place of ost among various treatment options for opioid dependence sifting through the evidence base
TRANSCRIPT

Place of OST among various treatment options for opioid
dependence: Sifting through the evidence-base
Debasish BasuPGIMER, Chandigarh
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Why is it important?
• Lots of misconceptions about opioid substitution therapy for opioid dependence
• Clinical relevance• Public health relevance• Policy relevance
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
The Agenda (a lot to cover!!!)• Long-term Course and Outcome of opioid dependence
and factors influencing it• Models of care and treatment choices, focusing on
abstinence-vs.-harm-reduction approaches• Role of OST as endorsed worldwide• Evidence for effectiveness of OST• What works in OST?• OST: The Caveats • Naltrexone: the poor cousin and a new promise• Potential harms of (improper) OST• Placing OST among treatment options in the Indian
situation Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

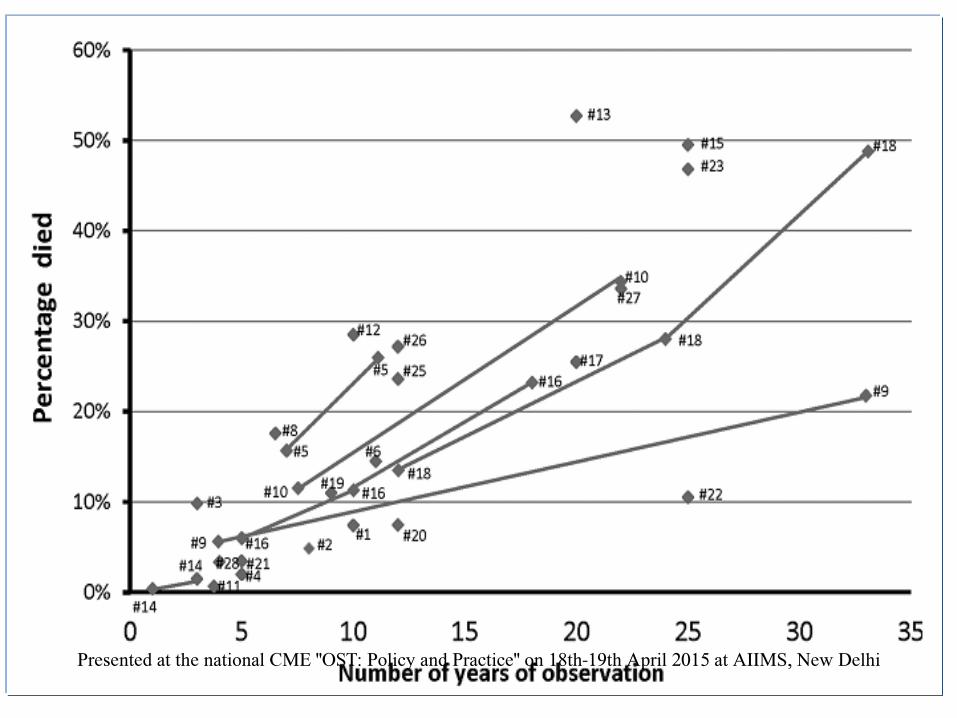
Course and Outcome of Opioid Dependence: SUMMARY
• Opioid dependence mostly is a chronic relapsing
condition, with multiple trajectories, turning points and
outcomes
• Outcome is measured on multiple domains
• Measured on a continuum rather than abstinence and
relapsePresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
“Let a hundred flowers bloom”
• Substance use disorders are multifactorial and biopsychosocial in nature
• Models of care are also diverse in their philosophy, orientation, settings and goals
• Models of care can be completely non-medical (spiritual, self-help, community support) or can be combined with medical models of care
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Models of Care• Within the traditional professional realm,
models can be:
– Primary-care vs. specialist centre based – acute vs. chronic– community vs. residential based– detoxification vs. rehabilitation– pharmacological vs. psychosocial– abstinence vs. harm reduction
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

ARTIFICIAL DICHOTOMIES!!!• Many of the above models of care are not strictly
dichotomous but rather represent polarities on a continuum of care
• Acute detoxification can be followed by chronic relapse prevention-oriented care
• Community care and long-term residential care, with various options in between, are all possible options
• Harm reduction can be the initial step towards eventual abstinence
• Current consensus favors endorsing a chronic care model, more community oriented, focused on rehabilitation/recovery, with a combination of pharmacological and psychosocial modalitiesPresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

