pharmacology
TRANSCRIPT

Must- Knows About Pharmacology Basics By: Dave Manriquez RN.

Basic concepts and Drug Categories
Pharmacy:
Pharmacotherapeutics:
Pharmacology:
Vital facts:
DEFINITION OF TERMS
Study of drug effects on living organisms
Use of drugs to tx,dx or prevent disease
Art of preparing and dispensing drugs

Vital facts:
DEFINITION OF TERMS
Person licensed to prepare and dispense drugs
Pharmacist:
Book containing list of products used in medicine
Pharmacopoeia:
Study of dosage/amount of drugs given in the treatment of diseases
Posology:
Chemical name:
Official name:
Generic name:
Vital facts:
Name given before it becomes official
Name listed in official publications
Precise constituents of the drug
Trademark/brand name:
Name given by drug manufacturer
DEFINITION OF TERMS

Brand/ Trade name
Generic name
Chemical name
DEFINITION OF TERMS
OTC drugs:
Orphan drugs:
Vital facts:
DEFINITION OF TERMS
Discovered drugs but aren’t financially viable. Hence, left by drug companies.
Drugs for self- medication
PHARMACOLOGY BASICS
A patient tells you “Nurse, can I take acetaminophen for my abdominal pain. It’s been aching since last night.” What is your best response and why?
Nursing teachings for OTCs: SAMPLE CASE

PHARMACOLOGY BASICS
A patient asks you “Nurse, if I don’t get any relief from my first dose of Aspirin, is it safe to take a second dose?” What is your best response?
Nursing teachings for OTCs: SAMPLE CASE

PHARMACOLOGY BASICS
A hypertensive patient is wondering why the other nurse asked him about what OTC drugs he was taking. He said “I never thought OTCs could cause hypertension.” Is there any truth to the patient’s statement?
Nursing teachings for OTCs: SAMPLE CASE

PHARMACOLOGY BASICS
A patient taking antibiotics gets upset and tells the nurse “Are you sure I should stop taking my Maalox just because I’m taking antibiotics?” Is there something wrong with the nurse’s instructions?
Nursing teachings for OTCs: SAMPLE CASE

od,bid,tid,qid
ad lib
ac, pc
Vital facts:
COMMON ABBREVIATIONS
OD, OS, OU
Rx take
elix
Tr
ss , ss
Vital facts:
COMMON ABBREVIATIONS
dil
One half
tincture
Dilute or dissolve
Category A
According to the Food and Drug Administration:
DRUG CATEGORIES (in r/t PREGNANCY)
Safe for human fetus

Category B
According to the Food and Drug Administration:
DRUG CATEGORIES (in r/t PREGNANCY)
Risk to animal fetus
Safe to animal fetus
Safe for human fetus
Inadequate studies on H.F.

According to the Food and Drug Administration:
DRUG CATEGORIES (in r/t PREGNANCY)
Category C
Adverse effects on animal fetus
Inadequate studies on H.F.

According to the Food and Drug Administration:
DRUG CATEGORIES (in r/t PREGNANCY)
Category D
Risk to human fetus
Given if benefits outweigh the risk

Category X
According to the Food and Drug Administration:
DRUG CATEGORIES (in r/t PREGNANCY)
Adverse effects on animal & human fetuses
Risks clearly outweigh the benefits
Universal Pharmacologic Nursing rule during pregnancy:
Never give any drug unless it is clearly needed

Tetracycline? Streptomycin?
Penicillin? Ampicillin? Cephalosporins? Erythromycin?
Can RIP be given to a TB gravida client?
Safe/ Unsafe drugs:
DRUG CATEGORIES (in r/t PREGNANCY)

Safe/ Unsafe drugs:
Antihistamines, Decongestants, Acetaminophen?
Quinine antimalarials? Non-quinine only
General anesthetics? Metronidazole?
DRUG CATEGORIES (in r/t PREGNANCY)

Isotretinoin:
Streptomycin:
Anticonvulsants (Phenytoin)
Unsafe drugs:
CHD, Cleft lip/ palate (steroids)
Nerve deafness
CNS defects
DRUG CATEGORIES (in r/t PREGNANCY)
Unsafe drugs:
Iodides:
Goiter and mental retardation
Lithium:
Congenital heart defects
Barbiturate, Aspirin:
Bleeding problems
DRUG CATEGORIES (in r/t PREGNANCY)

Pharmacodynamics

Peak plasma level:
Onset of action:
Definition of terms:
DRUG ACTIONS
Time when body initially responds to drug
Highest plasma level, Elimination rate=Absorption rate
Drug half-life: One half the previous dose
Plateau: Maintained concentration of drug in plasma thru series of scheduled doses
2 mechanisms:
Def’n:
Vital facts:
Process by which drug alters cell physiology
Being an agonist or an antagonist
PHARMACODYNAMICS

Receptor sites:
PHARMACODYNAMICS
Areas on the cell membranes where drugs act
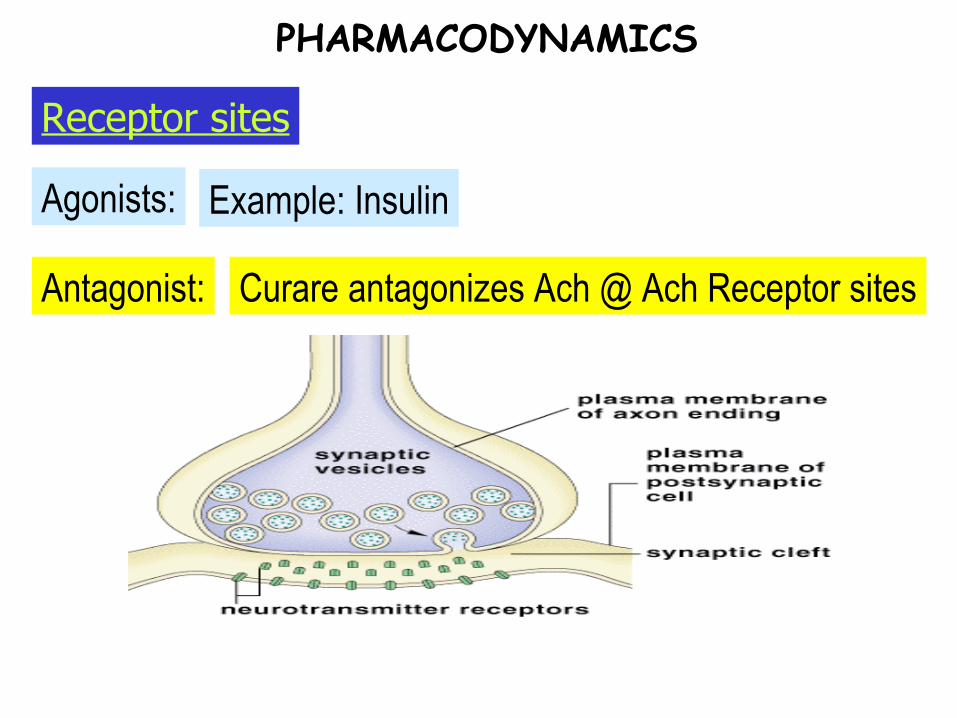
Antagonist:
Agonists:
Receptor sites
PHARMACODYNAMICS
Example: Insulin
Curare antagonizes Ach @ Ach Receptor sites
Other concepts:
PHARMACODYNAMICS
Selective toxicity: Drug attacks only those foreign cell systems
Example:
Penicillin vs.
Bacterial infections
Chemothera-peutic drugs vs.
Rapidly multiplying cells
Pharmacokinetics
Purpose of a loading dose:
Critical concentration:
Study of:
Basic concepts:
PHARMACOKINETICS
Absorption, distribution, metabolism, excretion of drugs
A.K.A. Therapeutic serum level
To reach critical concentration early
Examples: Digoxin, Aminophylline
PHARMACOKINETICS: ABSORPTION

Def’n.:
Vital facts:
Process by which drug passes into the bloodstream
PHARMACOKINETICS: ABSORPTION
Stress:
Pain:
Blood flow: The richer the BS, the faster
Slows down gastric emptying rate– slow absorption
May cause vasoconstriction– slow absorption
Food: May interfere with drug absorption
Factors that affect Drug Absorption:
PHARMACOKINETICS: ABSORPTION

Solubility:
pH:
Exercise: More blood flow to muscles, less to GIT– Slow absorption
Acidic drugs are best absorbed in acidic environment
Liquids absorbed faster than solids
Factors that affect Drug Absorption:
PHARMACOKINETICS: ABSORPTION
Ideal time for giving oral drugs:
Safest way to deliver drugs:
Oral route
1 hour ac/ 2 hours pc
Vital facts:
PHARMACOKINETICS: ABSORPTION

IM & gender differences:
Males more muscles reaches peak levels faster
IM & heat to injection site:
Increased absorption
Vital facts:
PHARMACOKINETICS: ABSORPTION

PHARMACOKINETICS: DISTRIBUTION
Eg:
1st organs to receive drug:
Definition:
Vital facts:
Movement of a drug from its site of absorption to its site of action
Highly vascular organs
Liver,kidneys, brain
PHARMACOKINETICS: DISTRIBUTION
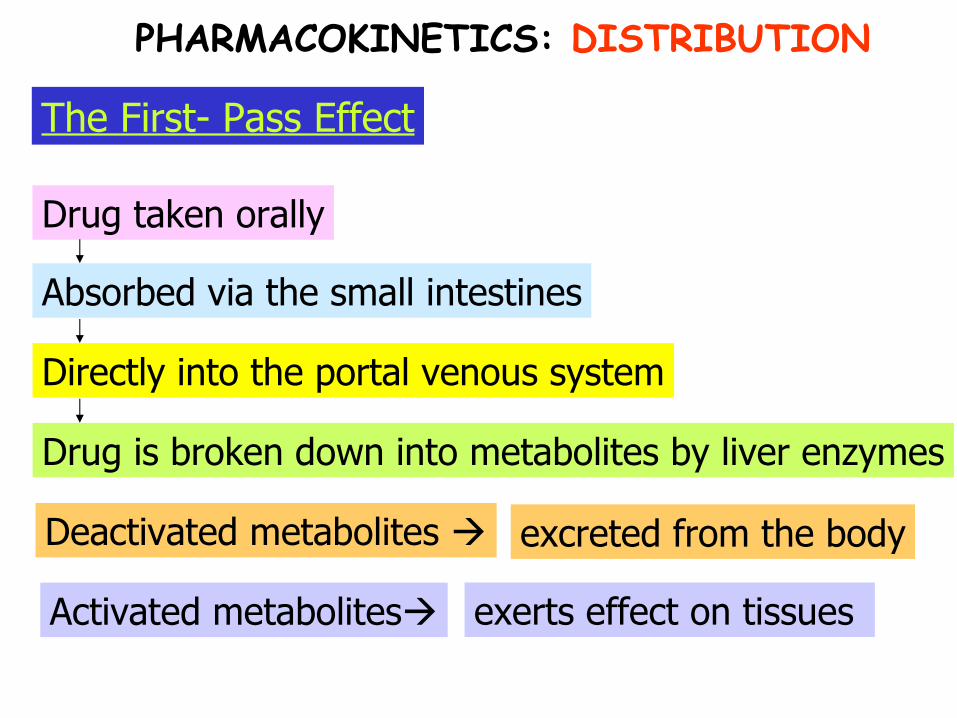
Drug is broken down into metabolites by liver enzymes
Deactivated metabolites
Activated metabolites
Directly into the portal venous system
Absorbed via the small intestines
Drug taken orally
The First- Pass Effect
excreted from the body
exerts effect on tissues
PHARMACOKINETICS: DISTRIBUTION
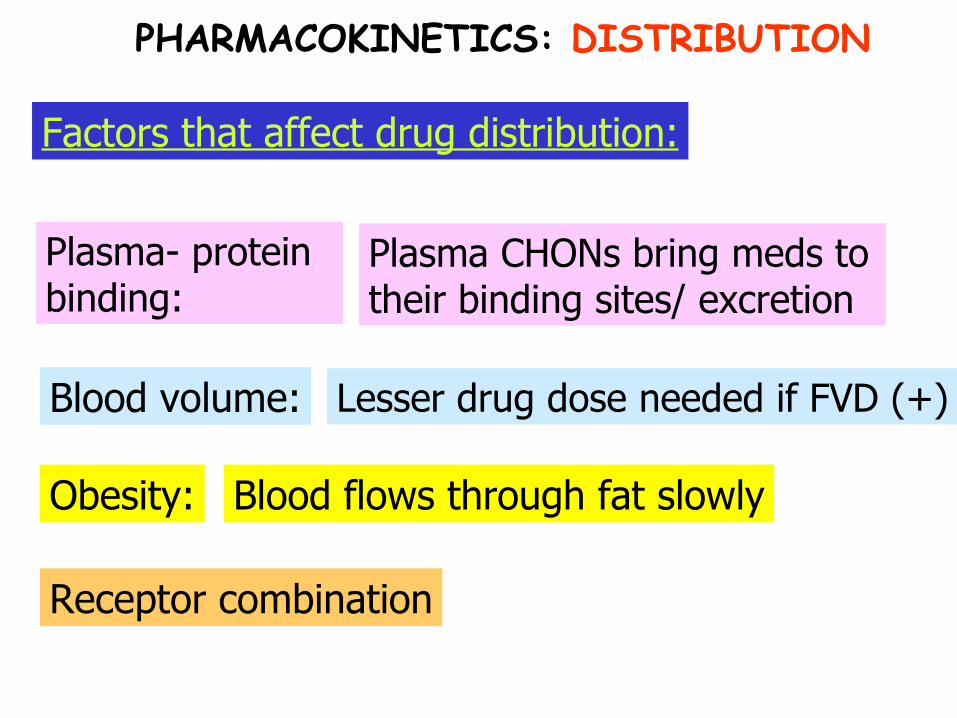
Obesity:
Blood volume:
Plasma- protein binding:
Plasma CHONs bring meds to their binding sites/ excretion
Lesser drug dose needed if FVD (+)
Blood flows through fat slowly
Receptor combination
Factors that affect drug distribution:
PHARMACOKINETICS: DISTRIBUTION
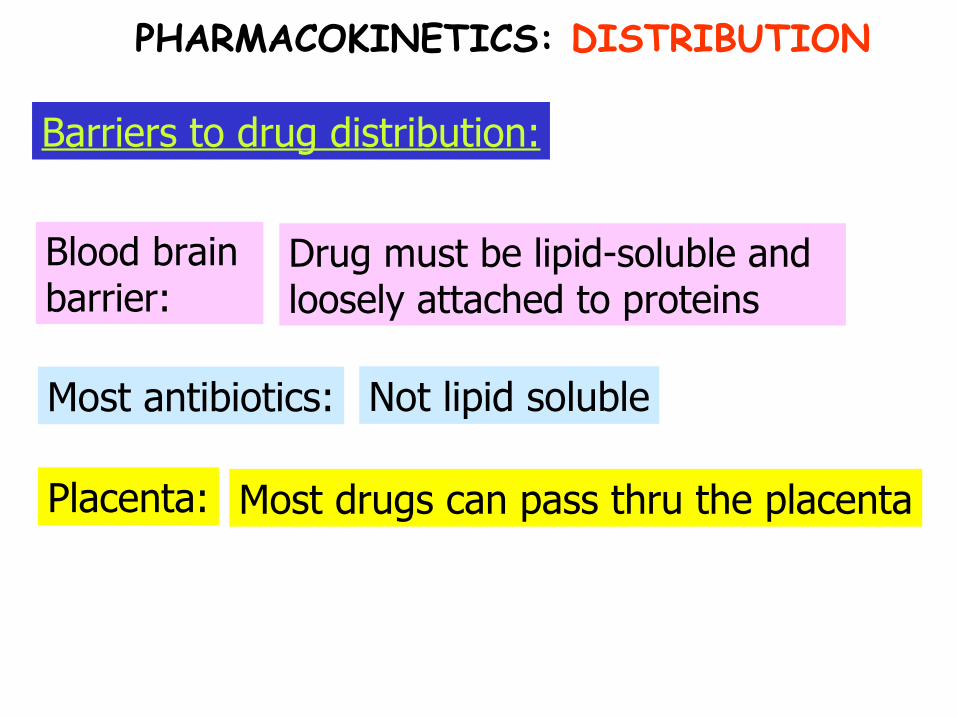
Placenta:
Most antibiotics:
Blood brain barrier:
Drug must be lipid-soluble and loosely attached to proteins
Not lipid soluble
Most drugs can pass thru the placenta
Barriers to drug distribution:
PHARMACOKINETICS: DISTRIBUTION
Trivia Time
What anti-inflammatory drug is ideal for meningitis?
PHARMACOKINETICS: DISTRIBUTION

Trivia Time: ANSWER
Dexamethasone
PHARMACOKINETICS: DISTRIBUTION
Critical thinking question:
Would you consider a person who has malnutrition at a higher risk for Aspirin toxicity? Why?
PHARMACOKINETICS: DISTRIBUTION

PHARMACOKINETICS: BIOTANSFORMATION
By-products:
Major site:
Definition:
Vital facts:Process by which a drug is converted to a less active form
Liver
Metabolites
Types of metabolites: Active and inactive
Impaired metabolism in… Older age, liver disease
PHARMACOKINETICS: METABOLISM

Drugs that increase metabolism:
Alcohol, nicotine, glucocorticoids
Drugs that may decrease metabolism:
Ketoconazole, Quinidine
PHARMACOKINETICS: METABOLISM
AKA: Detoxification
Vital facts:

PHARMACOKINETICS: EXCRETION

Other routes:
Common route of excretion:
Definition:
Vital facts:
Process by which metabolites and drugs are eliminated from the body
Urine
Feces, saliva,sweat,breast milk
Effect of old age: Decreased renal function
PHARMACOKINETICS: EXCRETION
Half- life:
Useful concepts:
Half-life x 8= removal from body
PHARMACOKINETICS: EXCRETION
Peak level:
Trough level:
15-30 minutes after giving the dose
15-30 minutes before giving the next dose
Question on half-life:
a.) Drug “x” has a half-life of 1 hour. How many hours will it take for drug “x” to be excreted away from the body?
b.) If it takes 16 hours for drug “y” to be excreted away from the body, what is its half-life?
PHARMACOKINETICS: EXCRETION

Drug effects and Misuse
Age:
Weight:
Factors influencing drug effects:
DRUG EFFECTS
The heavier, the more tissues to perfuse
Elderly doses are usually 1/3 – ½ usual dose
Psychological fx: Placebo effect (if you think it will, it will)
Tolerance: Example: Morphine
Nursing implications:
Combine with other drugs to potentiate effects (eg: NSAIDS plus Morphine)

Environment:
Drug polymorphism:
Variation in response to a drug due to factors such as age, gender,size and body composition
Warm/cold, Noisy/Silent
Illness: Liver, kidney disease
Time of administration: Empty vs. Full stomach
Factors influencing drug effects:
DRUG EFFECTS

Adverse effect:
Side effect:
Therapeutic effect: Desired effect
Unintended effect
More severe side effect – may justify drug discontinuation
Drug toxicity: Drug overdosage
Drug allergy: Immunologic reaction to a drug
Different types:
DRUG EFFECTS
Cross- allergies:
Drug allergy:
Succeeding allergic reactions are usually much worse than the 1st
Sulfa drugs
Allergic Reactions
DRUG EFFECTS

The Normal Distribution:
DRUG EFFECTS
Key action:
Epinephrine SQ q15-20 mins as prescribed
Usual time of occurrence:
Anaphylactic reaction:
Severe allergic reaction
W/in mins to 2 weeks
DRUG EFFECTS
Allergic Reactions

Dermatological rxns:
Mild: skin care. Severe: Stop & call doc
Blood dyscrasias:
Ensure periodic CBCs
DRUG EFFECTS
Allergic Reactions
Lacrimal tearing
Pruritus:
Angioedema: Due to increased capillary permeability
Itching with or without a rash
Respi:
GIT:
DRUG EFFECTS
Allergic Reactions: Manifestations
Wheezing and dyspnea
Diarrhea, nausea and vomiting

Drug tolerance Unusually low physiologic response to a drug
Cumulative effect:
Increasing response to repeated drug doses (Rate of administration exceeds Metabolism)
Different types:
DRUG EFFECTS

Drug interaction
Example:
Idiosyncratic effect:Unexpected and unique drug effect on an individual
Unusual underresponse to a drug
Potentiating/ Synergistic effect
Inhibiting effect
Different types:
DRUG EFFECTS

Higher blood dose of Penicillin for a longer time
Probenecid blocks excretion of Penicillin
Probenecid is added
Penicillin for bacterial infection
Potentiating effect: An example

Lesser dose of Codeine needed
More pain relief
Aspirin is added
Codeine for pain relief
Additive effect: An example

Example:
Iatrogenic disease:Disease unintentionally caused by medical therapy
Hepatotoxicity, Fetal malformations
Different types:
DRUG EFFECTS

Physiologic dependence
Drug dependence
Drug abuse
Different types:
DRUG MISUSE
Psychologic dependence
Drug habituation
Physiologic d.:
Drug dependence:
Drug abuse:
DRUG MISUSE
Inappropriate intake of a substance
Person’s need to take a drug
Need for the drug by body cells
Usual cells affected: CNS cells
Effect upon discontinuation: Withdrawal effects
Different types:
Drug habituation:
Pyschological d.:
DRUG MISUSE
Emotional dependence on a drug
Mild psychological dependence
Different types:
Drug Computations
Formula:
DRUG COMPUTATIONS
Dose on hand Dose Desired
=
Quantity on hand Quantity desired(x)
Formula:
DRUG COMPUTATIONS
Erythromycin 500 mg is ordered. It is supplied in a liquid form containing 250 mg in 5 ml.
Formula:
DRUG COMPUTATIONS
Dose on hand Dose Desired
=
Quantity on hand Quantity desired(x)
250 mg
5 mL
500 mg
1 Liter=__ quarts
Vital conversion values:
DRUG COMPUTATIONS
1 quart
1 Liter=__ pints 2 pints

