pi di dpain disorders - beat the boards! 30_anderson pain 2010.pdf · pi di dpain disorders...
TRANSCRIPT

P i Di dPain Disorders
Christopher Todd Anderson, MDChristopher Todd Anderson, MDUniversity of PennsylvaniaUniversity of PennsylvaniaUniversity of PennsylvaniaUniversity of [email protected]@mail.med.upenn.edu

Lecture ContentLecture Content PretestPretest DefinitionsDefinitions Basic anatomyBasic anatomy
Nociceptors, pathwaysNociceptors, pathways
Neuropathic painNeuropathic painS ll fib h l fib hS ll fib h l fib h Small fiber neuropathy vs. large fiber neuropathySmall fiber neuropathy vs. large fiber neuropathy
Injury and syndromesInjury and syndromes P tP t h ti l i TN / GN B t TENSh ti l i TN / GN B t TENS PostPost--herpetic neuralgia, TN / GN, Botox, TENS, herpetic neuralgia, TN / GN, Botox, TENS,
systemic disease, systemic disease, RadiculopathyRadiculopathy p yp y
2

Lecture Content continuedLecture Content continued Complex regional pain syndromesComplex regional pain syndromes Complex regional pain syndromesComplex regional pain syndromes ParsonageParsonage--TurnerTurner Central pain syndromesCentral pain syndromes Central pain syndromesCentral pain syndromes
Thalamic pain, phantom painThalamic pain, phantom pain
FibromyalgiaFibromyalgia FibromyalgiaFibromyalgia PosttestPosttest
3

Pretest

Question 1: A patient presents with a 1 year Q p p yhistory of a dysesthetic band like sensation around his feet up to his shins, he has p ,preserved strength and reflexes. The highest yield test is:y1.1. EMGEMG22 Nerve biopsyNerve biopsy2.2. Nerve biopsyNerve biopsy3.3. Broad lab panelBroad lab panel4.4. Skin biopsySkin biopsy5.5. Nerve conduction study for small fiber Nerve conduction study for small fiber yy
neuropathyneuropathy5

Question 2: TRPM8 is activated by
1.1. PinPin--prickprick22 HeatHeat2.2. HeatHeat3.3. ColdCold
A k f “A k f “k lk l ” i h i i Chi” i h i i Chi4.4. A pack of “A pack of “koolskools” in the winter in Chicago” in the winter in Chicago5.5. Scalding coffeeScalding coffee6.6. A chemical burn or lacerationA chemical burn or laceration
6

Question 3: Post-herpetic neuralgia:Question 3: Post herpetic neuralgia:
1.1. Follows reactivation of HHVFollows reactivation of HHV--662.2. Cannot be prevented but can be treatedCannot be prevented but can be treated3.3. Always is heralded by a dermatomal vesicular Always is heralded by a dermatomal vesicular 3.3. ways s e a ded by a de ato a ves cu aways s e a ded by a de ato a ves cu a
rashrash4.4. Should not associated with abnormal CSFShould not associated with abnormal CSF5.5. Has an FDAHas an FDA--approved vaccineapproved vaccine
7

Question 4: The etiology of Dejerine-Question 4: The etiology of Dejerine-Roussy syndrome is usually:
1.1. TumorTumor22 IdiopathicIdiopathic2.2. IdiopathicIdiopathic3.3. TraumaTrauma
S kS k4.4. StrokeStroke5.5. CNS infectionCNS infection6.6. Degenerative diseaseDegenerative disease
8

Question 5: Fibromyalgia
1.1. ExistsExists2.2. Does not existDoes not exist3.3. Has formal diagnostic criteriaHas formal diagnostic criteria4.4. Can be fatalCan be fatal5.5. Is more common in men and the elderlyIs more common in men and the elderly66 Has abnormal EMGHas abnormal EMG--NCS correlatesNCS correlates6.6. Has abnormal EMGHas abnormal EMG NCS correlatesNCS correlates
9
Some Definitions
HyperalgesiaHyperalgesia Extreme sensitiveness to painful stimuliExtreme sensitiveness to painful stimuli
Allodynia Allodynia Pain in response to a nonPain in response to a non--noxious mechanical stimulinoxious mechanical stimuli
HyperesthesiaHyperesthesiaAbnormal sensitivity to sensory stimulusAbnormal sensitivity to sensory stimulus
10 (Lancet, Vol. 353 May 8, 1999, J M Besson The Neurobiology of Pain)

Some Definitions (IASP)
Causalgia:Causalgia:A syndrome with sustained burning pain,A syndrome with sustained burning pain,A syndrome with sustained burning pain, A syndrome with sustained burning pain,
allodynia, and hyperpathia after a traumatic allodynia, and hyperpathia after a traumatic nerve lesionnerve lesion
Often combined with Often combined with vasomotor and sudomotor vasomotor and sudomotor dysfunction anddysfunction and
Later Later trophictrophic changeschanges
11
Some Definitions (IASP)
DysesthesiaDysesthesiaUnpleasant abnormal sensationsUnpleasant abnormal sensations——spontaneousspontaneousUnpleasant abnormal sensationsUnpleasant abnormal sensations spontaneous spontaneous
or evokedor evokedA dysesthesia should always be unpleasant A dysesthesia should always be unpleasant y y py y pA paresthesia should not be unpleasantA paresthesia should not be unpleasantIt should always be specified whether theIt should always be specified whether theIt should always be specified whether the It should always be specified whether the
sensations are spontaneous or evokedsensations are spontaneous or evoked
12

Some Definitions (IASP)Some Definitions (IASP) HyperpathiaHyperpathia HyperpathiaHyperpathiaA painful syndrome characterized by an A painful syndrome characterized by an
abnormally painfulabnormally painful reaction to a stimulusreaction to a stimulusabnormally painful abnormally painful reaction to a stimulusreaction to a stimulus, , especially a repetitive stimulusespecially a repetitive stimulus
It may occur with allodynia hyperesthesiaIt may occur with allodynia hyperesthesiaIt may occur with allodynia, hyperesthesia, It may occur with allodynia, hyperesthesia, hyperalgesia, or dysesthesiahyperalgesia, or dysesthesia
Faulty identification and localization of theFaulty identification and localization of theFaulty identification and localization of the Faulty identification and localization of the stimulus, delay, radiating sensation, and afterstimulus, delay, radiating sensation, and after--sensation may be presentsensation may be present
13
Some Definitions (IASP)
NociceptorNociceptorA receptor preferentially sensitive to a noxious A receptor preferentially sensitive to a noxious p p yp p y
stimulus or to a stimulus which would become stimulus or to a stimulus which would become noxious if prolongednoxious if prolonged
Noxious stimulusNoxious stimulusA noxious stimulus is one which is or could be A noxious stimulus is one which is or could be
damaging to tissuedamaging to tissue
14
Pain Receptors (Nociceptors)Pain Receptors (Nociceptors) Nociceptors exist as nearly free nerve endingsNociceptors exist as nearly free nerve endingsp y gp y gThermal or Thermal or mechanicalmechanical AA——delta fibers delta fibers
Conduct at 5Conduct at 5––30 meters / sec. (faster)30 meters / sec. (faster)They convey sharp prickling sensationsThey convey sharp prickling sensationsThey have a small receptive fieldThey have a small receptive field
PolymodalPolymodal nociceptors, unmyelinated C fibersnociceptors, unmyelinated C fibersThey respond to mechanical stimulation, orThey respond to mechanical stimulation, orChemical stimulation, or Chemical stimulation, or HeatHeat
They conduct more slowly at 0 5They conduct more slowly at 0 5 2 meters/sec2 meters/secThey conduct more slowly at 0.5They conduct more slowly at 0.5––2 meters/sec2 meters/sec Innervate approximately 1 square cm of skinInnervate approximately 1 square cm of skin15

