pkp techniques and tips - dry technique – instumentation; automated vs. manual –...
TRANSCRIPT
9/27/16
1
Corneal Transplantation for the Comprehensive
Ophthalmologist
Michael J. Taravella, MD Richard Davidson, MD University of Colorado
Rocky Mountain Lions Eye Institute 9/27/16 2
Financial Disclosure
• Dr. Taravella was a consultant for Surgical Specialties and has been involved in evaluating the Ultrafit trephine system and suture
• CURRENTLY I DO NOT RECEIVE ANY FINANCIAL SUPPORT, ROYALTIES OR OTHER FINANCIAL CONSIDERATIONS FROM ANGIOTECH/SURGICAL SPECIALTIES
9/27/16 3
Indications (EBAA)-2005
• Pseudophakic or aphakic bullous keratopathy --35%
• Endothelial dystrophy (Fuch’s)--10%
• keratoconus--10% • Trauma--3% • HSV/viral--2% • Regraft--10%
• Corneal dystrophy (stromal, macular, granular, lattice)--5%
• Corneal degenerations--4%
• Chemical injuries--.5% • Other--20% (post radial
keratotomy,uveitus, silicone oil,glaucoma)
9/27/16 4
Prognosis: (Best Indications 90%)
• Keratoconus • Endothelial dystrophies • Central scars • Corneal dystrophy(granular, lattice) • Unvascularized corneas in white quiet
eyes
9/27/16 5
Keratoconus
9/27/16 6
Fuch’s Dystrophy

9/27/16
2
9/27/16 7
DSAEK
• NOTE THAT DSAEK IS NOW THE PREFFERED METHOD OF SURGICAL TREATMENT FOR ENDOTHELIAL REPLACEMENT
• AS of 2011, about 50% of grafts in the US are DSAEK or EK
9/27/16 8
Granular dystrophy
9/27/16 9
Good Prognosis (90% success)
• Mild vascularity, lesion may involve corneal periphery
• Pseudophakic or Aphakic bullous keratopathy
• Inactive HSV
9/27/16 10
Pseudophakic Bullous Keratopathy
9/27/16 11
Poor Prognosis (50-75%) • Heavily vascularized quadrants
– 2 or more quadrants – chemical burns, OCP, Steven-Johnson
• Active HSV – Better prognosis with Acyclovir
• Multiple rejections • Uncontrolled glaucoma • Active inflammation
9/27/16 12
HSV Keratitis
9/27/16
3
9/27/16 13
Herpetic Stromal Keratitis
9/27/16 14
Severe Alkali Burn
9/27/16 15
Question 1
• Which of the following diagnosis has the best prognosis for success for a PKP? 1) HSV keratitis with active inflammation 2) A highly vascularized cornea with central
scarring following a chemical burn 3) A case of pseudophakic bullous keratopathy 4) Keratoconus with a dense central scar but
minimal blood vessels in the cornea 9/27/16 16
Definition of Success
• Clear, compact , thin graft • Improvement of VA of 2 or more lines • Low astigmatism (3 diopters)
9/27/16 17
Donor selection- Guidelines
• Age – Under 65?
• Endothelial Cell Count – >2500?
• Death to preservation time – 8 hours
• Storage media (OPTISOL) • Time to transplant
– Within 48-72hours 9/27/16 18
Pre-operative exam
• VA--overcorrect with contact lens • IOP: Tonopen • SLE • RETINA • LIDS, LASHES (trichiasis, exposure) • Schirmer’s Test
• Ocular Surface assessment • Fluoroscein, Lissamine green

9/27/16
4
9/27/16 19
Special Tests
• Ultrasound (Retinal detachment) – projection,color vision – Optic nerve (cupping)
• Visual Field testing • PAM
– Projected Acuity Meter
9/27/16 20
Question 2
• What is the definition of success for a cornea transplant? 1) A thin, clear compact graft with improvement
of vision of 2 or more lines and less than 3 diopters of astigmatism
2) Only if 20/20 vision is achieved 3) A graft is considered successful if there are
no rejection episodes in the first 3 years.
