pharmacodynamic and antiretroviral activities of combination
TRANSCRIPT
M A J O R A R T I C L E
Pharmacodynamic and Antiretroviral Activitiesof Combination Nanoformulated Antiretroviralsin HIV-1–Infected Human Peripheral BloodLymphocyte–Reconstituted Mice
Upal Roy,1,a JoEllyn McMillan,1,a Yazen Alnouti,5 Nagsen Gautum,5 Nathan Smith,1 Shantanu Balkundi,1 Prasanta Dash,1
Santhi Gorantla,1 Andrea Martinez-Skinner,1 Jane Meza,4 Georgette Kanmogne,1 Susan Swindells,2 Samuel M. Cohen,3
R. Lee Mosley,1 Larisa Poluektova,1 and Howard E. Gendelman1
1Department of Pharmacology and Experimental Neuroscience, College of Medicine, 2Department of Internal Medicine, College of Medicine,3Department of Pathology and Microbiology, College of Medicine, 4Department of Biostatistics, College of Public Health, and 5Department ofPharmaceutical Sciences, College of Pharmacy, University of Nebraska Medical Center, Omaha
Lack of adherence, inaccessibility to viral reservoirs, long-term drug toxicities, and treatment failures arelimitations of current antiretroviral therapy (ART). These limitations lead to increased viral loads, medicineresistance, immunocompromise, and comorbid conditions. To this end, we developed long-acting nanofor-mulated ART (nanoART) through modifications of existing atazanavir, ritonavir, and efavirenz suspensionsin order to establish cell and tissue drug depots to achieve sustained antiretroviral responses. NanoART’sabilities to affect immune and antiviral responses, before or following human immunodeficiency virus type 1infection were tested in nonobese severe combined immune-deficient mice reconstituted with human periph-eral blood lymphocytes. Weekly subcutaneous injections of drug nanoformulations at doses from 80 mg/kgto 250 mg/kg, 1 day before and/or 1 and 7 days after viral exposure, elicited drug levels that paralleled thehuman median effective concentration, and with limited toxicities. NanoART treatment attenuated viral rep-lication and preserved CD4+ Tcell numbers beyond that seen with orally administered native drugs. Theseinvestigations bring us one step closer toward using long-acting antiretrovirals in humans.
Long-acting, parenterally administered antiretroviralnanoformulations are of immediate need [1, 2]. Thosewho would benefit most are patients for whom drugadherence and availability are limited and/or those whocannot ingest drug formulations [2, 3], leading to viralresistance patterns [4]. As monocytes and monocyte-derived macrophages (MDMs) are reservoirs forhuman immunodeficiency virus type 1 (HIV-1) andcan uptake, transport, and release virus into infected
tissues, our laboratory developed long-acting nano-formulated antiretroviral therapy (nanoART) inmonocyte-macrophage carriers [5–11]. Surfactant com-position, size, and charge of the particles were evaluatedto optimize cell entry and release of atazanavir (ATV),ritonavir (RTV), and efavirenz (EFV) as these hydro-phobic drugs are easily encased and commonly used inthe clinic [7, 10–15]. Uptake and release of nanoARTinto and from MDMs were at drug levels at or beyondthe half-maximal effective concentration (EC50) (EFV,1.7–25 nM; RTV, 35–200 nM; ATV, 2–5 nM) [16] withlimited or no cytotoxicity. On the basis of these out-comes, the most effective ART nanoformulations wereselected for in vivo studies in HIV-1ADA–infected,nonobese diabetic, severe combined immunodeficientcommon cytokine receptor γ chain–deleted (NOD/scid-γc
null [NSG]) mice reconstituted with human peri-pheral blood lymphocytes (PBLs) (PBL-NSG mice) [17].Two schemes were used for testing. First, 1 dose of
Received 30 November 2011; accepted 27 January 2012; electronically pub-lished 17 July 2012.
aU. R. and J. M. contributed equally to this work.Correspondence: Howard E. Gendelman, MD, Department of Pharmacology and
Experimental Neuroscience, 985880 Nebraska Medical Center, Omaha, NE 68198-5880 ([email protected]).
The Journal of Infectious Diseases 2012;206:1577–88© The Author 2012. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/infdis/jis395
NanoART-Treated HIV-1–Infected Mice • JID 2012:206 (15 November) • 1577
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021

nanoART was injected subcutaneously 1 day before HIV-1ADAinfection with replicate native drugs given orally. Second, PBL-NSG mice were infected with HIV-1ADA before subcutaneousadministration of nanoART. ART activity was evaluated by de-termination of virus suppression and preservation of CD4+ Tcells. HIV-1gag RNA by real-time polymerase chain reaction(RT-PCR) in spleen and immunohistochemical quantitation ofinfected cells by staining for HIV-1p24 proteins were assessedwith CD4+ T-lymphocyte numbers. Systemic toxicities were en-hanced as a consequence of graft-versus-host disease (GVHD).These results provide proof-of-concept that stable nanoARTformulations provide sustained drug levels in serum and tissuesabove the EC50 and afford effective antiretroviral responses in-dependent of ex vivo macrophage loadings.
MATERIALS AND METHODS
Preparation and Characterization of nanoARTFree base RTV and EFV were obtained from Shengda Phar-maceutical Co and Hetero Labs Ltd, respectively. ATV-sulfatewas purchased from Gyma Laboratories of America Inc. Thesurfactant (excipient) used in generating all formulationswas poloxamer-188 (P188; Sigma-Aldrich) with or without1,2-distearoyl-phosphatidyl-ethanolamine-methyl-polyethyle-neglycol conjugate-2000 (mPEG2000-DSPE, Genzyme Phar-maceuticals LLC). Final synthesis of the nanosuspension wasachieved by either wet-milling or homogenization [18]. Druglevels were analyzed by reverse-phase high-performance liquidchromatography [7, 10, 12] and by ultraperformance liquidchromatography tandem mass spectrometry (UPLC-MS/MS)using a Waters ACQUITY UPLC coupled to an Applied Bio-systems 4000 Q TRAP quadruple linear ion trap hybrid massspectrometer [19]. For scanning electron microscopic exami-nations of nanoparticles, 10 µL of nanosuspension was dilutedin 1.5 mL of 0.2 µm filtered distilled water and prepared formorphologic examination using a Hitachi S4700 Field-Emis-sion Scanning Electron Microscope (Hitachi High Technolo-gies America, Inc). Human MDM uptake, retention, release,and antiviral activity of nanoART in vitro were determined[10]. Scoring of nanoART, including the polydispersity index(PDI), in vitro activity (particle uptake, drug retention andrelease, and antiretroviral activity), cytotoxicity, and pharma-cokinetics (PK), was made by assessment of decade-weightedratios (DWRs) [10]. This was determined for each nanoformu-lation where an arbitrary maximal (best) score of 10 was as-signed for each test performed. DWRs were calculated as areasunder the curve (AUC) for each formulation, proportional to10 AUC/AUCbest ratio. For example, a score of 9.7 reflected an8-hour nanoART drug “uptake value” of 29.6 µg drug/106
cells of 97% when compared to a “best” test result of 30.5 µg/106 cells seen in all assays. The DWR for in vitro activity ofeach formulation reflected the averages of differences for
nanoART uptake, retention, release, and antiretroviral activityin MDMs for each nanoART as compared to the best per-former. DWRs have been described in detail previously[10].Cell retention of drug was determined as drug remaining inthe cell whereas drug release was the amount of drug releasedinto media. Antiretroviral activity was determined over 15days. Scoring for in vitro toxicity was calculated as the averageof DWR based on highest alamarBlue (AbD Serotec) reduc-tion and lowest macrophage production of tumor necrosisfactor α (TNF-α). DWR scoring of PK was determined in vivoas a function of the highest serum drug levels in nanoART-treated mice (250 mg/kg, subcutaneous). Final scores werecomposite averages of all tests.
