plenary 3 - hysteroscopy - aagl · safety, efficacy and reproductive outcomes of hysteroscopic...
TRANSCRIPT

Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
Plenary 3 - Hysteroscopy
MODERATORS
Philip G. Brooks, MDAngelos G. Vilos, MD
Attilio Di Spiezio Sardo, MDKarina M. Haber, MD Nicholas A. Ryan, MD
Simone Ferrero, MD, PhDTadeusz Issat, MD
Lennie van Hanegem, MD
GLOBAL CONGRESSON MINIMALLY INVASIVE GYNECOLOGYNOV. 17-21, 2014 | Vancouver, British Columbia
43rd AAGL

Professional Education Information Target Audience This educational activity is developed to meet the needs of residents, fellows and new minimally invasive specialists in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.

Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 2 Safety, Efficacy and Reproductive Outcomes of Hysteroscopic Outpatient Metroplasty to Expand Dysmorphic Uteri (HOME‐DU Technique) A. Di Spiezio Sardo ........................................................................................................................................ 3 Office Essure in Septate Uterus and Double Cervix K.M. Haber .................................................................................................................................................... 5 Triptorelin, Letrozole and Ulipristal Acetate Treatment before Hysteroscopic Resection of Large Myomas: Prospective Comparative Study S. Ferrero ....................................................................................................................................................... 6 Resection of Retained Products of Conception with the Myosure XL N.A. Ryan ....................................................................................................................................................... 9 Diagnostic Work‐Up for Postmenopausal Bleeding – A Randomized Controlled Trial L. van Hanegem ................................................................................................................................ 10 A Randomized, Single Blind, Placebo‐Controlled Trial for the Pain Reduction during the Outpatient Hysteroscopy after Ketoprofen or Intravaginal Misoprostol T. Issat ......................................................................................................................................................... 13 Cultural and Linguistics Competency ......................................................................................................... 16
Plenary 3 ‐ Hysteroscopy
Moderators: Philip G. Brooks, Angelos G. Vilos
Faculty: Attilio Di Spiezio Sardo, Simone Ferrero, Karina M. Haber, Tadeusz Issat, Nicholas A. Ryan, Lennie van Hanegem
This session is comprised of presentations by experienced hysteroscopists who will describe how hysteroscopy can be used safely and more effectively to improve reproductive function and/or reduce symptoms of bleeding from retained products of conception, intracavitary myomata and/or congenitally deformed uteri. Studies of medications to reduce myoma size or decrease operative pain from hysteroscopies will be reported. Learning Objectives: At the conclusion of this course, the participant will be able to: 1) Describe the use of operative hysteroscopy in patients with various congenital uterine deformities, emphasizing the safety and efficacy of hysteroscopy in the management of abnormal uterine bleeding.
Course Outline 2:15 Safety, Efficacy and Reproductive Outcomes of Hysteroscopic Outpatient
Metroplasty to Expand Dysmorphic Uteri (HOME‐DU) Technique) A. Di Spiezio Sardo
2:25 Office Essure in Septate Uterus and Double Cervix K.M. Haber
2:31 Triptorelin, Letrozole and Ulipristal Acetate Treatment before Hysteroscopic Resection of Large Myomas: Prospective Comparative Study S. Ferrero
2:41 Resection of Retained Products of Conception with the Myosure XL N.A. Ryan
2:48 Diagnostic Work‐Up for Postmenopausal Bleeding – A Randomized Controlled Trial L. van Hanegem
2:58 A Randomized, Single Blind, Placebo‐Controlled Trial for the Pain Reduction during the Outpatient Hysteroscopy after Ketoprofen or Intravaginal Misoprostol T. Issat
3:15 Adjourn
Page 1

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Viviane F. Connor* Kimberly A. Kho* Frank D. Loffer, Medical Director, AAGL* Linda Michels, Executive Director, AAGL* M. Jonathon Solnik* Johnny Yi*
SCIENTIFIC PROGRAM COMMITTEE Arnold P. Advincula Consultant: Blue Endo, Intuitive Surgical, SurgiQuest Other: Royalties: CooperSurgical William M. Burke* Rosanne M. Kho* Ted T.M. Lee Consultant: Ethicon Endo‐Surgery Javier F. Magrina* Ceana H. Nezhat Consultant: Karl Storz Other: Medical Advisor: Plasma Surgical Other: Scientific Advisory Board: SurgiQuest Kevin J.E. Stepp Consultant: CONMED Corporation, Teleflex Other: Stock Ownership: Titan Medical Robert K. Zurawin Consultant: Bayer Healthcare Corp., CONMED Corporation, Ethicon Endo‐Surgery, Hologic, Intuitive Surgical FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Philip G. Brooks* Attilio Di Spiezio Sardo* Simone Ferrero* Karina M. Haber* Tadeusz Issat* Nicholas A. Ryan* Nehalennia (Lennie) van Hanegem* Angelos Vilos* Asterisk (*) denotes no financial relationships to disclose.
