pi is 0300571215000305
DESCRIPTION
JournalTRANSCRIPT

JJOD-2418; No. of Pages 10
Effectiveness of various toothpastes on dentinetubule occlusion
W.H. Arnold *, M. Prange, E.A. Naumova
Department of Biological and Material Sciences in Dentistry, Witten/Herdecke University, Witten, Germany
j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x
a r t i c l e i n f o
Article history:
Received 22 December 2014
Received in revised form
29 January 2015
Accepted 31 January 2015
Available online xxx
Keywords:
Toothpaste
Dentine
Dentine tubules
Root dentine
Hypersensitivity
a b s t r a c t
Objective: Dentine hypersensitivity is an increasing problem in dentistry. Several products
are available that claim to occlude open dentine tubules and to reduce dentine hypersensi-
tivity. The aim of this study was to investigate the effectiveness of several different products
on dentine tubule occlusion using qualitative and quantitative methods.
Materials and methods: Dentine discs were prepared from extracted human premolars and
molars. The dentine discs were brushed with 6 different experimental toothpastes, 1
positive control toothpaste and 1 negative control without toothpaste; the brushing simu-
lated a total brushing time of 1 year. Half of the discs were etched with lemon juice after
toothpaste application. Standardized scanning electron microphotographs were taken and
converted into binary black and white images. The black pixels, which represented the open
dentine tubules, were counted and statistically evaluated. Then, half of the dentine discs
were broken, and the occlusion of the dentine tubules was investigated using energy
dispersive X-ray spectroscopy (EDS).
Results: The number of open dentine tubules decreased significantly after brushing with 5 of
the 6 tested toothpastes. A significant effect was observed after acid erosion for 3 of the 6
tested toothpastes. EDS revealed partly closed dentine tubules after brushing with 3 tooth-
pastes; however, no partly closed dentine tubules were observed after acid erosion.
Conclusions: Some toothpastes are capable of partial dentine tubule occlusion. This occlu-
sion is unstable and can be removed with acid erosion.
Clinical significance: Desensitizing toothpastes are the most common products that are used
against dentine hypersensitivity, and these toothpastes affect dentine tubule occlusion.
# 2015 The Authors. Published by Elsevier Ltd. This is an open access article under the CC
BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.intl.elsevierhealth.com/journals/jden
1. Introduction
As the demographics of the human population change and as
the human population ages, more teeth remain in the mouths
of elderly people due to effective caries prevention and
periodontal disease management. Thus, dentine hypersensi-
tivity is becoming an increasing problem in dentistry.1,2
* Corresponding author at: Department of Biological and Material SGermany. Tel.: +49 2302926658; fax: +49 2302926661.
E-mail address: [email protected] (W.H. Arnold).
Please cite this article in press as: Arnold WH, et al. Effectiveness of variouhttp://dx.doi.org/10.1016/j.jdent.2015.01.014
http://dx.doi.org/10.1016/j.jdent.2015.01.0140300-5712/# 2015 The Authors. Published by Elsevier Ltd. This is
creativecommons.org/licenses/by-nc-nd/4.0/).
Dentine hypersensitivity and a possible cause for this
condition were described first by Gysi in 1900.3 Since then,
the mechanisms causing this type of pain have remained
controversial. Pulpal nerves from the plexus of Raschkow
extend into approximately 15% of the dentine tubule length.4
These nerves do not innervate the peripheral dentine.
Odontoblast processes may function as sensory receptors;
however, odontoblast destruction does not cause insensitive
ciences in Dentistry, Alfred Herrhausenstrasse 44, 58455 Witten,
s toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),
an open access article under the CC BY-NC-ND license (http://

j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x2
JJOD-2418; No. of Pages 10
dentine.5,6 In addition, no synaptic contacts exist between the
somatic nerves and odontoblasts.7 In 1968, Brannstrom
postulated the hydrodynamic theory, which hypothesizes
that fluid movement from the pulp towards the outer dentine
within the dentine tubules causes dentine sensation.8–10 The
hydrodynamic theory is now widely accepted as the cause of
dentine sensitivity. Open dentine tubules may be the reason
for the increased fluid movement that causes dentine
hypersensitivity.2,11–13 This possibility is supported by the
observation that dentine hypersensitivity directly correlates
with the number of open dentine tubules.14
Numerous home-use desensitizing products for the
treatment of dentine hypersensitivity are currently avail-
able. These products are divided into two categories:
products that block the pulp nerve response and products
that occlude open dentine tubules.1 The first group is
composed of products that contain potassium salts. Potassi-
um is thought to diffuse inside the dentine tubules and lower
the excitability of the pulpal nerve fibres. Several arguments
oppose this theory. One is that the diffusion distance in
human teeth is greater than that in tested animals. Another
argument is that the flow of dentinal fluid is outward from
the pulp towards the tooth surface, which would hinder
diffusion towards the pulp.16 The majority of home-use
desensitizing products belong to the second group and
contain a wide variety of active components. These active
components can be divided into several subgroups, which
are summarized in Table 1.