AnimalsMale NSG mice were purchased from the Jackson Laboratoryand housed in filter top cages with free access to food andwater under a 12-hour/12-hour light/dark cycle in accordancewith ethical guidelines for care of laboratory animals approvedby the Institutional Animal Care and Use Committee at theUniversity of Nebraska Medical Center.
Human Cell Isolation, Transplantation, and Viral InfectionHuman PBLs were purified from leukopaks by countercurrentcentrifugal elutriation and used to reconstitute NSG mice [20].PBLs were injected intraperitoneally into 8-week-old mice at30 × 106 PBLs per mouse [21]. For viral infections, the HIV-1ADA strain was propagated in human MDMs and was foundto be negative for endotoxin [22].
Biodistribution and Antiretroviral Activity of nanoARTTo determine dose-dependent serum drug concentrations andtissue distribution of nanoART, nonreconstituted NSG micewere injected subcutaneously on days 0 and 7 with nanoART(ATV and RTV at 80, 150, or 250 mg/kg). These correspondedto human doses of 6.5–20.3 mg/kg based on an interspeciesscaling factor of 12.3 [23]. Blood samples were collected atdays 1, 6, and 14 after drug administration (Figure 1A). Atstudy end (14 days after initial injection), tissue samples werecollected for drug biodistribution assay. NSG mice were recon-stituted with PBLs 7 days prior to subcutaneous nanoparticleadministration or oral drug delivery of native drugs(Figure 1B). One day after drug treatment, animals were in-fected intraperitoneally with HIV-1ADA at a dose of 104
median tissue culture infective dose per mouse. Animals werekilled on day 9 after drug treatment, and blood and tissuescollected for fluorescence-activated cell sorting (FACS) andviral load tests. PBL-reconstituted NSG mice were also infect-ed with HIV-1ADA after 7 days. Two doses of nanoART wereadministered subcutaneously, the first dose at 12 hours (day0) and the second at 7 days after infection. NanoART was ad-ministered as ATV and RTV at 250 mg/kg or ATV, RTV, and
1578 • JID 2012:206 (15 November) • Roy et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021
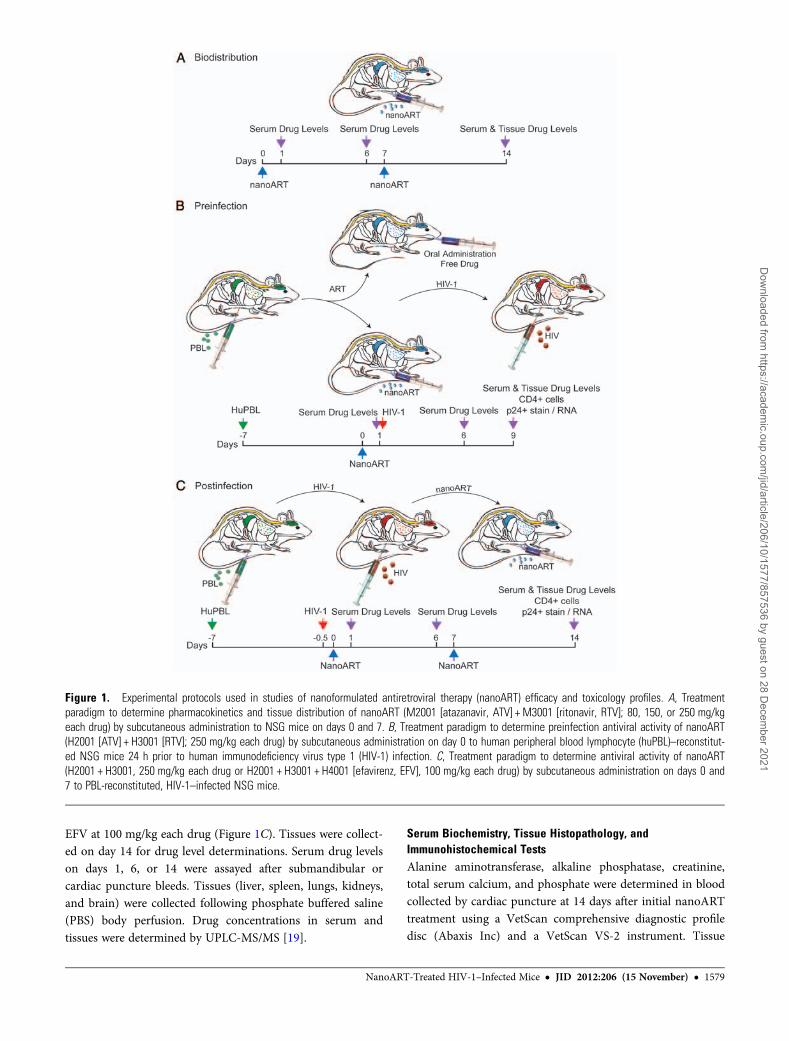
EFV at 100 mg/kg each drug (Figure 1C). Tissues were collect-ed on day 14 for drug level determinations. Serum drug levelson days 1, 6, or 14 were assayed after submandibular orcardiac puncture bleeds. Tissues (liver, spleen, lungs, kidneys,and brain) were collected following phosphate buffered saline(PBS) body perfusion. Drug concentrations in serum andtissues were determined by UPLC-MS/MS [19].
Serum Biochemistry, Tissue Histopathology, andImmunohistochemical TestsAlanine aminotransferase, alkaline phosphatase, creatinine,total serum calcium, and phosphate were determined in bloodcollected by cardiac puncture at 14 days after initial nanoARTtreatment using a VetScan comprehensive diagnostic profiledisc (Abaxis Inc) and a VetScan VS-2 instrument. Tissue
Figure 1. Experimental protocols used in studies of nanoformulated antiretroviral therapy (nanoART) efficacy and toxicology profiles. A, Treatmentparadigm to determine pharmacokinetics and tissue distribution of nanoART (M2001 [atazanavir, ATV] + M3001 [ritonavir, RTV]; 80, 150, or 250 mg/kgeach drug) by subcutaneous administration to NSG mice on days 0 and 7. B, Treatment paradigm to determine preinfection antiviral activity of nanoART(H2001 [ATV] + H3001 [RTV]; 250 mg/kg each drug) by subcutaneous administration on day 0 to human peripheral blood lymphocyte (huPBL)–reconstitut-ed NSG mice 24 h prior to human immunodeficiency virus type 1 (HIV-1) infection. C, Treatment paradigm to determine antiviral activity of nanoART(H2001 + H3001, 250 mg/kg each drug or H2001 + H3001 + H4001 [efavirenz, EFV], 100 mg/kg each drug) by subcutaneous administration on days 0 and7 to PBL-reconstituted, HIV-1–infected NSG mice.
