peter gonda conservative institute of m.r. Štefánik; socia fdn. slovakia financing of long term...
TRANSCRIPT

PETER GONDAConservative Institute of M.R. Štefánik; Socia Fdn.
SLOVAKIA
Financing of Long Term Care in Slovakia: Comparison with other
OECD Countries
„Development in Community-Based Care and Public Policy“
(IAHSA Conference „Creative Solutions for an Aging Society: Sharing the Wisdom, Norway, 27.-29. June 2005)

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 2
1. Starting points Long term care in Slovakia = virtual „system“
! System of LTC financing LTC for relevant clients (frail elderly and severe disabled people) does not exist, since:
• financing a care for any such client has absolutely different arrangements in social and health care system,
• even same or similar services in social and health sectors are financed differently = financing according to sectors and type of institutions, not clients and type of expenditure)
Slovakia (similarly as other new EU members) needs to built a system of LTC, including system of LTC financing.

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 3
1. Starting points Economic situation – still limiting factor of financing
social and health systems, because:
growing, but still insufficient performance of economic entities (Chart 1)
limited public sources for LTC financing, accompanied with public finance deficit and excessive and distorted public expenditure (high demands for other expenditures) – „crowding out in public expenditure“ – Chart 2
• growing, but still low income of many individuals and households (distinctively LTC clients: old age and disability retired)

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 4
1. Economic and political framework
Chart 1 Level of GDP per capita Slovakia to EU-15 and real change of GDP Slovakia
0
25
50
75
100
1995 1996 1997 1998 1999 2000 2001 2002 2003
GD
P S
lov
ak
ia /
EU
-15
(%
)
0
2
4
6
8
Re
al
ec
on
om
ic g
row
th (
%)
GDP Slov akia / EU-15 (%) Real change of GDP Slov . (%)
Source: Eurostat, Statistical Office of the SR

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 5
1. Starting points
Chart 2 Government expenditure by functions in Slovakia (2003)
Source: Author, Ministry of Finance of the SR
Other5,9%
General Public Service 11,9%
Defense4,3%
Security4,8%
Education10,4%Health
20,0%
Economy11,1%
Social Security31,6%

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 6
1. Starting points
Political situation: health and social reforms inter alia have lead to:
• improvement in conditions for multi-source financing• more transparent financial flows• higher and more clear responsibility of stakeholders, but also• stronger pressure on people from LTC target groups
Commitment of the Slovak Government to create new (integrated) LTC system, but its implementation was postponed to 2006 = risk of non-acceptance by new government
Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 7
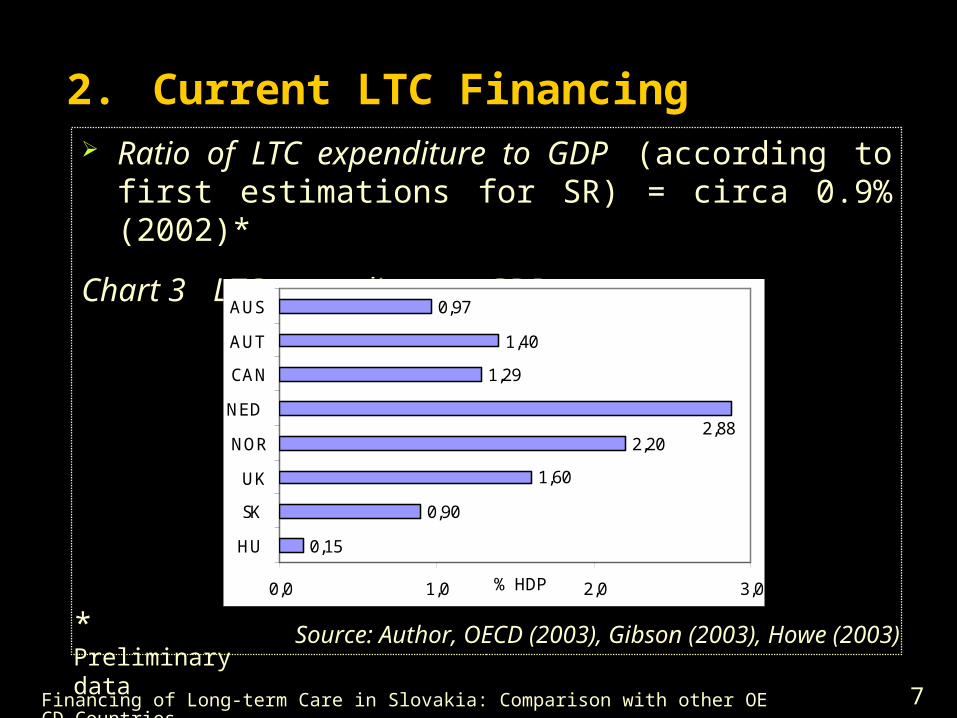
2. Current LTC Financing Ratio of LTC expenditure to GDP (according to first
estimations for SR) = circa 0.9% (2002)*
Chart 3 LTC expenditure to GDP
0,15
0,90
1,60
2,20
1,29
1,40
0,97
2,88
0,0 1,0 2,0 3,0
HU
SK
UK
NOR
NED
CAN
AUT
AUS
% HDP
Source: Author, OECD (2003), Gibson (2003), Howe (2003)* Preliminary data

