planning for the implementation of new diagnostic tests - · pdf fileplanning for the...
TRANSCRIPT

1 |
Workshop on the development of National Strategic Plans for TB Control Divonne, France, February 18th 2014
Planning for the implementation of new
diagnostic tests
Dr Christopher Gilpin
Laboratories, Diagnostics & Drug Resistance
WHO Global TB Programme, Geneva
GLOBAL TB PROGRAMME
2 |
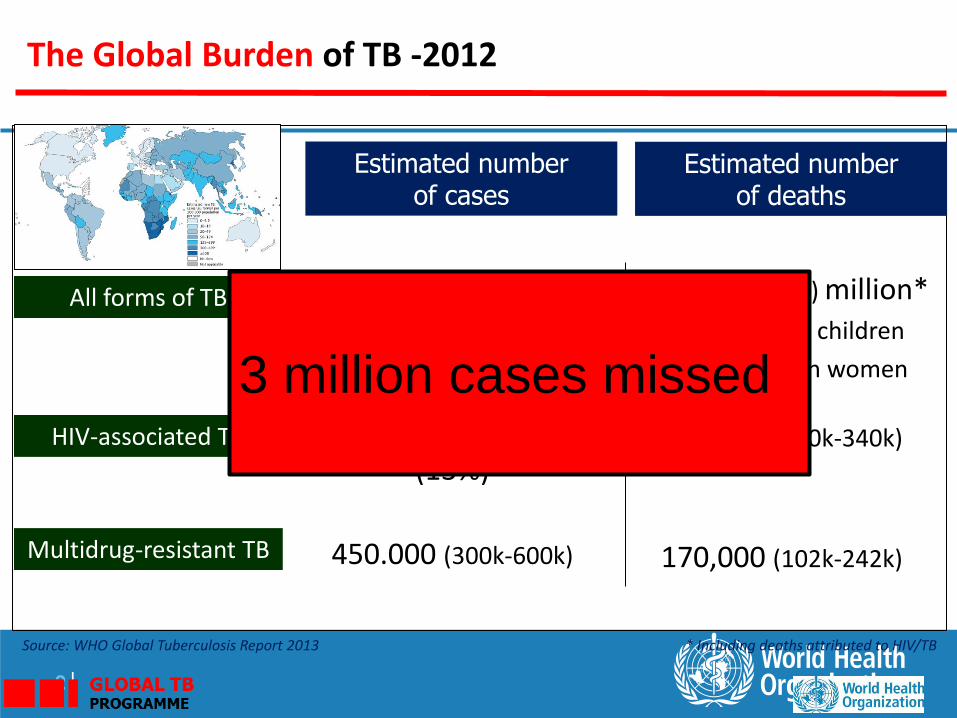
Estimated number of cases
Estimated number of deaths
1.3 (1.0-1.6) million* • 74.000 in children
• 410.000 in women
8.6 (8.3-9.0) million • 0.5 m in children
• 2.9 m in women
450.000 (300k-600k)
All forms of TB
Multidrug-resistant TB
HIV-associated TB 1.1 (1.0-1.2) million (13%)
320,000 (300k-340k)
Source: WHO Global Tuberculosis Report 2013 * Including deaths attributed to HIV/TB
The Global Burden of TB -2012
170,000 (102k-242k)
3 million cases missed
Outline
• WHO requirements for evaluation of new TB diagnostics
• Diagnostic pipeline
• Levels of laboratory services
• Diagnostic tools – what is necessary?
• Forecasting and quantification based on country specific edpidemiology
• Maintenance
• Technical assistance

Phase 1
Research and Development
Phase 2 Evaluation and Demonstration
Phase 3
WHO evidence assessment
GRADE
Phase 4 Phased uptake and
collection of evidence for
scale-up
Phase 5 Scale-up and policy refinement
Evidence required for WHO review of diagnostics