NanoART-Treated HIV-1–Infected Mice • JID 2012:206 (15 November) • 1579
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021
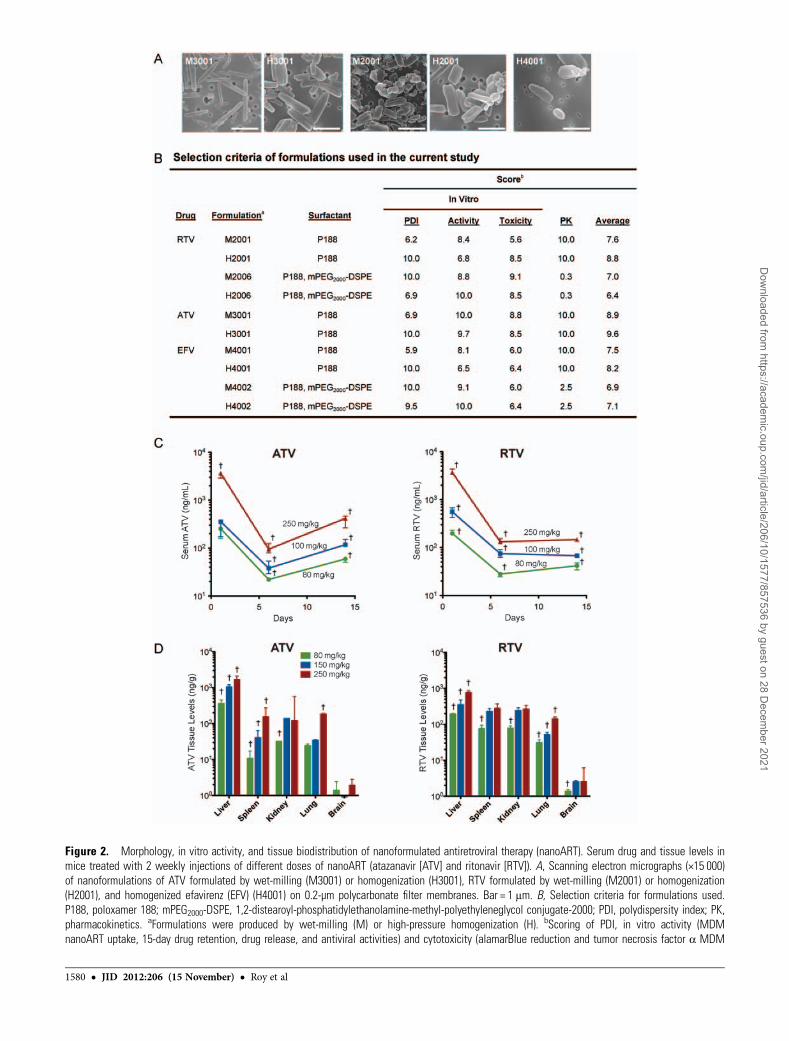
Figure 2. Morphology, in vitro activity, and tissue biodistribution of nanoformulated antiretroviral therapy (nanoART). Serum drug and tissue levels inmice treated with 2 weekly injections of different doses of nanoART (atazanavir [ATV] and ritonavir [RTV]). A, Scanning electron micrographs (×15 000)of nanoformulations of ATV formulated by wet-milling (M3001) or homogenization (H3001), RTV formulated by wet-milling (M2001) or homogenization(H2001), and homogenized efavirenz (EFV) (H4001) on 0.2-µm polycarbonate filter membranes. Bar = 1 μm. B, Selection criteria for formulations used.P188, poloxamer 188; mPEG2000-DSPE, 1,2-distearoyl-phosphatidylethanolamine-methyl-polyethyleneglycol conjugate-2000; PDI, polydispersity index; PK,pharmacokinetics. aFormulations were produced by wet-milling (M) or high-pressure homogenization (H). bScoring of PDI, in vitro activity (MDMnanoART uptake, 15-day drug retention, drug release, and antiviral activities) and cytotoxicity (alamarBlue reduction and tumor necrosis factor α MDM
1580 • JID 2012:206 (15 November) • Roy et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021
samples were collected on day 14, placed in 10% neutral buff-ered formalin, and embedded in paraffin. Five-micrometer-thick sections were cut and mounted on glass slides. Forhistopathological analysis, tissue sections were stained with he-matoxylin and eosin. Histopathological evaluations were per-formed in accordance with the guidelines of the Society ofToxicologic Pathology. Immunohistochemical staining usedmouse monoclonal antibodies (Dako) for HLA-DR (cloneCR3/43, 1:100) and HIV-1p24 (clone, Kal-1, 1:10) and thepolymer-based horseradish peroxidase–conjugated antimouseDako EnVision systems were used for secondary detection,then developed with 3,3-diaminobenzidine and counterstainedwith hematoxylin. Images were obtained with a NikonDS-Fi1 camera fixed to a Nikon Eclipse E800 microscope
using NIS-Elements F 3.0 software (Nikon Instruments). Thenumber of HIV-1p24+ cells per section was determined andexpressed as the percentage of total HLA-DR+ cells. For HIV-1gag RNA measurements, RNA from spleen sections was ex-tracted with TRIzol (Invitrogen) and reverse transcribed tocomplementary DNA with random hexamers and Moloneymurine leukemia virus reverse transcriptase (Invitrogen), andquantitative RT-PCR was performed [24].
FACS Analyses of T-Cell SubsetsAt study termination, blood samples were collected into ethyl-enediaminetetraacetic acid–coated tubes (BD Diagnostics),and spleen cells were resuspended in PBS. Blood leukocyte andspleen cell suspensions were tested for expression of human
Figure 2 Continued. production were determined as a decade weighted ratio (see Methods). Scoring of PK was determined as a function of thehighest serum drug levels 7 days after nanoART administration (250 mg/kg subcutaneously) to BALB/cJ mice. Drug levels of ATV and RTV weredetermined from serum on days 1, 6, and 14 (C) and tissues on day 14 (D) after 2 weekly subcutaneous injections of combined nanoART (ATV/RTV;M2001 + M3001; 80, 150, or 250 mg/kg each) given to nonreconstituted, noninfected NSG mice on days 0 and 7. Data are expressed as median ± 25th(serum) and 75th (serum and tissues) percentiles for 5 mice per group. Differences were determined by analysis of variance of rank-transformed valuesand Tukey post hoc analysis. †Significantly different from values for other doses at that day or tissue at P≤ .05.
