pneumoconiosis - postgraduate medical journalpneumoconiosis' (prendergrass and leopold, i945)....
TRANSCRIPT
599
PNEUMOCONIOSISBy A. MEIKLEJOHN, M.D.From the University of Glasgow7
HistoricalIn medical writings from the ' Epidemics of
Hippocrates' (460-370 B.C.) to the ' Treatise ofthe Diseases of Tradesmen' by Ramazzini (I633-I714), the historian may discover references to theoccurrence of lung diseases among workmen en-gaged in dusty occupations, but the significance ofthese passages is largely speculative. By contrastthe allusions contained in the texts (Meiklejohn,1947) of Benson's Patents, 1726 and 1732, forgrinding flints are precise and comprehensive:
' Any person ever so healthfull or strong work-ing in that business cannot probably survive abovetwo years, occasioned by the dust sucked into hisbody by the air he breaths, which being of a pon-derous nature, fixes there so closely that it is nowvery difficult to find persons which will engage inthe business, to the great obstruction and detri-ment of the said trade.'These statements appear authentic as it is re-
corded that calcined flint was introduced for use inearthenware manufacture in 1720 (Shaw, I829).Thackrah of Leeds (I832) discussed at length
the health of ' operatives subjected to dust' andever since physicians have recorded from their ownlocal experience the melancholy tale of dust, con-sumption and premature death. Knight (I830) apractitioner of Sheffield relates that, ' The forkgrinders who use a dry grindstone die at the agesof 28 and 32 ' and among the preventive measureswhich he recommends is that this occupationshould be confined to criminals.The disease then, as now, was incurable, and
so the demand was for prevention and control.There is scarcely a single modern measure or de-vice which is not recorded and discussed by theolder writers. Thackrah (I832) mentions sub-stitution of harmful by less noxious substances, ex-haust ventilation, wet processes in place of dry,face masks, alternation of employment and re-duced hours of labour. In a very interestingpassage he describes the benefits of natural waterinfusion through fissures in the rock in leadmines:
' The particles, on the contrary, are laid as theyare formed, by the continuous oozing, droppingand splashing of the insinuating water.'At a Scottish cotton mill we learn from Ritchie
(I828) about the complete enclosure of carding andspinning machines and how from the picking roomalone 828 lb. of cotton dust was collected in theexhaust chamber during a single year. CalvertHolland (i843) discussed the advantages of downdraught exhaust ventilation with flues under thefloor-as against overhead hoods and ducts.On the clinical side, early detection of the
disease by regular medical supervision, chestmeasurement, estimation of pulmonary vitalcapacity and inhalation therapy, all are noted.Lack ofco-operation by the workmen then as now
was a problem:' We remark with regret the men'sinattention to health, their indifference to the pre-vention of disease. They think nothing of in-jurious agents till their health is destroyed and thetime for prevention is past.' Employers haveresponsibilities and duties: ' It is especially in-cumbent on masters to regard the health of thepersons they employ; to examine the effects ofinjurious agents, to invent and provide remedies,and to enforce theit application.' But this cannotbe achieved voluntarily and so the need of FactoryActs is foreseen: ' Whatever improvement may beeffected without a legislative enactment . . . thisimprovement will be but temporary.' Finally, forthe physician, there is wise counsel: ' He must notbe content with the loose statements of thoughtlessand prejudiced workmen ' (Thackrah, I832), andnowadays I, personally, would venture to addemployers and trade union officials.
In support of their arguments these earlyauthors provide extensive statistical tables re-vealing the dreadful toll of fibroid phthisis in thei8th and igth centuries, but repetition here wouldserve little purpose; indeed by false comparisonsmight lead to a wholly unjustified complacencyabout the tragic present. I
The historical development of opinion on theetiology and pathology of lung diseases in trades-men requires brief notice, but before this it isnecessary to examine the evolution of the nomen-clature of the disease.