1cup=___ mL
Vital conversion values:
DRUG COMPUTATIONS
240 mL
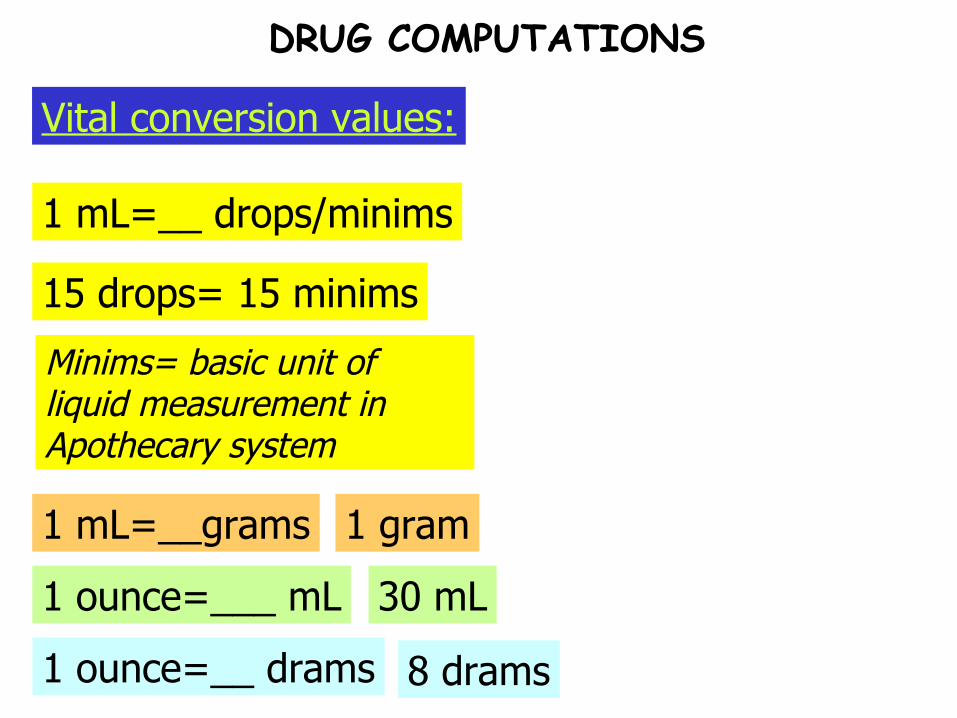
1 mL=__ drops/minims
Vital conversion values:
DRUG COMPUTATIONS
15 drops= 15 minims
1 mL=__grams 1 gram
1 ounce=___ mL 30 mL
Minims= basic unit of liquid measurement in Apothecary system
1 ounce=__ drams 8 drams

Vital conversion values:
DRUG COMPUTATIONS
1 tablespoon=___mL or ___teaspoons
15 mL= 3 teaspoons

1 gram(g)=___ grains
Vital conversion values:
DRUG COMPUTATIONS
60 grains (gr)= 1 mL
Grains= basic unit of solid measurement in Apothecary system

1 kg=__ lbs
Vital conversion values:
DRUG COMPUTATIONS
2.2 lbs

Vital conversion values:
DRUG COMPUTATIONS
1 gallon=___Liters/ quarts 4 Liters= 4 quarts
Vital conversion values:
DRUG COMPUTATIONS
1 mg =___ mcg 1,000 mcg
Convert 8 ounces to minims
Convert 2 pt to grains
Convert 30 pounds to ounces
Vital conversion values: Short exercise
DRUG COMPUTATIONS
It’s now time for actual problems!!!
Following mitral valve replacement surgery a client develops PVC’s. The health care provider orders a bolus of Lidocaine followed by a continuous Lidocaine infusion at a rate of 2 mg/minute. The IV solution contains 2 grams of Lidocaine in 500 cc of D5W. The infusion pump delivers 60 microdrops/cc. What rate would deliver 4 mg of Lidocaine/minute?
A) 60 microdrops/minuteB) 20 microdrops/minuteC) 30 microdrops/minuteD) 40 microdrops/minute
DRUG COMPUTATIONS
A client is receiving a standard concentration Heparin IV of 25,000 u Heparin in 250 ml D5W. The infusion is placed on an IV pump. The infusion rate is increased from 9 - 12 ml/hour. The Heparin dose is now ____ u/hr.
DRUG COMPUTATIONS
The health care provider orders an IV aminophylline infusion at 30 mg/hr. The pharmacy sends a 1,000 ml bag of D5W containing 500 mg of aminophylline. In order to administer 30 mg per hour, the RN will set the infusion rate at:A) 20 ml per hourB) 30 ml per hourC) 50 ml per hourD) 60 ml per hour
DRUG COMPUTATIONS
The following order is written for a clientwith deep vein thrombosis: Heparin 20,000units in 1000ml D5W to infuse at 1000 unitsof heparin per hour. How many ml of D5Wsolution should be administered per hour?A. 20B. 42C. 50D. 66
DRUG COMPUTATIONS
An infant who weighs 11 lb (5 kg) is toreceive 750 mg of antibiotic in a 24-hourperiod. The liquid antibiotic comes in a concentrationof 125 mg per 5 ml. If theantibiotic is to be given three times eachday, how many milliliters would the nurseadminister with each dose?A. 2B. 5C. 6.25D. 10
DRUG COMPUTATIONS
A physician orders 3000 mL of D5W to infuse over a 24-hour period. The drop factor is 10 drops per mL. A nurse sets the flow rate at how many drops per minute?
DRUG COMPUTATIONS

A patient who weighs 14 kg has a left lowerleg cellulitis. The drug ordered is ceftriaxonesodium (Rocephin), 75 mg/ kg/day IV piggy-backin two divided doses. Which of thefollowing amounts is correct for each dose?A. 105 mgB. 250 mgC. 525 mgD. 1050 mg
DRUG COMPUTATIONS

A patient with a deep vein thrombosis isreceiving 1200 units of heparin per hour,intravenously by infusion pump. The solutionavailable is heparin 25,000 units/500 ml.Which of the following is the correct pumpsetting?A. 20 ml/hrB. 58 ml/hrC. 24 ml/hrD. 13 ml/hr
DRUG COMPUTATIONS

A client has an order to receive 1000 ml ofintravenous fluids in 8 hours. The intravenousset delivers 60 microdrops per ml.The nurse should administer approximatelyhow many microdrops of fluid per minute?A. 21B. 40C. 63D. 125
DRUG COMPUTATIONS
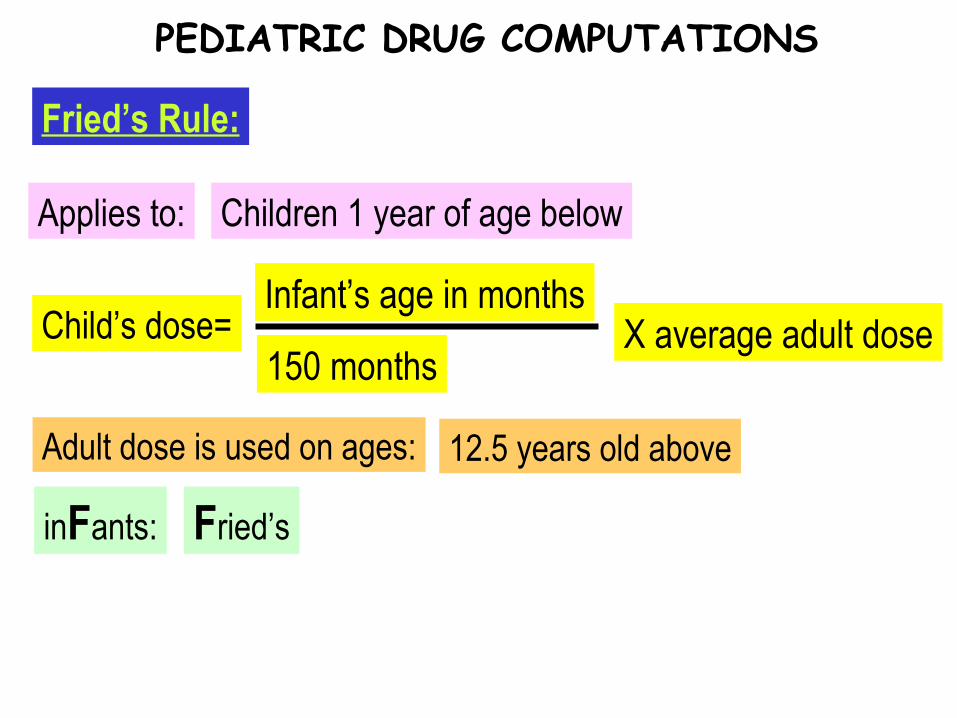
Child’s dose=
Applies to:
Fried’s Rule:
PEDIATRIC DRUG COMPUTATIONS
Children 1 year of age below
Infant’s age in months
150 months
Adult dose is used on ages: 12.5 years old above
X average adult dose
inFants: Fried’s

Child’s dose=
Applies to:
Young’s Rule:
PEDIATRIC DRUG COMPUTATIONS
Children ages 1 – 12 years old
Child’s age in years
Child’s age in years + 12
Young’s Years
X average adult dose

Child’s dose=
Applies to:
Clark’s Rule:
PEDIATRIC DRUG COMPUTATIONS
Any pediatric client
Weight of child in lbs.
150 pounds
Clark’s Calories (weight)
X average adult dose

Child’s dose=
Applies to:
Surface area calculation:
PEDIATRIC DRUG COMPUTATIONS
Any pediatric client
Surface area in square meters
1.73X average adult dose
The usual adult dose of Benadryl is 50 mg. What would be a safe dose for a child weighing 27 1bs?
a. 0.9 mgb. 1.8 mgc. 9.0 mgd. 18 mg
PEDIATRIC DRUG COMPUTATIONS
The average adult dose of meperidine is 75 mg. What dose would be appropriate for a 10-month-old infant?a. 50 mgb. 5 mgc. 25 mgd. 0.5 mg
PEDIATRIC DRUG COMPUTATIONS
Principles in Drug Administration

Medication Orders / Forms of Meds
Standing order:
Single order:
Stat order:
Types:
MEDICATION ORDERS
Given immediately and only once
Given once at a specified time
Carried out indefinitely until an order cancels it
May be carried out for a specified # of days
PRN order: Given as necessary according to nurse’s own judgment

June 2007 Board Exam question:
A drug is to be given every 4 hours as necessary for pain. It was last given at 8:00 a.m. When should it be given next?
a. 12:00 noon when the client complains of pain
b. Anytime as necessary whenever the client complains of pain
c. 4:00 p.m.
d. 12:00 noon with/ without pain
MEDICATION ORDERS
Name of drug to be given:
Date the order was written:
Client’s full name:
SIX Essential parts:
DRUG ORDER
First,middle initials and last name
Day,month and year
Generic names, Trade names
SIX Essential parts:
DRUG ORDER
Drug dosage: Amount and frequency
Method of administration
Signature of physician/ NP
Telephone orders – signed 1st by the nurse then by the physician within 24- 48 hours

Capsule:
FORMS OF MEDICATION
Why is the capsule colored? To aid in product identification
Is it necessary to open the capsule? Gelatin shell dissolves in stomach
Douches:
FORMS OF MEDICATION
Forms: Powder or liquid concentrations
Elixirs:
FORMS OF MEDICATION
Contents: Water+ alcohol+ Sorbitol + sweeteners

Suppositories:
FORMS OF MEDICATION
Position upon insertion: Left sims

Troches:
FORMS OF MEDICATION
Other names: Lozenges; Pastilles

Basic Principles
Cloudy medications?
Relabelling of med containers?
Unfamiliar medications? Never administer
Pharmacist
Return to pharmacy
Medication @ bedside? Never! Leave until client swallows the meds
Basic Principles:
ADMINISTERING MEDICATIONS
Pre-op meds during post-op?
Client vomits?
Endorsement of meds?
The nurse who prepares the drug is the only one who can give it.
Report to charge nurse/ physician
Assumed discontinued unless otherwise ordered
Medication error: Report to charge nurse/ physician
Basic Principles:
ADMINISTERING MEDICATIONS
Always assess client status before giving meds
Double check:
Identify the client:
Process:
ADMINISTERING MEDICATIONS
Check wristband with Medication Administration Record
Ask the client or another nurse to identify client

Process:
ADMINISTERING MEDICATIONS
Give the medication
Never leave @ bedside
Evaluate and document

Pharmacy:
Systems:
Physician:
Medication errors:
Illegible order
Interrupted to do other duties
Not all doses delivered
Individual: Order not transcribed properly
Knowledge: Similar medication names
ADMINISTERING MEDICATIONS
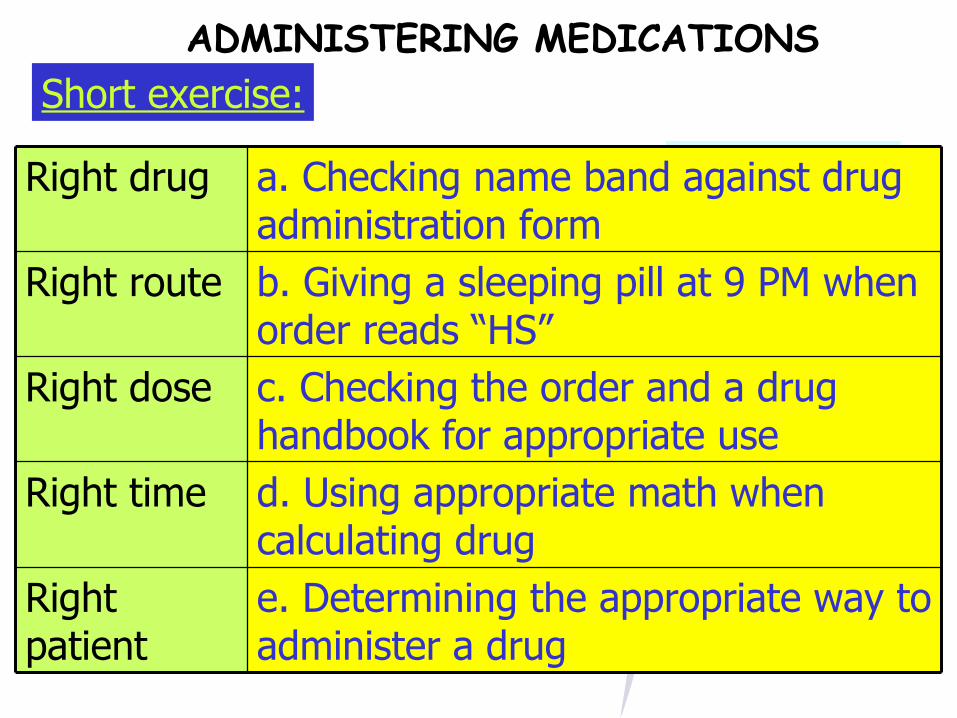
Short exercise:ADMINISTERING MEDICATIONS
e. Determining the appropriate way to administer a drug
Right patient
d. Using appropriate math when calculating drug
Right time
c. Checking the order and a drug handbook for appropriate use
Right dose
b. Giving a sleeping pill at 9 PM when order reads “HS”
Right route
a. Checking name band against drug administration form
Right drug

ADMINISTERING ORAL MEDICATIONS
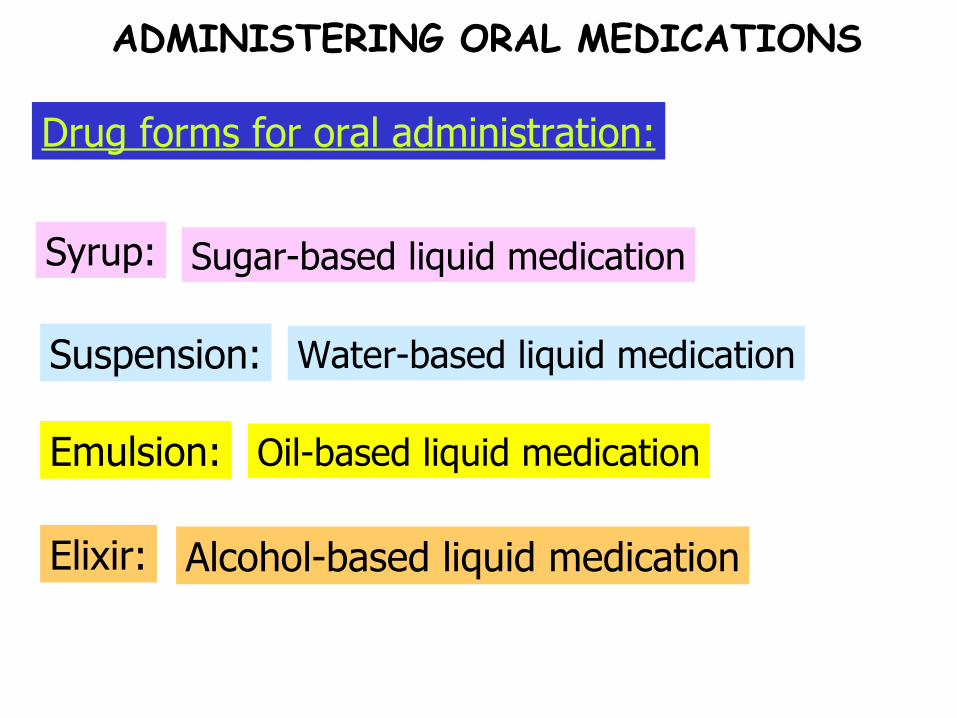
Emulsion:
Suspension:
Syrup: Sugar-based liquid medication
Water-based liquid medication
Oil-based liquid medication
Elixir: Alcohol-based liquid medication
Drug forms for oral administration:
ADMINISTERING ORAL MEDICATIONS

Sustained release:
Enteric coated: Irritating to GIT if crushed
Shorter duration of action if crushed
Drug forms for oral administration:
ADMINISTERING ORAL MEDICATIONS

Trivia Time
What guideline should be followed to allow for maximum absorption
of elixirs after giving?
ADMINISTERING ORAL MEDICATIONS
Trivia Time: ANSWER
Allow 30 minutes to elapse before giving water
ADMINISTERING ORAL MEDICATIONS

Measurement guide when reading liquid medications:
How many times do you verify the “right drug”?
Commonly asked questions?
ADMINISTERING ORAL MEDICATIONS
3x
Read at the bottom of the meniscus at eye level
Before, during and after giving the drug
Commonly asked questions?
ADMINISTERING ORAL MEDICATIONS
If there’s difficulty swallowing:
Place at back of mouth (stimulates swallowing reflex)
If client states that the drug you’re giving looks unfamiliar:
Withhold and double check the order
Trivia Time
Why are honey and essential food items avoided when mixing medications
for pediatric clients?
ADMINISTERING ORAL MEDICATIONS
Trivia Time: ANSWER
To prevent botulism; to ensure adequate nutrition
ADMINISTERING ORAL MEDICATIONS
To prevent nausea…
Pediatric clients:
Give chilled carbonated beverage before or immediately after giving the drug
If using a syringe to give a liquid med:
Place it along the side of the infant’s tongue
ADMINISTERING ORAL MEDICATIONS

I
Qu Quinidine
Isoniazid
E Erythromycin
T Tetracycline
Normally taken on an empty stomach with a full glass of water:
ADMINISTERING ORAL MEDICATIONS
A
C
R
P
S
Normally taken on an empty stomach with a full glass of water:
ADMINISTERING ORAL MEDICATIONS
Cephalosporin
Acetaminophen, Aspirin
Rifampin
Sulfonamides
Penicillin, Proprantheline
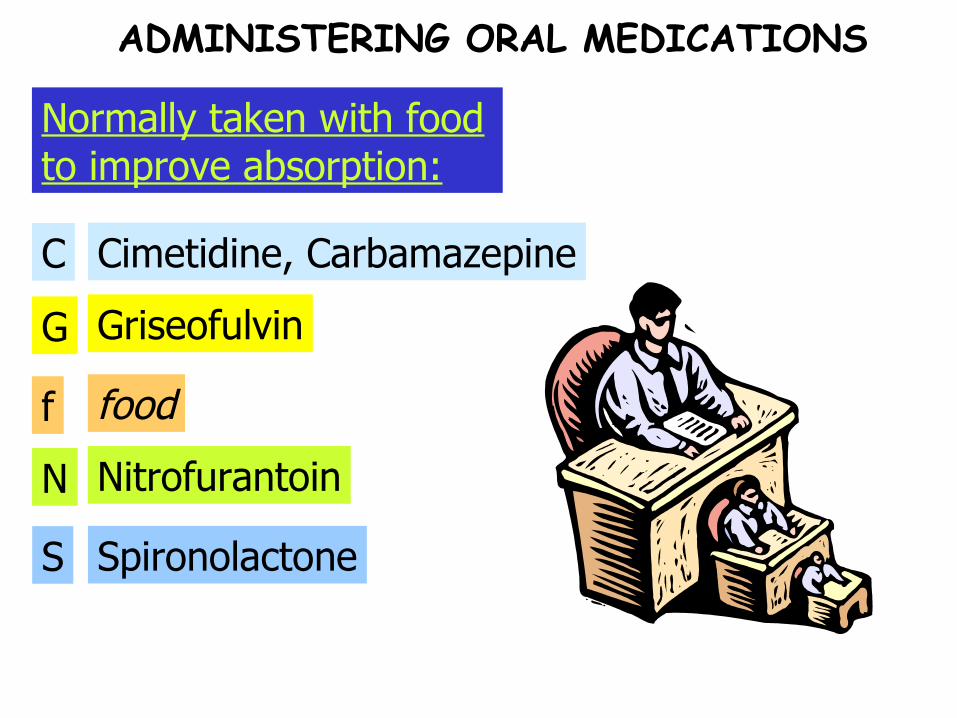
G
C Cimetidine, Carbamazepine
Griseofulvin
f food
N
S Spironolactone
Nitrofurantoin
Normally taken with food to improve absorption:
ADMINISTERING ORAL MEDICATIONS

