physician advisor clinical documentation integrity wolfson … newborn... · 2019-05-03 · abo...
TRANSCRIPT
J. Douglas Campbell MDPhysician AdvisorClinical Documentation IntegrityWolfson Children’s Hospital





Single live newborn with ankyloglossia
ROM – 1 SOI ‐ 1
BCBS ‐ improved reimbursementMedicaid (Staywell) no change
Minimum Documentation Required: 1. Lactation nurse to assess feeding secondary to anklyoglossia2. Follow up ankyloglossia with pediatrician / ENT


Single live newborn withcongenital hip dysplasia
ROM – 1SOI ‐ 1
BCBS ‐ improved reimbursementMedicaid (Staywell) – no change
Minimum Documentation Required ‐Presumed (suspected/probable/likely) developmental dysplasia ofthe hip (DDH) will require follow‐up hip ultrasound.

Single live newborn with Breech presentation
ROM –2SOI ‐ 1
BCBS –$ improved reimbursementMedicaid (Staywell) $improved
Minimum Documentation Required:Breech presentation – will require follow‐up ultrasound


Single live newborn with LGA
ROM – 1SOI ‐ 1
BCBS – no changeMedicaid (Staywell) – no change
Infants whose weight exceeds the 90th percentile for gestational age are classified as LGA
Minimum Documentation Required:Infant is LGA
Single live newborn withSGA
ROM –2SOI ‐ 1
BCBS – improved reimbursementMedicaid (Staywell) – improved
Minimum Documentation Required:Infant is SGA
Infants whose birthweight is below the 10th percentile, when plotted against gestational ageon a standard growth curve, are considered small for gestational age (SGA)

Single live newborn with Hypoglycemia
ROM –2SOI ‐ 1
BCBS – improved reimbursementMedicaid (Staywell) ‐ improved
Definition – blood glucose < 40 mg/dl & treated with GluTose gel or IV glucose
NOT treated with only formula or breast feeding

And the word HYPOGLYCEMIA
Not ‐ Low blood sugar Not ‐ Low serum glucose
Minimum Documentation Required:Hypoglycemia

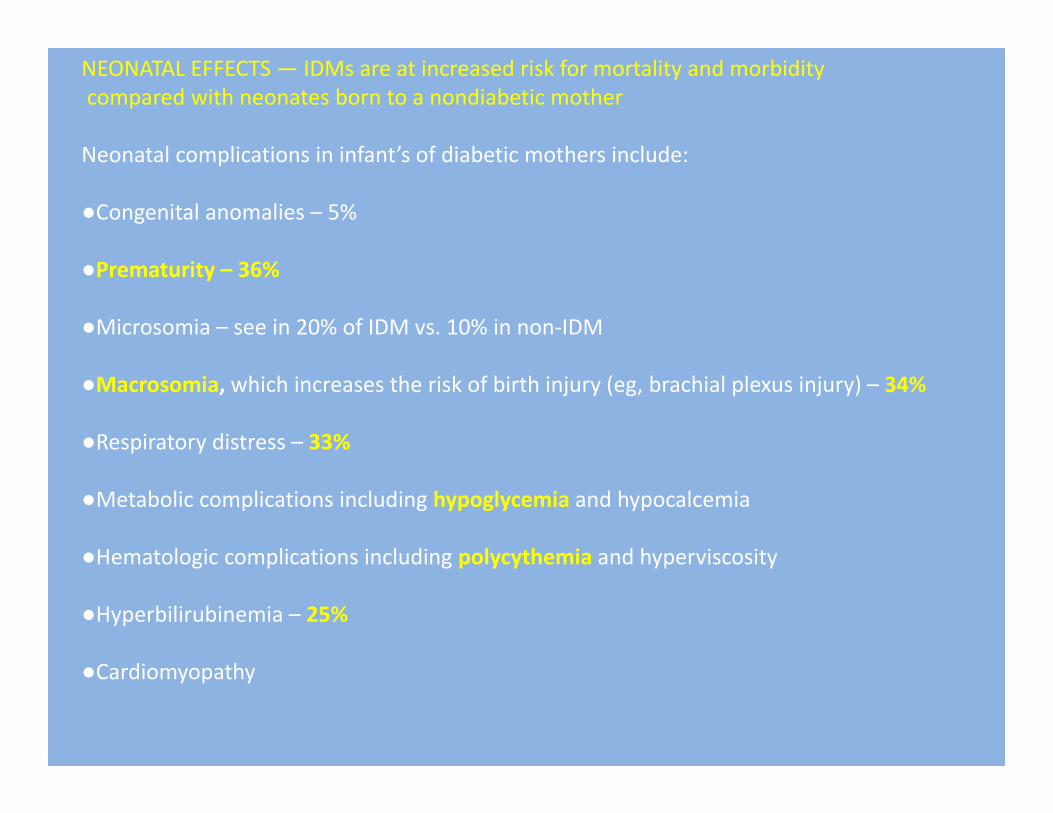
NEONATAL EFFECTS — IDMs are at increased risk for mortality and morbiditycompared with neonates born to a nondiabetic mother
Neonatal complications in infant’s of diabetic mothers include:
●Congenital anomalies – 5%
●Prematurity – 36%
●Microsomia – see in 20% of IDM vs. 10% in non‐IDM
●Macrosomia, which increases the risk of birth injury (eg, brachial plexus injury) – 34%
●Respiratory distress – 33%
●Metabolic complications including hypoglycemia and hypocalcemia
●Hematologic complications including polycythemia and hyperviscosity
●Hyperbilirubinemia – 25%
●Cardiomyopathy

