. We’ve seen some successes with the one-size-fits-all approach, but not the kind of successes we want.”
At the same time, Lytle believes school- and commu-nity-based researchers should re-examine their criteria for scientific rigor and acknowledge that their goals, like their methods, often differ markedly from those of clini-cal researchers. For example, while clinical research may seek to show a dramatic decrease in BMI across a small group of individuals using high-tech measurement tools, community-based research recognizes that small decreases in BMI across a very large population may have more dramatic results in terms of health outcomes. Commu-nity-based measures may focus on changes in the social and physical environment rather than on individual body composition, and they must be appropriate for non-medical settings. Lytle comments, “Based on published research, we don’t have an answer to how to prevent childhood obesity. Every review comes up with the same conclusion that we can’t say what the best practice is, but we can’t have people wait. We do know that the very proximal factors, such as motivation and education, aren’t enough. We need to focus on the physical environment, access and availability issues, and neighborhood effects. Where are the broader leverage points? As a field, this is what we’re trying to figure out.”

9Winter 2007
IV. The School Environment
enrollment in daily physical activity classes dropped from 42 percent in 1991 to 25 percent in 1999 (CDC, 2006).
Despite financial and other barriers faced by school com-munities, many authorities in childhood obesity preven-tion, including the Institute of Medicine (IOM), agree that children and adolescents must get more exercise at school, where they spend so many of their waking hours. Thirty minutes of moderate to vigorous physical activity (MVPA) per day is a common goal (IOM, 2005, p. 259). Strategies for achieving greater frequency and intensity of activity include:
• Introducing new physical activity curricula that emphasize cooperative games and continuous move-ment. The Sports, Play, and Active Recreation for Kids (SPARK) program is one example (Sallis et al., 1997);
• Offering attractive alternatives to traditional sports, such as dance, helps engage older students, especially girls, who are least likely to be active (IOM, 2005);
• Integrating physical activities throughout the school day (IOM, 2005); and
• Augmenting after-school and extracurricular programs for students as well as activity-related events or classes for families and staff (IOM, 2005).
In addition to increasing physical activity opportuni-ties, researchers have sought ways to objectively evaluate the quality of activity provided by these programs. Tools such as SOFIT (System for Observing Fitness Instruction Time) have been developed to assess an activity session’s duration and intensity (McKenzie, Sallis & Nader, 1991).
NutritionA second major area of interest in school-based obesity prevention is nutrition. The school environment, like that of society at large, often discourages healthy choices by providing students with too many attractively pack-aged, inexpensive, and unhealthy food options. This balance is difficult to change. Candy, soda, snack chips, and other energy-dense foods are often readily available to students through “a la carte” cafeteria programs, vend-ing machines, and fundraisers. As “competitive foods,” these offerings are not subject to the USDA’s regulations, which provide guidelines for the nutritional quality of food served as part of the National School Lunch Pro-gram (Greves & Rivara, 2006). Adding to the problem is the fact that resource-poor schools may be unwilling to give up the revenue the sales of competitive foods gener-ate, whether in the form of actual profits or in terms of
Recommendations:• Engagestudentsinatleast30minutesofmoderate
tovigorousphysicalactivityeachday.
• Encouragetheconsumptionofhealthyfoodsbyincreasingthenumberofhealthyoptions,pricingthoseoptionscompetitively,andreducingthenum-berofunhealthyfoodsoffered.
• Providehigh-qualityhealtheducationinareassuchasnutritionandphysicalfitness.
School-based research is prominent in childhood obesity prevention efforts in part because schools offer access to children in an educational setting that, at least in theory, can be modified more easily than home and community environments. School-based interventions typically aim to help students make healthier choices by providing them with health information while at the same time improving the environment in which their choices are made. Particular areas of interest include increasing the amount of physical activity students get each day, improv-ing the nutritional quality of food served at school, and integrating health education messages into existing school curricula. Initiatives in these areas require broad-based support, and education and outreach efforts ideally extend not only to students but to parents, teachers, and administrators as well.
Physical ActivityObservers of the school environment have noted that students move very little during the school day and the reasons for their inactivity are many. One survey of 157 physical education specialists trained in the Coordinated Approach to Child Health (CATCH) program suggests budgetary restrictions in many districts have discouraged investment in the curricula, staff, and equipment needed for high-quality physical activity programming (Barroso et al., 2005). At the same time, respondents reported that increasing demands for student performance in standard-ized testing leaves little time for nonacademic pursuits such as physical fitness (Barroso et al., 2005). Further-more, opportunities for physical activity that do exist often emphasize traditional, competitive games, such as baseball, which do not result in sustained cardiovascular activity or which may be unappealing to less athletically inclined students (Rees et al., 2006). Whether because of these factors or others, studies show that students’ partici-pation in physical activity at school tends to decline with age and over time; Youth Risk Behavior Survey (YRBS) data, for example, indicate that high school student