H
P Propranolol
Hydralazine
I Indomethacin
L. Lithium
Normally taken with food to improve absorption:
ADMINISTERING ORAL MEDICATIONS
ADMINISTERING SUBLINGUAL MEDICATIONS
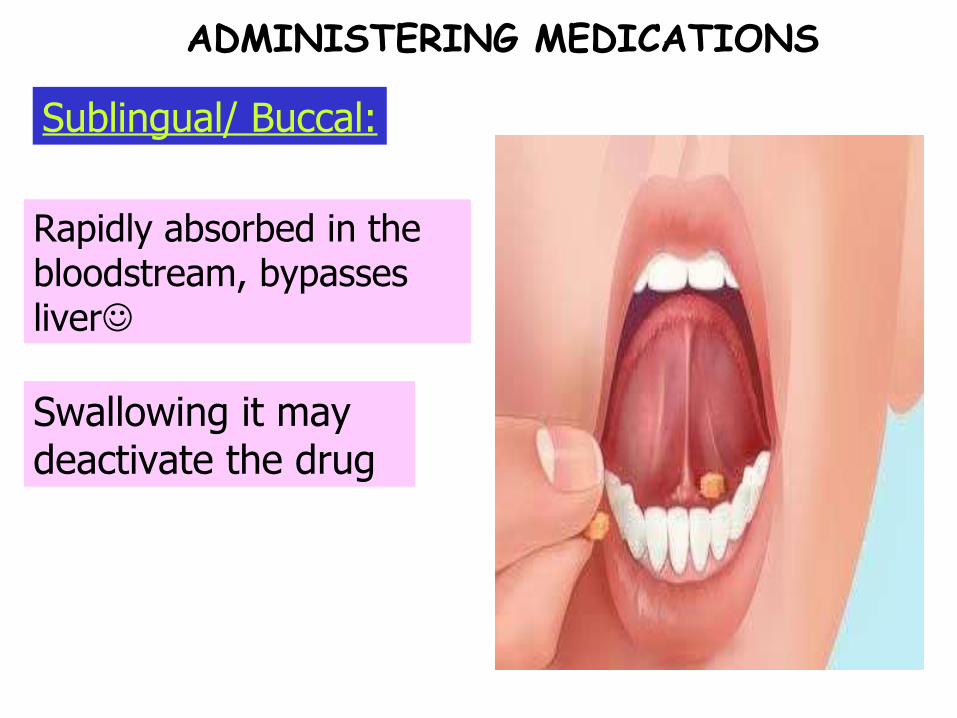
Sublingual/ Buccal:
Rapidly absorbed in the bloodstream, bypasses liver
Swallowing it may deactivate the drug
ADMINISTERING MEDICATIONS

ADMINISTERING TOPICAL MEDICATIONS

Ophthalmic:
ADMINISTERING MEDICATIONS
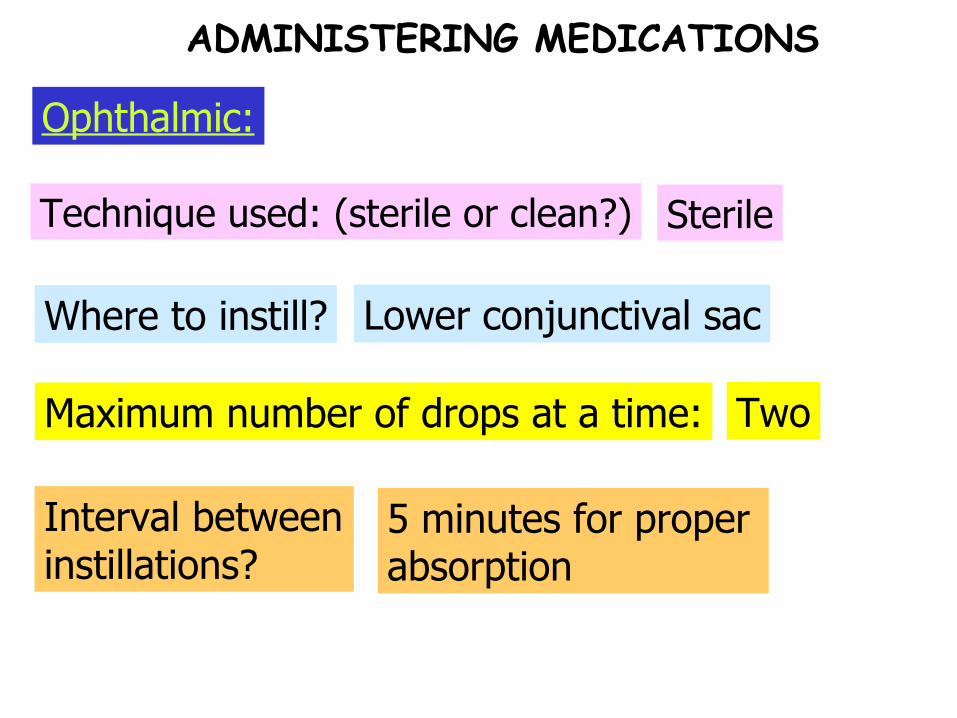
Maximum number of drops at a time:
Where to instill?
Technique used: (sterile or clean?) Sterile
Lower conjunctival sac
Two
Interval between instillations?
5 minutes for proper absorption
Ophthalmic:
ADMINISTERING MEDICATIONS

To prevent systemic absorption:
Closing of eyes: Gently but not tightly to avoid spillage
Press firmly on nasolacrimal duct for at least 30 secs.
Ophthalmic:
ADMINISTERING MEDICATIONS
Otic:
ADMINISTERING MEDICATIONS

Posn:
Using hot/cold soln:
Solution temperature: Warm/ body temperature
Nausea, vertigo, pain
Side-lying with ear being treated up
Straighten ear canal: pinna down & back: 0-3 y.o.
Otic:
ADMINISTERING MEDICATIONS
Straighten ear canal: pinna up & back: Above 3
Pos’n after:
To assist medication flow:
Where to instill: Along side of auditory canal
Press on tragus
Side-lying for another 5 minutes
To prevent spillage:
Place cotton loosely at auditory canal for 15-20 mins
Otic:
ADMINISTERING MEDICATIONS
Nasal:
ADMINISTERING MEDICATIONS
Upon inhalation:
Position:
Usual purpose: Astringent effect (shrinking effect)
Head tilted back (sit/lie)
Administer the spray
Position after: Keep head tilted back for an additional 5 minutes
Nasal:
ADMINISTERING MEDICATIONS
Daily sprays: Use alternate nares
Nebulization/ MDIs:
ADMINISTERING MEDICATIONS

After pressing canister:
Mouthpiece position:
Position: Semi/ high-fowler’s
1-2 inches away from mouth
Hold breath for 10 secs
A-B-C mnemonic
ADMINISTERING MEDICATIONS
Nebulization/ MDIs:
Time interval in between next dose: 1 minute

Trivia Time
What should you instruct the client to do if steroid medications
were given via MDI
ADMINISTERING MEDICATIONS

Trivia Time: ANSWER
Rinse mouth to prevent oral fungal infection
ADMINISTERING MEDICATIONS

Rectal Instillations/ Suppositories
ADMINISTERING MEDICATIONS

What to instruct the patient?
Position: Left- sims
Relax: breath thru mouth
What to wear? Gloves
How far do we insert?
Why that far? It’s beyond the internal sphincter
Instructions post- insertion:
Remain side-lying for at least 5-20 mins
Adult: 4 inches; child/ infant: 2 inches
ADMINISTERING MEDICATIONS
Rectal Instillations/ Suppositories
ADMINISTERING PARENTERAL MEDICATIONS

Sites:
Intradermal Injection:
Inner lower arm, upper chest/back, beneath scapulae
ADMINISTERING MEDICATIONS
To massage or not to massage? Don’t massage the site after
Needle gauge: 25-27
Upon insertion, needle is at… 10-15 degree angle, bevel up
ADMINISTERING MEDICATIONS
Intradermal Injection:
Needle length: 3/8” to ½”
June 2006 Board Exam question:
What is the angle of the needle bevel when performing intradermal injections?
a. Parallel to the skin
b. 10-15 degrees
c. 30-45 degrees
d. 90 degrees
MEDICATION ORDERS

June 2006 Board Exam question:
What is gauge of the needle used for intradermal injections?
a. 27
b. 23
c. 18
d. 20
MEDICATION ORDERS
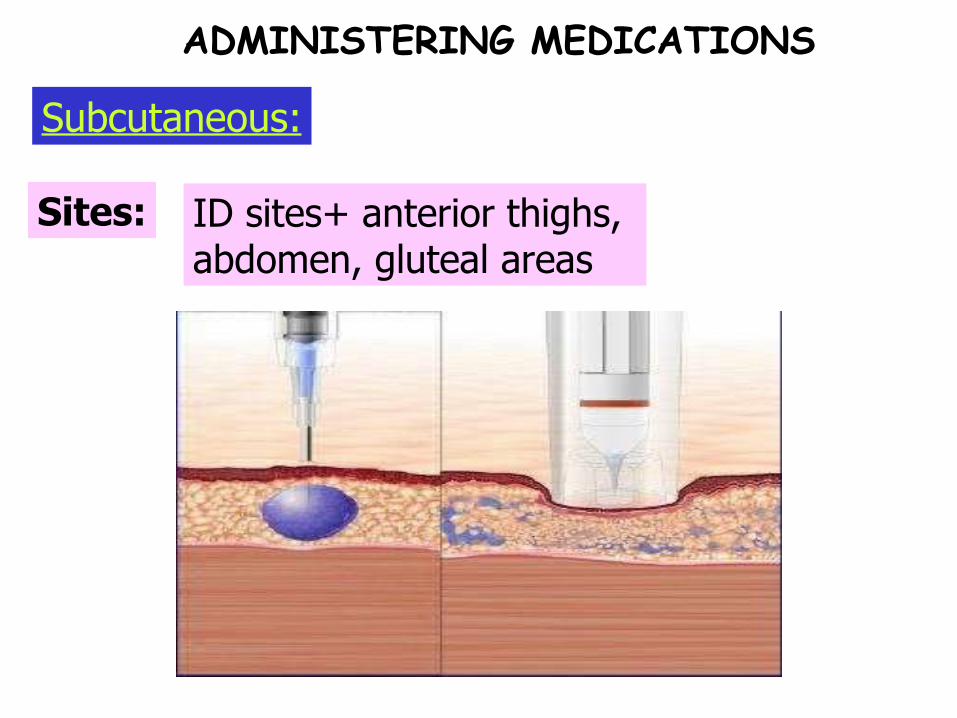
Sites:
Subcutaneous:
ID sites+ anterior thighs, abdomen, gluteal areas
ADMINISTERING MEDICATIONS
When injecting at 45 degrees:
Dosage:
Meds given SQ: Vaccines, insulin, heparin, narcotics
0.5-1mL
5/8 needle
Needle gauge: 25-27
Subcutaneous:
ADMINISTERING MEDICATIONS
When injecting at 90 degrees: 1/2 needle
For obese patients:
For thin patients: 45 degree angle of needle
90 degree angle of needle
ADMINISTERING MEDICATIONS
Subcutaneous:
For heparin injection: Do not aspirate nor massage
For insulin injections: Inject @ 90 but don’t massage
For other injections: Aspirate before injecting

Trivia Time
What should be ideally done if blood is seen upon withdrawal of the plunger?
ADMINISTERING MEDICATIONS

Trivia Time: ANSWER
Remove the needle and discard the medication/equipment
ADMINISTERING MEDICATIONS
Intramuscular:
ADMINISTERING MEDICATIONS

Possible sites:
Length:
Gauge: 20-23
1-2 inches
Gluteal, Vastus lateralis, deltoid
Intramuscular:
ADMINISTERING MEDICATIONS
ADMINISTERING MEDICATIONS
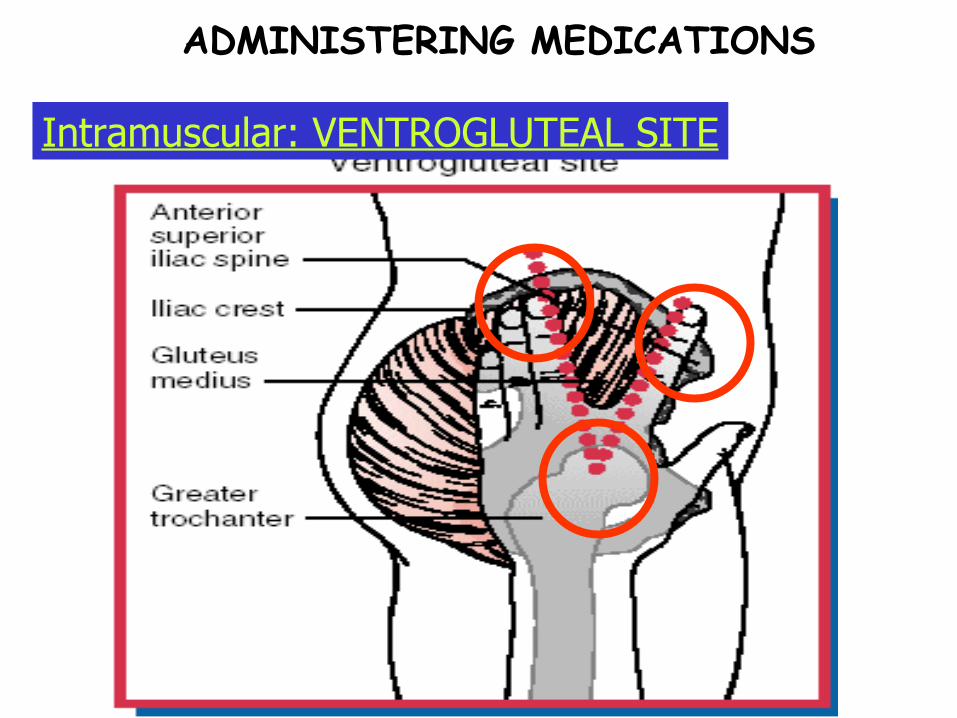
Intramuscular: VENTROGLUTEAL SITE
Abduct middle finger
Place index finger over ASIS
Hand heel over greater trochanter
Triangle formed below crest is the site
ADMINISTERING MEDICATIONS
Intramuscular: VENTROGLUTEAL SITE

ADMINISTERING MEDICATIONS
Intramuscular: VENTROGLUTEAL SITE

Muscle: Gluteus medius
Degree of contamination:
Lesser since it’s farther from rectal area
ADMINISTERING MEDICATIONS
Intramuscular: VENTROGLUTEAL SITE
Ventrogluteal:
Von Hochsteter’s Site: Ventrogluteal
formed is the V site
Vessel-free
Purpose of above instructions:
Instructions when side-lying:
Instructions when prone: Curl toes inward
Flex knee/hip
Relax muscles
ADMINISTERING MEDICATIONS
Intramuscular: VENTROGLUTEAL SITE

ADMINISTERING MEDICATIONS
Intramuscular: DORSOGLUTEAL SITE
Imaginary line from PSIS to GT

ADMINISTERING MEDICATIONS
Intramuscular: DORSOGLUTEAL SITE
4 quadrants– Upper outer quadrant
Risks:
Contraindicated age: Below 3 years old
Injury to sciatic nerve/ major blood vessel
ADMINISTERING MEDICATIONS
Intramuscular: DORSOGLUTEAL SITE

CHULOU H. PENALES, RN
ADMINISTERING MEDICATIONS
Vital fact:
Recommended site for infants
Intramuscular: VASTUS LATERALIS
ADMINISTERING MEDICATIONS
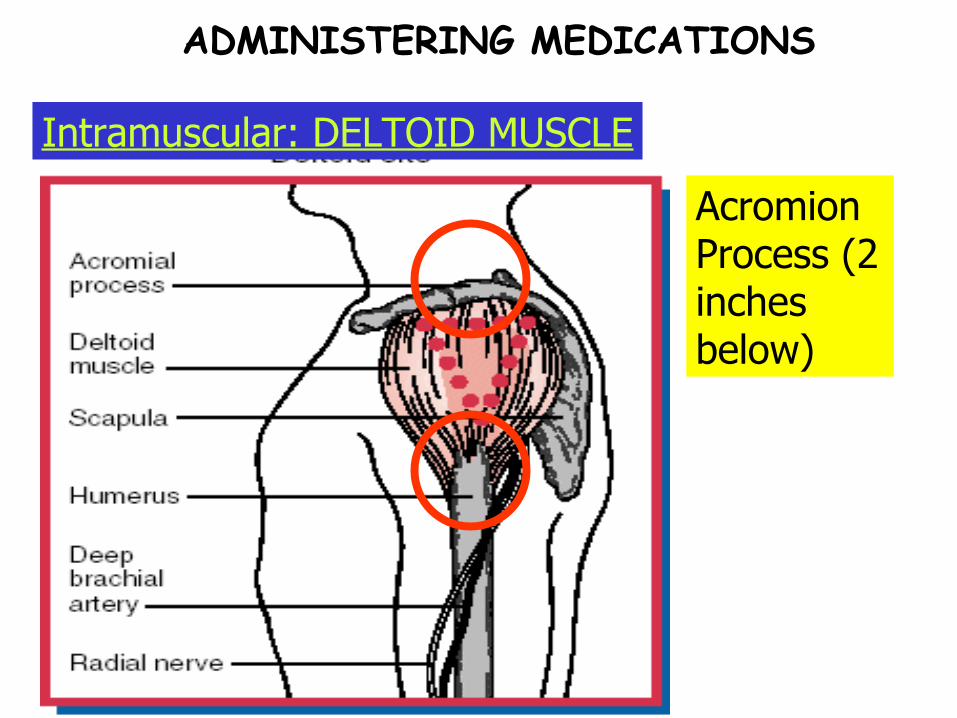
Intramuscular: DELTOID MUSCLE
Acromion Process (2 inches below)
Site is approx 2 inches from AP
Midpoint between AP & axillary fold
Acromion Process
ADMINISTERING MEDICATIONS
Intramuscular: DELTOID MUSCLE
Risks:
Deltoid: 0.5 – 2 mL
ADMINISTERING MEDICATIONS
Gluteus Medius: 1-5 mL
Relatively small muscle; possible injury to radial nerve & artery
Intramuscular: DELTOID MUSCLE
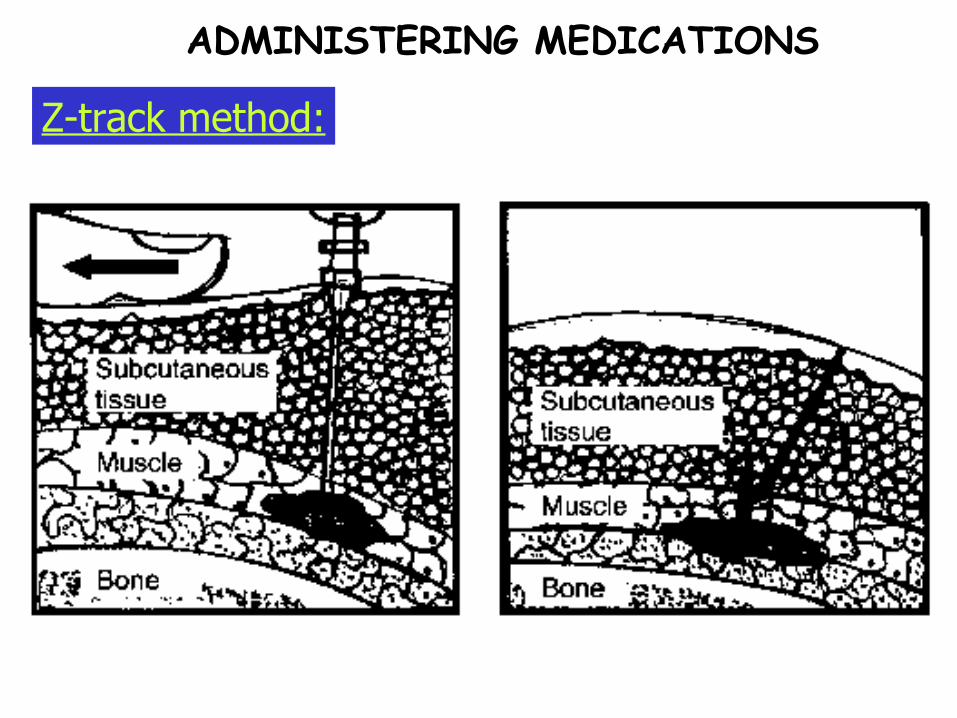
Z-track method:
ADMINISTERING MEDICATIONS

To massage or not to massage?
When is it used?
Z-track IM method:
Irritating meds (eg: Iron)
Do not massage.
ADMINISTERING MEDICATIONS
How to minimize discomfort pre-inj.:
Needle introduction:
Air lock technique: 0.2 mL air bubble
Introduce in a quick thrust
Cold compress
How to minimize discomfort upon needle withdrawal:
Support the tissues with cotton swabs
General Principles: Parenteral Medicatons
ADMINISTERING MEDICATIONS

The type of physician’s order that is carried out upon the judgment of the nurse, as required by the patient is:
a. Standing order
b. Single order
c. STAT order
d. PRN order
PRACTICE QUESTIONS
The most accurate method of identifying a client before drug administration is by:
a. Asking the client to state his name
b. Calling the client by his name
c. Asking a relative to identify the client
d. Checking the identification band/ bracelet of the client
PRACTICE QUESTIONS
Which of the following are true about absorption of medications
1. Rich blood flow promotes faster absorption of medications
2. Exercise enhances absorption of oral medications
3. High concentration of drugs promote a rapid effect
4. Liquid medications are more rapidly absorbed than solid medications
f. 1,2,3 b. 2,3,4 c. 1,3,4 d.1,2,3,4
PRACTICE QUESTIONS
During application of medication into the ear, which of the following is an inappropriate nursing action?
a. Warm the medication at room or body temperature
b. In an adult, pull the pinna upward
c. Instill the medication directly into the tympanic membrane
d. Press the tragus of the ear a few times to assist the flow of medication into the ear canal
PRACTICE QUESTIONS
Parenteral Medications and IV fluids

Extracellular fluidsIntracellular fluids
Division of Body fluids
40% of body weight 20% of body weight
PARENTERAL MEDICATION/ IV FLUIDS

Diffusion
Movement of Fluids
PARENTERAL MEDICATION/ IV FLUIDS
Osmosis
Movement of Fluids
PARENTERAL MEDICATION/ IV FLUIDS