Pain Receptors (Nociceptors)Pain Receptors (Nociceptors) CC--polymodal nociceptors (CPNs)polymodal nociceptors (CPNs)With enough stimulation they cause local With enough stimulation they cause local
vasogenic responsevasogenic response——reddened skinreddened skinCause an “axonal reflex” through a network of Cause an “axonal reflex” through a network of
dermal afferent fibersdermal afferent fibersFeedback to cause inflammation around the area of Feedback to cause inflammation around the area of
stimulationstimulation
Naturally occurring agents can activate andNaturally occurring agents can activate and Naturally occurring agents can activate and Naturally occurring agents can activate and sensitize nociceptorssensitize nociceptors
K i b d ki i hi i (fK i b d ki i hi i (fK+, serotonin, bradykinin, histamine (from K+, serotonin, bradykinin, histamine (from mast cells), Substance P….mast cells), Substance P….16
Menthol Receptor, TRPM8
A receptor for environmental cold and A receptor for environmental cold and mentholmenthol
“TRP“TRP melastatinmelastatin 8 or cold + menthol8 or cold + menthol TRP TRP melastatinmelastatin 8 or cold + menthol 8 or cold + menthol receptor 1 (CMR1)receptor 1 (CMR1)——is activated by is activated by chemical cooling agents (such as menthol)chemical cooling agents (such as menthol)chemical cooling agents (such as menthol) chemical cooling agents (such as menthol) or when temperatures drop below 26or when temperatures drop below 26 °°C”C”
17Nature 448, 204-208 (12 July 2007)

Menthol Receptor TRPM8Menthol Receptor TRPM8
18

Capsaicin Receptor (TRPV1)Capsaicin Receptor (TRPV1) “Transient receptor potential cation channel, “Transient receptor potential cation channel,
subfamily V, member 1” subfamily V, member 1” Activated by:Activated by:HeatHeatCapsaicinCapsaicinLo pHLo pHLow pHLow pH
Sensitized by inflammationSensitized by inflammation Desensitized by prolonged exposure toDesensitized by prolonged exposure to Desensitized by prolonged exposure to Desensitized by prolonged exposure to
capsaicincapsaicinThis is a proposed analgesic mechanism ofThis is a proposed analgesic mechanism ofThis is a proposed analgesic mechanism of This is a proposed analgesic mechanism of
capsaicincapsaicin19

M ReceptorsMu Receptors MuMu——receptors are opioid receptorsreceptors are opioid receptors MuMu receptors are opioid receptorsreceptors are opioid receptors They exist inThey exist in
Th d l hTh d l hThe dorsal hornThe dorsal hornOn terminals of nociceptor afferentsOn terminals of nociceptor afferentsDendrites of postsynaptic neuronsDendrites of postsynaptic neurons
TheyTheyInhibit the release of glutamateInhibit the release of glutamateInhibit the release of substance PInhibit the release of substance PInhibit the release of other neurotransmittersInhibit the release of other neurotransmitters
20

N i tNociceptors
Cell bodies are located in the dorsal root Cell bodies are located in the dorsal root ganglia and trigeminal gangliaganglia and trigeminal ganglia
Project to wideProject to wide--dynamic range neurons indynamic range neurons inProject to wideProject to wide dynamic range neurons in dynamic range neurons in spinal cord and then to contralateral spinal cord and then to contralateral corticospinal tract (and interneurons)corticospinal tract (and interneurons)corticospinal tract (and interneurons)corticospinal tract (and interneurons)
Thi d d i th th lThi d d i th th l Third order neurons are in the thalamusThird order neurons are in the thalamus21
Projections of A delta and C fibersProjections of A-delta and C fibers
AA delta and C fibers separate upon entering thedelta and C fibers separate upon entering the AA--delta and C fibers separate upon entering the delta and C fibers separate upon entering the spinal cordspinal cord
They travel in the tract of Lissauer and synapse inThey travel in the tract of Lissauer and synapse in They travel in the tract of Lissauer and synapse in They travel in the tract of Lissauer and synapse in the dorsal horn (lamina 1) and the substania the dorsal horn (lamina 1) and the substania gelatinosa (lamina 2), some Agelatinosa (lamina 2), some A--delta fibers also delta fibers also g ( ),g ( ),project to lamina Vproject to lamina V
From there they project to interneurons, inhibitory From there they project to interneurons, inhibitory and exitatory projection pathwaysand exitatory projection pathways
Afferent fibers use peptides and Afferent fibers use peptides and glutamateglutamate(excitatory) as their neurotransmitter(excitatory) as their neurotransmitter
22

Pain Pathways to the Brain SpinoSpino--thalamic tract thalamic tract To cortex, where is the pain?To cortex, where is the pain?
SpinoSpino--reticular tract reticular tract WakeWake--up!up!pp
SpinoSpino--mesencephalic tractmesencephalic tractTo PAG (let’s stop the pain)To PAG (let’s stop the pain)To PAG (let s stop the pain)To PAG (let s stop the pain)
SpinoSpino--cervical tractcervical tractC d ill l i i h d llC d ill l i i h d ll Cuneate and gracille nuclei in the medullaCuneate and gracille nuclei in the medulla
23

Pain Pathways to the Brain
Spinothalamic tractSpinothalamic tractSpinal cordSpinal cordVPLVPL ––thalamusthalamuscortexcortexSpinal cord Spinal cord VPL VPL thalamus thalamus cortexcortex
Spinoreticular tractSpinoreticular tractSpinal cordSpinal cordreticular formation (pons &reticular formation (pons &Spinal cord Spinal cord reticular formation (pons & reticular formation (pons &
medulla) medulla) thalamus thalamus cortexcortex Spinomesencephalic tractSpinomesencephalic tract Spinomesencephalic tractSpinomesencephalic tractSpinal cord Spinal cord PAG (pain modulation, PAG (pain modulation,
endorphins)endorphins)endorphins)endorphins)24

