pmb definition guideline for metastatic (including ... definition project... · pmb definition...
TRANSCRIPT

1 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
PMB definition guideline for metastatic (including advanced) oesophageal cancer

2 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
Disclaimer:
The metastatic stage oesophageal cancer benefit definition has been developed for the majority of
standard patients. These benefits may not be sufficient for outlier patients. Therefore Regulation 15(h) and
15(I) may be applied for patients who are inadequately managed by the stated benefits. The benefit
definition does not describe specific in-hospital management such as theatre, anaesthetists, anaesthetist
drugs and nursing care. However, these interventions form part of care and are prescribed minimum
benefits.
3 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
Table of contents
1. Introduction ………………......................................................................................................5
2. Scope and purpose…...........................................................................................................5
3. Epidemiology and burden of Disease................................................................................. .6
4. Investigation, diagnosis and staging ……………………………………………….....................6
5. Treatment options for metastatic stage oesophageal cancer.............................................. .7
6. Follow up Care ………………...............................................................................................10
7. References…...................................................................................................................... 13

4 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
Abbreviations
5FU Fluorouracil
AC Adenocarcinoma
ASCO American Society of Clinical Oncology
A-YLLs Absolute Years of Life Lost
CMS Council for Medical Schemes
CT Computed tomographic
DTPs Diagnosis treatment pairs
FBC Full Blood Count
GEJ Gastro-oesophageal junction
ICD International Classification of Diseases
IMRT Intensity-modulated radiation therapy
NCR National Cancer Registry
OC oesophageal cancer
PEG Percutaneous endoscopic gastrostomy
PMB Prescribed minimum benefit
SCC Squamous cell carcinoma
SEMS self-expanding metal stents
5 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
1. Introduction
1.1. The legislation governing the provision of the prescribed minimum benefits (PMBs) is contained in
the Regulations enacted under the Medical Schemes Act, 131 of 1998 (the Act). In respect of some
of the diagnosis treatment pairs (DTPs), medical scheme beneficiaries find it difficult to know their
entitlements in advance. In addition, medical schemes interpret these benefits differently, resulting
in a lack of uniformity of benefit entitlements.
1.2. The benefit definition project is coordinated by the Council for Medical Schemes (CMS) and aims
to define the PMB package as well as to guide the interpretation of the PMB provisions by relevant
stakeholders.
2. Scope and purpose
2.1. This is a recommendation for the diagnosis, treatment and care of individuals with metastatic
oesophageal cancer in any clinically appropriate setting as outlined in the Act.
2.2 The purpose is to improve clarity in respect of funding decisions by medical schemes, taking into
consideration evidence based medicine, affordability and in some instances cost-effectiveness.
Table 1: Possible ICD10 codes for identifying metastatic oesophageal cancer
ICD 10 code WHO description
C15.0 Malignant neoplasm, cervical part of oesophagus
C15.1 Malignant neoplasm, thoracic part of oesophagus
C15.2 Malignant neoplasm, abdominal part of oesophagus
C15.3 Malignant neoplasm, upper third of oesophagus
C15.4 Middle third of oesophagus
C15.5 Malignant neoplasm, lower third of oesophagus
C15.8 Malignant neoplasm, overlapping lesion of oesophagus
C15.9 Malignant neoplasm, oesophagus, unspecified
3. Epidemiology
3.1. Despite improved screening and treatment modalities, more than 50% of oesophageal cancer is
diagnosed in the advanced stages of disease (Shah, 2015). Many patients progress to metastatic disease
following treatment with curative intent. Although an improvement has been seen in reduction in Absolute
6 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
Years of Life Lost (A-YLLs) from 2005 to 2015, oesophageal cancer still remains ranked 7th in terms of A-
YLLs in the world (Global Burden of Disease Cancer Collaboration, 2016).
3.2. The prognosis remains poor in advanced or metastatic disease and the aim of treatment is to improve
survival and quality of life through palliative therapy (Berry, 2014).
