phy138y – nuclear and radiation section - u of t physicskey/phy138/suppl.notes/sniv... · rem...
TRANSCRIPT
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 1 of 15
PHY138Y – Nuclear and Radiation Section Supplementary Notes IV
The Biological Effects of Radiation Contents.
4.1 Introduction 4.2 Radiation Measures
4.2.1 The Relation between Exposure, Dose, and Fluence 4.2.2 Radiation Weighting Factors and Equivalent Dose
4.2.3 Tissue Weighting Factors and Effective Dose 4.2.4 Effective Dose 4.3 Environmental Exposure to Radiation 4.3.1 Natural Radiation Background 4.3.2 Man-Made Radiation Background 4.4 Interaction of Radiation with Biological Cells 4.5 Radiation – Risk or Benefit? 4.5.1 Symptoms of Exposure to High Radiation Dosage 4.5.2 Risks of Exposure to Low Radiation Dosage 4.5 Radiation in Therapy Appendix 4-A. High Dosage Studies Appendix 4-B. Low Dosage Studies Appendix 4-C. Risk from Low Dose Rates Appendix 4-D. Backup Reading in Knight References. I list below some of the sources I used in preparing this set of Supplementary Notes.
1. Russell K. Hobbie, Intermediate Physics for Medicine and Biology (3rd ed., AIP, 1997) 2. P.P. Dendy and B. Heaton, Physics for Radiologists (Blackwell, 1987). 3. Mark Oldham, Radiation Physics and Applications in Therapeutic Medicine, Physics
Education 36, 460-467 (2001): see the Reference section of the N&R Web page. 4. Thomas, R.G. (1994) The US radium luminisers: A case for a policy of ‘below regulatory
concern’ , J. Radiol. Prot., 14, 2, pp 141-153, 1994. 5. Zbigniew Jaworowski, Radiation Risk and Ethics, Physics Today 52(9) 24-29, Sept.1999. 6. R.D. Badawi, Nuclear Medicine , Physics Education 36, 452-459 (2001). 7. D.W.O. Rogers, Monte Carlo Techniques in Radiotherapy, Physics in Canada 58(2), 63-
77 (2002). 8. D.E.S. McNeill and K.G. McNeill, Notes for PHY238Y (Kishmul Resources, 2002). 9. http://www.hc-sc.gc.ca/english/iyh/environment/exposure.html#top ;Health Canada. 10. http://www.epa.gov/radon/;The US Environmental Protection Agency. 11. http://www.philrutherford.com/; all about radiation and its risks. 12. http://www.physics.isu.edu/radinf/risk.htm ; contributions to normal radiation loads. 13. http://www.tenorm.com/ncrp116icrp60.htm; effective dose. 14. http://www.cns-snc.ca/branches/Toronto/radiation/natural_and_human_radiation.html;
graph of Radiation from natural and man-made sources. 15. http://physics.nist.gov/PhysRefData/XrayMassCoef/cover.html); tables of absorption
coefficients from the US National Institute of Standards and Technology. 16. http://www.sciencedaily.com/releases/2001/10/011026075752.htm; article and links on
the Chernobyl nuclear accident (one of many).
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 2 of 15
4. The Biological Effects of Radiation.
4.1 Introduction. As radiation (X-rays, alpha, beta, or gamma rays) traverses matter, it causes ionization that can damage the cells through which it passes. At low levels, the body can repair such damage; however at higher levels, illness can result. Radiation can also be beneficial; at low dosage it provides an excellent diagnostic tool, while high doses are used to destroy cancer cells. Many different sources of radiation are used, including radioisotopes and beams of electrons, protons, neutrons and heavy ions. These notes investigate the effects of radiation on human biological matter.
4.2 Radiation Measures The biological effects of radiation depend on three factors: the energy deposited per unit mass, the distribution of the energy deposition, and the susceptibility to damage of the traversed tissue. This section explains how these effects are calculated.
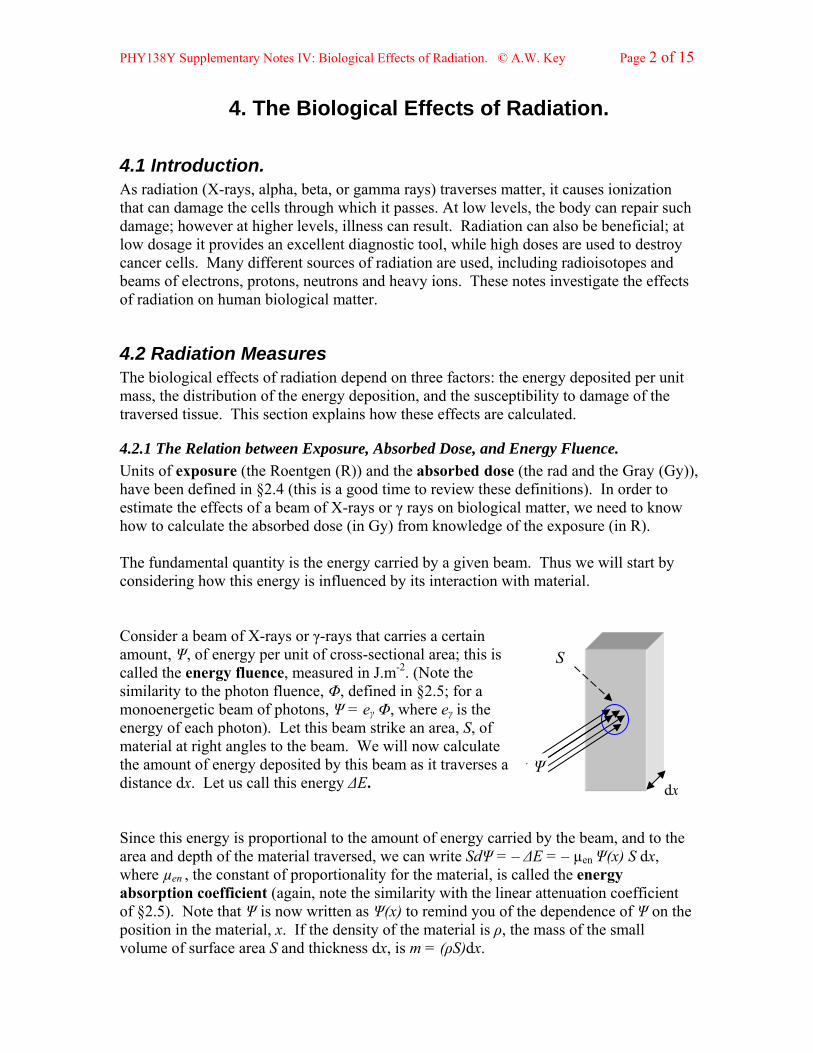
4.2.1 The Relation between Exposure, Absorbed Dose, and Energy Fluence. Units of exposure (the Roentgen (R)) and the absorbed dose (the rad and the Gray (Gy)), have been defined in §2.4 (this is a good time to review these definitions). In order to estimate the effects of a beam of X-rays or γ rays on biological matter, we need to know how to calculate the absorbed dose (in Gy) from knowledge of the exposure (in R). The fundamental quantity is the energy carried by a given beam. Thus we will start by considering how this energy is influenced by its interaction with material. Consider a beam of X-rays or γ-rays that carries a certain amount, Ψ, of energy per unit of cross-sectional area; this is called the energy fluence, measured in J.m-2. (Note the similarity to the photon fluence, Φ, defined in §2.5; for a monoenergetic beam of photons, Ψ = eγ Φ, where eγ is the energy of each photon). Let this beam strike an area, S, of material at right angles to the beam. We will now calculate the amount of energy deposited by this beam as it traverses a distance dx. Let us call this energy ΔE. dx
Ψ
S
Since this energy is proportional to the amount of energy carried by the beam, and to the area and depth of the material traversed, we can write SdΨ = – ΔE = – µen Ψ(x) S dx, where µen , the constant of proportionality for the material, is called the energy absorption coefficient (again, note the similarity with the linear attenuation coefficient of §2.5). Note that Ψ is now written as Ψ(x) to remind you of the dependence of Ψ on the position in the material, x. If the density of the material is ρ, the mass of the small volume of surface area S and thickness dx, is m = (ρS)dx.
