phyllodes breast tumor joint hospital surgical grand round 26 april 2014 ng yuen shan, sandy (tuen...
TRANSCRIPT

Phyllodes breast tumor
Joint Hospital Surgical Grand Round26 April 2014
Ng Yuen Shan, Sandy(Tuen Mun Hospital)

Phyllodes tumor Rare fibroepithelial breast tumor (1% of all
breast tumors, 2.5% of all fibroepithelial tumors)
A spectrum of disease Epithelial and cellular stromal component Histological classification:
Benign (60%) Borderline (20%) Malignant (20%) distant metastasis

Median age of presentation at 40-50 years Palpable mass with rapid growth, large size
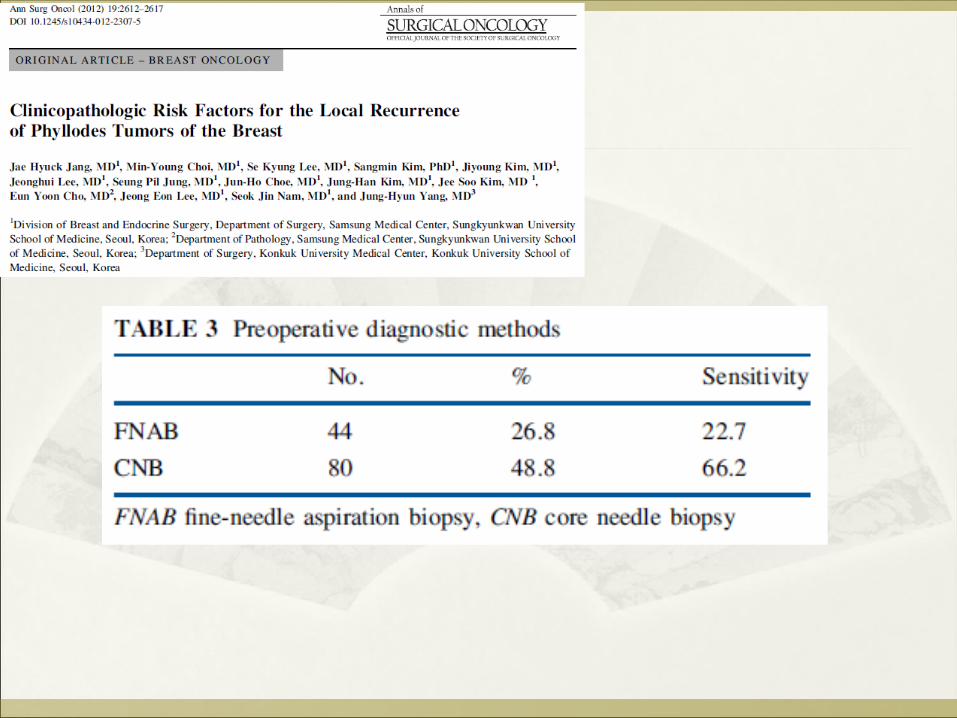
(>2cm) Poor pre-operative diagnostic accuracy

Case scenario
F/40 2.5cm L12H breast mass, interval growth. MMG/US: well-circumscribed lobulated mass FNAC: benign. Excisional pathology:
Benign phyllodes tumor Margin POSITIVE
Pok Oi Hospital A review of 28 consecutive patients with phyllodes
tumour excision in 2009-2012 in Pok Oi Hospital 11 operations performed for recurrent phyllodes tumour
(6 patients) have been excluded.

