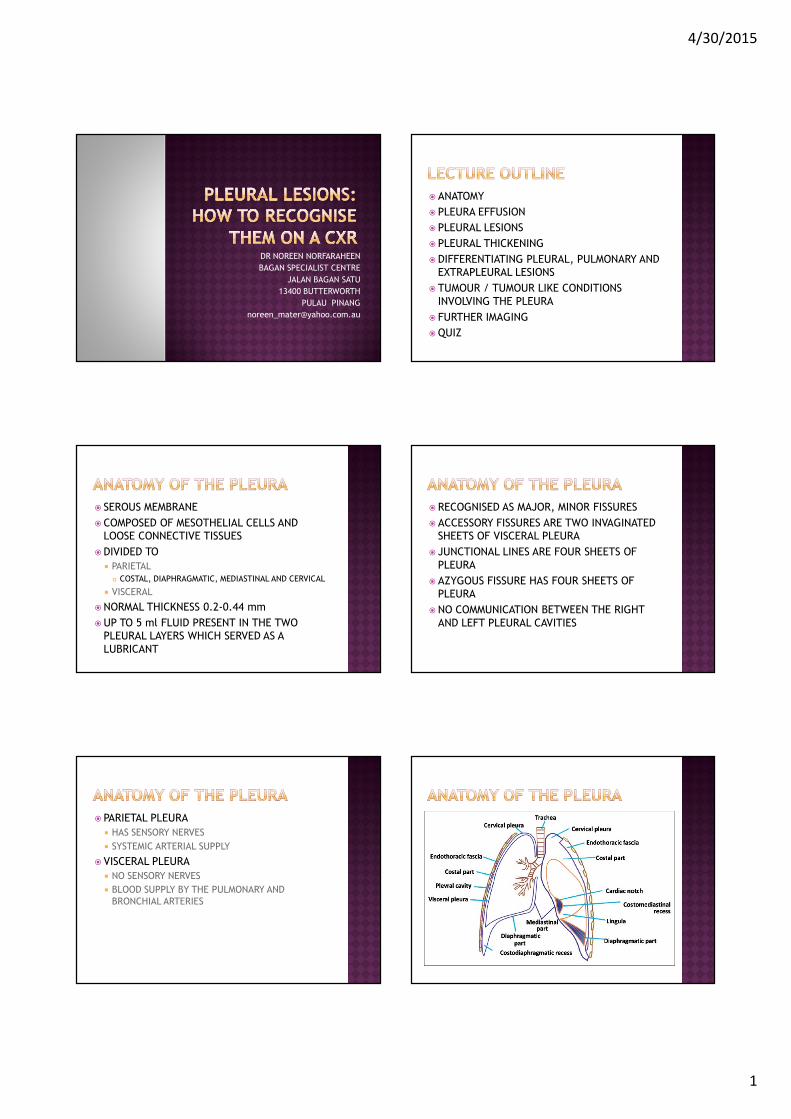
pleural lesions by dr noreen
TRANSCRIPT
4/30/2015
1
DR NOREEN NORFARAHEEN
BAGAN SPECIALIST CENTRE
JALAN BAGAN SATU
13400 BUTTERWORTH
PULAU PINANG
� ANATOMY
� PLEURA EFFUSION
� PLEURAL LESIONS
� PLEURAL THICKENING
�DIFFERENTIATING PLEURAL, PULMONARY AND
EXTRAPLEURAL LESIONS
� TUMOUR / TUMOUR LIKE CONDITIONS
INVOLVING THE PLEURA
� FURTHER IMAGING
�QUIZ
� SEROUS MEMBRANE
� COMPOSED OF MESOTHELIAL CELLS AND
LOOSE CONNECTIVE TISSUES
�DIVIDED TO
� PARIETAL
� COSTAL, DIAPHRAGMATIC, MEDIASTINAL AND CERVICAL
� VISCERAL
�NORMAL THICKNESS 0.2-0.44 mm
�UP TO 5 ml FLUID PRESENT IN THE TWO
PLEURAL LAYERS WHICH SERVED AS A
LUBRICANT
� RECOGNISED AS MAJOR, MINOR FISSURES
� ACCESSORY FISSURES ARE TWO INVAGINATED
SHEETS OF VISCERAL PLEURA
� JUNCTIONAL LINES ARE FOUR SHEETS OF
PLEURA
� AZYGOUS FISSURE HAS FOUR SHEETS OF
PLEURA
�NO COMMUNICATION BETWEEN THE RIGHT
AND LEFT PLEURAL CAVITIES
� PARIETAL PLEURA
� HAS SENSORY NERVES
� SYSTEMIC ARTERIAL SUPPLY
� VISCERAL PLEURA
� NO SENSORY NERVES
