pharmacotherapy of type 2 diabetes mellitus
TRANSCRIPT

1
Pharmacotherapy of Type 2 Diabetes Mellitus
Dr. Shamshi Azmi
Junior Resident
Dept. of Pharmacology

2
Diabetes mellitus: a group of common metabolic
disorders that share the phenotype of hyperglycemia.
Pathophysiology of type 2 diabetes mellitus. Harrison's Principles Of Internal Medicine. 19th ed.
Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL, et al., 2016. Print. page 2404
INTRODUCTION

3
• According to International Diabetes Federation 2015 , 1
in 11 adults (415 million) suffer with diabetes
worldwide, projecting that in 2040 this number will
increase to 642 million(1 in 10 adults).
• Studies have shown that India has a potential
epidemic of diabetes and by the year 2040, it will have
maximum increase in incidence of Diabetes mellitus.
"IDF Diabetes Atlas - 2015 Atlas". Diabetesatlas.org. N.p., 2016. Web. 26 Sept. 2016.


5
The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus: Report of the Expert
Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 20: 1183–1197, 1997

6
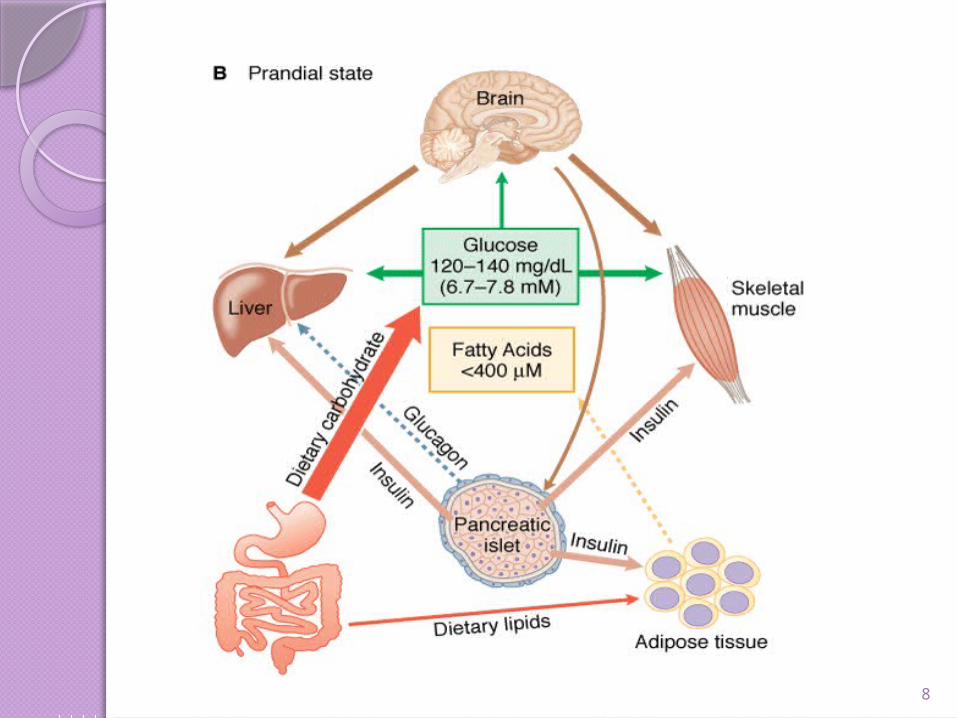
GLUCOSE HOMEOSTASIS

7
8

9

10
Phases Of InsuIin release
In non diabetic individuals-
50% of the total daily insulin -during basal period
Remainder -postprandial.
“First phase”: promotes peripheral utilization of the prandial
nutrient load, suppresses hepatic glucose production, and limits
postprandial glucose elevation. Begins within 2 min of nutrient
ingestion and continues for 10-15 minutes.
Second phase: follows and is sustained until normoglycemia is
restored.

