platelet and plasma transfusion policy. in blood transfusion guideline..pdf
DESCRIPTION
Platelet and plasma transfusion policy. In Blood transfusion guidelineTRANSCRIPT

Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.
Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.

Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.

Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.
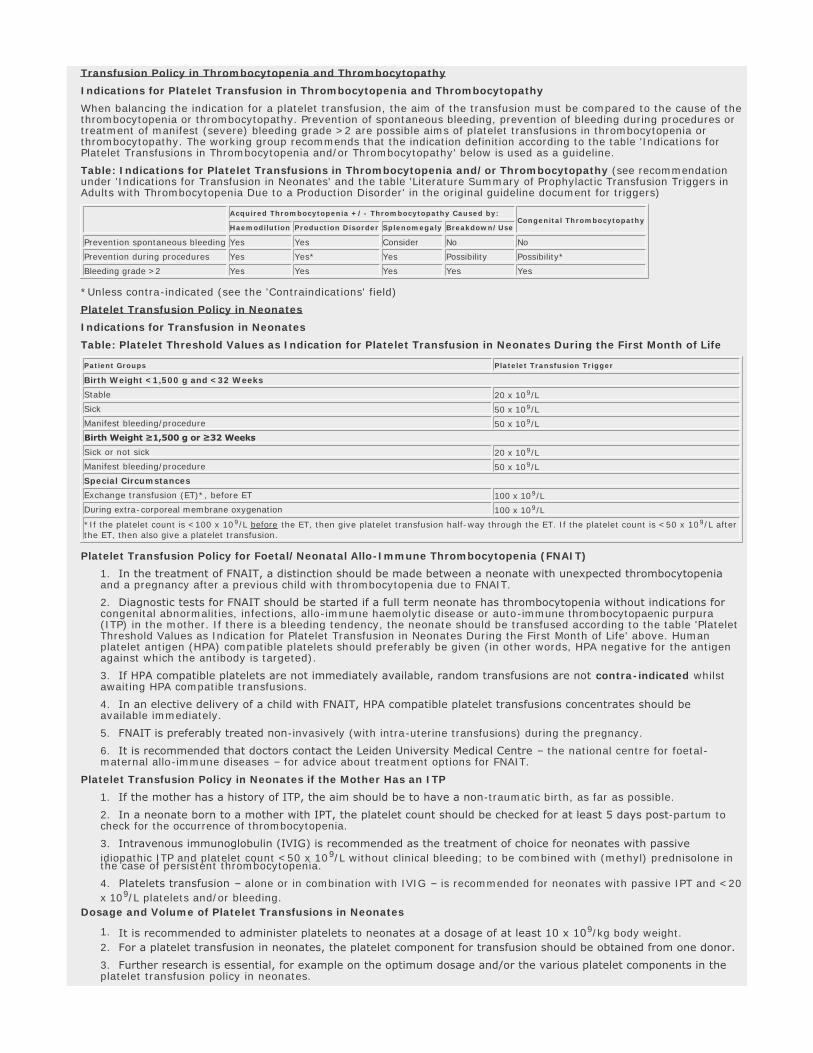
Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.
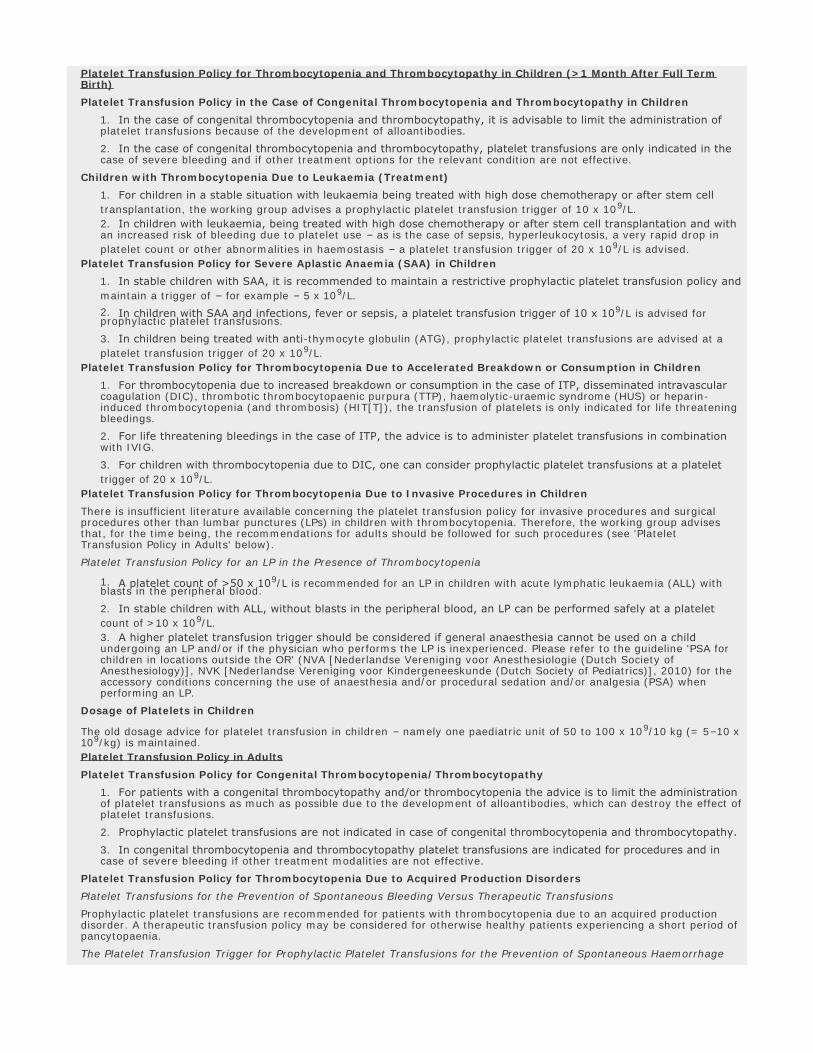
Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.

Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.