� BLOOD SUPPLY BY THE PULMONARY AND
BRONCHIAL ARTERIES
4/30/2015
2
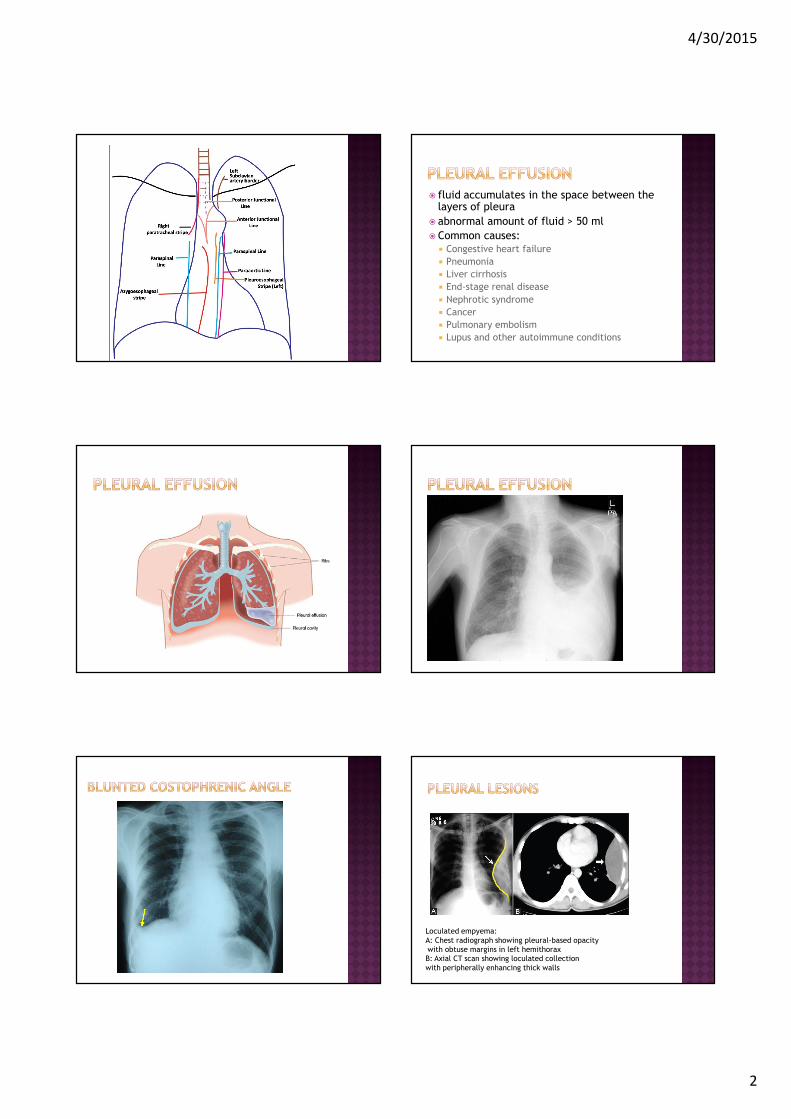
� fluid accumulates in the space between the layers of pleura
� abnormal amount of fluid > 50 ml
� Common causes:� Congestive heart failure
� Pneumonia
� Liver cirrhosis
� End-stage renal disease
� Nephrotic syndrome
� Cancer
� Pulmonary embolism
� Lupus and other autoimmune conditions
Loculated empyema:
A: Chest radiograph showing pleural-based opacity
with obtuse margins in left hemithorax
B: Axial CT scan showing loculated collection
with peripherally enhancing thick walls
4/30/2015
3
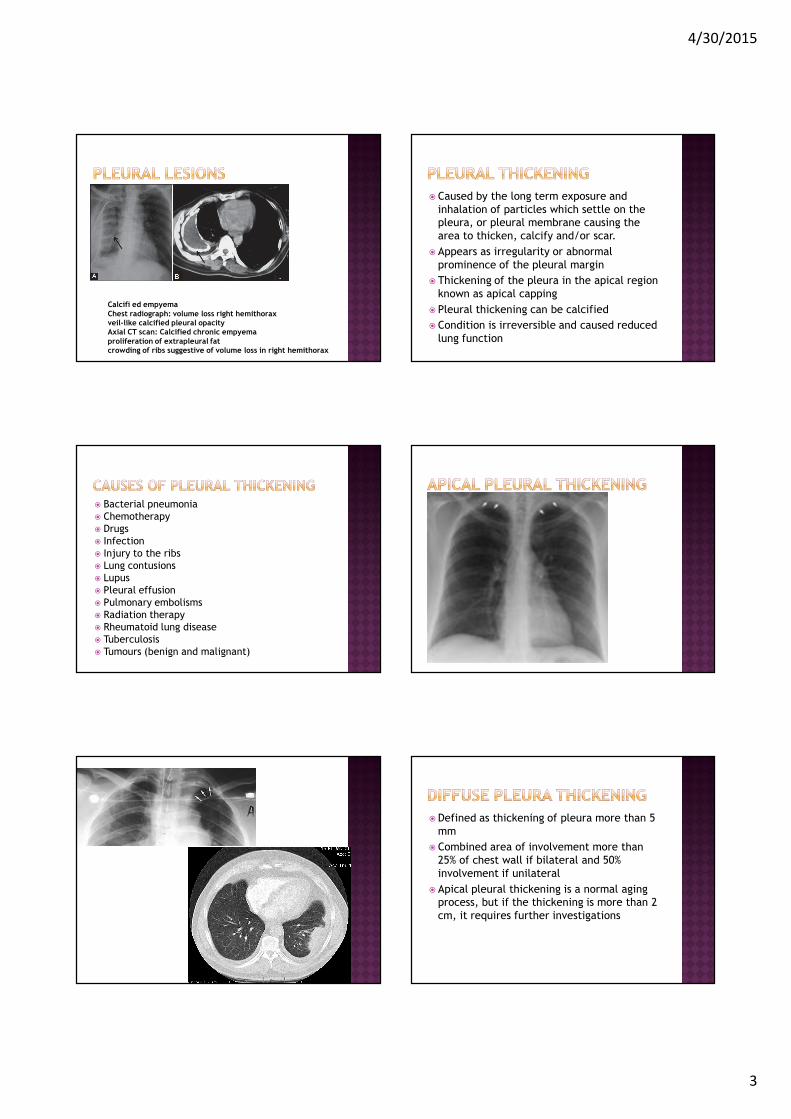
Calcifi ed empyemaChest radiograph: volume loss right hemithoraxveil-like calcified pleural opacityAxial CT scan: Calcified chronic empyemaproliferation of extrapleural fatcrowding of ribs suggestive of volume loss in right hemithorax
� Caused by the long term exposure and
inhalation of particles which settle on the
pleura, or pleural membrane causing the
area to thicken, calcify and/or scar.