25

26

Pathways PAG
Neurons in the PAG:Neurons in the PAG:Descend through posterior columnsDescend through posterior columnsDescend through posterior columnsDescend through posterior columnsInhibit second order nociceptive neuronsInhibit second order nociceptive neuronsActivate interneurons to downActivate interneurons to down--regulate painregulate painActivate interneurons to downActivate interneurons to down regulate pain regulate pain
networknetwork
27
Small Fiber NeuropathySmall Fiber Neuropathy Caused by damage to distal unmyelinated slowCaused by damage to distal unmyelinated slow--
d i fibd i fibconducting sensory fibersconducting sensory fibers Symptoms: insensitivity to heat and/or cold, Symptoms: insensitivity to heat and/or cold,
“ i kli t bbi j bbi ti li b i“ i kli t bbi j bbi ti li b i“prickling, stabbing, jabbing, tingling or burning “prickling, stabbing, jabbing, tingling or burning pain, numbness, or bandpain, numbness, or band--like sensation” like sensation”
Signs: loss of pain and temperature discriminationSigns: loss of pain and temperature discrimination Signs: loss of pain and temperature discrimination, Signs: loss of pain and temperature discrimination, often with preserved motor functionoften with preserved motor function
Hard to diagnose with EDX (EMGHard to diagnose with EDX (EMG NCS)NCS) Hard to diagnose with EDX (EMGHard to diagnose with EDX (EMG--NCS)NCS) Can do QST (quantitative sensory testing)Can do QST (quantitative sensory testing) Nerve biopsy not useful but skin biopsy can beNerve biopsy not useful but skin biopsy can be Nerve biopsy not useful but skin biopsy can be Nerve biopsy not useful but skin biopsy can be
usefuluseful28

Small Fiber Neuropathy CausesCauses: alcohol abuse, DM, idiopathic, Fabry disease, : alcohol abuse, DM, idiopathic, Fabry disease,
HIV, HIV medications, vasculitis, amyloidosis, HIV, HIV medications, vasculitis, amyloidosis, Friedrich ataxia, autonomic neuropathy, paraFriedrich ataxia, autonomic neuropathy, para--neoplasticneoplastic
WorkWork up:up: WorkWork--up: up: CBC, metabolic panel and liver enzymes, TFTs, HgB A1CBC, metabolic panel and liver enzymes, TFTs, HgB A1--c, c,
BB1212/ MMA/ tHcy, vitamins (E), FTA, ESR, HIV, ANA, / MMA/ tHcy, vitamins (E), FTA, ESR, HIV, ANA, paraneoplastic Abs, IFE. (“inflammogram”)paraneoplastic Abs, IFE. (“inflammogram”)
Thermal sensitivity testingThermal sensitivity testing TreatmentsTreatments: “anticonvulsants ” antidepressants anti: “anticonvulsants ” antidepressants anti-- TreatmentsTreatments: anticonvulsants, antidepressants, anti: anticonvulsants, antidepressants, anti--
inflammatories, immunosuppressants, lidocaine, inflammatories, immunosuppressants, lidocaine, mexilitene, opioids, topical agents, nerve blockade, mexilitene, opioids, topical agents, nerve blockade, , p , p g , ,, p , p g , ,nerve stimulators, PT, acupuncture, IVIg, nerve stimulators, PT, acupuncture, IVIg, plasmapheresisplasmapheresis29

Large Fiber Ne ropathLarge Fiber Neuropathy
S tS t Symptoms: Symptoms: In contrast to small fiber neuropathy In contrast to small fiber neuropathy WeaknessWeaknessLoss of reflexesLoss of reflexesAbnormal NCSAbnormal NCSReduced vibratory and position senseReduced vibratory and position sense
30

Postherpetic Neuralgia (PHN)p g ( ) Starts with herpes zoster (AKA shingles)Starts with herpes zoster (AKA shingles) ReRe--activation of varicella (HHVactivation of varicella (HHV--3)3) Symptoms:Symptoms:Starts with burning, itching, tingling, or pain Starts with burning, itching, tingling, or pain
within a lateralized dermatomewithin a lateralized dermatomebli ( i l d lbli ( i l d lProgresses to blisters (vessicular dermatomal Progresses to blisters (vessicular dermatomal
rash).rash).Can beCan be zoster sine herpetezoster sine herpete (meaning without rash)(meaning without rash)Can be Can be zoster sine herpete zoster sine herpete (meaning without rash)(meaning without rash)
Treatment:Treatment:Treat oster ith ac clo ir alc clo irTreat oster ith ac clo ir alc clo irTreat zoster with acyclovir, valcyclovir, Treat zoster with acyclovir, valcyclovir,
famcyclovirfamcyclovir31
Postherpetic Neuralgia (PHN)Postherpetic Neuralgia (PHN) Pain, (including hyperalgesia, allodynia…) Pain, (including hyperalgesia, allodynia…) ( g yp g y )( g yp g y )
after zoster has resolvedafter zoster has resolvedCan last months to yearsCan last months to yearsyyMore common in the elderlyMore common in the elderly
CSF can be abnormalCSF can be abnormal CSF can be abnormal CSF can be abnormal Treat with TCAs, “antiTreat with TCAs, “anti--convulsants” convulsants”
(carbamazepine gabapentin pregabalin)(carbamazepine gabapentin pregabalin)(carbamazepine, gabapentin, pregabalin), (carbamazepine, gabapentin, pregabalin), opioids, topical anesthetics, lidocaine patchopioids, topical anesthetics, lidocaine patchC i id kC i id k Corticosteroids not proven to workCorticosteroids not proven to work
32

Postherpetic Neuralgia (PHN)Postherpetic Neuralgia (PHN) In 2006, the Food and Drug Administration approved a In 2006, the Food and Drug Administration approved a , g pp, g pp
VZV vaccine (Zostavax) for use in people 60 and older VZV vaccine (Zostavax) for use in people 60 and older who have had chickenpox. When the vaccine becomes who have had chickenpox. When the vaccine becomes more widely available many older adults will for the firstmore widely available many older adults will for the firstmore widely available, many older adults will for the first more widely available, many older adults will for the first time have a means of preventing shingles. Researchers time have a means of preventing shingles. Researchers found that giving older adults the vaccine reduced the found that giving older adults the vaccine reduced the expected number of later cases of shingles by half. And in expected number of later cases of shingles by half. And in people who still got the disease despite immunization, the people who still got the disease despite immunization, the severity and complications of shingles were dramatically severity and complications of shingles were dramatically y p g yy p g yreduced. reduced. The shingles vaccine is only a preventive therapy The shingles vaccine is only a preventive therapy and is not a treatment for those who already have shingles and is not a treatment for those who already have shingles or postherpetic neuralgiaor postherpetic neuralgiaor postherpetic neuralgia. or postherpetic neuralgia.
From NINDS.govFrom NINDS.gov33
Trigeminal Neuralgia (Tic Doloureux) Brief paroxysms of Brief paroxysms of pain pain ddistributed istributed along along CN VCN VPain stabbing (lancinating or electrical) in qualityPain stabbing (lancinating or electrical) in qualityL t d t i tL t d t i tLast seconds to minutesLast seconds to minutes
Can be excruciating (suicide not uncommon in Can be excruciating (suicide not uncommon in past)past)past)past)
Can be elicited by eating, tooth brush, washingCan be elicited by eating, tooth brush, washing Asymptomatic betweenAsymptomatic between jolts of painjolts of pain Asymptomatic between Asymptomatic between jolts of painjolts of pain Typically older than 40 Typically older than 40 Can go years between recurrencesCan go years between recurrences Can go years between recurrences Can go years between recurrences
34