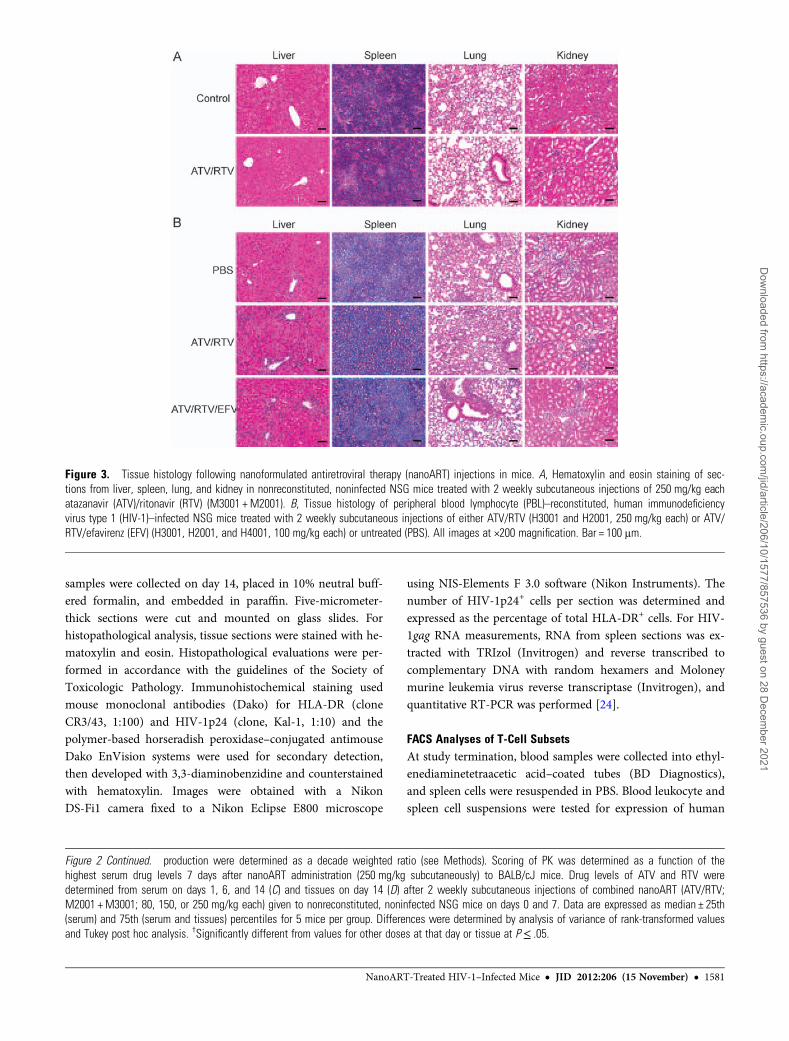
Figure 3. Tissue histology following nanoformulated antiretroviral therapy (nanoART) injections in mice. A, Hematoxylin and eosin staining of sec-tions from liver, spleen, lung, and kidney in nonreconstituted, noninfected NSG mice treated with 2 weekly subcutaneous injections of 250 mg/kg eachatazanavir (ATV)/ritonavir (RTV) (M3001 + M2001). B, Tissue histology of peripheral blood lymphocyte (PBL)–reconstituted, human immunodeficiencyvirus type 1 (HIV-1)–infected NSG mice treated with 2 weekly subcutaneous injections of either ATV/RTV (H3001 and H2001, 250 mg/kg each) or ATV/RTV/efavirenz (EFV) (H3001, H2001, and H4001, 100 mg/kg each) or untreated (PBS). All images at ×200 magnification. Bar = 100 μm.
NanoART-Treated HIV-1–Infected Mice • JID 2012:206 (15 November) • 1581
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021

CD45, CD3, CD4, and CD8 markers as 4-color combinations[25].
Statistical AnalysesBecause of limitations in sample size, descriptive statisticsused medians. Outcomes were compared between 2 groupsusing a Mann-Whitney test and data assessed among 3 ormore groups using 1-way analysis of variance after performinga rank transformation on the variables. Post hoc comparisonswere conducted using the Tukey method to adjust for multiple
comparisons. A P value ≤.05 was considered statisticallysignificant.
RESULTS
Characterization of nanoART FormulationsThe morphologic (shape), physicochemical (PDI and charge)and biologic characteristics (uptake, retention, release, and an-tiretroviral activity in MDMs) of the nanoARTs were assessed[7, 10, 12] (Figure 2). ATV nanoARTs were thin and rod-
Figure 4. Serum and tissue drug levels in human immunodeficiency virus type 1 (HIV-1)–infected peripheral blood lymphocyte (PBL)–NSG micetreated with 2 weekly injections of nanoformulated antiretroviral therapy (nanoART) combinations (atazanavir [ATV] and ritonavir [RTV] or ATV, RTV, andefavirenz [EFV]). Following subcutaneous injections of either ATV and RTV (H3001 and H2001; 250 mg/kg each) or ATV, RTV, and EFV (H3001, H2001,and H4001; 100 mg/kg each) given on days 0 and 7 to PBL-reconstituted, HIV-1–infected mice, drug levels of ATV, RTV, and EFV were determined inserum on days 1, 6 and 14 (A), and in liver, spleen, kidney, lung, and brain on day 14 (B). Data are expressed as median ± 25th (serum) and 75th (serumand tissues) percentiles for 8 mice per group.
Figure 5 Continued. spleen (right panel). A and B, Data are shown as individual data points and median ± 25th and 75th percentiles (bar ± whisker) for5–8 mice per group, analysis of variance of rank-transformed values, and significant differences determined by Tukey post hoc analyses, wherebyP < .01 compared to native drug–treated, PBL-reconstituted, HIV-1–infected mice. C, Tissue and serum drug levels of ATV (left panel) and RTV (rightpanel) on day 9 following subcutaneous injection of nanoART or native drugs to mice. Data are expressed as median ± 25th (serum) and 75th (serumand tissue) percentiles for 8 mice per group, analyzed by Mann-Whitney test and significant differences determined by Tukey post hoc analyses.*Significantly different from nanoART-treated, PBL-reconstituted, HIV-1–infected NSG mice at P≤ .01.