9/27/16 21
Question 3
• All of the following factors are considered in donor selection except: 1) Age 2) Cell count 3) Death to preservation time of donor and how
long donor has been in storage solution 4) Cause of death should not be related to
heart disease. 9/27/16 22
Operative Technique-Instruments
• To ring or not to ring? – Currently, preference is not to ring; may
be helpful in aphakic patients • Speculum • Trephine/punch selection • spatula • forceps • scissors
9/27/16 23
Suturing the Ring
• 6-0 vicryl suture on spatula needle • 2-3 mm from limbus
– through conjunctiva and into superficial sclera
– avoid perforation – suture TOWARDS cornea – avoid excess tension (astigmatism)
9/27/16 24
Suturing the Ring
9/27/16
5
9/27/16 25
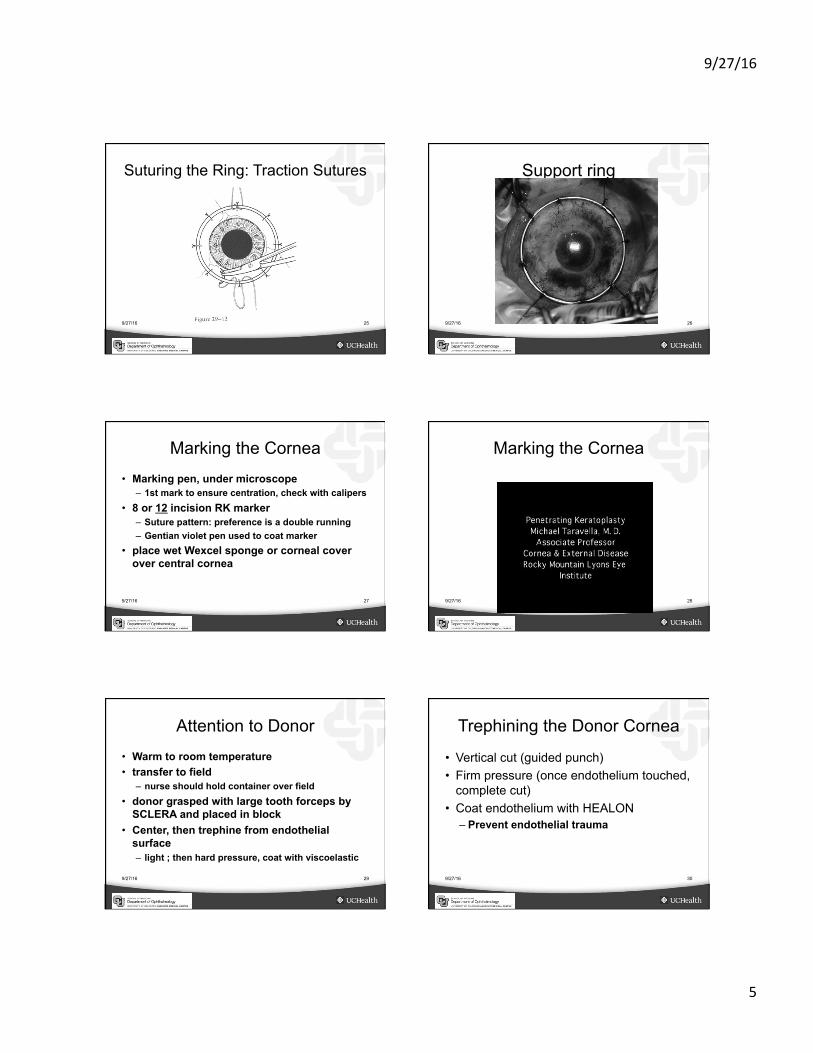
Suturing the Ring: Traction Sutures
9/27/16 26
Support ring
9/27/16 27
Marking the Cornea
• Marking pen, under microscope – 1st mark to ensure centration, check with calipers
• 8 or 12 incision RK marker – Suture pattern: preference is a double running – Gentian violet pen used to coat marker
• place wet Wexcel sponge or corneal cover over central cornea
9/27/16 28
Marking the Cornea
9/27/16 29
Attention to Donor
• Warm to room temperature • transfer to field
– nurse should hold container over field • donor grasped with large tooth forceps by
SCLERA and placed in block • Center, then trephine from endothelial
surface – light ; then hard pressure, coat with viscoelastic
9/27/16 30
Trephining the Donor Cornea
• Vertical cut (guided punch) • Firm pressure (once endothelium touched,
complete cut) • Coat endothelium with HEALON
– Prevent endothelial trauma

9/27/16
6
9/27/16 31
Trephining the Donor
9/27/16 32
Trephining the Donor
9/27/16 33
Trephination of Recipient
• Center under microscope – handheld versus suction – pressure in eye – perpendicular to iris/limbal plane
• Partial vs. full thickness
9/27/16 34
Suction Trephine
9/27/16 35
Trephining the recipient
9/27/16 36
Removing recipient button
• enter with micro-sharp blade • allow eye to decompress
– suprachoroidal hemorrhage • Corneal transplant scissors
– Cut to right up to 8 o’clock – Then cut to left – perpendicular, slight rim to protect iris and
help seal wound

9/27/16
7
9/27/16 37
Cutting the Recipient Cornea
9/27/16 38
Cutting the Recipient Cornea
9/27/16 39
Transfer donor to field
• Paton spatula • Right side up!!