The effect of strontium salts is thought to be attributable to
their ability to absorb onto the connective tissue of dentine
and to form strontium apatite, which may occlude the dentine
tubules.17–19 However, dentine tubule occlusion by strontium
salts has not been proven. Clinical studies have demonstrated
a reduction of pain perception in patients who used strontium
salts.20–22
Recent investigations have demonstrated that arginine
combined with calcium carbonate occlude dentine tubules
and that this deposit converts to calcium phosphate.13,23
However, many calcium phosphates are soluble in acidic
environments and, therefore, unstable upon dietary acid
challenge. Several randomized controlled clinical trials have
demonstrated clear treatment effects of arginine and calcium
carbonate toothpastes immediately and up to 8 weeks after
treatment.24–28
In vitro studies have shown that stannous fluoride
produces precipitates onto dentine; this precipitate is water-
and acid-resistant.29 These in vitro studies are supported by
Table 1 – Summary of substances that occlude dentinetubules.
Substance Literature
Strontium (chloride, acetate) 18,29,61
Stannous fluoride 30,31
Calcium sodium phosphosilicate 32,33,35,36
Oxalates 41,42,48
Fluorides 41
Arginine and calcium carbonate 2,15,23,24
Nanoparticles with various functionalizing agents 50–52,59,60
Please cite this article in press as: Arnold WH, et al. Effectiveness of variouhttp://dx.doi.org/10.1016/j.jdent.2015.01.014
randomized controlled clinical trials that demonstrated the
effective treatment of dentine hypersensitivity using stannous
fluoride.30,31
Calcium sodium phosphosilicates precipitate onto dentine
collagen as calcium phosphate and silicate, forming deposits
on the dentine surface and in dentine tubules.32–36 These
precipitates are water- and acid-resistant. Randomized con-
trolled clinical studies of calcium sodium phosphosilicates
have shown the effective treatment of dentine hypersensitiv-
ity compared to controls.37–40
Oxalates form calcium oxalate crystals within the dentine
tubules and act as desensitizing agents.41 This effect is
enhanced when combined with calcium chloride.42 Some
studies have demonstrated decreased hydrodynamic fluid
flow within the dentine tubules upon oxalate treatment, thus
reducing pain sensations.41,43–46 Another study demonstrated
that oxalates block dentinal fluid flow by forming precipitates
within the dentine tubules.47 However, a systematic review
regarding the effectiveness of oxalates in the treatment of
dentine hypersensitivity determined that that single treat-
ments of oxalates had no effect on dentine hypersensitivity
compared to placebos.48
The mechanisms of the action of fluorides in desensitiz-
ing dentine hypersensitivity remain unclear. Although most
toothpastes contain fluorides in some form, the incidence of
dentine hypersensitivity remain high. Fluorides, similar to
other desensitizing agents, may block the dentine tubules.
Fluorides enhance the mineralization of hydroxyapatite49
and may enhance hydroxyapatite formation within the
dentine tubules, which blocks fluid movement and reduces
pain. However, this enhancement has not been demon-
strated.
A novel approach in the development of desensitizing
agents is the use of various combinations of nanoparticles.50–
52 The idea behind this approach is that nanoparticles may
easily penetrate into dentine tubules and that these nano-
particles could act as mineralising agents that block fluid
movement within the dentine tubules when combined with
various agents.
Considering that almost all desensitizing agents claim to
occlude open dentine tubules, the aim of this study was to
investigate quantitatively the effectiveness of various sub-
stances on dentine tubule occlusion.
2. Material and methods
Seventy-eight caries-free extracted human molars were used
for this experimental study. The collection of the teeth was
approved by the ethical committee of Witten/Herdecke
University (116/2013). Informed verbal consent was obtained
from the patients before the use of the teeth. The teeth were
stored in 0.9% NaCl containing 0.1% thymol until use.
2.1. Experimental design
Dentine discs with a thickness of 3 mm were cut from the
teeth using a saw microtome (Leica 1600, Leitz, Wetzlar,
Germany). Twelve dentine discs were used for each brushing
experiment with the different toothpastes. The discs were
s toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),

Table 2 – Active ingredients of the desensitizing toothpastes used.
Toothpaste # Product name Active ingredient Company
1 Elmex Sensitive Professional Pro-Argin, calcium carbonate GABA
2 Sensodyne Rapid Strontium acetate Glaxo Smith Kline
3 Sensodyne Repair Stannous fluoride Glaxo Smith Kline
4 BioRepair Zinc-carbonate hydroxyapatite Dr. K. Wolff
5 Colgate Total Sensitive New silica Colgate-Palmolive
6 Dontodent Sensitive Tetrapotassium pyrophosphate, hydroxyapatite DM Dogeriemarkt
j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x 3
JJOD-2418; No. of Pages 10
mounted on specimen holders, and the dentine surface was
polished. Before the experiment, the dentine surface was
eroded with lemon juice (Hitchcock, Monchengladbach,
Germany) for 30 s. Then, the discs were placed in a tooth
brushing machine, and a tooth brushing time of six months
was simulated (2 h of continuous brushing, assuming 28 teeth
in an oral cavity and 2� 3 min tooth brushing per day). Slurries
were prepared in a dilution of 1:3 toothpaste/water mixture.
The dentine discs were brushed with the Dr. Best classic
(medium) toothbrush at 120 spm and a slurry flow rate during
tooth brushing of 10 ml per minute. The toothbrush load was
2 N. Six discs were prepared directly for scanning electron
microscopic (SEM) investigation, and the six remaining discs
were eroded with lemon juice for 30 s and then prepared for
SEM investigation.