3.3. In South Africa, patients typically present in late stages of disease and as a result oesophageal cancer
ranks as the 3rd most common cause of cancer death in the country (Global Burden of Disease Cancer
Collaboration, 2016).
3.4. Very little original research has been published in South Africa on oesophageal cancer (Loots, Sartorius,
Madiba, Mulder & Clarke, 2016).
4. Investigation, diagnosis and staging
4.1. Staging of OC is conventionally as per the American Joint Committee on Cancer (AJCC)/Union for
International Cancer Control (UICC) TNM staging system (7th Edition) , however this has recently been
updated to the 8th Edition which is published as 3 separate recommendations for staging (Rice, T.W.,
Ishwaran ,H., Hofstetter, W.L., Kelsen,D.P., Apperson-Hansen, C., Blackstone, 2016: 897-905; Rice et
al, 2016: 913-919; Rice et al , 2016: 906-912).
4.2. The diagnosis and staging of inoperable metastatic oesophageal cancer focuses more on distant
metastases and lymph nodes. The most common organ metastases are in the liver, lung and bone
(Varghese, Hofstetter, Rizk, Low, Darling, Watson, Mitchell & Krasna, 2013).
4.3. Chest x-ray is PMB level of care for the detection of pulmonary metastases
4.4. CT of the chest and abdomen is recommended as the optimal test for staging metastatic oesophageal
cancer (Varghese et al, 2013).
4.5. PET-CT is only recommended for locally advanced disease if the patient has already had a baseline PET
scan or if considering radical local therapy
4.6. Barium studies are recommended in localising disease, to exclude suspicion of a tracheoesophageal
fistula or confirming aspiration as in tight strictures or planning treatment thereof (Varghese et al, 2013).
4.7. Full blood count, liver function tests and renal function tests are PMB level of care
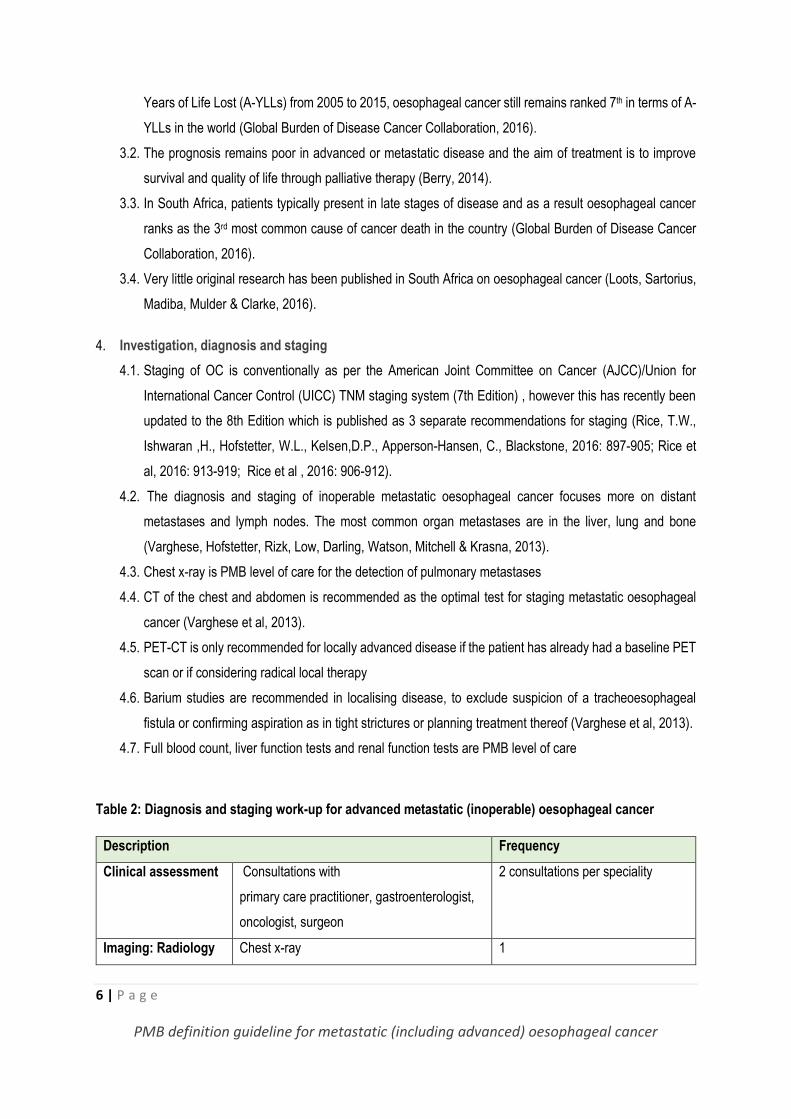
Table 2: Diagnosis and staging work-up for advanced metastatic (inoperable) oesophageal cancer
Description Frequency
Clinical assessment Consultations with
primary care practitioner, gastroenterologist,
oncologist, surgeon
2 consultations per speciality
Imaging: Radiology Chest x-ray 1
7 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
CT study of chest and abdomen
OR
1
PET-CT (FDG ) - )- if the patient has already
had a baseline PET scan or if considering
radical local therapy
1
Barium swallow with contrast
1
Imaging: Procedures Upper gastro-intestinal endoscopy 1
Bronchoscopy - Only on specialist motivation 1
Histological
assessment
Histology / Cytology 1
Pathology Full Blood Count (FBC) 1
Liver function test 1