Page 2

ATTILIO DI SPIEZIO SARDO, MD, PhDDepartment of Obstetrics and Gynecology
University “Federico II” of Naples
Diagnosing class U1 uteri…
Past
Present
“HOME-DU TECHNIQUE”
Ambulatory setting
Conscious sedation
5-mm hysteroscope
Vaginoscopic approach
5 Fr bipolar electrode
Polyethylene oxide-sodium carboxymethylcellulose gel
Population
T-shaped Tubular
I
IO
I
IO
Page 3
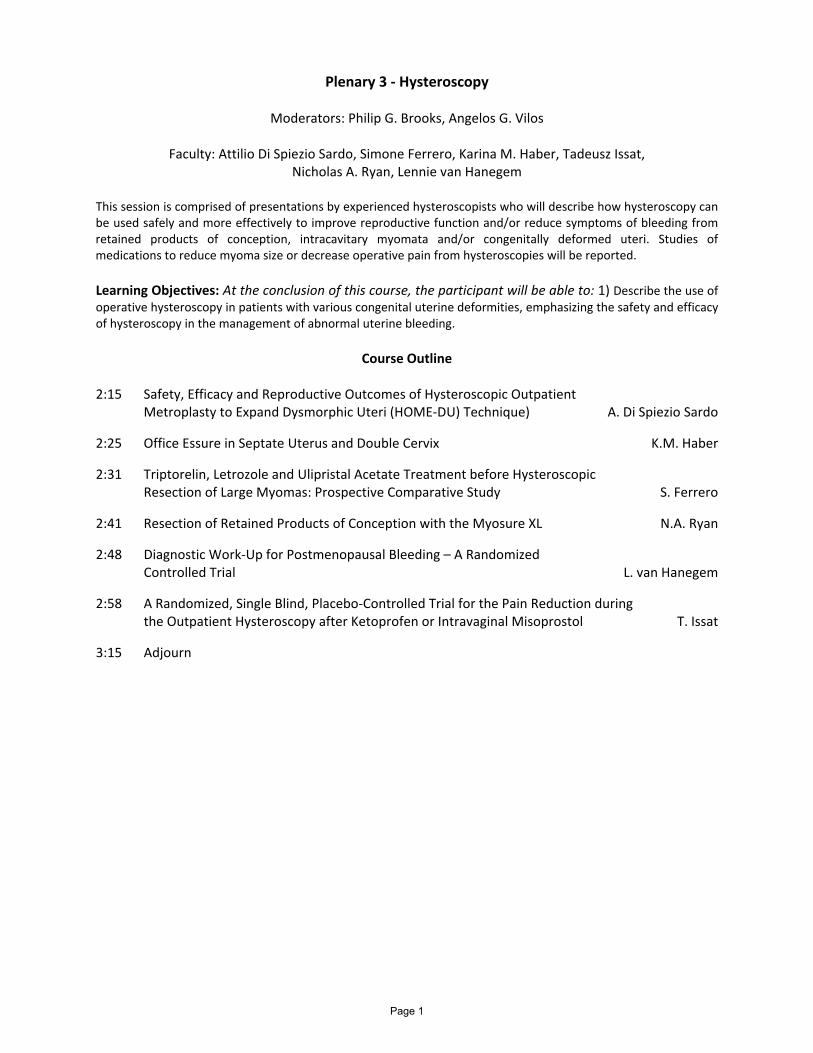
Anatomical results (1) Anatomical results (2)
Inclusion criteria Pregnancy Abortion rate
Term delivery rate
Live birth rate
Primaryinfertility (n=22)
12/22
(54%)
3/12
(25%)
9/12
(75%)
9/12
(75%)
Repeated earlyabortions ( 2)
(n=7)
5/7
(71%)
2/5
(40%)
2/5
(40%)
3/5
(60%)
Preterm delivery
(n=1)
0/1
(0,0%)
- - -
Total
(n=30)
17/30
(56%)
5/17
(29.4%)
11/17*
(64,7%)
12/17
(70.6%)
*only 1 case of preterm delivery (5,9%)
Functional results Perspectives
Further studies with a control group managed expectantly
Improvement of the uterine cavity morphology/volume vsendometrial injury
HOME-DU vs standard technique
Relevance of anti-adhesions treatment
The real voyage of discoveryconsists not in seeking newlandscapes, but having new
eyes
Proust
Page 4

Office Essure in Uterine Didelphys
Karina Haber, M.D.
Montefiore Medical Center, Bronx, New York
Study Objective: To show a unique case of office essure placement in a patient with a double vagina,
double cervix, and uterine didelphys.
Design: Step‐by‐step explanation of the technique using educative video.
Setting: Müllerian duct anomalies (MDA’s) occur in approximately 1% of the general population and are
associated with uterine, cervical, and vaginal abnormalities. Office based hysteroscopic sterilization has
been shown to be a well tolerated in women with normal female anatomy and has been concluded to
be good option for those who desire permanent sterility. In women with MDA’s, office hysteroscopy can
be used to confirm anatomical variations. In experienced hands, office based hysteroscopic sterilization
should be considered as a feasible option in women with a double vagina, double cervix, and/or uterine
anomalies.
Interventions: Office hysteroscopic placement of Essure device in a woman with a rare MDA and desires
permanent sterilization.
Conclusions: This technique of office‐based hysteroscopic sterilization is a reasonable choice for women
with Müllerian duct anomalies.
Page 5
TRIPTORELIN, LETROZOLE AND ULIPRISTAL ACETATE TREATMENT
BEFORE HYSTEROSCOPIC RESECTION OF LARGE MYOMAS: PROSPECTIVE
COMPARATIVE STUDY
Simone Ferrero, MD, PhD
Department of Obstetrics and Gynecology, San Martino Hospital and National
Institute for Cancer Research, University of GenoaItaly
AUTHORS’ DISCLOSURE
I have no financial relationships to disclose
OBJECTIVES OF THE STUDY
- Primary objective: to investigate the usefulness of preoperativetreatment with triptorelin (gonadotropin releasing hormoneagonist), letrozole (aromatase inhibitor) and ulipristal acetate(selective progesterone receptor modulator) in patientsundergoing hysteroscopic removal of large uterine submucosalmyomas (20-35 mm)
- Secondary objective: to assess the changes in myoma volumecaused by the three hormonal therapies
After this lecture, the attendee should implement the preoperativehormonal treatment prior to hysteroscopic myomectomy.
BACKGROUND
• Hysteroscopic resection is the standard treatment of submucosalmyomas.
• Contradictory results have been reported on the usefulness ofpreoperative administration of gonadotropin releasing hormone agonistsprior to hysteroscopic myomectomy (Muzii et al., 2010; Mavrelos et al.,2010; Kamath et al., 2014).
• Letrozole (a non-steroidal aromatase inhibitor) and ulipristal acetate (aselective progesterone-receptor modulator) have been used to decreasethe volume of uterine myomas and control uterine bleeding (Gurates etal., 2008; Parsanezhad et al., 2010; Donnez et al., 2012; Duhan et al.,2013; Song et al., 2013; Leone Roberti Maggiore et al., 2014; Donnezet al., 2014).
MATERIALS AND METHODS
Study design: single center prospective non-randomized comparative study
Study patients underwent either direct surgery (group S) or received a 3-month preoperative treatment with one of the following drugs:
- triptorelin (3.75 mg intramuscular injection every 28 days; group T)
- letrozole (2.5 mg/day; group L) *
- ulipristal acetate (5 mg/day; group U)* Letrozole is not approved for the treatment of uterine myomas by the FDA and Italian Ministry of Health and, therefore, the use of these drugs should be considered experimental
The choice of treatment was not randomized; treatment allocation was decided on the basis of the preference of the patients. Patients were informed in details on the potential adverse effects and on the cost of treatment.