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 3 of 15
As in §2.5, the above formalism immediately leads to the following expression for the absorption of energy as it traverses material: Ψ(x) = Ψ(0) exp(– µenx). This expression gives the value of the energy fluence at a depth x in the material. The energy fluence can now be related to the absorbed dose, which is the quantity of most interest in medical applications. The absorbed dose at a depth x , Dm(x), is just the energy absorbed by the slice of the material at the depth x – of thickness dx and surface area S - divided by the mass contained in the slice.
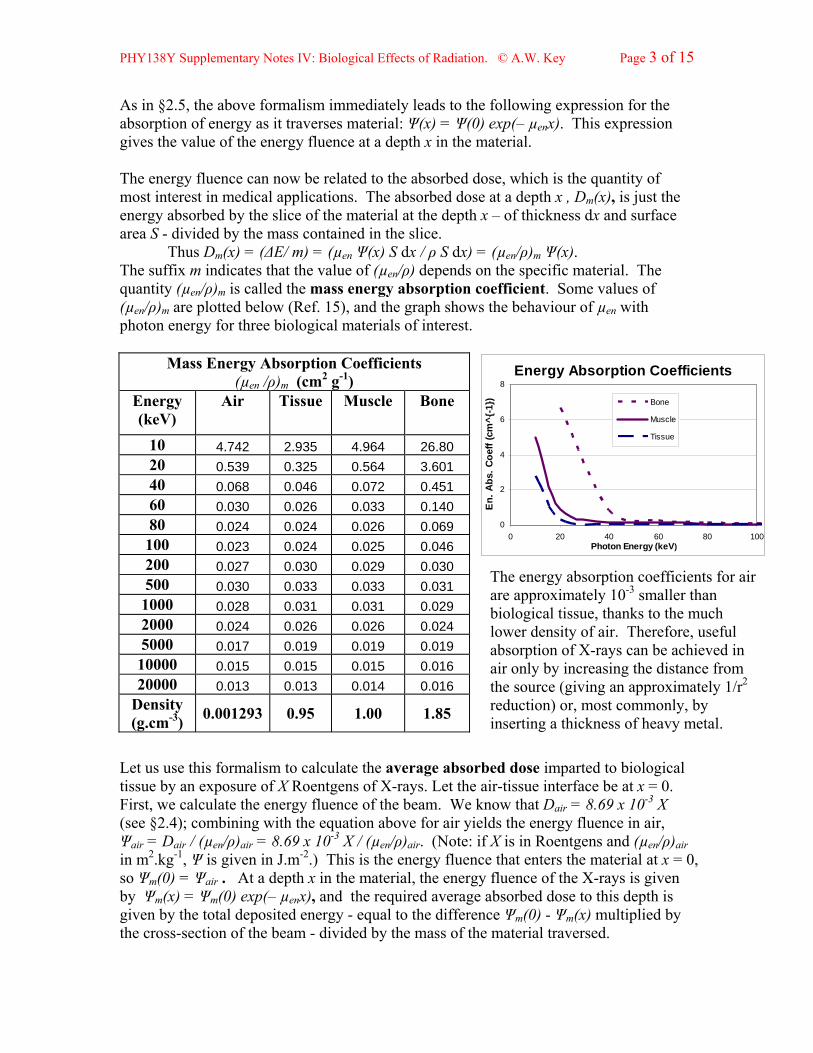
Thus Dm(x) = (ΔE/ m) = (µen Ψ(x) S dx / ρ S dx) = (µen/ρ)m Ψ(x). The suffix m indicates that the value of (µen/ρ) depends on the specific material. The quantity (µen/ρ)m is called the mass energy absorption coefficient. Some values of (µen/ρ)m are plotted below (Ref. 15), and the graph shows the behaviour of µen with photon energy for three biological materials of interest.
Mass Energy Absorption Coefficients
Let us use this formalism to calculate the average absorbed dose imparted to biological tissue by an exposure of X Roentgens of X-rays. Let the air-tissue interface be at x = 0. First, we calculate the energy fluence of the beam. We know that Dair = 8.69 x 10-3 X (see §2.4); combining with the equation above for air yields the energy fluence in air, Ψair = Dair / (µen/ρ)air = 8.69 x 10-3 X / (µen/ρ)air. (Note: if X is in Roentgens and (µen/ρ)air in m2.kg-1, Ψ is given in J.m-2.) This is the energy fluence that enters the material at x = 0, so Ψm(0) = Ψair . At a depth x in the material, the energy fluence of the X-rays is given by Ψm(x) = Ψm(0) exp(– µenx), and the required average absorbed dose to this depth is given by the total deposited energy - equal to the difference Ψm(0) - Ψm(x) multiplied by the cross-section of the beam - divided by the mass of the material traversed.
(µen /ρ)m (cm2 g-1) Energy (keV)
Air
Tissue
Muscle Bone
10 4.742 2.935 4.964 26.80 20 0.539 0.325 0.564 3.601 40 0.068 0.046 0.072 0.451 60 0.030 0.026 0.033 0.140 80 0.024 0.024 0.026 0.069 100 0.023 0.024 0.025 0.046 200 0.027 0.030 0.029 0.030 500 0.030 0.033 0.033 0.031 1000 0.028 0.031 0.031 0.029 2000 0.024 0.026 0.026 0.024 5000 0.017 0.019 0.019 0.019 10000 0.015 0.015 0.015 0.016 20000 0.013 0.013 0.014 0.016
Energy Absorption Coefficients
0
2
4
6
8
0 20 40 60 80Photon Energy (keV)
En.
Abs
. Coe
ff (c
m^{
-1})
100
Bone
Muscle
Tissue
The energy absorption coefficients for air are approximately 10-3 smaller than biological tissue, thanks to the much lower density of air. Therefore, useful absorption of X-rays can be achieved in air only by increasing the distance from the source (giving an approximately 1/r2 reduction) or, most commonly, by inserting a thickness of heavy metal.
Density (g.cm-3) 0.001293 0.95 1.00 1.85

PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 4 of 15
4.2.2 Radiation Weighting Factors and Equivalent Dose With 8000 times the mass and double the charge, a slow alpha will produce a much greater density of ionization than an electron that deposits the same total energy; both alpha and electron produce more density of ionization than a photon. Thus even though a photon may deposit the same total energy as an alpha, its energy is more spread out along its path and thus does less biological damage. Such effects are taken into account by "radiation weighting factors", WR *. The average absorbed dose (in Gy or rad) is converted to an "equivalent dose" by multiplying by WR. The unit of the equivalent dose is the Sievert (Sv), derived directly from the Gray. Thus, the Equivalent Dose in Sv is H = WR• (absorbed dose in Grays). This unit is named after Swedish scientist Rolf Sievert (1896-1960). An older unit, still used, is the rem (roentgen equivalent mammal), where rem = WR • (absorbed dose in rads). Obviously 1 Sv = 100 rem; 1 mrem = 10 µSv. Radiation Type WR (RBE) Radiation Type WR (RBE)
Photons*, electrons 1 α-particles 20 Protons 2 neutrons – function of energy
*WR = 1 can be used for the full range of X-ray energies used in this course.
The table gives some typical values of the radiation weighting factor for different types of radiation traversing “average” biological tissue. The larger values, for protons, alpha particles, and neutrons, correspond to the fact that these particles do more biological damage than X- or gamma rays in a given tissue.
4.2.3 Tissue Weighting Factors and Effective Dose Different tissues are more susceptible to damage than others, for the same density of ionization; they also have different susceptibilities to different types of risk, such as fatal or non-fatal cancers, hereditary risks, etc. The International Commission on Radiation Protection (ICRP) publishes calculated “tissue weighting factors”, WT , to take these effects and the size of the different organs into account for radiation protection purposes. The 2007 values (2007), averaged over gender and age, are shown in the table. Higher values of WT correspond to greater susceptibility to risk. The Equivalent Dose for each irradiated organ, HT,is multiplied by WT and summed over all organs to obtain what is called the Effective Dose**, discussed in the following section; Heff = Σ WT HT. The Effective Dose is measured in the same units as the Equivalent Dose (Sieverts).
