place logo here the value of medication therapy management services
TRANSCRIPT

Place Logo Here
The Value of The Value of Medication Therapy Medication Therapy
Management ServicesManagement Services
Place Logo Here
ORIGINS AND DEVELOPMENT ORIGINS AND DEVELOPMENT
OF MTMSOF MTMS

Place Logo Here
Milestones in the Evolution of the Pharmacist as a
Clinician
1949 – The Elliott Commission recommends that pharmaceutical education move toward a doctor of pharmacy degree.
1973 – APhA endorses the concept of “clinical pharmacy” in practice.
1975 – The Millis Commission recommends more clinical education and courses in social and behavioral sciences to recognize pharmacists’ growing patient care roles.

Place Logo Here
Milestones in the Evolution of the Pharmacist as a
Clinician
1990 – Hepler and Strand propose the concept of ‘Pharmaceutical Care’
“Pharmaceutical care is the responsible provision of drug therapy for the purpose of achieving definite outcomes that improve a patient’s quality of life”
1990 – OBRA ’90 requires pharmacists to perform DUR and to offer to counsel Medicaid patients; most states eventually extend these requirements to all patients.

Place Logo Here
Milestones in the Evolution of the Pharmacist as a
Clinician
1991 – APhA proposes Pharmacy’s mission:
“The mission of Pharmacy is to serve society as the profession responsible for the appropriate use of medications, devices and services to achieve optimal therapeutic outcomes”

Place Logo Here
Milestones in the Evolution of the Pharmacist as a
Clinician
1993 – NCPA proposes the concept of ‘Pharmacist Care’
“Pharmacist Care is a comprehensive approach to pharmacist-directed patient care management through which pharmacists provide an expanded level of patient care that focuses on disease prevention and wellness programs and includes monitoring, evaluating, counseling, intervening and directing medication-related therapies to enhance patient care and improve health outcomes”

Place Logo Here
Milestones in the Evolution of the Pharmacist as a
Clinician
2003 – Medicare Modernization Act (MMA) is passed; creates an outpatient prescription drug benefit for Medicare recipients. The MMA recognizes patients’ need for medication therapy management services (MTMS) and the role of pharmacists as providers of MTMS.

Place Logo Here
…To Medication Therapy Management Services
• The term MTMS became widely accepted after it was
included in the Medicare Modernization Act in 2003
• The foundation of MTMS was built through the
development of pharmaceutical care
• MTMS is not limited to any specific population or payer
group

Place Logo Here
Purpose of Medication Therapy Management
Services (MTMS)
• To optimize therapeutic outcomes
• To decrease the likelihood of adverse events
• To enhance patient understanding and adherence
• To reduce overall healthcare spending
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
Pharmacists’ Evolving Role
From Dispensing Services… …to a clinical
service provider

Place Logo Here
Pharmacy’s Definition of MTMS
• Services provided by a pharmacist that improve
treatment outcomes for individual patients
• A professional service to promote the safe and
effective use of medications
• A way to provide better care for patients– Promotes collaboration among the patient, the
pharmacist, and the patient’s other health care providers .
Bluml BM. Definition of medication therapy management: development of professionwide consensus. J Am Pharm Assoc. 2005;45:566–72

Place Logo Here
CMS MTMS Requirements
• The CMS MTMS Requirements only apply to the Medicare population
• CMS is regularly evaluating this service, and the program definitions will likey evolve over time.
• Currently, CMS requires that all Medicare Part D Plans have an MTMS program which:– Ensures optimum therapeutic outcomes for targeted
beneficiaries through improved medication use – Reduces the risk of adverse events
– Is developed in cooperation with licensed and practicing pharmacists and physicians
www.cms.hhs.gov

Place Logo Here
CMS MTMS Requirements
• Currently, CMS requires that all Medicare Part D Plans have an MTMS program which:– May be furnished by pharmacists or other qualified
providers
– May distinguish between services in ambulatory and institutional settings
– Is coordinated with any care management plan established for a targeted individual under a chronic care improvement program (CCIP)
– Describes the resources and time required to implement the program if using outside personnel and establishes the fees for pharmacists or others
www.cms.hhs.gov

Place Logo Here
Establishment of Billing Codes
• Three ‘pharmacist only’ CPT professional service codes to bill third-party payers for MTM Services delivered face-to-face between a pharmacist and a patient– 99605 is to be used for a first-encounter service (up to
15 minutes) – 99606 is to be used for a follow-up encounter with an
established patient (up to 15 minutes) – 99607 may be used with either 99605 or 99606 to bill
additional 15-minute increments.
• Classified as Category 1 and became eligible for use January 1, 2008.
Beebe M, Dalton JA, Espronceda M, et. al. Current Procedural Terminology 2009. American Medical Association: Chicago, IL.