�0 Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
contracts with soda and snack food manufacturers, some of whom provide schools with support for extracurricular activities such as sports teams in exchange for advertising and sales opportunities. School staff, especially food ser-vice employees, are often concerned that if healthy foods are offered, participation in school lunch programs will decrease as will the ability to recoup costs. A national sur-vey of school nutrition services representatives found that these perceptions are hard to change, despite the anec-dotal evidence from the field suggesting that competitive pricing programs promoting the sale of healthy foods have failed to result in negative financial consequences (Greves & Rivara, 2006).
Even in well-funded schools, however, unhealthy foods are common; they are often used in the context of class-room parties or as rewards for good behavior, a practice that may underscore the value of these foods for students. Furthermore, federally funded school lunch programs, though highly regulated in terms of nutritional content, are not always as healthy or appetizing as they might be. With many schools employing the services of outside contractors for food service, students’ meals may travel hundreds of miles before reaching them, and strict rules concerning meal composition limit the use of some healthful ingredients such as soy-based proteins (Bauer et al., 2006). Factors such as these serve to undermine the good intentions of even the most nutrition-conscious students.
Public health practitioners have sought to address the food environment of schools by increasing healthy options, making options more attractive, and engaging students in the process of food preparation and produc-tion. In these ways, program planners hope to create what is sometimes referred to as a “person-environment fit,” in which students have the environmental supports they need to make healthy choices. In addition to simply substituting healthy offerings for unhealthy ones, efforts to improve the food environment and introduce students to new food include:
• Adoption of classroom tasting and cooking curricula, such as California State Department of Health Ser-vice’s Harvest of the Month (2005);
• School cafeteria initiatives, such as the Johns Hopkins Center for a Livable Future’s Meatless Monday proj-ect, which introduced and promoted low-fat, meat-less foods into the menu (Johns Hopkins Bloomberg School of Public Health, 2005).
• Food and nutrition education programs, such as Food is Elementary by Dr. Antonia Demas, that teach school gardening, nutrition education, and cooking skills (Food Studies Institute, 2006); and
• Competitive pricing programs aimed at making healthy foods a better value and more attractive to students in terms of cost and variety. The CHIPS (Changing Individuals’ Purchase of Snacks) program as implemented in Minnesota middle schools is one example (French, 2003).
Through programs such as these, public health practitio-ners attempt to redefine students’ relationships with food by changing both individual attitudes and social norms to support the consumption of healthy foods, especially fruits and vegetables, while discouraging opportunities for students to take in empty calories.
Health Education in Schools
A third area of focus in school-based research is health education related to nutrition and physical activity. Stud-ies such as CATCH have shown that classroom teachers often have difficulty using traditional health education curricula for several reasons. First, because health-related knowledge is not part of required scholastic assessments, it is often covered superficially and without the curricu-lar support devoted to other subjects (Hoelscher et al., 2004). In order to provide health education in an ongo-ing fashion, teachers often note the need to tie health information to existing curricula, and math and science classes have proven to be a particularly good fit in this regard (Hoelscher et al., 2004). Additionally, some teach-ers feel they lack the knowledge necessary to teach health topics. Many obesity prevention interventions, therefore, acknowledge the need to extend health education activi-ties to include teachers and parents. The Eat Well and Keep Moving program is one example of an integrated approach that incorporates teachers and families in health education efforts (Gortmaker et al., 1999).

��Winter 2007
SPOTLIGHT
Benjamin Caballero, MD, PhDBenjamin Caballero, a profes-sor in international health and human nutrition at the Johns Hopkins Bloomberg School of Public Health, has been at the forefront of childhood obesity prevention through research including the Pathways study. Based in 41 elementary schools, Pathways was a random-ized controlled trial of over
1,700 American Indian third-, fourth-, and fifth-graders (Caballero et al., 2003). Pathways was designed to be a culturally sensitive, ecological approach to school-based obesity prevention (Davis et al., 1999), and involved four primary components: 1) classroom curricula related to physical fitness and nutrition; 2) a physical activity curriculum known as SPARK (Sports, Play, and Active Recreation for Kids); 3) collaboration with food service staff to lower the fat content of school food; and 4) family events and resources. Though the study did not result in changes in children’s body composition, Pathways researchers did show improvements in students’ dietary fat intake and health knowledge.
In discussing school-based work in obesity prevention, Caballero emphasizes that high-quality interventions do not necessarily result in decreased BMI, even when students’ energy intake decreases and physical activity increases; his literature review of 15 school-based inter-ventions showed only one was successful in terms of low-ering BMI. In Caballero’s opinion, many confounding factors—such as increased eating outside the school set-ting—may mask healthy changes happening in schools. For this reason, he stresses the importance of developing intermediary measures for studying obesity. He explains, “We need to consider additional kinds of measures. Attitudes and other psychosocial factors are important. We should also learn from researchers with experience in environmental exposures to better understand the physi-cal environment’s impact on obesity.”
Caballero also emphasizes the need to take an integrated approach to understanding obesity: “We’ve tended to approach obesity prevention in the same way as obesity treatment—restricting people’s diets, for example—and in the real world this doesn’t work. There’s no single approach for making a dent in the problem.” Comparing obesity prevention to campaigns in the 1980s and 90s to reduce tobacco use, Caballero believes that research-ers need to work to understand obesity in the context of parenting, family life, school settings, and the broader community and policy environments. While the school setting is important, he wants researchers to understand that schools are only part of the solution and that, fur-thermore, teachers and administrators in these settings are often facing a wide array of serious and more immediate problems, from school violence to performance mandates to staff turnover, which may limit their involvement in obesity prevention efforts. Caballero believes that by bringing in more stakeholders, including community leaders, politicians, and industry leaders, public health researchers may be able to develop more effective and sustainable interventions.

�2 Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
V. The Built Environment and Neighborhood Factors
families negotiate the challenges of the built environment (Staunton et al., 2003).
Diet, like physical activity, is also determined in part by the built environment; families who have easy access to affordable, high-quality fruits and vegetables are more likely to consume them (Sallis & Glanz, 2006). Research-ers have noted with concern that low-income communi-ties offer below-average access to supermarkets and fresh produce, but greater access to liquor stores, as compared to wealthier neighborhoods (Moore & Diez Roux, 2006). Public health practitioners have attempted to improve availability of and access to healthy foods in low-income communities by establishing farmers markets, instituting mobile vending routes, and partnering with local mer-chants for “corner store enhancement” to provide a greater selection of competitively priced fruits and vegetables (Bolen & Hecht, 2003, p. 18). The Baltimore Healthy Stores Project, implemented by Dr. Joel Gittelsohn, conducted by the Bloomberg School’s Center for Human Nutrition, is one intervention that targets the built envi-ronment in low-income communities by improving the nutritional quality of food offered in local grocery and convenience stores, providing special labels to identify healthy choices, and creating health education materials to raise public awareness of these efforts. Policy efforts to increase affordability of healthy food through food aid programs such as Women, Infants and Children (WIC) and food stamps are another example (Quaid, 2006).
Recommendations• Makecommunitiesmorewalk-ableandbike-able.
• Increaseaccesstohealthyfoods.
Studies of the built environment in the context of child-hood obesity prevention emphasize the effect that city or community planning efforts, or lack thereof, may have on children’s health behaviors. As the name implies, the built environment includes structures such as sidewalks, playgrounds, and markets that impact opportunities for health, but also extends to more abstract ideas about neighborhood design and governance that impact com-munity dynamics, safety, and other social interactions. The built environment has been of particular interest to those involved in health disparities research because it is directly associated with many barriers to health, such as limited availability of and access to fresh produce and other healthy foods, and the exposure to crime often experienced by people living in resource-poor communi-ties. Urban factors such as crowding are often the first to come to mind in regard to the built environment, but suburban and rural communities also experience struc-tural barriers to health, such as a lack of sidewalks and limited street connectivity.
In terms of physical activity, researchers focusing on the built environment note that many factors associated with urban and suburban development limit children’s oppor-tunity for unstructured recreation outside the home. Concerns about crime are a leading reason that parents keep their children indoors, but traffic and a lack of well-maintained playgrounds and greenways are also impor-tant (Salmon & Timperio, 2007; Gordon-Larsen et al., 2000). Researchers in public health study the effects such factors have on health behaviors, and, in particular, the use of GIS analysis has emerged as a powerful assessment tool (Sallis & Glanz, 2006). At the same time, others have sought to improve the built environment, particularly with the intention of establishing communities that are well-suited for walking, biking and recreational activi-ties. Such efforts include community planning activities designed to improve sidewalks and bike paths as well as community organization efforts to provide supervision and social support for active transportation. The National Highway Traffic Safety Administration’s Safe Routes to School is one example of a program aimed at helping