Organ or Tissue WT ΣWT Colon, Lung, Breast, Stomach, Bone Marrow 0.12 0.60
Gonads 0.08 0.08 Bladder, Oesophagus, Thyroid, Liver 0.04 0.16
Bone, Skin, Salivary Glands, Brain 0.01 0.04
Other Organs (grouped) 0.12 0.12
* Knight, section 42.7 (p.1373) uses the term Relative Biological Effectiveness – RBE. The term ‘Quality Factor’, denoted by Q or QF, is also in common use. ** Knight’s use of the term ‘effective dose’ (bottom of p. 1373) is unconventional.
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 5 of 15
4.2.4 Effective Dose The Effective Dose (Heff) is intended to allow direct comparison of the biological risks (cancer and hereditary effects) caused by different radiation exposures to different parts of the body. Though the calculation of the tissue weighting factors is difficult, the idea is simple. Since most environmental radiation irradiates the whole body (§4.3), Heff is intended to normalize the calculations to equivalent “whole body” exposures for purposes of comparison. Since the type of radiation and the type of the tissue irradiated affect the level of risk, both radiation and tissue weighting factors are used. For example, a dose of 1 Sv to the gonads (WT =0.08) is expected to produce as great a risk of fatal cancer as a whole body dose of 0.08 Sv . WT is defined in such a way that the sum of the weighting factors taken over all organs of the body is equal to 1: Σ WT = 1. If only a fraction of the organ is irradiated, the result for that organ must be multiplied by that fraction.
4.3 Environmental Exposure to Radiation We are continuously exposed to a wide variety of radiation, both natural and man-made, from cosmic rays, from the air we breathe, from the ground, from buildings, from our food, from medical or dental diagnostics, even from our own – and others’ – bodies. This section will explore the background environmental radiation.
4.3.1 Natural Radiation Background About 80% of the total radiation we receive comes from natural sources. The worldwide average dose is 2.4 mSv per year, but there is huge variation from place to place – from 1 mSv/yr to over 700 mSv/yr! According to Health Canada, the amount of natural radiation we receive is between 2 to 4 mSv/yr. The radiation received by people living on the Canadian Shield or at higher altitudes is greater than the average, due to the increased terrestrial or cosmic ray background r
Background Radiation - average from natural sources
68%
13%
10%
9%
RADON
HUMAN BODYCOSMIC RAYS
SOIL AND ROCK
Data from the USEnvironmental Protection Agency
espectively.
he greatest contributor to the natural background, and to its wide variation, is the gas
at
. t,
d
Inside buildings, Radon can accumulate up to ten times that amount.
TRadon; this gas is chemically inert, and has a half-life of 3.8 days. It is one of the by-products in the decay chain of 238U and 232Th, which are present in most rocks and soillevels of several parts per million, and ten times that in some rocks such as granite and sedimentary rocks. Both of these isotopes have half-lives of several million years, and both decay chains produce Radium, which decays into isotopes of Radon, mainly 222
86 Rn(The radioactivity of this and similar decay chains generate heat in the earth’s cruswhich maintains the temperature of the earth necessary to sustain life on earth). The Radon decay chain produces a number of heavy metals, mainly polonium, bismuth anlead. These nuclei, being charged, can attach themselves to particles of dust which are then inhaled; the overall half-life of the Radon daughters is 22 years. In the open air, depending on location, the radioactive level is several tenths of a pCi per litre of air.
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 6 of 15
Nuclide Activit
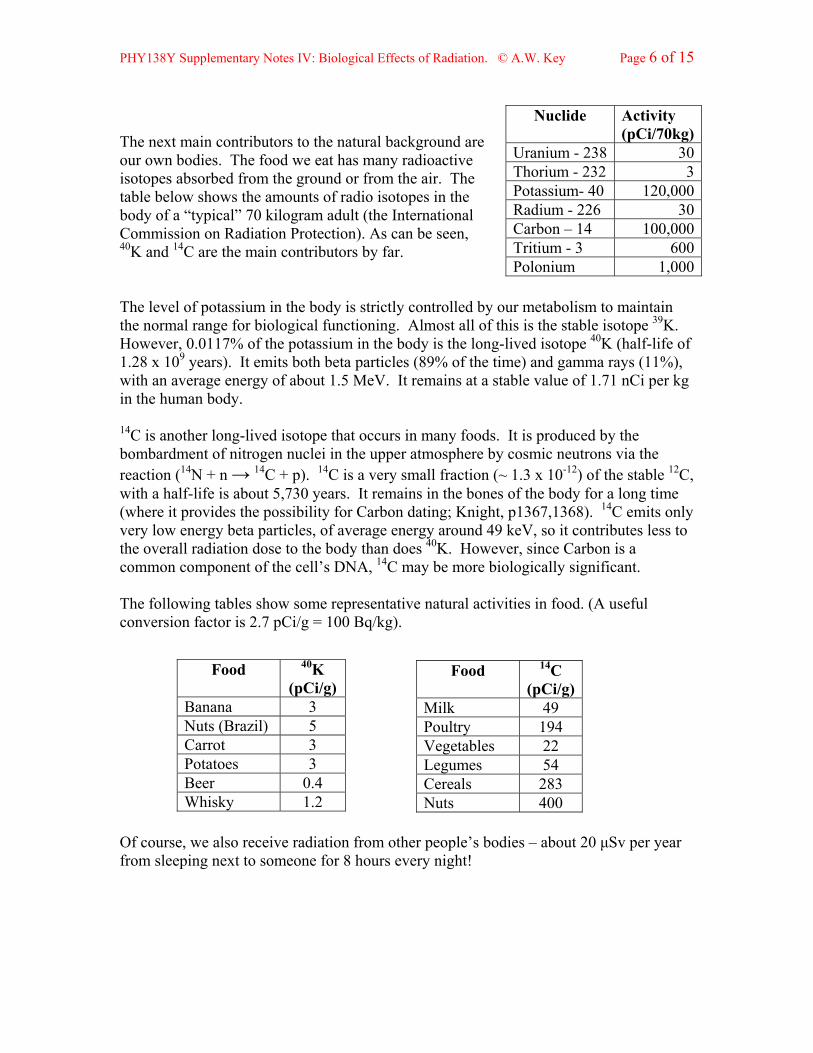
The next main contributors to the natural background are ur own bodies. The food we eat has many radioactive
he level of potassium in the body is strictly controlled by ou to maintae normal range for biological functioning. Almost all of this is the stable isotope 39K.
f
ved isotope that occurs in many foods. It is produced by the bardment of nitrogen nuclei in the upper atmosphere by cosmic neutrons via the
le 12C, e
onversion factor is 2.7 pCi/g = 100 Bq/kg).
f course receive ra ion from other people’s bodies – about 20 μSv per year om sleeping next to someone for 8 hours every night!
y (pCi/70kg)
Ur 8 0anium - 23 3oThorium - 232 3Potassium- 40
isotopes absorbed from the ground or from the air. The table below shows the amounts of radio isotopes in the body of a “typical” 70 kilogram adult (the International Commission on Radiation Protection). As can be seen, 40K and 14C are the main contributors by far.
120,000Radium - 226 30Carbon – 14 100,000Tritium - 3 600Polonium 1,000
T r metabolism in thHowever, 0.0117% of the potassium in the body is the long-lived isotope 40K (half-life o1.28 x 109 years). It emits both beta particles (89% of the time) and gamma rays (11%), with an average energy of about 1.5 MeV. It remains at a stable value of 1.71 nCi per kg in the human body.