Inclusion criteria:
- premenopausal age
- myomas graded as type 0, type 1 or type 2 according to the FIGO classification (Munro et al., 2011) with diameter between 20 and 35 mm
Exclusion criteria:
- associated polyps
- associated non-hysteroscopic surgical procedures
- > 2 myomas requiring hysteroscopic resection
Page 6

Evaluation of myomas
• the largest diameter and volume of the submucosal myomas (VOCAL, GE Healthcare, Milwaukee, WI, USA) were assessed by transvaginal ultrasonography
• office diagnostic hysteroscopy was performed to verify that the characteristics of the myomas were compatible with the inclusion criteria of the study
• on the day of surgery, a second transvaginal ultrasonography was performed to evaluate the changes in volume of the myomas in the groups receiving preoperative medical treatments
Hysteroscopic resection of the myomas
• the procedures were performed under general anesthesia in a day-surgery setting
• two skilled senior gynecologic endoscopists performed the procedures
• the procedures were performed in the early follicular phase in patients included in group S and in the last week of treatment in patients included in the other study groups
• hysteroscopic resection was performed by the slicing technique using a continuous flow 8.5 mm 12° resectoscope with bipolar 24 Fr loop 0.2 mm wire electrodes (Olympus, Hamburg, Germany)
• intraoperative ultrasonography was used when required
Surgical outcomes
• Operative time, calculated from the introduction up to the extraction of the resectoscope
• Total surgical time, calculated from the dilatation of the cervical canal up to the complete extraction of the myomas
• Absorbed fluid, calculated by subtracting the fluid collected from the total fluid instilled
• Intraoperative and postoperative complications
• Operative difficulty, evaluated by surgeons using a 10-point linear visual analog scale (VAS)
• Postoperative patient pain and satisfaction, evaluated 5 hours after surgery by using two VAS scales
• Completeness of resection, assessed by ultrasonography performed and follow-up consultations (at 1 and 3 months from surgery)
Statistical analysis
• An interim-analysis was performed and the results are presented in the current study
• The chi-squared test was used to compare categorical variables
• The one way analysis of variance was used to compare normally distributed continuous variables between the four study groups; the Holm-Sidak method was used to perform pairwise multiple comparisons. The Kruskal-Wallis one-way analysis of variance on ranks was used for the comparison of continuous variable that were not normally distributed; the Dunn’s method was used to perform multiple comparisons
• Data were analyzed with SPSS software version 20.0 (SPSS Inc., Chicago, IL)
• A p < .05 was considered statistically significant.
RESULTS
FLOW CHART SHOWING RECRUITMENT AND WOMEN’S PROGRESS THROUGH THE STUDY
Group S(n = 23)
Group T(n = 20)
Group L(n = 11)
Group U(n = 7)
p Total(n = 61)
Age (years, mean ± SD) 35.0 ± 4.7 36.3 ± 5.4 36.8 ± 5.1 38.4 ± 4.3 .419 36.1 ± 5.0
Nulliparous (n,%) 7 (30.4%) 5 (25.0%) 3 (27.3%) 2 (28.6%) .984 17 (27.9%)
Abnormal uterine bleeding (n, %) * 16 (69.6%) 14 (70.0%) 7 (63.6%) 5 (71.4) .981 42 (68.9%)
Infertility (n, %) * 8 (34.8%) 5 (25.5%) 0 (0.0%) 1 (14.3%) .142 14 (23.0%)
Miscarriage (n, %) * 4 (17.4%) 1 (5.0%) 2 (18.2%) 0 (0.0%) .390 7 (11.5%)
Diameter of the largest myoma (cm, mean ± SD) 2.7 ± 0.5 2.8 ± 0.4 3.0 ± 0.4 2.9 ± 0.3 .254 2.8 ± 0.4
Volume of the largest myoma (cm3, mean ± SD) 7.4 ± 3.5 7.2 ± 3.2 8.0 ± 3.2 8.6 ± 2.4 .722 7.6 ± 3.2
Number of myomas (n, median, range) 1 (1-2) 1 (1-2) 1 (1-2) 1 (1-2) .900 1 (1-2)
Total myoma volume (cm3, mean ± SD) 8.8 ± 3.7 8.4 ± 3.9 9.8 ± 5.9 9.7 ± 3.6 .783 8.9 ± 4.1
* Sometimes more than one for the same patient
DEMOGRAPHIC AND CLINICAL CHARACTERISTICS OF THE STUDY POPULATION
All medical treatments caused a significant decrease in the volume of the largest myoma(group T, p < .001; group L, p < .001; group U, p = .006)
The percentage decrease in myoma volume was lower in group U (-21.0%) than in groupT (-37.1%; p = .001) and in group L (-34.5%; p = .010)
CHANGES IN THE VOLUME OF THE LARGEST MYOMA CAUSE BY 3-MONTH HORMONAL TREATMENT
OPERATIVE RESULTS
Group S(n = 23)
Group T(n = 20)
Group L(n = 11)
Group U(n = 7)
p Pairwise multiple comparison procedures
Operative time (minutes, mean ± SD) 29.7 ± 8.6 21.1 ± 6.4 20.9 ± 5.5 25.89 ± 3.0 < .001 p < .001 group S vsgroup T;
p < .001 group S vsgroup L *
Total surgical time (minutes, mean ±SD)
36.7 ± 8.4 26.4 ± 6.4 26.1 ± 5.5 31.1 ± 4.4 < .001 p < .001 group S vsgroup T;
p < .001 group S vsgroup L *
Volume of fluid infused during hysteroscopy (l, mean ± SD)
7.9 ± 2.5 6.2 ± 2.0 5.4 ± 2.0 7.2 ± 2.6 .017 .004 group S vs group L
Volume of fluid absorbed (ml, mean ±SD)
457 ± 139 340 ± 112 366 ± 111 371 ± 103 .019 p = .003 group S vsgroup T;
p = .048 group S vsgroup L *
Operative difficulty (VAS, median, range)
3.6
(1.2-6.5)
2.0
(1.0-4.3)
1.9
(0.7-5.7)
2.8
(0.79-6.6)
.004 p < .05 group S vsgroup T ^
Incomplete resection (n,%) 1 (4.3%) 0 (0.0%) 0 (0.0%) 0 (0.0%) .641
* Holm-Sidak method; ^ Dunn’s method
There was no case of uterine perforation or fluid overload.