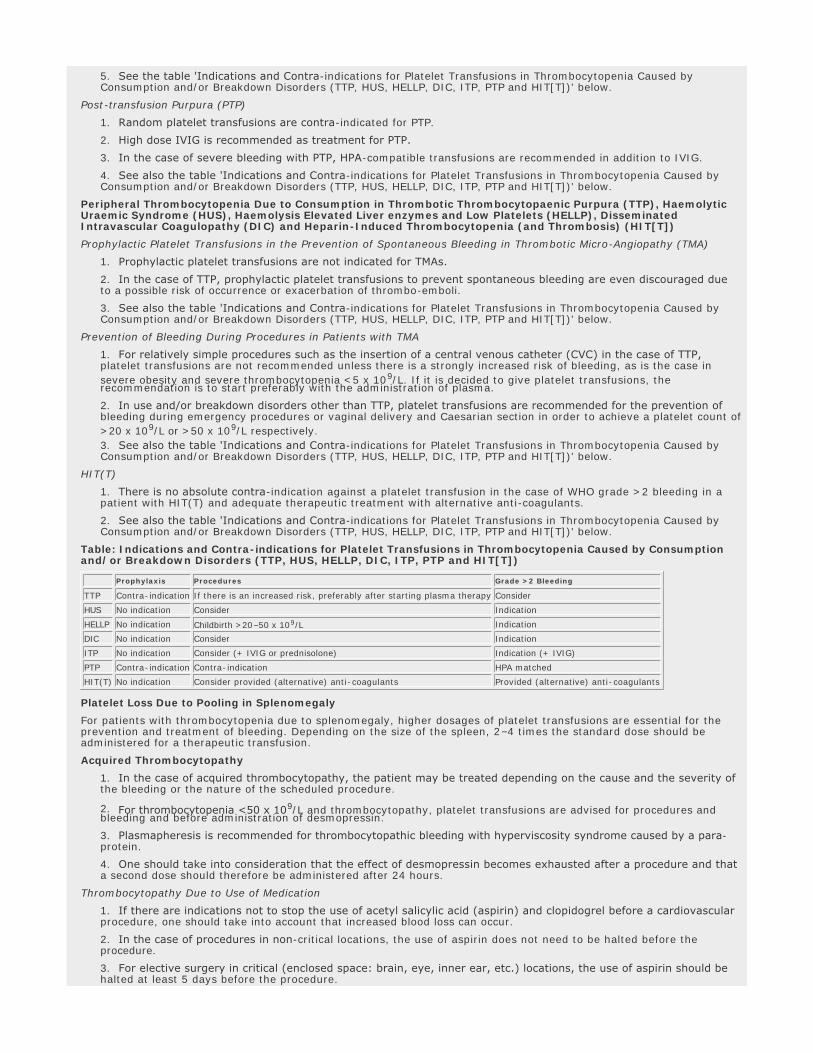
Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.
Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.

Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.

Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.
Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.
Guideline Summary NGC-9178
Guideline Title
Platelet and plasma transfusion policy. In: Blood transfusion guideline.
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Guideline Status
This is the current release of the guideline.
Scope
Disease/Condition(s)
Thrombocytopenia or thrombocytopathy
Guideline Category
Evaluation
Management
Prevention
Risk Assessment
Treatment
Clinical Specialty
Critical Care
Emergency Medicine
Family Practice
Gastroenterology
Hematology
Internal Medicine
Neurological Surgery
Nursing
Obstetrics and Gynecology
Oncology
Orthopedic Surgery
Pediatrics
Preventive Medicine
Rheumatology
Surgery
Thoracic Surgery
Intended Users
Advanced Practice Nurses
Hospitals
Nurses
Pharmacists
Physician Assistants
Physicians
Public Health Departments
Guideline Objective(s)
l To create a multi-disciplinary guideline on transfusion policy of blood and blood components
l To stimulate a more uniform clinical thinking and acting in the field of blood transfusion
l To confirm the role of nurses in blood transfusions
l To incorporate new national initiatives – such as the creation of the Transfusion Register for Irregular antibodies andX match problems (TRIX) database for irregular red cell antibodies
l To clinically evaluate transfusion and the clinical transfusion research to support the basis for guideline developmentand skills improvement of employees involved in blood transfusion, with a focus on the hospital situation
Target Population
Patients of all ages in the Netherlands who might require platelet or plasma transfusions, either in the hospital or outside the hospital, for example in the independent treatment centres (ITC) and via home care organisations
Interventions and Practices Considered
1. Indication for platelet transfusion in specific neonate populations l Foetal/neonatal allo-immune thrombocytopenia
l Neonates when mother has an auto-immune thrombocytopaenic purpura (ITP)
2. Indication for platelet transfusion in specific child populations l Congenital thrombocytopenia and thrombocytopathy in children
l Children with thrombocytopenia due to leukaemia
l Severe aplastic anaemia (SAA) in children
l Accelerated breakdown or consumption in children
l Children undergoing invasive procedures
3. Indication for platelet transfusion in specific adult populations l Congenital thrombocytopenia/thrombocytopathy
l Acquired production disorders
l Peripheral thrombocytopenia due to antibodies
l Thrombocytopenia due to antibodies consumption in thrombotic thrombocytopaenic purpura (TTP), haemolytic uraemic syndrome (HUS), haemolysis elevated liver enzymes and low platelets (HELLP), disseminated intravascular coagulopathy (DIC) and heparin-induced thrombocytopenia (and thrombosis) (HIT[T])
l Platelet loss due to pooling in splenomegaly
l Acquired thrombocytopathy
4. Platelet transfusion practices l Selection of human leukocyte antigen (HLA) and human platelet antigen (HPA) compatible donors
l Supporting treatments for therapy-resistant bleeding: erythrocyte transfusion, inhibition of fibrinolysis and recombinant factor VIIa (rFVIIa) erythrocyte transfusions
l Determination of dosage and volume of platelet transfusion in neonates, children and adults
Major Outcomes Considered
l Mortality
l Complication rates from plasma or platelet infusions
l Rate of change in platelet count
l Change in transfusion requirement
l Rate of transfusion failure (refractoriness)
Methodology
Methods Used to Collect/Select the Evidence
Hand-searches of Published Literature (Primary Sources)
Hand-searches of Published Literature (Secondary Sources)
Searches of Electronic Databases
Description of Methods Used to Collect/Select the Evidence
Relevant articles were found by performing systematic search actions in the Cochrane Library, Medline and EMBASE. The languages were limited to Dutch, English, German and French. Manual searches were also performed. The search was performed from 2003 (Medline) and for some questions also in EMBASE or CINAHL up to and including February 2008.
After the literature search, the result was evaluated by the working group members and the articles were evaluated for clinical relevance. If there was a possibility that the initial question could be answered with the article, the article was included in the selection.
Number of Source Documents
Not stated
Methods Used to Assess the Quality and Strength of the Evidence
Expert Consensus
Weighting According to a Rating Scheme (Scheme Given)
Rating Scheme for the Strength of the Evidence
Categorisation of Methodological Quality of Individual Studies
*This classification only applies in situations where controlled trials are not possible due to ethical or other reasons. If these are possible, then the classification for interventions applies.