1582 • JID 2012:206 (15 November) • Roy et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021

Figure 5. Antiretroviral activities of nanoformulated antiretroviral therapy (nanoART) administered prior to human immunodeficiency virus type 1 (HIV-1)exposure. NanoART was delivered on day 0 as a combination of atazanavir (ATV) and ritonavir (RTV) (250 mg/kg each H3001 and H2001, subcutane-ously) to peripheral blood lymphocyte (PBL)–reconstituted NSG mice. Native drugs (250 mg/kg each ATV and RTV in PBS) were delivered by oral gavageon day 0. Mice were infected with HIV-1ADA on day 1. Spleens were harvested on day 9 after drug injection. A, Fluorescence-activated cell sortinganalysis shows the percentage of human CD4+ among total CD3+ T cells (left panel) and CD4+/CD8+ T-cell ratios (right panel) for spleens from individualmice. B, Percentages of HIV-1p24–expressing cells among human HLA-DR+ cells were determined from cell counts of immunohistochemistry fromsplenic tissues (left panel). HIV-1gag RNA expression normalized to glyceraldehyde-3-phosphate dehydrogenase (GAPDH) messenger RNA expression in
NanoART-Treated HIV-1–Infected Mice • JID 2012:206 (15 November) • 1583
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021
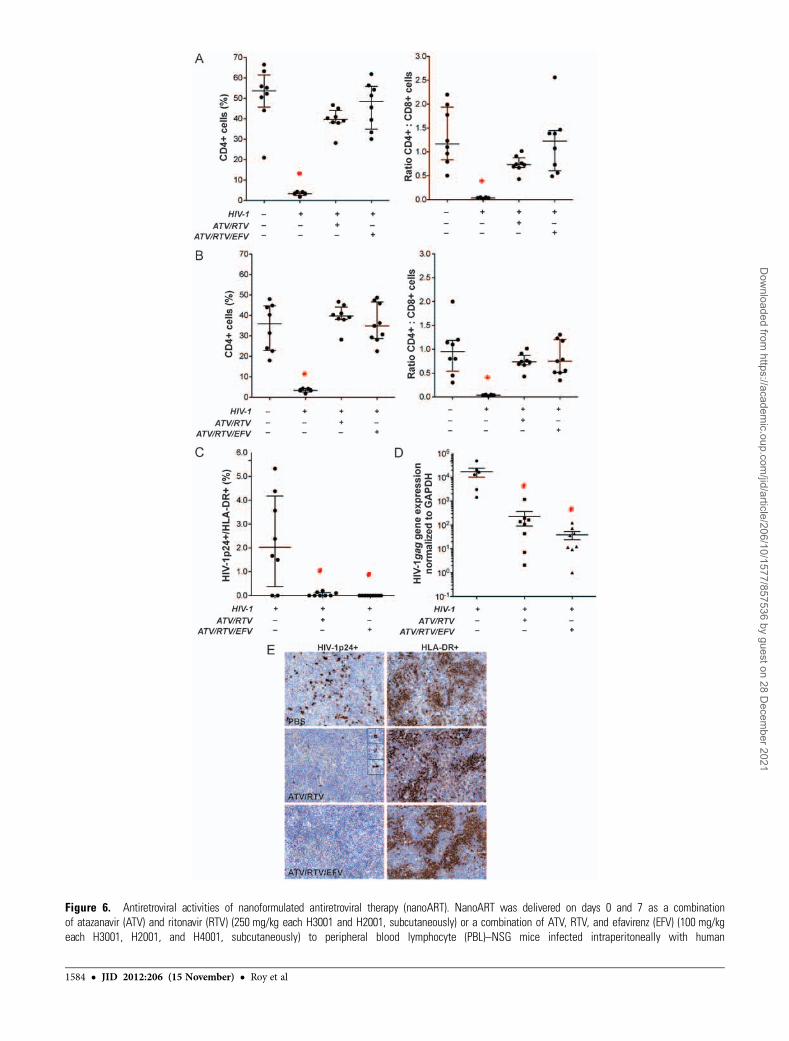
Figure 6. Antiretroviral activities of nanoformulated antiretroviral therapy (nanoART). NanoART was delivered on days 0 and 7 as a combinationof atazanavir (ATV) and ritonavir (RTV) (250 mg/kg each H3001 and H2001, subcutaneously) or a combination of ATV, RTV, and efavirenz (EFV) (100 mg/kgeach H3001, H2001, and H4001, subcutaneously) to peripheral blood lymphocyte (PBL)–NSG mice infected intraperitoneally with human
1584 • JID 2012:206 (15 November) • Roy et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021

shaped whereas RTV nanoARTs were plumper particles. EFVparticles were short and rectangular-shaped. Particle sizesranged from 281 nm (M3001) to 470 nm (H4001) (Supple-mentary Table 1), with PDI being lower for homogenizedthan for wet-milled particles (0.200 [H2001] to 0.288[M3001]). All particles were negatively charged (−31.6 mV[H3001] to −13.5 mV [M2001]). MDM uptake of the nano-particles and intracellular retention and release were similarfor wet-milled or homogenized formulations (Figure 2B). An-tiretroviral efficacies of the nanoformulations in MDM infect-ed with HIV-1ADA were drug-dependent [11].
Based on in vitro screening, the nanoART formulationsM2001, H2001, M3001, H3001, and H4001 were selected foranimal studies [6, 10, 18]. The “M” prefix designation in the for-mulation nomenclature refers to those produced by wet-milling,while the “H” refers to those prepared by homogenization(Figure 2B). Milled formulations performed within the topquartiles in uptake, retention, release, and antiretroviral effica-cy tests in MDMs [10]; however, the formulations showedmore limitations in size and PDI and greater toxicities as de-termined by decreased alamarBlue reduction and increasedMDM TNF-α production (Figure 2B) [6, 11]. Formulationswere administered to BALB/cJ mice in a pilot “survey.” Apartial PK evaluation demonstrated that formulations contain-ing the P188 surfactant produced sustained serum and tissuedrug concentrations (Figure 2B; Supplementary Figure 1)through 7 days after injection. Taken together, these data serveas selection criteria for the P188-containing nanoformulations(M2001, H2001, M3001, H3001, and H4001) for use in thecurrent animal investigations.
Nanotoxicology ProfilingSerum chemistry metabolic profiling and tissue histopatholog-ical analyses were conducted in control NSG mice injectedsubcutaneously with M3001 and M2001 (combination ATVand RTV) at ≤250 mg/kg for each drug. Treatment was ad-ministered in 2 doses, on days 0 and 7. Normal serum chemis-try profiles (Supplementary Table 2) were seen. Of interest,histopathology of both untreated and nanoART-treated miceshowed minor extramedullary hematopoiesis [26] and unevenliver glycogenation. Supplemental studies, performed in
normal BALB/cJ mice, showed a 2-fold increase and decreasein platelet counts and blood lymphocyte counts, respectively,at 14 days following treatment with 100 mg/kg nanoART(data not shown). The decline in lymphocyte counts was alsoobserved following treatment with native drugs.
We next assessed whether PBL reconstitution and/or HIV-1infection might exacerbate any nanoART toxicity. Thus, HIV-1–infected PBL-NSG mice were administered PBS (no drug);nanoART (ATV and RTV, 250 mg/kg, or ATV, RTV, andEFV, 100 mg/kg, subcutaneously) (Figure 1C). In PBS-treated,HIV-1–infected PBL-NSG mice, serum transaminase levelswere approximately 2-fold (149.4 U/L) higher than normal(Supplementary Table 2). Histopathological assessment ofliver sections confirmed substantive numbers of lymphocytesin the pericentral regions of PBS- and nanoART-treated mice(Figure 3B). A few necrotic hepatocytes were also observed,consistent with GVHD [27, 28].
Pharmacodynamic AnalysesTo determine the nanoART dose(s) required to achieve thera-peutic serum drug concentrations, pharmacodynamic analyseswere performed in normal NSG mice following subcutaneousadministration of 80, 150, or 250 mg/kg ATV and RTV.Median drug concentrations declined 2 orders of magnitude(log10) from day 1 to day 6 (Figure 2C) and at day 6 were 94.8ng/mL and 132 ng/mL, respectively, in the 250mg/kg-dosegroup. This drop was due to drug metabolism. Notably, ATVconcentrations at day 14 were higher than day 6 levels. In thehigh-dose group, ATV concentrations at day 14 were 417 ng/mL above the median plasma concentrations seen in ATV-treated patients [29]. In contrast, there were no differences inserum concentrations of RTV at day 14 compared with day 6.