��Winter 2007
SPOTLIGHT
Penny Gordon-Larsen, PhDPenny Gordon-Larsen is an assistant professor of nutrition at the University of North Carolina School of Public Health, where her research focuses on the socio-demo-graphic and environmental determinants of obesity. Gordon-Larsen is one of
only a few researchers to focus specifically on the rela-tionship between obesity and the built environment, an interest that was sparked by her dissertation work in West Philadelphia, Pennsylvania. “In my [community-based participatory research] work, I talked to kids to try to understand the challenges they faced living in an urban environment. What about the urban environment predisposed inner city kids to obesity? One issue that just kept coming up was that despite understanding the need for healthy diet and activity, the kids couldn’t actually get fruits and vegetables. They lived in an environment with easy access to high-fat, energy-dense foods, and without safe access to recreational facilities.” Through the Univer-sity of Pennsylvania Center for Community Partnerships’ Urban Nutrition Initiative (2007), Gordon-Larsen and her colleagues were able to use research to guide public health practice. Specifically, the center has worked to increase the availability of food by instituting after-school fruit and vegetable stands, school-based gardens, and fam-ily fitness centers along with nutrition education.
Discussing her current work, Gordon-Larsen feels research on the built environment is becoming both more common and more sophisticated, thanks in part to the growing popularity of GIS analysis. At this point researchers have firmly established the importance of this area of study: “We have good evidence that poor commu-nities are at a disadvantage in terms of healthy foods and physical activity, whether directly in terms of availability or indirectly in terms of concerns about crime.” Gordon-Larsen emphasizes, however, that research related to the built environment is still in its infancy and has intro-duced many new challenges. “It’s very hard to implement and collect intervention data aimed at changing the built
environment because we don’t live in an experimental world,” she says. For this reason researchers must be on the lookout for “natural experiments” in which policy and environment changes give researchers opportunities for making before-and-after comparisons.
In terms of advancing future studies, Gordon-Larsen believes researchers need to pursue more rigorous lon-gitudinal study designs. She is in the process of finish-ing a longitudinal database that will help her describe the effects of environmental change on behaviors. Her primary targets are modifiable factors, such as individuals’ distance from and access to fitness facilities, which can be used to inform policy, as well as more general character-ization of the physical environment. “The urban-rural-suburban gradations commonly used in research are so big. So we’re trying to characterize these areas in more detail so that we can understand what it really means to live in suburbia, for example.”
Gordon-Larsen advises researchers with an interest in the built environment to partner with their counter-parts in geography and urban planning to facilitate the negotiation of data. She explains, “Researchers need to understand the intricacy of working with large databases [such as a national GIS database]. If you’re not careful with quality, you won’t get the data you need to support the research.” Gordon-Larsen hopes that as work related to the built environment gains recognition in the area of obesity, researchers with other behavioral interests such as alcohol and tobacco use will join her efforts.

�4 Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
VI. Marketing, Industry, and Public Policy
The public health community has attempted to counter the effects of detrimental marketing by creating compet-ing messages that promote health, by educating youth to be more media savvy, and by using media to build sup-port for prevention-related policy initiatives. The CDC’s VERB Campaign, for example, is a well-known com-munication intervention that used a variety of media to impart the message that being physically active is socially desirable (Huhman et al., 2005). Similarly, curricula such as the National Institute of Child Health & Human Development’s Media Smart Youth: Eat, Think, and Be Active! are designed to help children and adolescents become more critical consumers of marketing messages (2005). Finally, media have been an avenue for public dis-course about the national diet in recent years with social critics attracting widespread attention for such work as Schlosser’s Fast Food Nation (2001). In these ways, counter-narratives have been constructed to compete with the commercial marketing messages that encourage the consumption of unhealthy foods.
If the aforementioned strategies take an oppositional stance to marketing and corporate interests, an alter-native tactic that has gained ground in recent years is more cooperative in nature; in several notable instances, industry leaders have been persuaded to adopt self-regula-tory measures. For example, in an agreement brokered by former President Bill Clinton, Arkansas Governor Mike Huckabee, and the American Heart Association, major manufacturers of soft drinks have agreed to replace the sale of beverages with added sugars in schools with water and fruit juices (Burros & Warner, 2006). Through the application of public pressure for corporate responsibil-ity, businesses may be encouraged to operate in ways more conducive to children’s health, and the Institute of Medicine and others have recommended that efforts in this area continue (IOM, 2006).
At the same time, critics of these efforts argue that indus-try self-regulation is not always strong or well-enforced enough to result in significant change. Given the urgency of the obesity crisis, they believe that external regulation by the federal government is also merited (Kelly, 2005). However, despite increased attention to the issue, includ-ing a recent forum held by the Federal Trade Commission (2006) at the urging of the IOM, proponents of federal regulation have made little headway to date against strong political opposition.
Recommendations• Advocateforregulationofyouthmarketing.
• Strengthenconsumers’abilitytomakeinformedfoodchoices,gainaccesstoaccurateinformation,andtakeanactiveroleininfluencingfoodpolicy.
In addition to individual and environmental factors, eco-nomic and political considerations must feature promi-nently in any discussion of the public health response to childhood obesity. More specifically, how can public health messages compete with for-profit corporations that have billions of dollars to spend marketing energy-dense foods and sedentary entertainment to children and youth? What constitutes predatory advertising, and how can youth advocates work to regulate potentially harmful media influences? What can be done at the policy level to create incentives for the production of health-promoting foods and products? Questions such as these that consider the political and economic aspects of obesity are essential for understanding key macro-level targets of intervention, which include the areas of youth marketing and national food policy, among others.
Youth MarketingThe marketing of unhealthy foods to youth has been widely discussed in the public health community as a contributing factor to the obesity epidemic, and poses a particular concern given the pervasiveness of advertis-ing media and the vulnerability of children and youth to advertising messages (IOM, 2000). The majority of youth marketing occurs through television with studies showing that the average child watches as many as 400,000 televi-sion ads each year; movies, the Internet, print materials, and advertising in schools also contribute to exposure (Committee on Communications, American Academy of Pediatrics, 2006). Studies have consistently shown that even in very young children television viewing is posi-tively correlated with consumption of advertised foods, which are often of low nutritional value (Wiecha et al., 2006). Ironically, at the same time television ads promote unhealthy consumption, they may also foster poor body image in viewers by idealizing thin or even underweight body types that children and adolescents may find impos-sible to attain through healthy means. Through content analysis of available media as well as survey studies, researchers work to characterize the media environment and to determine its effects on children and adolescents.