Filtration
Movement of Fluids
PARENTERAL MEDICATION/ IV FLUIDS
Exercise Question:
What is the mechanism by which Mannitol decreases IOP in patients with Glaucoma?
a. Diffusion
b. Osmosis
c. Filtration
d. Diuresis
PARENTERAL MEDICATION/ IV FLUIDS
Exercise Question:
The movement of air from the environment into the lungs follows what principle of gas movement?
a. Diffusion
b. Osmosis
c. Respiration
d. Filtration
PARENTERAL MEDICATION/ IV FLUIDS
Exercise Question:
Who among the following are at highest risk for dehydration?
a. A breastfeeding 8-month old infant
b. A 17 year-old with fever
c. A 61 year-old man jogging
d. A pregnant woman
PARENTERAL MEDICATION/ IV FLUIDS

Above 40 y.o.: 40-50%
Fast fact: Body fat is inversely proportional to body fluids.
Adult: 50-60%
Infant: 60-70%
Neonate: 70-80 %
Fluids as Percentage of Body weight
PARENTERAL MEDICATION/ IV FLUIDS

Urine
Lungs (Insensible)
Average daily adult output:
1400-1500 mL
350-400 mL
350-400 mL
100 mL
Skin (Insensible)
Sweat
Feces
Total
100-200mL
2,300-2,600 mL
PARENTERAL MEDICATION/ IV FLUIDS
Osmotic/ Oncotic pressureHydrostatic pressure
Pressures within the Blood vessel
Pushing force of a fluid against the walls that contain it
Pulling power of a solution for water
PARENTERAL MEDICATION/ IV FLUIDS

Trivia Time
What happens when hydrostatic pressure exceeds osmotic/oncotic
pressure?
PARENTERAL MEDICATION/ IV FLUIDS
Trivia Time: ANSWER
3rd space fluid shift: manifested by decreased urine output. Occurs in
burns, peritonitis, massive bleeding into a joint/cavity.
PARENTERAL MEDICATION/ IV FLUIDS

Trivia Question:
Are osmolality and Osmolarity the same?
PARENTERAL MEDICATION/ IV FLUIDS

Osmolarity:
Osmolality:
Osmolality vs Osmolarity
Solute / Kg of Water
Solute/ Kg of a solution
PARENTERAL MEDICATION/ IV FLUIDS

Osmolality vs Osmolarity
Can we use the terms interchangeably? Yes
If osmolality is high, what is the osmotic pressure of that solution?
High
PARENTERAL MEDICATION/ IV FLUIDS

Osmolality And Sodium
Major plasma solute that determines Osmolality: Na
Formula for estimated Osmolality: 2 x Serum Na
Na: 135-145 mEq/L
Serum Osmolality: 270-290 mOsm/L
PARENTERAL MEDICATION/ IV FLUIDS
Isotonic solution
Types of solutions:
PARENTERAL MEDICATION/ IV FLUIDS

Indications: Dehydration or any ECF volume deficit
Types of solutions: ISOTONIC
Same osmolality as plasma Osmolality:
PARENTERAL MEDICATION/ IV FLUIDS

Normal Saline(PNSS; 0.9% NaCl): NaCl
ISOTONIC Solutions:
Ringer’s Sol’n.: Na,K,Ca
Lactated Ringer’s: Ringer’s + Lactate & Chloride
PARENTERAL MEDICATION/ IV FLUIDS
Trivia Question:
Do most isotonic fluids contain dextrose,
magnesium or bicarbonate?
NO
PARENTERAL MEDICATION/ IV FLUIDS
5% Dextrose in water (D5W)
Lactated Ringer’s Solution
0.9% Saline (NS)
Memory tip: commonly used solutions
Isotonic Solutions
5% Dextrose in .225% Saline (5% D/ 1.4 NS)
Exceptions to the memory tip on hypertonic solutions
PARENTERAL MEDICATION/ IV FLUIDS

Hypertonic solution
Types of solutions:
PARENTERAL MEDICATION/ IV FLUIDS
Indications: Hyponatremia
Types of solutions: HYPERTONIC
Used in limited doses in carefully controlled settings via an infusion pump
Precaution:
Hypernatermia & FVORisks:
Close monitoring (V/S; Lungs; Neuro; Na)
Nursing action:
PARENTERAL MEDICATION/ IV FLUIDS

Sample Question:
This hypertonic solution may be given via IV push for hypoglycemia in a code situation:
a. 50% Dextrose
b. 10% Dextrose
c. PNSS
d. 5% Saline
PARENTERAL MEDICATION/ IV FLUIDS
Sample Question:
This hypertonic solution is used to treat newborns with hypoglycemia as part of the treatment protocol:
a. 5% Dextrose
b. 10% Dextrose
c. Plain LR
d. 5% Saline
PARENTERAL MEDICATION/ IV FLUIDS

TYPES OF INTRAVENOUS SOLUTIONS
10 % Dextrose in water (D10W)
5% Saline (5% NS)
3% Saline (3% NS)
Memory tip: anything that’s above 0.9% or any combinations
Hypertonic Solutions
5% Dextrose in 0.9% Saline (5% D/NS)
5% Dextrose in 0.45% Saline (5% D/ 1/2NS)
5% Dextrose in lactated ringer’s solution

Trivia Question:
Do most hypertonic solutions provide calories to cells?
Yes
PARENTERAL MEDICATION/ IV FLUIDS

Hypotonic solution
Types of solutions:
PARENTERAL MEDICATION/ IV FLUIDS
Indications: Cellular dehydration
Types of solutions: HYPOTONIC
Acute brain injuryMajor contraindication:
PARENTERAL MEDICATION/ IV FLUIDS
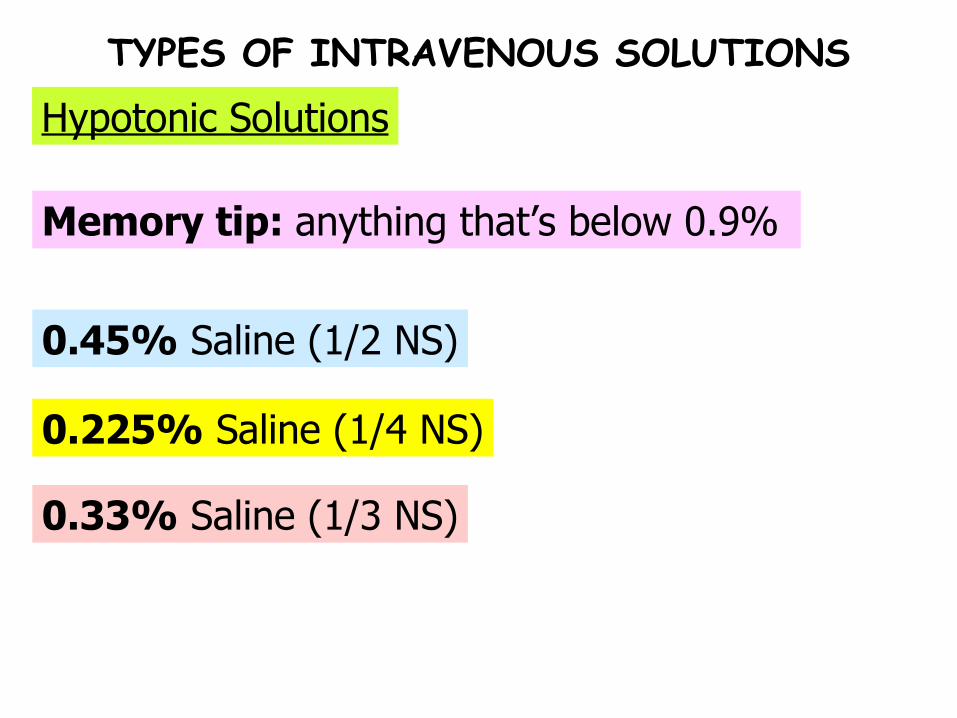
TYPES OF INTRAVENOUS SOLUTIONS
0.33% Saline (1/3 NS)
0.225% Saline (1/4 NS)
0.45% Saline (1/2 NS)
Memory tip: anything that’s below 0.9%
Hypotonic Solutions
Sample Question:
If 1 liter of 0.45 saline/ 0.225 saline is given to patient, how much of it actually enters the cells
a. 1 Liter
b. 800 mL
c. 500 mL
d. 200 mL
PARENTERAL MEDICATION/ IV FLUIDS

Sample Question:
Does D5W provide adequate nutritional calories?
No, but it does prevent ketosis
PARENTERAL MEDICATION/ IV FLUIDS
Colloid volume expanders
Types of solutions:
PARENTERAL MEDICATION/ IV FLUIDS

Indications: Acute volume loss
Types of solutions: Colloid volume expanders
Albumin, Dextran, HetastarchExamples:
PARENTERAL MEDICATION/ IV FLUIDS

Air embolism prevention by: Priming IV tubing
Change IV tubing every: 72 hours
Change IV needle insertion site every:
15-20 minutes
PARENTERAL MEDICATION/ IV FLUIDS
IV Fluid therapy guidelines:
Regulate IV every:
72 hours

Infiltration:
IV INFUSION COMPLICATIONS

Skin appearance:
Skin temp:
Definition:
Infiltration:
Needle out of vein, accumulates in SQ tissue
Cold
Pale with edema
IV flow rate: Decreases or stops
Backflow of blood: Absent
Nursing action: Change the IV site and apply warm compress
IV INFUSION COMPLICATIONS

Thrombophlebitis:
IV INFUSION COMPLICATIONS
Skin appearance:
Skin temp:
Causes:
Thrombophlebitis:
Irritating solutions, overuse of vein
Warm
Redness and edema
Palpation findings: Vein feels hard and cordlike
Prevention: Change IV site every 72 hours
Nursing action: Change site and apply cold compress then warm compress
IV INFUSION COMPLICATIONS
Circulatory Overload:
IV INFUSION COMPLICATIONS

Patient position:
Action:
Symptoms:Increased BP,HR, Dyspnea, Crackles, Weight gain
Slow infusion to KVO rate then call doctor
High-fowler’s position
Possible medications: Diuretics and bronchodilators
Circulatory Overload:
IV INFUSION COMPLICATIONS

Drug Overload:
IV INFUSION COMPLICATIONS
Action:
Symptoms: Dizziness, shock, fainting
Slow infusion to KVO rate then call doctor
Drug Overload:
IV INFUSION COMPLICATIONS
Pulmonary Embolism:
IV INFUSION COMPLICATIONS
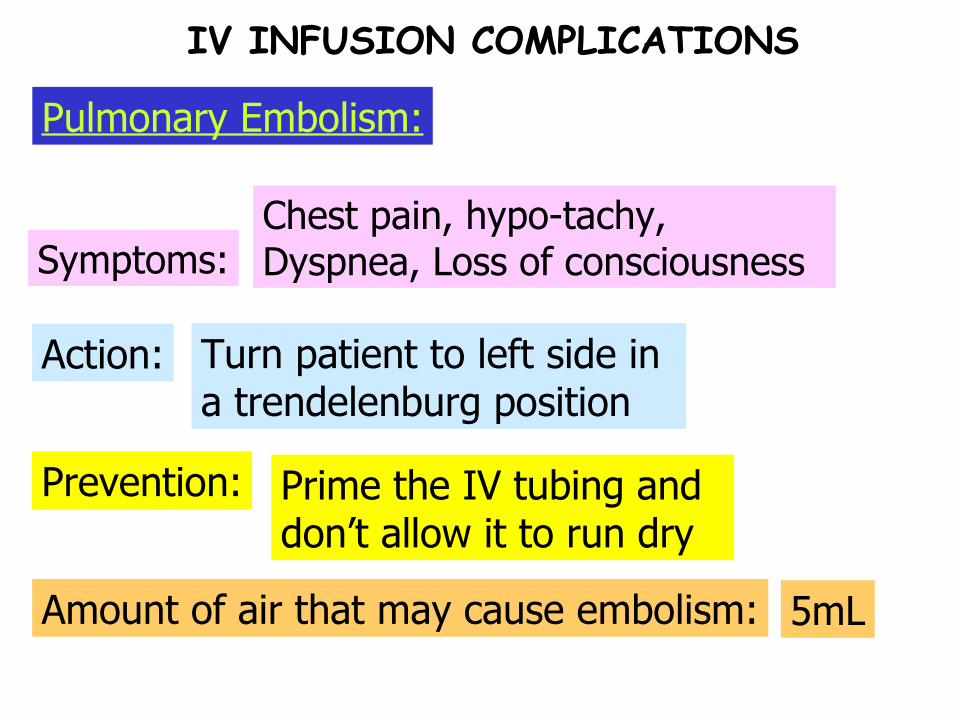
Prevention:
Action:
Symptoms:Chest pain, hypo-tachy, Dyspnea, Loss of consciousness
Turn patient to left side in a trendelenburg position
Prime the IV tubing and don’t allow it to run dry
Amount of air that may cause embolism: 5mL
IV INFUSION COMPLICATIONS
Pulmonary Embolism:
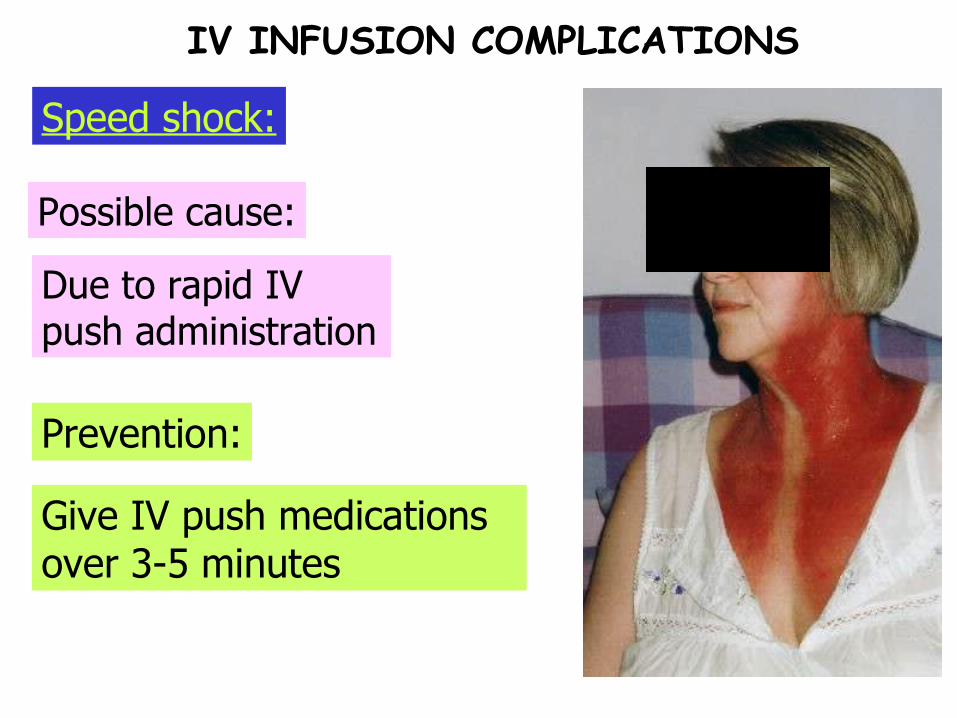
Prevention:
Possible cause:
Due to rapid IV push administration
Give IV push medications over 3-5 minutes
IV INFUSION COMPLICATIONS
Speed shock:

Insulin Therapy and Oral Hypoglycemics
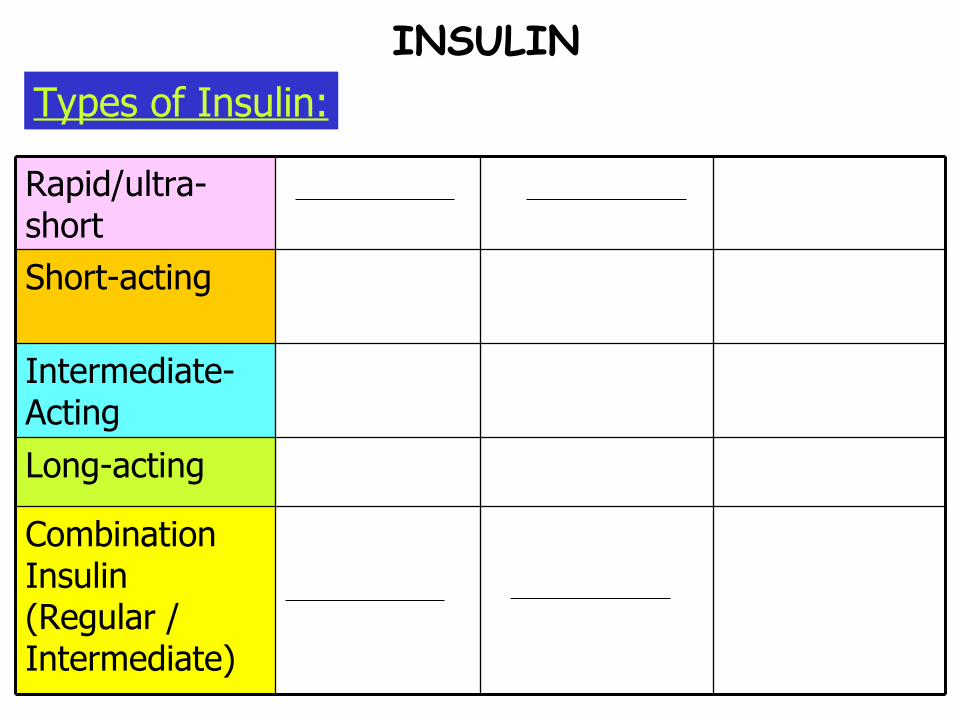
Combination Insulin (Regular / Intermediate)
Long-acting
Intermediate- Acting
Short-acting
Rapid/ultra-short
INSULINTypes of Insulin:
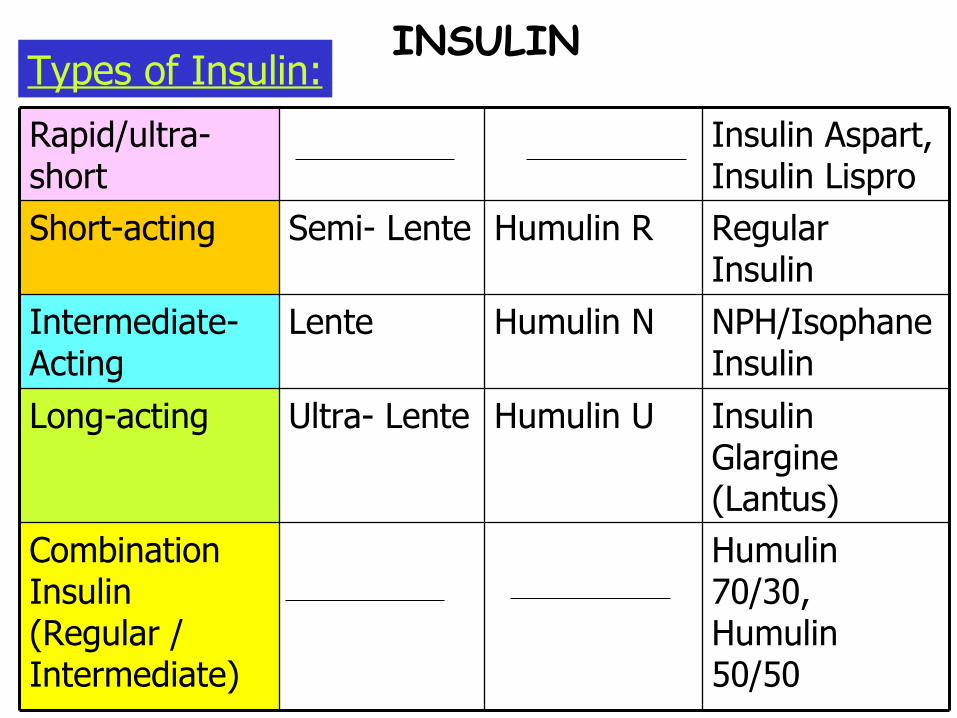
Ultra- Lente
Lente
Semi- Lente
Humulin U
Humulin N
Humulin R
Humulin 70/30, Humulin 50/50
Combination Insulin (Regular / Intermediate)
Insulin Glargine (Lantus)
Long-acting
NPH/Isophane Insulin
Intermediate- Acting
Regular Insulin
Short-acting
Insulin Aspart, Insulin Lispro
Rapid/ultra-short
INSULINTypes of Insulin:
Long-acting
Intermediate acting
Short acting
Rapid
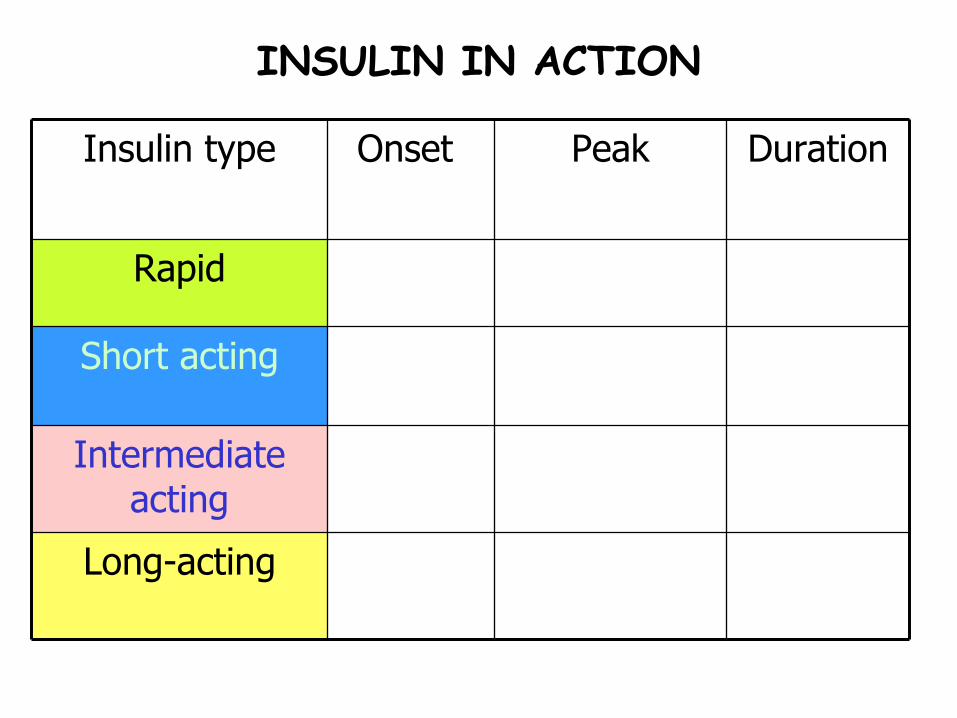
DurationPeakOnset Insulin type
INSULIN IN ACTION

x2x3 +10/ 3Long-acting
x3x3 + 10/ 2Intermediate acting
x32-4 hoursKEY VALUE
/ 2Short acting
x3.5-1.5 hours
/ 2Rapid
DurationPeakOnset Insulin type
INSULIN IN ACTION