14C is another long-libomreaction (14N + n → 14C + p). 14C is a very small fraction (~ 1.3 x 10-12) of the stabwith a half-life is about 5,730 years. It remains in the bones of the body for a long tim(where it provides the possibility for Carbon dating; Knight, p1367,1368). 14C emits only very low energy beta particles, of average energy around 49 keV, so it contributes less tothe overall radiation dose to the body than does 40K. However, since Carbon is a common component of the cell’s DNA, 14C may be more biologically significant. The following tables show some representative natural activities in food. (A useful c
Food 40K Food 14C (pCi/g)
O , we also diatfr
(pCi/g) Banana 3 Milk 49 Nuts (Brazil) 5 Carrot 3 Potatoes 3 Beer
Poultry 194 Vegetables 22 Legumes 54 Cereals 283 Nuts 400
0.4 Whisky 1.2
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 7 of 15
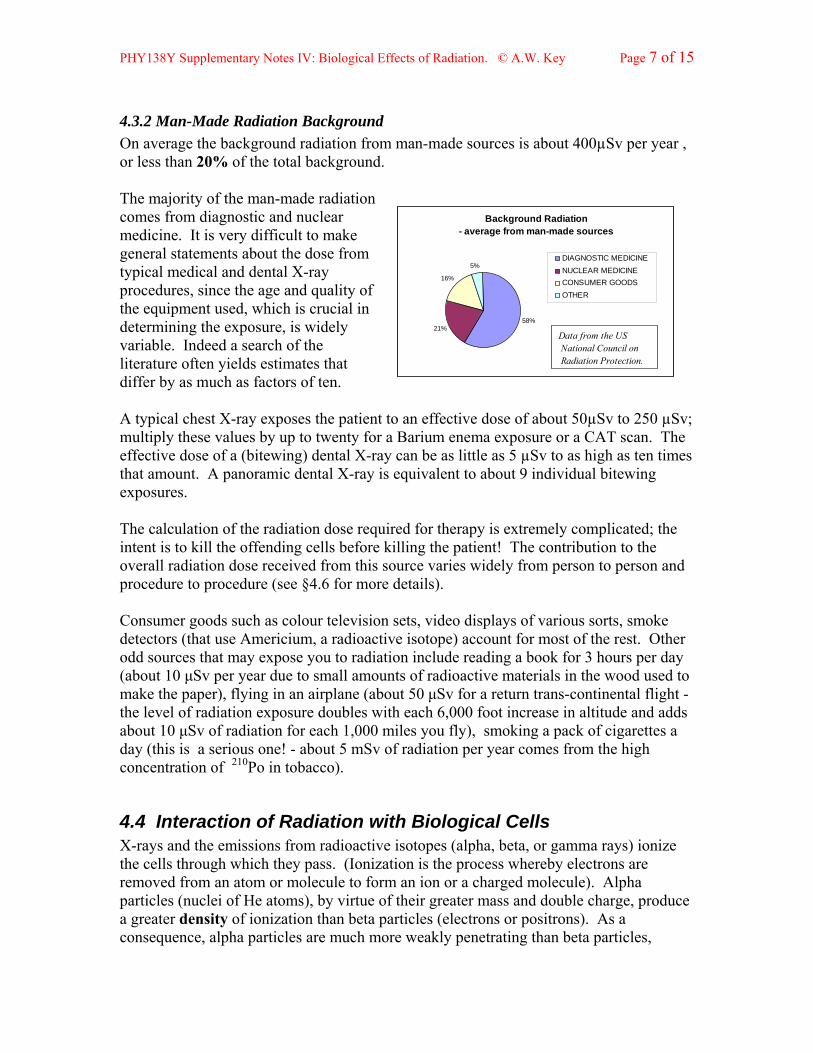
4.3.2 Man-Made Radiation Background On average the background radiation from man-made sources is about 400µSv per year , or less than 20% of the total background. The majority of the man-made radiation comes from diagnostic and nuclear medicine. It is very difficult to make general statements about the dose from typical medical and dental X-ray procedures, since the age and quality of the equipment used, which is crucial in determining the exposure, is widely variable. Indeed a search of the literature often yields estimates that differ by as much as factors of ten.
Background Radiation - average from man-made sources
58%21%
16%
5%DIAGNOSTIC MEDICINE NUCLEAR MEDICINECONSUMER GOODSOTHER
Data from the US National Council onRadiation Protection.
A typical chest X-ray exposes the patient to an effective dose of about 50µSv to 250 µSv; multiply these values by up to twenty for a Barium enema exposure or a CAT scan. The effective dose of a (bitewing) dental X-ray can be as little as 5 µSv to as high as ten times that amount. A panoramic dental X-ray is equivalent to about 9 individual bitewing exposures. The calculation of the radiation dose required for therapy is extremely complicated; the intent is to kill the offending cells before killing the patient! The contribution to the overall radiation dose received from this source varies widely from person to person and procedure to procedure (see §4.6 for more details). Consumer goods such as colour television sets, video displays of various sorts, smoke detectors (that use Americium, a radioactive isotope) account for most of the rest. Other odd sources that may expose you to radiation include reading a book for 3 hours per day (about 10 μSv per year due to small amounts of radioactive materials in the wood used to make the paper), flying in an airplane (about 50 μSv for a return trans-continental flight - the level of radiation exposure doubles with each 6,000 foot increase in altitude and adds about 10 μSv of radiation for each 1,000 miles you fly), smoking a pack of cigarettes a day (this is a serious one! - about 5 mSv of radiation per year comes from the high concentration of 210Po in tobacco).
4.4 Interaction of Radiation with Biological Cells X-rays and the emissions from radioactive isotopes (alpha, beta, or gamma rays) ionize the cells through which they pass. (Ionization is the process whereby electrons are removed from an atom or molecule to form an ion or a charged molecule). Alpha particles (nuclei of He atoms), by virtue of their greater mass and double charge, produce a greater density of ionization than beta particles (electrons or positrons). As a consequence, alpha particles are much more weakly penetrating than beta particles,
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 8 of 15