��Winter 2007
Federal Food PolicyConcerns about childhood obesity have led to greater attention to the role of the federal government in other areas as well, and the USDA’s National School Lunch Program (NSLP) and the Farm Bill are two examples. The NSLP, which provides meals to approximately 30 million students each school day, currently issues nutri-tional guidelines that specify certain nutritional standards for the food, including limits on the number of allowable calories from fat. However, critics of the NSLP, including the Institute of Medicine, argue that these guidelines are outdated and note, for example, that the NSLP currently makes no requirements for serving fruits and vegetables (2005). Particularly because the NSLP serves as a daily source of food for many low-income youth who are at increased risk for obesity, policy initiatives aimed at improving and enforcing nutritional standards for the NSLP may prove to be an effective strategy for obesity prevention (Weiss & Smith, 2004).
The importance of the national Farm Bill is another area of federal policy that is emerging as important to the public health response to obesity. This agricultural policy encourages the production of certain commodities, such as corn and soy, over other crops including fruits and vegetables (see Spotlight: David Wallinga). If the priori-ties of the Farm Bill were shifted to favor the production of healthier foods, advocates believe that policymakers could significantly impact the national food environment (Schoonover & Muller, 2006). Furthermore, because the Farm Bill plays a role in dictating the foods offered through the NSLP, it presents an especially attractive tar-get for intervention. Public health professionals work to build public support for policy reform in these and other areas to help ensure that consumers have greater access to healthy foods and nutritional information about those foods.
SPOTLIGHT
David Wallinga, MDDavid Wallinga, director of the Food and Health Program at the Institute for Agriculture and Trade Policy (IATP) in Minneapolis, advocates and conducts research concern-ing how food production and packaging impacts public health, and especially the health of children. IATP programs focus, for example, on industrial contaminants
deposited in the food chain, and on farm practices result-ing in chemical residues and antibiotic resistance. IATP also advocates for more sustainable food systems that provide not only healthier food but also better social, environmental, and economic health for communities. Wallinga stresses that chemical additives are not the only way current agricultural practices are problematic; America’s lopsided emphasis on the production of soy and corn has contributed to the proliferation and ready acces-sibility of high-calorie, low-nutrient foods that encourage obesity. Sustained by Farm Bill policies, these “commod-ity” crops are overproduced, driving down their price. As a result, processed foods using corn and soy derivatives such as high-fructose corn syrup and hydrogenated cook-ing oils, can be produced cheaply and with high profit margins, often edging out healthier foods in the national diet. Indeed, Wallinga notes that obesity rates have risen in step with the rising production and consumption of high-fructose corn syrup, which are made possible by the Farm Bill because of financial support for these crops.Given that the production of artificially inexpensive com-modity grains largely benefits food processors and large-scale meat producers rather than farmers (Schoonover & Muller, 2006), Wallinga looks forward to future collabo-ration between the public health and farming communi-ties. In particular, he hopes that sustained advocacy will one day transform the Farm Bill, which benefits the busi-ness interests of a select few, into what he calls a “Healthy Food Bill,” which, by encouraging the production of healthy foods, will sustain both the people who grow food as well as those who eat it.

�� Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
VII. The Ethnicity Gap and Cultural Contexts
Recommendation• Engagelocalgovernmentsandcommunitygroups,
particularlythosemostaffectedbyobesity,incom-munityandpolicyinitiative.
Obesity rates have increased in almost all sectors of the U.S. population, but some groups suffer more than oth-ers, including women in certain ethnic and racial minori-ties. Obesity affects almost half of African American women, for example, as compared to less than one-third of white women, and this population difference begins in childhood (Flegal et al., 2002). Lower socioeconomic status is also associated with obesity, though this asso-ciation may be weakening over time (Wang & Zhang, 2006). Many public health researchers are interested in understanding mechanisms of ethnic and racial dispari-ties in obesity and in addressing those factors to reduce the ethnicity gap (Gordon-Larsen et al., 2006). Racial disparities may arise through many pathways, includ-ing population differences in access to healthy food, safe places to exercise, and time to engage in either. Psycho-biological factors may also play a role. For example, the stress hormone cortisol may also affect obesity, and racial minorities may experience more stress due to social and economic factors including the effects of living in an unequal society (Gordon-Larsen et al., 2006).
In studying differences in obesity rates across popula-tions, many have pointed to the need to arrive at a more nuanced understanding of the cultural context for eating and physical activity. How do different cultures encour-age or discourage obesity? How does American consumer culture impact traditional patterns of diet and physical activity? What are cultural norms related to body image? What modifications of traditional recipes will be accepted as healthier but still appealing alternatives? Researchers of cultural context argue that these questions are critical not only to understanding obesity on a theoretical level, but to designing culturally appropriate interventions as well. In particular, many believe that additional qualitative research is needed to provide in-depth analysis of cultural phenomena.
This appreciation of the role of cultural influences often goes hand in hand with a desire to engage populations in a more participatory approach to obesity prevention so as to translate local knowledge into action. Specifically, public health advocates have sought to organize local and community organizations to respond to the problem of obesity in their own localities. Food security--the abil-ity to access the food needed for health--is one issue that has gained traction in recent years, as community groups have employed arguments of social justice to secure more equitable access to fresh fruits and vegetables and other healthy foods. The Garden of Eden Project, which orga-nized church-based produce markets in African American communities in St. Louis, Missouri, is one example of this approach (Baker et al., 2006). Funding agencies are increasingly encouraging, and even requiring, their grant-ees to secure community participation, underscoring the importance of this approach.