Place Logo Here
• Medication Therapy Management services (MTMS)
describe face-to-face patient assessment and
intervention as appropriate, by a pharmacist
• MTMS includes the following documented elements:
– review of the pertinent patient history
– medication profile (prescription and non-prescription)
– recommendations for improving health outcomes and treatment compliance.
Beebe M, Dalton JA, Espronceda M, et. al. Current Procedural Terminology 2009. American Medical Association: Chicago, IL.
CPT Code Definition of MTMS

Place Logo Here
ACTIVITIES INCLUDED IN ACTIVITIES INCLUDED IN MTMSMTMS

Place Logo Here
MTMS Activities
• Assess patients’ health status
• Devise medication treatment plan
• Select, modify and administer medications
• Review current medications and identify drug-related problems
• Communicate care to other providers
• Provide patient education
• Refer patients for broader disease management services
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com
Place Logo Here
The Spectrum of Pharmacist-Provided MTMS
• Comprehensive or Targeted Medication Therapy Reviews • Adherence Services
– Based on the number and/or type of medications
• Targeted Medication Intervention Programs – High-alert and/or high-cost medications – Targeted patient population (i.e. geriatrics, pediatrics)
• Disease State Management – Interdisciplinary approach to achieve therapeutic goals – Example disease states: Diabetes, Cholesterol, Asthma
• Health and Wellness Services– Immunizations– Wellness screenings – Smoking cessation – Weight management
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
Components of the MTMS Core Elements Service Model
• Medication Therapy Review (MTR) – a review of all medications including prescription, nonprescription,
herbal products, and other dietary supplements
• Personal Medication Record (PMR)
• Medication-Related Action Plan (MAP) for the patient
• Intervention and/or Referral
• Documentation and Follow-Up
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
Medication Therapy Reviews
• A Medication Therapy Review
(MTR) is provided at routine
intervals by a pharmacist– Annual comprehensive MTR– Additional comprehensive
MTRs as needed
• Targeted MTR at any time to address new or ongoing medication-related problems
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
What Do Patients Get From Care Aligned With the MTMS Core Elements Model?
A complete list of all of their medications:Personal Medication Record(PMR)
A guide for managing theirmedications and relatedconditions:Medication-Related Action Plan(MAP)
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
Value of a Personal Medication Record
“The medication record helps give the doctors a better picture of what’s going on with me.”

Place Logo Here
Value of MTMS
“Having the help of a person who specializes in medications, which
impacts me on a daily basis—putting drugs in my body.”

Place Logo Here
PHARMACISTS ROLE IN THE PHARMACISTS ROLE IN THE
HEALTH CARE TEAMHEALTH CARE TEAM

Place Logo Here
they are integral members of the
health care team!
Pharmacists do not work in
silos….

Place Logo Here
Physicians Value Pharmacists
“Working with the pharmacist has helped me to focus on the things that only I can do as a physician.”

Place Logo Here
Evaluate appropriateness, effectiveness, safety, and compliance with medications
Identify drug therapy problems
Exp
erienced
Decisio
n M
aking
PractitionerM
edic
atio
n E
xper
ien
ce Patient
Therapeutic Relationship
Philosophy of Practice
Social Obligation
Responsibility to identify, resolve, and prevent drug therapy problems
Patient-centered approach
Caring
Today’s wants and needs
Responsibility to participate in information sharing and decision making
ASSESSMENT
CARE PLAN
Resolve drug therapy problems Establish goals of therapy Interventions
FOLLOW-UP
Evaluate progress in meeting goals of therapy
Record actual patient outcomes Reassess new problems
Medication Therapy Management Process

Place Logo Here
Pharmacist/Prescriber Relationship

Place Logo Here
Pharmacist’s Communication
with other Health Providers
• Pharmacists will communicate regularly with patient’s primary care provider, and other health care team members as appropriate
– Describe assessment
– Describe and rationalize recommendations for medication
changes
– Recommendations for follow-up