BASIC TREATMENT APPROACHES FOR OPIOID DEPENDENCE
• Based on time course:– Short-term (detoxification, ‘cold turkey’)– Long-term
• Based on modality:– Pharmacological (“Medication-assisted treatment”)– Non-pharmacological (Psychosocial, self-help)
• Based on treatment goal:– Abstinence (“Relapse prevention”)– Harm reduction (“Maintenance”/ “Substitution”)Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

MEDICATION-ASSISTED TREATMENT OF OPIOID DEPENDENCE (MATOD)
• Two OPPOSITE Approaches!– Opioid Agonist / Partial Agonist
• Methadone• Buprenorphine• Levo-acetyl alpha methadol (LAAM)• Slow-release morphine• Tincture of opium• Heroin!
– Opioid antagonist• Naltrexone
– Oral– Sustained-release (implant or depot injection)
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Potential goals of treatment
Abstinence-based
Priority on cessation of drug use
Harm reduction
Aims to decrease the adverse health, social and economic consequences of drug use, even if the user can’t or won’t cease all drug use in the short term
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Abstinence-oriented vs. Harm-reduction oriented approaches
• Common goals:– Reduction of (illicit) substance use– Reduction of physical & psychosocial
complications– Enhancement of functioning– Improvement in quality of life
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Abstinence-orientedvs. Harm-reduction oriented approaches
• Basic premise:
–Complete abstinence from ALLsubstance use
– Reduction of physical & psychosocial complications– Enhancement of functioning– Improvement in quality of life
• Achieving the 1st objective others will follow• Risk: if 1st not achieved patient is “out” of the
system! all other objectives (including the 1st!) lostPresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Abstinence-oriented vs. Harm-reduction oriented approaches
• Basic premise:– Retention in treatment network!
– Reduction of (illicit) substance use
–Reduction of physical & psychosocial complications (“harm”)
– Enhancement of functioning– Improvement in quality of life
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Abstinence-oriented vs. Harm-reduction oriented approaches
• Shift of emphasis:– Retain the patient