� Appears as irregularity or abnormal
prominence of the pleural margin
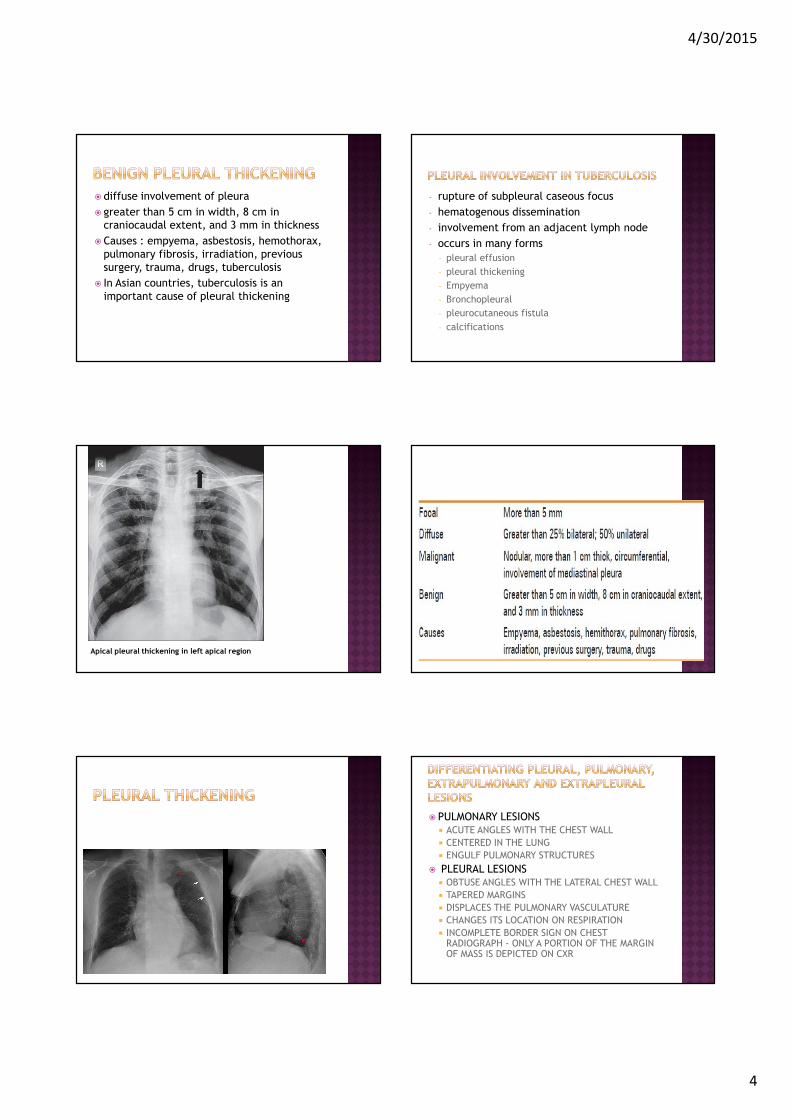
� Thickening of the pleura in the apical region
known as apical capping
� Pleural thickening can be calcified
� Condition is irreversible and caused reduced
lung function
� Bacterial pneumonia
� Chemotherapy
� Drugs
� Infection
� Injury to the ribs
� Lung contusions
� Lupus
� Pleural effusion
� Pulmonary embolisms
� Radiation therapy
� Rheumatoid lung disease
� Tuberculosis
� Tumours (benign and malignant)
�Defined as thickening of pleura more than 5
mm
� Combined area of involvement more than
25% of chest wall if bilateral and 50%
involvement if unilateral
� Apical pleural thickening is a normal aging
process, but if the thickening is more than 2
cm, it requires further investigations
4/30/2015
4
� diffuse involvement of pleura
� greater than 5 cm in width, 8 cm in
craniocaudal extent, and 3 mm in thickness
� Causes : empyema, asbestosis, hemothorax,
pulmonary fibrosis, irradiation, previous
surgery, trauma, drugs, tuberculosis
� In Asian countries, tuberculosis is an
important cause of pleural thickening
- rupture of subpleural caseous focus
- hematogenous dissemination
- involvement from an adjacent lymph node
- occurs in many forms
- pleural effusion
- pleural thickening
- Empyema
- Bronchopleural
- pleurocutaneous fistula
- calcifications
Apical pleural thickening in left apical region
� PULMONARY LESIONS� ACUTE ANGLES WITH THE CHEST WALL