Despite the propensity for abnormalities associated with maternal diabetes, many IDM’s are born without any complications or abnormalities

Single live newborn that is“Infant of diabetic mother”
ROM ‐ 1SOI ‐ 1
BCBS ‐ no change Medicaid (Staywell) – no change
Minimal Documentation Required :Infant of diabetic mother with gestational / Non‐gestational diabetes (Type I or Type II)
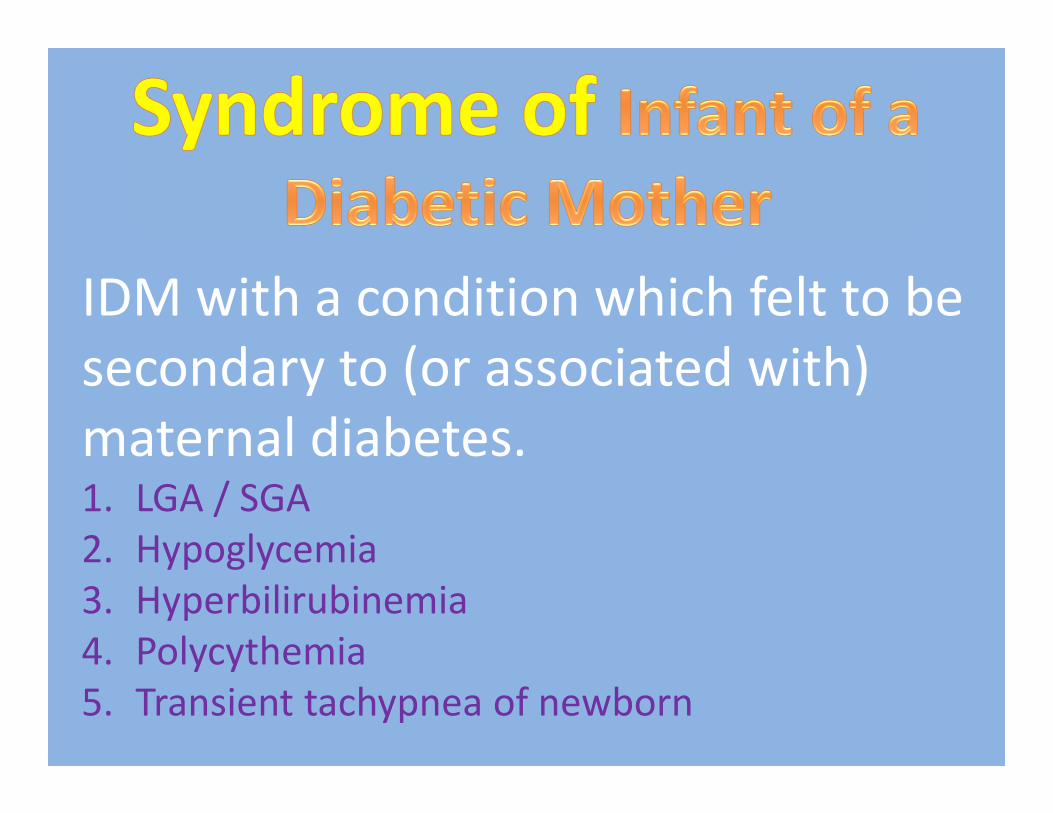
IDM with a condition which felt to be secondary to (or associated with)maternal diabetes.1. LGA / SGA2. Hypoglycemia3. Hyperbilirubinemia4. Polycythemia5. Transient tachypnea of newborn