9/27/16 40
Transferring The Donor
9/27/16 41
Suturing • 10-0 nylon
– 4 cardinals, 1st 2 must be 90 degrees apart • Running, double running, interrupted
combination – 16 interrupted for beginners – 8 interrupted with 16 bite running in between
• Good transition technique for learning how to place a running suture
– 24 bite running (least forgiving) • Depth of bite--full thickness?
9/27/16 42
Suturing Tips • Goal --good anterior and posterior wound
apposition – Deep bites – 1mm on donor side, 1.5 mm on recipient – avoid dulling needle tip or bending needle – use RK marker to help space bites
• Tighten sutures carefully! – keratometer; don’t pinch, don’t over-
tighten

9/27/16
8
9/27/16 43
Advantages of a Double Running Suture
• Harder to learn – Can cut first running while placing second
• But excellent anterior wound apposition – Wound leaks are rare with this pattern
• Criss-Cross pattern creates zone of compression – Back-up suture if one running breaks – Anti-torque – 10-0 versus 11-0 for second suture
• 11-0 may not have enough tensile strength
9/27/16 44
Suturing The Cornea: First Two Knots
9/27/16 45
Placing the Cardinal Sutures
9/27/16 46
Suturing the Cornea: Order of Placement
9/27/16 47
Interrupted Sutures: Knots
9/27/16 48
Tightening the Running Suture

9/27/16
9
9/27/16 49
Tightening a Running Suture
• Start at surgeon 6 o’clock – Tighten by lifting suture, not pinching
• Sinskey hook or one side of tying forceps • Left side first, then right side
– Counter then clockwise
• Hold on to one end while tightening
• GOAL= remove slack; do not overtighten
9/27/16 50
Placing the Double Running Suture
9/27/16 51
Corneal Transplant: Single Running Suture
9/27/16 52
Question 4
• Which of the following is true in terms of suturing a corneal transplant? 1)7-0 Vicryl is the best choice for suture material 2) An interrupted suture technique is best for vascularized cornea 3) 10-0 nylon is too small a diameter to have proper tensile strength for most corneal transplants
9/27/16 53
Refill Anterior Chamber
• Sidell test (flourescein) for wound leaks • Watch iris carefully, avoid incarceration • Viscoelastic inside eye at end of
procedure?
9/27/16 54
Filling the AC and checking for wound leaks
9/27/16
10
9/27/16 55
Subconjunctival injections • Cefazolin (cephlasporin) • Celestone or Dexamethasone • gentamicin : Don’t recommend !