Renal function 1
5. Treatment options for metastatic stage oesophageal cancer
Treatment in locally advanced and metastatic oesophageal cancer is largely based on systemic therapies or
palliative management. Improvement in overall survival is unlikely and therefore quality of life issues are important
with a focus on managing pain, dysphagia and bleeding.
The use of radical therapy vs palliative therapy in locally advanced disease is based on patient factors (age,
performance status, symptoms, anthropometric measures, biochemistry and haem) as well as tumor factors
(location, size, length risk of occult metastases). Patients who have localized disease and are amenable to radical
therapy may be candidates for treatments such as chemoradiotherapy (definitive), chemotherapy followed by
assessment for surgery or radiotherapy. In this instance a PET-CT scan is recommended to rule out metastatic
disease if the CT is unclear to avoid protracted, unnecessary treatment.
5.1. Surgical management
The following surgical interventions of oesophageal cancer are PMB level of care for metastatic
disease:
- Dilatation
- Stenting
- Percutaneous endoscopic gastrostomy (PEG)

8 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
5.1.1. Dilatation may be used to facilitate endoscopic ultrasound where strictures limit access or pre-
stenting (American Society for Gastrointestinal Endoscopy Standards of Practice Committee,
2013).
5.1.2. Dilatation may be used in severe obstruction where the patient is still able to swallow liquids
however the risk of perforation is high and symptom alleviation is better achieved with stenting.
(American Society for Gastrointestinal Endoscopy Standards of Practice Committee, 2013;
NCCN Guidelines Version 2, 2016)
5.1.3. The most recent Cochrane Systematic Review (2014) of the treatment of dysphagia in
oesophageal cancer does not recommend dilatation either as monotherapy or in combination
with other modalities as a comparative intervention to stenting and other modalities such as
brachytherapy however dilatation is used pre-stenting (Dai, Li, Xie, Liu, Zhang, Zhou, Pan &
Yang, 2014).
5.1.4. Self-expanding metal stents (SEMS) are a recommended palliation therapy for patients with
dysphagia and/or fistula. Metal stents are preferred over plastic stents with lower adverse events
and improved clinical benefits (Dai et al, 2014; Spaander, Baron, Siersema, Fuccio,
Schumacher, Escorsel, Garcia-Pagán, Dumonceau, Conio, de Ceglie, Skowronek, Nordsmark,
Seufferlein, Van Gossum, Hassan, Repici & Bruno, 2016).