Operation type Indication Total no.
Margin +ve
Simple enucleation
Benign breast mass 5 3 (60%)
Wide local excision
Clinical/ pathological diagnosis of phyllodes tumour
20 2 (10%)
Mastectomy Large tumor-breast ratio, or suspicious malignant
4 1 (25%)

Margin status and histological grade
Involved Touch/ close <1 cm >/= 1 cm
Malignant 2 0 4 2
Borderline 1 2 3 3
Benign 3 3 3 3
Close follow-up

Margin-involved outcomes Age Grade Tumour
size (cm)Primary Operation
FU duration (months)
Lost to FU
Reoperation
Patient A 63 Malignant 3.2 WLE 48 No No
Patient B 48 Malignant 11 Mastectomy 18 No No
Patient C 42 Borderline 6 WLE 14 No Mastectomy for co-existing DCIS
Patient D 50 Benign 7.5 Enucleation 57 No Wide local excision for recurrent phyllodes
Patient E 21 Benign 3.5 Enucleation 35 Yes No
Patient F 40 Benign 2.2 Enucleation 47 No No
Mean FU period: 36 months
POH case series
Results:Local recurrence rate in margin-involved = 16.7%No recurrence was detected in close or clear margin.
Conclusion: Margin status of the primary resection is probably the most important factor in determining risk of recurrence.