MIXING INSULIN (R. N. Mnemonic)
R=
N=
Note: never shake the vial ‘cos it creates bubbles leading to inaccurate dosing. Roll it between your palms instead.
Draw Regular Insulin First (Clear)
Draw NPH Insulin Next (Cloudy)
INSULINDawn phenomenon vs. Somogyi Effect
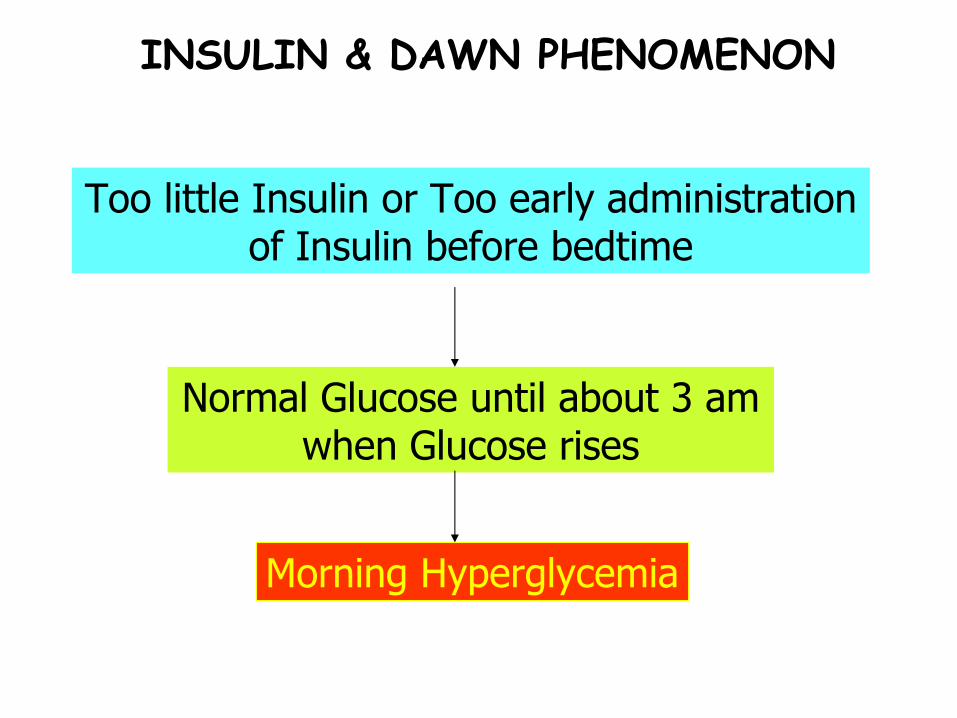
INSULIN & DAWN PHENOMENON
Too little Insulin or Too early administration of Insulin before bedtime
Normal Glucose until about 3 am when Glucose rises
Morning Hyperglycemia

INSULIN & SOMOGYI EFFECT
Too much Insulin or too little bedtime snack before bedtime
Normal Glucose until about 3 am when Glucose lowers to HYPOGLYCEMIC levels
Morning Hyperglycemia
Counterregulatory hormones
SNS Rebound effect
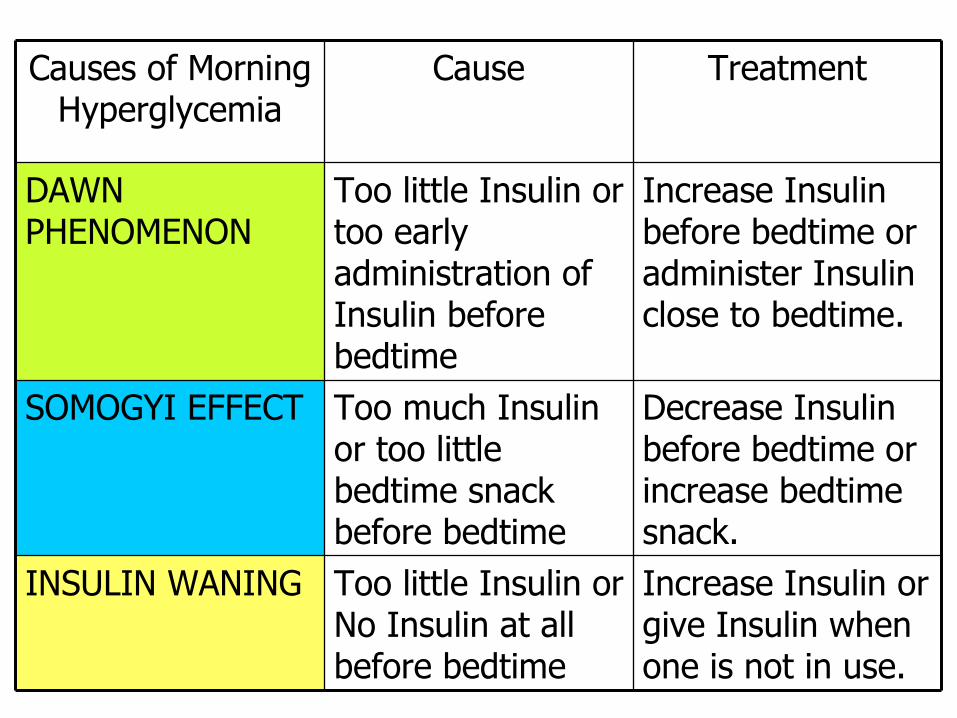
Decrease Insulin before bedtime or increase bedtime snack.
Too much Insulin or too little bedtime snack before bedtime
SOMOGYI EFFECT
Increase Insulin or give Insulin when one is not in use.
Too little Insulin or No Insulin at all before bedtime
INSULIN WANING
Increase Insulin before bedtime or administer Insulin close to bedtime.
Too little Insulin or too early administration of Insulin before bedtime
DAWN PHENOMENON
TreatmentCauseCauses of Morning Hyperglycemia
Treatment
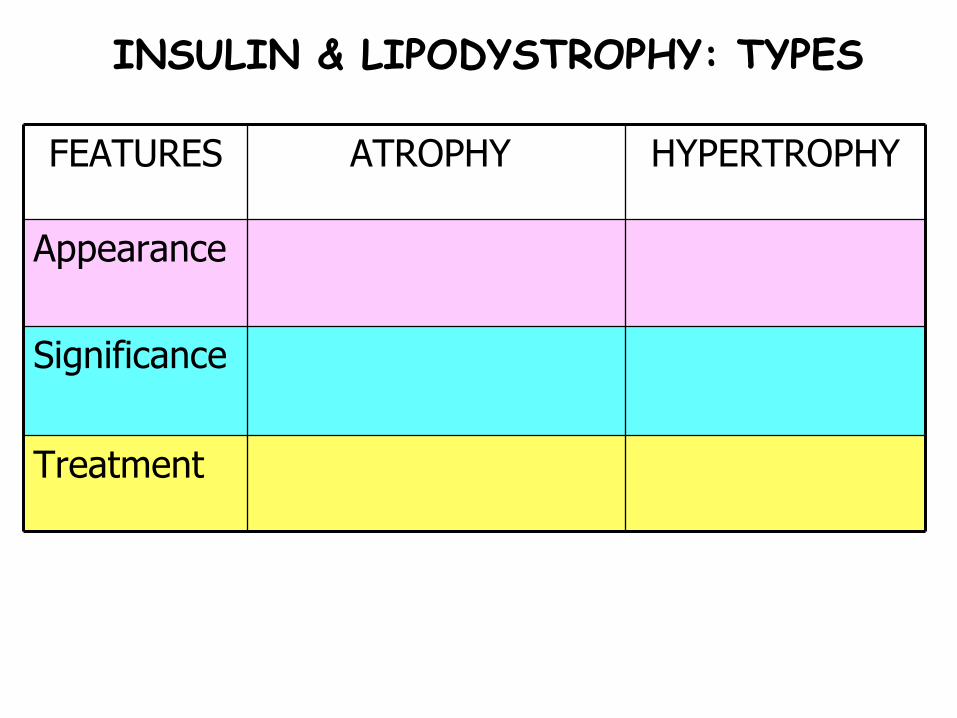
Significance
Appearance
HYPERTROPHYATROPHY FEATURES
INSULIN & LIPODYSTROPHY: TYPES

Rotate injection sites
Inject pure human insulin into atrophic area
Treatment
Impaired insulin absorption
Cosmetic only, physiologically harmless
Significance
Scar tissue at the injection site
Dimpling/ pitting at injection site
Appearance
HYPERTROPHYATROPHY FEATURES
INSULIN & LIPODYSTROPHY: TYPES
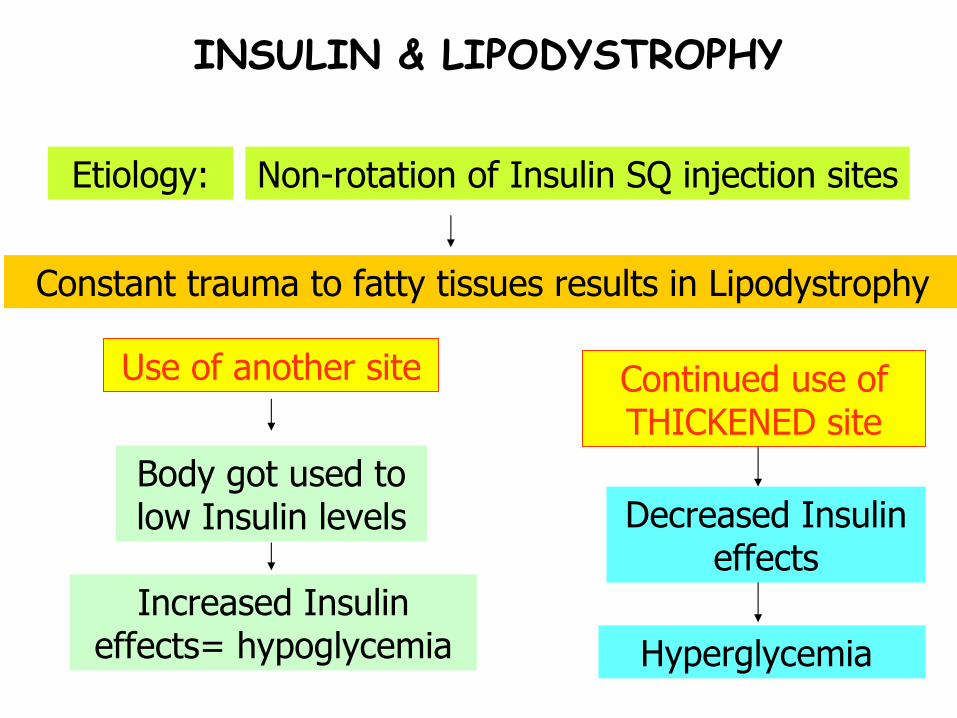
INSULIN & LIPODYSTROPHY
Non-rotation of Insulin SQ injection sites
Constant trauma to fatty tissues results in Lipodystrophy
Continued use of THICKENED site
Decreased Insulin effects
Hyperglycemia
Use of another site
Body got used to low Insulin levels
Increased Insulin effects= hypoglycemia
Etiology:
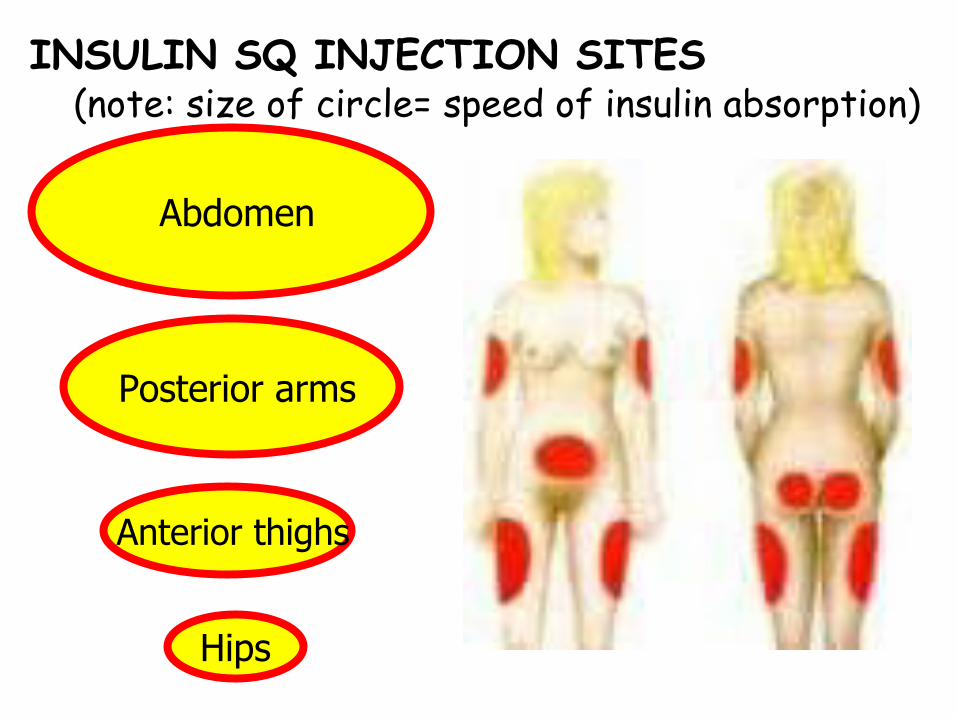
Abdomen
Anterior thighs
Hips
Posterior arms
INSULIN SQ INJECTION SITES (note: size of circle= speed of insulin absorption)

Trivia Time
How frequent should injection sites be rotated?
INSULIN SQ INJECTION SITES

INSULIN SQ INJECTION SITES
Trivia Time: ANSWER
Every 2-3 weeks
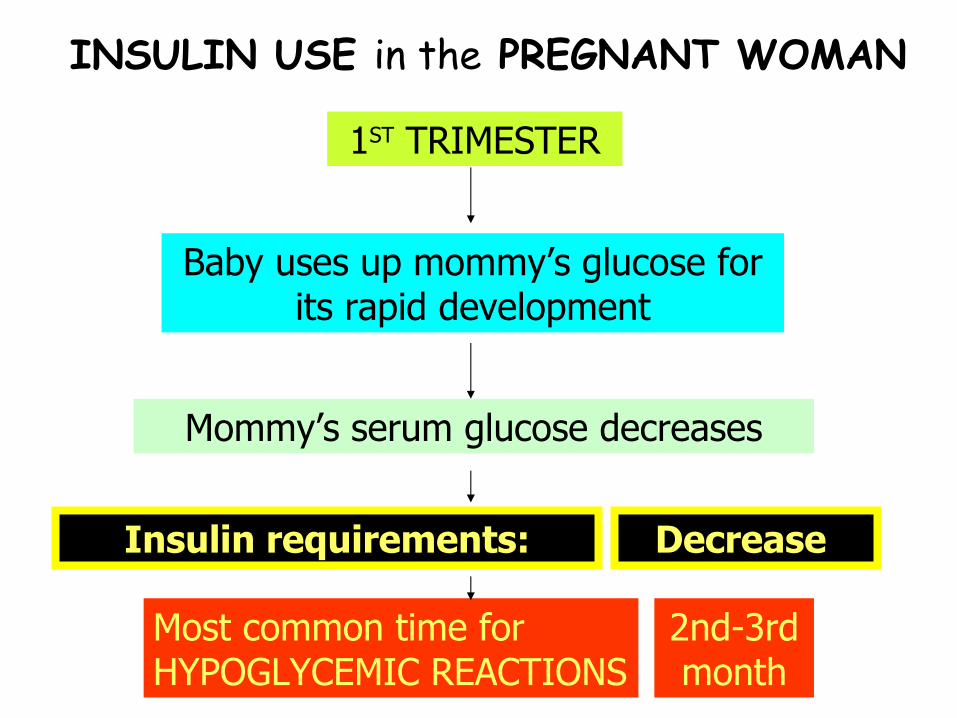
INSULIN USE in the PREGNANT WOMAN
1ST TRIMESTER
Baby uses up mommy’s glucose for its rapid development
Mommy’s serum glucose decreases
Insulin requirements:
Most common time for HYPOGLYCEMIC REACTIONS
Decrease
2nd-3rd month
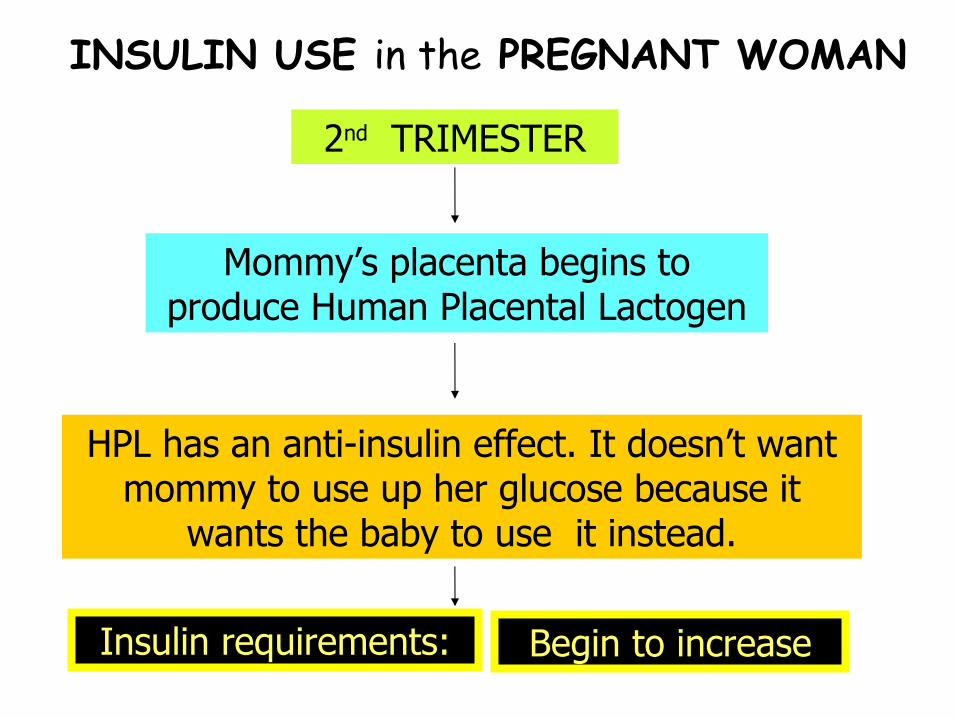
INSULIN USE in the PREGNANT WOMAN
2nd TRIMESTER
Mommy’s placenta begins to produce Human Placental Lactogen
HPL has an anti-insulin effect. It doesn’t want mommy to use up her glucose because it
wants the baby to use it instead.
Insulin requirements: Begin to increase

INSULIN USE in the PREGNANT WOMAN
3rd TRIMESTER
Mommy’s Placenta continues to produce HPL
High HPL levels significantly decrease Insulin’s effectivity
Insulin requirements:
Most common time for INSULIN RESISTANCE
Rise significantly
6th month
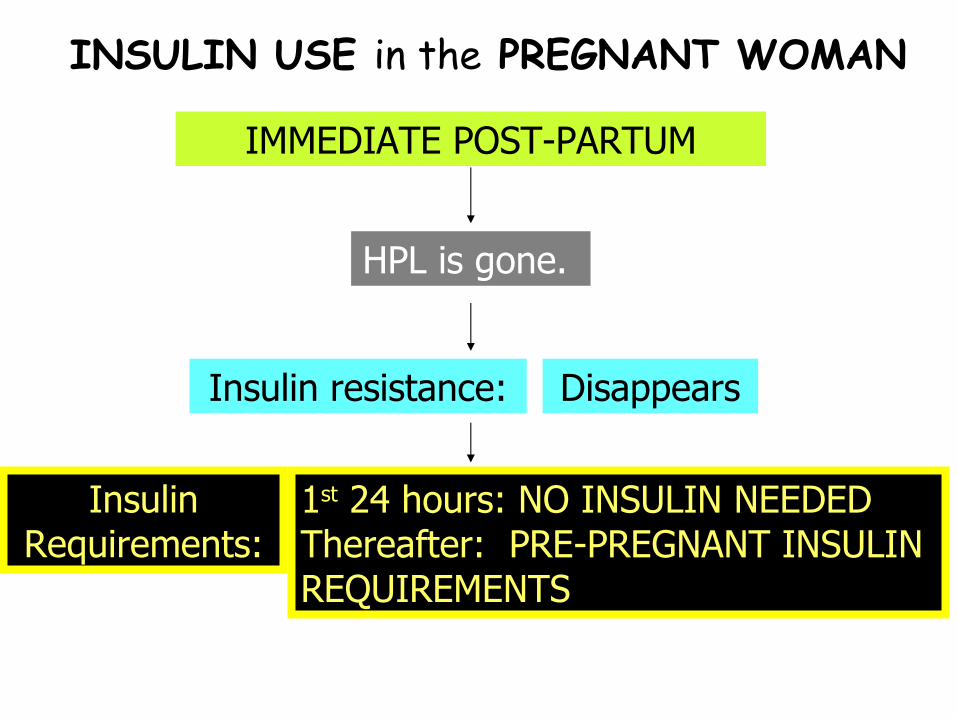
INSULIN USE in the PREGNANT WOMAN
IMMEDIATE POST-PARTUM
HPL is gone.
Insulin resistance:
Insulin Requirements:
Disappears
1st 24 hours: NO INSULIN NEEDED Thereafter: PRE-PREGNANT INSULIN REQUIREMENTS
ORAL HYPOGLYCEMICS