5.2. Chemotherapy for locally advanced unresectable oesophageal cancer
5.2.1. The recurrence rate in patients who receive chemotherapy for metastatic oesophageal cancer
is generally high with a decline in performance status following first-line treatment thereby
limiting treatment options as second line therapy. Higher response rates (up to 65 percent) are
reported in phase II trials evaluating combination therapy in patients with advanced
oesophageal and gastric cancer. However, almost without exception, response rates have
been lower in the setting of randomized trials. Furthermore, whether higher response rates
seen with combination as compared with single agent chemotherapy translate into longer
response duration or survival remains uncertain. The decision rests with the clinicians’
assessment and is based on clinical condition.
5.2.2. The medicines listed below may be used in recognised combinations.
9 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
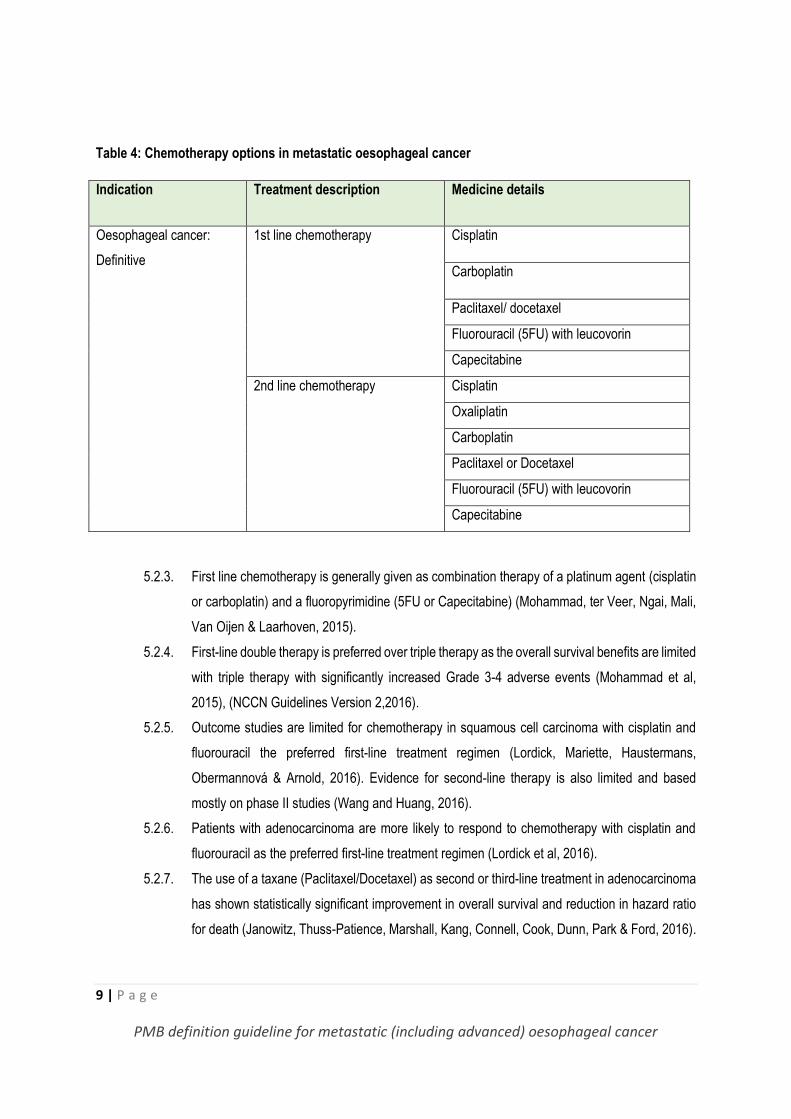
Table 4: Chemotherapy options in metastatic oesophageal cancer
Indication Treatment description Medicine details
Oesophageal cancer:
Definitive
1st line chemotherapy Cisplatin
Carboplatin
Paclitaxel/ docetaxel
Fluorouracil (5FU) with leucovorin
Capecitabine
2nd line chemotherapy Cisplatin
Oxaliplatin
Carboplatin
Paclitaxel or Docetaxel
Fluorouracil (5FU) with leucovorin
Capecitabine
5.2.3. First line chemotherapy is generally given as combination therapy of a platinum agent (cisplatin
or carboplatin) and a fluoropyrimidine (5FU or Capecitabine) (Mohammad, ter Veer, Ngai, Mali,
Van Oijen & Laarhoven, 2015).