�7Winter 2007
SPOTLIGHT
Shiriki Kumanyika, PhDShiriki Kumanyika studies obesity treatment and preven-tion with a focus on culture and ethnicity. A professor of epidemiology at the Univer-sity of Pennsylvania School of Medicine, Kumanyika was the principal investiga-tor of the recently completed SHARE (Supporting Healthy Activity and Eating Right
Everyday) study. SHARE paired African American par-ticipants with family members or friends to investigate the role of interpersonal relationships in weight-related lifestyle modification (Kumanyika, 2003). Through cultural tailoring and social support, Kumanyika and her colleagues were hoping to increase their participants’ ability to make and sustain changes in their eating and activity practices over a two-year period. Results are currently being analyzed, including responses to an exit questionnaire about how specific cultural adaptations were viewed by the participants.
Kumanyika emphasizes that studies such as SHARE are critical to understanding the social and cultural contexts that contribute to the persistent ethnicity gap in obesity prevalence. In discussing her work, she notes that African American women are particularly vulnerable to obesity, citing a number of possible determinants of overeat-ing, including stress, history of material deprivation, and the prominent role of food in cultural celebrations. Kumanyika says the problem of obesity related to over-eating may be self-perpetuating: “Seeing so many heavy African Americans makes people think it’s natural, that they don’t need to be concerned about higher rates of obesity in this population. In reality, the excess of obesity is far from benign.”
In the future, Kumanyika hopes to see more emphasis placed on qualitative research and integration of knowl-edge from a wider range of disciplines to help practitio-ners develop an understanding of culture beyond mere food preferences. To facilitate this work, she founded
the African American Collaborative Obesity Research
ing the quality, quantity, and translation of research in African American communities. Kumanyika believes researchers need to take a deeper look into the role that food plays in people’s lives, whether in terms of stress relief, social interaction, or parenting, in order to tailor interventions in a more meaningful way. “I think we health professionals, who divide up health problems to study them, need to make sure we put everything back together as we go back into the population,” she said. “All of the changes that have happened in society that affect how people behave are part of an integrated system of how we live. For example, relationships between parental employment, stress, and disadvantage flow directly to how children are parented, including how children are fed. The factors leading to many [chronic] diseases are similar, and we could save money and time if we stud-ied them in context.” In terms of qualitative methods, Kumanyika emphasizes the importance of unstructured interviews, ethnography, and participant observation. She has found content analysis especially valuable, and her work is informed, in part, by feminist literature such as bell hooks’ Sisters of the Yam (1994), which serves as one of many examples of how knowledge from the humanities can be relevant to public health.
In addition to cultural factors, Kumanyika believes the public health community should continue to exam-ine environmental factors, such as targeted marketing campaigns and increased availability of unhealthy foods in communities of color, and how these factors impact obesity levels. In her view, through a contextualized, integrated approach, researchers may be more successful in reaching those who are currently suffering most from obesity, people of color.
Network (AACORN, www.aacorn.org) aimed at increas-

�� Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
VIII. Conclusion
Research literature indicates that findings related to child-hood obesity prevention are best described as “mixed” and that researchers remain years away from establishing the evidence-based best practice models used in other areas of public health and medicine. Nevertheless, leaders in the field are largely in agreement on a number of impor-tant points. First, individually focused efforts aimed at awareness and education are necessary but not sufficient for addressing the complex problem of childhood obesity. Instead, public health researchers must adopt a multi-pronged, ecological approach that acknowledges social, physical, and policy environments critical to achieving and maintaining health. Second, experts emphasize the importance of a sustained approach to obesity research and prevention activities. The sustained approach is
important because diet and nutrition issues are par-ticularly vulnerable to fads and the public and media’s reaction and interpretation of research. Health behaviors and, in turn, body composition are the result of years of daily practice and socialization, bounded by socio-envi-ronmental and physiologic constraints. They are, there-fore, resistant to any single or short-term intervention. Instead, sustained and integrated efforts ranging from local initiatives to national policies are needed to create environments that better support health behaviors. Given the magnitude and severity of the problem, few areas of public health intervention hold as great an opportunity to contribute to the overall health, longevity, and quality of life of future generations.