T i i l N l iTrigeminal Neuralgia
CausesCausesVascular compressionVascular compressionMS (demyelinating)MS (demyelinating)Tumors Tumors Basilar artery aneurysm Basilar artery aneurysm TraumaTraumaIdiopathicIdiopathic
35

T i i l N l iTrigeminal NeuralgiaW kW k f d l i l b MRIf d l i l b MRIWorkWork--up: for underlying cause: labs, MRI, up: for underlying cause: labs, MRI, MSMS workwork--up (demyelination)up (demyelination)
36

Trigeminal Neuralgia——Trigeminal NeuralgiaPharmacological Treatment Carbamazepine/Carbamazepine/trileptaltrileptal GabapentinGabapentinpp BaclofenBaclofen PhenytoinPhenytoinyy ValproateValproate TCATCA TCATCA NSAIDsNSAIDs
37
Trigeminal Neuralgia——TreatmentS i lS i l Surgical:Surgical:Microvascular decompressionMicrovascular decompressionBalloon compressionBalloon compressionGlycerol injection (kills the nerve)Glycerol injection (kills the nerve)RadiosurgeryRadiosurgeryRadiofrequency lesioningRadiofrequency lesioning
38

Glossopharyngeal NeuralgiaSi ilSi il i i l l i f CNi i l l i f CN Similar to Similar to trigeminal neuralgia except for CN trigeminal neuralgia except for CN involvedinvolvedU il lU il l UnilateralUnilateralPharynx (posterior), soft palate, tongue base, ear, Pharynx (posterior), soft palate, tongue base, ear,
mastoid (any area in this region)mastoid (any area in this region)mastoid (any area in this region)mastoid (any area in this region) Swallowing, yawning, coughing or speaking Swallowing, yawning, coughing or speaking
(any oro(any oro pharyngeal activity) can cause painpharyngeal activity) can cause pain(any oro(any oro--pharyngeal activity) can cause painpharyngeal activity) can cause pain Medicines are similar to those for trigeminal Medicines are similar to those for trigeminal
neuralgia (“AEDs”)neuralgia (“AEDs”)neuralgia ( AEDs )neuralgia ( AEDs )39
Botox in the Treatment of Pain:Botox in the Treatment of Pain: Cochrane
Medicinal and injection therapies for Medicinal and injection therapies for h i l k di dh i l k di dmechanical neck disordersmechanical neck disorders
40Paul Michael J Peloso1 et al. , Cervical Overview Group Cochrane Database of Systematic Reviews 2007, Issue 3. Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Botox in the Treatment of Pain:Cochrane
“Ch i k di d i h i h di l fi di“Ch i k di d i h i h di l fi di “Chronic neck disorders with or without radicular findings or “Chronic neck disorders with or without radicular findings or headache, there was headache, there was moderate evidence from 5 high quality trials moderate evidence from 5 high quality trials that Botulinum toxin A intramuscular injections had similar that Botulinum toxin A intramuscular injections had similar effects to saline in improving paineffects to saline in improving pain (pooled SMD:(pooled SMD: 0 39 95%CI0 39 95%CI 1 251 25effects to saline in improving pain effects to saline in improving pain (pooled SMD: (pooled SMD: --0.39, 95%CI 0.39, 95%CI --1.25 1.25 to 0.47), disability or global perceived effect.”to 0.47), disability or global perceived effect.”
“Authors’ conclusions: “Authors’ conclusions: Th i d id f h b fi f i h lTh i d id f h b fi f i h lThere is moderate evidence for the benefit of intravenous methylThere is moderate evidence for the benefit of intravenous methyl--prednisolone given within eight hours of acute whiplash, from a single prednisolone given within eight hours of acute whiplash, from a single trial. Lidocaine injection into myofascial trigger points appears trial. Lidocaine injection into myofascial trigger points appears effective in two trialseffective in two trials There is moderate evidence that BotulinumThere is moderate evidence that Botulinumeffective in two trials. effective in two trials. There is moderate evidence that Botulinum There is moderate evidence that Botulinum toxin A is not superior to saline injection for chronic MND. toxin A is not superior to saline injection for chronic MND. Muscle Muscle relaxants, analgesics and NSAIDs had limited evidence and unclear relaxants, analgesics and NSAIDs had limited evidence and unclear benefits ”benefits ”benefits.benefits.
……Limited trials though……Limited trials though41

Botox in the Treatment of Pain: AAN
42http://www.aan.com/practice/guideline

Botox in the Treatment of Pain: AANAAN
43http://www.aan.com/practice/guideline
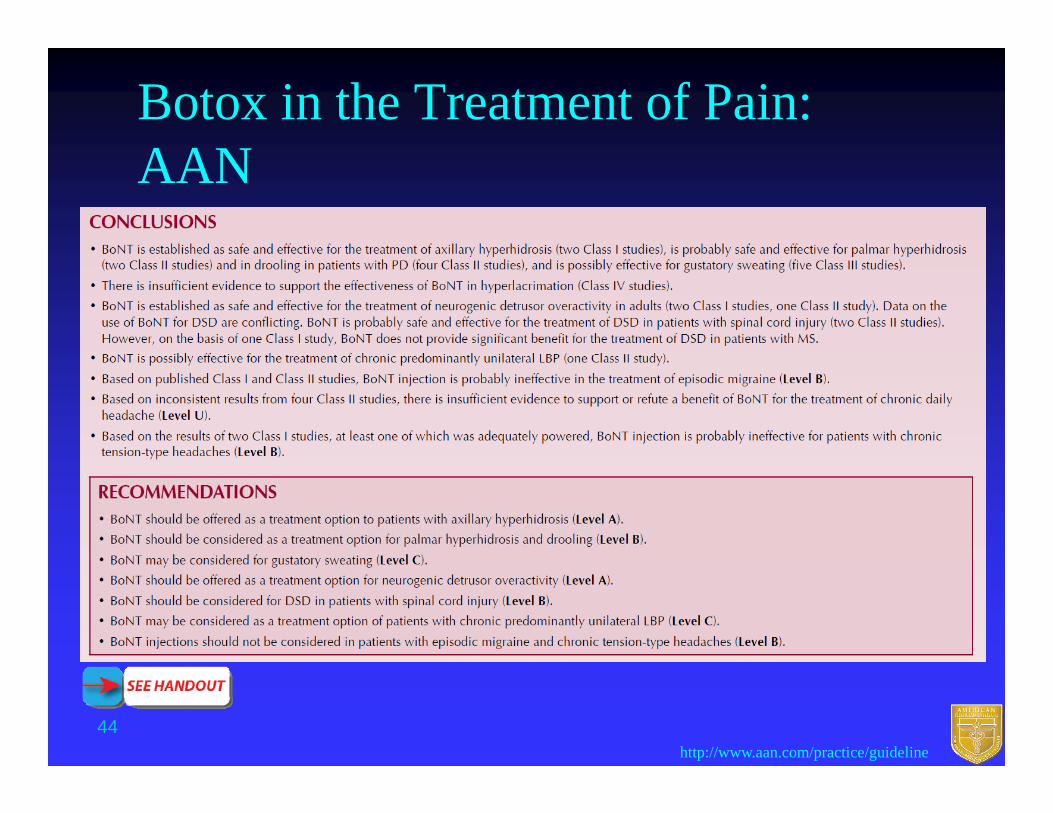
Botox in the Treatment of Pain: AANAAN
44http://www.aan.com/practice/guideline