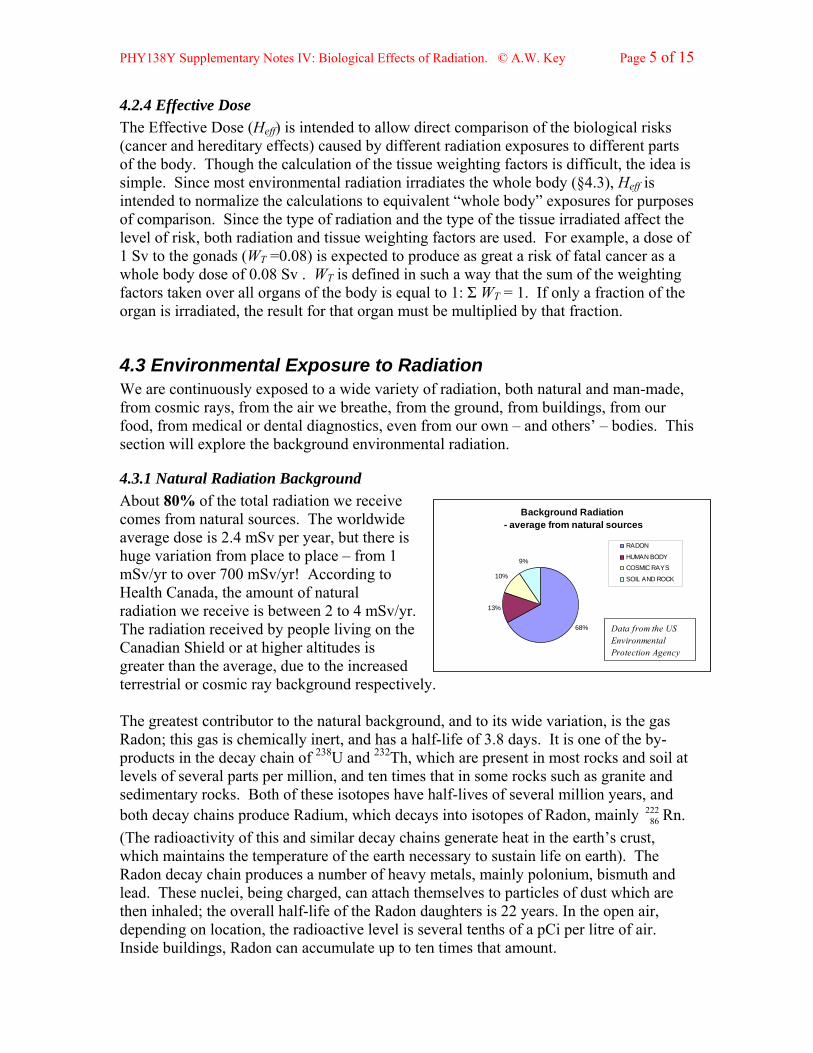
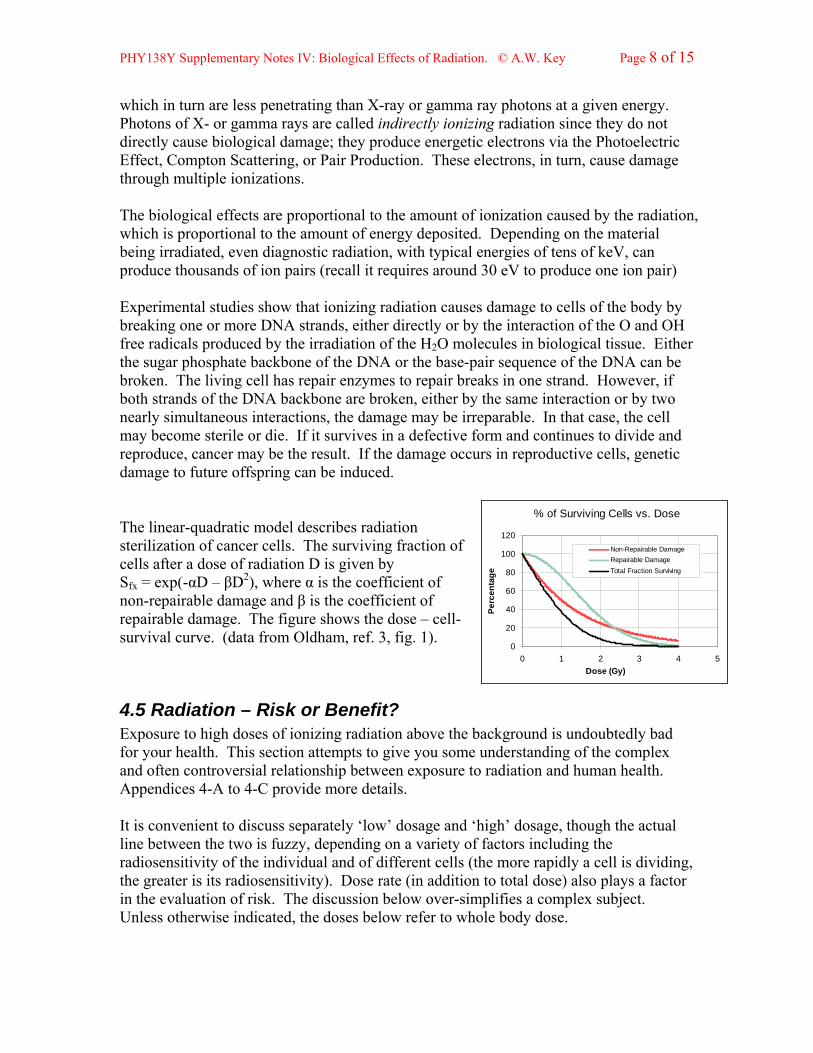
which in turn are less penetrating than X-ray or gamma ray photons at a given energy. Photons of X- or gamma rays are called indirectly ionizing radiation since they do not directly cause biological damage; they produce energetic electrons via the Photoelectric Effect, Compton Scattering, or Pair Production. These electrons, in turn, cause damage through multiple ionizations. The biological effects are proportional to the amount of ionization caused by the radiation, which is proportional to the amount of energy deposited. Depending on the material being irradiated, even diagnostic radiation, with typical energies of tens of keV, can produce thousands of ion pairs (recall it requires around 30 eV to produce one ion pair) Experimental studies show that ionizing radiation causes damage to cells of the body by breaking one or more DNA strands, either directly or by the interaction of the O and OH free radicals produced by the irradiation of the H2O molecules in biological tissue. Either the sugar phosphate backbone of the DNA or the base-pair sequence of the DNA can be broken. The living cell has repair enzymes to repair breaks in one strand. However, if both strands of the DNA backbone are broken, either by the same interaction or by two nearly simultaneous interactions, the damage may be irreparable. In that case, the cell may become sterile or die. If it survives in a defective form and continues to divide and reproduce, cancer may be the result. If the damage occurs in reproductive cells, genetic damage to future offspring can be induced. % of Surviving Cells vs. Dose
0
20
40
60
80
100
120
0 1 2 3 4 5Dose (Gy)
Perc
enta
ge
Non-Repairable DamageRepairable DamageTotal Fraction Surviving
The linear-quadratic model describes radiation sterilization of cancer cells. The surviving fraction of cells after a dose of radiation D is given by Sfx = exp(-αD – βD2), where α is the coefficient of non-repairable damage and β is the coefficient of repairable damage. The figure shows the dose – cell-survival curve. (data from Oldham, ref. 3, fig. 1).
4.5 Radiation – Risk or Benefit? Exposure to high doses of ionizing radiation above the background is undoubtedly bad for your health. This section attempts to give you some understanding of the complex and often controversial relationship between exposure to radiation and human health. Appendices 4-A to 4-C provide more details. It is convenient to discuss separately ‘low’ dosage and ‘high’ dosage, though the actual line between the two is fuzzy, depending on a variety of factors including the radiosensitivity of the individual and of different cells (the more rapidly a cell is dividing, the greater is its radiosensitivity). Dose rate (in addition to total dose) also plays a factor in the evaluation of risk. The discussion below over-simplifies a complex subject. Unless otherwise indicated, the doses below refer to whole body dose.
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 9 of 15
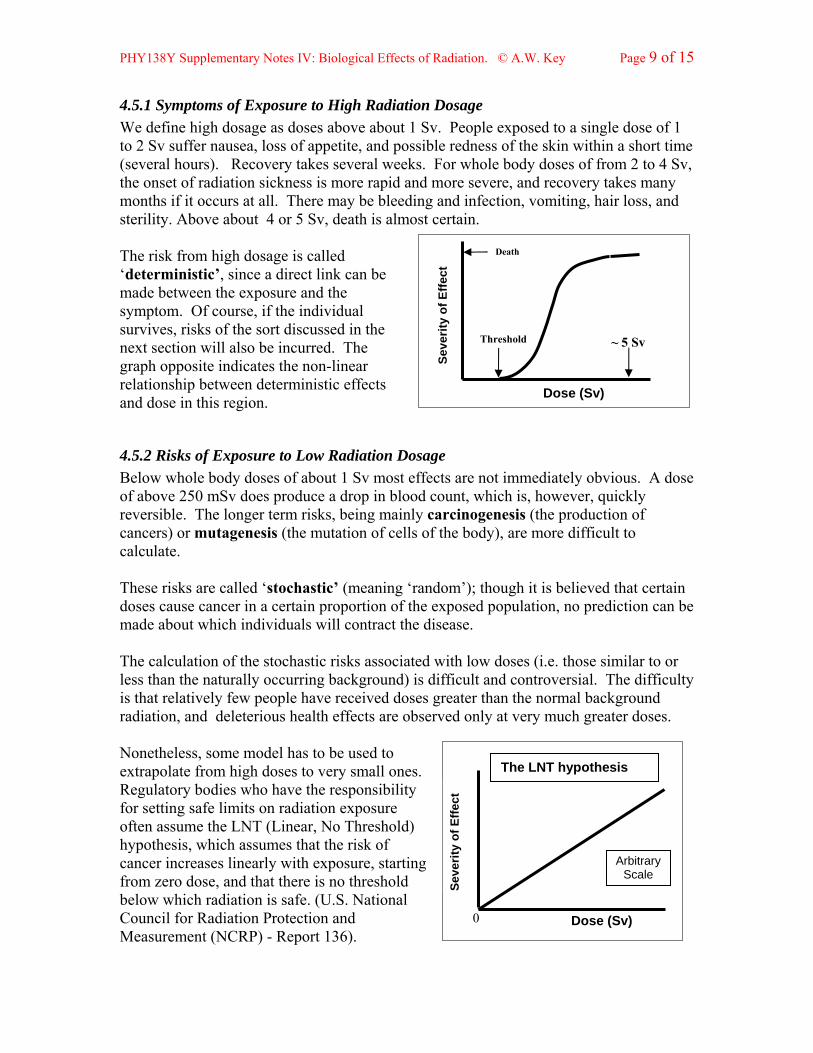
4.5.1 Symptoms of Exposure to High Radiation Dosage We define high dosage as doses above about 1 Sv. People exposed to a single dose of 1 to 2 Sv suffer nausea, loss of appetite, and possible redness of the skin within a short time (several hours). Recovery takes several weeks. For whole body doses of from 2 to 4 Sv, the onset of radiation sickness is more rapid and more severe, and recovery takes many months if it occurs at all. There may be bleeding and infection, vomiting, hair loss, and sterility. Above about 4 or 5 Sv, death is almost certain.