�9Winter 2007
References
Centers for Disease Control and Prevention. (2006). Overweight and obesity: State-based programs: Social Eco-logical Model. Retrieved May 20, 2007, from http://www.cdc.gov/nccdphp/dnpa/obesity/state_programs/se_model.htm.
Centers for Disease Control and Prevention. (2006). YRBSS: Youth Risk Behavior Surveillance System. Retrieved February 15, from http://www.cdc.gov/HealthyYouth/yrbs/index.htm.
Centers for Disease Control and Prevention. (2007). 2000 CDC Growth Charts: United States. Retrieved Janu-ary 19, 2007, from http://www.cdc.gov/growthcharts/.
Centers for Disease Control and Prevention. (2007). Body Mass Index: About body mass index for children and teens. Retrieved June 26, 2007, from http://www.cdc.gov/nccd-php/dnpa/bmi/childrens_BMI/about_childrens_BMI.htm#using%20an%20adult%20BMI%20calculator.
Centers for Disease Control and Prevention. (2007). Overweight and obesity: Childhood overweight: Consequences. Retrieved January 10, 2007, from http://www.cdc.gov/nccdphp/dnpa/obesity/childhood/consequences.htm.
Centers for Disease Control and Prevention. (2007). Overweight and obesity: Childhood overweight: Overweight prevalence. Retrieved January 10, 2007, from http://www.cdc.gov/nccdphp/dnpa/obesity/childhood/prevalence.htm.
Centers for Disease Control and Prevention. (2007). Prevalence of overweight among children and adolescents. Retrieved September 20, 2007, from http://www.cdc.gov/nchs/products/pubs/pubd/hestats/overweight/overwght_child_03.htm#Table%201.
Committee on Communications, American Academy of Pediatrics. (2006). Children, adolescents, and advertising. Pediatrics, 118(6), 2563-69.
Davis, S. M., Going, S. B., Helitzer, D. L., Teufel, N. I., Snyder, P., Gittelsohn, J., et al. (1999). Pathways: A culturally appropriate obesity-prevention program for American Indian schoolchildren. American Journal of Clinical Nutrition, 69(suppl), 796S-802S.
Ebbeling, C. B., Pawlak, D. B., & Ludwig, D. S. (2002). Childhood obesity: Public-health crisis, common sense cure. Lancet, 360, 473-82.
Baker, E. A., Kelly, C., Barnidge, E., Strayhorn, J., Schootman, M., Struthers, J., & Griffith, D. (2006). The Garden of Eden: Acknowledging the impact of race and class in efforts to decrease obesity rates. American Journal of Public Health, 96(7), 1170-114.
Barroso, C. S., McCullum-Gomez, C., Hoelscher, D. M., Kelder, S. H., & Murray, N. G. (2005). Self-reported barriers to quality physical education by physical educa-tion specialists in Texas. Journal of School Health, 75(8), 313-19.
Bauer, K. W, Patel, A., Prokop, L. A., & Austin, S. B. (2006). Swimming upstream: faculty and staff members from urban middle schools in low-income communities describe their experience implementing nutrition and physical activity initiatives. Preventing Chronic Disease, 3 (2):A37.
Birnbaum, A. S., Lytle, L. A., Story, M., Perry, C. L., & Murray, D. M. (2002). Are differences in exposure to a multicomponent school-based intervention associated with varying dietary outcomes in adolescents? Health Education and Behavior, 29(4), 427-43.
Bolen, E., & Hecht, K. (2003). Neighborhood groceries: New access to healthy food in low-income communities. California Food Policy Advocates. Retrieved February 15, 2007, from http://www.cfpa.net/Grocery.PDF.
Bray, G. A., Nielsen, S. J., & Popkin, B. M. (2004). Consumption of high-fructose corn syrup in beverages may play a role in the epidemic of obesity. American Journal of Clinical Nutrition, 79(4), 537-43.
Burros, M., & Warner, M. (2006, May 4). Bot-tlers agree to a ban on sweet drinks. New York Times. Retrieved February 23, 2007, from http://www.nytimes.com/2006/05/04/health/04soda.html?ex=1304395200&en=80149e91b4b733bb&ei=5088&partner=rssnyt&emc=rss#.
Caballero, B., Clay, T., Davis, S. M., Ethelbah, B., Rock, B. H., Lohman, T., et al. (2003). American Journal of Clinical Nutrition, 78, 1030-38.
California State Department of Health Service. (2005). Harvest of the month: Growing healthy students. Retrieved January 10, 2007, from http://www.harvestofthemonth.com.

20 Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
Eisenberg, M. E., Neumark-Sztainer, D., & Story, M. (2003). Associations of weight-based teasing and emo-tional well-being among adolescents. Archives of Pediatric and Adolescent Medicine, 157, 733-38.
Eisenmann, J. C., Heelan, K. A., & Welk, G. J. (2004). Assessing body composition among 3- to 8-year-old chil-dren: Anthropometry, BIA, and DXA. Obesity Research, 12(10), 1633-40.
Elder, J. P., Lytle, L., Sallis, J. F., Young, D. R., Steckler, A., Simons-Morton, D., et al. (2006). A description of the social-ecological framework used in the trial of activ-ity for adolescent girls (TAAG). Health Education Research Advance Access. Retrieved January 14, 2007, from http://her.oxfordjournals.org/cgi/content/abstract/cyl059v1.
Fagot-Campagna, A., Pettitt, D.J., Engelgau, M.M., Burrows, N. R., Geiss, L.S., Valdez, R., et al. (2000). Type 2 diabetes among North American children and adolescents: An epidemiologic review and a public health perspective. Journal of Pediatrics, 136(5) , 664-72.
Federal Trade Commission. (2006). Perspectives on mar-keting, self-regulation, & childhood obesity. Retrieved June 26, 2007, from http://www.ftc.gov/os/2006/05PerspectivesOnMarketingselfRegulation&ChildhoodObesityFTCandHHSReportonJointWorkshop.pdf.
Flegal, K.M., Carroll, M.D., Ogden, C.L., Johnson, C.L. (2002). Prevalence and trends in obesity among US adults, 1999-2000. JAMA, 288(14), 1723-27.
Food Studies Institute. (2006). Food is Elementary. Retrieved June 25, 2007, from http://www.foodstudies.org/Curriculum/index.htm.
Fontaine, K. R., Redden, D. T., Wang, C., Westfall, A. O., Allison, D. B. (2003). Years of life lost due to obesity. Journal of the American Medical Association, 289(2), 187-93.
French, S.A. (2003). Pricing effects on food choices. Journal of Nutrition, 133(3), 841S-43S.
Gordon-Larsen, P., Adair, L. S., Nelson, M. C., & Popkin, B. M. (2004). Five-year obesity incidence in the transition period between adolescence and adulthood: The National Longitudinal Study of Adolescent Health. American Journal of Clinical Nutrition, 80(3), 569-75.
Gordon-Larsen, P., McMurray, R. G., & Popkin, B. M. (2000). Determinants of adolescent physical activity and inactivity patterns. Pediatrics, 105(6), E83.
Gortmaker, S. L., Cheung, L. W., Peterson, K. E., Cho-mitz, G., Cradle, J. H., Dart, H., et al. (1999). Impact of a school-based interdisciplinary intervention on diet and physical activity among urban primary school children: Eat well and keep moving. Archives of Pediatric and Ado-lescent Medicine, 153(9), 975-83.
Greves, H. M., & Rivara, F. P. (2006). Report card on school snack food policies among the United States’ largest school districts in 2004-2005: Room for improve-ment. International Journal of Behavior, Nutrition, and Physical Activity, 3, 1.
Hoelscher, D. M., Feldman, H. A., Johnson, C. C., Lytle, L. A., Osganian, S. K., Parcel, G. S., et al. (2004). School-based health education programs can be main-tained over time: Results from the CATCH institutional-ization study. Preventive Medicine, 38(5), 594-606.
hooks, b. (1994). Sisters of the yam: Black women and self-recovery. Cambridge, MA: South End Press.
Huang, T. T., & Horlick, M. N. (2007). Trends in child-hood obesity research: A brief analysis of NIH-supported efforts. Journal of Law, Medicine, & Ethics, 35(1) 148-53.
Huhman, M., Potter, L. D., Wong, F. L., Banspach, S. W., Duke, J. C., & Heitzler, C. D. (2005). Effects of a mass media campaign to increase physical activity among children: Year-1 results of the VERB campaign. Pediatrics, 116(2), e277-84.
Institute of Medicine. (2005). Preventing childhood obesity: Health in the balance. Washington, DC: National Academies Press.
Institute of Medicine. (2006). Food marketing to chil-dren and youth: Threat or opportunity? Washington, DC: National Academies Press.
Johns Hopkins Bloomberg School of Public Health. (2002). Public health schools offer their support to “Meatless Monday” Health Campaign. Retrieved June 25, 2007, from http://www.jhsph.edu/publichealthnews/press_releases/PR_2002/meatless_deans.html.
Keith, S. W., Redden, D. T., Katzmarzyk, P. T., Boggiano, M. M., Hanlon, E. C., Benca, R. M., et al. (2006). Puta-tive contributors to the secular increase in obesity: explor-ing the roads less traveled. International Journal of Obesity, 30(11), 1585-94.
Kelly B. (2005). To quell obesity, who should regulate food marketing to children? Global Health, 1, 9.