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 8
2. Current LTC Financing Structure of LTC expenditure (2002)*:
1. Low expenditure on institutional care as % of total LTC spending (circa 38%) does not mean adequate domination home and community care
2. Expenditure on benefits (55% of total expenditure) exceeds the costs on services (45%)
3. Expenditure in social care (circa 90%) considerable dominate to the health care expenditure (10%)
4. Public expenditure (92%) significantly exceeds the private (8%).

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 9
2. Current LTC Financing
Community – institutional mix
REASON of this paradox (1): structure of „non-institutional“ care
- home and community care = 7% of total expenditure
- benefits intended to home care 21% of total expend.
- benefits no intended to care 34% of total expenditure
Home and community care, incl. cash benefits to home care, in SR > home and community share in many OECD countries, but but it is contrary in case „without all cash benefits“ (Chart 4)

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 10
2. Current LTC Financing
Community – institutional mix
Chart 4 Institutional vs. home and community care
Notes: (1) Expenditure on home/community care (and total expenditure) include also benefits directly related to care, but no compensation benefits.
(2) Expenditure on home/community care (and total expend.) do not include cash benefits.
Source: Author, OECD (2003)
62
84 85 7969
58
84
38
16 15 2131
42
16
0%
50%
100%
G AUS CAN NED SCOT SK (1) SK (2)
Institution. Home / Community

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 11
2. Current LTC Financing Public-private mix
Chart 5 Comparing public and private expenditure (2002)
Source: Autor, OECD (2003), Howe (2003)
0% 50% 100%
Public Private

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 12
2. Current LTC Financing
Public-private mix of financing
Predomination of public source (about 92% in 2002) is result of:
! significant difference between financing relevant clients in health care and social system, since:
- health care – almost „free of charge“ access to services (with marginal user fees for dental care, related services, issuing prescription, drugs...
- social system – means tested payments for services in facilities (partially for lodging, boarding, maintenance and attendance care)...

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 13
2. Current LTC Financing Public-private mix: financing
Predomination of public source is also result of:
! difference between type of public source
- health care – from mandatory and public social/health insurance (financed by public and private Health Insurance Companies)
- social system – from taxes (financed by central and local governments)
Since social system is dominant, thus taxes are main sources of (public) LTC are taxes (general taxation)
– similar as in Norway and UK, but in contrary to „contributions system“ in Netherlands (Chart 5)

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 14
2. Current LTC Financing
Chart 6 Comparison of public sources in selected countries
Victoria (AUS)
Austria Ontario (CAN)
Netherlands
Norway Scotland (UK)
SLOVAKIA
Taxation
x
x
x
x
x
x
(in social sector)
Public
Mandat.
soc./health insurance
x
(negligible
)
x x
(in health sector)
Source: Author, OECD (2003), Howe (2003)