Postoperative patient pain was minimal and non significantly different among the four study groups (p = .538).
Similarly, patient satisfaction was similar in the four study groups (p = .762).
Page 7

DISCUSSION
• Preoperative treatment with triptorelin and letrozole facilitates the hysteroscopic resection of large uterine submucosal myomas by decreasing the operative time and the volume of fluid absorbed.
• The surgical advantages of preoperative hormonal therapies should be balanced with the incidence of adverse effects and with the cost of treatments.
• The operative results obtained in group S demonstrate that hysteroscopic myomectomy can be safely performed in most of the patients without the administration of preoperative hormonal treatment.
• In selected cases with multiple myomas or in case of procedures performed by less experienced surgeons, the shrinking of the myomas may allow to perform hysteroscopic procedures in patients that would be candidate to more invasive surgical techniques or to obtain a complete myoma resection during a single surgical procedure.
DISCUSSION
LIMITATIONS OF THE STUDY:
- the study was not randomized, it is likely that economical issues and knowledge of thepotential adverse effects of treatment influenced the choice of the patients
- the different mode of drug administration
- the small number of patients assigned to treatment with letrozole and ulipristal acetate
- the surgeons performing hysteroscopy were not blinded to the treatment received by thepatients
FUTURE RESEARCH:
- to evaluate the efficacy of ulipristal acetate in the treatment of submucosal uterinemyomas
- to compare in randomized study with larger sample size the efficacy of treatment withletrozole and triptorelin prior to hysteroscopic resection of large submucosal myomas
- to assess the role of preoperative hormonal therapies in patients with > 2 large FIGOtype 2 myomas that are currently treated by multiple hysteroscopic procedures or bymore invasive surgical techniques
• Donnez J, Tatarchuk TF, Bouchard P, et al. Ulipristal acetate versus placebo for fibroid treatment before surgery. N Engl J Med.2012;366:409-20.
• Donnez J, Tomaszewski J, Vázquez F, et al. Ulipristal acetate versus leuprolide acetate for uterine fibroids. N Engl J Med.2012;366:421-32.
• Donnez J, Vazquez F, Tomaszewski J, et al. Long-term treatment of uterine fibroids with ulipristal acetate. Fertil Steril.2014;101:1565-73.
• Duhan N, Madaan S, Sen J. Role of the aromatase inhibitor letrozole in the management of uterine leiomyomas in premenopausalwomen. Eur J Obstet Gynecol Reprod Biol. 2013;171:329-32.
• Gurates B, Parmaksiz C, Kilic G, et al. Treatment of symptomatic uterine leiomyoma with letrozole. Reprod Biomed Online.2008;17:569-74.
• Kamath MS, Kalampokas EE, Kalampokas TE. Use of GnRH analogues pre-operatively for hysteroscopic resection of submucousfibroids: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2014;177:11-8.
• Leone Roberti Maggiore U, Scala C, Venturini PL, et al. Preoperative treatment with letrozole in patients undergoing laparoscopicmyomectomy of large uterine myomas: a prospective non-randomized study. Eur J Obstet Gynecol Reprod Biol. 2014;181C:157-162.
• Muzii L, Boni T, Bellati F, et al. GnRH analogue treatment before hysteroscopic resection of submucous myomas: a prospective,randomized, multicenter study. Fertil Steril. 2010;94:1496-9.
• Mavrelos D, Ben-Nagi J, Davies A, et al. The value of preoperative treatment with GnRH analogues in women with submucousfibroids: a double-blind, placebo-controlled randomized trial. Hum Reprod. 2010;25:2264-9.
• Munro MG, Critchley HO, Fraser IS; FIGO Menstrual Disorders Working Group. The FIGO classification of causes of abnormaluterine bleeding in the reproductive years. Fertil Steril. 2011;95:2204-8.
• Parsanezhad ME, Azmoon M, Alborzi S, et al. A randomized, controlled clinical trial comparing the effects of aromatase inhibitor(letrozole) and gonadotropin-releasing hormone agonist (triptorelin) on uterine leiomyoma volume and hormonal status. FertilSteril. 2010;93:192-8.
• Song H, Lu D, Navaratnam K, et al. Aromatase inhibitors for uterine fibroids. Cochrane Database Syst Rev. 2013;10:CD009505.
REFERENCES
Page 8

Resection of Retained Products of Conception with the Myosure XL
Nicholas Ryan, MD
Baylor College of Medicine, Houston, Texas
Study Objective: To demonstrate a novel technique for resection of retained products of conception
using the MyoSure XL® (Hologic, Bedford, MA) device.
Design: Step‐by‐step explanation of the technique using video.
Setting: A 33 year old G2P1001 had a missed abortion at approximately 10 weeks gestation and
underwent a dilatation and suction curettage at an outlying hospital. The procedure was complicated by
a 2 liter blood loss that required transfusion. She presented two weeks later with recurrent vaginal
bleeding. Ultrasound confirmed retained products of conception with a possible arteriovenous
malformation. Hematocrit at this time was 23.1%. She underwent bilateral uterine artery embolization
(UAE) using Gelfoam® (Pfizer, New York, NY). Ten days following UAE, she underwent hysteroscopic
resection of the retained products of conception using the MyoSure XL device.
Interventions: Hysteroscopic resection of retained products of conception using the MyoSure XL device.
Conclusions: In certain circumstances, retained products of conception following dilatation and
curettage can be safely and effectively resected under direct visualization using the MyoSure XL device.
This technique could theoretically reduce the likelihood of perforation, confirm complete removal of the
lesion, and facilitate minimal dissection into the myometrium and disruption of the opposing uterine
walls to effectively reduce the risk of Asherman’s syndrome.