Pipeline for new TB diagnostics

PROGRESS AT A GLANCE – 2013 Global Report
Molecular Detection MTB and drug resistance
Alere Q, Alere, USA B-SMART, LabCorp, USA Gendrive MTB/RIF ID, Epistem, UK LATE-PCR, Brandeis University, USA GeneXpert XDR cartridge, Cepheid, USA TruArray MDR-TB, Akkoni, USA INFINITIMTB Assay, AutoGenomics, USA
Nonmolecular technologies TB Rapid Screen, Global BioDiagnostics, USA TBDx, Signature Mapping Medical Sciences, USA
Culture-based technologies BNP Middlebrook, NanoLogix, USA MDR-XDR TB Color Test, FIND, Switzerland /
Imperial College, UK TREK Sensititre MYCOTB MIC plate, Trek
Diagnostic Systems/ Thermo Fisher Scientific, USA
Molecular Detection MTB and drug resistance
iCubate System, iCubate, USA TB drug resistance array, Capital Bio, China NATeasy TB Diagnostic kit, Ustar
Biotechnologies, China Truelab/Truenat MTB, Molbio/bigtec
Diagnostics, India
Molecular Detection MTB +/- drug resistance
TB LAMP, Eiken, Japan Genotype MTBDRsl, Hain Lifescience,
Germany
Volatile Organic Compounds BreathLink, Menssana Research, USA Prototype breathanalyzer device, Next
Dimensions Technology, USA
Nonmolecular technologies Alere Determine TB-LAM, Alere,
USA
Molecular Detection of MTB and drug resistance
Xpert MTB/RIF (pulmonary extrapulmonary and paediatric samples)
Lineprobe assays for the detection of MTB and rifampicin resistance conferring mutations in AFB smear positive sputum or MTB cultures Microscopy
Light and LED Microscopy Same-day -diagnosis
Culture-based technologies Commercial liquid culture systems and rapid
speciation Non-commercial culture and DST (MODS,
NRA, CRI)
Commercial serodiagnostics (ALL MANUFACTURERS)
Interferon-gamma release assays for the detection of active TB (ALL SETTINGS)

Technologies endorsed by WHO • MTB and drug resistance
Xpert MTB/RIF (pulmonary extrapulmonary and
paediatric samples)
Lineprobe assays for the detection of MTB and
rifampicin resistance conferring mutations in AFB smear
positive sputum or MTB cultures
• Microscopy
Light and LED Microscopy
Same-day -diagnosis
• Culture-based technologies
Commercial liquid culture systems and rapid speciation
Non-commercial culture and DST (MODS, NRA, CRI)

WHO recommended diagnostics for use at different levels of laboratory sophistication
*Available at: http://www.who.int/tb/dots/laboratory/policy/en
Biosafety Levels for
TB Laboratories
High TB risk precautions
•Culture, DST, LPA (cultures)
Moderate TB risk precautions
• liquifying (processing) samples
Low TB risk precautions
•Microscopy, Xpert

High TB Risk Precautions
TB containment laboratory
• Double door airlock
• Separate air inlet
• Venting of BSC via thimble
• Aerosol containment
• Negative pressure monitoring
• Uni-directional airflow
• PPE
• Autoclave for waste disposal
• Necessary for performing culture and DST
Why perform culture?
• Culture in Liquid media – up to six weeks – Reference method
• Culture on solid media – up to eight weeks
• Given the diagnostic delay – culture is NOT a good diagnostic tool
• Essential for performing DST to second-line drugs
• Necessary for monitoring patient response to treatment

12
1. Liquefaction 2. Sample decanted 3. Decontamination NaOH 4. Vortex 5. Phosphate Buffer
Complexity of performing sputum culture and line probe assays
6. Centrifugation 7. Decant 8. Re-suspend 9. Inoculation

Why perform LPA?
• LPA can be used to detect rifampicin and isoniazid conferring mutations in
– AFB smear positive specimens
– Positive TB cultures
• Results can be available in 24 hrs
• Secondline LPA NOT recommended
• Needs sophisticated laboratory
• Needs good referral mechanisms
• Suitable for high throughput testing at
Central or Regional laboratory level

Additional infrastructure for LPA
1. Laboratory infrastructure to address biosafety and contamination control
1. Containment laboratory for DNA extraction
2. At least two additional rooms needed for DNA pre-amplification and post-amplification processes
2. Appropriately well train staff supervised by experience technologists in molecular biology
3. Multiple pieces of equipment
4. Stringent laboratory protocols needed
– SOPs, Internal QC, External QA,
rpoB
katG
CC
AC
TU
B
rpoB
rpoB
rpoB
rpoB
rpoB
rpoB
rpoB
rpoB
rpoB
rpoB
rpoB
rpoB
rpoB
WT1
WT2
WT3
WT4
WT5
WT6
WT7
WT8
MU
T1
MU
T2A
MU
T2B
MU
T3
katG
katG
katG
katG
WT
MU
T1
MU
T2
inh
Ain
hA
in
hA
in
hA
in
hA
in
hA
in
hA
WT
1W
T2
MU
T1
MU
T2
MU
T3A
MU
T3B
inhA
TU
B
katG
WT
katG
MU
T
rpoB
MU
T
inh
A W
T
inh
A M
UT
++ + +- --+
+
--+ -+
+- +- - +++
--
+- - - +-
- +- +
RMP
++ +
+++
++++
se
nsit
ive
resis
tan
t
INH
se
nsit
ive
resis
tan
t#
1
2
3
4
5
+