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 15
2. Current LTC Financing
Public-private mix in a social and health systemsChart 7 Example of structure of financing social and health facilities
Retirement Home
State
Budget
69%
Out of
23%
Local
Budget
s
8%
Geriatric departments
Other22,5%
Out of pocke
t0,1%
Social Health Insurance
77,4%
S OCIAL
HEALTH
Source: MoH SR, MLSaF SR, author
Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 16
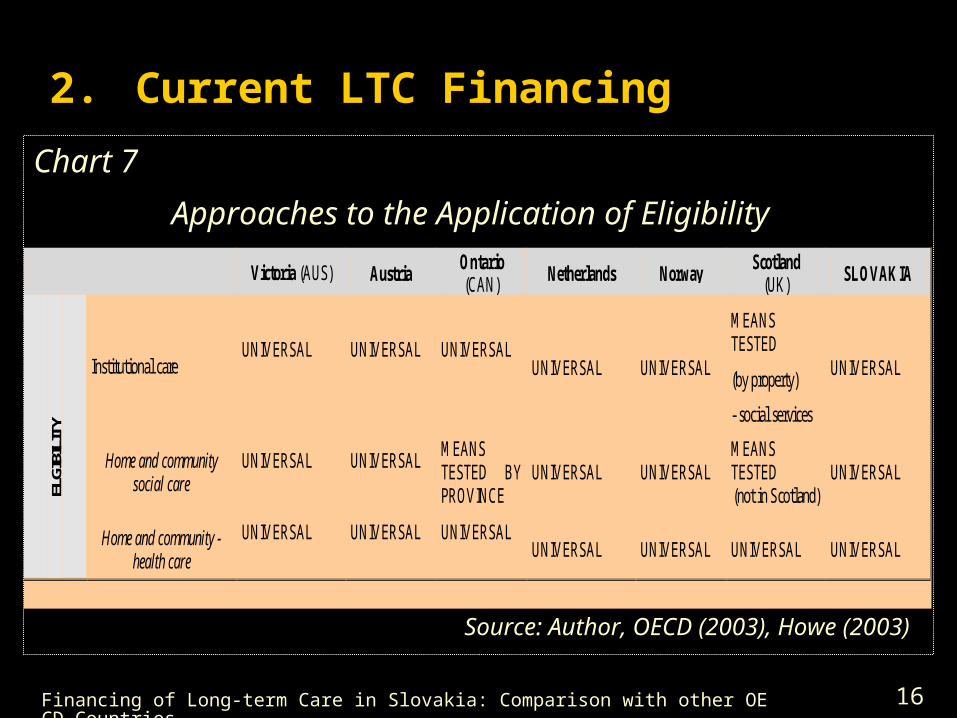
2. Current LTC Financing
Chart 7
Approaches to the Application of Eligibility
Source: Author, OECD (2003), Howe (2003)
Victoria (AUS) Austria Ontario (CAN) Netherlands Norway
Scotland (UK) SLOVAKIA
Institutional care UNIVERSAL
UNIVERSAL
UNIVERSAL
UNIVERSAL UNIVERSAL
MEANS TESTED
(by property)
- social services
UNIVERSAL
Home and community social care
UNIVERSAL
UNIVERSAL
MEANS TESTED BY PROVINCE
UNIVERSAL UNIVERSAL MEANS TESTED (not in Scotland)
UNIVERSAL
ELGI
BILI
TY
Home and community - health care
UNIVERSAL
UNIVERSAL
UNIVERSAL
UNIVERSAL UNIVERSAL UNIVERSAL UNIVERSAL

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 17
2. Current LTC Financing
Chart 9 Approaches to the Application of Co-payments
Source: Author, OECD (2003), Howe (2003)
Victoria (AUS) Austria Ontario (CAN) Netherlands Norway Scotland
(UK) SLOVAKIA
Institutional care
MEANS TESTED (income and assets)
MEANS TESTED Additional payments to cover real costs
MEANS TESTED
(over income limit)
- by province
MEANS TESTED (income) - for food and housing (nominal amounts)
MAX. 80% of client´s income
MEANS TESTED ( assets ) - social only (personal care)
MEANS TESTED (income
(in social facilities only)
Home and community social care
MEANS TESTED (income and paying capability)
Additional payments to cover real costs
MEANS TESTED (income) - by province
MEANS TESTED
(by income)
MEANS TESTED (so-called optimum payments)
MEANS TESTED By local administration
(not in Scotland)
MEANS TESTED (by income) C
O-P
AY
ME
NT
S
Home and community - health care
MEANS TESTED (income and paying capability)
-
-
MEANS TESTED (by income) nominal amounts
-
x (apart from
NHS)
-

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 18
2. Current LTC Financing
Chart 10 Comparisons of Approaches to the LTC Integration
Victoria (AUS)
Austria Ontario (CAN) Netherlands Norway Scotland
(UK) SLOVAKIA
Social vs. Health LTC Services INTEGRATED
Separated by service types a
INTEGRATED within health sector
INTEGRATED within health sector (AWBZ)
INTEGRATED on local level
- separated (partially integrated in Scotland)c
- (diverse)d
LTC services providers INTEGRATED CONSISTENT
PRINCIPLES INTEGRATED within health sector
INTEGRATED
-
(partially in Scotland)c
- (diverse)
With
in th
e LT
C s
yste
m
Target groups INTEGRATED INTEGRATED -
INTEGRATED within health sector
-
LTC
sys
tem
com
pare
d to
Hea
lth a
nd S
ocia
l Se
ctor
s
LTC service vs. social and health sectors
INDEPENDENT.
INDEPENDENT. INTEGRATED
PART OF HEALTH SECTOR (AWBZ)
INTEGRATED on local level
INTEGRATED WITHIN SOCIAL SECTOR
-
Source: Author, OECD (2003), Howe (2003)