Margin-involved phyllodes tumor
Why does it matter? What to do next? How to “prevent”?
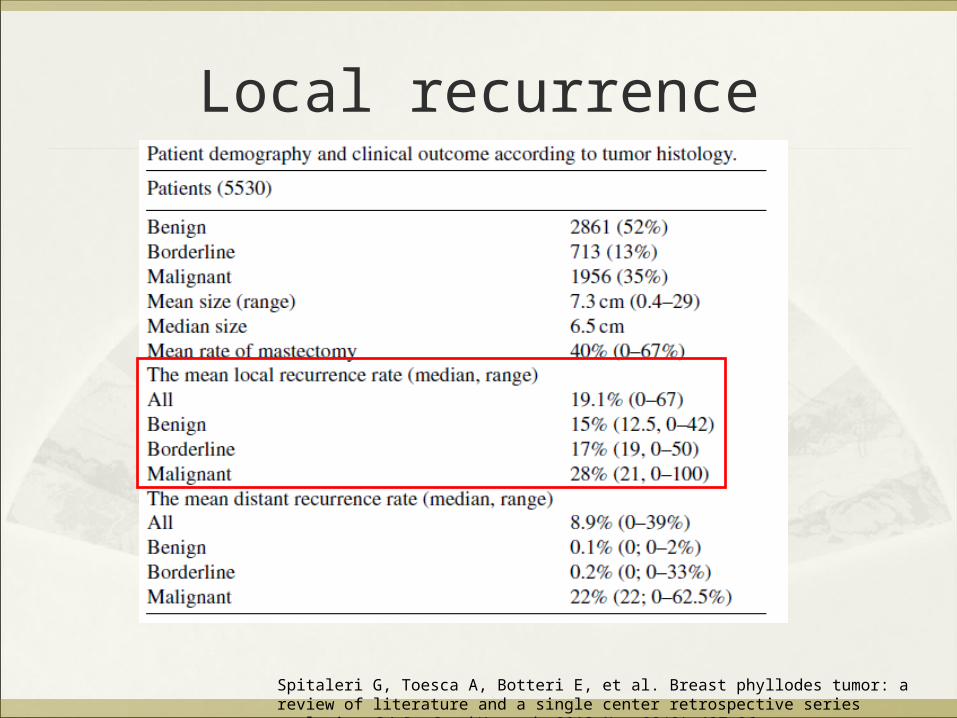
Local recurrence
Spitaleri G, Toesca A, Botteri E, et al. Breast phyllodes tumor: a review of literature and a single center retrospective series analysis. Crit Rev Oncol Hematol. 2013 Nov;88(2):427-36.
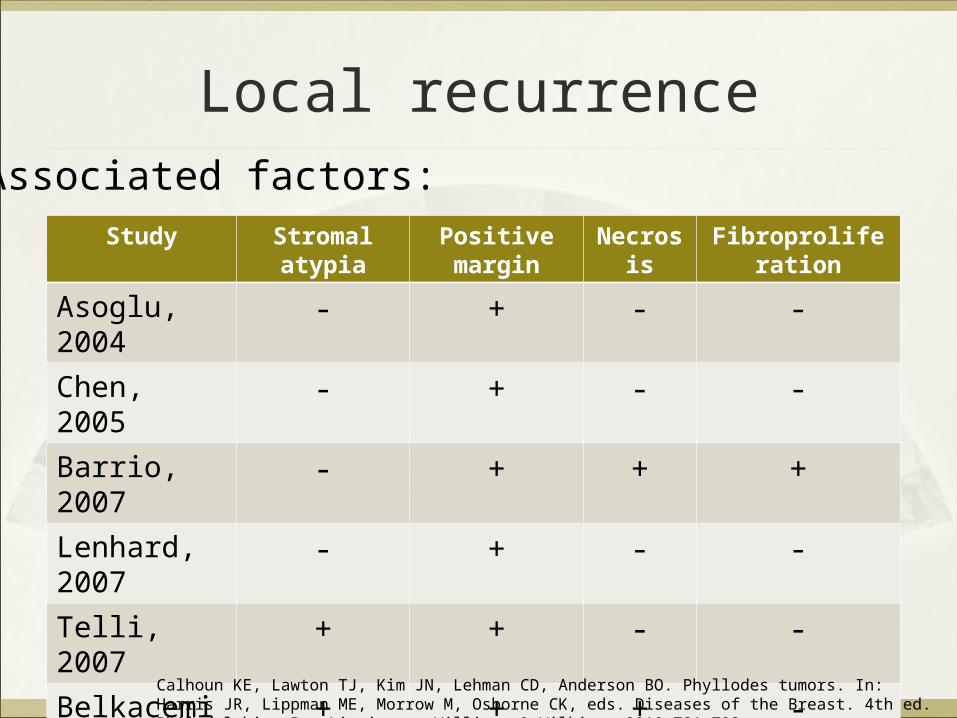
Local recurrence
Study Stromal atypia Positive margin Necrosis Fibroproliferation
Asoglu, 2004 - + - -Chen, 2005 - + - -Barrio, 2007 - + + +Lenhard, 2007 - + - -Telli, 2007 + + - -Belkacemi, 2008
+ + + -
Associated factors:
Calhoun KE, Lawton TJ, Kim JN, Lehman CD, Anderson BO. Phyllodes tumors. In: Harris JR, Lippman ME, Morrow M, Osborne CK, eds. Diseases of the Breast. 4th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2010:781-792.
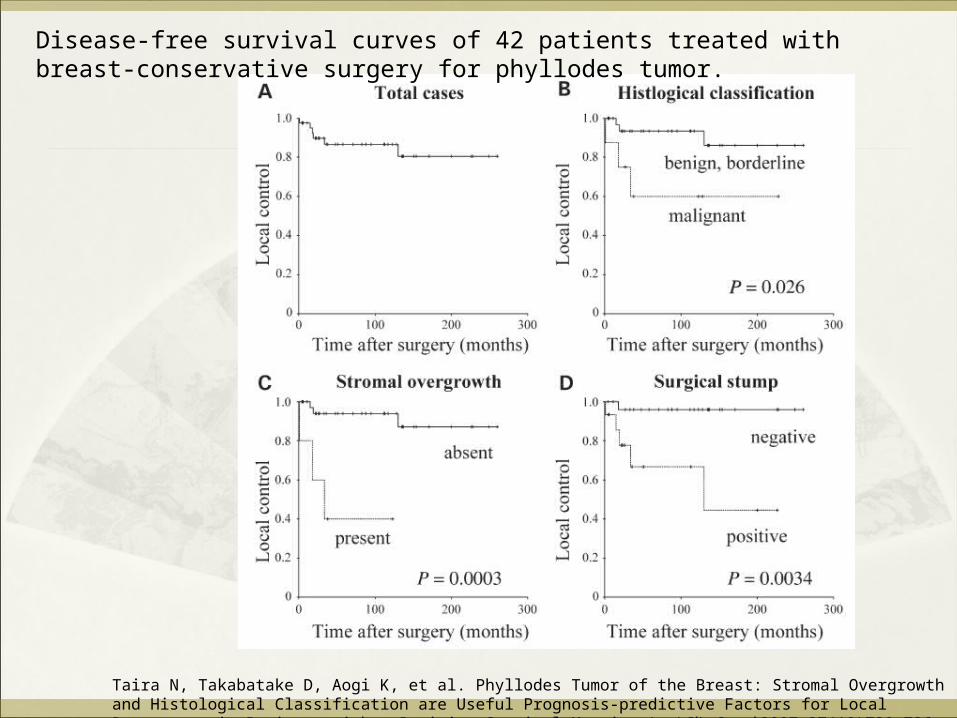
Disease-free survival curves of 42 patients treated with breast-conservative surgery for phyllodes tumor.
Taira N, Takabatake D, Aogi K, et al. Phyllodes Tumor of the Breast: Stromal Overgrowth and Histological Classification are Useful Prognosis-predictive Factors for Local Recurrence in Patients with a Positive Surgical Margin. Jpn J Clin Oncol 2007;37(10)730–736