Why perform Xpert MTB/RIF
1. Laboratory infrastructure similar to that for microscopy is required
2. Can be de-centralised for testing at lower levels of the laboratory network
3. Suitable for the diagnosis of TB and rifampicin resistance in AFB smear-negative and smear-positive individuals
4. New WHO policy recommendations issued for use in adults children and extrapulmonary TB
Smear neg.
Co
nd
ition
al recom
men
datio
n
All individuals
presumed to have TB
Initial TB
diagnostic test
Smear
microscopy
Xpert MTB/RIF A.
B.
C.
Strong recommendation
All individuals at
risk of MDR-TB (TB
confirmed and TB
suspected)
Xpert MTB/RIF
Xpert MTB/RIF
Strong recommendation
HIV (+) individuals
(or HIV unknown in
high HIV settings)
suspected of
having TB
Conditional recommendation
Adults presumed to
have TB but not at
risk of MDR-TB or
HIV associated TB
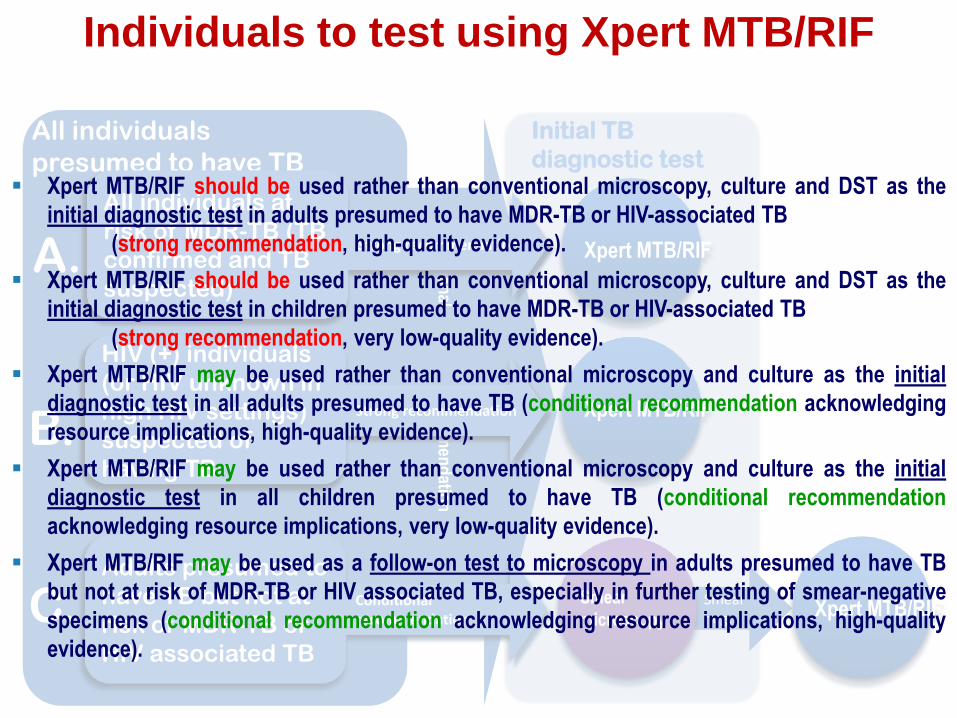
Individuals to test using Xpert MTB/RIF
Xpert MTB/RIF should be used rather than conventional microscopy, culture and DST as the
initial diagnostic test in adults presumed to have MDR-TB or HIV-associated TB
(strong recommendation, high-quality evidence).
Xpert MTB/RIF should be used rather than conventional microscopy, culture and DST as the
initial diagnostic test in children presumed to have MDR-TB or HIV-associated TB
(strong recommendation, very low-quality evidence).
Xpert MTB/RIF may be used rather than conventional microscopy and culture as the initial
diagnostic test in all adults presumed to have TB (conditional recommendation acknowledging
resource implications, high-quality evidence).
Xpert MTB/RIF may be used rather than conventional microscopy and culture as the initial
diagnostic test in all children presumed to have TB (conditional recommendation
acknowledging resource implications, very low-quality evidence).
Xpert MTB/RIF may be used as a follow-on test to microscopy in adults presumed to have TB
but not at risk of MDR-TB or HIV associated TB, especially in further testing of smear-negative
specimens (conditional recommendation acknowledging resource implications, high-quality
evidence).