� CENTERED IN THE LUNG
� ENGULF PULMONARY STRUCTURES
� PLEURAL LESIONS � OBTUSE ANGLES WITH THE LATERAL CHEST WALL
� TAPERED MARGINS
� DISPLACES THE PULMONARY VASCULATURE
� CHANGES ITS LOCATION ON RESPIRATION
� INCOMPLETE BORDER SIGN ON CHEST RADIOGRAPH - ONLY A PORTION OF THE MARGIN OF MASS IS DEPICTED ON CXR
4/30/2015
5
� EXTRAPLEURAL LESIONS
� arise from extrapleural fat, ribs, intercostal
muscles, and neurovascular bundle
� displace the extrapleural fat inward
� PLEURAL LESIONS
� do not cause erosion of ribs and displace the
extrapleural fat outward
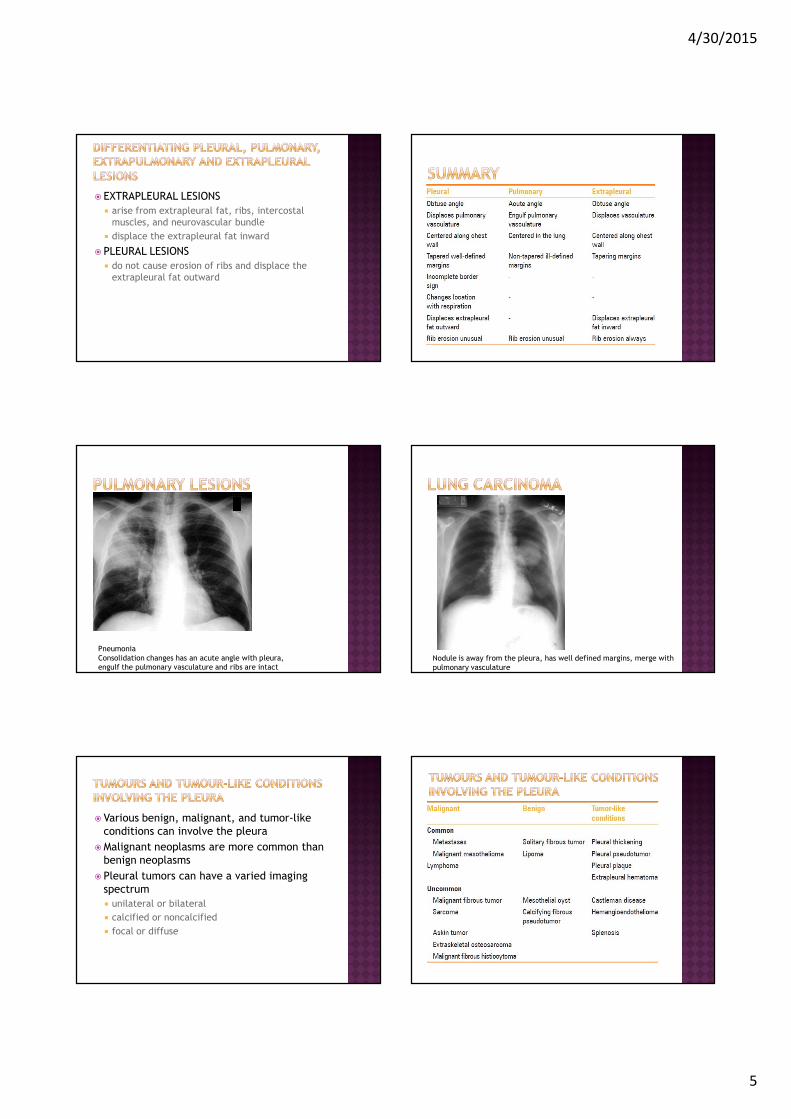
Pneumonia
Consolidation changes has an acute angle with pleura,
engulf the pulmonary vasculature and ribs are intactNodule is away from the pleura, has well defined margins, merge with
pulmonary vasculature
� Various benign, malignant, and tumor-like
conditions can involve the pleura
�Malignant neoplasms are more common than
benign neoplasms
� Pleural tumors can have a varied imaging
spectrum
� unilateral or bilateral
� calcified or noncalcified
� focal or diffuse
4/30/2015
6
� deposits of hyalinized collagen fibers in the
parietal pleura
�may be calcified or noncalcified
� on imaging, pleural plaques are seen as focal
pleural thickening
� Caused by previous exposure to asbestos
�Usually solitary
� Also known as localized fibrous tumor or
pleural mesothelioma
� age group of 45-60 years
�Mostly benign
� 20% malignant