Keywords: Retained products of conception; Operative hysteroscopy; MyoSure XL
Page 9
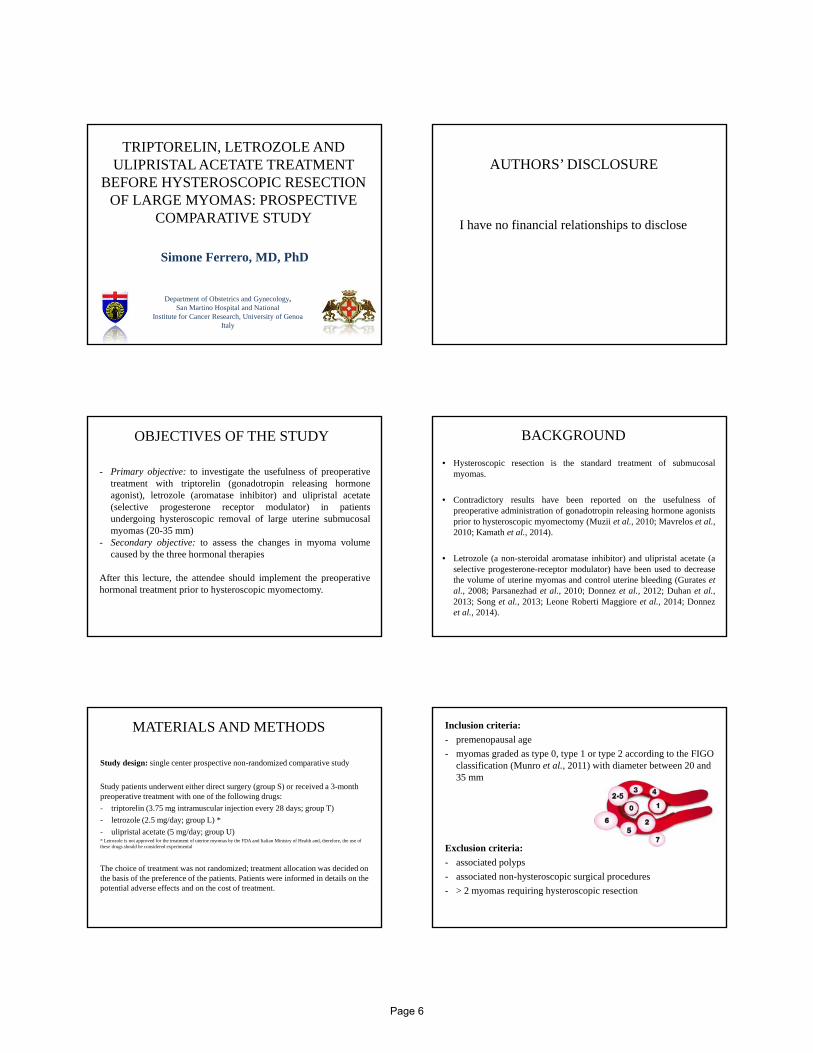
Diagnostic work-up for postmenopausal bleeding
a randomized clinical trial
N. van Hanegem, MDMaastricht UMC+
The Netherlands
Disclosures
I have no financial relationships to disclose.
How to handle a patient with:
• a first episode of postmenopausal bleeding• an endometrial thickness of > 4 mm and • a benign histology after endometrial sampling.
Learning objectives Diagnostic work-up PMP bleeding1,2,3
Vaginal examination, Cervical cytology and TVS
Endometrium > 4 mm or non-measurable
Endometrialbiopsy
Benign histology
??
Insufficientsample
Hysteroscopy
(Pre)malignancy
Treatment
Endometrium ≤ 4 mm
Expectantmanagement
Recurrentbleeding
Histology(hysteroscopy)
• Regardless of endometrial thickness4,5:• No abnormalities 50%• Endometrial carcinoma 10%• Endometrial polyp 20%
• Sensitivity endometrial biopsy for endometrial cancer: 92-95%6,7
• Endometrial thickness > 4 mm8,9:• 40% endometrial polyps• No evidence that removal of polyps can reduce
recurrent bleeding
Patients with postmenopausal bleeding
Does further work-up for and treatment of benign endometrial lesions reduce the risk of recurrent
postmenopausal bleeding?
Scientific question
Page 10

Randomized clinical trial
P Women with postmenopausal bleeding
I Hysteroscopy
C Expectant management
O Recurrent bleeding within 1 year• Recurrent bleeding > 1 year• (Pre)malignancy
Study designInclusioncriteria: •Postmenopausal bleeding•Double endometrial thickness > 4 mm•Benign histology after endometrial biopsy
Exclusioncriteria:•Abnormal cervical cytology•Aromatase-inhibitor/anti-estrogen
Sample size: 50% reduction of recurrent bleeding (drop-out rate 20%; power 80%; α 5%)
N=200
Methods
Intervention:• Diagnostic hysteroscopy. In case of an
endometrial polyp, polypectomy was performed.
Comparison:• No further diagnostic work-up.
All patients were instructed to contact theoutpatient clinic in case of recurrent bleeding andcontacted for follow-up after 1 year.
Methods: Allocation Results: flow chart
200 women included
98 hysteroscopy 87 received assigned intervention
102 exp managementnobody had hysteroscopy
2 lost to follow-up 7 follow-up ongoing
3 follow-up ongoing
95 included in analysesMedian follow up 60 weeks
93 included in analysesMedian follow up 63 weeks
RR 0.91 (95% CI 0.63-1.3)
Results: Recurrent bleeding < 1 year
Recurrent bleeding
No recurrent bleeding
Hysteroscopy 14 (14%) 84 98
Expectantmanagement
16 (17%) 77 93
30 161 191
87 of 98 women received allocated intervention.