11

12
PATHOGENESIS OF TYPE 2 DM

13
The two metabolic defects that characterize type 2 DM are
(1) Insulin resistance
(2) β-cell dysfunction that is manifested as inadequate insulin
secretion in the face of insulin resistance and hyperglycemia

14

Overall goal

Insulin secretagogues
Sulfonylureas
Meglitinide analogues
GLP-1 receptor agonist
DPP-4 inhibitors
Overcome insulin resistance
• Biguanides
• Thiazolidinediones
Misc.
• α- Glucosidase
inhibitors
• Amylin analogue
• SGLT-2 inhibitors
• Dopamine D2
receptor agonist

17

Biguanides (AMPK activator)

19
β CELL ATP SENSITIVE K+ CHANNEL
Octamer composed of four K+ channel subunits and four sulfonylurea subunits.
Insulin secretagogues
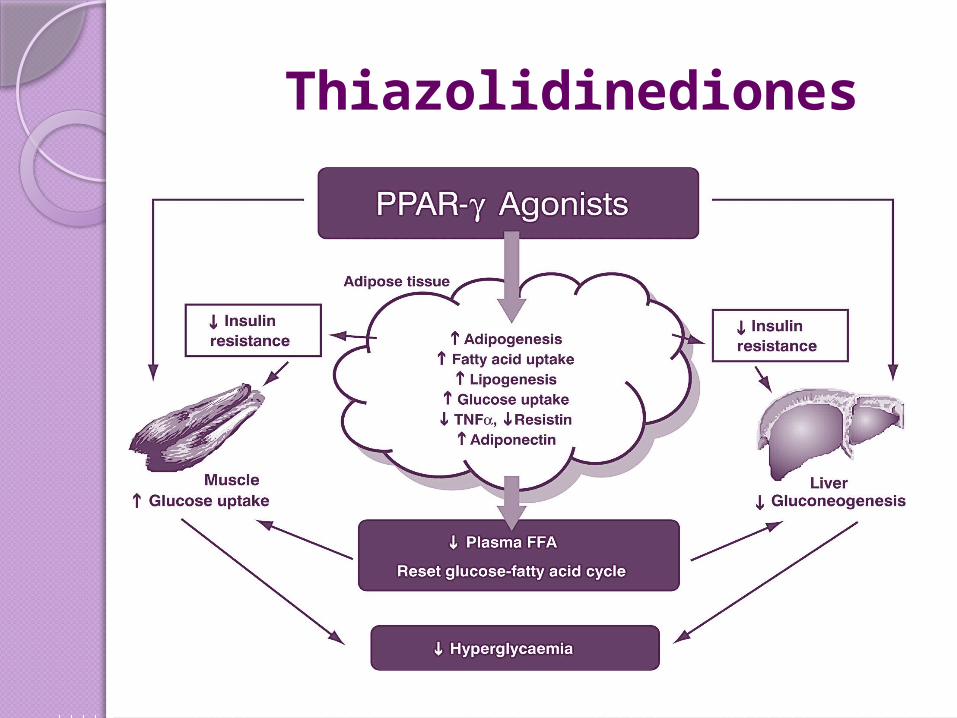
Thiazolidinediones

21

Alpha-Glucosidase Inhibitors

23

Major transporter of glucose in the kidney
• Nearly exclusively expressed in the kidney
• Responsible for ~90% of renal glucose reabsorption in the proximal tubule
Proximal Tubule
Na+K+
ATPase
Glucose
GLUT2
Glucose
SGLT2
BloodLumen
Na+

Amylin analogue

26
ADA 2016 Guidelines

27

28

29

30
Criteria for testing for diabetes in asymptomatic adults
Testing should be considered in all adults who are obese and have additional risk factors like:
physical inactivity
first-degree relative with diabetes
high-risk race/ethnicity (e.g., African American, Latino, Native American, Asian American, Pacific Islander)
women who delivered a baby weighing 9 lb or were diagnosed with GDM
women with PCOD
Hypertension
HDL cholesterol level <35 mg/dL and/or a TG level >250 mg/dL
history of CVD

31
thank you

32

Target Class
Glycogen synthase kinase-3 Inhibitors
Glucokinase Activators
Protein tyrosine phosphatase-1b Inhibitors
Liver selective glucocorticoid receptors Antagonist
Glucagon receptor Antagonist
α-lipoic acid Agonist
AMP-activated protein kinase Agonist