Intervention Diagnostic Accuracy of Research Damage or Adverse Effects, Etiology,
Prognosis*
A1 Systematic review of at least two studies performed independently of each other at level A2
A2 Randomised, double-blind,
comparative clinical study of good
quality and sufficient size
Research with respect to a reference test (a 'golden standard'),
with previously defined limits and independent evaluation of the
results of test and gold standard, concerning a sufficiently large
series of consecutive patients who have only had the index test
and reference test
Prospective cohort study of sufficient
size and follow-up, with adequate
checks for 'confounding' and sufficient
exclusion of selective follow-up.
B Comparative study, but not with all
the characteristics as mentioned
under A2 (these also include patient-
control study, cohort study)
Study compared to a reference test, but not including all the
characteristics mentioned under A2
Prospective cohort study, but not
including all characteristics as
mentioned under A2 or a retrospective
cohort study or patient-control study
C Non-comparative study
D Expert opinion
Methods Used to Analyze the Evidence
Review of Published Meta-Analyses
Systematic Review with Evidence Tables
Description of the Methods Used to Analyze the Evidence
The guidelines and reviews that were found were evaluated for quality by the chairmen with the aid of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.
Methods Used to Formulate the Recommendations
Expert Consensus
Description of Methods Used to Formulate the Recommendations
Composition of the Core Group and Working Group
The blood transfusion policy guideline working group had a multi-disciplinary composition: as many professionals as possible from various disciplines – involved in blood transfusion – were asked to participate. In composing the working group, a balanced representation was sought of the various disciplines involved, the geographical distribution of the members and the proportion of academic to non-academic institutions. Members of the working group were invited to takepart in the working group via the relevant (scientific) associations based on their personal expertise and/or affinity with the subject. They did not receive any payment and/or reimbursement of travel costs for their presence at working group meetings. A small core group was formed from the members of the working group. The working group was chaired by two chairmen, who also acted as chairmen for the core group. The working group members and core group members acted independently and were mandated by their association for participation in the working group.
Working Method for Guideline Development
The revision started with an inventory of the bottlenecks observed in practice with the Blood Transfusion guideline from 2004, which served as a starting point for the revision. The working group members were asked to consult their association members to name and create an inventory of these bottlenecks. The relevant patient groups (see also under 'Patient perspective' in the original guideline document) were also asked to name and create an inventory of the bottlenecks that they experience in the practical situation. Once the bottlenecks had been collected, they were categorised in the relevant chapter. Seven initial questions were distilled from the prioritised bottlenecks for elaboration by a Centraal BegeleidingsOrgaan (CBO) advisor.
Core Group Working Method
The primary task of the core group was to monitor the progress of the entire process, including the results of the working group. The core group members were each responsible for the end result of one or more chapters. The core group also collaborated with the CBO in the final editing of the guideline.
Working Group Working Method
The working group worked on the creation of a draft guideline over a period of two and a half years. The entire working group met on several occasions for plenary discussion, development and approval of the draft texts. The working group worked in small sub-groups outside the plenary meetings on the revision of chapters for the guideline. Some working group members were involved in the revision of several chapters. For each chapter, one working group member was responsible for the revision of the chapter, supported by the core group member(s) with ultimate responsibility.
The CBO information specialist wrote the draft evidence text. These draft evidence texts were then evaluated by the relevant sub-working groups and supplemented with other considerations from the practical setting and recommendationsbased on the conclusions from the scientific literature and these other considerations.
All draft texts were discussed several times in the plenary working group, commented on and eventually approved.
Texts developed by the working group were then edited by the core group and the CBO to form the draft guideline. Prof. W.G. van Aken, internist n.p., read the draft texts in the final phase critically and made suggestions for improvement.
Where there continued to be a lack of evidence based knowledge on certain subjects despite new literature, the working group – based on discussion and consensus – formulated suggestions and recommendations.
Other Considerations
In order to make a recommendation, in addition to scientific proof, there were also other important aspects such as patient perspective, organisational aspects and costs.
Rating Scheme for the Strength of the Recommendations
See the 'Rating Scheme for the Strength of the Evidence' field for definitions of levels A1-C.
Level of Conclusions
1 Research of level A1 or at least 2 studies performed independently at level A2, with consistent results2 1 study of level A2 or at least 2 studies performed independently at level B3 1 study at level B or C4 Expert opinion
Cost Analysis
Cost-efficacy data are available in the original Dutch language guideline.
Method of Guideline Validation
External Peer Review
Internal Peer Review
Description of Method of Guideline Validation
The draft guideline, which could be consulted via the Centraal BegeleidingsOrgaan (CBO) website, was submitted to the relevant associations with mandated representatives in the working group for a consultation round (see the original guideline document for mandating organisations). The relevant groups listed under 'Patient perspective' in the original guideline document were also specifically asked to comment on the Blood Transfusion draft guideline. The resulting comments were processed in the definitive draft guideline. Following inclusion of the comments, the draft guideline was submitted to the associations for authorisation and it was approved on 1 August 2011.
Recommendations
Major Recommendations
Note from the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) and the National Guideline Clearinghouse (NGC): The Blood Transfusion Guideline has been divided into individual summaries covering blood components, laboratory aspects, chronic and acute anemia, platelet and plasma transfusions, side effects,and techniques to save blood. In addition to the current summary, the following are available:
l Blood components: characteristics, indications, logistics and administration
l Laboratory aspects
l Chronic anaemia
l Transfusion policy for acute anaemia
l Transfusion reactions and related conditions
l Blood saving techniques and medications
Transfusion Policy in Thrombocytopenia and Thrombocytopathy
Indications for Platelet Transfusion in Thrombocytopenia and Thrombocytopathy
When balancing the indication for a platelet transfusion, the aim of the transfusion must be compared to the cause of thethrombocytopenia or thrombocytopathy. Prevention of spontaneous bleeding, prevention of bleeding during procedures or treatment of manifest (severe) bleeding grade >2 are possible aims of platelet transfusions in thrombocytopenia or thrombocytopathy. The working group recommends that the indication definition according to the table 'Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy' below is used as a guideline.
Table: Indications for Platelet Transfusions in Thrombocytopenia and/or Thrombocytopathy (see recommendation under 'Indications for Transfusion in Neonates' and the table 'Literature Summary of Prophylactic Transfusion Triggers in Adults with Thrombocytopenia Due to a Production Disorder' in the original guideline document for triggers)
*Unless contra-indicated (see the 'Contraindications' field)
Platelet Transfusion Policy in Neonates
Indications for Transfusion in Neonates
Table: Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life
Platelet Transfusion Policy for Foetal/Neonatal Allo-Immune Thrombocytopenia (FNAIT)
1. In the treatment of FNAIT, a distinction should be made between a neonate with unexpected thrombocytopenia and a pregnancy after a previous child with thrombocytopenia due to FNAIT.