Corresponding tissue drug levels in nanoART-treatedanimals were determined at day 14. Livers of animals treatedwith 250 mg/kg nanoART contained 1656 ng/g ATV and 758ng/g RTV (Figure 2D). ATV levels were 120–183 ng/g tissue inspleen, kidney, and lung. RTV levels were 276 and 264 ng/gtissue in spleen and kidney, respectively, and 141 ng/g in lung.Drug levels in brain were at the limit of detection. Of interest,ATV and RTV levels in liver, spleen, kidney, and lung differedby dose. On the basis of these results, a dose of 250 mg/kg ATV
Figure 6 Continued. immunodeficiency virus type 1 (HIV-1)ADA 12 h before initial nanoART dose. Peripheral blood and spleens were collected on day14 after initial nanoART injection. Fluorescence-activated cell sorting analyses show the percentage of human CD4+ among total CD3+ T cells (leftpanels) and CD4+/CD8+ T-cell ratios (right panels) for peripheral blood (A) and spleen (B) from individual mice. C, Percentages of HIV-1p24–expressingcells among human HLA-DR+ cells were determined from cell counts of immunostained serial sections through spleens of PBL-reconstituted, HIV-1ADA–infected PBL-NSG mice. D, HIV-1gag RNA expression in spleen normalized to glyceraldehyde-3-phosphate dehydrogenase (GAPDH) messenger RNAexpression. E, Expression of human HLA-DR and HIV-1p24 in alternate serial sections of splenic tissues from HIV-1–infected NSG mice treated withPBS vehicle (top panels), ATV and RTV (middle panels), or ATV, RTV, and EFV (bottom panels). Spleens were collected on day 14 after initial nanoARTinjection, sectioned, immunostained with antibodies specific for HLA-DR or HIV-1p24, followed by secondary antibodies conjugated with horseradishperoxidase, and were visualized by 3,3-diaminobenzidine . A–D, Data are shown as individual data points and median ± 25th and 75th percentiles (bar± whisker) for 3–8 mice per group, analyzed by analysis of variance of rank-transformed values and significant differences determined by Tukey posthoc analysis, whereby P≤ .05 compared to (*) nontreated, nonreconstituted, noninfected NSG mice and (#) nontreated, HIV-1–infected PBL-NSG mice.
NanoART-Treated HIV-1–Infected Mice • JID 2012:206 (15 November) • 1585
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021

and RTV (H3001 and H2001) was chosen for assessment ofantiviral efficacy. Here, NSG mice were reconstituted withhuman PBLs 7 days prior to a single does of nanoART, and 24hours later were infected with HIV-1ADA. In the second experi-mental paradigm, nanoART was administered subcutaneously,12 hours after HIV-1ADA infection (day 0) and again on day7. Biodistribution studies were used to confirm that nanoARTtreatment achieves therapeutic serum concentrations of ATV inPBL-reconstituted, HIV-1–infected mice (Figure 4A). SerumATV concentrations decreased from day 1 to day 6, but in-creased to 256 ng/mL and 88 ng/mL on day 14 in animalstreated with ATV and RTV or ATV, RTV, and EFV, respective-ly. Of note, median ATV concentrations on day 14 in the ATVand RTV group were above the minimum effective ATV serumconcentration for humans of 150 ng/mL [30]. Serum EFV con-centration was 4–6-fold lower than that of RTV or ATV(Figure 4A) and was significantly lower than the minimalplasma therapeutic concentration of 1000 ng/mL [31].
Next, we determined tissue drug levels in HIV-1–infectedPBL-NSG mice on day 14 after nanoART treatment on days0 and 7 (Figure 4B). In contrast to nanoART treatment innormal NSG mice (Figure 2D), median spleen ATV levelswere 3-fold higher than in liver (Figure 4B). Spleen ATVlevels were commonly variable and in several mice were 16000–17 000 ng/g [27, 28]. Median liver ATV levels were 761ng/g and 287 ng/g in animals treated with ATV and RTV andATV, RTV, and EFV, respectively. In mice treated with ATVand RTV or ATV, RTV, and EFV, RTV levels were 3–4-foldhigher in liver (900 ng/g and 268 ng/g, respectively) than inspleen (211 ng/g and 90 ng/g, respectively). Levels of drug(ATV and RTV with EFV) in the skin at the site of injection(s) were 1.1–1.6 mg drug per gram tissue serving as a poten-tial depot for drug.
Antiviral Activities of nanoART Administered Before HIV-1InfectionAntiviral activities of nanoART together with PK and biodistri-bution studies were performed. PBL-reconstituted NSG micewere treated with nanoART or native drugs 1 day prior toHIV-1 infection, and viral activity was determined 9 days afterdrug administration. HIV-1 infection results in loss of humanCD4+ T cells in PBL-reconstituted immunodeficient mice [21,32–35]. Thus, as an indicator of viral infection, levels of humanCD4+ and CD8+ T cells as percentages of total human CD3+ Tcells and CD4+/CD8+ T-cell ratios were determined from FACSanalyses of spleen cells taken at study termination (9 days afterdrug treatment). Levels of human CD45+ T cells were similar inall treatment groups (1.7% ± 0.4%, 2.2% ± 0.4%, and 1.4% ±0.3% of total cells for PBS-, native drug-, and nanoART-treatedmice, respectively). Low spleen CD4+ T cells and CD4+/CD8+
T-cell ratios were observed in PBS-treated HIV-1–infectedanimals (Figure 5A). To determine the level of HIV-1 infection,
HIV-1p24 expression among HLA-DR+ cells in spleen was de-termined. NanoART treatment significantly reduced HIV-1p24+ cells in the spleen and reduced spleen HIV-1gag geneexpression (Figure 5B). In contrast, treatment with native drugdid not decrease the number or expression levels of HIV-1p24+
cells in the spleen. At day 9, drug levels in serum and peripheraltissues were higher in nanoART-treated mice than in thosegiven native drug (Figure 5C).
Suppression of Acute HIV-1 Infection by nanoARTTo determine whether nanoART could suppress preexistingHIV infection, HIV-1–infected PBL-NSG mice were treatedwith nanoART 12 hours and 7 days after infection, then sacri-ficed on day 14. Levels of human CD45+ T cells (as percentageof total cells in peripheral blood and spleen [blood, 59.2% ±6.5% to 73.9% ± 2.9%; spleen, 22.3% ± 7.2% to 29.8% ± 4.9%])did not differ significantly among treatment groups. In HIV-1–infected animals not treated with nanoART, percentages ofCD4+ T cells and CD4+/CD8+ T-cell ratios were significantlydecreased in both peripheral blood (Figure 6A) and spleen(Figure 6B) compared with uninfected animals. Importantly,in nanoART-treated (ATV/RTV or ATV/RTV/EFV) HIV-1–infected animals, there was no difference in levels of CD4+ Tcells and CD4+/CD8+ T-cell ratios from those observed in un-infected mice. The level of HIV infection was determined byimmunohistochemical quantitation of HIV-1p24–expressingcells among HLA-DR+ cells in spleen. Both ATV/RTV andATV/RTV/EFV treatments significantly reduced the numberof HIV-1p24+ stained cells in the spleen, although a few weredetected in some sections from the ATV and RTV treatmentgroup (Figure 6C and 6E). Suppression of HIV-1 replicationwas also determined in spleen by PCR measurements forHIV-1gag gene expression. Treatment with ATV/RTV andATV/RTV/EFV reduced viral gene expression by 2 and 3orders of magnitude (log10), respectively (Figure 6D), althoughthe difference between the 2 treatments was not statisticallysignificant. Taken together, these results demonstrate thatweekly dosing with nanoART can reduce HIV-1 viral infec-tion to nearly undetectable levels.