5.2.4. First-line double therapy is preferred over triple therapy as the overall survival benefits are limited
with triple therapy with significantly increased Grade 3-4 adverse events (Mohammad et al,
2015), (NCCN Guidelines Version 2,2016).
5.2.5. Outcome studies are limited for chemotherapy in squamous cell carcinoma with cisplatin and
fluorouracil the preferred first-line treatment regimen (Lordick, Mariette, Haustermans,
Obermannová & Arnold, 2016). Evidence for second-line therapy is also limited and based
mostly on phase II studies (Wang and Huang, 2016).
5.2.6. Patients with adenocarcinoma are more likely to respond to chemotherapy with cisplatin and
fluorouracil as the preferred first-line treatment regimen (Lordick et al, 2016).
5.2.7. The use of a taxane (Paclitaxel/Docetaxel) as second or third-line treatment in adenocarcinoma
has shown statistically significant improvement in overall survival and reduction in hazard ratio
for death (Janowitz, Thuss-Patience, Marshall, Kang, Connell, Cook, Dunn, Park & Ford, 2016).

10 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
5.2.8. Taxanes may be used in combination as first-line therapy or monotherapy as second-line
treatment (Lordick et al, 2016; NCCN Guidelines Version 2, 2016).
5.2.9. Capecitabine has been shown to be well tolerated as first-line treatment in combination with
cisplatin or paclitaxel (Lee, Kim, Kim, Lee, Park, Im, & Park, 2015).
5.2.10. Perioperative chemotherapy is recommended in locally advanced adenocarcinoma of the
thoracic oesophagus with the combination of a platinum agent and fluorouracil being the best
studied (Lordick et al, 2016; Malthaner, Wong, Spithoff, Rumble & Zuraw, 2016).
5.3. Radiation therapy
5.3.1. Brachytherapy compared to SEMS has shown to have gradual improvement over SEMS in
managing dysphagia and quality of life with time and is suggested as an alternative to SEMS
based on performance status (Dai et al, 2014; NCCN Guidelines Version 2, 2016).
5.3.2. Single dose brachytherapy may be recommended as palliative treatment in metastatic disease
with improved tolerability and symptom relief compared to stenting (Lordick et al, 2016).
5.3.3. Few studies have evaluated the cost-effectiveness of brachytherapy as palliative treatment with
2 studies suggesting similar total medical costs with another showing significantly higher costs
for the brachytherapy group. Brachytherapy can be combined with external beam radiotherapy
or offered after stent insertion. External beam may also be combined with stent insertion (Homs,
Steyerberg, Eijkenboom, Tilanus, Stalpers, Bartelsman, Van Lanschot, Wijrdeman, Mulder,
Reinders, Boot, Aleman, Kuipers, & Siersema, 2004; Polinder, Homs, Siersema, Steyerberg,
2004; Wenger, Johnsson, Bergquist, Nyman, Ejnell, Lagergren, Ruth & Lundell, 2005).
Table 5. Radiation therapy in locally advanced oesophageal cancer
Conventional Radiation therapy
Palliation: 5#: conventional single volume / Conventional multiple volumes
Palliation: 10#: conventional single volume / Conventional multiple volumes
Brachytherapy: single dose brachytherapy in palliative setting
6. Follow up care
6.1. Follow-up and surveillance in metastatic disease should focus on patient quality of life with optimal
symptom management and patient support (Lordick et al, 2016).