2. Diagnostic tests for FNAIT should be started if a full term neonate has thrombocytopenia without indications for congenital abnormalities, infections, allo-immune haemolytic disease or auto-immune thrombocytopaenic purpura (ITP) in the mother. If there is a bleeding tendency, the neonate should be transfused according to the table 'Platelet Threshold Values as Indication for Platelet Transfusion in Neonates During the First Month of Life' above. Human platelet antigen (HPA) compatible platelets should preferably be given (in other words, HPA negative for the antigen against which the antibody is targeted).
3. If HPA compatible platelets are not immediately available, random transfusions are not contra-indicated whilst awaiting HPA compatible transfusions.
4. In an elective delivery of a child with FNAIT, HPA compatible platelet transfusions concentrates should be available immediately.
5. FNAIT is preferably treated non-invasively (with intra-uterine transfusions) during the pregnancy.
6. It is recommended that doctors contact the Leiden University Medical Centre – the national centre for foetal-maternal allo-immune diseases – for advice about treatment options for FNAIT.
Platelet Transfusion Policy in Neonates if the Mother Has an ITP
1. If the mother has a history of ITP, the aim should be to have a non-traumatic birth, as far as possible.
2. In a neonate born to a mother with IPT, the platelet count should be checked for at least 5 days post-partum to check for the occurrence of thrombocytopenia.
3. Intravenous immunoglobulin (IVIG) is recommended as the treatment of choice for neonates with passive idiopathic ITP and platelet count <50 x 109/L without clinical bleeding; to be combined with (methyl) prednisolone in the case of persistent thrombocytopenia.
4. Platelets transfusion – alone or in combination with IVIG – is recommended for neonates with passive IPT and <20
x 109/L platelets and/or bleeding.
Dosage and Volume of Platelet Transfusions in Neonates
1. It is recommended to administer platelets to neonates at a dosage of at least 10 x 109/kg body weight.
2. For a platelet transfusion in neonates, the platelet component for transfusion should be obtained from one donor.
3. Further research is essential, for example on the optimum dosage and/or the various platelet components in the platelet transfusion policy in neonates.
Platelet Transfusion Policy for Thrombocytopenia and Thrombocytopathy in Children (>1 Month After Full Term Birth)
Platelet Transfusion Policy in the Case of Congenital Thrombocytopenia and Thrombocytopathy in Children
1. In the case of congenital thrombocytopenia and thrombocytopathy, it is advisable to limit the administration of platelet transfusions because of the development of alloantibodies.
2. In the case of congenital thrombocytopenia and thrombocytopathy, platelet transfusions are only indicated in the case of severe bleeding and if other treatment options for the relevant condition are not effective.
Children with Thrombocytopenia Due to Leukaemia (Treatment)
1. For children in a stable situation with leukaemia being treated with high dose chemotherapy or after stem cell transplantation, the working group advises a prophylactic platelet transfusion trigger of 10 x 109/L.
2. In children with leukaemia, being treated with high dose chemotherapy or after stem cell transplantation and with an increased risk of bleeding due to platelet use – as is the case of sepsis, hyperleukocytosis, a very rapid drop in
platelet count or other abnormalities in haemostasis – a platelet transfusion trigger of 20 x 109/L is advised.
Platelet Transfusion Policy for Severe Aplastic Anaemia (SAA) in Children
1. In stable children with SAA, it is recommended to maintain a restrictive prophylactic platelet transfusion policy andmaintain a trigger of – for example – 5 x 109/L.
2. In children with SAA and infections, fever or sepsis, a platelet transfusion trigger of 10 x 109/L is advised for prophylactic platelet transfusions.
3. In children being treated with anti-thymocyte globulin (ATG), prophylactic platelet transfusions are advised at a
platelet transfusion trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Accelerated Breakdown or Consumption in Children
1. For thrombocytopenia due to increased breakdown or consumption in the case of ITP, disseminated intravascular coagulation (DIC), thrombotic thrombocytopaenic purpura (TTP), haemolytic-uraemic syndrome (HUS) or heparin-induced thrombocytopenia (and thrombosis) (HIT[T]), the transfusion of platelets is only indicated for life threatening bleedings.
2. For life threatening bleedings in the case of ITP, the advice is to administer platelet transfusions in combination with IVIG.
3. For children with thrombocytopenia due to DIC, one can consider prophylactic platelet transfusions at a platelet trigger of 20 x 109/L.
Platelet Transfusion Policy for Thrombocytopenia Due to Invasive Procedures in Children
There is insufficient literature available concerning the platelet transfusion policy for invasive procedures and surgical procedures other than lumbar punctures (LPs) in children with thrombocytopenia. Therefore, the working group advises that, for the time being, the recommendations for adults should be followed for such procedures (see 'Platelet Transfusion Policy in Adults' below).
Platelet Transfusion Policy for an LP in the Presence of Thrombocytopenia
1. A platelet count of >50 x 109/L is recommended for an LP in children with acute lymphatic leukaemia (ALL) with blasts in the peripheral blood.
2. In stable children with ALL, without blasts in the peripheral blood, an LP can be performed safely at a platelet count of >10 x 109/L.
3. A higher platelet transfusion trigger should be considered if general anaesthesia cannot be used on a child undergoing an LP and/or if the physician who performs the LP is inexperienced. Please refer to the guideline 'PSA for children in locations outside the OR' (NVA [Nederlandse Vereniging voor Anesthesiologie (Dutch Society of Anesthesiology)], NVK [Nederlandse Vereniging voor Kindergeneeskunde (Dutch Society of Pediatrics)], 2010) for the accessory conditions concerning the use of anaesthesia and/or procedural sedation and/or analgesia (PSA) when performing an LP.
Dosage of Platelets in Children
The old dosage advice for platelet transfusion in children – namely one paediatric unit of 50 to 100 x 109/10 kg (= 5–10 x109/kg) is maintained.
Platelet Transfusion Policy in Adults
Platelet Transfusion Policy for Congenital Thrombocytopenia/Thrombocytopathy
1. For patients with a congenital thrombocytopathy and/or thrombocytopenia the advice is to limit the administration of platelet transfusions as much as possible due to the development of alloantibodies, which can destroy the effect ofplatelet transfusions.