–Reduce the harms – Enhancement of functioning– Improvement in quality of life
– ………..Continue efforts to reduce substance abuse– …………But not at the cost of losing the patient!
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Major Harm Reduction approaches for opioid-using IDUs
• Opioid substitution therapy • Needle-syringe exchange programs• Reducing sex-related harm, e.g., condom
distribution programs• Anti-retroviral therapy (for HIV+ patients)
…………………………………………• Education & Counseling!
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Opioid Substitution treatment(OST)
• Extensively investigated, used in developed world since late 1960s
• Synonymous Term - Maintenance / replacement
• Prescription of medically safe, long acting agonist
• Eliminates drug hunger and produces cross-tolerance
• Value lies in the opportunity it provides for user to stabilize
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Philosophy of Agonist Substitution• Agonist medications:• Medically safe• Long acting drug, often OD• Known purity/potency• Usually oral/sublingual • Combined with counseling &
psychosocial rehabilitation
Drugs of abuse:
Illicit
Medically unsafe
Short acting drug
Of unknown purity/ potency
Multiple doses needed
I.V. use
Associated criminal activities
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
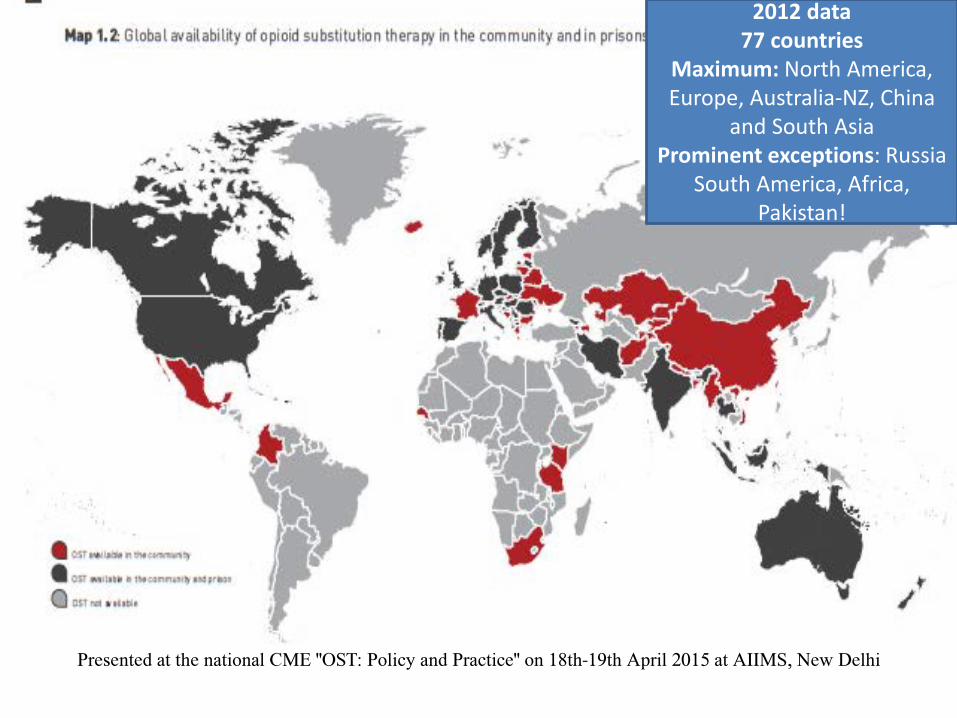
2012 data77 countries
Maximum: North America, Europe, Australia-NZ, China
and South AsiaProminent exceptions: Russia
South America, Africa, Pakistan!
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
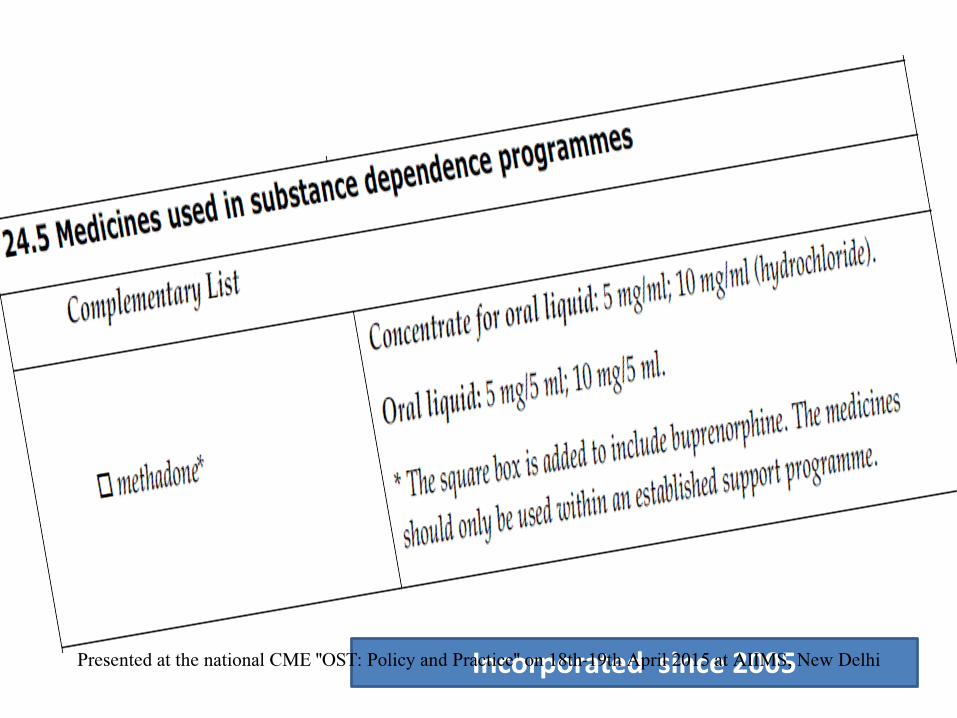
Incorporated since 2005Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
OK, OK, but where is the evidence?
Over 100 randomized controlled studies of opioid maintenance treatment
Many countries – USA, Australia, Netherlands, Switzerland, Italy, UK, Germany, Austria, China, Thailand, Spain and Sweden......Turkey, Hungary, Poland, Malaysia, Singapore..........watch this space..............
Eight Cochrane reviews till 2014 - Included 52 studies and 12,075 participants
Amato et al 2005 – “mega-review” of reviewsPresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