Single live newborn with “Syndrome of infant ofdiabetic mother”
ROM ‐2SOI ‐ 1
BCBS – improved reimbursementMedicaid (Staywell) ‐ improved
Let’s l k at documentation:
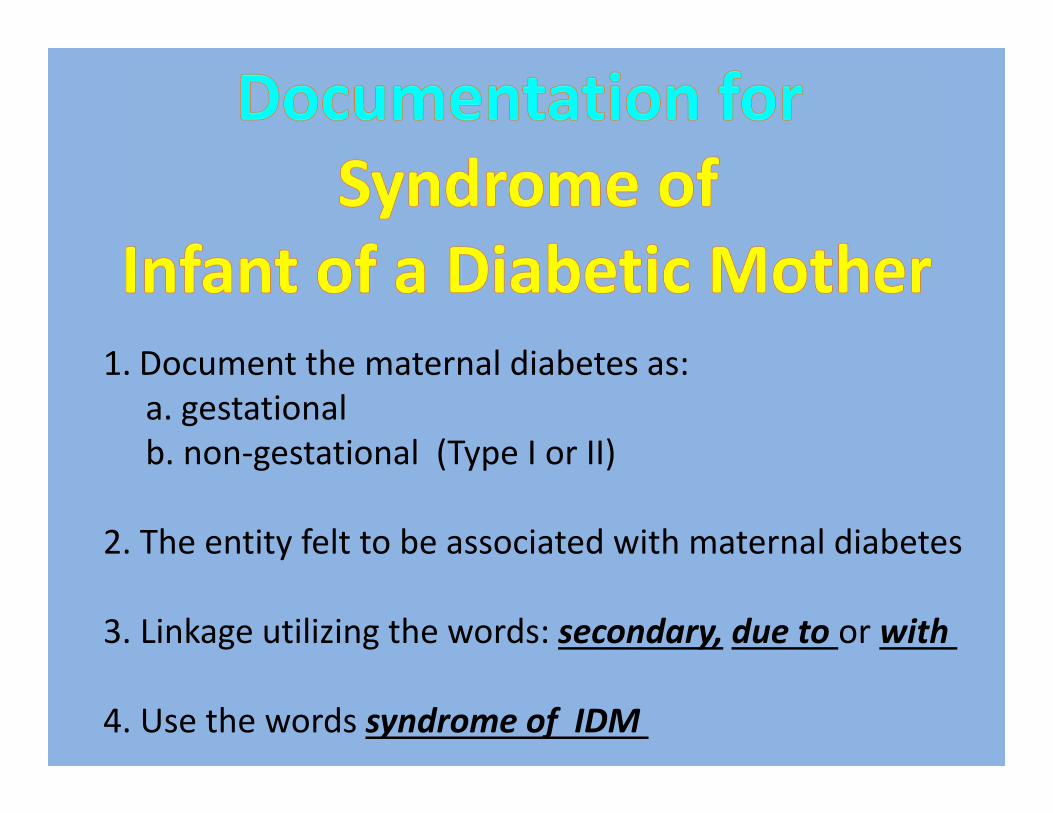
1. Document the maternal diabetes as: a. gestational b. non‐gestational (Type I or II)
2. The entity felt to be associated with maternal diabetes
3. Linkage utilizing the words: secondary, due to or with
4. Use the words syndrome of IDM
1. Infant large for gestation age secondary to syndromeof infant of a diabetic mother with gestational diabetes
2. Infant small for gestation age due to syndromeof infant of a diabetic mother with Type I diabetes
3. Infant with hypoglycemia secondary to syndromeof infant of a diabetic mother with Type II diabetes
4. Infant with polycythemia with syndromeof infant of a diabetic mother with gestational diabetes
Secondary to > due to >> with