Place Logo Here
Medication Recommendations
• Pharmacists may make recommendations in several ways:– Directly to the patient
• Over-the-counter changes, general adherence tips, managing side effects
– Through the prescriber• Changes in prescription medications
– Directly to the patient under a collaborative practice agreements
• Allows pharmacists to make adjustments to prescription medications via protocol

Place Logo Here
VALUE OF VALUE OF MTMSMTMS

Place Logo Here APhA. Pharmacists Improving Care and Reducing Costs for
Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
How do we define value?
• Value on investment
– Economic• Overall cost savings or cost
– Clinical• Improvements in health outcomes
– Humanistic• Patient satisfaction, improved quality of life, worker productivity

Place Logo Here
EVIDENCE OF THE VALUE OF EVIDENCE OF THE VALUE OF
MTMSMTMS

Place Logo Here
Studies Illustrating Value of MTMS
• Asheville Project: Diabetes
• Asheville Project: Asthma
• Diabetes Ten City Challenge
• Minnesota Experience Project

Place Logo Here
Asheville Project: Diabetes
• Evaluation of outcomes following community based provision of MTMS to patients with diabetes covered by a self-insured employer group
• Longitudinal study with pre- and post- data
• Participants were provided incentives including waiver of all copays for diabetes medications and supplies
• 5 years of follow-up data
• 187 participants entered the program, with 26 continuing at 5 years
Cranor CW, Bunting BA, Christensen DB. J Am Pharm Assoc. 2003;43:173–84.

Place Logo Here
Asheville Project: Diabetes
• Pharmacists performed the following as part of this study:
– Set and monitored treatment goals
– Glucometer training
– Adherence monitoring
– Basic physical assessment, including foot exam, blood pressure and weight
– Diabetes education
– Referral to other providers as needed
Cranor CW, Bunting BA, Christensen DB. J Am Pharm Assoc. 2003;43:173–84.

Place Logo Here
Clinical Outcomes of MTMSThe Asheville Project - Diabetes
Cranor CW, Bunting BA, Christensen DB. J Am Pharm Assoc. 2003;43:173–84.
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
Asheville Total Health Care Costs1
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000
Baseline 1 2 3 4 5
Follow-up Year
Mean
Co
st
/ P
ati
en
t /
Year
Medical $ Diabetes Rx Other Rx
Cranor CW, Bunting BA, Christensen DB. J Am Pharm Assoc. 2003;43:173-84.
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
Average Annual Diabetic Sick-Leave Usage (City of Asheville)
12.6
6
8.46
5.68 5.81 5.67 6.01
0
2
4
6
8
10
12
14
Basel
ine
Year
1
Year
2
Year
3
Year
4
Year
5
Year
6
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
Key Findings: Asheville Diabetes
• Economic benefit
– Total health care costs for patients decreased
– Prescription costs increased, but medical costs decreased
• Clinical benefit
– Significant improvement seen in A1C and LDL
• Humanistic benefit
– Decreased sick leave; increased worker productivity
Cranor CW, Bunting BA, Christensen DB. J Am Pharm Assoc. 2003;43:173-84.

Place Logo Here
Asheville Project: Asthma
• Evaluation of outcomes following community based provision of MTMS to patients with asthma covered by a self-insured employer group
• Longitudinal study with pre- and post- data
• Participants were provided incentives including waiver of all copays for asthma medications and supplies
• 5 years of follow-up data
• 207 participants entered the programBunting BA, Cranor CW. JAPhA. 2006; 46:133-147.

Place Logo Here
Asheville Project: Asthma
• Pharmacists served as care managers and met with subjects an average of every 3 months
– Reviewed asthma action plans
– Medication assessments of inhaler use
– Assessment of inhaler technique
– Review of symptoms and peak flow meter readings
– Recommendations for treatment changes were sent to physician
Bunting BA, Cranor CW. JAPhA. 2006; 46:133-147.

Place Logo Here
Economic Outcomes of MTMSThe Asheville Project - Asthma
Bunting BA, Cranor CW. JAPhA. 2006; 46:133-147.
0
2
4
6
8
10
12
14
Percentage
BY3 BY2 BY1 Y1 Y2 Y3 Y4 Y5
% Patients withER/ Hospital Events

Place Logo Here
Clinical Outcomes of MTMSThe Asheville Project - Asthma
Improved Asthma control
sustained over 5 years
Bunting BA, Cranor CW. JAPhA. 2006; 46:133-147.
APhA. Pharmacists Improving Care and Reducing Costs for Your Plan Participants. Available at: www.pharmacist.com

Place Logo Here
Key Findings: Asheville Asthma
• Economic benefit
– Decreased percentage of asthma patients requiring emergency and hospital care
• Clinical benefit
– Improved asthma control sustained over 5 years
(as evidenced by FEV1 measurements)
Bunting BA, Cranor CW. JAPhA. 2006; 46:133-147.