– (retinal toxicity) – Most infections are gram positive
9/27/16 56
Collagen Shield
• Soak in commercially available Moxifloxacin and Dexamethasone – 5 drops each – 5 minutes before applying – High pulse of meds to Anterior Chamber
9/27/16 57
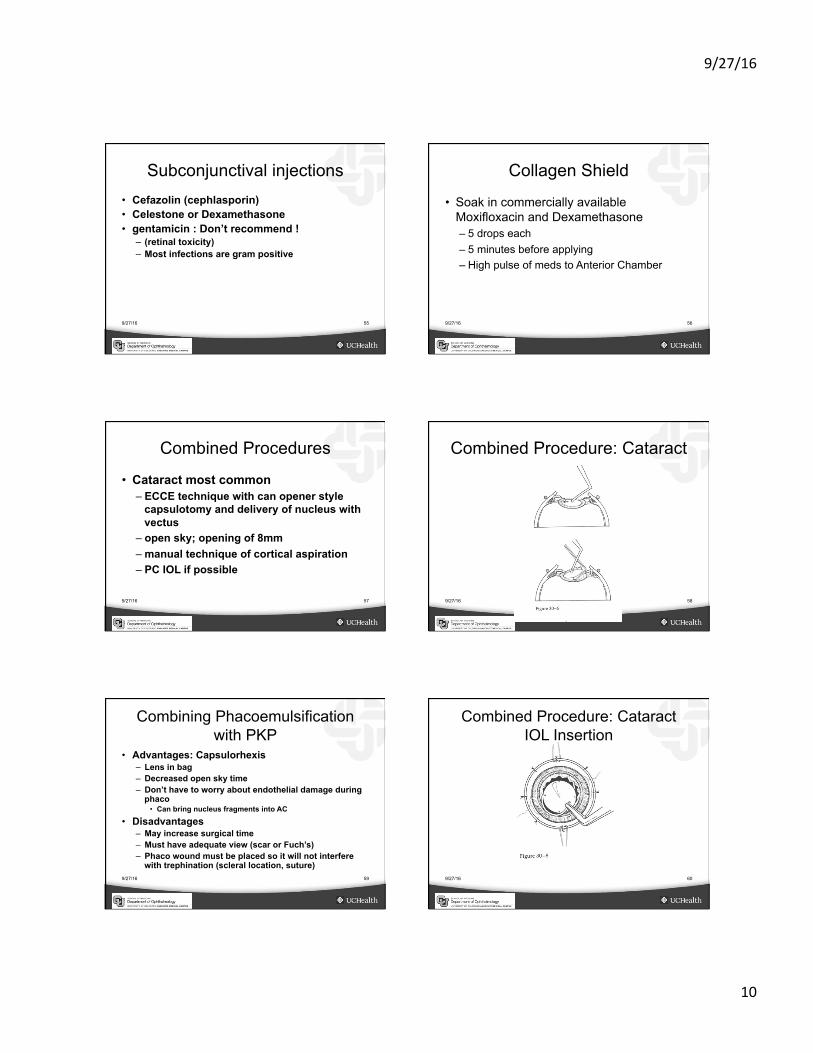
Combined Procedures
• Cataract most common – ECCE technique with can opener style
capsulotomy and delivery of nucleus with vectus
– open sky; opening of 8mm – manual technique of cortical aspiration – PC IOL if possible
9/27/16 58
Combined Procedure: Cataract
9/27/16 59
Combining Phacoemulsification with PKP
• Advantages: Capsulorhexis – Lens in bag – Decreased open sky time – Don’t have to worry about endothelial damage during
phaco • Can bring nucleus fragments into AC
• Disadvantages – May increase surgical time – Must have adequate view (scar or Fuch’s) – Phaco wound must be placed so it will not interfere
with trephination (scleral location, suture) 9/27/16 60
Combined Procedure: Cataract IOL Insertion

9/27/16
11
9/27/16 61
Intraocular Lens Exchange
• Closed loop IOL – haptics cocooned in iris; special technique
• iris clip lens--watch for suture or clip • flexible loop AC IOL may be left in place • PC IOL may be left in place
– centration, haptic position
9/27/16 62
IOL replacement options • PC IOL in sulcus if enough capsular
support • Sutured-in PC IOL
– time consuming technique – blind passage of needle – risk of hemorrhage,tilt, exposure of
sutures • Flexible loop AC IOL
– proper size critical; angle support; PAS
9/27/16 63
Anterior Vitrectomy
• Aggressive removal of any vitreous in anterior segment in contact with the iris is recommended – dry technique – instumentation; automated vs. manual – endpoint?