Why?
S/e to look out for:
Major suffix: -mide, -ride, -zide
Anorexia
It may potentiate hypoglycemia
Pregnancy alert:
Oral hypoglycemics are teratogenic!
SULFONYLUREAS
Vital facts:
SULFONYLUREASCommon names:
• *Chlorpropamide(Diabinese)
• Tolbutamide (Orinase)
• Glimepiride (Amaryl)
• Glipizide (Glucotrol)
• Glyburide (DiaBeta)
First Generation
Second Generation
2nd:
1st: Urine
Urine & bile
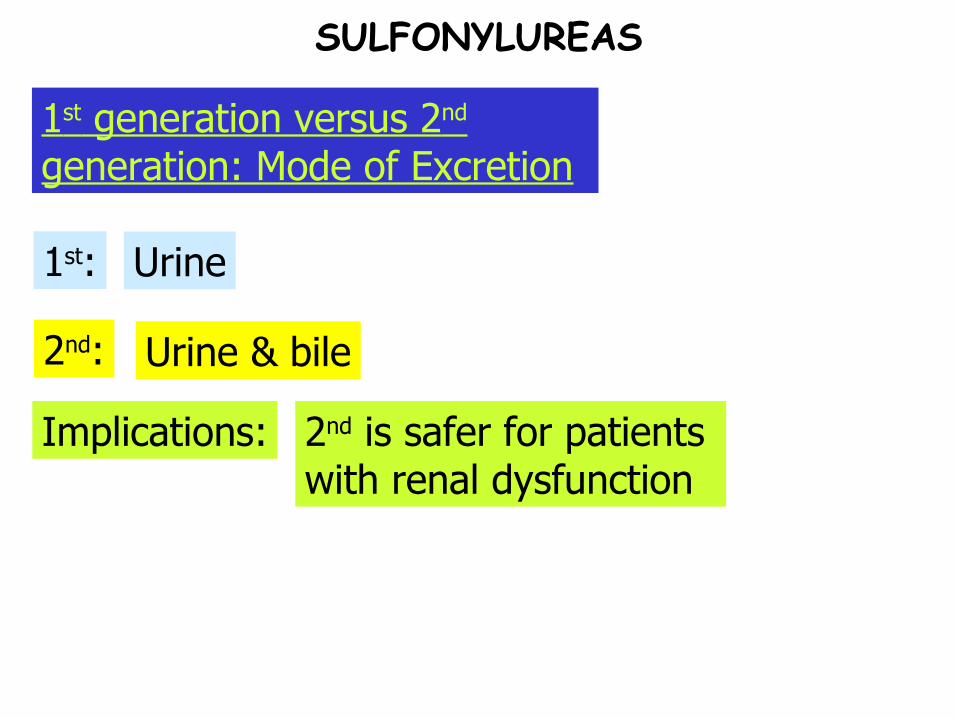
SULFONYLUREAS
1 st generation versus 2 nd generation: Mode of Excretion
Implications: 2nd is safer for patients with renal dysfunction
2nd:
1st: Shorter
Longer (1-2x/day dosing)
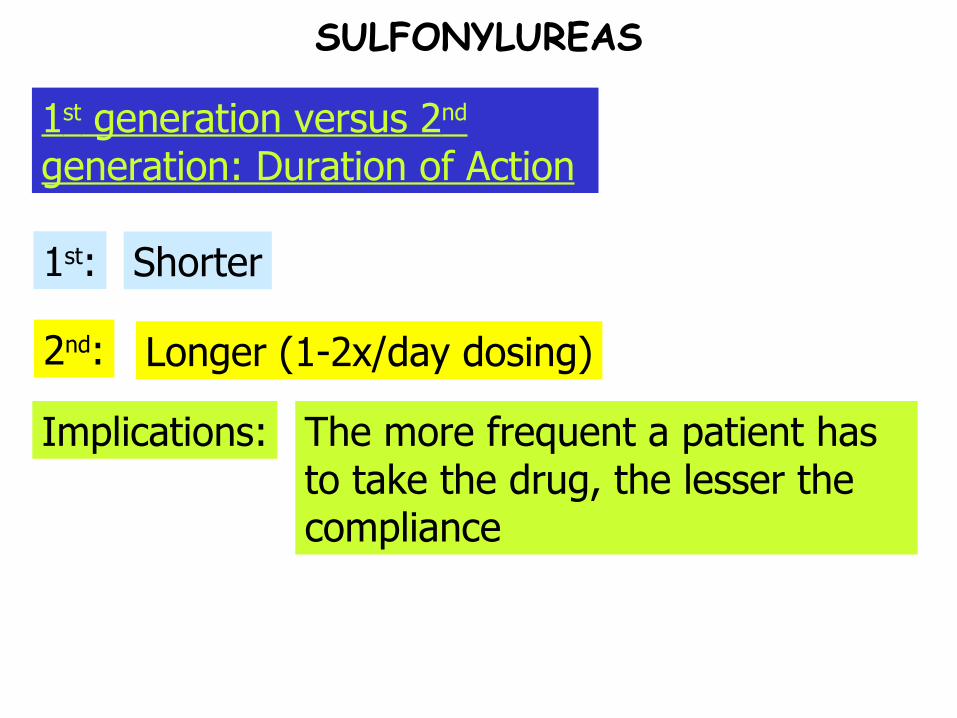
SULFONYLUREAS
1 st generation versus 2 nd generation: Duration of Action
Implications: The more frequent a patient has to take the drug, the lesser the compliance

2nd:
1st: High
Low
SULFONYLUREAS
1 st generation versus 2 nd generation: Cardiovascular disease risk

Stimulate beta cells to produce Insulin
Increase the number of insulin receptors
Improve Insulin binding to insulin receptors
Insulin levels rise
Glucose deposited into the cells
SULFONYLUREAS
Hypoglycemic effect
Action:
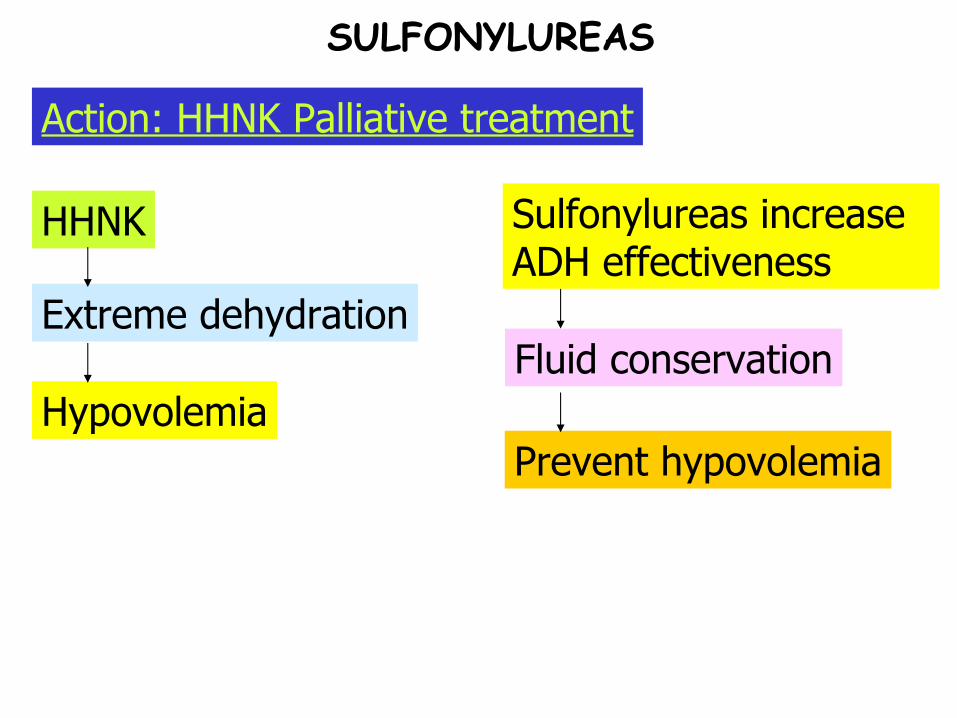
Hypovolemia
Extreme dehydration
HHNK
Prevent hypovolemia
Fluid conservation
SULFONYLUREAS
Action: HHNK Palliative treatment
Sulfonylureas increase ADH effectiveness

So what if it’s short?
Half-life:
Major suffix: -glinide
Very short
Lesser hypoglycemic effect
Indication: Adjuncts to sulfonylureas
MEGLITINIDES
Vital facts:
MEGLITINIDESCommon names:
• Nateglinide (Starlix)
• Repaglinide (Prandin)
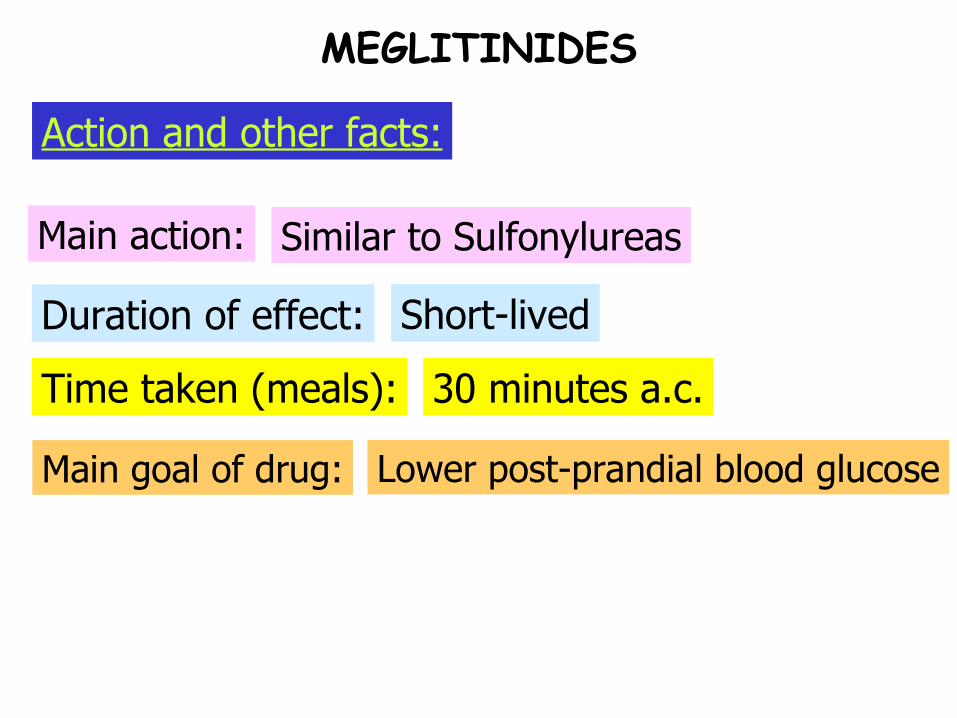
Time taken (meals):
Duration of effect:
Main action: Similar to Sulfonylureas
Short-lived
30 minutes a.c.
Main goal of drug: Lower post-prandial blood glucose
MEGLITINIDES
Action and other facts:
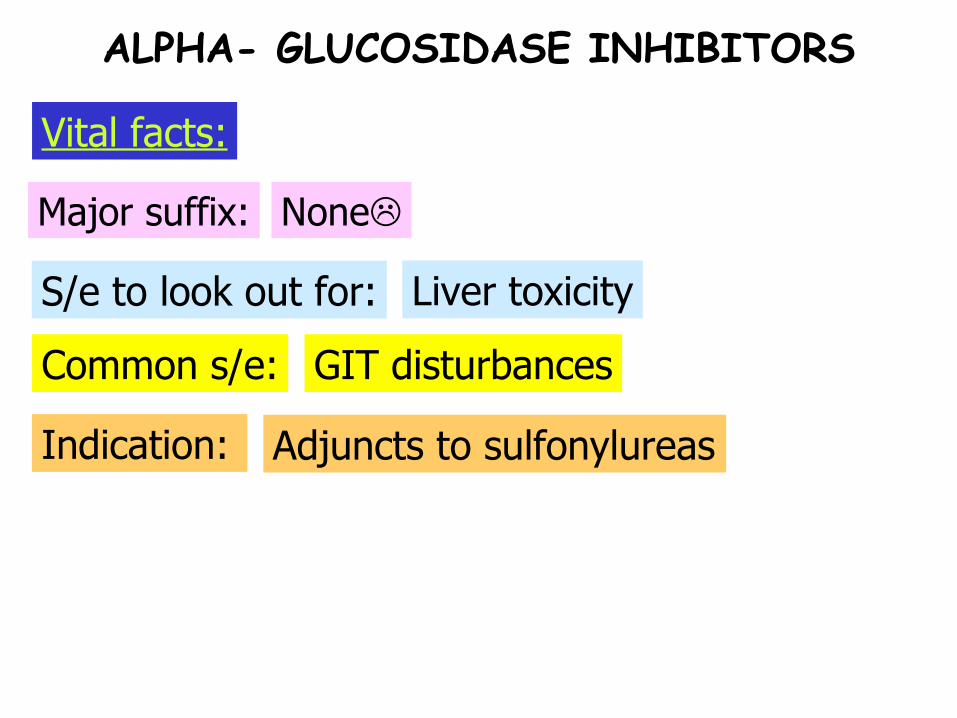
Common s/e:
S/e to look out for:
Major suffix: None
Liver toxicity
GIT disturbances
Indication: Adjuncts to sulfonylureas
ALPHA- GLUCOSIDASE INHIBITORS
Vital facts:

ALPHA- GLUCOSIDASE INHIBITORS.
Common names:
• Acarbose (Precose)
• Miglitol (Glyset)

ALPHA- GLUCOSIDASE INHIBITORS
Alpha- glucosidase inhibition
Delayed glucose absorption from GIT into blood
Mild hypoglycemic effects
Adjunct to Sulfonylureas
Temporary prevention of complex Carbohydrates breakdown
Decreased hyperglycemia after eating
Action:
Common s/e:
S/e to look out for:
Major suffix: None
Liver toxicity
GIT disturbances
Indication: Adjuncts to sulfonylureas
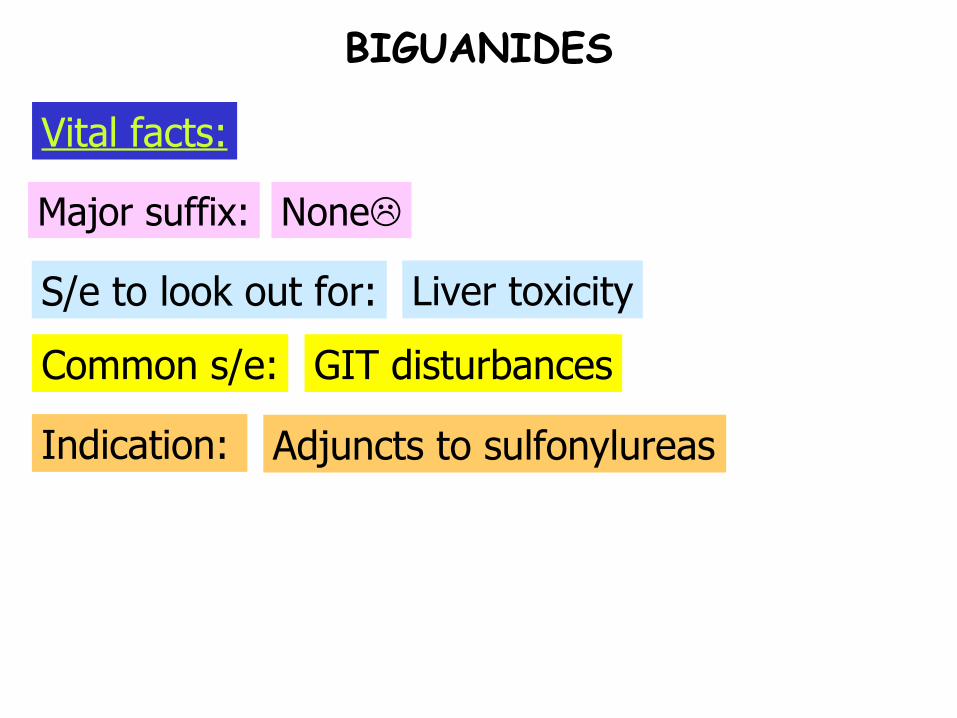
BIGUANIDES
Vital facts:

BIGUANIDESExample:
• Metformin (Glucophage)
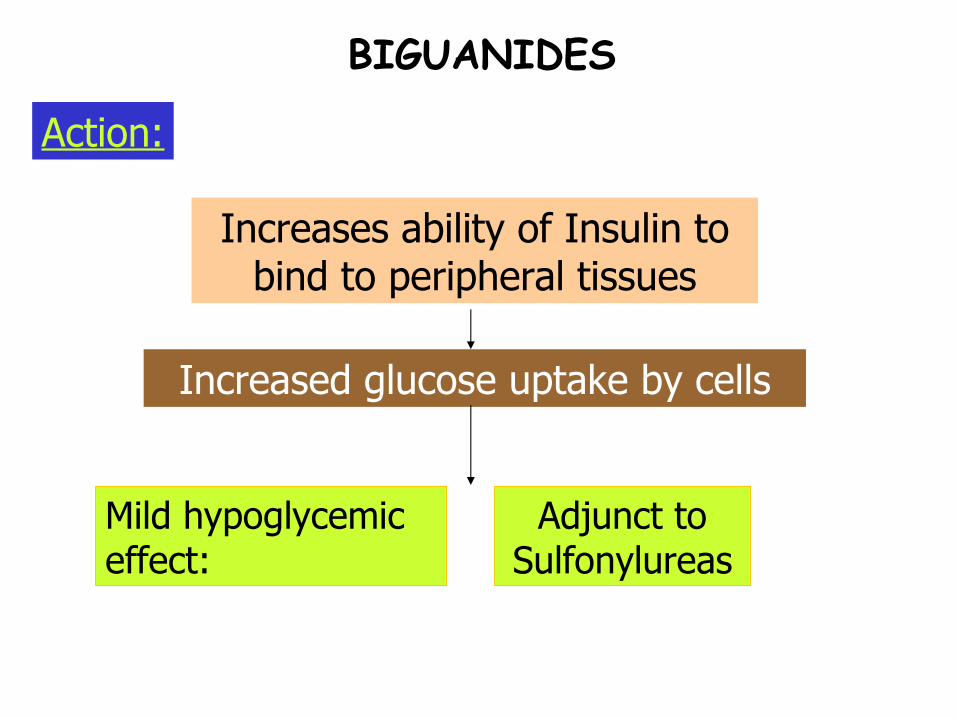
BIGUANIDES
Increases ability of Insulin to bind to peripheral tissues
Increased glucose uptake by cells
Mild hypoglycemic effect:
Adjunct to Sulfonylureas
Action:

Trivia Time
What acid-base imbalance could occur with the intake of Biguanides?
BIGUANIDES
Trivia Time: ANSWER
Lactic acidosis
BIGUANIDES

S/e #2:
S/e #1:
Major suffix: -glitazone
Fluid retention edema
Hepatotoxicity Jaundice
Indication: Adjuncts to sulfonylureas
THIAZOLIDINEDIONES
Vital facts:
THIAZOLIDINEDIONESCommon names:
• Pioglitazone (Actos)
• Rosiglitazone (Avandia)
THIAZOLIDINEDIONES
Decreases peripheral resistance to Insulin
Increased glucose uptake by cells
Mild hypoglycemic effects
Action:
ANTI-HYPOGLYCEMICSMajor Suffix: none
Major considerations:
Common names:
• Dextrose (Glucose, Glutose, Insta-glucose)
• Diazoxide (Proglycem)
• Glucagon (Glucogen)
• Octreotide (Sandostatin)
Each medication has its own unique way of working and also has its own set of side-effects.

DIAZOXIDE
Diazoxide as a Vasodilator:
Venous stasis:
Dependent edema = weight gain
Low Venous return = Hypotension
blood pools in veins

DIAZOXIDE
Inhibits B-cells from producing Insulin: Anti-sulfonylurea
Increase peripheral insulin resistance
Reduced Insulin action
Hyperglycemic effect
Diazoxide as an anti-hypoglycemic agent:
DEXTROSE
LOW DOSE:
Purpose:
Risk for irritation at IV site:
10% glucose maximum
Nutrition/ hydration
Low risk for irritation at IV site
Dextrose @ low doses:

DEXTROSE
HIGH DOSE:
Purpose:
Risk for irritation at IV site:
70% glucose maximum
Treatment of Hypoglycemia
High risk for irritation at IV site
Dextrose @ low doses:
Sample Question:
The nurse teaches a type 2 DM client how to recognize and report adverse drug reactions. Which of the following is a common adverse reaction to Glipizide?
a. Headache
b. Constipation
c. Hypotension
d. Photosensitivity
ORAL HYPOGLYCEMICS
HYPOGLYCEMIA

Tachycardia, sweating, tremors, nervousness, hunger
Think of Sx when you feel extremely hungry
SNS stimulation
Hypoglycemic reaction:
High insulin but low glucose intake
HYPOGLYCEMIA: SIMPLE PATHOPHYSIOLOGY
Blood glucose < 60 mg/dl
HYPOGLYCEMIA
Trivia Time
What may be the only sign of hypoglycemia in an unconscious person?