� 80% arises from the visceral pleura
�On imaging appears as a soft tissue pleural-based neoplasm with areas of necrosis, hemorrhage, cystic changes and calcification
�Heterogeneous enhancement is seen post-contrast
�Differentiation of benign and malignant fibrous tumors is difficult on imaging
� Requires biopsy
� Features suggestive of malignancy are presence of calcification, effusion, atelectasis, mediastinal shift and chest wall invasion
� Presence of stalk suggests benign nature
� On CT, the stalk is identified as a linear soft tissue extending into the pleura/interlobar fissure/hilum
� Presence of stalk is also confirmed by change in its location on respiration
� Other clinical manifestations are clubbing, hypertrophic osteoarthropathy and hypoglycemia
� Hypoglycemia occurs as a result of the production of insulin-like growth factor II (IGF-II) by these tumors
� Hypertrophic osteoarthropathy occurs as a result of production of ectopic growth hormone-like substance and is more common with tumors greater than 7 cm
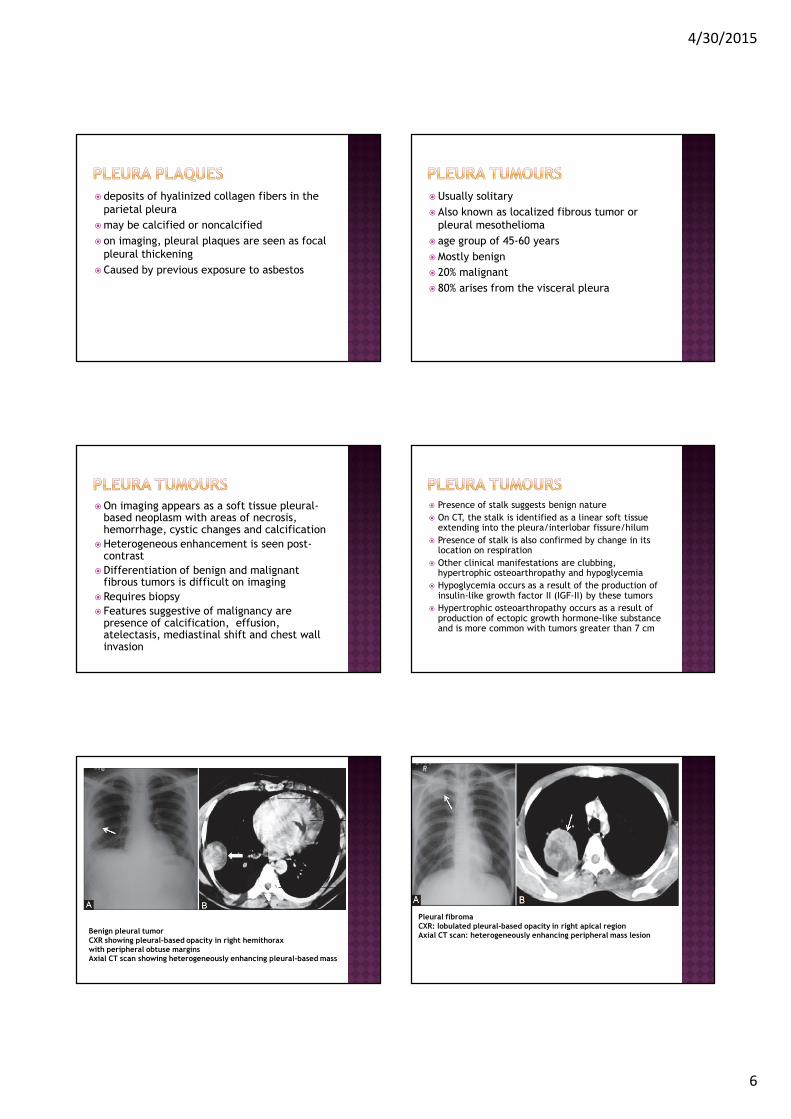
Benign pleural tumorCXR showing pleural-based opacity in right hemithoraxwith peripheral obtuse marginsAxial CT scan showing heterogeneously enhancing pleural-based mass
Pleural fibromaCXR: lobulated pleural-based opacity in right apical regionAxial CT scan: heterogeneously enhancing peripheral mass lesion
4/30/2015
7
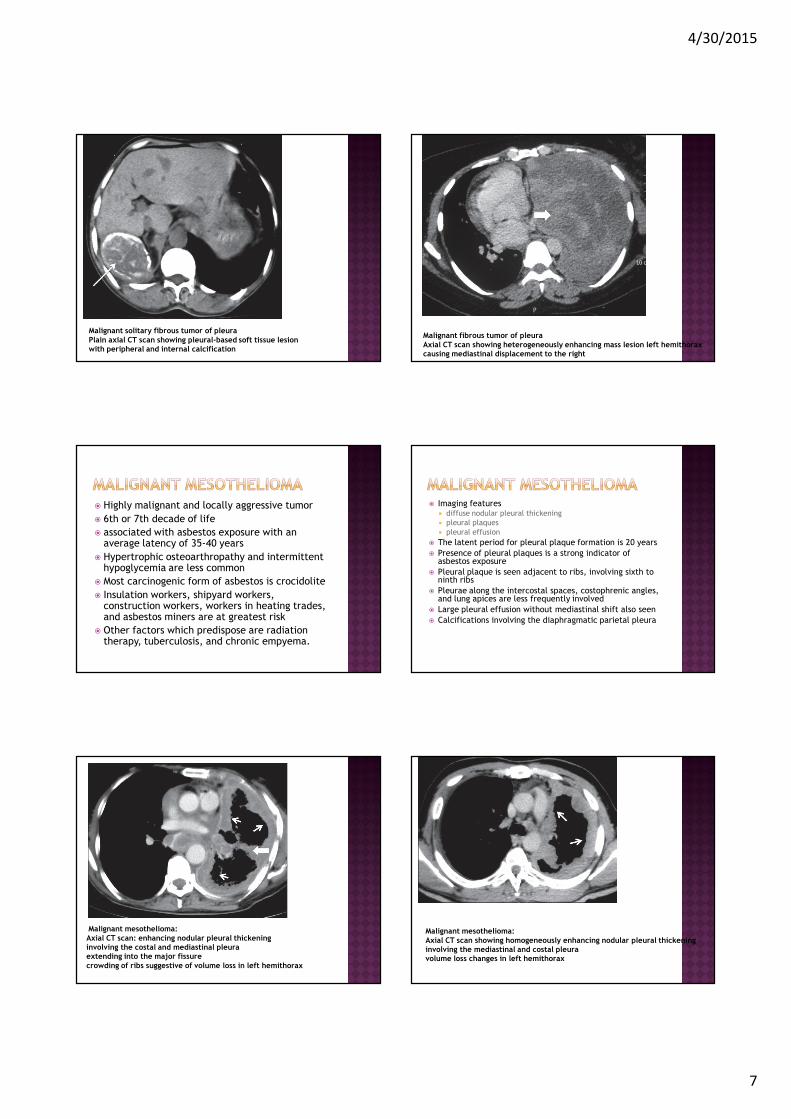