9/27/16 64
Anterior Vitrectomy
9/27/16 65
Synechiolysis
• Blunt cyclodyalasis spatula or closed scissors – does it help? – avoid iris touch to back of cornea
9/27/16 66
Glaucoma Procedures
• Pressure should be well controlled • Consider filter or tube shunt procedure
prior to graft – Medications can be toxic to surface of
graft • Flat chamber can compromise graft
9/27/16
12
9/27/16 67
Post-op Care
• Usual regimen: 1 day, 1week, 1 month – may increase frequency of follow-up if needed
• Antibiotic choice – Polymixin/Trimethoprim or Ofloxacin/
Moxifloxacin – Topical Steroid coverage
• Prednisolone Acetate 1%
9/27/16 68
Intraoperative Complications • Expulsive choroidal hemorrhage
– incidence: .5% to 3% – myopia, glaucoma, hypertension, age – Prevention: soft eye, slow decompression
• mannitol, massage • Management
– recognition! – finger over trephination site, posterior
sclerotomy; close with 9-0 nylon or 9-0 vicryl interrupted
– Corneal “tacks”
9/27/16 69
Common Probems (EARLY)
• Epithelium – Patch 1st few days or bandage lens – toxicity of medications – preservative free tears – if chronic; punctal occlusion and tarsorrhaphy
• Wound leak – patch or bandage lens – resuture if no improvement in a few DAYS
9/27/16 70
Monitor Intraocular pressure
• Tonopen • Beta-blockers, ORAL carbonic
anhydrase inhibitors, alpha-adrenergic agents – Avoid pilocarpine in early post-op period – Trusopt: Endothelial toxicity? – Xalatan? (Prostaglandin analog)
• CME and inflammation • Critical to success of graft!!
9/27/16 71
Intermediate complications
• Poor wound apposition – resuture if necessary
• Astigmatism – monitor with topography, qualitative keratometer – selective suture removal
• Or add sutures (microdehiscence) – adjustment of running 10-0 nylon
• sinskey hook, tying forceps; avoid pinching
9/27/16 72
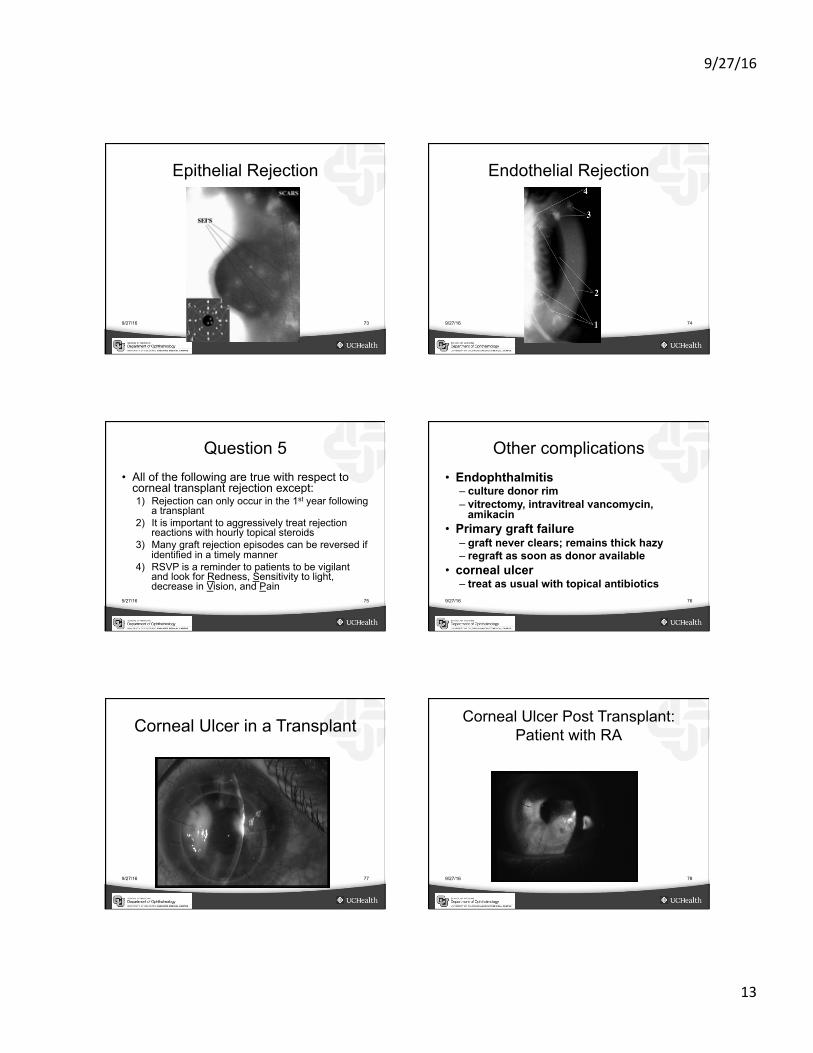
Late complications
• Rejection – Eye red, vision drops, increase in discomfort – Corneal edema involving donor, not recipient – KP, Khoudadoust line – can have epithelial rejection
• Increase topical steroids – consider systemic steroids, subconjunctival
injection – cyclosporine topically?