Results: (pre)malignancy in hysteroscopy-group
Hysteroscopy N=87Hysteroscopy N=87
Polyp N=46Polyp N=46
Benign N=38
Benign N=38
Hyperplasia+atypiaN=5
Hyperplasia+atypiaN=5
HysterectomyHysterectomy
Hyperplasia+atypiaN=3
Hyperplasia+atypiaN=3
CarcinomaN=2
CarcinomaN=2
Carcinoma N=1Carcinoma N=1No result
N=2No result
N=2
No polyp N=41No polyp N=41
Page 11
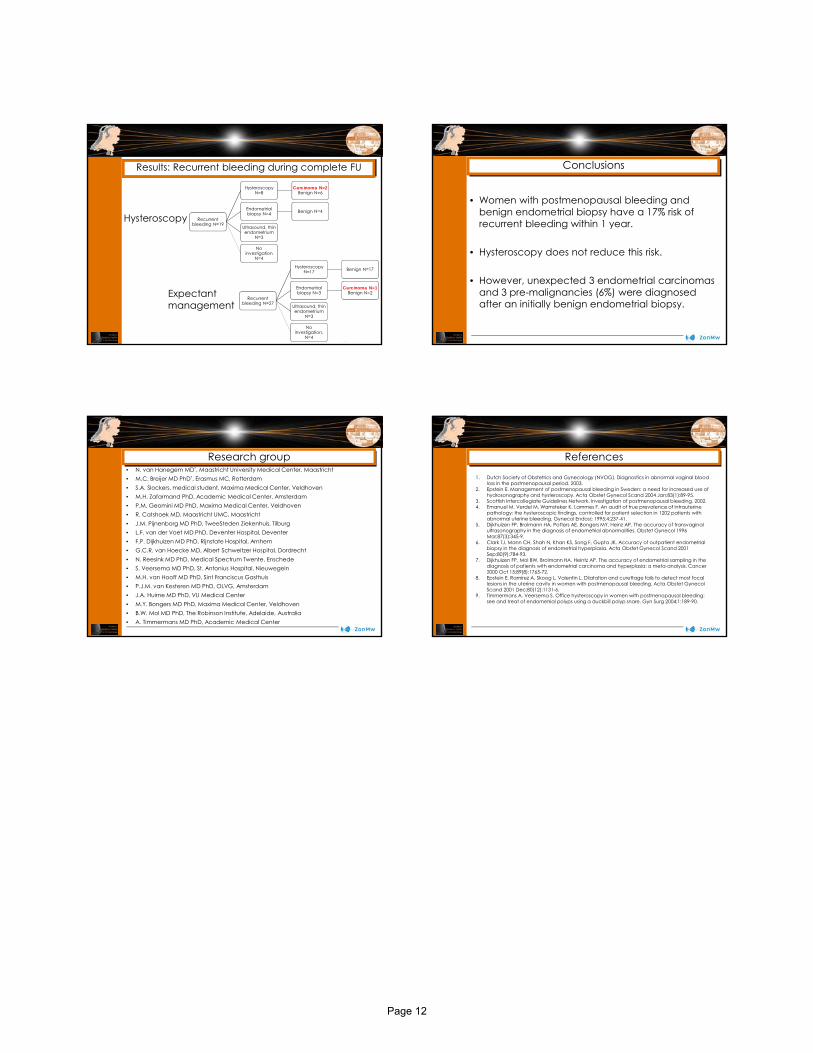
Results: Recurrent bleeding during complete FU
Hysteroscopy
Recurrentbleeding N=27
HysteroscopyN=17 Benign N=17
Endometrialbiopsy N=3
Carcinoma N=1 Benign N=2
Ultrasound, thinendometrium
N=3
No investigation,
N=4
Expectant management
Recurrentbleeding N=19
HysteroscopyN=8
Carcinoma N=2 Benign N=6
Endometrialbiopsy N=4 Benign N=4
Ultrasound, thinendometrium
N=3
No investigation
N=4
• Women with postmenopausal bleeding and benign endometrial biopsy have a 17% risk of recurrent bleeding within 1 year.
• Hysteroscopy does not reduce this risk.
• However, unexpected 3 endometrial carcinomas and 3 pre-malignancies (6%) were diagnosed after an initially benign endometrial biopsy.
Conclusions
Research group• N. van Hanegem MD*, Maastricht University Medical Center, Maastricht• M.C. Breijer MD PhD*, Erasmus MC, Rotterdam• S.A. Slockers, medical student, Maxima Medical Center, Veldhoven• M.H. Zafarmand PhD, Academic Medical Center, Amsterdam• P.M. Geomini MD PhD, Maxima Medical Center, Veldhoven• R. Catshoek MD, Maastricht UMC, Maastricht• J.M. Pijnenborg MD PhD, TweeSteden Ziekenhuis, Tilburg• L.F. van der Voet MD PhD, Deventer Hospital, Deventer• F.P. Dijkhuizen MD PhD, Rijnstate Hospital, Arnhem• G.C.R. van Hoecke MD, Albert Schweitzer Hospital, Dordrecht• N. Reesink MD PhD, Medical Spectrum Twente, Enschede• S. Veersema MD PhD, St. Antonius Hospital, Nieuwegein• M.H. van Hooff MD PhD, Sint Franciscus Gasthuis• P.J.M. van Kesteren MD PhD, OLVG, Amsterdam• J.A. Huirne MD PhD, VU Medical Center• M.Y. Bongers MD PhD, Maxima Medical Center, Veldhoven• B.W. Mol MD PhD, The Robinson Institute, Adelaide, Australia• A. Timmermans MD PhD, Academic Medical Center
References
1. Dutch Society of Obstetrics and Gynecology (NVOG). Diagnostics in abnormal vaginal blood loss in the postmenopausal period. 2003.
2. Epstein E. Management of postmenopausal bleeding in Sweden: a need for increased use of hydrosonography and hysteroscopy. Acta Obstet Gynecol Scand 2004 Jan;83(1):89-95.
3. Scottish Intercollegiate Guidelines Network. Investigation of postmenopausal bleeding. 2002. 4. Emanuel M, Verdel M, Wamsteker K, Lammes F. An audit of true prevalence of intrauterine
pathology: the hysteroscopic findings, controlled for patient selection in 1202 patients with abnormal uterine bleeding. Gynecol Endosc 1995;4:237-41.
5. Dijkhuizen FP, Brolmann HA, Potters AE, Bongers MY, Heinz AP. The accuracy of transvaginal ultrasonography in the diagnosis of endometrial abnormalities. Obstet Gynecol 1996 Mar;87(3):345-9.
6. Clark TJ, Mann CH, Shah N, Khan KS, Song F, Gupta JK. Accuracy of outpatient endometrial biopsy in the diagnosis of endometrial hyperplasia. Acta Obstet Gynecol Scand 2001 Sep;80(9):784-93.
7. Dijkhuizen FP, Mol BW, Brolmann HA, Heintz AP. The accuracy of endometrial sampling in the diagnosis of patients with endometrial carcinoma and hyperplasia: a meta-analysis. Cancer 2000 Oct 15;89(8):1765-72.