Malignant solitary fibrous tumor of pleuraPlain axial CT scan showing pleural-based soft tissue lesionwith peripheral and internal calcification
Malignant fibrous tumor of pleuraAxial CT scan showing heterogeneously enhancing mass lesion left hemithoraxcausing mediastinal displacement to the right
� Highly malignant and locally aggressive tumor
� 6th or 7th decade of life
� associated with asbestos exposure with an average latency of 35-40 years
� Hypertrophic osteoarthropathy and intermittent hypoglycemia are less common
� Most carcinogenic form of asbestos is crocidolite
� Insulation workers, shipyard workers, construction workers, workers in heating trades, and asbestos miners are at greatest risk
� Other factors which predispose are radiation therapy, tuberculosis, and chronic empyema.
� Imaging features� diffuse nodular pleural thickening
� pleural plaques
� pleural effusion
� The latent period for pleural plaque formation is 20 years
� Presence of pleural plaques is a strong indicator of asbestos exposure
� Pleural plaque is seen adjacent to ribs, involving sixth to ninth ribs
� Pleurae along the intercostal spaces, costophrenic angles, and lung apices are less frequently involved
� Large pleural effusion without mediastinal shift also seen
� Calcifications involving the diaphragmatic parietal pleura
Malignant mesothelioma:Axial CT scan: enhancing nodular pleural thickening involving the costal and mediastinal pleuraextending into the major fissurecrowding of ribs suggestive of volume loss in left hemithorax