2.2. Toothpastes
Five different commercially available toothpastes against
hypersensitivity were used. All toothpastes had different
active components, which are summarized in Table 2. The
following toothpastes were used: Elmex toothpaste (CP-
GABA, Hamburg, Germany; toothpaste 0), which served as
the positive control; Elmex Sensitive Professional (CP-GABA,
Hamburg, Germany; toothpaste 1); Sensodyne Rapid (Glaxo
Smith Kline, Brentford, Middlesex, United Kingdom; tooth-
paste 2); Sensodyne Repair (Glaxo Smith Kline, Brentford,
Middlesex, United Kingdom; toothpaste 3); BioRepair Sensi-
tive (Dr. K. Wolff GmbH, Bielefeld, Germany; toothpaste 4);
Colgate Total Sensitive (Colgate-Palmolive, Hamburg,
Germany; toothpaste 5); and Dontodent Sensitive (DM-
Drogerie Markt, Karlsruhe, Germany; toothpaste 6). Six
dentine discs were only brushed with artificial saliva as the
negative controls.7
Fig. 1 – Preparation of microphotographs for the quantitative det
converted binary black and white image.
Please cite this article in press as: Arnold WH, et al. Effectiveness of variouhttp://dx.doi.org/10.1016/j.jdent.2015.01.014
2.3. SEM investigation
All specimens were dehydrated in graded acetone, critical
point dried and sputter-coated with gold palladium. Then, the
specimens were examined under a scanning electron micro-
scope (Zeiss Sigma VP, Zeiss, Oberkochen, Germany) at 20 kV
acceleration voltage. Standardized images of the dentine discs
were acquired at a magnification of 1000�. Twenty images
were acquired per disc. In addition, energy dispersive X-ray
spectroscopy (EDS, EDAX Ametec; Mahwah, NJ, USA) and
the accompanying product software were used to observe
the penetration of the toothpaste into the dentine tubules.
The X-ray signal for silicon served as evidence for the
toothpaste. Surface scans were made to study the covering
of the discs. Then, the specimens were frozen in liquid N2,
fractured and the penetration of silica from the toothpastes
into the open dentine tubules was studied.
2.4. Quantitative analysis of dentine tubule occlusion
The standardized SEM microphotographs were imported into
ImageJ software (NIH, USA) and converted into binary images.
The black (open dentine tubules) and white (occluded dentine
tubules and dentine) pixels (Fig. 1) were counted, and the
numbers were transferred into a Microsoft Excel worksheet.
2.5. Statistical analysis
The mean of all black pixels of each disc was calculated. These
mean values were compared between the different tooth-
pastes using the Wilcoxon–Mann–Whitney test for indepen-
dent variables and post hoc Bonferroni adjustment, which
resulted in a final p value of 0.0083. Descriptive statistics are
presented as boxplots. All calculations were performed with
ermination of closed dentine tubules. (a) SEM image and (b)
s toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),

j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x4
JJOD-2418; No. of Pages 10
SPSS (IBM Corporation, Armonk, NY, USA; Rel. 21) statistical
software.
3. Results
3.1. Quantitative evaluation
After tooth brushing, significant differences were found
between the brushed only negative control (#7) and tooth-
pastes 2 and 5. No differences were found between the
negative control and toothpastes 1, 3, 4 and 6 (Fig. 2). A
significant difference was found between the positive control
toothpaste (#0) and test toothpastes 2, 3, 4, 5 and 6 (Fig. 3). After
erosion with lemon juice, significant differences were found
between the negative control (#7) and toothpastes 2, 4 and 6
but not between the negative control and toothpastes 1, 3 and
5 (Fig. 4). After erosion with lemon juice, the number of open
dentine tubules was significantly different between the
positive control toothpaste and test toothpastes 3, 5, and 6
(Fig. 5).
3.2. SEM investigation combined with EDS analysis
The surface scans of the discs demonstrated irregular
coverage of the dentine surfaces by silica. No evidence of
silicon was found near the dentine surface within the open
dentine tubules of both controls (Fig. 6/0 and 6/7). A scattered
thin layer of silicon covered the dentine surface after the
Fig. 2 – Boxplot graphics of the quantitative determination of op
the negative control (without toothpaste). Significant difference
and 5.
Please cite this article in press as: Arnold WH, et al. Effectiveness of variouhttp://dx.doi.org/10.1016/j.jdent.2015.01.014
application of toothpaste 1 (Fig. 6/1). A clear thin layer of
silicon covered the dentine surface and the openings of the
dentine tubules after the application of toothpaste 2 (Fig. 6/2).
No clear silicon layer was observed after the application of
toothpaste 3 (Fig. 6/3). Several occluded dentine tubules were
found after the application of toothpaste 4 (Fig. 6/4). Neither a
silicon layer on the dentine surface nor occluded dentine
tubules were observed after the application of toothpastes 5
and 6 (Fig. 6/5 and 6/6).