2�Winter 2007
Kimm, S. Y., & Obarzanek, E. (2002). Childhood obe-sity: A new pandemic of the new millennium. Pediatrics, 110(5), 1003-1007.
Krebs-Smith, S. M., Cook, A., Subar, A. F., Cleveland, L., Friday, J., & Kahle, L. L. (1996). Fruit and vegetable intakes of children and adolescents in the United States. Archives of Pediatric & Adolescent Medicine, 150(1), 81-86.
Kumanyika, S. (2003). SHARE overview. Retrieved Janu-ary 10, 2007, from http://www.cceb.upenn.edu/pages/share/overview.html.
Kumanyika, S., Jeffery, R. W., Morabia, A., Ritenbaugh, C., & Antipatis, V. J. (2002). Public Health Approaches to the Prevention of Obesity (PHAPO) Working Group of the International Obesity Task Force (IOTF). Obesity prevention: The case for action. International Journal of Obesity and Related Metabolic Disorders, 26(3), 425-36.
Lytle, L., Kubik. M., Perry, C., et al. (2006). Influencing healthful food choices in school and home environments: Results from the TEENS study. Preventive Medicine, 43, 8-13.
Lytle, L. A., Murray, D. M., Perry C. L., Storey, M., Bir-mbaum, A. S., Kubik, M. Y., et al. (2004). School-based approaches to affect adolescents’ diets: Results from the TEENS study. Health Education & Behavior, 31, 270-87.
McKenzie, T. L., Sallis, J. F., & Nader, P. R. (1991). SOFIT: System for observing fitness instruction time. Journal of Teaching in Physical Education, 11, 195-205.
Moore, L. V, & Diez Roux, A. V. (2006). Associations of neighborhood characteristics with the location and type of food stores. American Journal of Public Health, 96(2), 325-31.
Narayan, K. M., Boyle, J. P., Thompson, T. J., Sorensen, S. W., & Williamson, D. F. (2003). Lifetime risk for dia-betes mellitus in the United States. Journal of the American Medical Association, 290(14), 1884-90.
National Institute of Child Health & Human Develop-ment. (2005). Media Smart Youth: Eat, Think, and Be Active! Retrieved February 25, 2007, from http://www.nichd.nih.gov/msy/msy.htm.
Nicklas, T. A., Elkasabany, A., Srinivasan, S. R., & Beren-son, G. (2001). Trends in nutrient intake of 10-year-old children over two decades (1973-94) : The Bogalusa Heart Study. American Journal of Epidemiology, 153(10), 969-77.
Nord, M., Andrews, M., & Carlson, S. (2005). House-hold food insecurity in the United States, 2004. USDA Economic Research Service, Economic Research Report Number 11.
Potts-Datema, B. (2004). Healthy kids—Healthy adults: Teaching kids how to live a healthy life. Retrieved Septem-ber 20, 2007, from http://www.nasbe.org/publications/Calories_In_Calories_Out/PDF%20Documents%20for%20web/Mr.%20Bill%20Potts-Datema%20-%20Healthy%20Kids%20Healthy%20AdultsbTeaching%20Kids%20How%20to%20Live%20a%20Healthy%20Life.pdf.
Quaid, L. (2006). Government adding fruits and veg-etables to WIC moms’ shopping list. Retrieved September 20, 2007, from http://www.dhs.ca.gov/director/owh/owh_main/pubs_events/news_articles/well_women/08.2006wicfood.pdf.
Razak, F., Anand, S. S., Shannon, H., Vuksan, V., Davis, B., Jacobs, R., Teo, K. K., et al. (2007). Defining obe-sity cut points in a multiethnic population. Circulation, 115(16), 2111-2118.
Rees, R., Kavanagh, J., Harden, A., Shepherd, J., Brun-ton, G., Oliver, S., Oakley, A. (2006). Young people and physical activity: A systematic review matching their views to effective interventions. Health Education Research, 21(6), 806-825.
Ritenbaugh, C., Kumanyika, S.K, Jeffrey, R.W., Morabia, A., & Antipatis, V.J. (1999). Caught in the causal web: A new perspective on social factors affecting obesity. Healthy Weight Journal, 13, 88-89.
Robert Wood Johnson Foundation. (2007). Program areas: Childhood obesity. Retrieved September 20, 2007, from http://www.rwjf.org/programareas/programarea.jsp?pid=1138.
Romero-Corral, A., Montori, V. M., Somers, V. K., Korinek, J., Thomas, R. J., Allison, T. G., et al. (2006). Association of bodyweight with total mortality and with cardiovascular events in coronary artery disease: A system-atic review of cohort studies. Lancet, 368(9536), 666-78.
Sallis, J.F., & Glanz, K. (2006). The role of built environ-ments in physical activity, eating, and obesity in child-hood. The Future of Children, 16(1), 89-108.
Sallis, J.F., McKenzie, T.L., Alcaraz, J.E., Kolody, B., Faucette, N., Hovell, M.F. (1997). The effects of a 2-year physical education program (SPARK) on physical activity and fitness in elementary school students. Sports, Play and Active Recreation for Kids. American Journal of Pub-lic Health, 87(8), 1328-34.