DISCUSSION
We manufactured injectable long-acting antiretroviral combi-nations and tested them in a disease-relevant animal system.Our data demonstrate that nanoformulations of commonlyused protease inhibitors that show efficacy in cell-based labo-ratory tests [7, 10] can be used successfully in rodent modelsof HIV-1 disease to halt loss of CD4+ T cells and attenuateviral replication. The results are in line with drug concentra-tions detected in sera and tissue. Toxicology profiles revealthat the drugs are well-tolerated.
1586 • JID 2012:206 (15 November) • Roy et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021

The need for alternative antiretroviral formulations is clearbased on complexities of many existing regimens, difficultieswith adherence, lack of targeting viral reservoirs, emergence ofdrug resistance, and toxicities [2, 13]. Moreover, in patientswho abuse drugs and show poor adherence to ART regimens,acclerated virologic resistance and transmission can be seen[36]. Adding to such concerns is the availability of ART inresource-limited settings [37–39]. Thus, the need for alterna-tive therapies is timely [30, 40].
Cell-mediated drug delivery is a novel concept that employsintracellular recycling and late endosomes as reservoirs fordrug [8]. Monocyte-macrophages offer a particularly attractivecell delivery system. Although the role played by macrophagesin the current study is not certain, the established reservoirsand drug stability suggest that these cells serve as nanoparticledepots. Moreover, the observation that drugs delivered by nano-formulations can be stored in recycling endosomal compart-ments in macrophages may explain the observed long-actingnature of the drugs [9]. Although the promise of cell-mediateddelivery of drugs is real, its perils demand equal consideration.This includes immune reactions elicited against the particle,untoward reactions against the excipients, and effects on thecell and tissues, as well as effects on its function consequent toharboring the crystal for periods of weeks [41, 42].
Also limitations are acknowledged in the experimental ap-proach. For example, NSG mice as recipients of human PBLscommonly develop GVHD [27]. Thus, it is difficult to draw afirm conclusion on any nanoART hepatic toxicities in theseanimals. Nonetheless, such systems, as developed in thisreport, represent a new strategy for treating HIV-1 disease.The further design of nanoparticle carriers for such drug de-livery may include decorating the particle with specific cellligands that target virus-infected cell surface antigens. More-over, the particle compositions used in these studies makenanoART translation to humans viable. Taken together, tar-geted drug delivery and ease of access to ART as nanoformu-lated medicines are real and convincing and demand furtherinvestigation for human use.
Supplementary Data
Supplementary materials are available at The Journal of Infectious Diseasesonline (http://www.oxfordjournals.org/our_journals/jid/). Supplementarymaterials consist of data provided by the author that are published tobenefit the reader. The posted materials are not copyedited. The contentsof all supplementary data are the sole responsibility of the authors. Ques-tions or messages regarding errors should be addressed to the author.
Notes
Acknowledgments. We thank Tanuja Gutti, Jaclyn Knibbe, and RamVeerhubhotla for their expert technical assistance; Michel Kanmogne forstatistical support; and Drs Han Chen and You Zhou of the University ofNebraska–Lincoln electron microscopy core for assistance with the scan-ning electron microscopy.
Financial support. This work was supported by the National Insti-tutes of Health (grant numbers 1P01 DA028555, 2R01 NS034239, 2R37NS36126, P01 NS31492, P20RR 15635, P01MH64570, and P01 NS43985[to H. E. G.]) and by a research grant from Baxter Healthcare.Potential conflicts of interest. All authors: No reported conflicts.All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to thecontent of the manuscript have been disclosed.
References
1. Broder MS, Chang EY, Bentley TG, Juday T, Uy J. Cost effectivenessof atazanavir-ritonavir versus lopinavir-ritonavir in treatment-naivehuman immunodeficiency virus-infected patients in the United States.J Med Econ 2011; 14:167–78.
2. Swindells S, Flexner C, Fletcher CV, Jacobson JM. The critical needfor alternative antiretroviral formulations, and obstacles to their devel-opment. J Infect Dis 2011; 204:669–74.
3. Chesney MA, Ickovics J, Hecht FM, Sikipa G, Rabkin J. Adherence: anecessity for successful HIV combination therapy. AIDS 1999; 13(suppl A):S271–8.
4. Braithwaite RS, Shechter S, Roberts MS, et al. Explaining variability inthe relationship between antiretroviral adherence and HIV mutationaccumulation. J Antimicrob Chemother 2006; 58:1036–43.
5. Batrakova EV, Li S, Brynskikh AM, et al. Effects of pluronic and dox-orubicin on drug uptake, cellular metabolism, apoptosis and tumorinhibition in animal models of MDR cancers. J Control Release 2010;143:290–301.
6. Bressani RF, Nowacek AS, Singh S, et al. Pharmacotoxicology ofmonocyte-macrophage nanoformulated antiretroviral drug uptake andcarriage. Nanotoxicology 2011; 5:592–605.
7. Nowacek AS, McMillan J, Miller R, Anderson A, Rabinow B, Gendel-man HE. Nanoformulated antiretroviral drug combinations extenddrug release and antiretroviral responses in HIV-1-infected macro-phages: implications for neuroAIDS therapeutics. J NeuroimmunePharmacol 2010; 5:592–601.
8. Batrakova EV, Gendelman HE, Kabanov AV. Cell-mediated drug de-livery. Expert Opin Drug Deliv 2011; 8:415–33.
9. Kadiu I, Nowacek A, McMillan J, Gendelman HE. Macrophage endo-cytic trafficking of antiretroviral nanoparticles. Nanomedicine (Lond)2011; 6:975–94.
10. Nowacek AS, Balkundi S, McMillan J, et al. Analyses of nanoformu-lated antiretroviral drug charge, size, shape and content for uptake,drug release and antiviral activities in human monocyte-derived mac-rophages. J Control Release 2011; 150:204–11.
11. Balkundi S, Nowacek AS, Veerhubotla RS, et al. Comparative manu-facture and cell-based delivery of antiretroviral nanoformulations. IntJ Nanomedicine 2011; 6:3393–3404.
12. Nowacek AS, Miller RL, McMillan J, et al. NanoART synthesis, char-acterization, uptake, release and toxicology for human monocyte-macrophage drug delivery. Nanomedicine (Lond) 2009; 4:903–17.