11 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
6.2. The American Society of Clinical Oncology (ASCO) recommends in its Choosing Wisely campaign of
2013 to “avoid using positron emission tomography or positron emission tomography–computed
tomography scanning as part of routine follow-up care to monitor for cancer recurrence in asymptomatic
patients who have finished initial treatment to eliminate the cancer unless there is high-level evidence that
such imaging will change the outcome” (Schnipper, Lyman, Blayney, Hoverman, Raghavan, Wollins &
Schilsky, 2013).
6.3. The use of PET as a follow-up to detect recurrence in oesophageal does not improve survival outcomes
at 2 years (Healy, Yin, Reddy & Wong, 2016).
12 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
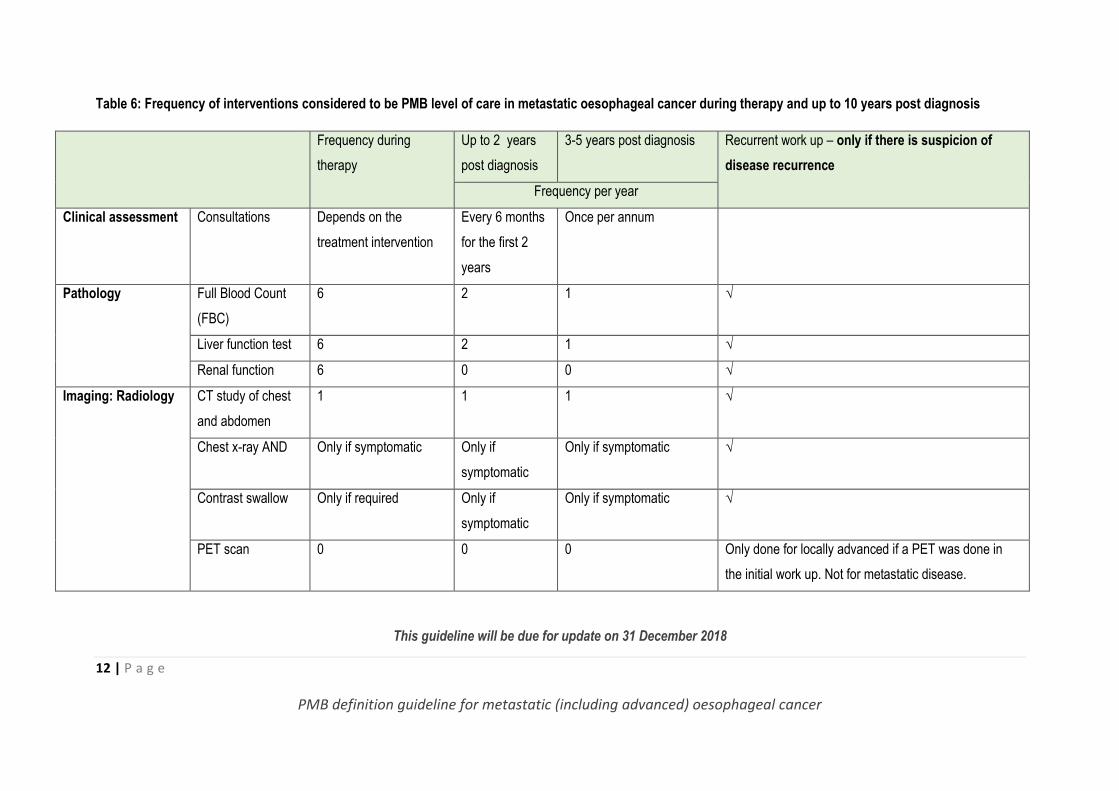
Table 6: Frequency of interventions considered to be PMB level of care in metastatic oesophageal cancer during therapy and up to 10 years post diagnosis
Frequency during
therapy
Up to 2 years
post diagnosis
3-5 years post diagnosis Recurrent work up – only if there is suspicion of
disease recurrence
Frequency per year
Clinical assessment Consultations Depends on the
treatment intervention
Every 6 months
for the first 2
years
Once per annum
Pathology Full Blood Count
(FBC)
6 2 1 √
Liver function test 6 2 1 √
Renal function 6 0 0 √
Imaging: Radiology CT study of chest
and abdomen
1 1 1 √
Chest x-ray AND Only if symptomatic Only if
symptomatic
Only if symptomatic √
Contrast swallow Only if required Only if
symptomatic
Only if symptomatic √
PET scan 0 0 0 Only done for locally advanced if a PET was done in
the initial work up. Not for metastatic disease.