TENS in the Treatment of Pain: AAN
45http://www.aan.com/practice/guideline

TENS in the Treatment of Pain: AAN
46http://www.aan.com/practice/guideline

Pain Related to Other Systemic Diseases and IllnessesDiseases and Illnesses CancerCancer
Opioids, opioid patches, opioid pumps, opioid Opioids, opioid patches, opioid pumps, opioid rotation, PCArotation, PCA
Na+ channel blockers AEDsNa+ channel blockers AEDsNa+ channel blockers, AEDsNa+ channel blockers, AEDs PhentolaminePhentolamineClonidineClonidine TCAsTCAs SNRIsSNRIsMexilitineMexilitine
Cancer: find the cause (often a new dx is found)Cancer: find the cause (often a new dx is found) Paraneoplastic syndromes with neuropathyParaneoplastic syndromes with neuropathy
AntiAnti--HuHu47

Pain Related to Other Systemic Diseases and Illnesses
MS t l i i ith ti itMS t l i i ith ti it MS, central pain, pain with spasticityMS, central pain, pain with spasticityBaclofen, Baclofen, neurontinneurontin, baclofen pump, baclofen pumpBenzodiazepinesBenzodiazepinesppManyMany
HIV HIV Drugs for “neuropathic pain”Drugs for “neuropathic pain”Drugs for neuropathic pain Drugs for neuropathic pain InteractionsInteractions
Myelopathic pain (often after SC injury/trauma)Myelopathic pain (often after SC injury/trauma)y p p ( j y )y p p ( j y )Burning sensation, autonomic instabilityBurning sensation, autonomic instability Treat with: drugs, rehab, dorsal root entry zone lesioning, Treat with: drugs, rehab, dorsal root entry zone lesioning,
spinal cord stimulation intrathecal opioid pumpsspinal cord stimulation intrathecal opioid pumpsspinal cord stimulation, intrathecal opioid pumpsspinal cord stimulation, intrathecal opioid pumps
48

RadiculopathiesRadiculopathies
49
Radic lopathiesRadiculopathies Radix =root + neuropathyRadix =root + neuropathy Radix =root + neuropathyRadix =root + neuropathy 7 cervical vertebral bodies/8 cervical roots7 cervical vertebral bodies/8 cervical rootsThe nerve root exiting between two vertebral The nerve root exiting between two vertebral
bodies is numbered by the lower vertebral body bodies is numbered by the lower vertebral body l h i b hl h i b hFor example, the C6 nerve root exits between the For example, the C6 nerve root exits between the
C5C5––C6 vertebrae and should be effected by a C6 vertebrae and should be effected by a C5C5 6 disc bulge or herniation6 disc bulge or herniationC5C5––6 disc bulge or herniation6 disc bulge or herniation
Referred painReferred pain
50

Radic lopath : AnatomRadiculopathy: Anatomy
51From http://www.neuroanatomy.wisc.edu/

RadiculopathiesRadiculopathies
Spinal roots MUSCLE (function)
C 5/6 DELTOID BICEPSBICEPS BRACHIORADIALIS INFRASPINATUS SUPRASPINATUS
C 6/7 PRONATOR TERESC 6/7 PRONATOR TERES FLEXOR CARPI ULNARIS
C 7 TRICEPS LATISSIMUS DORSILATISSIMUS DORSI
C 7/8 (extensors and flexors of the wrist)
T 1 (intrinsic muscles of the hand)
52
T 1 (intrinsic muscles of the hand)
Adapted From http://www.neuroanatomy.wisc.edu/

RadiculopathiesRadiculopathies
Spinal roots INERVATED MUSCLE (function)
L 2/3 ILIOPSOASL 2/3 ILIOPSOAS
L 3 ADDUCTOR LONGUS
L 3/4 VASTUS LATERALISL 3/4 VASTUS LATERALISVASTUS MEDIALIS
L 5 Ankle dorsiflexors (eversion and inversion) & hi bd t& hip abductors
S 1 Ankle plantar flexors & hip extensors
53Adapted From http://www.neuroanatomy.wisc.edu/

Radic lopathRadiculopathy DiagnosisDiagnosis DiagnosisDiagnosis
Exam + history + knowledge of the cord and brachial Exam + history + knowledge of the cord and brachial plexus anatomyplexus anatomyp yp y
For exact determination of severity, MRI, CT For exact determination of severity, MRI, CT myelography or CSF exam may be required.myelography or CSF exam may be required.
Indications for surgery:Indications for surgery: Intractable Intractable painpain
S i l i t bilitS i l i t bilit Spinal instabilitySpinal instability Progressive weakness with loss of functionProgressive weakness with loss of function
54

Complex Regional Pain Syndrome
Formerly called reflex sympathetic Formerly called reflex sympathetic dystrophy (and/or causaglia)dystrophy (and/or causaglia)y p y ( g )y p y ( g )
Now divided into Now divided into CRPS type I (akin to causalgia)CRPS type I (akin to causalgia)CRPS type I (akin to causalgia)CRPS type I (akin to causalgia)CRPS type II (there is the presence of a known CRPS type II (there is the presence of a known
nerve injury)nerve injury)nerve injury)nerve injury)On EDX pain extends outside of the distribution of On EDX pain extends outside of the distribution of
the known nerve injurythe known nerve injury
55

Complex Regional Pain SyndromeCRPS ICRPS I CRPS ICRPS I
Initiating noxious event, often traumaInitiating noxious event, often traumaNot limited to a single nerveNot limited to a single nervePain is disproportionate to the expected initial Pain is disproportionate to the expected initial
injuryinjury
56

Complex Regional Pain SyndromeCRPS tCRPS t CRPS, symptomsCRPS, symptoms
EdemaEdemaSkin blood flow changesSkin blood flow changesAllodyniaAllodyniaSudomotor changesSudomotor changesggLimb and bone atrophyLimb and bone atrophy
57

Complex Regional Pain SyndromeCRPS (th i f h i )CRPS (th i f h i ) CRPS (theories of mechanism)CRPS (theories of mechanism)CC--polymodal nociceptors develop polymodal nociceptors develop
h iti ith iti ithypersensitivityhypersensitivitySympathetic hyperSympathetic hyper--responsiveness onto responsiveness onto
nociceptorsnociceptorsnociceptorsnociceptorsAberrant nerve sproutsAberrant nerve sprouts
A tifi i l d h ti t i iA tifi i l d h ti t i iArtificial and ephaptic transmissionArtificial and ephaptic transmissionWindWind--up of wide dynamic range central up of wide dynamic range central
neuronsneurons58