8. Epstein E, Ramirez A, Skoog L, Valentin L. Dilatation and curettage fails to detect most focal lesions in the uterine cavity in women with postmenopausal bleeding. Acta Obstet GynecolScand 2001 Dec;80(12):1131-6.
9. Timmermans A, Veersema S. Office hysteroscopy in women with postmenopausal bleeding: see and treat of endometrial polyps using a duckbill polyp snare. Gyn Surg 2004;1:189-90.
Page 12

A randomized, single blind, placebo-controlled trial for the pain reduction
during the outpatient hysteroscopy after Ketoprofen or intravaginal Misoprostol
Tadeusz Issat, MD, PhD
Department of Reproductive Health, Institute of Mother and Child Warsaw, Poland
DisclosureI have no financial relationships to disclose.
Known factors that might reduce pain during office hysteroscopy
Pain reduction
Lidocaine gel
Tramadol iv.
Transcutaneous electrical nerve
stimulation
Intrauterine and intracervical
lidocaine
Sublingual buprenorphine
Reduction inwaiting time for
procedure
Guidelines
„..RCOG: women withoutcontraindications shouldbe advised to considertaking standard doses ofnon-steroidal anti-inflammatory agents(NSAIDs) around 1 hourbefore their scheduledoutpatient hysteroscopyappointment with the aimof reducing pain in theimmediate postoperativeperiod.. .”
Study design
RCTMisoprostol arm:
vaginal Misoprostol (400 μg) and 100 ml of 5% intravenous
glucose
Ketoprofen arm: iv Ketoprofen
(50mg/1ml) in 100 ml of 5% glucose and intravaginal
placebo
Placebo arm: intravaginal
placebo and 100ml of 5% iv glucose
Aim of the study was to assess the pain during and after outpatient hysteroscopy, depending on the use of intravaginal Misoprostol (400 μg), intravenous non-steroidal
anti-inflammatory agent Ketoprofen (1mg/1ml) or placebo
Inclusion and exclusion criteria
• aged over 18
• agreed to participate in the study and a written informed consent was obtained
• indications for office hysteroscopy
• women with a possible pregnancy
• lower genital tract infections • gestational trophoblastic disease • presence of endocervical polyps • asthma• acute porphyria • hepatitis • renal failure• lactation • oversensitivity to one of the
agents endometrial polyps measuring more than 30mm
Inclusion criteria Exclusion criteria
Page 13
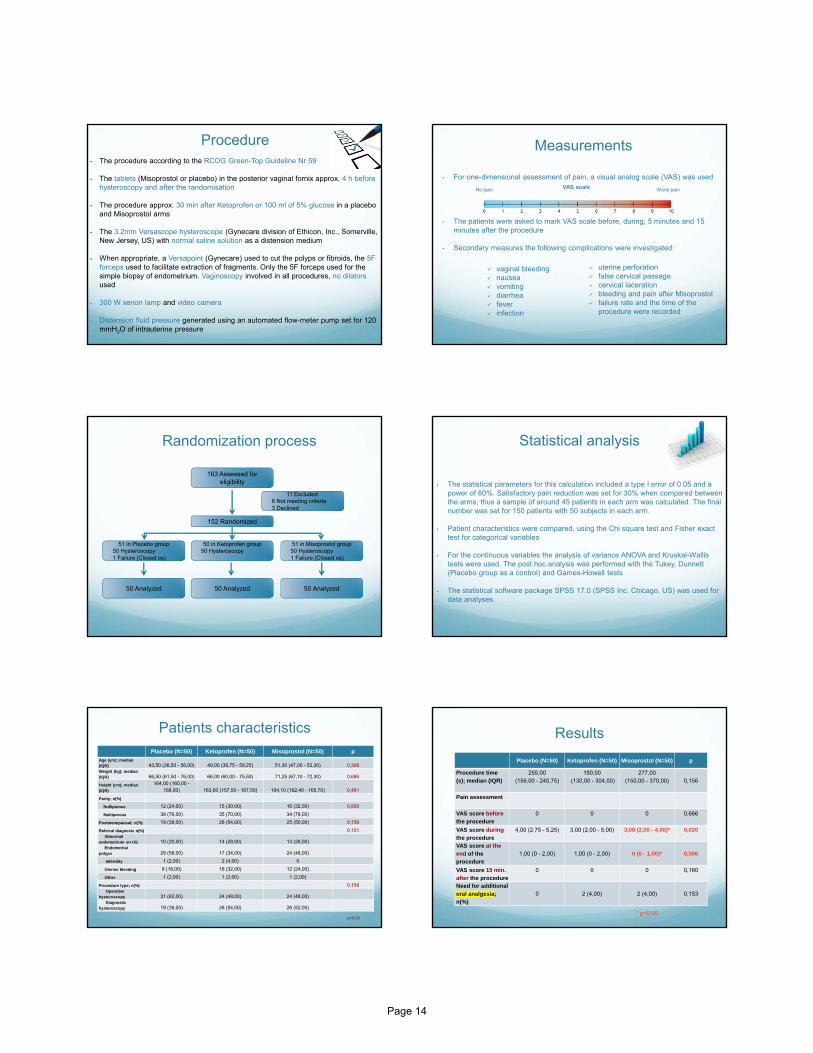
Procedure• The procedure according to the RCOG Green-Top Guideline Nr 59
• The tablets (Misoprostol or placebo) in the posterior vaginal fornix approx. 4 h before hysteroscopy and after the randomisation
• The procedure approx. 30 min after Ketoprofen or 100 ml of 5% glucose in a placebo and Misoprostol arms
• The 3.2mm Versascope hysteroscope (Gynecare division of Ethicon, Inc., Somerville, New Jersey, US) with normal saline solution as a distension medium
• When appropriate, a Versapoint (Gynecare) used to cut the polyps or fibroids, the 5F forceps used to facilitate extraction of fragments. Only the 5F forceps used for the simple biopsy of endometrium. Vaginoscopy involved in all procedures, no dilators used
• 300 W xenon lamp and video camera
• Distension fluid pressure generated using an automated flow-meter pump set for 120 mmH2O of intrauterine pressure
• For one-dimensional assessment of pain, a visual analog scale (VAS) was used
• The patients were asked to mark VAS scale before, during, 5 minutes and 15 minutes after the procedure
• Secondary measures the following complications were investigated:
Measurements
No pain Worst painVAS scale
uterine perforation false cervical passage cervical laceration bleeding and pain after Misoprostol failure rate and the time of the
procedure were recorded
vaginal bleeding nausea vomiting diarrhea fever infection
163 Assessed for eligibility
11 Excluded:� 8 Not meeting criteria� 3 Declined
152 Randomized
50 Analyzed
51 in Misoprostol group� 50 Hysteroscopy� 1 Failure (Closed os)
50 in Ketoprofen group� 50 Hysteroscopy
51 in Placebo group� 50 Hysteroscopy� 1 Failure (Closed os)
50 Analyzed50 Analyzed
Randomization process Statistical analysis
• The statistical parameters for this calculation included a type I error of 0.05 and a power of 80%. Satisfactory pain reduction was set for 30% when compared between the arms, thus a sample of around 45 patients in each arm was calculated. The final number was set for 150 patients with 50 subjects in each arm.