This guideline will be due for update on 31 December 2018
13 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
7. References
American Society for Gastrointestinal Endoscopy Standards of Practice Committee. 2013. Endosocopy in the
assesment and treatment of esophageal cancer. Gastrointestinal Endoscopy, 77(3): 328-34.
Berry, M. 2014. Esophageal cancer: staging system and guidelines for staging and treatment. A review. Journal
of Thoracic Diseases, 6(S3):S289-S297.
Dai, Y., Li, C., Xie, Y., Liu, X., Zhang, J., Zhou, J., Pan, X. & Yang, S. 2014. Interventions for dysphagia in
oesophageal cancer. Cochrane Database of Systematic Reviews, 10: CD005048.
Global Burden of Disease Cancer Collaboration. 2016. Global, Regional, and National Cancer Incidence,
Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years for 32 Cancer
Groups, 1990 to 2015. A Systematic Analysis for the Global Burden of Disease Study. Journal of the American
Medical Association- Oncology, E1-E25.
Healy, M.A., Yin, H., Reddy, R.M. & Wong, S.L. 2016. Use of Positron Emission Tomography to Detect
Recurrence and Associations With Survival in Patients With Lung and Esophageal Cancers. Journal of the
National Cancer Institute, 108:7.
Homs, M.Y., Steyerberg, E.W., Eijkenboom, W.M., Tilanus, H.W., Stalpers, L.J., Bartelsman, J.F., van Lanschot,
J.J., Wijrdeman, H.K., Mulder, C.J., Reinders, J.G., Boot, H., Aleman, B.M., Kuipers, E.J. & Siersema, P.D. 2004.
Single-dose brachytherapy versus metal stent placement for the palliation of dysphagia from oesophageal
cancer: multicentre randomised trial. Lancet, 364 (9444): 1497-504.
Janowitz, T., Thuss-Patience, P., Marshall, A., Kang, J.H., Connell, C., Cook, N., Dunn, J., Park, S.H. & Ford, H.
2016. Chemotherapy vs supportive care alone for relapsed gastric, gastroesophageal junction, and oesophageal
adenocarcinoma: a meta-analysis of patient-level data. British Journal of Cancer, 114(4): 381-7.
Lee, S.J., Kim, S., Kim, M., Lee, J., Park, Y.H., Im, Y.H. & Park, S.H. 2015. Capecitabine in combination with
either cisplatin or weekly paclitaxel as a first-line treatment for metastatic esophageal squamous cell carcinoma:
a randomized phase II study. BioMed Central Cancer, 15: 693.
Loots, E., Sartorius, B., Madiba, T.E., Mulder, C.J. & Clarke, D.L. 2016. Is Clinical Research in Oesophageal
Cancer in South Africa in Crisis? A Systematic Review. World Journal of Surgery, Vol. ePub ahead of print.
Lordick, F., Mariette, C., Haustermans, K., Obermannová, R. & Arnold, D. 2016. Oesophageal Cancer: ESMO
Clinical Practice Guidelines. Annals of Oncology, 27 (5):v50-v57.
Malthaner, R.A., Wong, R.K.S., Spithoff, K., Rumble, R.B. & Zuraw, L. 2016. Gastrointestinal Cancer Disease
Site Group. Preoperative or postoperative therapy for resectable esophageal cancer. Program in Evidence-
based Care Evidence-based Series No: 2-11 Version 4. 2008.
Mohammad, N., ter Veer, E., Ngai, L., Mali, R., van Oijen, M. & Laarhoven, H. 2015. Optimal first-line
chemotherapeutic treatment in apteints with locally advanced or metastatic esophagogastric carcinoma: triplet
versus doublet chemotherapy: a systematic literature review and meta-analysis. Cancer Metastatis Review,
34:421-441.