Malignant mesothelioma:Axial CT scan showing homogeneously enhancing nodular pleural thickening involving the mediastinal and costal pleuravolume loss changes in left hemithorax
4/30/2015
8
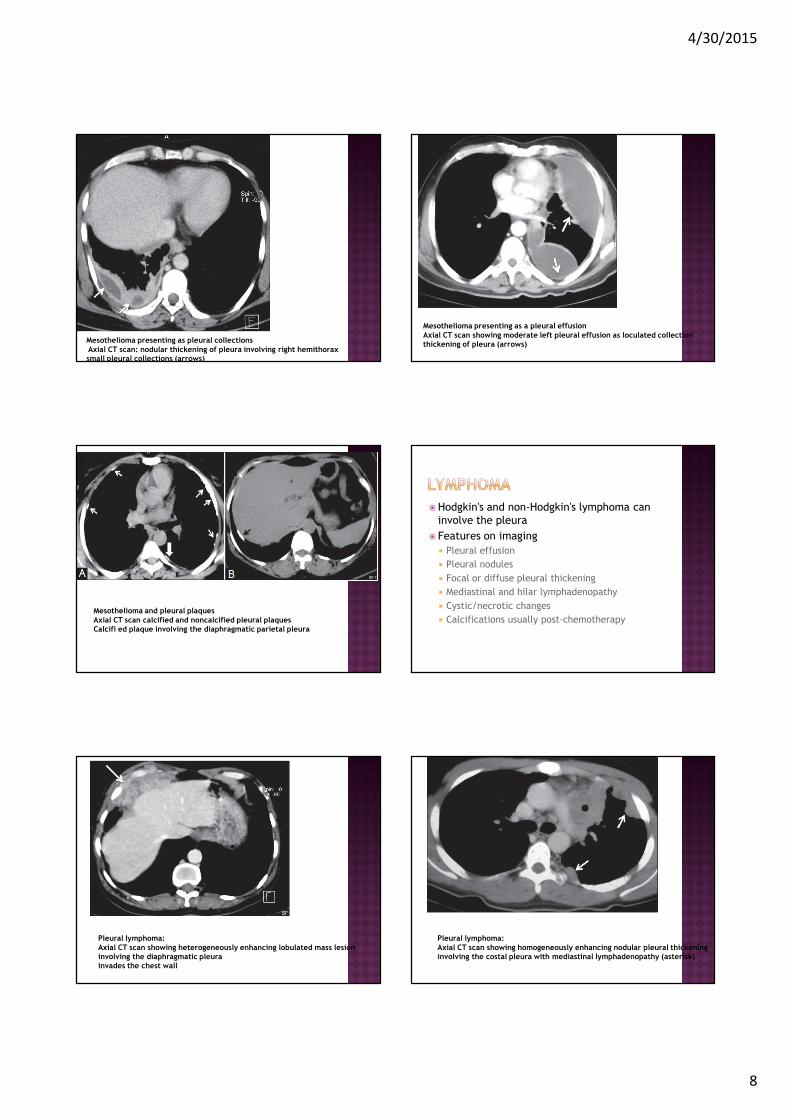
Mesothelioma presenting as pleural collectionsAxial CT scan: nodular thickening of pleura involving right hemithoraxsmall pleural collections (arrows)
Mesothelioma presenting as a pleural effusionAxial CT scan showing moderate left pleural effusion as loculated collectionthickening of pleura (arrows)
Mesothelioma and pleural plaquesAxial CT scan calcified and noncalcified pleural plaquesCalcifi ed plaque involving the diaphragmatic parietal pleura
�Hodgkin's and non-Hodgkin's lymphoma can
involve the pleura
� Features on imaging
� Pleural effusion
� Pleural nodules
� Focal or diffuse pleural thickening
� Mediastinal and hilar lymphadenopathy
� Cystic/necrotic changes
� Calcifications usually post-chemotherapy
Pleural lymphoma: Axial CT scan showing heterogeneously enhancing lobulated mass lesion involving the diaphragmatic pleura invades the chest wall
Pleural lymphoma: Axial CT scan showing homogeneously enhancing nodular pleural thickening involving the costal pleura with mediastinal lymphadenopathy (asterisk)
4/30/2015
9
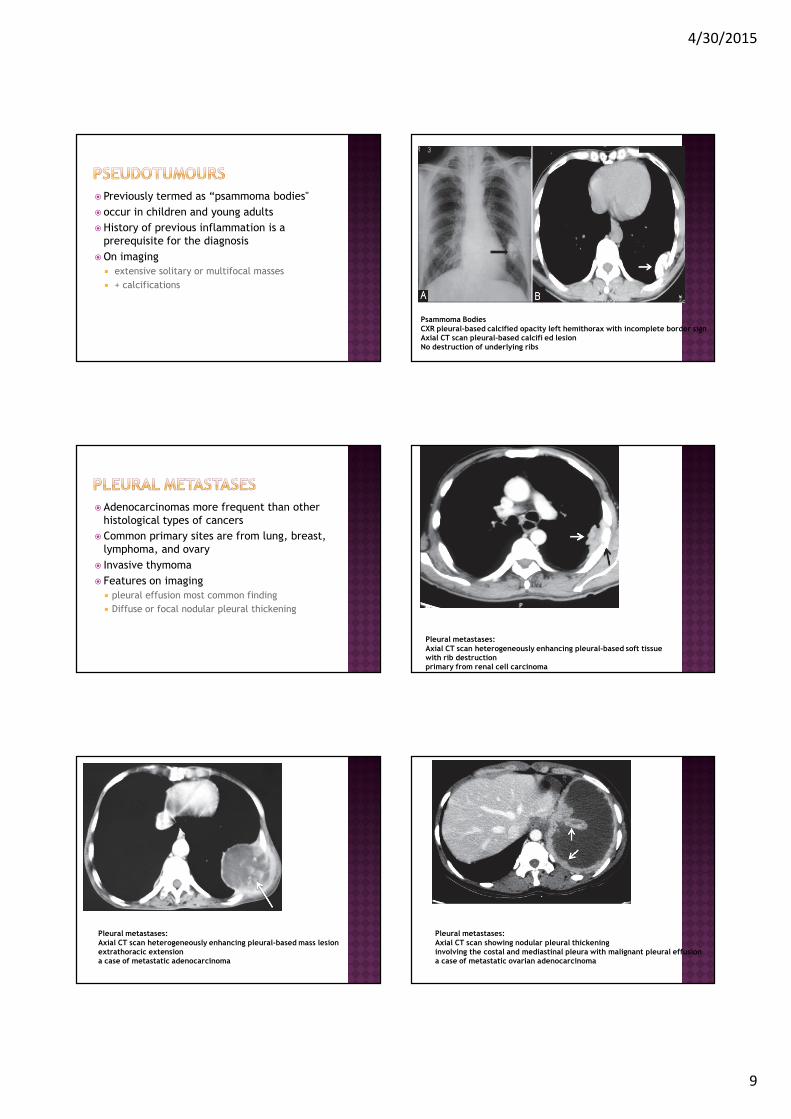
� Previously termed as “psammoma bodies"
� occur in children and young adults
�History of previous inflammation is a