~ 5 Sv
Seve
rity
of E
ffect
The risk from high dosage is called ‘deterministic’, since a direct link can be made between the exposure and the symptom. Of course, if the individual survives, risks of the sort discussed in the next section will also be incurred. The graph opposite indicates the non-linear relationship between deterministic effects and dose in this region.
4.5.2 Risks of Exposure to Low Radiation Dosage Below whole body doses of about 1 Sv most effects are not immediately obvious. A dose of above 250 mSv does produce a drop in blood count, which is, however, quickly reversible. The longer term risks, being mainly carcinogenesis (the production of cancers) or mutagenesis (the mutation of cells of the body), are more difficult to calculate. These risks are called ‘stochastic’ (meaning ‘random’); though it is believed that certain doses cause cancer in a certain proportion of the exposed population, no prediction can be made about which individuals will contract the disease. The calculation of the stochastic risks associated with low doses (i.e. those similar to or less than the naturally occurring background) is difficult and controversial. The difficulty is that relatively few people have received doses greater than the normal background radiation, and deleterious health effects are observed only at very much greater doses. Nonetheless, some model has to be used to extrapolate from high doses to very small ones. Regulatory bodies who have the responsibility for setting safe limits on radiation exposure often assume the LNT (Linear, No Threshold) hypothesis, which assumes that the risk of cancer increases linearly with exposure, starting from zero dose, and that there is no threshold below which radiation is safe. (U.S. National Council for Radiation Protection and Measurement (NCRP) - Report 136).
DOSE (Sv)
Threshold
Death
Dose (Sv)
Dose (Sv) 0
Arbitrary Scale
The LNT hypothesis
Seve
rity
of E
ffect
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 10 of 15
This hypothesis suggests that the approximate overall risk coefficient for cancer and heritable effects is about 5 x 10-5 times the number of mSv received, or about 5% per Sv. This means that, for instance, a dose of 50 mSv is estimated to increase the probability of contracting fatal cancer by 5 • 10-5 • 50 = 0.0025, or 0.25% over and above the “normal” risk of about 25%.
However, many experts have pointed out that the extrapolation from the known deleterious effects at high dosage to very low doses is not justifiable. Many scientists would agree that the LNT theory is extremely conservative, if not simply wrong (see Appendix 4-C ).
In summary, the weight of evidence seems to support the statement made in 1996 by the Health Physics Society: “In accordance with current knowledge of radiation health risks, the Health Physics Society recommends against quantitative estimation of health risks below an individual dose of 5 rem in one year or a lifetime dose of 10 rem (100 mSv) in addition to background radiation. Risk estimation in this dose range should be strictly qualitative accentuating a range of hypothetical health outcomes with an emphasis on the likely possibility of zero adverse health effects. The current philosophy of radiation protection is based on the assumption that any radiation dose, no matter how small, may result in human health effects, such as cancer and hereditary genetic damage. There is substantial and convincing scientific evidence for health risks at high dose. Below 10 rem (100 mSv) (which includes occupational and environmental exposures), risks of health effects are either too small to be observed or are non-existent.” (My bolding.)
The Canadian Nuclear Safety Commission sets limits on the amount of radiation allowable in the workplace; 50 mSv in one year, and 100 mSv over five years. Additional regulations apply to pregnant women, since it is thought that potential damage is high for fetal cells. Particularly at risk are workers in medical or dental institutions where X-ray equipment is in use, and in the nuclear industry.
For purposes of comparison, here are some activities that increase your chances of dying by 1 part in a million: 1.4 cigarettes, 40 tbs. of peanut butter, 2 days in New York city, 40 miles in a car, 6 minutes canoeing, 0.1 mSv of radiation.
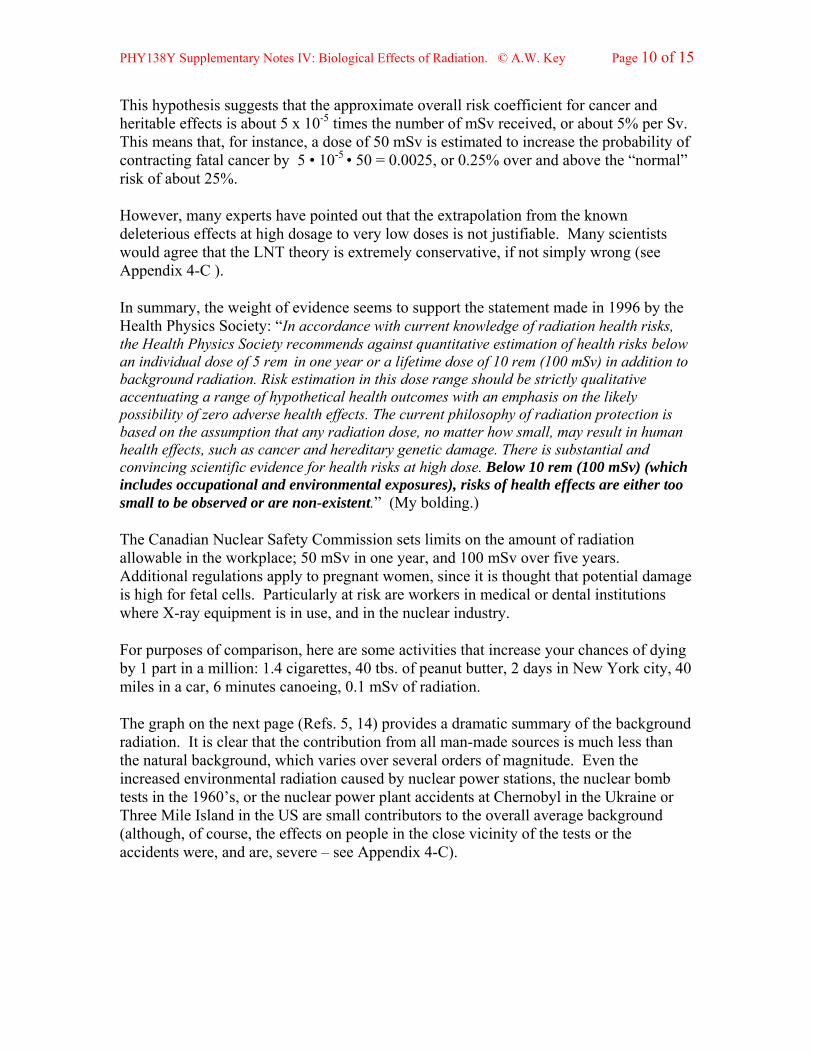
The graph on the next page (Refs. 5, 14) provides a dramatic summary of the background radiation. It is clear that the contribution from all man-made sources is much less than the natural background, which varies over several orders of magnitude. Even the increased environmental radiation caused by nuclear power stations, the nuclear bomb tests in the 1960’s, or the nuclear power plant accidents at Chernobyl in the Ukraine or Three Mile Island in the US are small contributors to the overall average background (although, of course, the effects on people in the close vicinity of the tests or the accidents were, and are, severe – see Appendix 4-C).