Taira N, Takabatake D, Aogi K, et al. Phyllodes Tumor of the Breast: Stromal Overgrowth and Histological Classification are Useful Prognosis-predictive Factors for Local Recurrence in Patients with a Positive Surgical Margin. Jpn J Clin Oncol 2007;37(10)730–736

Margin-involved phyllodes tumor
Why does it matter? Predictor of local recurrence
What to do next? How to “prevent”?

Stromal growth as a predictive factor of local recurrence in positive margin cases One of the malignant features
Taira N, Takabatake D, Aogi K, et al. Phyllodes Tumor of the Breast: Stromal Overgrowth and Histological Classification are Useful Prognosis-predictive Factors for Local Recurrence in Patients with a Positive Surgical Margin. Jpn J Clin Oncol 2007;37(10)730–736
If margin positive…

If margin positive…
Some authors had suggested “wait-and-see” policy for benign phyllodes tumor
Chua, 1989 (106 patients)
Zurrida, 1992 (216 patients): recurrence 8%
Chua CL, Thomas A, Ng BK. Cystosarcoma phyllodes: a review of surgical options. Surgery 1989;105(2 Pt 1):141-147Zurrida S, Bartoli C, Galimberti V, et al. Which therapy for unexpected phyllodes tumour of the breast? Eur J Cancer 1992;28(2-3):654-657
Management strategy ofMargin-involved phyllodes tumor
Benign “wait-and-see” Malignant Re-excision Follow-up every 6 months for initial 2-3 years
(highest chance of recurrence) Then yearly Self breast examination Clinical suspicion on follow-up: triple assessment

Margin-involved phyllodes tumor
Why does it matter? What to do next? How to “prevent”?