4. Discussion
Gingival recession results in exposed dentine, which is the
primary cause of dentine hypersensitivity and which is an
increasing problem in dentistry. Consequently, several differ-
ent strategies have been developed for the treatment of
dentine hypersensitivity. These strategies emphasize the
application of various types of desensitizing dentifrices, which
are recommended as appropriate treatments in most cases.53
In principle, two alternative dentine hypersensitivity treat-
ment methods exist. The first method is the blockage of the
nerve transmission in the pulp, and the second method is
dentine tubule occlusion to block the hydrodynamic mecha-
nism in the dentine tubules. Potassium ions block the nerve
response of the A-beta and A-delta nerve fibres1 and diminish
the pain caused by external stimuli. Several different
potassium-containing toothpastes are available. Potassium-
based toothpastes are often combined with other ingredients
en dentine tubules after tooth brushing. Comparison with
s were observed between the controls and toothpastes 2
s toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),
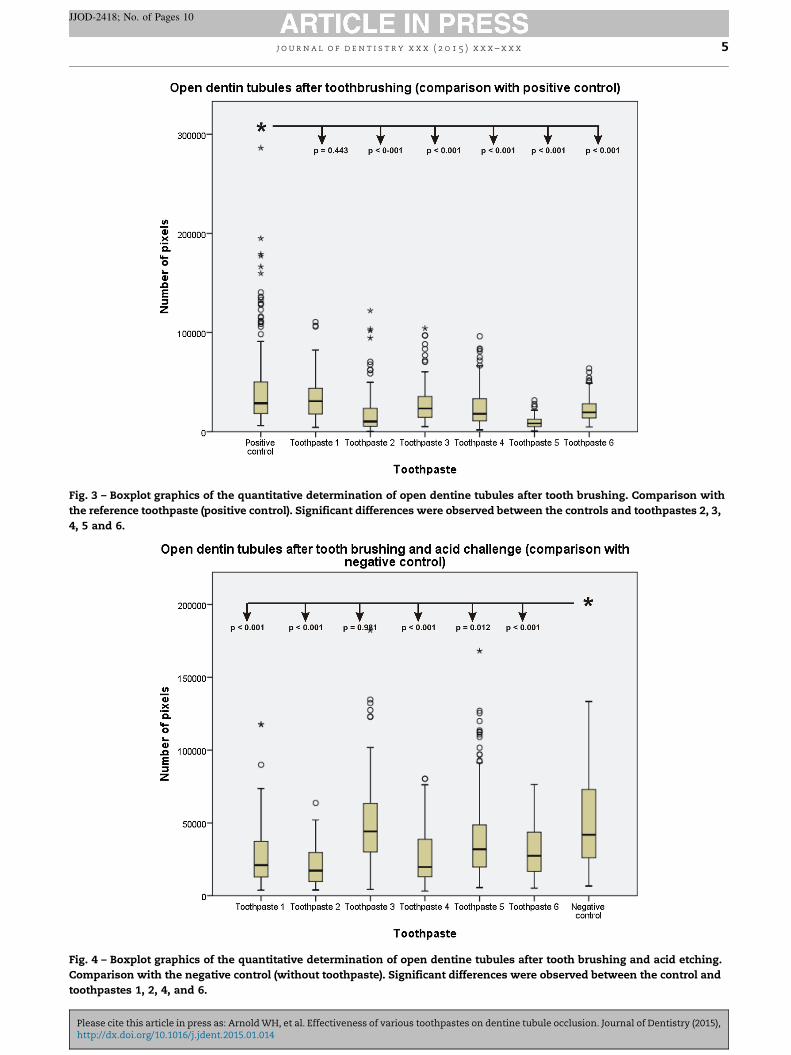
Fig. 3 – Boxplot graphics of the quantitative determination of open dentine tubules after tooth brushing. Comparison with
the reference toothpaste (positive control). Significant differences were observed between the controls and toothpastes 2, 3,
4, 5 and 6.
Fig. 4 – Boxplot graphics of the quantitative determination of open dentine tubules after tooth brushing and acid etching.
Comparison with the negative control (without toothpaste). Significant differences were observed between the control and
toothpastes 1, 2, 4, and 6.
j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x 5
JJOD-2418; No. of Pages 10
Please cite this article in press as: Arnold WH, et al. Effectiveness of various toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),http://dx.doi.org/10.1016/j.jdent.2015.01.014

Fig. 5 – Boxplot graphics of the quantitative determination of open dentine tubules after tooth brushing and acid etching.
Comparison with the reference toothpaste (positive control). Significant differences were observed between the control and
toothpastes 3, 5, and 6.
j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x6
JJOD-2418; No. of Pages 10
to increase the benefits, and numerous clinical studies
regarding potassium-based toothpastes have been performed,
with differing results. Some of these studies reported no
difference between potassium-based toothpastes and regular
fluoridated toothpastes,54,55 whereas other studies raised
some doubts regarding the clinical evidence of the effectivity
of potassium-containing toothpastes.11,56–58 One toothpaste
that was used in this study contained potassium and
hydroxyapatite for the occlusion of dentine tubules; however,
occlusion could not be verified.
Dentine tubule occlusion is achieved in two different ways,
by either the deposition of an occluding layer on top of the
dentine or the introduction of occluding material into dentine
tubules. Insoluble salts usually form a thin deposition on the
dentine. Hydroxyapatite; arginine, in combination with calcium
carbonate (Pro-Argin technology)2,15,23,24; or various nanopar-
ticles with different functionalised agents50,59,60 are used for the
induction of intratubular mineralisation. Several different
active ingredients are available and are summarized in Table 2.