• Patient characteristics were compared, using the Chi square test and Fisher exact test for categorical variables
• For the continuous variables the analysis of variance ANOVA and Kruskal-Wallis tests were used. The post hoc analysis was performed with the Tukey, Dunnett(Placebo group as a control) and Games-Howell tests
• The statistical software package SPSS 17.0 (SPSS Inc. Chicago, US) was used for data analyses.
Patients characteristics
Placebo (N=50) Ketoprofen (N=50) Misoprostol (N=50) p
Age (yrs); median (IQR) 43,50 (36,50 - 56,00) 49,00 (39,75 - 59,25) 51,30 (47,00 - 52,30) 0,398Weight (kg); median (IQR) 66,50 (61,50 - 76,00) 66,00 (60,00 - 75,50) 71,25 (67,10 - 72,30) 0,686
Height (cm); median (IQR)
164,00 (160,00 -168,00) 163,00 (157,50 - 167,50) 164,10 (162,40 - 165,70) 0,481
Parity; n(%)
Nulliparous 12 (24,00) 15 (30,00) 16 (32,00) 0,890
Multiparous 38 (76,00) 35 (70,00) 34 (78,00)
Postmenopausal; n(%) 19 (38,00) 26 (54,00) 25 (50,00) 0,159
Referral diagnosis n(%) 0,151Abnormal
endometrium on US 10 (20,00) 14 (28,00) 13 (26,00)Endometrial
polyps 29 (58,00) 17 (34,00) 24 (48,00)
Infertility 1 (2,00) 2 (4,00) 0
Uterine bleeding 9 (18,00) 16 (32,00) 12 (24,00)
Other 1 (2,00) 1 (2,00) 1 (2,00)
Procedure type; n(%) 0,159Operative
hysteroscopy 31 (62,00) 24 (48,00) 24 (48,00)Diagnostic
hysteroscopy 19 (38,00) 26 (54,00) 26 (52,00)
p>0.05
Placebo (N=50) Ketoprofen (N=50) Misoprostol (N=50) p
Procedure time (s); median (IQR)
255,00 (156,00 - 240,75)
190,00(130,00 - 304,00)
277,00 (150,00 - 370,00) 0,156
Pain assessment
VAS score before the procedure
0 0 0 0,666
VAS score during the procedure
4,00 (2,75 - 5,25) 3,00 (2,00 - 5,00) 3,00 (2,00 - 4,00)* 0,020
VAS score at the end of theprocedure
1,00 (0 - 2,00) 1,00 (0 - 2,00) 0 (0 - 1,00)* 0,006
VAS score 15 min. after the procedure
0 0 0 0,160
Need for additional oral analgesia; n(%)
0 2 (4,00) 2 (4,00) 0,153
* p<0.05
Results
Page 14

Results
The median VAS scores measured directly after the procedure
The median VAS scores measured during the procedure
Vaginal misoprostol reduces pain during and at the end of the outpatient hysteroscopy when compared to non-steroidal anti-inflammatory agents or
placebo
VAS score during and after the hysteroscopy and time of procedure
VAS scores measured during the procedure and the time
of hysteroscopy
VAS scores measured after the procedure and the time of
hysteroscopy
Objective
• 400 μg vaginal misoprostol administrated 4 hours before the procedure of outpatient hysteroscopy appears to be a better alternative to NSAID's in terms of pain reduction during and directly after the procedure.
• This observation does not depend on the patients’ age, hormonal status, parity or type of the procedure (operative or diagnostic).
Thank you
References:
• RCOG Green-top Guideline No.59 Best Practice in Outpatient Hysteroscopy March 2011 • Deffieux X, Gauthier T, Menager N, Legendre G, Agostini A, Pierre F. Hysteroscopy: guidelines for clinical
practice from the French College of Gynaecologists and Obstetricians. Eur J Obstet Gynecol Reprod Biol. 2014 Jul;178:114-22
• Van den Bosch T, Van Schoubroeck D, Daemen A, Domali E, Vandenbroucke V, De Moor B, Deprest J, Timmerman D. Lidocaine does not reduce pain perception during gel instillation sonography or subsequent office hysteroscopy: results of a randomized trial. Gynecol Obstet Invest. 2011;71(4):236-239
• Floris S, Piras B, Orrù M, Silvetti E, Tusconi A, Melis F, Tuveri M, Piga M, Paoletti AM, Melis GB. Efficacy of intravenous tramadol treatment for reducing pain during office diagnostic hysteroscopy. Fertil Steril. 2007 Jan;87(1):147-151
• De Angelis C, Perrone G, Santoro G, Nofroni I, Zichella L. Suppression of pelvic pain during hysteroscopy with a transcutaneous electrical nerve stimulation device. Fertil Steril. 2003 Jun;79(6):1422-1427.
• Munro MG, Brooks PG. Use of local anesthesia for office diagnostic and operative hysteroscopy. J Minim Invasive Gynecol. 2010 Nov-Dec;17(6):709-718
• Agdi M, Tulandi T. Outpatient hysteroscopy with combined local intracervical and intrauterine anesthesia. Gynecol Obstet Invest. 2010;69(1):30-2
• Lin YH, Hwang JL, Huang LW, Chen HJ. Use of sublingual buprenorphine for pain relief in office hysteroscopy. J Minim Invasive Gynecol. 2005 Jul-Aug;12(4):347-350.
Page 15

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
Page 16