Trivia Time: ANSWER
Diaphoresis
HYPOGLYCEMIA

Brain is depleted of glucose
Hypoglycemic coma
HYPOGLYCEMIA: SIMPLE PATHOPHYSIOLOGY
Brain damage: paralysis, cognitive impairment
Dangers of Hypoglycemia:
Inadequate glucose to support brain activity
Trivia Time
Between a DKA coma and Hypoglycemic coma, which one is
more serious and why?
HYPOGLYCEMIA
Trivia Time: ANSWER
Hypoglycemic coma
HYPOGLYCEMIA
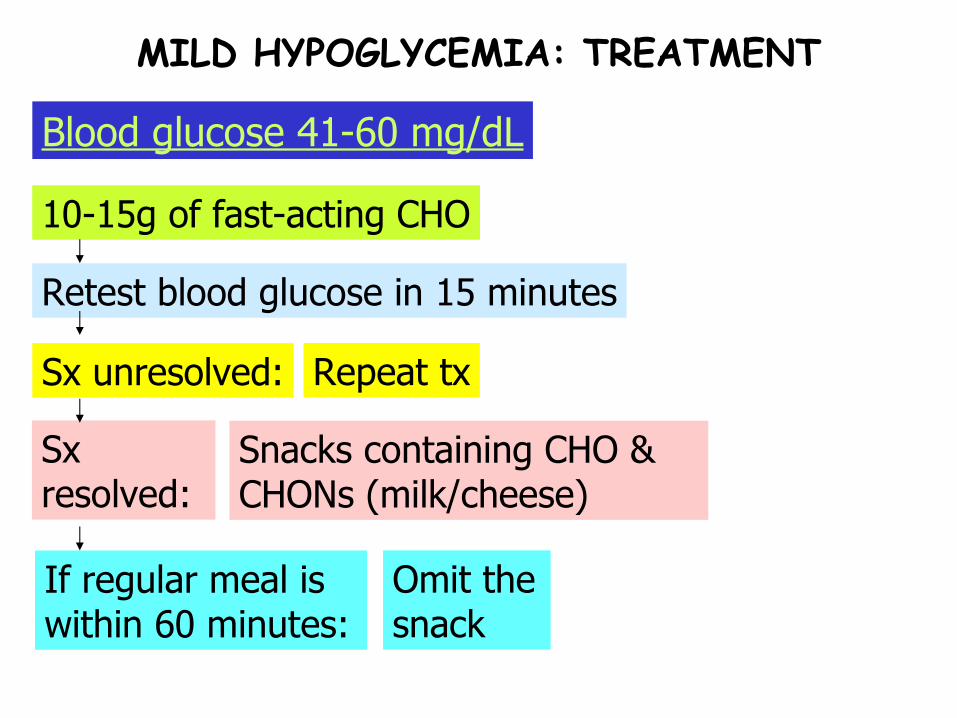
Sx resolved:
If regular meal is within 60 minutes:
Sx unresolved:
Retest blood glucose in 15 minutes
10-15g of fast-acting CHO
Blood glucose 41-60 mg/dL
MILD HYPOGLYCEMIA: TREATMENT
Repeat tx
Snacks containing CHO & CHONs (milk/cheese)
Omit the snack
Same with Mild Hypoglycemia
Blood glucose 21-40 mg/dL
MODERATE HYPOGLYCEMIA: TREATMENT

Upon arrival @ hospital:
Once conscious:
Still unconscious after ten minutes:
Unconscious:
Blood glucose 20 mg/dL below
SEVERE HYPOGLYCEMIA: TREATMENT
SQ/ IM Glucagon
2nd dose of Glucagon
Give small meal
Give IV 25-50 mL of Dextrose 50% in water
A client is taking NPH insulin every morning. The nurse instructs the client that the most likely time for a hypoglycemic reaction to occur is:
a. 2-4 hours after administration
b. 6-14 hours after administration
c. 16-18 hours after administration
d. 18-24 hours after administration
PRACTICE QUESTIONS
A client is brought to the ER in an unresponsive state, and a diagnosis of HHNK is made. The nurse would prepare immediately to initiate which of the following anticipated physician orders?
a. 100 units of NPH insulin
b. Endotracheal intubation
c. IV replacement of Sodium Bicarbonate
d. IV infusion of Normal Saline
PRACTICE QUESTIONS
A client is admitted with a diagnosis of DKA. The initial blood glucose level was 950 mg/dL. A continuous IV infusion of regular insulin is initiated along with intravenous rehydration with normal saline. The serum glucose level is now 240 mg/ dL. The nurse would next prepare to administer which of the following?
a. IV fluids containing 5% dextrose
b. NPH insulin SQ
c. An ampule of 50% dextrose
d. Phenytoin for seizure prevention
PRACTICE QUESTIONS
A client with DM visits a health care clinic. The client’s DM previously had been well controlled with glyburide (Diabeta), 5mg PO daily, but recently the fasting blood glucose has been running to 180-200 mg/dl. Which medication ,if added to the client’s regimen, may have contributed to the hyperglycemia?
a. Prednisone (Deltasone)
b. Atenolol (Tenormin)
c. Phenelzine (Nardil)
d. Allopurinol (Zyloprim)
PRACTICE QUESTIONS
If NPH insulin has been injected SQ at 6:00 am, the client would be assessed for any hypoglycemic reaction at:
a. 12NN to 2:00 pm
b. 6:00am the following day
c. 8:00am -10:00 am
d. 1:00 pm – 7:00pm
PRACTICE QUESTIONS

Oxygen Therapy
Anemic hypoxia:
Circulatory hypoxia:
Hypoxemic hypoxia:
Indication: Hypoxia
OXYGEN THERAPY
VP imbalances, Hypoventilation
Cardiogenic shock
Anemia
Histotoxic hypoxia: CO, Cyanide poisoning

25-50
90 above
60-90
40-60
20-40
O2 %(FiO2)
Oxygen Tent
5-10Venturi Mask
6-15Non- Rebreather
6-15Partial Rebreather
6-8Face Mask
2-6Nasal Cannula
LPMDELIVERY SYSTEM
OXYGEN THERAPY
Low Flow Systems High Flow Systems
Non-constant O2% delivered
Contributes partially to the gas the patient breathes
Oxygen is delivered independent of the pt’s. breathing
Constant O2%
FiO2 varies with pt’s breathing Constant FiO2
e.g. :Face mask T-piece, Tracheostomy collars
Low-Flow vs. High Flow Systems
OXYGEN THERAPY
LPM% of O2 (FiO2)
Mnemonic: 24 hours in 1 day
OXYGEN THERAPY (% of O2 DELIVERED : LPM)

540
436
332
228
124
LPM% of O2 (FiO2)
Mnemonic: 24 hours in 1 day
OXYGEN THERAPY (% of O2 DELIVERED : LPM)

True or false:
Oxygen is a medication. Hence, it must be prescribed by a physician.
There is no danger of fire when oxygen is used since it is contained in a green tank
Oxygen administration may be done at the client’s home.
There is no such thing as oxygen toxicity
OXYGEN THERAPY
Build-up of oxygen free radicals
Cells metabolize oxygen
O2 > 50% for more than 48 hours
Oxygen toxicity:
Free radicals can damage/ kill cells
OXYGEN THERAPY
Signs and Symptoms:
Why?
Ideal diet: Rich in Vitamin E, C & Beta-Carotene
It’s rich on anti-oxidants
Oxygen toxicity:
OXYGEN THERAPY
Substernal discomfort
Dyspnea & Fatigue
X-ray: Alveolar infiltrates
Progressive Resp.
Difficulty
OXYGEN THERAPY
Nasal cannula

OXYGEN THERAPY
Skin integrity alert:
Duration of use:
Recommended LPM:
Nasal cannula
Water-soluble jelly to nares as needed
Long-term use
Flow rates higher than 6 LPM are useless.
OXYGEN THERAPY
Consequence of flow rates>6-8lpm:
Nasal cannula
Air swallowing, mucosa drying

OXYGEN THERAPY
Face mask

OXYGEN THERAPY
Recommended LPM:
Safety alert:
Limitations:
Face mask
Minimum of 5 LPM to prevent rebreathing of exhaled air
Watch for aspiration
Limited ability to clear mouth
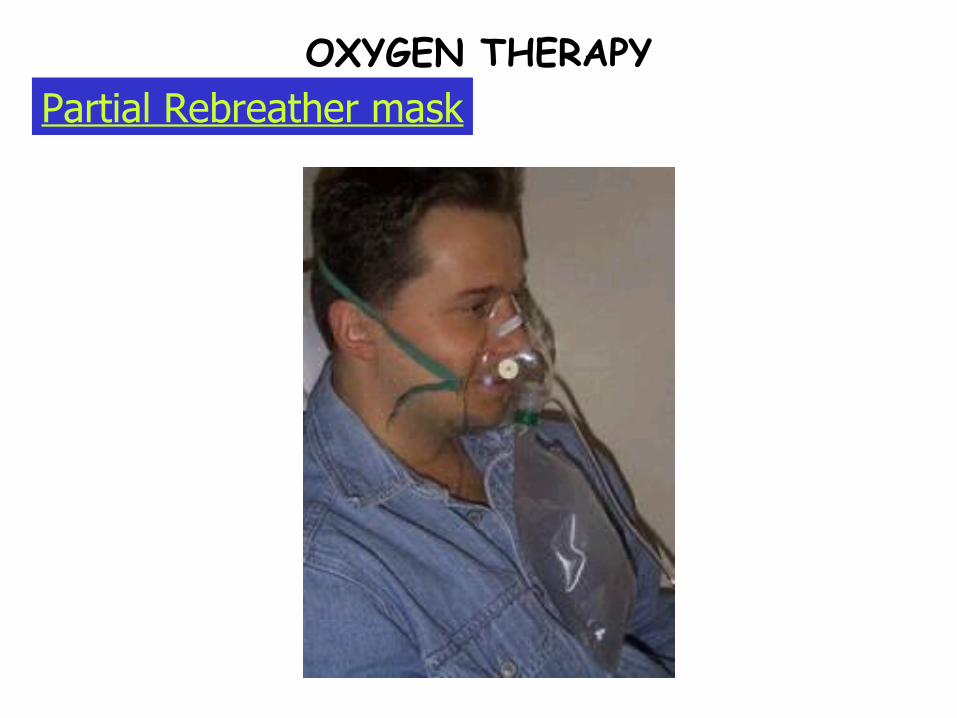
Partial Rebreather maskOXYGEN THERAPY

Why rebreathe?
Mechanism:
Partial Rebreather maskOXYGEN THERAPY
1/3 of exhaled tidal volume is rebreathed.
Such air is O2 rich.
The initial 1/3 exhaled air was mainly
the dead space
Deflation means :
Safety alert!
Partial Rebreather maskOXYGEN THERAPY
R.B. must be 2/3 full with inhalation
Deflation means decreased O2 delivered.
Reservoir bag must not deflate completely!
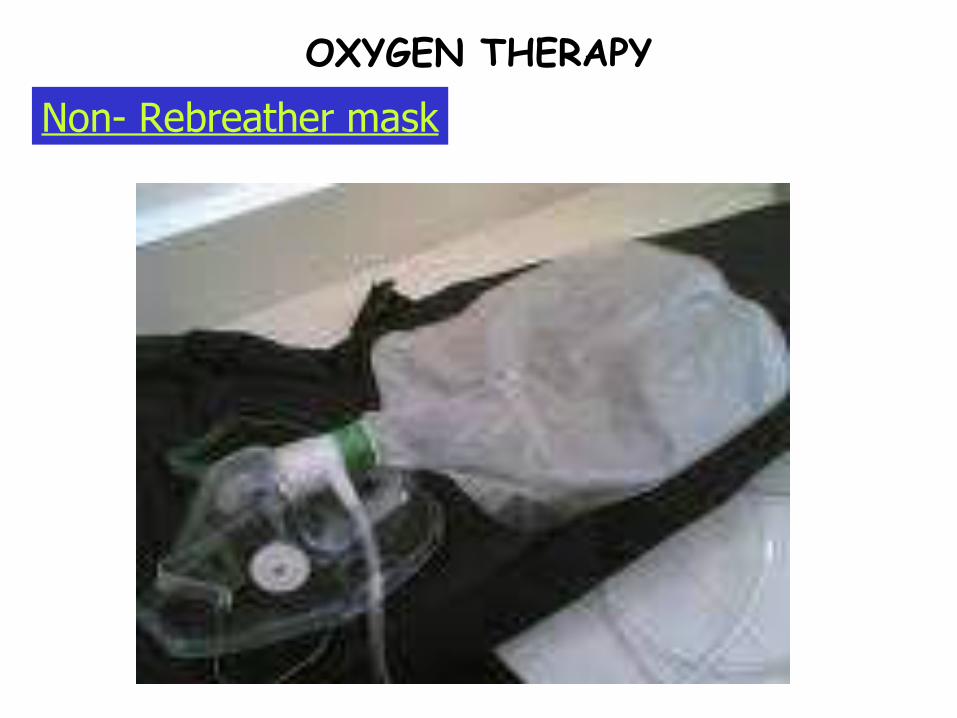
OXYGEN THERAPY
Non- Rebreather mask

OXYGEN THERAPY
Guidelines:
Air inhaled:
O2 delivered:
Non- Rebreather mask
Bag deflation consequence:
Same guidelines with partial rebreather masks
Only Pure O2 is inhaled
Highest amount of O2 delivered
Suffocation can result with bag deflation
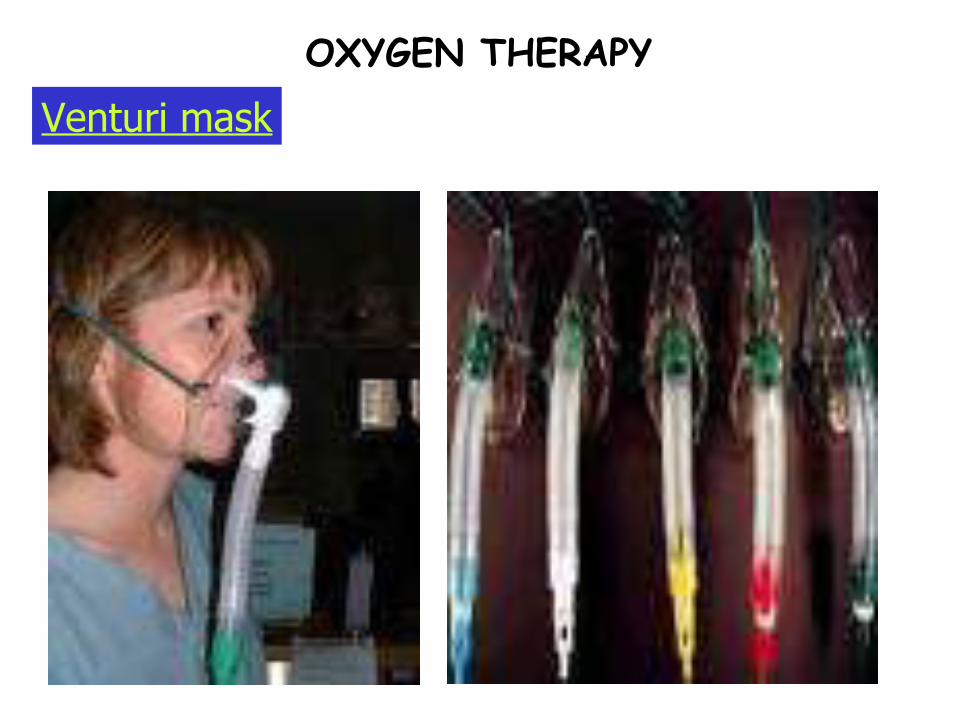
OXYGEN THERAPY
Venturi mask
OXYGEN THERAPY
Mechanism:
Oxygen delivery:
Venturi mask
Exact proportion of room air + o2 is inhaled
Most accurate oxygen delivery system
The oxygen administration device preferred for patients with COPD is:
a. Nasal cannula
b. Oxygen tent
c. Venturi mask
d. Oxygen hood
PRACTICE QUESTIONS

Which of the following is not to be included in the nursing interventions for a client receiving oxygen therapy?
a. Place a “No Smoking” sign at the bedside
b. Place the client in semi-fowler’s position
c. Place sterile water into the oxygen humidifier
d. Lubricate the nares with oil to prevent dryness of the mucous membrane
PRACTICE QUESTIONS

Which of the following is the most accurate oxygen delivery system?
a. Nasal cannula
b. Oxygen tent
c. Venturi mask
d. Oxygen hood
PRACTICE QUESTIONS
Which of the following oxygen delivery system would be ideal to use in someone who has just been diagnosed with CO poisoning?
a. Nasal cannula
b. Oxygen tent
c. Venturi mask
d. Non-rebreather face mask
PRACTICE QUESTIONS
After exposure in the clinical area, you know that the color of the oxygen tank is:
a. Gray
b. Blue
c. Green
d. Light pink
PRACTICE QUESTIONS

Blood Transfusion
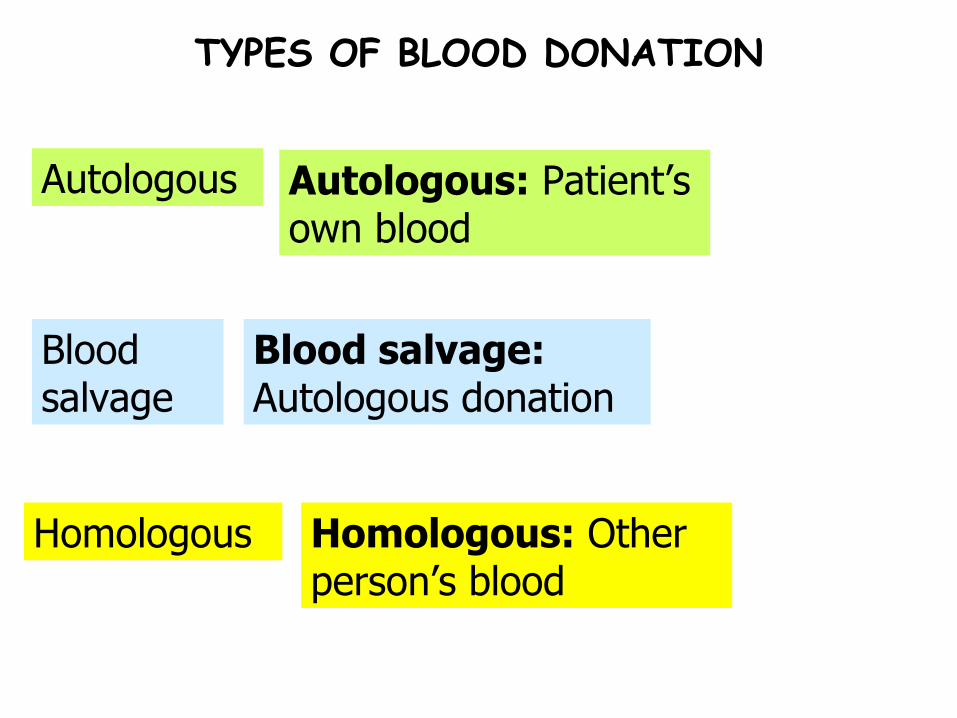
TYPES OF BLOOD DONATION
Homologous
Blood salvage
Autologous
Homologous: Other person’s blood
Blood salvage: Autologous donation
Autologous: Patient’s own blood

Plasmapheresis
Stem Cell harvest
Erythrocyta-pheresis
Leukapheresis
Platelet pheresis
PURPOSE: to remove…TYPE
TYPES OF APHERESIS
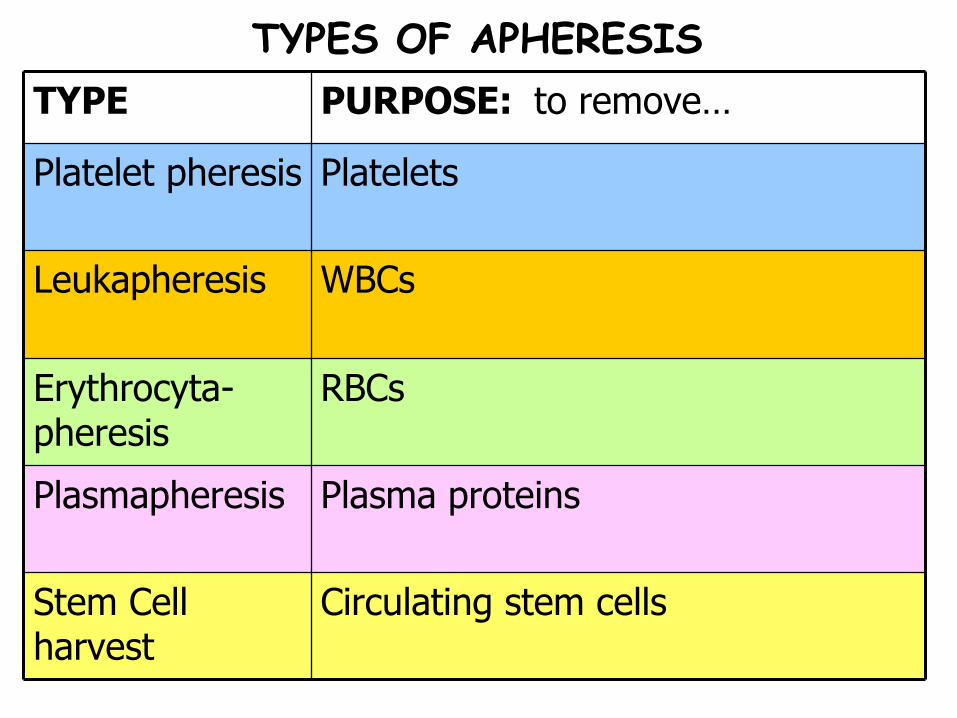
Plasma proteinsPlasmapheresis
Circulating stem cellsStem Cell harvest
RBCsErythrocyta-pheresis
WBCsLeukapheresis
PlateletsPlatelet pheresis
PURPOSE: to remove…TYPE
TYPES OF APHERESIS

Single donor plateletsFresh Frozen Plasma
Random platelets
Packed RBCs
Whole blood
INDICATION/SCOMPOSITIONTYPE
BLOOD/ BLOOD COMPONENTS
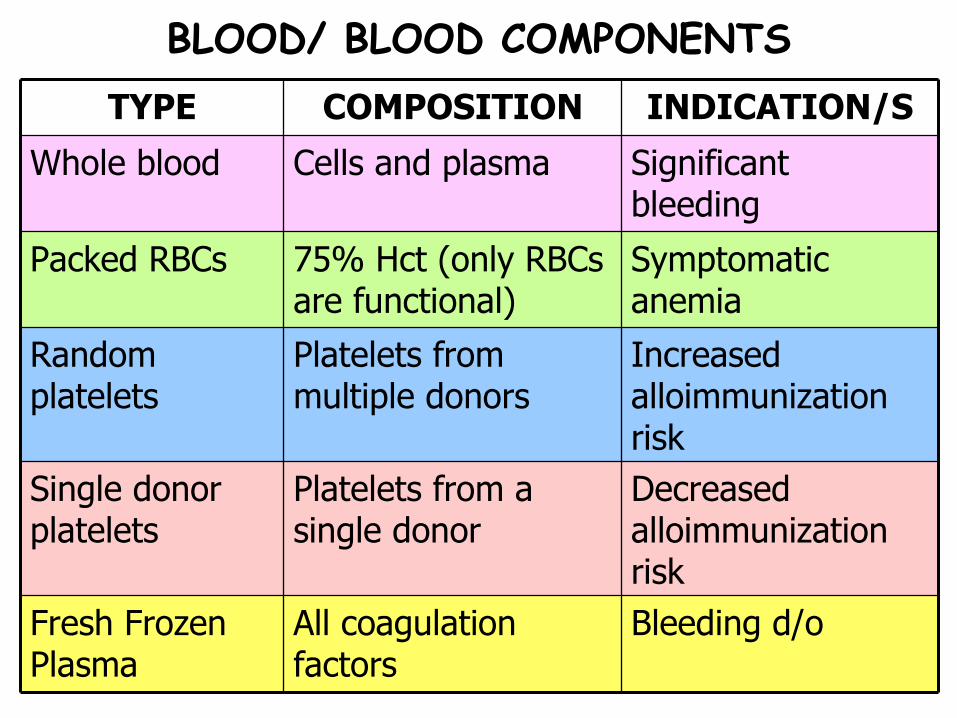
Decreased alloimmunization risk
Platelets from a single donor
Single donor platelets
Bleeding d/oAll coagulation factors
Fresh Frozen Plasma
Increased alloimmunization risk
Platelets from multiple donors
Random platelets
Symptomatic anemia
75% Hct (only RBCs are functional)
Packed RBCs
Significant bleeding
Cells and plasmaWhole blood
INDICATION/SCOMPOSITIONTYPE
BLOOD/ BLOOD COMPONENTS