Place Logo Here
Diabetes Ten City Challenge
• Employer-funded, collaborative health management program for diabetes using community-based pharmacists in 10 cities across the USA– Pharmacists were located in:
• Independent pharmacies• Chain pharmacies• Ambulatory care clinics
• On-site workplace locations • Participants received waived co-pays for medications.• 573 patients participated
Fera T., Bluml BM, Ellis WM. JAPhA. 2009; 49(3): 383-391.
Place Logo Here
Diabetes Ten City Challenge
• Pharmacists performed the following as part of this study:
– Applied a prescribed process of care based on clinical assessments and progress to goals
– Worked with patients to set individualized self-management goals
– Recommended changes in therapy when appropriate
Fera T., Bluml BM, Ellis WM. JAPhA. 2009; 49(3): 383-391.

Place Logo Here
10 City Challenge Economic Outcomes after Year 1
0123456789
Cost in Millions
MedicalCosts
Medicationcosts
PharmacyServices
Costs
TotalHealth Care
Costs
Baseline
Year 1ProjectedYear 1Actual
Fera T., Bluml BM, Ellis WM. JAPhA. 2009; 49(3): 383-391.
Place Logo Here
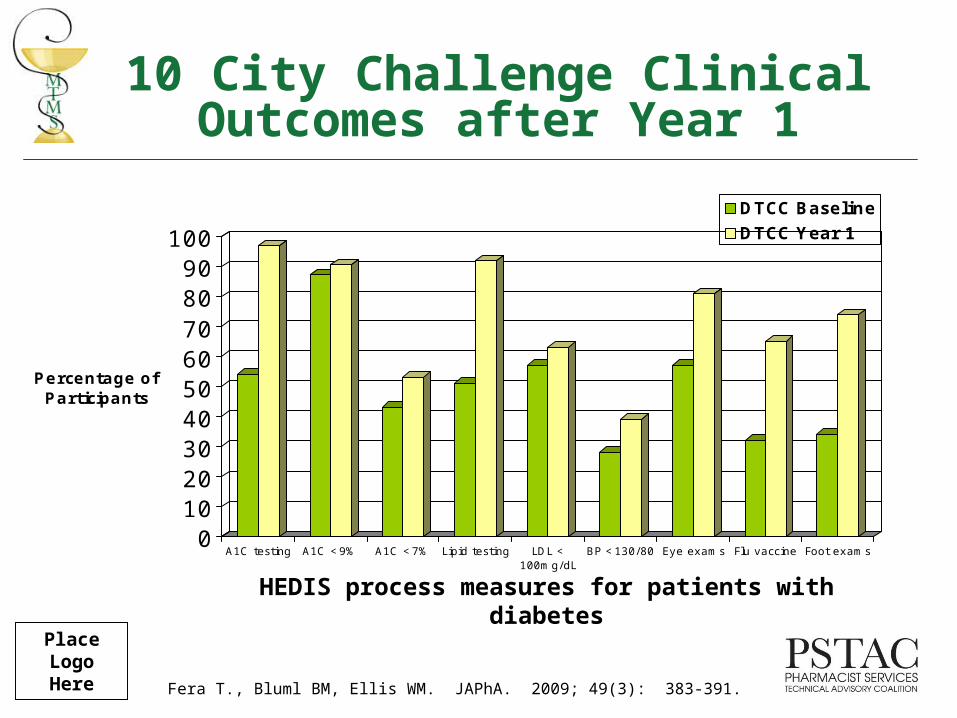
10 City Challenge Clinical Outcomes after Year 1
0102030405060708090
100
Percentage of Participants
A1C testing A1C <9% A1C <7% Lipid testing LDL <100mg/dL
BP <130/80 Eye exams Flu vaccine Foot exams
DTCC Baseline
DTCC Year 1
HEDIS process measures for patients with diabetes
Fera T., Bluml BM, Ellis WM. JAPhA. 2009; 49(3): 383-391.