Xpert
MTB/RIF
assay
TB not
detected
TB
detected;
Rif
sensitive
TB
detected;
Rif
sensitive
WHO recommended
regimen for MDR-TB
with INH;
Registration as RR-TB
• WHO recommended
first-line treatment;
• Registration as
bacteriologically
confirmed TB
If TB still
suspected
Further investigation (CXR,
repeat Xpert MTB/RIF,
culture, etc..)
DST to at least RIF; INH;
Quinolones; SL injectable
TB
detected;
Rif
resistant
Repeat
Xpert
MTB/RIF
In groups with low
risk of MDR-TB
TB
detected;
Rif
resistant
Modify treatment based on
the DST results;
Update registration
WHO recommended
regimen for MDR-TB with
INH;
Registration as RR-TB
DST to at least INH;
Quinolones; SL injectable
In groups with high
risk of MDR-TB
Modify treatment
based on the DST
results;
Update registration
In case of discordance
on Rif result refer sample
for sequencing
Interpretation of test results

National strategy and objectives
Planning for infrastructure improvement
Planning for procurement of goods (shelf-life)
Quantifying and forecasting needs
Developing a supply chain (cold) for TB laboratories
Which diagnostics will be used?
At which level - peripheral, district, regional, central?
Which diagnostic algorithm will be
implemented?
What infrastructure needs to be established or
upgraded?
How many labs?
At which level?
Is a specimen transport and referral
system adapted to this new plan?
Procurement planning is directly linked to the
National TB Plan

WHO
TB Planning and budgeting tool
Ready-made framework for planning/budgeting for each component of TB control
Menu driven system
Summary tables and figures automatically produced
Choosing country via menu system selects correct set of epidemiology/ demographic/financial historical data, projections and default values
Guidance available within tool
Application options to enhance user-friendliness

Example: Pakistan
# MDR patients (projections)

What diagnostics are needed for
previously treated patients?
• Need estimates of the
number of previously
treated persons based on
case notifications.
• Need to estimate proportion
of rifampicin resistance
e.g Pakistan
• 14,000 previously treated
persons
• 30% Rifampicin resistance
among previously treated
• 3% Rif resistance among
new cases
14,000 persons require a rapid DST – Xpert MTB/RIF or LPA 4,200 persons (30% of 14,000)(MDR-TB patients) will require culture and DST for secondline drugs Each person will require additional cultures for monitoring response to therapy – up to 12 cultures per person or 50,400 cultures Need many more Xpert tests to detect 3% RIF resistance among new cases – aim for 20% by 2015
What diagnostics are needed for
previously treated patients?
• 14,000 persons require a rapid DST – Xpert MTB/RIF or LPA
• The structure of the laboratory network and referral
mechanism will determine which tests to use where.
• If network is well structured testing can be de-centralised and
test previously treated persons using Xpert
• If only the central level is strong a larger proportion of the
tests could be referred to the central level for testing by
LPA(where capacity already exists)
• A combination of specimen referral for LPA and de-
centralized Xpert testing can be used
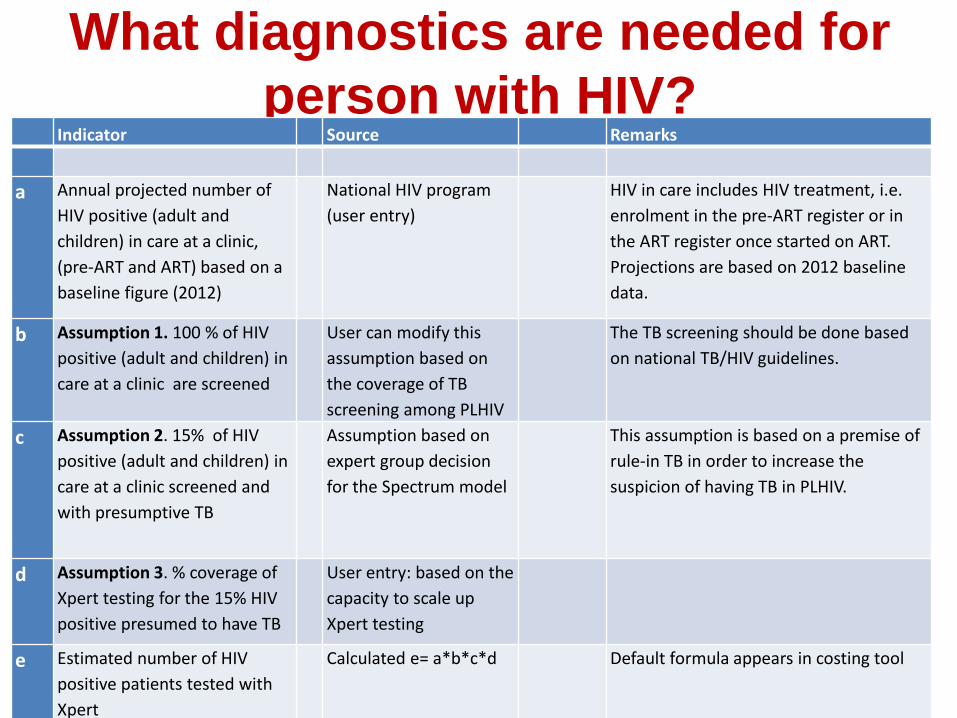
What diagnostics are needed for
person with HIV? Indicator Source Remarks
a Annual projected number of
HIV positive (adult and
children) in care at a clinic,
(pre-ART and ART) based on a
baseline figure (2012)
National HIV program
(user entry)
HIV in care includes HIV treatment, i.e.
enrolment in the pre-ART register or in
the ART register once started on ART.
Projections are based on 2012 baseline
data.
b Assumption 1. 100 % of HIV
positive (adult and children) in
care at a clinic are screened
User can modify this
assumption based on
the coverage of TB
screening among PLHIV
The TB screening should be done based
on national TB/HIV guidelines.
c Assumption 2. 15% of HIV
positive (adult and children) in
care at a clinic screened and
with presumptive TB
Assumption based on
expert group decision
for the Spectrum model
This assumption is based on a premise of
rule-in TB in order to increase the
suspicion of having TB in PLHIV.
d Assumption 3. % coverage of
Xpert testing for the 15% HIV
positive presumed to have TB
User entry: based on the
capacity to scale up
Xpert testing
e Estimated number of HIV
positive patients tested with
Xpert
Calculated e= a*b*c*d Default formula appears in costing tool