22 Perspectives on Childhood Obesity Prevention: Recommendations from Public Health Research and Practice
Salmon, J., & Timperio, A. (2007). Prevalence, trends and environmental influences on child and youth physical activity. Medicine and Sport Science, 50, 183-99.
Schlosser, E. (2001). Fast food nation: The dark side of the all-American meal. New York: Houghton Mifflin Company.
Schoonover, H., & Muller, M. (2006). Food without thought: How U.S. policy contributes to obesity. Retrieved January 20, 2007, from http://www.iatp.org/iatp/publi-cations.cfm?accountID=258&refID=80627.
Schwartz M.B., & Brownell K.D. (2007). Actions neces-sary to prevent childhood obesity: creating the climate for change. Journal of Law, Medical & Ethics, 35(1):78-89
Staunton, C. E, Hubsmith, D., & Kallins, W. (2003). Promoting safe walking and biking to school: The Marin County success story. American Journal of Public Health, 93(9), 1431-4.
Strauss, R. S., & Pollack, H. A. (2003). Social marginal-ization of overweight children. Archives of Pediatric and Adolescent Medicine, 157, 746-52.
United States Department of Health & Human Services. (2007). The surgeon general’s call to action: Overweight and obesity at a glance. Retrieved September 20, 2007, from http://www.surgeongeneral.gov/topics/obesity/calltoaction/fact_glance.htm.
Urban Nutrition Initiative. (2007). University of Penn-sylvania Center for Community Partnerships. Retrieved March 20, 2007, from http://www.urbannutrition.org.
Wang, Y., & Beydoun, M. A. (2007). The obesity epi-demic in the United States—Gender, age, socioeconomic, racial/ethnic, and geographic characteristics: A system-atic review and meta-regression analysis. Epidemiologic Reviews. Retrieved June 21, 2007, from http://epirev.oxfordjournals.org/cgi/reprint/mxm007v1.
Wang, Y., Zhang, Q. (2006). Are American children and adolescents of low socioeconomic status at increased risk of obesity? Changes in the association between overweight and family income between 1971 and 2002. American Journal of Clinical Nutrition, 84(4), 707-16.
Weiss, R.I., & Smith, JA. (2004). Legislative approaches to the obesity epidemic. Journal of Public Health Policy, 25(3-4), 379-90.
Wiecha, J. L., Peterson, K. E., Ludwig, D. S., Kim, J., Sobol, A., & Gortmaker, S. L. (2006). When children eat what they watch: Impact of television viewing on dietary intake in youth. Archives of Pediatric and Adolescent Medicine, 160(4), 436-42.

2�Winter 2007
Appendix I: Reports Reviewed
Bolen, E, & Hecht, K. (2003). Neighborhood groceries: New access to healthy food in low-income communities. San Francisco, CA: California Food Policy Advocates.
Budd, G. M., & Volpe, S. L. (2006). School-based obe-sity prevention: Research, challenges, and recommenda-tions. Journal of School Health, 76(10), 485-95.
Centers for Disease Control and Prevention. (1996). Guidelines for school health programs to promote lifelong healthy eating. Morbidity and Mortality Weekly Report 45, no. RR-9,1-41.
Ebbeling, C. B., Pawlak, D. B., & Ludwig, D. S. (2002). Childhood obesity: Public-health crisis, common sense cure. Lancet, 360(9331), 473-82.
Hill, J. O., & Trowbridge, F. L. (1998). Childhood obe-sity: Future directions and research priorities. Pediatrics, 101(3), 570-574.
Kimm, S. Y. S., & Obarzanek, E. (2002). Childhood obesity: A new pandemic of the new millennium. Pediatrics, 110(5), 1003-1007.
Koplan, J. P., Liverman, C. T., & Kraak, V. I,; Committee on Prevention of Obesity in Children and Youth. (2005). Preventing childhood obesity: Health in the balance. Journal of the American Dietetic Association, 105(1):131-8.
Flynn, M. A., McNeil, D. A., Maloff, B., Mutasingwa, D., Wu, M., Ford, C., & Tough, S. C. (2006). Reducing obesity and related chronic disease risk in children and youth: A synthesis of evidence with “best practice” recom-mendations. Obesity Review, 7(Suppl 1), 7-66.
Foxhall, K. (2006). Beginning to begin: Reports from the battle on obesity. American Journal of Public Health, 96(12), 2106-2112.
Institute of Medicine. (2005). Preventing childhood obesity: Health in the balance. Washington, DC: National Academies Press.
Institute of Medicine. (2007). Progress in preventing child-hood obesity: How do we measure up? Washington, DC: National Academies Press.
Story, M., Kaphingst, K. M., & French, S. (2006). The role of schools in obesity prevention. The Future of Chil-dren,16(1),109-42.
Wechsler, H., McKenna, M. L., Lee, S. M., & Dietz, W. H. (2004). The role of schools in preventing childhood obesity. The State Education Standard, 5(2), 4-12.
Appendix II: Key Consultants
JaniceBowie,PhD, Assistant Professor, Department of Health, Behavior, and Society, Johns Hopkins Bloom-berg School of Public Health
BenjaminCaballero,MD,PhD, Professor, Department of International Health, Division of Human Nutrition, Johns Hopkins Bloomberg School of Public Health
PennyGordon-Larsen,PhD, Assistant Professor, Depart-ment of Nutrition, University of North Carolina School of Public Health
ShirikiKumanyika,PhD, Professor of Epidemiology, University of Pennsylvania School of Medicine
LeslieLytle,PhD, Professor, Division of Epidemiology and Community Health, University of Minnesota
FelicityNorthcott,PhD, Lecturer, School of Arts & Sci-ences, Women’s Studies, Johns Hopkins University
MargaritaTreuth,PhD, Associate Professor, Department of International Health, Division of Human Nutrition, Johns Hopkins Bloomberg School of Public Health
LaraTrifiletti,PhD, Assistant Professor, Center for Injury Research and Policy, Columbus Children’s Hospital, Ohio State University
DavidWallinga,MD,MPA, Director of the Food and Health Program, Institute for Agriculture and Trade Policy
YoufaWang,PhD, Assistant Professor, Department of International Health, Division of Human Nutrition, Johns Hopkins Bloomberg School of Public Health