prerequisite for the diagnosis
�On imaging
� extensive solitary or multifocal masses
� + calcifications
Psammoma BodiesCXR pleural-based calcified opacity left hemithorax with incomplete border signAxial CT scan pleural-based calcifi ed lesion No destruction of underlying ribs
� Adenocarcinomas more frequent than other
histological types of cancers
� Common primary sites are from lung, breast,
lymphoma, and ovary
� Invasive thymoma
� Features on imaging
� pleural effusion most common finding
� Diffuse or focal nodular pleural thickening
Pleural metastases:Axial CT scan heterogeneously enhancing pleural-based soft tissue with rib destruction primary from renal cell carcinoma
Pleural metastases:Axial CT scan heterogeneously enhancing pleural-based mass lesion extrathoracic extension a case of metastatic adenocarcinoma
Pleural metastases:Axial CT scan showing nodular pleural thickening involving the costal and mediastinal pleura with malignant pleural effusiona case of metastatic ovarian adenocarcinoma
4/30/2015
10
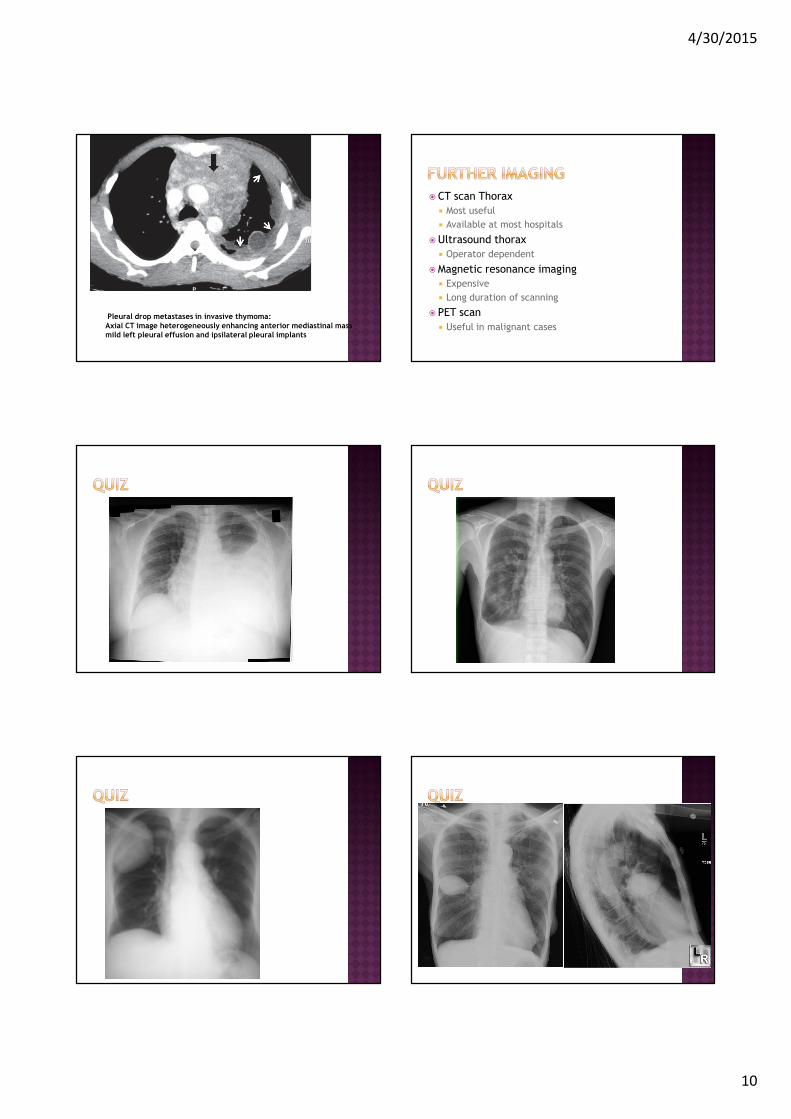
Pleural drop metastases in invasive thymoma: Axial CT image heterogeneously enhancing anterior mediastinal mass mild left pleural effusion and ipsilateral pleural implants
� CT scan Thorax
� Most useful
� Available at most hospitals
�Ultrasound thorax
� Operator dependent
�Magnetic resonance imaging
� Expensive
� Long duration of scanning
� PET scan
� Useful in malignant cases