2. Prophylactic platelet transfusions are not indicated in case of congenital thrombocytopenia and thrombocytopathy.
3. In congenital thrombocytopenia and thrombocytopathy platelet transfusions are indicated for procedures and in case of severe bleeding if other treatment modalities are not effective.
Platelet Transfusion Policy for Thrombocytopenia Due to Acquired Production Disorders
Platelet Transfusions for the Prevention of Spontaneous Bleeding Versus Therapeutic Transfusions
Prophylactic platelet transfusions are recommended for patients with thrombocytopenia due to an acquired production disorder. A therapeutic transfusion policy may be considered for otherwise healthy patients experiencing a short period of pancytopaenia.
The Platelet Transfusion Trigger for Prophylactic Platelet Transfusions for the Prevention of Spontaneous Haemorrhage
1. In the case of a standard risk of bleeding, a transfusion trigger of 10 x 109/L is recommended for prophylactic platelet transfusions.
2. If there are additional clinical complications that promote bleeding, it is recommended that the platelet transfusion trigger be increased to 20 x 109/L for prophylactic platelet transfusions.
3. For patients with an indication for anti-coagulant treatment, it is recommended to increase the platelet transfusion
trigger to 50 x 109/L in order to prevent spontaneous bleeding; this is not evidence based.
4. For patients who have recently (past 5 days) experienced a World Health Organization (WHO) grade >2 bleed, it isrecommended to increase the threshold for a platelet transfusion to 20 x 109/L and to analyse or remove other risk factors.
Platelet Transfusion Dose in Platelet Transfusions for the Prevention of Spontaneous Bleeding
A dose of approximately 3.5 x 1011 (this is the dose of a standard preparation and contains 5 x 109 platelets/kg for a patient of 70 kg) is recommended for prophylactic platelet transfusions in adults.
Platelet Transfusion Policy for the Prevention of Bleeding in (Elective) Procedures
The following table can be used as a rule of thumb for platelet target values to prevent bleeding during common, electiveprocedures.
Table: Target Values for Platelets During Procedures
Platelet Transfusions for the Treatment of Bleeding
1. In the case of a severe bleed (WHO grade ≥3), platelets should be transfused until the bleeding stops and/or the platelet count is >50 x 109/L.
2. With respect to bleeding in enclosed spaces of vital organs – such as the brain, the nervous system and the eye – the advice is to transfuse platelets to a platelet count of >100 x 109/L.
Peripheral Thrombocytopenia Due to Antibodies
Auto-immune Thrombocytopaenic Purpura (ITP)
1. Prophylactic platelet transfusions for the prevention of spontaneous bleeding are not indicated in ITP.
2. For elective procedures in ITP patients, the recommended treatment is prednisolone or IVIG, alone or in combination with platelet transfusions if necessary.
3. With ITP, platelets should preferably be administered after IVIG.
4. In patients with ITP and severe WHO grade >2 bleeding, (high dose) platelet transfusions are recommended and this is also the case if it is not possible to wait for the effect of a therapeutic dose of IVIG.
5. See the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Post-transfusion Purpura (PTP)
1. Random platelet transfusions are contra-indicated for PTP.
2. High dose IVIG is recommended as treatment for PTP.
3. In the case of severe bleeding with PTP, HPA-compatible transfusions are recommended in addition to IVIG.
4. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Peripheral Thrombocytopenia Due to Consumption in Thrombotic Thrombocytopaenic Purpura (TTP), Haemolytic Uraemic Syndrome (HUS), Haemolysis Elevated Liver enzymes and Low Platelets (HELLP), Disseminated Intravascular Coagulopathy (DIC) and Heparin-Induced Thrombocytopenia (and Thrombosis) (HIT[T])
Prophylactic Platelet Transfusions in the Prevention of Spontaneous Bleeding in Thrombotic Micro-Angiopathy (TMA)
1. Prophylactic platelet transfusions are not indicated for TMAs.
2. In the case of TTP, prophylactic platelet transfusions to prevent spontaneous bleeding are even discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Prevention of Bleeding During Procedures in Patients with TMA
1. For relatively simple procedures such as the insertion of a central venous catheter (CVC) in the case of TTP, platelet transfusions are not recommended unless there is a strongly increased risk of bleeding, as is the case in
severe obesity and severe thrombocytopenia <5 x 109/L. If it is decided to give platelet transfusions, the recommendation is to start preferably with the administration of plasma.
2. In use and/or breakdown disorders other than TTP, platelet transfusions are recommended for the prevention of bleeding during emergency procedures or vaginal delivery and Caesarian section in order to achieve a platelet count of
>20 x 109/L or >50 x 109/L respectively.
3. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
HIT(T)
1. There is no absolute contra-indication against a platelet transfusion in the case of WHO grade >2 bleeding in a patient with HIT(T) and adequate therapeutic treatment with alternative anti-coagulants.
2. See also the table 'Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])' below.
Table: Indications and Contra-indications for Platelet Transfusions in Thrombocytopenia Caused by Consumption and/or Breakdown Disorders (TTP, HUS, HELLP, DIC, ITP, PTP and HIT[T])
Platelet Loss Due to Pooling in Splenomegaly
For patients with thrombocytopenia due to splenomegaly, higher dosages of platelet transfusions are essential for the prevention and treatment of bleeding. Depending on the size of the spleen, 2–4 times the standard dose should be administered for a therapeutic transfusion.
Acquired Thrombocytopathy
1. In the case of acquired thrombocytopathy, the patient may be treated depending on the cause and the severity of the bleeding or the nature of the scheduled procedure.
2. For thrombocytopenia <50 x 109/L and thrombocytopathy, platelet transfusions are advised for procedures and bleeding and before administration of desmopressin.
3. Plasmapheresis is recommended for thrombocytopathic bleeding with hyperviscosity syndrome caused by a para-protein.
4. One should take into consideration that the effect of desmopressin becomes exhausted after a procedure and that a second dose should therefore be administered after 24 hours.
Thrombocytopathy Due to Use of Medication
1. If there are indications not to stop the use of acetyl salicylic acid (aspirin) and clopidogrel before a cardiovascular procedure, one should take into account that increased blood loss can occur.
2. In the case of procedures in non-critical locations, the use of aspirin does not need to be halted before the procedure.
3. For elective surgery in critical (enclosed space: brain, eye, inner ear, etc.) locations, the use of aspirin should be halted at least 5 days before the procedure.
4. For emergency procedures or bleeding under aspirin therapy, a standard dose platelet transfusion should be sufficient; at least 2 doses are necessary in the case of combined use with clopidogrel.