Phyllodes tumor
Difficult preoperative diagnosis…..
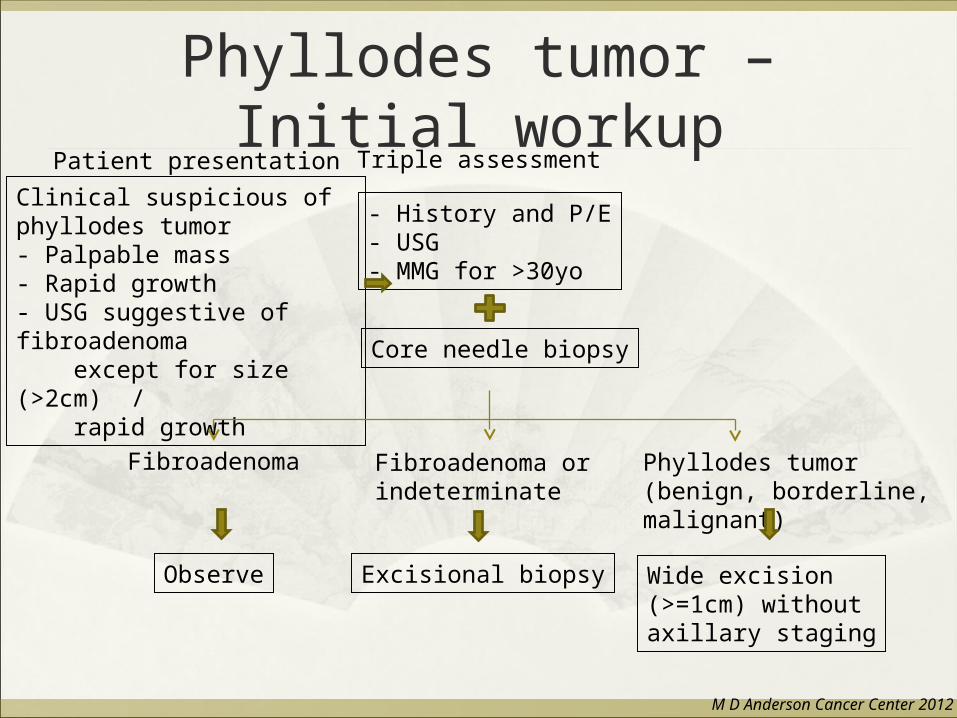
Phyllodes tumor – Initial workup
Clinical suspicious of phyllodes tumor- Palpable mass- Rapid growth- USG suggestive of fibroadenoma except for size (>2cm) / rapid growth
- History and P/E- USG- MMG for >30yo
Core needle biopsy
Fibroadenoma or indeterminate
Phyllodes tumor (benign, borderline, malignant)
Observe
Fibroadenoma
Excisional biopsy Wide excision (>=1cm) without axillary staging
Patient presentation Triple assessment
M D Anderson Cancer Center 2012
Margin-involved phyllodes tumor
Why does it matter What to do next How to “prevent”
?