Place Logo Here
Key Findings: 10 City Challenge
• Economic benefit
– Total health care costs were less than predicted
– Prescription costs increased, but overall health care
costs decreased
• Clinical benefit
– Increased percentage of patients meeting HEDIS process measurement goals for patients with diabetes
Fera T., Bluml BM, Ellis WM. JAPhA. 2009; 49(3): 383-391.
Place Logo Here
Minnesota Experience Project
• Evaluation of MTMS provided at 6 ambulatory care clinics over 1 year
• 285 patients received MTMS
• HEDIS goals for hypertension and dyslipidemia were evaluated
• Study patients were required to have 1 of 12 study conditions
• Return on investment was calculated at 12:1
Isetts, et al., J Am Pharm Assoc. 2008;48(2):203-211

Place Logo Here
Minnesota Experience Project
• Pharmacists in this study:
– Used a consistent and systematic patient care process
– Established goals of therapy in collaboration with patients and primary care providers
– Made recommendations for changes in therapy as appropriate
Isetts, et al., J Am Pharm Assoc. 2008;48(2):203-211

Place Logo Here
Economic Outcomes from the Minnesota Experience
Project
$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
Facilities (- 57.9%)
Professional (- 11.1%)
Prescriptions (+ 19.5%)
Total Cost (- 31.5%)
1 YearbeforeMTM
1 YearafterMTM
Place Logo Here
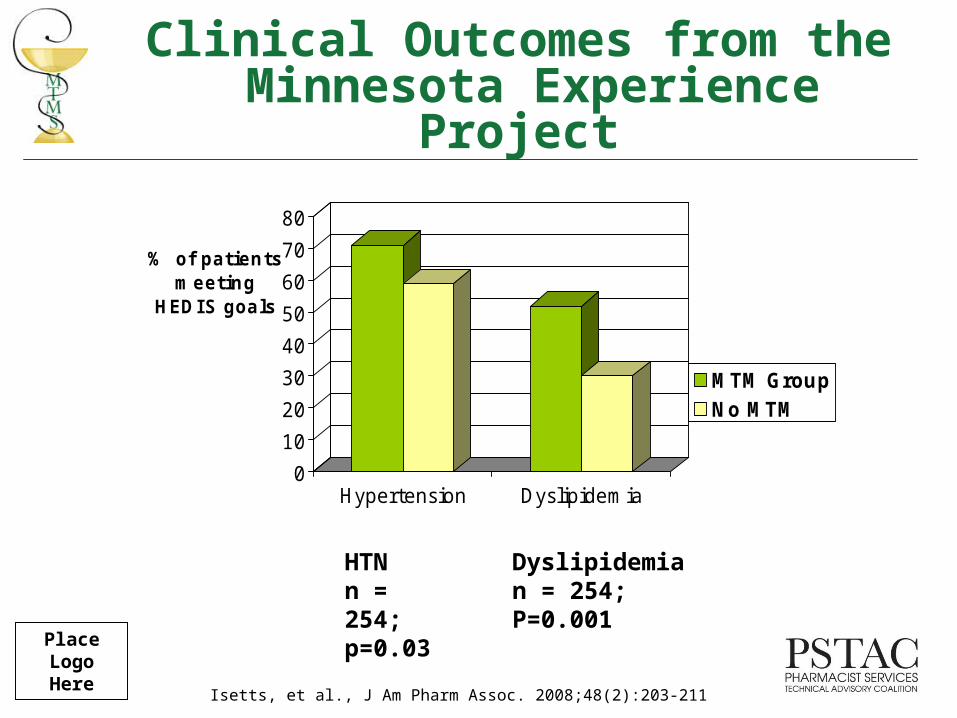
Clinical Outcomes from the Minnesota Experience
Project
HTN n = 254;p=0.03
Dyslipidemia n = 254;P=0.001
Isetts, et al., J Am Pharm Assoc. 2008;48(2):203-211
0
10
20
30
40
50
60
70
80
Hypertension Dyslipidemia
% of patients meeting
HEDIS goals
MTM GroupNo MTM

Place Logo Here
Key Findings: Minnesota Experience
Project• Economic benefit
– A 12:1 return on investment was seen
– Savings was seen in facilities costs
– Per person per year costs decreased from $11,965 to $8,197
• Clinical benefit
– The MTM intervention group had a higher percentage of patients meeting HEDIS goals for hypertension and dyslipidemia

Place Logo Here
Limitations of Current Evidence
• Most of the data comes from self-insured employer groups
• Individual studies are small– Ten City Challenge was the largest with 573 participants
• Much of the evidence is focused on specific disease states