In vitro studies have shown that strontium acetate or
strontium chloride (SrCl2) treatment forms small crystalline
deposits on the dentine surface, which can easily be washed
away.29,61 Controversial reports regarding the clinical effects
of strontium exist. Several studies have reported positive
effects of SrCl2 or Sr acetate on dentine hypersensitivity
relief.17,19,28,36,62 One study found that SrCl2 is less effective
than conventional fluoride-containing products.21 Another
Please cite this article in press as: Arnold WH, et al. Effectiveness of variouhttp://dx.doi.org/10.1016/j.jdent.2015.01.014
study found no significant differences between SnCl2-contain-
ing toothpastes and conventional fluoride-containing tooth-
pastes.55 However, only one study that reported a positive
effect of SrCl2 and that fulfilled the criteria for evidence-based
dentistry has been identified.63,64 Sr acetate was shown to
form a thin occluding layer on the dentine surface in the
present in vitro study; however, no tags could be found in the
tubule openings.
Another active ingredient is SnF2. Several studies regarding
the clinical efficacy of SnF2 have been published, with
controversial results. Some studies reported positive effects
of SnF2,30,31,65 whereas another study was neutral and found
no difference between SnF2-containing toothpastes and
conventional toothpastes.66 No dentinal occlusion of the
cross-sections of dentine could be observed after treatment
with SnF2-containing toothpaste in the present study. The top
view demonstrated single occluded tubules.
Oxalates were introduced for the treatment of dentine
hypersensitivity in the early 1980s. Some studies reported good
effectiveness of oxalates in reducing dentine hypersensitivi-
ty.41,44–46 This effectiveness may be due to the precipitation of
oxalates within the dentine tubules and to their relative
insolubility, which reduces hydraulic conductivity in the
dentine tubules.47,67 However, a meta-analysis of the published
papers regarding oxalates found little evidence regarding a
positive clinical effect of oxalates.48 No oxalate-containing
toothpaste was tested in the present study.
s toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),

Fig. 6 – Cross-sections of dentine discs with dentine tubule occlusion. The toothpastes are identified by EDS silicon mapping
(pink). Ca is mapped in blue. A weak positive signal for silicon is visible on the surface but not in the tubule openings after
treatment with toothpastes 1, 2 and 7. No signal could be detected after treatment with toothpastes 3, 5, and 6. Several
dentine tubules were occluded after treatment with toothpaste 4.
j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x 7
JJOD-2418; No. of Pages 10
Please cite this article in press as: Arnold WH, et al. Effectiveness of various toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),http://dx.doi.org/10.1016/j.jdent.2015.01.014

j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x8
JJOD-2418; No. of Pages 10
A relatively new method is arginine-calcium carbonate
technology (Pro-Argin technology), which was introduced in
2002.68 Several in vitro studies demonstrated a good occluding
effect of Pro-Argin technology on open dentine tubules.34,69–72
Clinical studies of Pro-Argin technology supported the in vitro
results and showed instant relief of dentine hypersensitivi-
ty.24,73
Currently, no in vitro or in vivo studies regarding the
occluding effects of zinc-carbonate hydroxyapatite on dentine
tubules are available; only reports regarding the effects of
zinc-carbonate hydroxyapatite on enamel have been pub-
lished. Several occluded dentine tubules could be found in the
dentine cross-sections after zinc-carbonate hydroxyapatite
treatment (toothpaste # 4) in the present study. This finding
was supported by the surface scan results, and this occluding
effect was not resistant to acid challenge with lemon juice.
5. Conclusion
Taken together, these results indicate that certain toothpastes
occlude dentine tubules. This occlusion is superficial and may
be dissolved with acids. Dentine tubule occlusion is dependent
on the active ingredient and is not complete in any of the
tested toothpastes.
Acknowledgments
The authors would like to thank Mrs. Susanne Haußman for
her technical assistance preparing the SEM specimens. Elmex
toothpaste was provided by CP Gaba, Hamburg, Germany.
r e f e r e n c e s
1. Addy M, West NX. The role of toothpaste in the aetiologyand treatment of dentine hypersensitivity. Monographs inOral Science 2013;23:75–87.
2. Cummins D. Dentin hypersensitivity: from diagnosis to abreakthrough therapy for everyday sensitivity relief. Journalof Clinical Dentistry 2009;20:1–9.
3. Gysi A. An attempt to explain the sensitivness of dentine.British Journal of Dental Science 1900;43:865–8.
4. Byers MR, Dong WK. Autoradiographic location of sensorynerve endings in dentin of monkey teeth. The AnatomicalRecord 1983;205:441–54.
5. Hirvonen TJ, Narhi MV. The effect of dentinal stimulation onpulp nerve function and pulp morphology in the dog. Journalof Dental Research 1986;65:1290–3.
6. Lilja J, Nordenvall KJ, Branstrom M. Dentin sensitivity,odontoblasts and nerves under desiccated or infectedexperimental cavities. A clinical, light microscopic andultrastructural investigation. Swedish Dental Journal 1982;6:93–103.
7. Byers MR, Kish SJ. Delineation of somatic nerve endings inrat teeth by radioautography of axon-transported protein.Journal of Dental Research 1976;55:419–25.
8. Brannstrom M, Astrom A. The hydrodynamics of thedentine; its possible relationship to dentinal pain.International Dental Journal 1972;22:219–27.
9. Brannstrom M, Linden LA, Johnson G. Movement of dentinaland pulpal fluid caused by clinical procedures. Journal ofDental Research 1968;47:679–82.
Please cite this article in press as: Arnold WH, et al. Effectiveness of variouhttp://dx.doi.org/10.1016/j.jdent.2015.01.014
10. Matthews B, Vongsavan N. Interactions between neural andhydrodynamic mechanisms in dentine and pulp. Archives ofOral Biology 1994;39:87S–95S.