HTA 2007• Reviewed 31 systematic reviews!• …Plus 28 more RCTs since 2001 till 2006• Consistent evidence that both methadone and
buprenorphine are 2-4 times better than no drug/placebo – in retaining patients– In reducing illicit drug use
• Reduced crime to a variable extent• Improved functioning• Reduced mortality Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Methadone Maintenance 50 – 80%
LAAM Maintenance 50 – 80%
Buprenorphine-Naloxone Maintenance 40 - 50%
Oral Naltrexone Maintenance 10 – 30%
Extended-release Naltrexone Maintenance 40 – 50%
“Drug Free” (non-pharmacological) 5 – 30%
Short-term Detoxification (any mode) 5 – 20% (limited data)
COMPARE: 2-year Treatment Retention with different regimes
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

• 33 studies• >10,000 participants• Consistent evidence for reduction in drug-
related risk behaviours for HIV infection• Less consistent evidence for reduction in sex-
related risk behaviours
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

• 8-country (Asia, Europe, Australia)
• Mostly LAMIC countries• Prospective cohort
study• 726 participants• 6-month outcomes
• ~70% retention across all sites
• Significant reduction in:– Illicit drug use– Risk behaviors– Crime rate
• Significant increase in:– Physical & mental health– General well-being
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

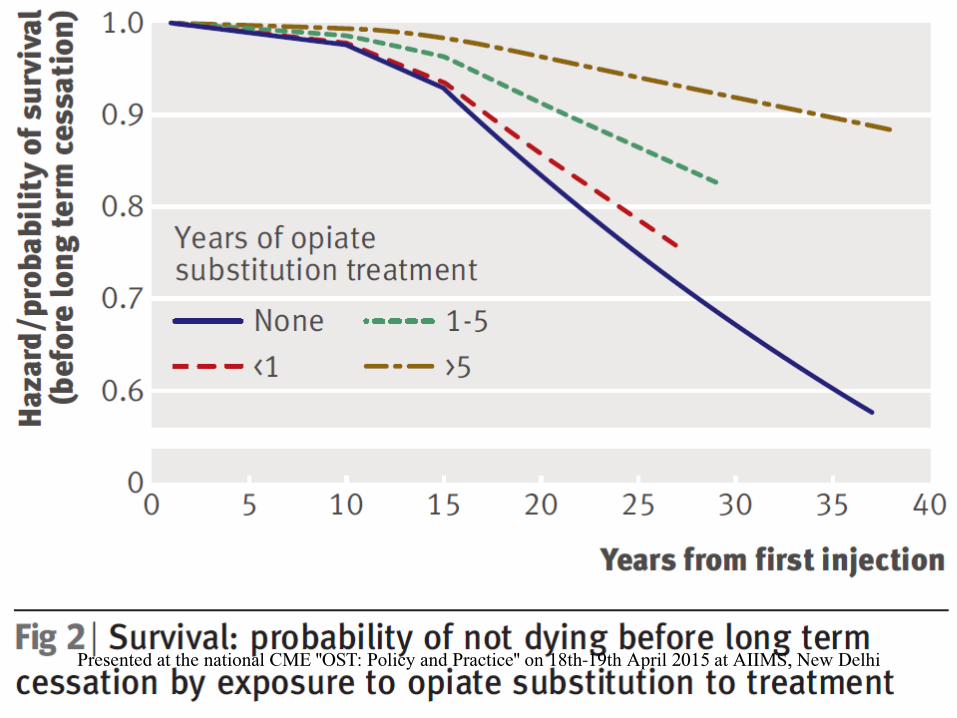
What about mortality?
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Summing up…….evidence base for OST• Retention in treatment +++
• Reduction in illicit opioid use +++
• Reduction in mortality ++
• Reduction in rate of HIV and HCV ++
• Improved employment, health, & social function +
• Improved Quality of Life +
• Reduction in crime + / ±
• Reduction in risk behaviour + (injection); ± (sex)
• Reduction in other drug use - (no effect) Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