Complex Regional Pain SyndromeCRPS I diff ti l DCRPS I diff ti l D CRPS I differential DxCRPS I differential DxCRPS II (missed discrete nerve injury)CRPS II (missed discrete nerve injury)Fx, local injuryFx, local injuryCellulitisCellulitisRaynaudsRaynaudsThrombangitis obliteransThrombangitis obliteransDM neuropathyDM neuropathyGoutGout
59

C l R i l P i S dComplex Regional Pain Syndrome
CRPS I dx testsCRPS I dx testsScintigraphyScintigraphyg p yg p yThermographyThermographyRadiography & Imaging (MRI)Radiography & Imaging (MRI)g p y g g ( )g p y g g ( )
60

C l R i l P i S dComplex Regional Pain Syndrome
CRPS treatmentCRPS treatmentNSAIDs, ketorolacNSAIDs, ketorolacAntidepressants (TCAs)Antidepressants (TCAs)CCBs, AlphaCCBs, Alpha--2 agonists2 agonistsCorticosteroidsCorticosteroidsRegional, local blockade, surgical techniques, Regional, local blockade, surgical techniques, g , , g q ,g , , g q ,
spinal cord stimulation, sympathectomyspinal cord stimulation, sympathectomyMirror box therapyMirror box therapy
61

Parsonage-Turner Syndrome Brachial plexitis Brachial plexitis (AKA acute brachial neuropathy or neuralgic(AKA acute brachial neuropathy or neuralgic(AKA acute brachial neuropathy or neuralgic (AKA acute brachial neuropathy or neuralgic
amyotrophy)amyotrophy)Inflammatory condition affection some or mostInflammatory condition affection some or mostInflammatory condition affection some or most Inflammatory condition affection some or most
of the brachial plexusof the brachial plexusVery painful, severe shoulder pain with Very painful, severe shoulder pain with y p , py p , p
weakness, numbness, and dysesthesias of the weakness, numbness, and dysesthesias of the arm. Pain with movementarm. Pain with movement
On exam does not conform to single nerve or On exam does not conform to single nerve or nerve rootnerve rootYou will find yourself baffled trying to localize the You will find yourself baffled trying to localize the
lesionlesion62

Parsonage T rner S ndromeParsonage-Turner Syndrome Brachial plexitisBrachial plexitis Brachial plexitis Brachial plexitis More common in menMore common in men
R idR idRapid onsetRapid onsetUnilateral (rarely Unilateral (rarely
bil t l)bil t l)bilateral)bilateral)Often defies Often defies
localization to alocalization to alocalization to a localization to a specific root or single specific root or single nervenervenervenerve
63
Parsonage-Turner Syndrome Brachial plexitis causesBrachial plexitis causes
PostPost--infectious or infectiousinfectious or infectious PostPost--vaccinalvaccinal P tP t i li l PostPost--surgicalsurgical PostPost--traumatrauma PostPost--radiationradiation PostPost radiationradiationBacterialBacterial Systemic illness (very common)Systemic illness (very common)y ( y )y ( y )HereditaryHereditary
64
P T S dParsonage-Turner Syndrome Brachial plexitis workBrachial plexitis work--upup
Labs (broad)Labs (broad)MRIMRIMRIMRI EDXEDX
T t tT t t Treatment:Treatment:Underlying causeUnderlying causePain controlPain controlPTPT
65

Thalamic PainThalamic Pain
66

ThalamocorticalThalamocorticalRadiations
CMCM CentromedianCentromedianLDLD Lateral dorsalLateral dorsalLPLP Lateral posteriorLateral posteriorLPLP Lateral posteriorLateral posteriorMDMD Medial dorsalMedial dorsalVAVA Ventral anteriorVentral anteriorVIVI VentralVentral intermedialintermedial
Internal medullary laminaIntralaminar nuclei
Other medial nucleiMidline (median) nuclei
Anteriornuclei
VIVI Ventral Ventral intermedialintermedialVLVL Ventral lateralVentral lateralVPLVPL Ventral posterolateralVentral posterolateralVPMVPM Ventral posteromedialVentral posteromedial
( )Intrathalamic adhesion
Pulvinar
Medial i l t
ppgeniculate body
Lateral geniculate body
Acousticpathway
Optic tractFromcerebellumReticular
Fromglobus pallidusand SN
67
Somesthetic from head(trigeminal nerve)
pnucleus
Somesthetic from body
Thalamic Pain:S d f j iSyndrome of Dejerine-Roussy
Oft ft th l iOft ft th l i t kt k (l(l Often occurs after a thalamic Often occurs after a thalamic strokestroke (less common (less common in MS and tumors)in MS and tumors)Occlusion of a thalamogeniculate branches off the PCAOcclusion of a thalamogeniculate branches off the PCAOcclusion of a thalamogeniculate branches off the PCAOcclusion of a thalamogeniculate branches off the PCA
Onset after stroke can be delayed by monthsOnset after stroke can be delayed by months Localization: ventroLocalization: ventro posteriorposterior lateral lesionslateral lesions Localization: ventroLocalization: ventro--posteriorposterior--lateral lesionslateral lesions Can start with numbness and over time progress to Can start with numbness and over time progress to
pain or allodyniapain or allodyniapain or allodyniapain or allodynia Tx: Tricyclics or anticonvulsants such as GPN, Tx: Tricyclics or anticonvulsants such as GPN,
CBZ, OXC, LTGCBZ, OXC, LTGCBZ, OXC, LTGCBZ, OXC, LTG
68

Phantom Limb SyndromePhantom Limb Syndrome Persistent perception of a limb that has been Persistent perception of a limb that has been
l dl dlost or amputatedlost or amputated Very common (90%Very common (90%––98% incidence)98% incidence) Can be instantaneousCan be instantaneous The perception is often unpleasant or painfulThe perception is often unpleasant or painful The perception is often unpleasant or painfulThe perception is often unpleasant or painful Can be chronic and debilitatingCan be chronic and debilitating
I i d di fI i d di f Important in our understanding of Important in our understanding of neuroplasticity and cortical topography (PET, neuroplasticity and cortical topography (PET, h fMRI d MEG)h fMRI d MEG)then fMRI and MEG)then fMRI and MEG)
69

Phantom Limb Syndrome Symptoms occur in people who have had a limb Symptoms occur in people who have had a limb
removed AND people who are born without a limbremoved AND people who are born without a limb Risk factors: Risk factors:
PrePre--amputation pain or infectionamputation pain or infectionB i d lB i d lBeing an adultBeing an adult
Symptoms include: Symptoms include: P i ( t )P i ( t ) Pain (most common) Pain (most common) Pleasurable sensations (rare)Pleasurable sensations (rare) Sensation of clothing jewelry or other manipulationSensation of clothing jewelry or other manipulation Sensation of clothing, jewelry, or other manipulationSensation of clothing, jewelry, or other manipulation Sensation that the limb is still there and functional Sensation that the limb is still there and functional
(patients may forget it’s gone, try to walk on a missing leg (patients may forget it’s gone, try to walk on a missing leg and fall)and fall)
Telescoping (over time); the phantom shrinksTelescoping (over time); the phantom shrinks70