11. Markowitz K, Pashley DH. Discovering new treatments forsensitive teeth: the long path from biology to therapy.Journal of Oral Rehabilitation 2008;35:300–15.
12. Petersson LG. The role of fluoride in the preventivemanagement of dentin hypersensitivity and root caries.Clinical Oral Investigations 2013;17:S63–71.
13. Petrou I, Heu R, Stranick M, Lavender S, Zaidel L, CumminsD, et al. A breakthrough therapy for dentin hypersensitivity:how dental products containing 8% arginine and calciumcarbonate work to deliver effective relief of sensitive teeth.Journal of Clinical Dentistry 2009;20:23–31.
14. Absi EG, Addy M, Adams D. Dentine hypersensitivity. Thedevelopment and evaluation of a replica technique to studysensitive and non-sensitive cervical dentine. Journal ofClinical Periodontology 1989;16:190–5.
15. Peacock JM, Orchardson R. Effects of potassium ions onaction potential conduction in A- and C-fibers of rat spinalnerves. Journal of Dental Research 1995;74:634–41.
16. Pashley DH, Matthews WG. The effects of outward forcedconvective flow on inward diffusion in human dentinein vitro. Archives of Oral Biology 1993;38:577–82.
17. Gedalia I, Brayer L, Kalter N, Richter M, Stabholz A. Theeffect of fluoride and strontium application on dentin:in vivo and in vitro studies. Journal of Periodontology1978;49:269–72.
18. Kun L. Etude biophysique des modifications des tissuesdentaires provoquees par l’application totale de Strontium.Schweiz Monatschr Zahnheilk 1976;86:661–7.
19. Ross MR. Hypersensitive teeth: effect of strontium chloridein a compatible dentifrice. Journal of Periodontology1961;32:49–53.
20. Gillam DG, Newman HN, Davies EH, Bulman JS. Clinicalefficacy of a low abrasive dentifrice for the relief of cervicaldentinal hypersensitivity. Journal of Clinical Periodontology1992;19:197–201.
21. Pearce NX, Addy M, Newcombe RG. Dentinehypersensitivity: a clinical trial to compare 2 strontiumdensensitizing toothpastes with a conventional fluoridetoothpaste. Journal of Periodontology 1994;65:113–9.
22. Silverman G, Berman E, Hanna CB, Salvato A, FratarcangeloP, Bartizek RD, et al. Assessing the efficacy of threedentifrices in the treatment of dentinal hypersensitivity. TheJournal of the American Dental Association 1996;127:191–201.
23. Lavender SA, Petrou I, Heu R, Stranick MA, Cummins D,Kilpatrick-Liverman L, et al. Mode of action studies on a newdesensitizing dentifrice containing 8.0% arginine, a highcleaning calcium carbonate system and 1450 ppm fluoride.American Journal of Dentistry 2010;23:14A–9A.
24. Ayad F, Ayad N, Zhang YP, DeVizio W, Cummins D, MateoLR. Comparing the efficacy in reducing dentinhypersensitivity of a new toothpaste containing 8.0%arginine, calcium carbonate, and 1450 ppm fluoride to acommercial sensitive toothpaste containing 2% potassiumion: an eight-week clinical study on Canadian adults. Journalof Clinical Dentistry 2009;20:10–6.
25. Docimo R, Montesani L, Maturo P, Costacurta M, BartolinoM, Zhang YP, et al. Comparing the efficacy in reducingdentin hypersensitivity of a new toothpaste containing 8.0%arginine, calcium carbonate, and 1450 ppm fluoride to abenchmark commercial desensitizing toothpastecontaining 2% potassium ion: an eight-week clinical studyin Rome, Italy. Journal of Clinical Dentistry 2009;20:137–43.
26. Fu Y, Li X, Que K, Wang M, Hu D, Mateo LR, et al. Instantdentin hypersensitivity relief of a new desensitizingdentifrice containing 8.0% arginine, a high cleaning calciumcarbonate system and 1450 ppm fluoride: a 3-day clinical
s toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),

j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x 9
JJOD-2418; No. of Pages 10
study in Chengdu, China. American Journal of Dentistry2010;23:20A–7A.
27. Que K, Fu Y, Lin L, Hu D, Zhang YP, Panagakos FS, et al.Dentin hypersensitivity reduction of a new toothpastecontaining 8.0% arginine and 1450 ppm fluoride: an 8-weekclinical study on Chinese adults. American Journal of Dentistry2010;23:28A–35A.
28. Schiff T, Delgado E, Zhang YP, DeVizio W, Cummins D,Mateo LR. The clinical effect of a single direct topicalapplication of a dentifrice containing 8.0% arginine, calciumcarbonate, and 1450 ppm fluoride on dentinhypersensitivity: the use of a cotton swab applicator versusthe use of a fingertip. Journal of Clinical Dentistry 2009;20:131–136.
29. Addy M, Mostafa P. Dentine hypersensitivity. I. Effectsproduced by the uptake in vitro of metal ions, fluoride andformaldehyde onto dentine. Journal of Oral Rehabilitation1988;15:575–85.
30. Blong MA, Volding B, Thrash WJ, Jones D. Effects of a gelcontaining 0.4% stannous fluoride on dentinalhypersensitivity. Dental Hygiene 1985;59:489–92.