5. Research is necessary to determine the benefit of platelet transfusions in (cerebral) haemorrhage during the use ofplatelet inhibitors.
6. Platelet transfusions – alone or in combination with desmopressin – are necessary in the case of an acute intervention with the use of anti-IIb/IIIa inhibitors in order to absorb the antibodies.
Platelet Transfusions in Practice
Selection of Human Leukocyte Antigen (HLA) (HPA) Compatible Donors
1. Screening for HLA antibodies is recommended if the 1-hour corrected count increment (CCI) of a fresh ABO compatible platelet transfusion is <7.5 twice in a row in a patient without clinical factors that could explain this (this is then a case of platelet refractoriness).
2. If ABO and HLA compatible transfusions result in a CCI <7.5 – in the absence of clinical factors that could explain this – serological analysis for platelet specific antigens (HPA) is recommended.
3. The working group is of the opinion that communication between treating doctor, hospital transfusion service and the Clinical Consultative Service of the Blood Supplier is essential for effective implementation and support with HLA matched platelet transfusions.
ABO/Rh-D Selection
See ' Platelet characteristics' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration and 'ABO Compatibility of Platelets' in the NGC summary of the DIHG guideline Laboratory aspects.
Supporting Treatments for Therapy-Resistant Bleeding
Erythrocyte Transfusion, Inhibition of Fibrinolysis and Recombinant Factor VIIa (rFVIIa) Erythrocyte Transfusions
1. For patients with thrombocytopenia and bleeding – who cannot be, or are poorly, corrected with platelet transfusions, it is recommended to consider increasing the haematocrit to >0.30 L/L in order to reduce the tendency to bleed.
2. In patients with thrombocytopenia and mucous membrane bleeding (bleeding from nose and gums, menorrhagia), anti-fibrinolytic medication can be considered to reduce the tendency to bleed. Fibrinolysis inhibition is contra-indicated in haematuria because of the risk of thrombus formation in the urinary tract.
3. It is recommended that a (preferably national) registration takes place of the use of rFVIIa for bleeding in patientswith thrombocytopenia and that protocols be developed for evaluation and reporting of the effect of the use of rFVIIa for this indication.
IVIG
Administration of IVIG before a platelet transfusion is not recommended in the case of refractoriness due to HLA antibodies.
Plasma Transfusions for Non-surgical Patients
See 'Plasma' in the NGC summary of the DIHG guideline Blood components: characteristics, indications, logistics and administration for the indications for plasma.
Plasma Transfusions in Children
1. Treatment with plasma or plasmapheresis is generally not indicated in children with d+ HUS.
2. Treatment with plasma or plasmapheresis is recommended for children with atypical (dneg) HUS or recurrent HUS ina transplanted kidney.
3. After therapeutic plasma administration, prophylactic plasma transfusions are indicated in children with TTP causedby a congenital ADAMTS-13 deficiency.
Plasma Transfusions in Adults
Plasmapheresis for Primary TMAs
1. Treatment of HELLP syndrome with plasma(pheresis) is not recommended, unless there has been either no improvement or deterioration has occurred >72 hours post-partum.
2. Plasma administration is recommended as therapy of choice for TTP and for atypical (dneg) HUS.
3. Plasma administration/plasmapheresis is indicated for TTP and HUS before or shortly after childbirth.
4. Plasmapheresis is preferred to plasma transfusion for the treatment of thrombotic thrombocytopaenic purpura (TTP) or atypical (dneg) HUS.
5. For the time being, methylene blue treated plasma is not recommended for the treatment of thrombotic micro-angiopathies (TMA)/thrombotic thrombocytopaenic purpura (TTP).
Secondary TMAs
1. Plasma(pheresis) is not recommended for TMA associated with extensively metastasised carcinoma.
2. Plasma(pheresis) is not recommended for post stem cell transplant (SCT) and post bone marrow transplant (BMT) induced TMA.
3. Plasma(pheresis) is not recommended for TMA caused by cytostatics.
4. Plasma(pheresis) is not recommended for cyclosporin A or tacrolimus (FK 506) induced TMA.
5. Plasmapheresis is recommended for TMA induced by ticlopidine, clopidogrel and a number of other medications.
6. Plasmapheresis is recommended for HIV induced TMA.
7. Plasmapheresis can be considered in the rare combination of TMA and catastrophic anti-phospholipid syndrome if standard treatment provides insufficient effect.
Supplementation of Clotting Factors for Deficiencies
1. In the case of procedures, it is recommended to take into consideration the dilution coagulopathy due to plasmapheresis treatment with a daily frequency (or every other day) without plasma as substitution liquid.
2. Treatment with plasma does not have a role in vitamin K deficiency and/or the tapering of oral anti-coagulants (vitamin K antagonists).
3. For the tapering of anti-fibrinolytics in the case of bleeding, it is recommended to administer plasma or a fibrinogen preparation – based on aPTT and fibrinogen level – in addition to tranexamic acid in the case of an prolonged activated partial thromboplastin time (aPTT) and a low fibrinogen level.
Plasma Transfusion Policy for Severe DIC with Bleeding
In patients with DIC who are bleeding, need to undergo an invasive procedure or have some other severe risk of bleeding,treatment with plasma, supplemented by a fibrinogen concentrate if necessary, should be considered.
Plasma Component Choice and Blood Group Incompatibility
1. Further research is essential to be able to recommend the optimal plasma component in relation to indication and patient.
2. Further research on the effects of ABO compatible but not ABO identical plasma is recommended and it is preferable to transfuse in an ABO identical manner.
Acquired Thrombocytopenia +/- Thrombocytopathy Caused by:Congenital Thrombocytopathy
Haemodilution Production Disorder Splenomegaly Breakdown/Use
Prevention spontaneous bleeding Yes Yes Consider No No
Prevention during procedures Yes Yes* Yes Possibility Possibility*
Bleeding grade >2 Yes Yes Yes Yes Yes
Patient Groups Platelet Transfusion Trigger
Birth Weight <1,500 g and <32 Weeks
Stable 20 x 109/L
Sick 50 x 109/L
Manifest bleeding/procedure 50 x 109/L
Birth Weight ≥1,500 g or ≥32 Weeks
Sick or not sick 20 x 109/L
Manifest bleeding/procedure 50 x 109/L
Special Circumstances
Exchange transfusion (ET)*, before ET 100 x 109/L
During extra-corporeal membrane oxygenation 100 x 109/L
*If the platelet count is <100 x 109/L before the ET, then give platelet transfusion half-way through the ET. If the platelet count is <50 x 109/L afterthe ET, then also give a platelet transfusion.