National Comprehensive Cancer Network. 2016. Esophageal and Esophagogastric junction cancers. NCCN
Guidelines Version 2.
14 | P a g e
PMB definition guideline for metastatic (including advanced) oesophageal cancer
Polinder, S., Homs, M.Y., Siersema, P.D., Steyerberg, E.W. & Group. 2004. Dutch SIREC Study. Cost study of
metal stent placement vs single-dose brachytherapy in the palliative treatment of oesophageal cancer. British
Journal of Cancer, 90(11): 2067-72.
Rice, T.W., Ishwaran, H., Kelsen, D.P., Hofstetter, W.L., Apperson-Hansen, C., Blackstone, E.H. & Investigators.
2016. Worldwide Esophageal Cancer Collaboration. Recommendations for neoadjuvant pathologic staging
(ypTNM) of cancer of the esophagus and esophagogastric junction for the 8th edition AJCC/UICC staging
manuals. Diseases of the Esophagus, 29(8): 906-912.
Rice, T.W., Ishwaran, H., Blackstone, E.H., Hofstetter, W.L., Kelsen, D.P., Apperson-Hansen, C. & Investigators.
2016. Worldwide Esophageal Cancer Collaboration. Recommendations for clinical staging (cTNM) of cancer of
the esophagus and esophagogastric junction for the 8th edition AJCC/UICC staging manuals. Diseases of the
Esophagus, 29(8): 913-919.
Rice, T.W., Ishwaran, H., Hofstetter, W.L., Kelsen, D.P., Apperson-Hansen, C., Blackstone, E.H. & Investigators.
2016. Worldwide Esophageal Cancer Collaboration. Recommendations for pathologic staging (pTNM) of cancer
of the esophagus and esophagogastric junction for the 8th edition AJCC/UICC staging manuals. Diseases of the
Esophagus, 29(8): 897-905.
Schnipper, L.E., Lyman, G.H., Blayney, D.W., Hoverman, J.R., Raghavan, D., Wollins, D.S. & Schilsky, R.L.
2013. American Society of Clinical Oncology top five list in oncology. Journal of Clinical Oncology, 31(34):4362-
70.
Shah, M. 2015. Update on Metstatic Gastric and Esophageal Cancers. Journal of Clinical Oncology, 33(16):
1760-1769.
Spaander, M.C., Baron, T.H., Siersema, P.D., Fuccio, L., Schumacher, B., Escorsel,l À., Garcia-Pagán, J.C.,
Dumonceau, J.M., Conio, M., de Ceglie, .A., Skowronek, J., Nordsmark, M., Seufferlein, T., Van Gossum, A.,
Hassan, C., Repici, A. & Bruno, M.J.2016. Esophageal stenting for benign and malignant disease: European
Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy, 48(10): 939-48.
Varghese, T.K., Hofstetter, W.L., Rizk, N.P., Low, D.E., Darling, G.E., Watson, T.J., Mitchell, J.D. & Krasna, M.J.
2013. The Society of Thoracic Surgeons guidelines on the diagnosis and staging of patients with esophageal
cancer. Annals of Thoracic Surgery, 96: 346-356.
Wang, X. & Huang, J. 2016. Irinotecan plus fluorouracil-based regimen as second or third-line chemotherapy for
recurrent or metastatic esophageal squamous cell carcinoma. Thoracic Cancer, 7: 246–250.
Wenger, U., Johnsson, E., Bergquist, H., Nyman, J., Ejnell, H., Lagergren, J., Ruth, M. & Lundell, L. 2005. Health
economic evaluation of stent or endoluminal brachytherapy as a palliative strategy in patients with incurable
cancer of the oesophagus or gastro-oesophageal junction: results of a randomized clinical trial. European
Journal of Gastroenterology and Hepatology, 17(12): 1369-77.