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 11 of 15
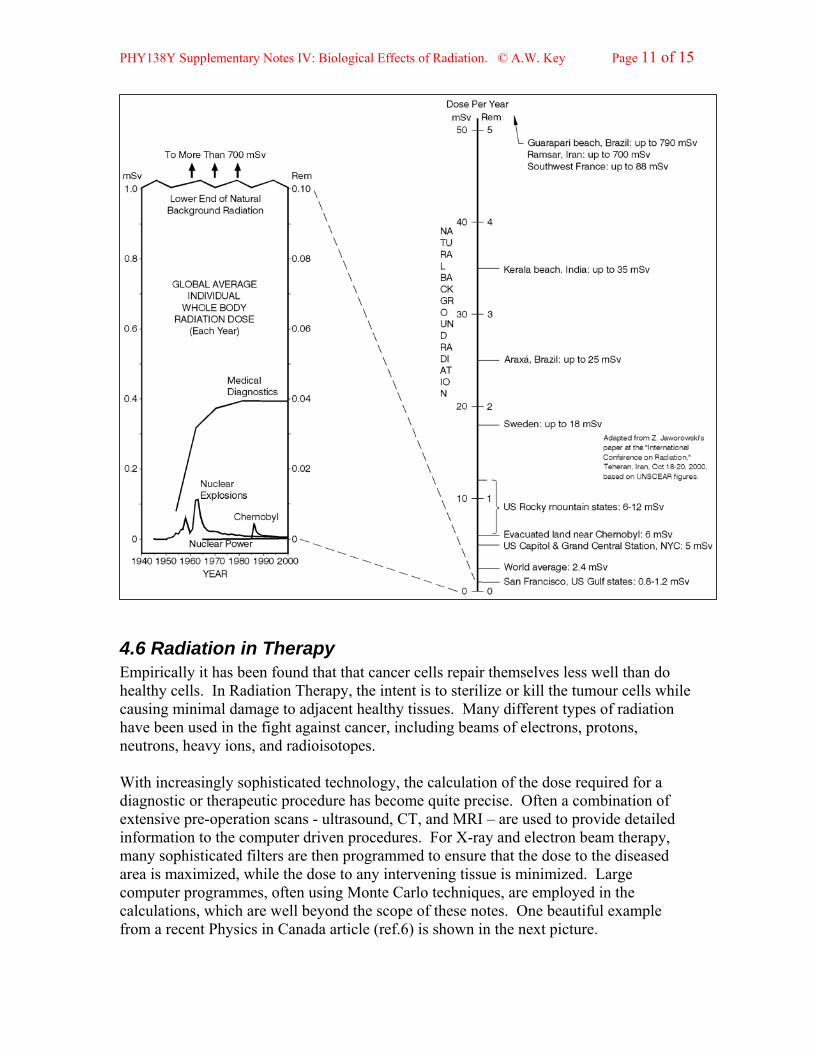
4.6 Radiation in Therapy Empirically it has been found that that cancer cells repair themselves less well than do healthy cells. In Radiation Therapy, the intent is to sterilize or kill the tumour cells while causing minimal damage to adjacent healthy tissues. Many different types of radiation have been used in the fight against cancer, including beams of electrons, protons, neutrons, heavy ions, and radioisotopes. With increasingly sophisticated technology, the calculation of the dose required for a diagnostic or therapeutic procedure has become quite precise. Often a combination of extensive pre-operation scans - ultrasound, CT, and MRI – are used to provide detailed information to the computer driven procedures. For X-ray and electron beam therapy, many sophisticated filters are then programmed to ensure that the dose to the diseased area is maximized, while the dose to any intervening tissue is minimized. Large computer programmes, often using Monte Carlo techniques, are employed in the calculations, which are well beyond the scope of these notes. One beautiful example from a recent Physics in Canada article (ref.6) is shown in the next picture.
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 12 of 15
This shows the results of a calculation of an electron beam treatment designed to avoid dose to the lungs, using a Monte Carlo ‘dose engine’ to generate the isodose lines (the coloured lines along each of which the dose is constant). Both X-rays and electrons are used for Radiation Therapy. However, photons penetrate further in tissue than electrons (see §2.5). Thus gamma or X-rays can produce electrons at depth without causing an excessive dose to the intervening healthy tissue. X-ray energies of several MeV are used for this application. Electron beams, or ‘softer’ X-rays (10 to 100keV) at high exposures are most useful for treating tumours that are close to the surface of the body. Beams of other particles have also been used, though these require more complicated and expensive machinery. Protons or nuclei of helium and more massive charged particles have particularly useful properties; since the rate of energy loss increases rapidly with decreasing particle speed, they give rise to a sharp rise in the ionization near the end of their range. Thus, for such particles, the maximum ionization volume can be precisely defined. In Canada, the only proton radiation therapy facility is located at the Tri-Universities Meson Factory accelerator (TRIUMF) in Vancouver. It is mainly used for treating eye tumours, where very precise irradiation is required. Since healthy cells recover faster than cancer cells, a large number of smaller doses delivered over a period is more effective than one large dose delivered at one time. This is called the fractionation of the dose. When treating a tumour with a fractionated dose, the beam is directed at the tumour from a different direction at each exposure to maximize the dose to the tumour while minimizing the exposure to the surrounding healthy tissue. This is called rotation therapy. A total dose of 50 to 60 Gy, spread over 25 to 30 daily sessions is typical. In addition to beams of electrons and X-rays, radioisotopes are widely used for therapy. The following set of notes, SNV, develops this subject, and gives some examples of simple dose calculations.
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 13 of 15
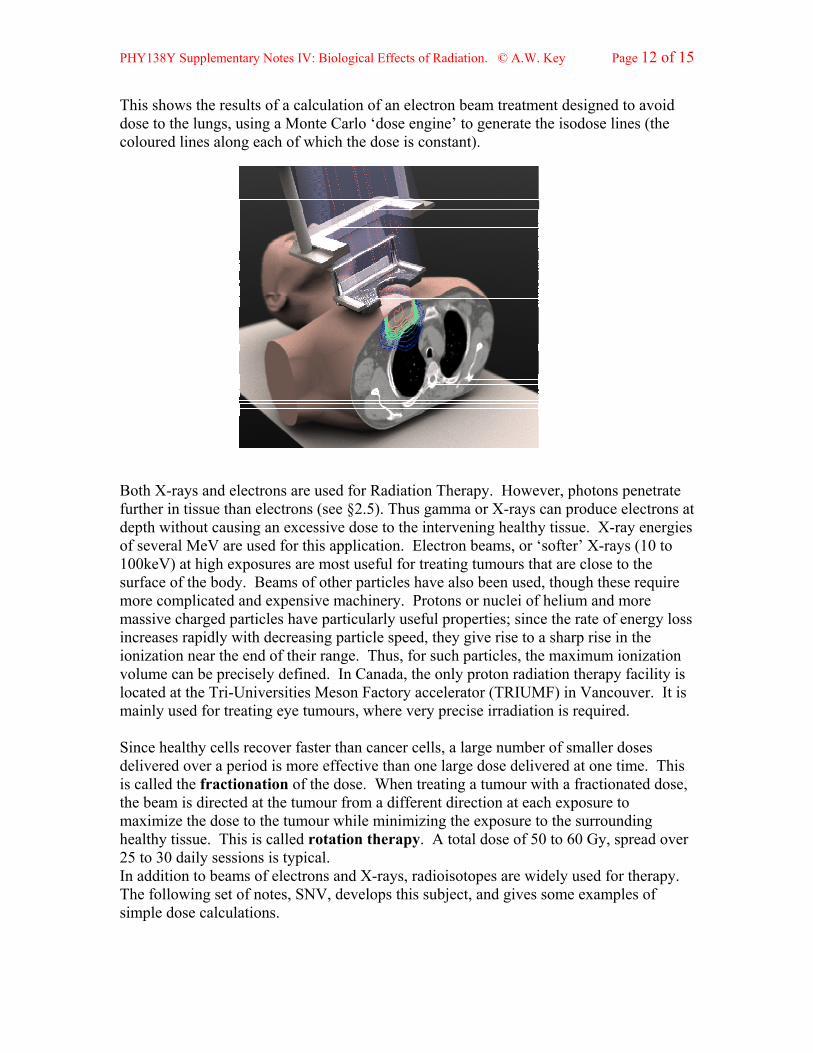
Appendix 4-A. High Dosage Studies The results of the atomic bomb attacks on Hiroshima and Nagasaki at the end of the Second World War might be expected to provide useful data. The exposure in this case was from high energy gammas and neutrons. However, even people located beyond 1 km from the central explosion, where the radiation dose had dropped to around 1 Sv, were killed by the mechanical blast, not by the radiation. Nonetheless, follow-up studies show that survivors of these blasts have greater incidence of cancers than the general population. No. of
People Exposed.
Received Dose (Sv)
No. of Dead
31 1 – 2 0 43 2 – 4 1 21 4 – 6 7 20 > 6 20 Ref.7: D.E.S.& K.G.McNeill
The disaster at Chernobyl, the Ukranian nuclear reactor, provides the best data so far. This accident sent a huge radioactive cloud around the world, and rendered the immediate area unfit for human habitation for the foreseeable future. The table shows the fate of the 115 people most severely exposed (mainly firefighters).