Thank you
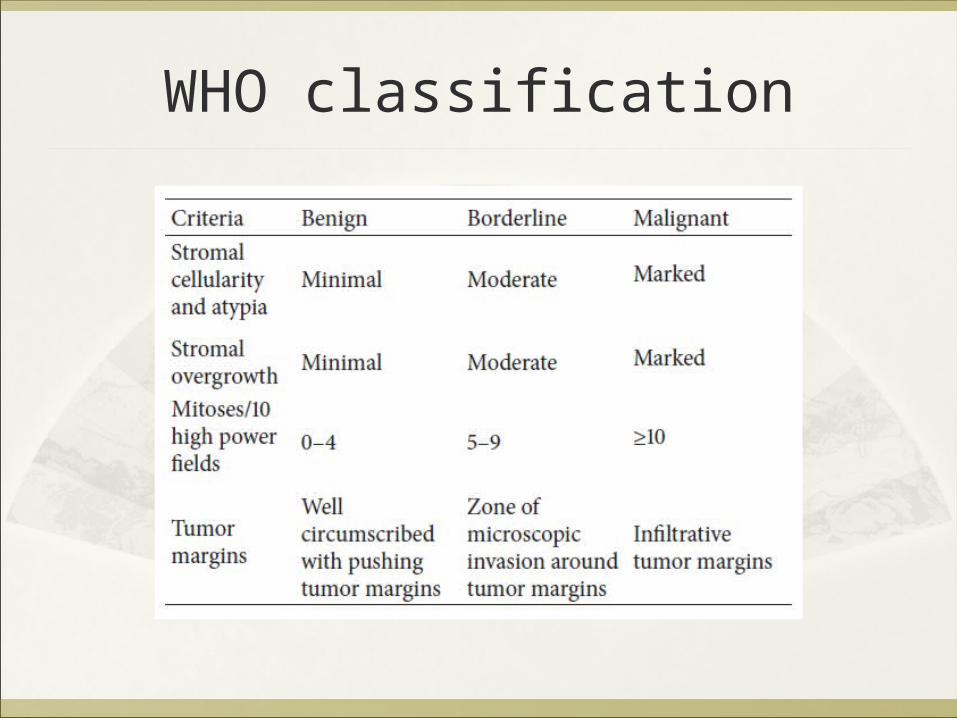
WHO classification
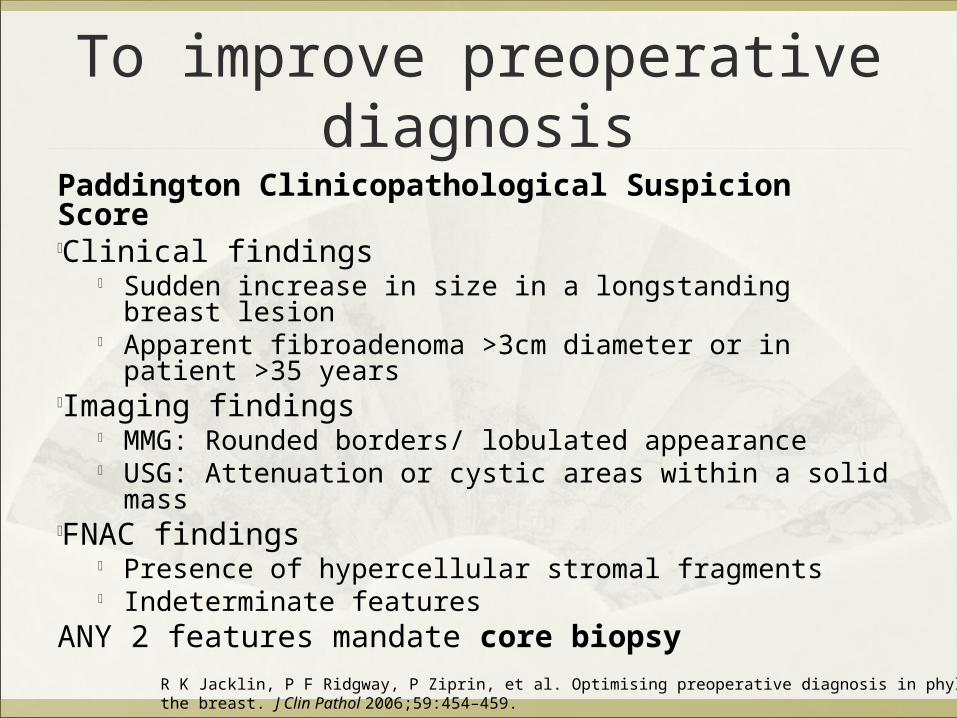
To improve preoperative diagnosisPaddington Clinicopathological Suspicion ScoreClinical findings
Sudden increase in size in a longstanding breast lesion Apparent fibroadenoma >3cm diameter or in patient >35
yearsImaging findings
MMG: Rounded borders/ lobulated appearance USG: Attenuation or cystic areas within a solid mass
FNAC findings Presence of hypercellular stromal fragments Indeterminate features
ANY 2 features mandate core biopsyR K Jacklin, P F Ridgway, P Ziprin, et al. Optimising preoperative diagnosis in phyllodes tumour ofthe breast. J Clin Pathol 2006;59:454–459.

Phyllodes tumor - Recurrence
Local recurrent breast mass after excision of phyllodes tumor
- History and P/E- MMG, USG- Core needle biopsy- Consider chest imaging
No metastatic disease Metastatic disease
Re-excision with wide margins without axillary staging
Consider post-op RT
As soft tissue sarcoma
Patient presentation Workup
M D Anderson Cancer Center 2012