Phantom Limb S ndromePhantom Limb Syndrome Mechanism:Mechanism: Mechanism:Mechanism:Cortical remappingCortical remapping
DD ff i f f hff i f f hDeDe--afferentation of areas of the sensory afferentation of areas of the sensory homunculushomunculus
M t f f ti l i t dM t f f ti l i t d ff t dff t dMovement of functional areas into deMovement of functional areas into de--afferented afferented areasareas
Resulting cortical overResulting cortical over lap between delap between de afferentedafferentedResulting cortical overResulting cortical over--lap between delap between de--afferented afferented areas and functional regionsareas and functional regions
Proven with early PET studies now with fMRIProven with early PET studies now with fMRIProven with early PET studies, now with fMRI Proven with early PET studies, now with fMRI and MEGand MEG
71
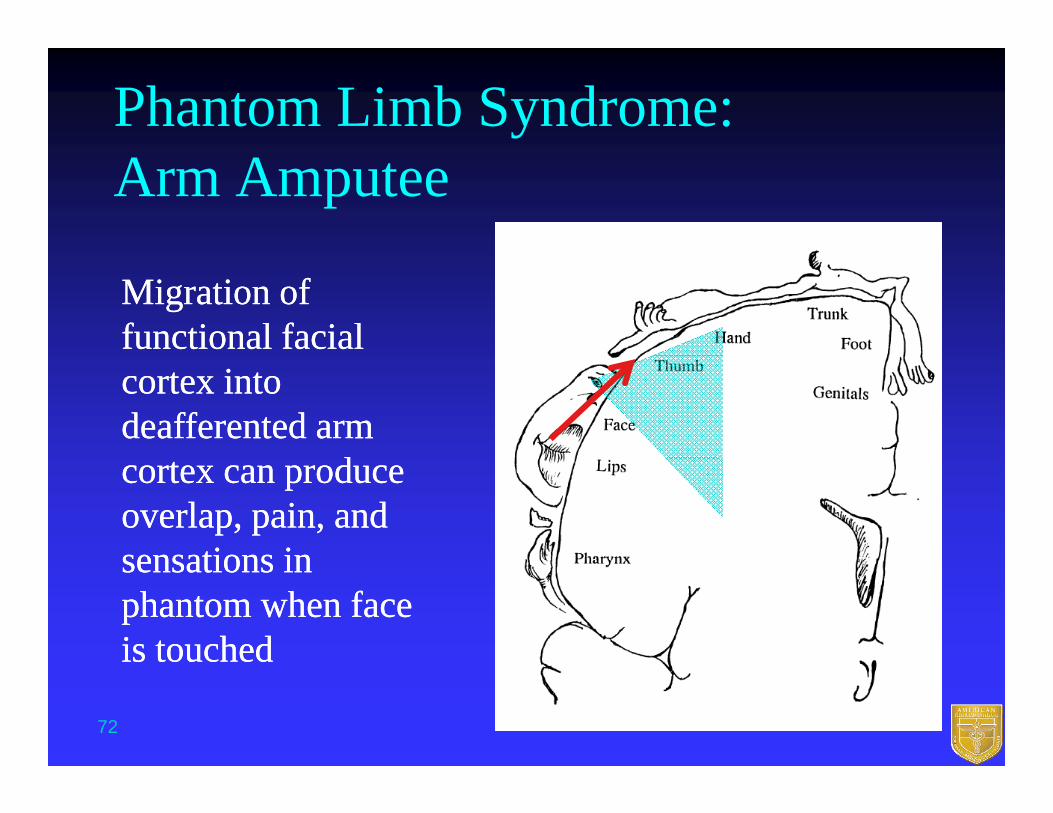
Phantom Limb Syndrome: Arm Amputee
Migration of Migration of functional facial functional facial cortex into cortex into deafferenteddeafferented arm arm
ddcortex can produce cortex can produce overlap, pain, and overlap, pain, and sensations insensations insensations in sensations in phantom when face phantom when face is touchedis touched
72

Fibromyalgia (From IASP)Fibromyalgia (From IASP) Fibromyalgia syndrome (FM) is defined as:Fibromyalgia syndrome (FM) is defined as: Fibromyalgia syndrome (FM) is defined as:Fibromyalgia syndrome (FM) is defined as: “A common “A common rheumatologicalrheumatological syndrome syndrome
characterized by chronic diffusecharacterized by chronic diffusecharacterized by chronic, diffuse characterized by chronic, diffuse musculoskeletal pain and tenderness with a musculoskeletal pain and tenderness with a number of associated symptoms amongnumber of associated symptoms amongnumber of associated symptoms, among number of associated symptoms, among which sleep disturbances, fatigue, and which sleep disturbances, fatigue, and affective dysfunction are particularlyaffective dysfunction are particularlyaffective dysfunction are particularly affective dysfunction are particularly frequent”frequent”
73
See: References 1. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292:2388–95. 2. Russell IJ, Bieber CS. Myofascial pain and fibromyalgia syndrome. In: McMahon SB, Koltzenburg M, editors. Melzack and Wall’s textbook of pain, 5th ed. Edinburgh: Churchill Livingstone; 2005. p. 669–81. and http://www.iasp-pain.org

Fibromyalgia (from IASP)
EpidemiologyEpidemiology“Affects 2%“Affects 2%––10% of the population, in all ages,10% of the population, in all ages, Affects 2%Affects 2% 10% of the population, in all ages, 10% of the population, in all ages,
ethnic groups, and culturesethnic groups, and cultures7 times more common in females7 times more common in femalesIn the United States, about 15% of patients In the United States, about 15% of patients
receive disability funding”receive disability funding”y gy g
74Adapted from http://www.iasp-pain.org

Fibromyalgia (From IASP)y g ( ) DiagnosticDiagnostic CriteriaCriteria From the American College of Rheumatology From the American College of Rheumatology
Committee in 1990:Committee in 1990:A history of widespread pain (involving all 4 limbs A history of widespread pain (involving all 4 limbs
and the trunk) of at least 3 months’ durationand the trunk) of at least 3 months’ durationTenderness to digital palpation (with a pressure of Tenderness to digital palpation (with a pressure of
4 kg) in at least 11 of 18 (9 symmetrical) 4 kg) in at least 11 of 18 (9 symmetrical) predetermined body districts called tender points (apredetermined body districts called tender points (apredetermined body districts called tender points (a predetermined body districts called tender points (a tender point is defined as a site of exquisite tender point is defined as a site of exquisite tenderness in soft tissues, in contrast to the triggertenderness in soft tissues, in contrast to the triggertenderness in soft tissues, in contrast to the trigger tenderness in soft tissues, in contrast to the trigger points of myofascial pain syndrome)”points of myofascial pain syndrome)”
75Adapted from http://www.iasp-pain.org