31. Thrash WJ, Dodds MW, Jones DL. The effect of stannousfluoride on dentinal hypersensitivity. International DentalJournal 1994;44:107–18.
32. Earl JS, Leary RK, Muller KH, Langford RM, Greenspan DC.Physical and chemical characterization of dentin surfacefollowing treatment with NovaMin technology. Journal ofClinical Dentistry 2011;22:62–7.
33. Cummins D. Advances in the clinical management of dentinhypersensitivity: a review of recent evidence for the efficacyof dentifrices in providing instant and lasting relief. Journalof Clinical Dentistry 2011;22:100–7.
34. Joshi S, Gowda AS, Joshi C. Comparative evaluation ofNovaMin desensitizer and Gluma desensitizer on dentinaltubule occlusion: a scanning electron microscopic study.Journal of Periodontal & Implant Science 2013;43:269–75.
35. LaTorre G, Greenspan DC. The role of ionic release fromNovaMin (calcium sodium phosphosilicate) in tubuleocclusion: an exploratory in vitro study using radio-labeledisotopes. Journal of Clinical Dentistry 2010;21:72–6.
36. Layer TM. Development of a fluoridated, daily-usetoothpaste containing NovaMin technology for thetreatment of dentin hypersensitivity. Journal of ClinicalDentistry 2011;22:59–61.
37. Du Min Q, Bian Z, Jiang H, Greenspan DC, Burwell AK, ZhongJ, et al. Clinical evaluation of a dentifrice containing calciumsodium phosphosilicate (novamin) for the treatment ofdentin hypersensitivity. American Journal of Dentistry2008;21:210–4.
38. Litkowski L, Greenspan DC. A clinical study of the effect ofcalcium sodium phosphosilicate on dentin hypersensitivity– proof of principle. Journal of Clinical Dentistry 2010;21:77–81.
39. Pradeep AR, Sharma A. Comparison of clinical efficacy of adentifrice containing calcium sodium phosphosilicate to adentifrice containing potassium nitrate and to a placebo ondentinal hypersensitivity: a randomized clinical trial. Journalof Periodontology 2010;81:1167–73.
40. Salian S, Thakur S, Kulkarni S, LaTorre G. A randomizedcontrolled clinical study evaluating the efficacy of twodesensitizing dentifrices. Journal of Clinical Dentistry2010;21:82–7.
41. Greenhill JD, Pashley DH. Effects of desensitizing agents onthe hydraulic conductance of human dentine in vitro.Journal of Dental Research 1981;60:686–98.
42. Suge T, Kawasaki A, Ishikawa K, Matsuo T, Ebisu S. Effectsof pre- or post-application of calcium chloride on occludingability of potassium oxalate for the treatment of dentinhypersensitivity. American Journal of Dentistry 2005;18:121–5.
Please cite this article in press as: Arnold WH, et al. Effectiveness of variouhttp://dx.doi.org/10.1016/j.jdent.2015.01.014
43. Addy M, Dowell P. Dentine hypersensitivity: effect ofinteractions between metal salts, fluoride andchlorhexidine on the uptake by dentine. Journal of OralRehabilitation 1986;13:599–605.
44. Pashley DH, Galloway SE. The effects of oxalate treatmenton the smear layer of ground surfaces of human dentine.Archives of Oral Biology 1985;30:731–7.
45. Pashley DH, Livingston MJ, Reeder OW, Horner J. Effects of thedegree of tubule occlusion on the permeability of humandentine in vivo. Archives of Oral Biology 1978;23:1127–33.
46. Pashley DH, O’Meara JA, Kepler EE, Galloway SE, ThompsonSM, Stewart FP. Dentin permeability. Effects of desensitizingdentifrices in vitro. Journal of Periodontology 1984;55:522–5.
47. Cuenin MF, Scheidt MJ, O’Neal RB, Strong SL, Pashley DH,Horner JA, et al. An in vivo study of dentin sensitivity: therelation of dentin sensitivity and the patency of dentintubules. Journal of Periodontology 1991;62:668–73.
48. Cunha-Cruz J, Stout JR, Heaton LJ, Wataha JC. Dentinhypersensitivity and oxalates: a systematic review. Journal ofDental Research 2011;90:304–10.
49. Naumova EA, Gaengler P, Zimmer S, Arnold WH. Influenceof individual saliva secretion on fluoride bioavailability. TheOpen Dentistry Journal 2010;4:185–90.
50. Kovtun A, Kozlova D, Ganesan K, Biewald C, Seipold N,Gaengler P, et al. Chlorhexidine-loaded calcium phosphatenanoparticles for dental maintenance treatment:combination of mineralising and antibacterial effects. RSCAdvances 2012;2:870–5.
51. Tian L, Peng C, Shi Y, Guo X, Zhong B, Qi J, et al. Effect ofmesoporous silica nanoparticles on dentinal tubuleocclusion: an in vitro study using SEM and image analysis.Dental Materials Journal 2014;33:125–32.
52. Wang R, Wang Q, Wang X, Tian L, Liu H, Zhao M, et al.Enhancement of nano-hydroxyapatite bonding to dentinthrough a collagen/calcium dual affinitive peptide fordentinal tubule occlusion. Journal of Biomaterials Applications2014;29:268–77.
53. Canadian Advisory Board on Dentin Hypersensitivity.Consensus-based recommendations for the diagnosis andmanagement of dentin hypersensitivity. Journal of theCanadian Dental Association 2003;69:221–6.