Procedure Platelets x 109/L
Arthrocentesis >50
Ascites/pleural puncture (thin needle) N/A
Ascites drain, pleural drain and pericardial drain >50
Bone marrow aspiration N/A
Bone marrow biopsy (Jamshidi needle) N/A
Blind organ biopsy or puncture >50
Bronchoscopy with biopsy or brush >50
Insertion of central venous catheter >50
Removal of central venous catheter N/A
Small intestine biopsy >50
Electromyogram (EMG) >20
Endoscopy + deep loop biopsy or polypectomy large polyp >50
Endoscopy without biopsy >20
Endoscopy with 'ordinary biopsy' >50
Endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy >50
Eye surgery (except cataract) >100
Laparoscopy without biopsy >50
Laparoscopy with biopsy or procedure >50
Laser coagulation (not retina) N/A
Liver biopsy (percutaneous) >50
Lumbar puncture >20*
Myelography, radiculo-saccography >50
Neurosurgery >100
Pacemaker implantation >50
Percutaneous transhepatic cholangiography >50
Plexus anaesthesia, epidural >50
Seldinger arterial >50
Muscle biopsy >50
Sclerosing oesophageal varices >50
Tooth/molar extractions >50
Thoracoscopy/arthroscopy >50
*In the case of leukaemic blasts in the peripheral blood: >50 x 109/L
Prophylaxis Procedures Grade >2 Bleeding
TTP Contra-indication If there is an increased risk, preferably after starting plasma therapy Consider
HUS No indication Consider Indication
HELLP No indication Childbirth >20–50 x 109/L Indication
DIC No indication Consider Indication
ITP No indication Consider (+ IVIG or prednisolone) Indication (+ IVIG)
PTP Contra-indication Contra-indication HPA matched
HIT(T) No indication Consider provided (alternative) anti-coagulants Provided (alternative) anti-coagulants
Clinical Algorithm(s)
None provided
Evidence Supporting the Recommendations
Type of Evidence Supporting the Recommendations
The type of evidence supporting the recommendations is not specifically stated.
Benefits/Harms of Implementing the Guideline Recommendations
Potential Benefits
Appropriate and safe management of patients who might require platelet or plasma transfusions
Potential Harms
l Systematic reviews concluded that more research is necessary before conclusions can be drawn on the efficacy and adverse effects of the various plasma components.
l Dilution coagulopathy can occur in the case of daily plasmapheresis (or every other day) with a non-plasma substitution agent. Thrombosis has been described incidentally with the use of albumin as a substitution liquid; the estimated incidence is 0.060% to 0.14%. Bleeding has very rarely been described.
l The effect of desmopressin has not been examined in thrombocytopenia <50 x 109/L and is not authorised for use inpregnancy or with suspected cerebral haemorrhage. Cerebral and cardiac infarction have been described as complications in renal patients. It is useful to determine the bleeding time to monitor the effect of desmopressin.
l In the case of thrombotic thrombocytopaenic purpura (TTP), prophylactic platelet transfusions to prevent spontaneous bleeding are discouraged due to a possible risk of occurrence or exacerbation of thrombo-emboli.
See also the National Guideline Clearinghouse (NGC) summary of the Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) guideline Transfusion reactions and related conditions.
Contraindications
Contraindications
l There are many sub-types of type 2 von Willebrand Disease (vWD) and desmopressin is contra-indicated for type 2B because it can cause platelet aggregation and thrombocytopenia. Type 2A is treatable with desmopressin. Desmopressin is not effective for the very rare type 3.
l Desmopressin is also contra-indicated in cardiac decompensation.
l Prophylactic and procedure-related platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
l Platelet transfusion is contra-indicated for thrombotic thrombocytopaenic purpura (TTP), because the occurrence of cerebral infarction has been described following platelet transfusions. A review of the literature shows that there is no convincing evidence of damage due to platelet transfusions in TTP patients. The efficacy of prophylactic platelet transfusions for TTP has also not been demonstrated.
l The guideline on neuraxis blockade and anti-coagulants states that every form of neuraxis blockade is contra-indicated with IIb/IIIa inhibitors.
l Fibrinolysis inhibition is contra-indicated in haematuria due to the risk of thrombus formation in the urinary tract.
l Random platelet transfusions are contra-indicated for post-transfusion purpura (PTP).
Qualifying Statements
Qualifying Statements
Guidelines are not legal instructions, but rather scientifically substantiated and/or broadly accepted insights and recommendations that care providers should follow in order to offer good quality care. As guidelines are based on 'the average patient', care providers can, if necessary, deviate from the recommendations in the guideline in individual cases. Sometimes it may even be essential to deviate from guidelines if the patient's situation demands this. However, if a conscious decision is made to deviate from the guideline, a case must be made for this and it must be documented. One should also consider whether this should be discussed with the patient, or whether the patient should be informed.
Implementation of the Guideline
Description of Implementation Strategy
The guideline was initially disseminated through the websites of scientific and professional associations that were involved and made available through the website of the Centraal BegeleidingsOrgaan (CBO; www.cbo.nl ).
The definitive guideline will be disseminated amongst the associations and will be available in digital format. The recommendations of the guideline will be presented at scientific meetings of the relevant scientific associations. An announcement of this guideline will be submitted for publication to the Netherlands Journal of Medicine, the Journal for Blood Transfusion and the Netherlands Journal of Clinical Chemistry and Laboratory Medicine.
In order to stimulate the implementation and evaluation of this guideline, internal indicators have been developed, whichallow for the implementation to be measured by random sampling. In general, indicators give the care providers the opportunity to evaluate whether they are providing the desired care. This enables them also to identify subjects for improvement of the care provision. The internal indicators that were developed for this guideline are discussed in Chapter9 of the original guideline document.
Implementation Tools
Audit Criteria/Indicators
Foreign Language Translations
Quick Reference Guides/Physician Guides
For information about availability, see the Availability of Companion Documents and Patient Resources fields below.
Institute of Medicine (IOM) National Healthcare Quality Report Categories
IOM Care Need
Getting Better
Living with Illness
Staying Healthy
IOM Domain
Effectiveness
Safety
Identifying Information and Availability
Bibliographic Source(s)
Platelet and plasma transfusion policy. In: Blood transfusion guideline. Utrecht (The Netherlands): Dutch Institute for Healthcare Improvement CBO; 2011. p. 209-77. [291 references]
Adaptation
Not applicable: The guideline was not adapted from another source.