9/27/16
13
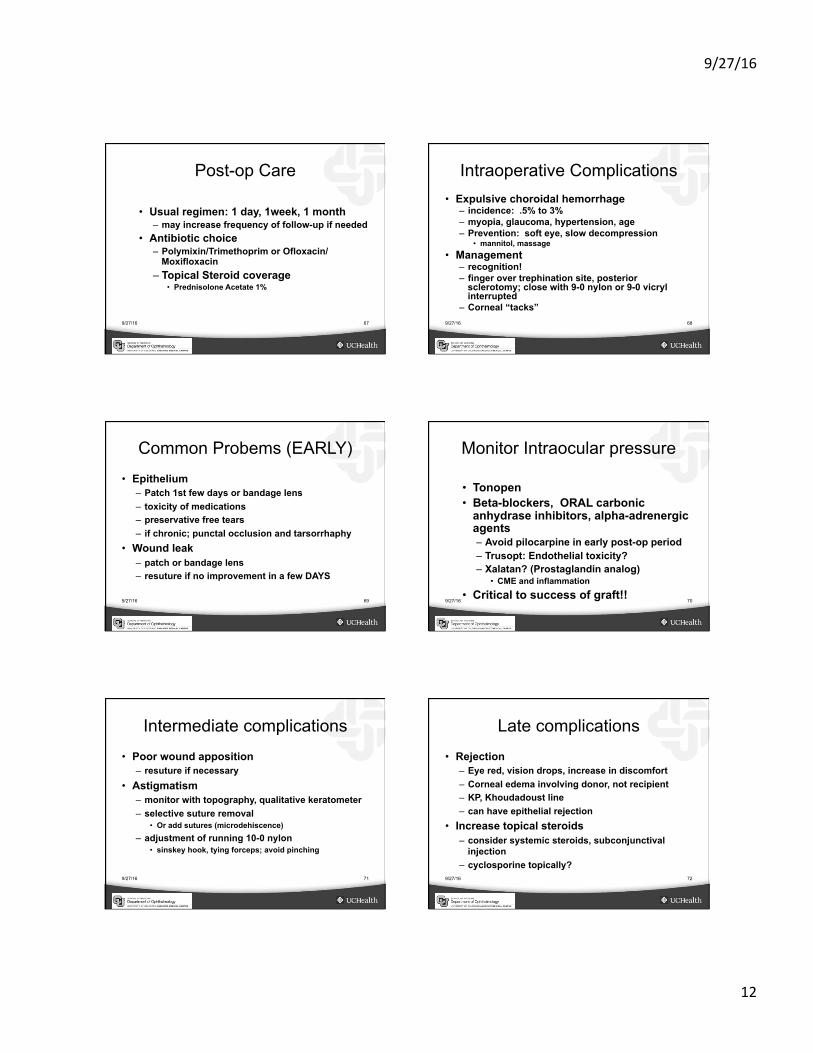
9/27/16 73
Epithelial Rejection
9/27/16 74
Endothelial Rejection
9/27/16 75
Question 5 • All of the following are true with respect to
corneal transplant rejection except: 1) Rejection can only occur in the 1st year following
a transplant 2) It is important to aggressively treat rejection
reactions with hourly topical steroids 3) Many graft rejection episodes can be reversed if
identified in a timely manner 4) RSVP is a reminder to patients to be vigilant
and look for Redness, Sensitivity to light, decrease in Vision, and Pain
9/27/16 76
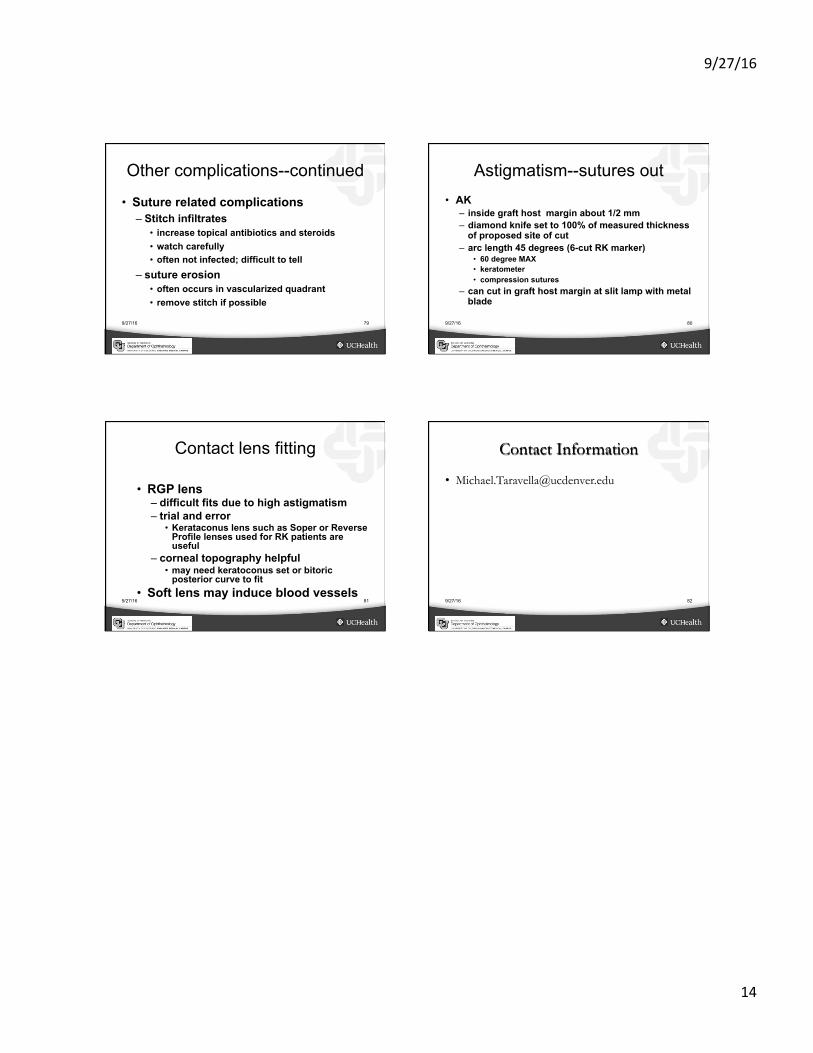
Other complications • Endophthalmitis
– culture donor rim – vitrectomy, intravitreal vancomycin,
amikacin • Primary graft failure
– graft never clears; remains thick hazy – regraft as soon as donor available
• corneal ulcer – treat as usual with topical antibiotics
9/27/16 77
Corneal Ulcer in a Transplant
9/27/16 78
Corneal Ulcer Post Transplant: Patient with RA
9/27/16
14
9/27/16 79
Other complications--continued
• Suture related complications – Stitch infiltrates
• increase topical antibiotics and steroids • watch carefully • often not infected; difficult to tell
– suture erosion • often occurs in vascularized quadrant • remove stitch if possible
9/27/16 80
Astigmatism--sutures out • AK
– inside graft host margin about 1/2 mm – diamond knife set to 100% of measured thickness
of proposed site of cut – arc length 45 degrees (6-cut RK marker)
• 60 degree MAX • keratometer • compression sutures
– can cut in graft host margin at slit lamp with metal blade
9/27/16 81
Contact lens fitting
• RGP lens – difficult fits due to high astigmatism – trial and error
• Kerataconus lens such as Soper or Reverse Profile lenses used for RK patients are useful
– corneal topography helpful • may need keratoconus set or bitoric
posterior curve to fit • Soft lens may induce blood vessels
9/27/16 82
Contact Information