54. Gillam DG, Bulman JS, Jackson RJ, Newman HN. Comparisonof 2 desensitizing dentifrices with a commercially availablefluoride dentifrice in alleviating cervical dentine sensitivity.Journal of Periodontology 1996;67:737–42.
55. West NX, Addy M, Jackson RJ, Ridge DB. Dentinehypersensitivity and the placebo response. A comparison ofthe effect of strontium acetate, potassium nitrate andfluoride toothpastes. Journal of Clinical Periodontology1997;24:209–15.
56. Orchardson R, Gillam DG. Managing dentinhypersensitivity. The Journal of the American Dental Association2006;137:990–8. quiz 1028–9.
57. Pashley DH, Tay FR, Haywood VB, Collins MC, Drisco CL.Dentin hypersensitivity: consensus-basedrecommendations for the diagnosis and management ofdentin hypersensitivity. Inside Dentistry 2008;4:1–35.
58. Poulsen S, Errboe M, Lescay Mevil Y, Glenny AM. Potassiumcontaining toothpastes for dentine hypersensitivity.Cochrane Database of Systematic Reviews 2006;3:CD00176.
59. Lee SY, Kwon HK, Kim BI. Effect of dentinal tubule occlusionby dentifrice containing nano-carbonate apatite. Journal ofOral Rehabilitation 2008;35:847–53.
60. Tschoppe P, Zandim DL, Martus P, Kielbassa AM. Enameland dentine remineralization by nano-hydroxyapatitetoothpastes. Journal of Dentistry 2011;39:430–7.
61. Addy M, Mostafa P. Dentine hypersensitivity. II. Effectsproduced by the uptake in vitro of toothpastes onto dentine.Journal of Oral Rehabilitation 1989;16:35–48.
s toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),

j o u r n a l o f d e n t i s t r y x x x ( 2 0 1 5 ) x x x – x x x10
JJOD-2418; No. of Pages 10
62. Mason S, Hughes N, Sufi F, Bannon L, Maggio B, North M, et al.A comparative clinical study investigating the efficacy of adentifrice containing 8% strontium acetate and 1040 ppmfluoride in a silica base and a control dentifrice containing1450 ppm fluoride in a silica base to provide immediate reliefof dentin hypersensitivity. Journal of Clinical Dentistry 2010;21:42–8.
63. Karim BF, Gillam DG. The efficacy of strontium andpotassium toothpastes in treating dentine hypersensitivity:a systematic review. International Journal of Dentistry2013;2013:573258.
64. Minkoff S, Axelrod S. Efficacy of strontium chloride in dentalhypersensitivity. Journal of Periodontology 1987;58:470–4.
65. He T, Barker ML, Biesbrock AR, Miner M, Qaqish J, Sharma N.A clinical study to assess the effect of a stabilized stannousfluoride dentifrice on hypersensitivity relative to a marketedsodium fluoride/triclosan control. Journal of Clinical Dentistry2014;25:13–8.
66. Sharma N, Roy S, Kakar A, Greenspan DC, Scott R. A clinicalstudy comparing oral formulations containing 7.5% calciumsodium phosphosilicate (NovaMin), 5% potassium nitrate,and 0.4% stannous fluoride for the management of dentinhypersensitivity. Journal of Clinical Dentistry 2010;21:88–92.
67. Pereira JC, Segala AD, Gillam DG. Effect of desensitizingagents on the hydraulic conductance of human dentinsubjected to different surface pre-treatments – an in vitrostudy. Dental Materials 2005;21:129–38.
Please cite this article in press as: Arnold WH, et al. Effectiveness of variouhttp://dx.doi.org/10.1016/j.jdent.2015.01.014
68. Kleinberg I. SensiStat. A new saliva-based composition forsimple and effective treatment of dentinal sensitivity pain.Dentistry Today 2002;21:42–7.
69. Cummins D. The efficacy of a new dentifrice containing8.0% arginine, calcium carbonate, and 1450 ppm fluoridein delivering instant and lasting relief of dentinhypersensitivity. Journal of Clinical Dentistry 2009;20:109–14.
70. Parkinson CR, Butler A, Willson RJ. Development of an acidchallenge-based in vitro dentin disc occlusion model. Journalof Clinical Dentistry 2010;21:31–6.
71. Parkinson CR, Willson RJ. An in vitro investigation of twocurrently marketed dentin tubule occlusion dentifrices.Journal of Clinical Dentistry 2011;22:6–10.
72. Patel R, Chopra S, Vandeven M, Cummins D. Comparison ofthe effects on dentin permeability of two commerciallyavailable sensitivity relief dentifrices. Journal of ClinicalDentistry 2011;22:108–12.
73. Nathoo S, Delgado E, Zhang YP, DeVizio W, Cummins D,Mateo LR. Comparing the efficacy in providing instant reliefof dentin hypersensitivity of a new toothpaste containing8.0% arginine, calcium carbonate, and 1450 ppm fluoriderelative to a benchmark desensitizing toothpaste containing2% potassium ion and 1450 ppm fluoride, and to a controltoothpaste with 1450 ppm fluoride: a three-day clinicalstudy in New Jersey, USA. Journal of Clinical Dentistry2009;20:123–30.
s toothpastes on dentine tubule occlusion. Journal of Dentistry (2015),