ABO Isoimmunization
Mother Blood group O – newborn type A or BSome Group O moms have anti‐A, anti‐B IgG antibodiesCan result in hemolysis in fetus/newbornMore common and more severe in African AmericansCan occur with first pregnancy Less severe than Rh incompatibility 55/1000 live births

1.Coombs2.Hemoglobin 3.Reticulocyte count4.Bilirubin
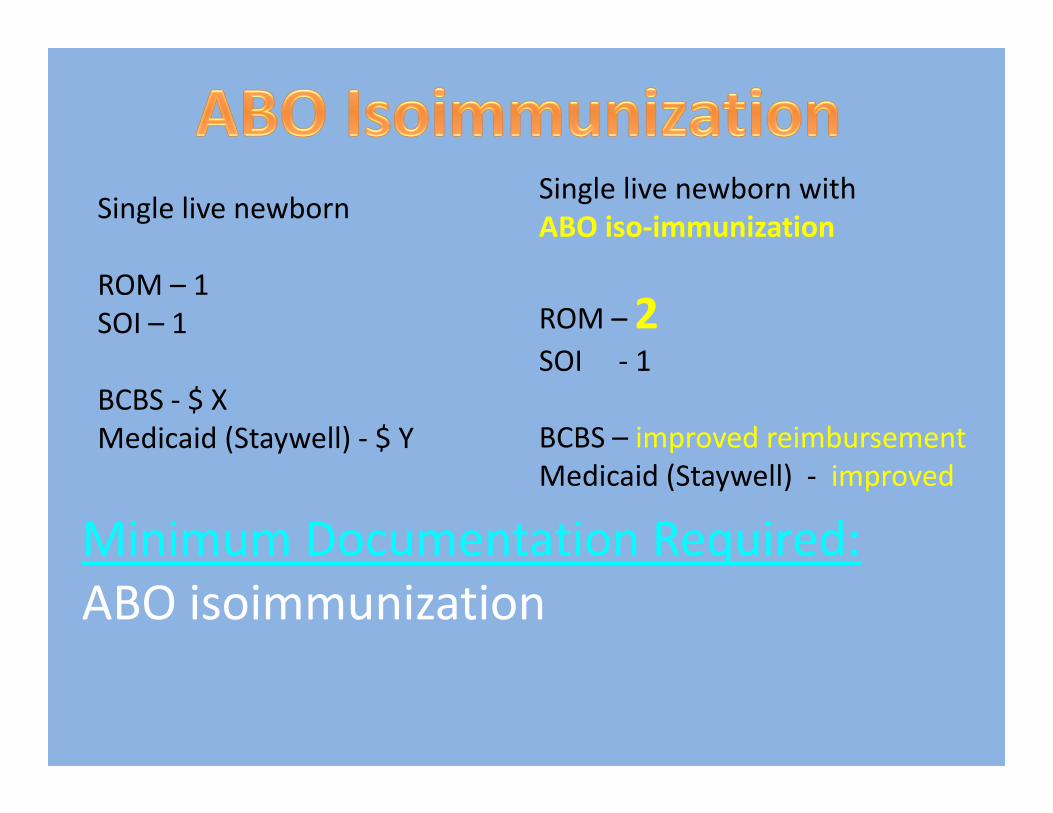
Single live newborn with ABO iso‐immunization
ROM –2SOI ‐ 1
BCBS – improved reimbursementMedicaid (Staywell) ‐ improved
Minimum Documentation Required:ABO isoimmunization
Single live newborn
ROM – 1SOI – 1
BCBS ‐ $ XMedicaid (Staywell) ‐ $ Y


< 37 completed weeks gestation
Minimum Documentation Required :Premature / Preterm


Why leave iton the tree?
Why leave it on the table?