13. Nowacek A, Gendelman HE. NanoART, neuroAIDS and CNS drugdelivery. Nanomedicine (Lond) 2009; 4:557–74.
14. Dou H, Grotepas CB, McMillan JM, et al. Macrophage delivery ofnanoformulated antiretroviral drug to the brain in a murine model ofneuroAIDS. J Immunol 2009; 183:661–9.
15. Dou H, Destache CJ, Morehead JR, et al. Development of a macro-phage-based nanoparticle platform for antiretroviral drug delivery.Blood 2006; 108:2827–35.
16. Robinson BS, Riccardi KA, Gong YF, et al. BMS-232632, a highlypotent human immunodeficiency virus protease inhibitor that can beused in combination with other available antiretroviral agents. Antimi-crob Agents Chemother 2000; 44:2093–9.
17. Berges BK, Rowan MR. The utility of the new generation of human-ized mice to study HIV-1 infection: transmission, prevention, patho-genesis, and treatment. Retrovirology 2011; 8:65.
NanoART-Treated HIV-1–Infected Mice • JID 2012:206 (15 November) • 1587
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021

18. Balkundi S, Nowacek AS, Roy U, Martinez-Skinner A, McMillan J,Gendelman HE. Methods development for blood borne macrophagecarriage of nanoformulated antiretroviral drugs. J Vis Exp 2010; (46)pii:2460.
19. Huang J, Gautam N, Bathena SP, et al. UPLC-MS/MS quantificationof nanoformulated ritonavir, indinavir, atazanavir, and efavirenz inmouse serum and tissues. J Chromatogr B Analyt Technol BiomedLife Sci 2011; 879:2332–8.
20. Gendelman HE, Orenstein JM, Martin MA, et al. Efficient isolationand propagation of human immunodeficiency virus on recombinantcolony-stimulating factor 1-treated monocytes. J Exp Med 1988;167:1428–41.
21. Poluektova LY, Munn DH, Persidsky Y, Gendelman HE. Generation ofcytotoxic T cells against virus-infected human brain macrophages in amurine model of HIV-1 encephalitis. J Immunol 2002; 168:3941–9.
22. Gendelman HE, Genis P, Jett M, Zhai QH, Nottet HS. An experimen-tal model system for HIV-1-induced brain injury. Adv Neuroimmunol1994; 4:189–93.
23. Stoddart CA, Bales CA, Bare JC, et al. Validation of the SCID-hu Thy/Liv mouse model with four classes of licensed antiretrovirals. PLoSOne 2007; 2:e655.
24. Poluektova L, Gorantla S, Faraci J, Birusingh K, Dou H, GendelmanHE. Neuroregulatory events follow adaptive immune-mediated elimi-nation of HIV-1-infected macrophages: studies in a murine model ofviral encephalitis. J Immunol 2004; 172:7610–7.
25. Gorantla S, Makarov E, Finke-Dwyer J, et al. CD8+ cell depletion ac-celerates HIV-1 immunopathology in humanized mice. J Immunol2010; 184:7082–91.
26. Ohbo K, Suda T, Hashiyama M, et al. Modulation of hematopoiesis inmice with a truncated mutant of the interleukin-2 receptor gammachain. Blood 1996; 87:956–67.
27. Pino S, Brehm MA, Covassin-Barberis L, et al. Development of novelmajor histocompatibility complex class I and class II-deficient NOD-SCID IL2R gamma chain knockout mice for modeling human xenoge-neic graft-versus-host disease. Methods Mol Biol 2010; 602:105–17.
28. King MA, Covassin L, Brehm MA, et al. Human peripheral blood leu-cocyte non-obese diabetic-severe combined immunodeficiency inter-leukin-2 receptor gamma chain gene mouse model of xenogeneicgraft-versus-host-like disease and the role of host major histocompati-bility complex. Clin Exp Immunol 2009; 157:104–18.
29. Best BM, Letendre SL, Brigid E, et al. Low atazanavir concentrationsin cerebrospinal fluid. AIDS 2009; 23:83–7.
30. AIDSinfo, Panel on Antiretroviral Guidelines for Adults and Adoles-cents. Guidelines for the use of antiretroviral agents in HIV-1-infectedadults and adolescents. Department of Health and Human Services.
Available at http://www.aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf. Accessed 2 November 2011.
31. Lopez-Cortes LF, Ruiz-Valderas R, Marin-Niebla A, Pascual-CarrascoR, Rodriguez-Diez M, Lucero-Munoz MJ. Therapeutic drug monitor-ing of efavirenz: trough levels cannot be estimated on the basis ofearlier plasma determinations. J Acquir Immune Defic Syndr 2005;39:551–6.
32. Mosier DE. Distinct rate and patterns of human CD4+ T-celldepletion in hu-PBL-SCID mice infected with different isolatesof the human immunodeficiency virus. J Clin Immunol 1995; 15:130S–3S.
33. Mosier DE, Gulizia RJ, MacIsaac PD, Torbett BE, Levy JA. Rapid lossof CD4+ T cells in human-PBL-SCID mice by noncytopathic HIVisolates. Science 1993; 260:689–92.
34. Gorantla S, Santos K, Meyer V, et al. Human dendritic cells transducedwith herpes simplex virus amplicons encoding human immunodeficien-cy virus type 1 (HIV-1) gp120 elicit adaptive immune responses fromhuman cells engrafted into NOD/SCID mice and confer partial protec-tion against HIV-1 challenge. J Virol 2005; 79:2124–32.
35. Gorantla S, Sneller H, Walters L, et al. Human immunodeficiencyvirus type 1 pathobiology studied in humanized BALB/c-Rag2-/-gammac-/- mice. J Virol 2007; 81:2700–12.
36. Wood E, Hogg RS, Yip B, et al. Rates of antiretroviral resistanceamong HIV-infected patients with and without a history of injectiondrug use. AIDS 2005; 19:1189–95.
37. Gilks CF, Crowley S, Ekpini R, et al. The WHO public-health ap-proach to antiretroviral treatment against HIV in resource-limited set-tings. Lancet 2006; 368:505–10.
38. Brinkhof MW, Pujades-Rodriguez M, Egger M. Mortality of patientslost to follow-up in antiretroviral treatment programmes in resource-limited settings: systemic review and meta-analysis. PLoS One 2009; 4:e5790.
39. World Health Organization. Antiretroviral therapy for HIV infectionin adults and adolescents: recommendations for a public health ap-proach, 2006 revision. http://www.who.int/hiv/pub/guidelines/artadultguidelines.pdf. Accessed 17 November 2011.
40. Huff-Rousselle M, Simooya O, Kabwe V, et al. Pharmacovigilanceand new essential drugs in Africa: Zambia draws lessons from itsown experiences and beyond. Glob Public Health 2007; 2:184–203.
41. Kabanov AV, Gendelman HE. Nanomedicine in the diagnosisand therapy of neurodegenerative disorders. Prog Polym Sci 2007; 32:1054–82.
42. Gendelman HE, Kabanov A, Linder J. The promise and perils ofCNS drug delivery: a video debate. J Neuroimmune Pharmacol 2008;3:58.
1588 • JID 2012:206 (15 November) • Roy et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/206/10/1577/857536 by guest on 28 D
ecember 2021