What diagnostics are needed for
person with HIV?
• Annual projected of the number of HIV positive persons in care
• Assume: 100% screening
• Assume: 15% with presumptive
• Consider % coverage of Xpert
• e.g Africa context
• 100,000 PLHIV in care
• Need to test 20-30% have symptoms of TB
Up to 30,000 persons will require a rapid diagnostic test – Xpert MTB/RIF (depending on Xpert coverage) Assuming 3% MDR-TB among new cases of TB in PLHIV Up to 900 persons (MDR-TB patients) will require culture and DST for secondline drugs Each person will require additional cultures for monitoring response to therapy – up to 12 cultures per person or 10,800 cultures
Planning for facility maintenance
• Annual certification of BSC – Costs vary depending on setting
• Centrifuge maintenance
• GeneXpert module calibration
• Autoclave
• Monitoring integrity of ducted exhaust
• Building maintenance – Need to consider approx. 10% of facility cost needed for
annual maintenance

Technical Assistance
• Collaboration agreements
• Quality assurance
• Appropriate biosafety
• Diagnostic algorithms
• Functional networks
• Rational planning with laboratory experts

Acknowledgements Laboratory, Diagnostics and Drug Resistance unit in the WHO Global TB Programme: Karin Weyer, Fuad Mirzayev, Wayne van Gemert, Jean Iragena, Fraser Wares, Ernesto Jaramillo, Dennis Falzon, Vineet Bhatia, Henriikka Huttunen, Lynne Harrop, Diego Zallocco

Item Cost Comment
A
Equipment
GeneXpert 4 module with
laptop (Ex-Works price) $17,500.00 >60% price reduction compared to EU/US
B Shipment $1,000.00 Depends on destination
C UPS $1,000.00 Local purchase, price depends on the market
and back up capacity of UPS
D Printer $200.00 Local purchase, price depends on the market,
optional
E Maintenance Annual calibration costs $1,800.00 Highest price if done in Cepheid Toulouse,
when web-based drops to 450USD
F
Consumables
Cost per cartridge $9.98 85% price reduction compared to EU
G Number of working days per
year 250 Number can vary depending on local context
H Average number of tests per
instrument /day 12
Number can vary depending on working
hours
I Number of tests/1 year/ full
load 1 instrument 3000 G*H
J
Losses due to
error/incorrect use (high
estimate 10%)
300 10% of I
K HR costs Technician annual salary $5,000.00 Country-specific
L Training and TA $5,000.00 Depends on the needs
M Installation costs $19,700.00 A+B+C+D
N
Running costs
(annual, 1
instrument)
$34,734.00 E+F*(I+J)
O GRAND TOTAL $64,434.00 N+M+L+K
Xpert MTB/RIF – What is needed?