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 19
2. Current LTC Financing Chart 11 Comparison of containing the costs of LTC
COST RESTRICTIONS Victoria (AUS)
Austria Ontario (CAN)
Netherlands Norway Scotland (UK) SLOVAKIA
- on demand side
x (by asses. committee
ACAT)
x
(stoppage of hospitalisation benefit disbursement)
x
-
x
(professional needs assessment)
x (budget limitation - UK)
x (e.g. by asses. committee)
- on supply side
x (number of places, level
resources, etc. restricted)
x
(benefit reduction in certain client categories)
x
-
x (partially, on the basis of resource availability on local level)
x
x (budget limitations on local level and hard budgetary
constraints - Health Ins. Companies)
Source: Author, OECD (2003), Howe (2003)

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 20
3. Current problems and future risks Main problems of current financing:
excessive share of public financing and low pressure on personal responsibility (particularly marginal private financing in health part of LTC)
absolutely different arrangements of LTC financing in social and health parts (sector-based financing)
financing does not correspond to character of expenses (nursing care, related services...) and to different responsibilities of payers
Insufficient focusing on real needs clients, their families and relatives as part of home and community care.

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 21
3. Current problems and future risks
insufficient cost restrictions, e.g. on demand side followed from no strict „gate-keeper“ (missing clear link between assessment and financing)
huge portion of cash benefits, mainly allowances does not relating to care (but income support) in comparison with lack of services
low weight of home and community services and their problematic financing by Local and Regional Self-governments (with no clear responsibilities)
inefficient financing with additional costs and negative impacts on quality and efficient accessibility of services.

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 22
3. Current problems and future risks
Community–institutional mix
Key problems of home and community care followed from:
• no strict responsibilities of local and regional self-governments for financing LTC (splited between them each other and between them and central government), e.g.
Example: contradictory responsibility in providing attendance care by Local Governments and cash Home Care Benefit (HCB) by Central Government
RESULT: rapid increasing of recipients of HCB, thereby increasing also costs = risks for financing in future

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 23
3. Current problems and future risks Pressures on the increase of LTC expenses due to:
• ageing of population – considerably increasing population over 65 after 2011 (Chart 12) and earlier significant rising of number citizens over 80 years (Chart 13),
• rising requirements of clients, their families and client organizations to acquire more services with higher quality,
• expected increase in difficult diseases, incl. chronic diseases various forms of handicaps...
• new, more expensive, technologies, devices...

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 24
3. Current problems and future risks
Chart 12 Year on year increase of Slovak citizens over 65 years
Source: Infostat (2003), Author, MoH SR
0
9000
18000
27000

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 25
3. Current problems and future risks
Chart 13 Number of Slovak citizens over 80 years
120
170
220
2005 2010 2015 2020 2025
tis.
Source: Infostat (2002), Author, MoH SR

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 26
4. Systemic change of LTC financing
MAIN OBJECTIVE
= to create financially sustainable system, which will support overall goal of new integrated LTC system „improving quality, accessibility and effectiveness LTC for persons with functional disabilities and thereby improving quality of their life and quality of life their famililies and relatives“.
Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 27
4. Systemic change of LTC financing KEY PRINCIPLES
= universal entitlement of assessed individuals to care on standard level with strictly controlled expenses limited by the budget and with requirements of means tested co-payments
= multi-source financing (public-private mix) with same setting of conditions for all entities
= strict link between assessment and financing
= financing according to (real need of) client and type of expenses
= preference financing of home and community-based care in comparison with financing of institutional care

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 28
4. Systemic change of LTC financing
PROPOSED FINANCING – conceptual framework
1. Public sources = financing LTC on a standard level for assessed clients
1.1 Taxes – intended for financing social part of LTC
- State Budget: cash benefits (also for aids and equipment)
- Local and Regional Budgets: financing social services in home, community, and residential care
1.2 Public health insurance – intended for financing health part of LTC (mainly nursing care)

Financing of Long-term Care in Slovakia: Comparison with other OECD Countries 29
4. Systemic change of LTC financing2. Private sources
2.1 Client = financing of costs on related services (total cost of boarding and housing), but with regard his/her
financial possibilities
- responsibility of Local Government to finance part of payment for client, who is not able to pay full costs
2.2 Other (voluntary) – from clients, relatives, sponsors...
DESIRABLE RESULTS:
shifting weight of responsibility from Central Government to clients and Self-Governments
shifting weight of LTC expenditure from cash benefits to home and community services...