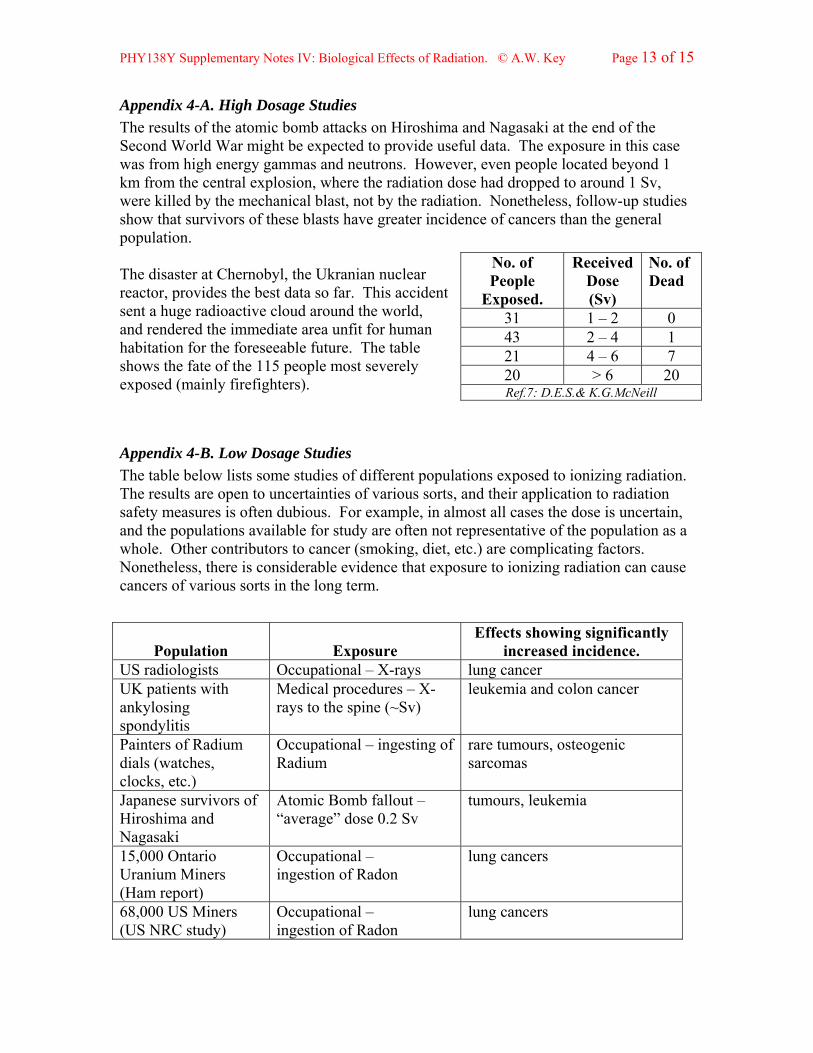
Appendix 4-B. Low Dosage Studies The table below lists some studies of different populations exposed to ionizing radiation. The results are open to uncertainties of various sorts, and their application to radiation safety measures is often dubious. For example, in almost all cases the dose is uncertain, and the populations available for study are often not representative of the population as a whole. Other contributors to cancer (smoking, diet, etc.) are complicating factors. Nonetheless, there is considerable evidence that exposure to ionizing radiation can cause cancers of various sorts in the long term.
Population
Exposure
Effects showing significantly increased incidence.
US radiologists Occupational – X-rays lung cancer UK patients with ankylosing spondylitis
Medical procedures – X-rays to the spine (~Sv)
leukemia and colon cancer
Painters of Radium dials (watches, clocks, etc.)
Occupational – ingesting of Radium
rare tumours, osteogenic sarcomas
Japanese survivors of Hiroshima and Nagasaki
Atomic Bomb fallout – “average” dose 0.2 Sv
tumours, leukemia
15,000 Ontario Uranium Miners (Ham report)
Occupational – ingestion of Radon
lung cancers
68,000 US Miners (US NRC study)
Occupational – ingestion of Radon
lung cancers
PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 14 of 15
There has been considerable fear that the increased environmental radiation caused by the nuclear bomb tests in the 1960’s and the nuclear power plant accidents at Chernobyl or Three Mile Island may have caused a significant increase in world-wide deaths due to cancer. Although the graph in §4.5.2 shows that the effects are small when averaged over the world, the long term effects for people exposed in these accidents is severe. The radioactive fallout from the world’s worst nuclear accident at Chernobyl affects 5 million people, mainly in Ukraine, Belarus, and Russia, and it is now estimated that over 9000 people have died of cancer caused by the radiation. A study of people in the Ukraine who were exposed as children to the fallout from Chernobyl shows that the risk of thyroid cancer rises with the dose received (mainly from 131I in the milk of cows that grazed on contaminated pastures). Effects of the Chernobyl accident have even been detected in areas remote from the Ukraine where radioactive fallout from the accident was detected. For people who were living in some regions of Sweden that received considerable 137Cs fallout, one study has shown a small but statistically significant increase with dose of cancers of all types.
The mutagenesis caused by radiation leads to concerns about long-term genetic effects. These are obviously difficult to study and identify. Results reported by geneticists at the University of Leicester in 2004, show that radiation causes a large increase in the mutation rate of DNA in male reproductive (or germ) cells which increases with dosage. However, though transgeneration effects of radiation-produced mutations have been demonstrated in laboratory mice, there is, so far, no evidence of any statistically significant genetic damage passed on to future generations in any human population (including the progeny of the Japanese atomic bomb survivors).
Appendix 4-C. Risk from Low Dose Rates The rate of dose is also important; obviously a dose received in a fraction of a second (Hiroshima) will have a very different effect from the same dose received over a year (Ontario miners). Attempts to estimate the risk from low dose rates are hampered by the difficulties indicated in §4.5.2. As an example of such a calculation, the U.S. National Council for Radiation Protection and Measurement, using the LNT hypothesis, estimates that between 1 in 10 to 1 in 7 of all lung-cancer deaths (about 15,000 to 22,000 per year in the US) are caused by exposure to naturally occurring radon in the home. In comparison, around 50,000 Americans annually are killed in traffic accidents. However, where data exists, the results seem to indicate that low dose rates of radiation (i.e. those similar to or less than the naturally occurring background) have negligible effects on human biology. One study shows that there is 15% less cancer in US states where the background radiation is high than the US average. Another high-statistics study was carried out in 1980 on two groups of 70,000 people each in China’s Guangdong province (ref. 4). One group had an annual radiation dose of about 1 mSv, while the other had about three times that amount, due to the different terrestrial environment. No short-term or long-term health differences were found between the two groups. Indeed, there has been no statistically significant effect demonstrated at doses below about 100 mSv at any dose rate.

PHY138Y Supplementary Notes IV: Biological Effects of Radiation. © A.W. Key Page 15 of 15
These facts have led several researchers to question the validity of the dose limits considered safe by the NCRP and other regulatory bodies. Dr. Gunnar Walinder, the renowned Swedish radiobiologist (an associate of Rolf Sievert) even has a monograph entitled Has Radiation Protection Become a Health Hazard? (see ref. 14). Zbigniew Jaworowski (ref. 4) has pointed out that “the fear of small doses … is about as justified as the fear that a … temperature of 20 oC may be hazardous because, at 200 oC, one can easily get third degree burns”.
There is even some suggestion that exposure to radiation may be hormetic (meaning that low doses have a beneficial effect, while higher doses may be harmful). While this concept has not been endorsed by any of the regulatory radiation agencies, it has not been disproved, and does have its adherents. Several old gold and uranium mines in Montana even boast of the health advantages of low levels of radiation, and, for a fee, you can sit in the mines to breathe in the radon gas and drink the radioactive water! Recently, Professor Doug Boreham of McMaster University has shown that developing mouse fetuses are protected by prior exposure to low doses of radiation against the effects of in utero irradiation that interfere with normal embryonic development. His work also suggests that genetic effects can influence the risk of radiation damage.
Appendix 4-D. Backup Reading in Knight The table lists some of the relevant sections in Knight.
Section in SNIV Corresponding Sections in Knight
4.2.1, 4.2.2 42.7 (p. 1373,1374) 4.3.1 42.5 (p.1367,1368)
1 May 2007