Fibromyalgia (from IASP)Fibromyalgia (from IASP) Management:Management:ggPsychological or psychiatric supportPsychological or psychiatric supportPT, exercise (aerobic, strengthening), with the PT, exercise (aerobic, strengthening), with the , ( , g g),, ( , g g),
addition of physical modalities, massage or TENSaddition of physical modalities, massage or TENSMedications:Medications:Tricyclic antidepressants , Tricyclic antidepressants , SNRIs, SNRIs, ,,SSRIs, SSRIs, AntiAnti--epileptics (gabapentin, pregabalin)epileptics (gabapentin, pregabalin)AntiAnti epileptics (gabapentin, pregabalin)epileptics (gabapentin, pregabalin)
76Adapted from http://www.iasp-pain.org

Posttest(repeat of pretest questions)
77

Question 1: A patient presents with a 1 year Question 1: A patient presents with a 1 year Q p p yQ p p yhistory of a dysesthetic band like sensation history of a dysesthetic band like sensation around his feet up to his shins, he has around his feet up to his shins, he has p ,p ,preserved strength and reflexes. The highest preserved strength and reflexes. The highest yield test is:yield test is:yy1.1. EMGEMG22 Nerve biopsyNerve biopsy2.2. Nerve biopsyNerve biopsy3.3. Broad lab panelBroad lab panel4.4. Skin biopsySkin biopsy5.5. Nerve conduction study for small fiber Nerve conduction study for small fiber yy
neuropathyneuropathy78

Explanation Question 1
Small fiber neuropathy often presents with a Small fiber neuropathy often presents with a dysesthetic band like sensation around the feet to dysesthetic band like sensation around the feet to the ankles, with preserved strength and reflexes the ankles, with preserved strength and reflexes (unlike large fiber neuropathy). There is a broad (unlike large fiber neuropathy). There is a broad differential and laborator st dies ma ield andifferential and laborator st dies ma ield andifferential and laboratory studies may yield an differential and laboratory studies may yield an underlying cause. EMG, NCS, and nerve biopsies underlying cause. EMG, NCS, and nerve biopsies of extremely low yield Skin biopsy and thermalof extremely low yield Skin biopsy and thermalof extremely low yield. Skin biopsy and thermal of extremely low yield. Skin biopsy and thermal testing may aid in diagnosis.testing may aid in diagnosis.
79

Question 2: TRPM8 is activated byQuestion 2: TRPM8 is activated by
1.1. PinPin--prickprick22 HeatHeat2.2. HeatHeat3.3. ColdCold
A k f “A k f “k lk l ” i h i i Chi” i h i i Chi4.4. A pack of “A pack of “koolskools” in the winter in Chicago” in the winter in Chicago5.5. Scalding coffeeScalding coffee6.6. A chemical burn or lacerationA chemical burn or laceration
80

Explanation Question 2
TRPM8 is the cold + menthol receptor. It is TRPM8 is the cold + menthol receptor. It is actually activated by menthols and activity actually activated by menthols and activity y y yy y yis enhanced by coldis enhanced by cold
81

Question 3: PostQuestion 3: Post--herpetic neuralgia:herpetic neuralgia:Question 3: PostQuestion 3: Post herpetic neuralgia:herpetic neuralgia:
1.1. Follows reactivation of HHVFollows reactivation of HHV--662.2. Cannot be prevented but can be treatedCannot be prevented but can be treated3.3. Always is heralded by a dermatomal vesicular rashAlways is heralded by a dermatomal vesicular rash3.3. ways s e a ded by a de ato a ves cu a asways s e a ded by a de ato a ves cu a as4.4. Should not associated with abnormal CSFShould not associated with abnormal CSF55 Has an FDAHas an FDA--approved vaccineapproved vaccine5.5. Has an FDAHas an FDA approved vaccineapproved vaccine
82

Explanation Question 3 In 2006 the Food and Drug Administration approved aIn 2006 the Food and Drug Administration approved a In 2006, the Food and Drug Administration approved a In 2006, the Food and Drug Administration approved a
VZV vaccine VZV vaccine (Zostavax) (Zostavax) for use in people 60 and older for use in people 60 and older who have had chickenpox. When the vaccine becomes who have had chickenpox. When the vaccine becomes
id l il bl ld d lt ill f th fi tid l il bl ld d lt ill f th fi tmore widely available, many older adults will for the first more widely available, many older adults will for the first time have a means of preventing shingles. Researchers time have a means of preventing shingles. Researchers found that giving older adults the vaccine reduced the found that giving older adults the vaccine reduced the expected number of later cases of shingles by half. And in expected number of later cases of shingles by half. And in people who still got the disease despite immunization, the people who still got the disease despite immunization, the severity and complications of shingles were dramaticallyseverity and complications of shingles were dramaticallyseverity and complications of shingles were dramatically severity and complications of shingles were dramatically reduced. reduced. The shingles vaccine is only a preventive therapy The shingles vaccine is only a preventive therapy and is not a treatment for those who already have shingles and is not a treatment for those who already have shingles
th ti l ith ti l ior postherpetic neuralgiaor postherpetic neuralgia
83 From NINDS.gov

Question 4: The etiology of DejerineQuestion 4: The etiology of Dejerine--Question 4: The etiology of DejerineQuestion 4: The etiology of Dejerine--Roussy syndrome is usually:Roussy syndrome is usually:
1.1. TumorTumor22 IdiopathicIdiopathic2.2. IdiopathicIdiopathic3.3. TraumaTrauma
S kS k4.4. StrokeStroke5.5. CNS infectionCNS infection6.6. Degenerative diseaseDegenerative disease
84
Explanation Question 4
The etiology of DejerinneThe etiology of Dejerinne--Roussy Roussy syndrome is usually ischemic strokesyndrome is usually ischemic stroke——y yy yocclusion of thalamogeniculate branches off occlusion of thalamogeniculate branches off the PCAthe PCA
85

Q ti 5 Fib l iQ ti 5 Fib l iQuestion 5: FibromyalgiaQuestion 5: Fibromyalgia
1.1. ExistsExists2.2. Does not existDoes not exist3.3. Has formal diagnostic criteriaHas formal diagnostic criteria4.4. Can be fatalCan be fatal5.5. Is more common in men and the elderlyIs more common in men and the elderly6.6. Has abnormal EMGHas abnormal EMG--NCS correlatesNCS correlates
86

Explanation Question 5
Fibromyalgia has formal diagnostic criteria, it Fibromyalgia has formal diagnostic criteria, it is more common in women and is not fatal. is more common in women and is not fatal. There are various abnormal correlative There are various abnormal correlative findings in research studies but no objective findings in research studies but no objective g jg jdiagnostic tests.diagnostic tests.
Whether it “exists” as an independent diseaseWhether it “exists” as an independent disease Whether it exists as an independent disease Whether it exists as an independent disease is a matter or controversy (right now)is a matter or controversy (right now)
87

Questions and Answers

Answer KeyQ ti 1 3Q ti 1 3 Question 1: 3Question 1: 3
Question 2: 4Question 2: 4 Question 3: 5Question 3: 5 Question 4: 4Question 4: 4 Question 4: 4Question 4: 4 Question 5: 3Question 5: 3
89