WHAT WORKS IN OST?
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

WHAT WORKS IN OST?
THE 4 DIMENSIONS OF EFFECTIVE OST• Dose• Duration• Direction• Delivery
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

DOSE
• Most cases of failed (or diverted) OST are due to under dosing
• Many cases of failed (or diverted) OST is due to under dosing!
• The correct dose should be able to:– Effectively suppress craving and withdrawal– Effectively ameliorate any rewarding effect of illicit
opioid– Steer clear of producing intoxication/sedation/
’kick’Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

DURATION• There is nothing like “Time-Limited” OST!• Most studies show that at least 1 year of continuous
OST is needed often much longer (1-5 years) occasionally, indefinite
• The termination of OST should ALWAYS be by mutual agreement between patient, provider and family
• Duration should be adequate to help the patient ‘stabilize’ in life (w.r.t. work, family, hobbies, lifestyle, crime-free, spiritual affiliation, and a ‘non-addict identity’ in society)
• However, mindless and directionless ‘parking’ on OST does not help eitherPresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
DIRECTION
• “A directionless OST programme is like a rudderless ship”
• Needs good clinical leadership, governance and supervision
• Focus on recovery (in functional terms), rather than only on either abstinence or non-illicit drug use
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

DELIVERY
• OST programs must have an effective model of delivery (rather than being a ‘methadone swallowing’ or drug dispensing window)
• Organizational issues are vitally important • Helpful staff attitude and therapeutic alliance• Counseling and psychosocial support is
mandatory • Accountability, monitoring, and evaluation of
program delivery is vitalPresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

OST: THE CAVEATS
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

3 studies;870 patients
2 used BPN, 1 baclofen
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Authors’ Conclusions
• At present, there is no sufficient evidence for effectiveness of any kind of maintenance treatment for opium dependence.
• Opium has considerable pharmacologic differences with morphine and heroin. Opium is less harmful and its use by injection is rare. Opium users have a different socio-economic profile compared with heroin users and show a lesser degree of unemployment, homelessness and criminal behaviour.
• Therefore, the already available evidence for effectiveness of various pharmacologic maintenance approaches in treatment and harm reduction of heroin dependence might not be exactly applicable for the dependence on less harmful opioids, like opium.”Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Authors’ Conclusions
• “However, it is up to clinicians to assess the individual patients for severity of opium dependence and resultant problems, previous attempts at treatment and the possible balance of harms and benefits from pharmacologic maintenance treatments,
• discuss it with their patients and their families
• and make appropriate decisions based on their clinical judgment.”
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

11 studies;2678 participants
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Authors’ Conclusions
• “Overall, the findings suggest that such interventions have an impact on reducing drug use and criminal activity to a variable extent.
• We found no significant differences between any of the drug comparisons (methadone vs. buprenorphine, diamorphine and naltrexone) on any of the outcome measures.
• Aside from any practical implications relating to administration or the cost of the drug this suggests that one drug does not perform better than another.”
• Caution: small studies, risk of biasPresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
MEDICATION-ASSISTED TREATMENT OF OPIOID DEPENDENCE (MATOD)
• Two OPPOSITE Approaches!– Opioid Agonist / Partial Agonist
• Methadone• Buprenorphine• Levo-acetyl alpha methadol (LAAM)• Slow-release morphine• Tincture of opium• Heroin!
– Opioid antagonist• Naltrexone
– Oral– Sustained-release (implant or depot injection)
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

13 studies;1198 participants
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Main Results• “Comparing naltrexone versus placebo or no pharmacological
treatments, no statistically significant difference were noted for all the primary outcomes considered.
• The only outcome statistically significant in favour of naltrexone is re-incarceration, RR 0.47 (95%CI 0.26-0.84).
• Considering only studies were patients were forced to adherence, a statistical significant difference in favour of naltrexone was found for retention and abstinence, RR 2.93 (95%CI 1.66-5.18).
• The percentage of people retained in treatment in the included studies is however low (28%).”
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Authors’ conclusions
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
3.5 times higher mortality than in methadone maintained patientsPrimarily because of opioid overdose following naltrexone
discontinuationPresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