Protein tyrosine phosphatase-1b inhibitors
Protein tyrosine phosphatase-1b causes: Dephosphorylation of Insulin receptorsDephosphorylation of Januskinase receptors associated with leptin
Negative regulation of insulin signalling and insulin resistanceInhibition of leptin mediated regulation of food intake
Hyperglycemia and obesity
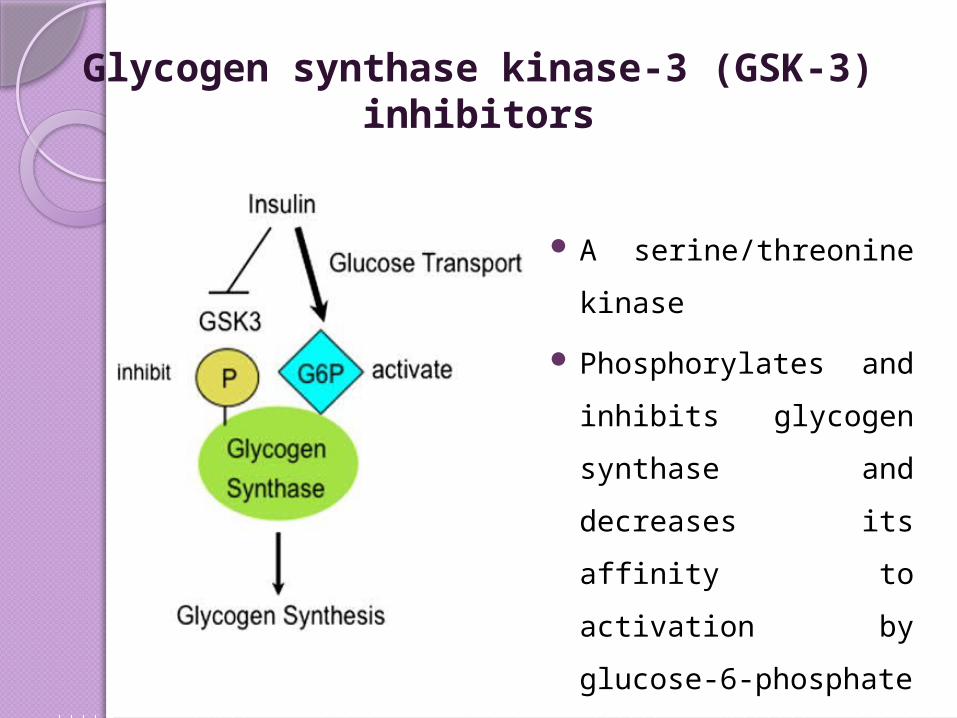
Glycogen synthase kinase-3 (GSK-3) inhibitors
A serine/threonine kinase
Phosphorylates and inhibits
glycogen synthase and
decreases its affinity to
activation by glucose-6-
phosphate

Glycogen phosphorylase inhibitors Glycogen Glycogen phosphorylase Glucose-1-phosphate Phosphoglucomutase Glucose-6-phosphate---------> Glycolytic
pathwayGlycogen phosphorylase can serve a potential
therapeutic target to decrease hepatic glucose production
Phase II trials of GSK-1362885.

37
SYNDROMES A few patients with homozygous mutations in the INSR gene have
been described, which causes Donohue syndrome or Leprechaunism. This autosomal recessive disorder results in a totally non-functional insulin receptor. These patients have low-set, often protuberant, ears, flared nostrils, thickened lips, and severe growth retardation.
In most cases, the outlook for these patients is extremely poor, with death occurring within the first year of life.
Other mutations of the same gene cause the less severe Rabson-Mendenhall syndrome, in which patients have characteristically abnormal teeth,hypertrophic gingiva (gums), and enlargement of the pineal gland.
Both diseases present with fluctuations of the glucose level: After a meal the glucose is initially very high, and then falls rapidly to abnormally low levels.

38
Drugs causing hyperglycemia Glucocorticoids, Beta blockers (nonselective)Atypical antipsychoticsProtease inhibitorsDiureticsPhenytoinThyroid hormonesPentamidine