Place Logo Here
Summary of evidence of Value of MTMS
• Economic
– Multiple studies have shown positive results on total health care costs, creating a positive return on investment
• Clinical
– Multiple studies have indicated improved in clinical outcomes, specifically in diabetes, asthma, hypertension and dyslipidemia
• Humanistic
– The Asheville project has demonstrated reduced employee sick days and increased productivity.
Fera T., Bluml BM, Ellis WM. JAPhA. 2009; 49(3): 383-391.Isetts, et al., J Am Pharm Assoc. 2008;48(2):203-211Bunting BA, Cranor CW. JAPhA. 2006; 46:133-147.
Cranor CW, Bunting BA, Christensen DB. J Am Pharm Assoc. 2003;43:173-84.

Place Logo Here
ELEMENTS OF MTMS ELEMENTS OF MTMS
BENEFIT DESIGNBENEFIT DESIGN

Place Logo Here
Elements of MTMS Plan Design
• Eligibility
• Reimbursement structure
• Member engagement strategy– Incentives
Place Logo Here
Eligibility
• Eligibility for a MTMS benefit can be based on:
– Number of medications
– Specific chronic conditions
– Total amount of prescription expenditures

Place Logo Here
Reimbursement Structure
• Recommend utilizing the MTMS CPT billing codes
• May use them as defined as time-based codes, or use a cross-walk relative value scale

Place Logo Here
Example: Minnesota Medicaid
• MHCP will reimburse only for face-to-face encounters and based on the lowest of five patient need levels, according to the following qualifying criteria:– The number of medications the patient is currently
taking;– The number of drug therapy problems the patient has
at present; and– The number of medical conditions for which the
patient is currently being treated.• CPT Codes (Time Based Codes)
Based on adopted Minnesota Medicaid law– 99605– 99606– 99607

Place Logo Here
Example: MN Medicaid Payment Structure
LevelAssessment of
Drug-related needs
Identification of Drug Therapy Problems
Complexity-of-Care Planning & FU
Evaluation
Approx. Face-to-
Face Time
Bill CPT Code
Units
1Problem-focused-at least 1 medication
Problem-focused 0 drug therapy problems
Straightforward 1 medical condition 15 min.
99605 or99606
1 unit
2
Expanded Problem-at least 2 medications
Expanded Problem at least 1 drug therapy problem
Straightforward 1 medical condition
16-30 min.
99605 or99606 and
1 unit
99607 1 unit
3
Detailed-at least 3-5 medications
Detailed at least 2 drug therapy problems
Low complexity at least 2 medical conditions
31-45 min.
99605 or99606 and
1 unit
99607 2 units
4
Expanded Detailed-at least 6-8 medications
Expanded Detailed at least 3 drug therapy problems
Moderate Complexity at least 3 medical conditions
46-60 min.
99605 or 99606 and
1 unit
99607 3 units
5
Comprehensive- >= 9 medications
Comprehensive at least >4 drug therapy problems
High Complexity at least >= 4 medical conditions
60 + min.
99605 or 99606 and
1 unit;
99607 4 units

Place Logo Here
Example: Outcomes Pharmaceutical Health Care
Pharmacist Service CPT Codes
Comprehensive Medication Review 99605 + 99607
Physician Consultation 99606 + 99607
Patient Compliance Consultation 99606 + 99607
Patient Education/Monitoring 99606

Place Logo Here
Member Engagement Strategy
• May offer copay reductions or waivers
– For all medications– For medication associated with a targeted medical condition
(i.e., diabetes)
• Offer reduced copay (or none) for MTMS

Place Logo Here
What’s In It For the Payer?
• MTMS results in decreased overall healthcare costs
– Prescription costs will likely increase, but this is compensated by an overall decrease in costs
• Pharmacists can provide MTMS as a member of the health care team and medical home model
• Increased member satisfaction
• Mechanisms for MTMS claims processing are well established through CPT codes

Place Logo Here
What’s In It For the Patient?
• MTMS provides patients with improved health outcomes from optimizing medication use
– This includes decrease emergency department visits and hospitalizations
• Increased understanding of medications and disease management
• Improved quality of life
Place Logo Here
Summary
• Medications are a standard in the care of chronic diseases
• Pharmacist delivered Medication Therapy Management Services are well documented to decrease health care costs while increasing the quality of health care