Albumin
Cryoprecipitate
INDICATION/SCOMPOSITIONTYPE
BLOOD/ BLOOD COMPONENTS
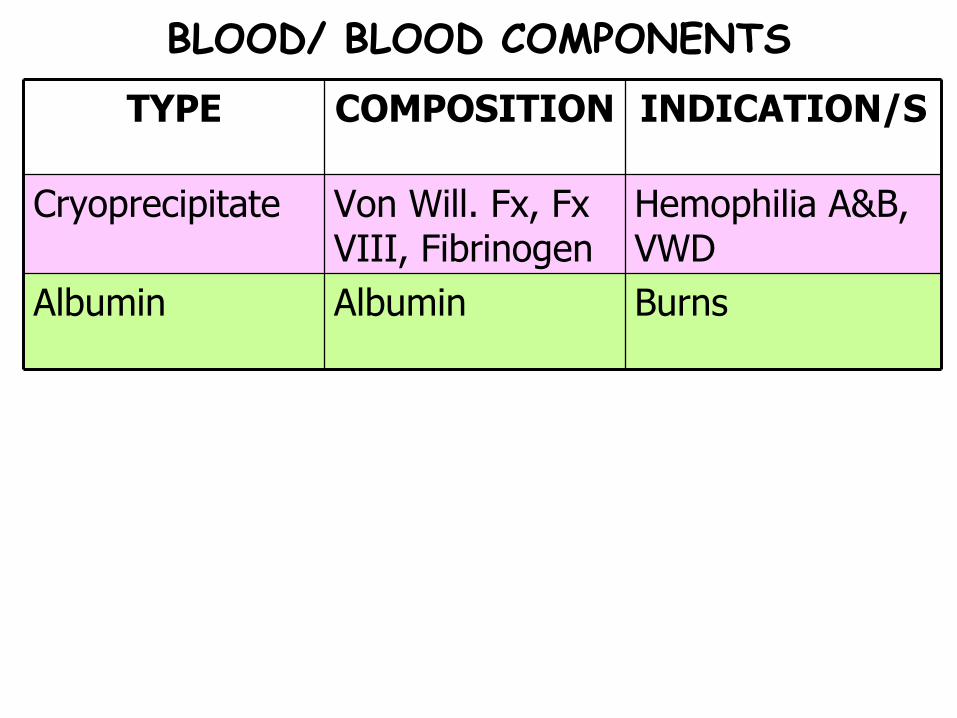
Burns AlbuminAlbumin
Hemophilia A&B, VWD
Von Will. Fx, Fx VIII, Fibrinogen
Cryoprecipitate
INDICATION/SCOMPOSITIONTYPE
BLOOD/ BLOOD COMPONENTS

Blood Components
A single unit of whole blood contains ___ ml and __ ml of an anticoagulant.
PRBCs are stored at __ degrees Celsius and can be stored up to ___ days with special preservatives.
Platelets must be stored at ____ temperature and can last only __ day/s.
To prevent clumping, platelets are gently _______ while stored.
Fresh frozen plasma can last up to __ year/s as long as it remains ______.
BLOOD/ BLOOD COMPONENTS
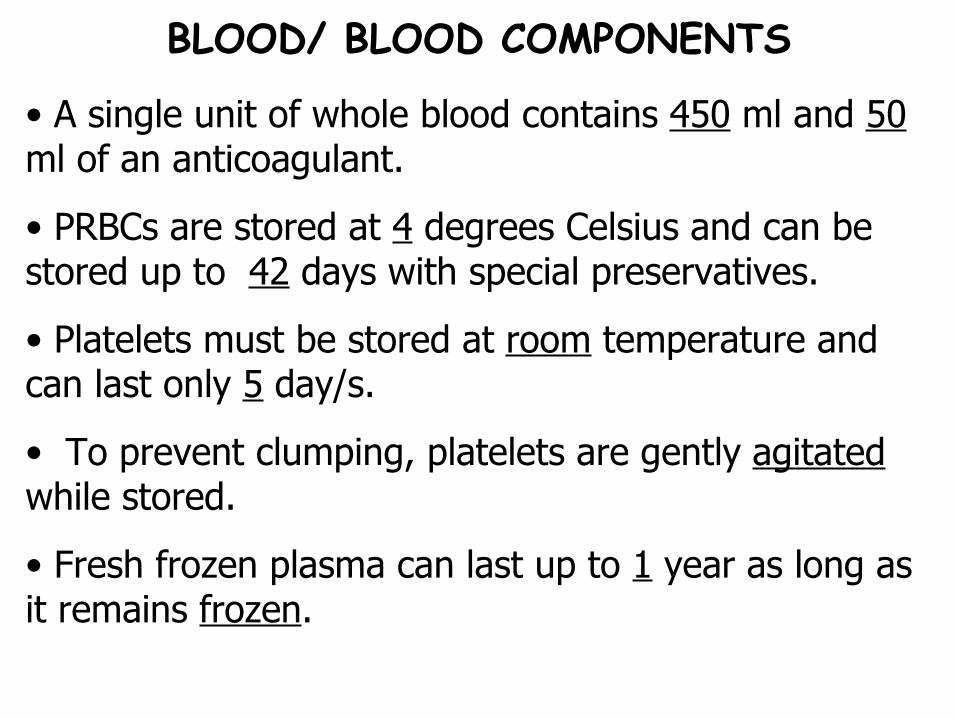
• A single unit of whole blood contains 450 ml and 50 ml of an anticoagulant.
• PRBCs are stored at 4 degrees Celsius and can be stored up to 42 days with special preservatives.
• Platelets must be stored at room temperature and can last only 5 day/s.
• To prevent clumping, platelets are gently agitated while stored.
• Fresh frozen plasma can last up to 1 year as long as it remains frozen.
BLOOD/ BLOOD COMPONENTS
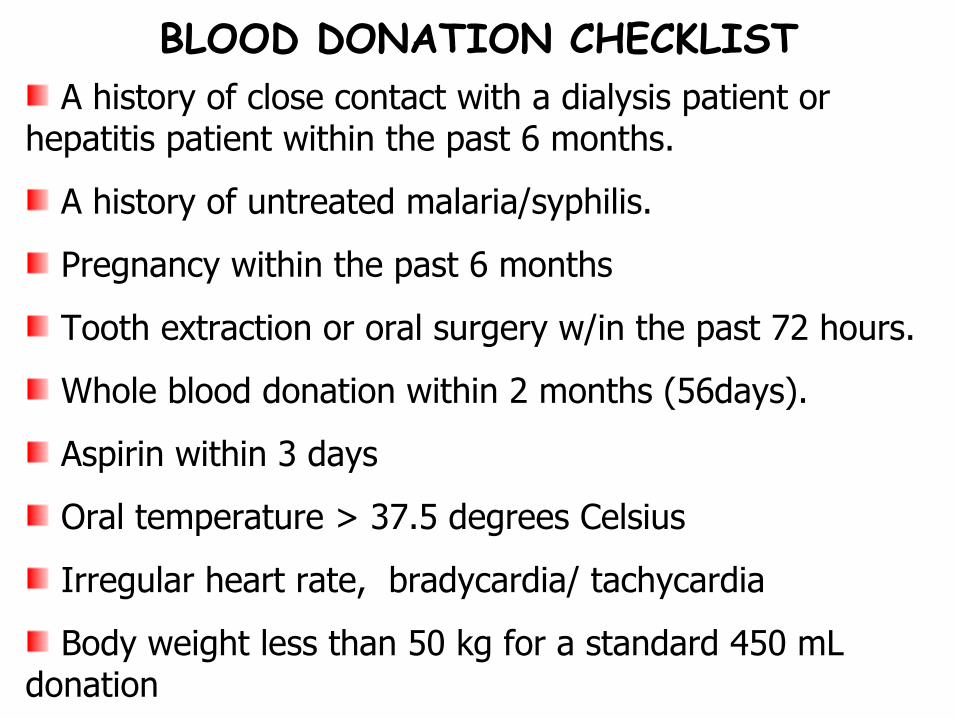
A history of close contact with a dialysis patient or hepatitis patient within the past 6 months.
A history of untreated malaria/syphilis.
Pregnancy within the past 6 months
Tooth extraction or oral surgery w/in the past 72 hours.
Whole blood donation within 2 months (56days).
Aspirin within 3 days
Oral temperature > 37.5 degrees Celsius
Irregular heart rate, bradycardia/ tachycardia
Body weight less than 50 kg for a standard 450 mL donation
BLOOD DONATION CHECKLIST
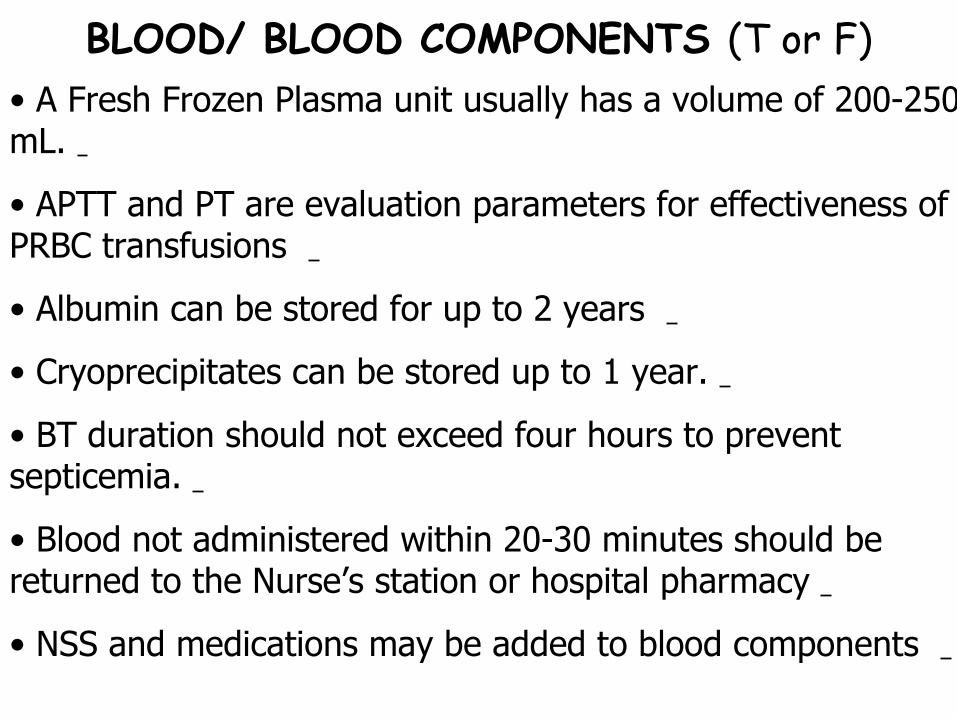
• A Fresh Frozen Plasma unit usually has a volume of 200-250 mL.
• APTT and PT are evaluation parameters for effectiveness of PRBC transfusions
• Albumin can be stored for up to 2 years
• Cryoprecipitates can be stored up to 1 year.
• BT duration should not exceed four hours to prevent septicemia.
• Blood not administered within 20-30 minutes should be returned to the Nurse’s station or hospital pharmacy
• NSS and medications may be added to blood components
BLOOD/ BLOOD COMPONENTS (T or F)
• A Fresh Frozen Plasma unit usually has a volume of 200-250 mL. T
• APTT and PT are evaluation parameters for effectiveness of PRBC transfusions. F: Fresh Frozen Plasma(APTT and PT)
• Albumin can be stored for up to 2 years. F: 5 years
• Cryoprecipitates can be stored up to 1 year. T
• BT duration should not exceed four hours to prevent septicemia. T
• Blood not administered within 20-30 minutes should be returned to the Nurse’s station or hospital pharmacy. F: Blood bank
• NSS and medications may be added to blood components. F: only NSS may be added if blood is highly viscous
BLOOD/ BLOOD COMPONENTS (T or F)

3. Baseline data:
2. Lab results:
1. Doc’s Order
Cross-matching and Blood typing
Vital signs
4. At least 2 nurses should check:
Serial number, BT, Rh factor, Expiry date, Screening tests (VDRL & HBsAg)
The Procedure:
BLOOD TRANSFUSION
7. Initial BT rate:
6. Needle gauge & filter:
5. Warm blood to room temp:
Gauge 18
10 gtts/ min for 15-20 mins
8. Duration (Whole blood, Packed RBC): 4 hours
20 mins.
The Procedure:
BLOOD TRANSFUSION
Rewarmer/ towel
8. Duration (platelets, cryoprecipitates):
Can I stop the BT in the presence of an adverse reaction?
Can I give dextrose with the BT?
Can I mix medications with the BT? No
No -- hemolysis
Yes
Drill Questions:
BLOOD TRANSFUSION
3. Collect!
2. Start!
1. Stop! Stop the BT
Start an IV line (0.9% NaCl)
Collect urine specimen
4. Monitor! Monitor V/S
5. Send! Send unused blood and set to blood bank
Transfusion reaction guidelines:
BLOOD TRANSFUSION
7. Document!
6. Administer!
Antihistamines, diuretics, bronchodilators
Transfusion reaction guidelines:
BLOOD TRANSFUSION

Sx
Allergic
Acute Hemolytic
Febrile, Non-Hemolytic
TxETIOLOGYTYPE
TRANSFUSION COMPLICATIONS
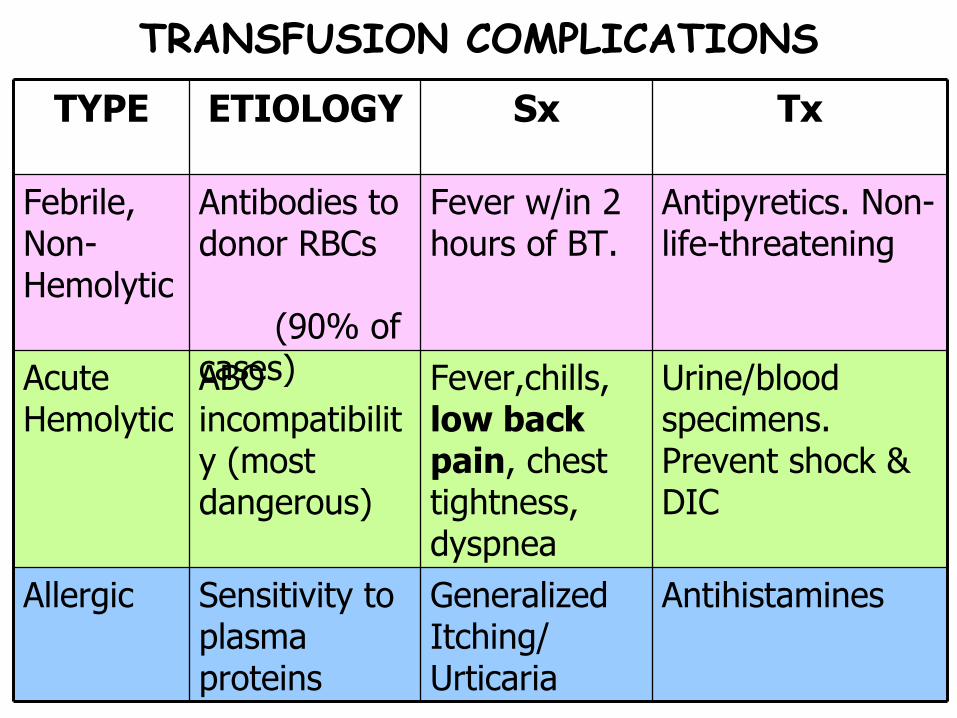
Generalized Itching/ Urticaria
Fever,chills, low back pain, chest tightness, dyspnea
Fever w/in 2 hours of BT.
Sx
AntihistaminesSensitivity to plasma proteins
Allergic
Urine/blood specimens. Prevent shock & DIC
ABO incompatibility (most dangerous)
Acute Hemolytic
Antipyretics. Non-life-threatening
Antibodies to donor RBCs (90% of cases)
Febrile, Non-Hemolytic
TxETIOLOGYTYPE
TRANSFUSION COMPLICATIONS
Sx
Circulatory Overload
Bacterial Contamination
TxETIOLOGYTYPE
TRANSFUSION COMPLICATIONS
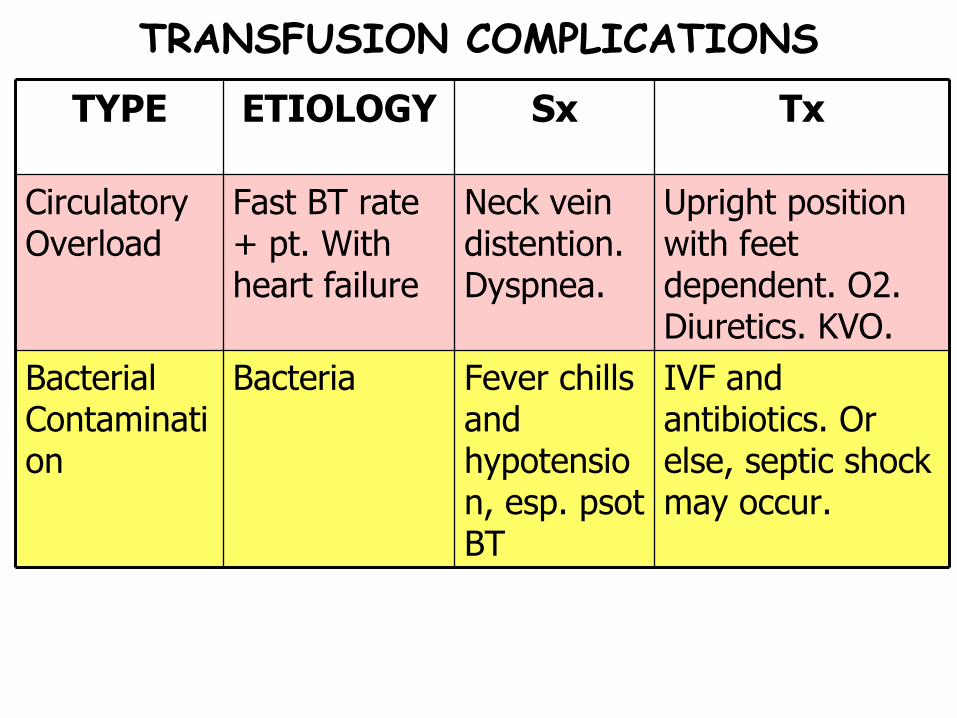
Fever chills and hypotension, esp. psot BT
Neck vein distention. Dyspnea.
Sx
Upright position with feet dependent. O2. Diuretics. KVO.
Fast BT rate + pt. With heart failure
Circulatory Overload
IVF and antibiotics. Or else, septic shock may occur.
Bacteria Bacterial Contamination
TxETIOLOGYTYPE
TRANSFUSION COMPLICATIONS
• Crossmatching for platelets is usually not required.
• The volume in a unit of platelets may vary from 50 –70 ml to 200-400 ml.
• Platelets can be administered up to 48 hours after receipt from the blood bank
• Platelets should be administered over 1-2 hours only
• Platelet counts are normally evaluated at 1 hour and 1 day post-transfusion.
• Fresh frozen plasma are usually infused within 6 hours of thawing.
BLOOD/ BLOOD COMPONENTS (T or F)
• Crossmatching for platelets is usually not required. T
• The volume in a unit of platelets may vary from 50 –70 ml to 200-400 ml. T
• Platelets can be administered up to 48 hours after receipt from the blood bank. F: immediately upon receipt
• Platelets should be administered over 1-2 hours only. F: 15-30 minutes only.
• Platelet counts are normally evaluated at 1 hour and 1 day post-transfusion. T
• Fresh frozen plasma are usually infused within 6 hours of thawing. T
BLOOD/ BLOOD COMPONENTS (T or F)
After obtaining a unit of blood from the blood bank, the nurse next looks for which of the following members of the health care team to assist in checking the unit of the blood?
a. Blood bank technician
b. Registered nurse
c. Medical Student
d. Phlebotomis
PRACTICE QUESTIONS

After checking the unit of blood with another nurse, the nurse would assess for which of the following items just before beginning the transfusion?
a. Vital signs
b. Latest hematocrit level
c. Skin color
d. Urine output
PRACTICE QUESTIONS
A nurse has just received an order to transfuse a unit of packed RBCs for an assigned client. In planning coverage for the client assignment, the nurse asks if another nurse will be available to check on the other assigned clients for how long when the unit of blood is hung?
a. 5 minutes
b. 15 minutes
c. 30 minutes
d. 45 minutes
PRACTICE QUESTIONS

A client has an order to receive a unit of packed RBCs. A nurse would obtain which of the following IV solutions from the IV storage area to hang with the blood product at the client’s bedside?
a. 0.9% Sodium Chloride
b. Lactated Ringer’s
c. 5% dextrose in 0.9% Sodium Chloride
d. 5% dextrose in 0.45% Sodium Chloride
PRACTICE QUESTIONS

A nurse who is about to begin a blood transfusion knows that blood cells start to deteriorate after a certain period of time. The nurse checks which of the following items carefully before beginning the transfusion to ensure that this has not happend?
a. Blood identification number
b. Expiration date
c. Blood group and type
d. Presence of clots
PRACTICE QUESTIONS
DAVE MANRIQUEZ, RN
End of LectureThank you so much for your attention!!!