• “Due to the lack of alternatives to naltrexone and stronger family control of compliance (adherence), naltrexone is more effective for relapse prevention and abstinence stabilization in Russia than in Western countries.
• Long-acting, sustained-release formulations (injectable and implantable) seem particularly effective compared with oral formulations.”Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
2008
Only one RCT includedNo definitive conclusions
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

2012
“While naltrexone implant treatment may show some efficacy as part of an integrated program, more research is needed.”
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
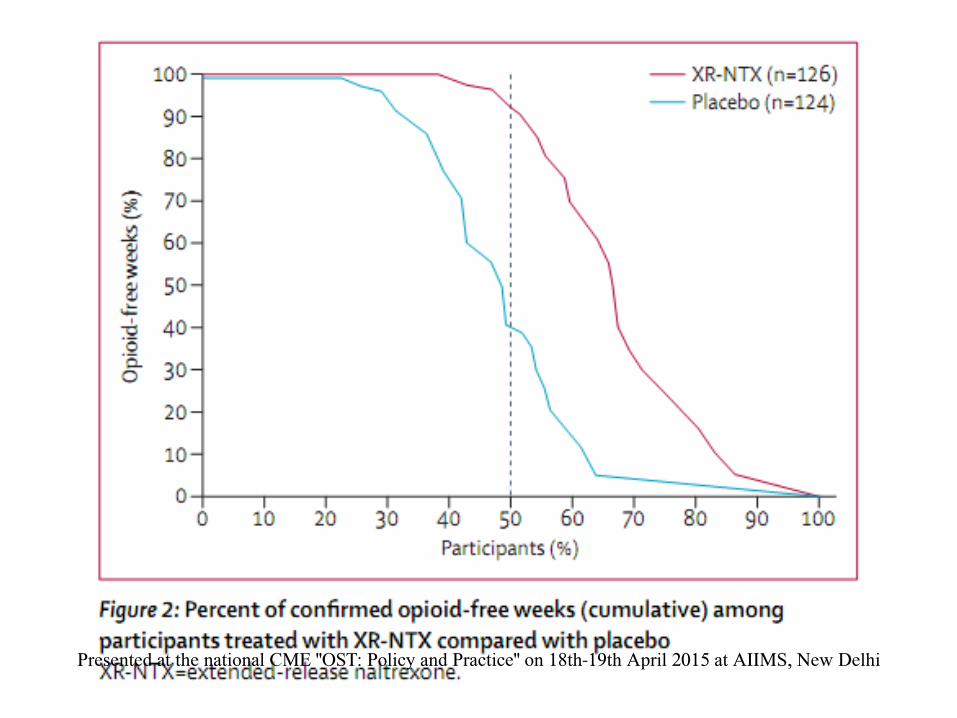
• “A once-monthly supervised pharmacological treatment with proven efficacy that is free of physical dependence and is not subject to illegal diversion might aid community and cultural acceptance of opioid dependence pharmacotherapy and provide a useful treatment option for many patients.”
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

OST: THE CAVEATS
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

OST……A DOUBLE-EDGED SWORD!
• Opioid agonists like methadone, buprenorphine and tramadol are themselves opioids, with all the psychoactive and addictive properties of opioids
• When used properly, it can save and re-build lives
• When used improperly, it can cause damage just like any other opioids
• Hence the whole issue rests upon a “proper”, “balanced” or “rational” use of OST
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

POTENTIAL HARMS OF OST
• Creating – and maintaining – an iatrogenic (= caused by the treatment itself) physiological dependence
• Fostering addiction by overuse of the opioid agonist drugs
• Endangering the lives of people with combined overdose of buprenorphine and other nervous system depressants such as alcohol or benzodiazepines
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

POTENTIAL HARMS OF OST• Generating a parallel market of these potentially
addictive drugs by diversion of legally obtained buprenorphine (through prescription of doctors) for abuse by self or others, by: – Asking for a much higher dose of buprenorphine than
actually needed or for a much longer period– Getting prescriptions written from multiple doctors– ‘Faking’ opioid addiction– Even ‘proxy’ patients (‘uncle’ getting prescriptions for his
‘opioid addict nephew’), etc. – The system has become such that the prescribing doctor
sells the medicine at a higher price (2-3 times higher) and then these are further sold off in the “market” at a further much higher price
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