Date Released
2011
Guideline Developer(s)
Dutch Institute for Healthcare Improvement CBO - Professional Association
Source(s) of Funding
The Blood Transfusion Policy guideline project was financed by The Netherlands Organisation for Health Research and Development (ZonMw) within the programme Knowledge Policy Quality of Curative Care.
The Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) is extremely grateful to the Sanquin Blood Supply Foundation for financing this translation.
Guideline Committee
Dutch Institute for Healthcare Improvement Centraal BegeleidingsOrgaan (CBO) (DIHG) Working Group
Composition of Group That Authored the Guideline
Core Group Members: F.J.L.M. Haas (Chairman), Prof. D.J. van Rhenen, Prof. R.R.P. de Vries (Chairman), Mrs M.A.M. Overbeeke, Dr V.M.J. Novotny, Dr Ch.P. Henny
Working Group Members: Prof. A. Brand, internist-haematologist, manager of research & education, Sanquin Blood Supply Region SW, Department of Research & Education, Leiden; Ms H. de Bruijn-van Beek, general secretary board, Sanquin Blood Supply, Amsterdam; Dr C.L. van der Poel, transfusion doctor-epidemiologist, Secretary for medical affairs, Sanquin Blood Supply, Group personnel, Amsterdam; Dr E.A.M. Beckers, transfusion specialist, University Medical Centre, Haematology Department, Maastricht; T. Reker, transplant coordinator, University Medical Centre, Groningen [until 01-05-2009]; Ms N.W.M. Gerrits, senior nurse haematology/oncology, Onze Lieve Vrouwe Gasthuis, ward C6, Amsterdam; Dr Ch.P. Henny, anaesthesiologist, Academic Medical Centre, Anaesthesiology department, Amsterdam; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr A.W.M.M. Koopman-van Gemert, anaesthesiologist-intensivist, Albert Schweitzer Hospital, location Dordtwijk, Anaesthesiology department, Dordrecht; Dr V.M.J. Novotny, internist-haematologist/blood transfusion specialist, St. Radboud University Medical Centre, Haematology department, Nijmegen; Mrs M.A.M. Overbeeke, biologist, head of Immunohaematology department, Sanquin Blood Supply, Diagnostics Division, Amsterdam; Mrs M. Smelt, haemovigilance employee, St. Antonius Hospital, Clinical Chemistry Laboratory, Nieuwegein; Dr M.R. Schipperus, internist-haematologist, Haga Hospital, Haematology department, The Hague; Dr J. Schönberger, cardiothoracic surgeon, CatharinaHospital, Department of Cardiothoracic Surgery, Eindhoven; Dr R.Y.J. Tamminga, paediatrician, oncologist-haematologist, University Medical Centre, Beatrix Children's Clinic, Groningen; Dr C.H. van Ommen, paediatrician-haematologist, Academic Medical Centre, department of Paediatric Haematology, Amsterdam; Dr. E. Lopriore, paediatrician-neonatologist, Leiden University Medical Centre, department of neonatology, Leiden; Dr R.C.R.M. Vossen, clinical chemist,Orbis Medical Centre, clinical chemistry & haematology laboratory, Sittard; Dr J. Slomp, clinical chemist, Medical SpectrumTwente, Laboratory, Enschede; Prof. D.J. van Rhenen, internist-haematologist, division director Sanquin Blood Supply, SWRegion, Rotterdam; Dr J.J. Zwaginga, staff member blood transfusion service, head of stem cell therapy centre, Leiden University Medical Centre, department of Immunohaematology, Leiden; Dr B.J. Biemond, internist-haematologist, Academic Medical Centre/University of Amsterdam, department of Internal Medicine, Amsterdam; Dr J.Th.M. de Wolf, internist-haematologist, University Medical Centre, Groningen (until 01-04-2009); Dr R.E.G. Schutgens, internist-haematologist, University Medical Centre, Utrecht (as of 15-04-2009); Dr P.J. Kabel, physician-microbiologist, Regional Laboratory for Public Health, LMMI department, Tilburg; Dr G.C.M.L. Page-Christiaens, perinatologist, University Medical Centre, Obstetric department, Utrecht; Dr J.G. Loeber, clinical chemist, head of laboratory, RIVM, LIS department, Bilthoven (Chapter 9: Indicators); Dr A. Castel (up to and including February 2009); Dr Y.B. de Rijke, (as of March 2009), clinical chemist, Erasmus Medical Centre, department of Clinical Chemistry, Rotterdam; H.E. Polak, anaesthesiology nurse, Via Sana Clinic, Mill; Prof. R.J. Porte, University Medical Centre, department of Surgery, Groningen; W.G. Horstmann (up to and including March 2009)]; D.B. van der Schaaf, orthopaedic surgeon, Sint Maartens Clinic, Orthopaedics department, Nijmegen (as of April 2009)
Financial Disclosures/Conflicts of Interest
No relationships relevant to this guideline of working group members with the pharmaceutical industry were reported.
Guideline Status
This is the current release of the guideline.
Guideline Availability
Electronic copies: Available in English and Dutch from http://www.diliguide.nl/document/2903 .
Availability of Companion Documents
Quality indicators are available in Chapter 9 of the original guideline document .
In addition, a pocket guide is available in Dutch from http://www.diliguide.nl/document/2903 .
Patient Resources
None available
NGC Status
This NGC summary was completed by ECRI Institute on October 9, 2012. The information was verified by the guideline developer on November 14, 2012.
Copyright Statement
This summary is based on the original guideline, which is subject to the guideline developer's copyright restrictions.
Disclaimer
NGC Disclaimer
The National Guideline Clearinghouse™ (NGC) does not develop, produce, approve, or endorse the guidelines representedon this site.
All guidelines summarized by NGC and hosted on our site are produced under the auspices of medical specialty societies, relevant professional associations, public or private organizations, other government agencies, health care organizations or plans, and similar entities.
Guidelines represented on the NGC Web site are submitted by guideline developers, and are screened solely to determinethat they meet the NGC Inclusion Criteria which may be found at http://www.guideline.gov/about/inclusion-criteria.aspx.
NGC, AHRQ, and its contractor ECRI Institute make no warranties concerning the content or clinical efficacy or effectiveness of the clinical practice guidelines and related materials represented on this site. Moreover, the views and opinions of developers or authors of guidelines represented on this site do not necessarily state or reflect those of NGC, AHRQ, or its contractor ECRI Institute, and inclusion or hosting of guidelines in NGC may not be used for advertising or commercial endorsement purposes.
Readers with questions regarding guideline content are directed to contact the guideline developer.