POTENTIAL HARMS OF OST
• Patients who are in genuine need of long-term opioid maintenance treatment may be left out because of the huge siphoning off of buprenorphine in the parallel market
• Thus, finally, bringing the whole philosophy and practice of OST into disrepute (‘giving OST a bad name’)!
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

FranceFinland
GermanyItaly
PortugalAustria
DenmarkSweden
SwitzerlandUK
AustraliaMalaysia
USAIndia?
Range of diversion: 6% - 67%!Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

CONCERN IN MALAYSIA!
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

• In 2006-07, Malaysian Govt. banned BUP and switched over to BNX only.
• Following this, injection of S/L BNX actually increased in 44%!
• Many felt the unpleasant sensations of naloxone, but still continued.
• In some cases, injection sharing and benzodiazepines abuse also increased.
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

….And over to AUSTRALIA
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

• Most systematic data • Most diversion of BPN, followed by BNX and
methadone• Among OST clients, the reported rate of
injection of BPN > BNX = methadone• The street price of BNX increased from 2007
to 2008, and in 2008 was equivalent to that for BPN
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Latest from SwedenPresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
• Structured interviews were conducted with 411 patients from eleven OST programs.
• 24% reported diversion in past month• 67% reported diversion lifetime after OST• Peer interviewers detected more (37%) last-
month diversion than researcher interviewers (17%)!
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

…What about India?
• Study: Post-marketing Surveillance of Buprenorphine & Naloxone Combination for Treatment of Opioid Dependence
• Ray R et al., AIIMS, Sept. 2009• Total no. of patients: 158
– Heroin Dependent: 87.2%– Opium Dependent: 5.2%– Other opioid: 7.6%
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Qualitative Data
• Abuse• Use of prescription buprenorphine (as injectable ) by
dissolving• Self report of use in more than prescribed dose
– 210 observations (18.6%) out of a total of 1132– 1/4th reported of seeing others injecting – Mixing with 5 -10 ml of injection Avil– Pleasurable effect immediately after the injection– Less pleasurable than injection of heroin or pure
BuprenorphinePresented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Despite these blips….
The benefits of OST clearly far outweigh the risks associated it,
…..if the programmes are conducted well
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

• “The evidence strongly supports the use of agonist therapies to reduce opioid use and to retain patients in treatment……
• The evidence for antagonist therapies is weak.
• Oral naltrexone demonstrates poor adherence and increased mortality rates.
• Early evidence looks more favorable for extended-release naltrexone, which has the advantages that it is not subject to misuse or diversion and that it does not present a risk of overdose on its own.”
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Specific issues in the Indian situation• More prevalent use of lower-potency opioids and in lower
doses (except pure heroin – chitta) than in the West• Much lower doses needed for effective OST• Often patient and family focus on abstinence Strong role
for patient-family-physician collaboration for decision making regarding particular type of treatment need to listen to patient and family preference
• Family supervision and contingency patterns usually stronger than in the West need to be effectively utilized
• There are far too less number of qualified and trained personnel, and far too less number of accredited systems to run effective OST programme in India needs to improve
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Specific issues in the Indian situation• Monitoring, accountability, structured support programme
and evaluation often slack or deficient needs to improve• Capacity to enroll patients for OST in structured programmes
is much lower needs to improve• Clinical practice guidelines need to be followed• Innovations are needed in formulation and delivery
programmes keeping the Indian context in mind• The legal and policy environment is currently too strict
needs re-look to achieve a correct balance between efficacy and accessibility on one hand, and safety and accountability on the other
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi
Specific issues in the Indian situation
• With these caveats, OST has a definite and very important role to play in the treatment scenario for opioid dependence in India
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi

• Those who are looking for “a miracle cure” for addictions will never find it
• …….Those who are not, miracle might find them some day…….
Presented at the national CME "OST: Policy and Practice" on 18th-19th April 2015 at AIIMS, New Delhi