Nomenclature and its SignificanceDuring the i8th century the dust diseases of the
lungs were identified by terms descriptive of theclinical features, asthma, rot, phthisis or con-
Si
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

6oo POSTGRADUATE MEDICAL JOURNAL December 1949
sumption, to which was prefixed the name of theassociated trade, as in knife-grinders' asthma andpotters' rot. The next phase in nomenclature wasrelated to the study of morbid anatomical changesin the lungs observed at necropsy. In I838Stratton proposed the term anthracosis to describethe appearances which he had observed in a coal-miner's lungs. Later, about i866, Zenker re-corded the presence of red iron oxide in the lungsof women engaged in handling this powder. Thiscondition he named siderosis and for the variousaffections of the lungs produced by the inhalationof dust-like particles he proposed the generic titlepneumonokoniosis (nvev'p'ov, lung and KOVL5,dust). Following this practice Visconti, in I870,introduced the term silicosis for those cases inwhich the noxious dust was composed of silex orflint, and Merkel added chalicosis when fine gravelor stone was the offending agent. Byssinosis wasthe form associated with the inhalation of cotton,flax and linen dusts. Thus a stage of finality wasreached whereby pneumonokoniosis was recog-nized as the general title signifying a condition ofdust disease of the lung. Under this heading cer-tain varieties were identified and named accordingto the causative dust, anthracosis, siderosis, sili-cosis, chalicosis and byssinosis. Collectively theseconstituted the pneumonokonioses or dust diseasesof the lungs. At present there is considerable con-fusion in the use of these terms as exemplified bythis definition in the current CompensationAct (I946) in South Africa: ' " Silicosis " meansany form of pneumoconiosis due to the inhalationof mineral dust.'
So in effect silicosis may mean asbestosis. Thisreflects the fact that the original generic term hasproved awkward and pedantic in regular use. Inpractice it has become shortened to pneumo-koniosis; an attempt to abbreviate it still further tokoniosis failed. Two forms of spelling, pneumo-koniosis and pneumoconiosis, are in regular use,but the latter receives most favour throughout theworld and is the only spelling recorded in the' New Oxford Dictionary ' (I909 edition). Classicalscholars agree that both spellings are defensible,but omission of the central ' no ' is wrong, render-ing the term etymologically meaningless. Usageand convenience, however, have established theshorter form; the need is to adopt a uniformspelling.With the advance in knowledge of pathology of
dust affections of the lungs, a more seriousdifficulty has arisen, namely, interpretation of theterm pneumoconiosis. Does it signify simply theaccumulation of dust in the lungs, a dust-riddenstate, or does it involve the concept of disease, adeparture from health ? That 'there is no agree-ment is reflected in such distinctions as are im-
plied in ' active' and ' inert' dusts and ' benignpneumoconiosis ' (Prendergrass and Leopold,I945). The problem is still further complicatedby attempts to embrace certain legal and ad-ministrative considerations in relation to work-men's compensation (Fletcher, 1948). And againhow are we to regard byssinosis, bagassosis,berylliosis, aluminosis, manganese pneumonitis,bronchomycoses and a host of others ? The con-fusion is world-wide and 4,as become so great thatit almost appears as if the original terminologyshould be abandoned and that some authoritativebody such as the International Labour Officeshould endeavour to formulate and establish aclassification and nomenclature for universal use.At present in this country the practical every-
day consideration is the legal definition for pur-poses of workmen's compensation under theNational Insurance (Industrial Injuries) Act, I946.'"Pneumoconiosis " means fibrosis of the
lungs due to silica dust, asbestos dust or otherdust, and includes the condition of the lungsknown as dust reticulation.'
This is fully discussed in the contribution byDr. Sutherland.
Pathology and EtiologyThe earliest references to the noxious effects of
substances inhaled into the lungs are to theclinical manifestations in certain occupations,notably metalliferous mining. Thus Hippocrateswrites of 'the wan complexion and the difficultyof breathing of the metal diggers' and GeorgiusAgricola (I557) remarks that 'when the dust iscorrosive it ulcerates the lungs and producesconsumption.'Apart from recording the same illness in an
ever increasing number of trades and occupations,no advance occurred until the igth century whenstudy of the morbid anatomical changes atnecropsy permitted correlation with the clinicalmanifestations. Diemerbroek (I832) relates that' in dissecting the bodies of masons, dead fromasthmatic affections, he found heaps of sand intheir lungs, and in dividing the pulmonary sub-stance, he seemed to be cutting a sandy body.'Gregory (I83I) describes the lungs of a miner asbeing infiltrated with black matter resembling, ifnot identical with, coal.
Calvert Holland (I843) is among the earliestobservers to suggest that in cutlery grinders'asthma the ' structural modifications in the lungsare of two distinct types and so admit of an easyclassification.'
' In the one case, they (the symptoms) wereoften accompanied with considerable constitutionalvigour, and though harassing in the extreme,interfered comparatively little with the appetite
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

December 1949 MEIKLEJOHN: Pneumoconiosis 6oi
FIG. i.-Male aged 40 years. Radiographic appearances natural for age.
or the digestive functions; and in connection withthese symptoms, the chest was observed to beprominent and well-developed. In the other case,the thorax was remarked to be flat and contracted,the powers of life feeble, and the animal frame ex-hibiting indications of gradual emaciation.'The same author gives an equally compre-
hensive account of the marked structural changesin the lungs, among which he particularly notesthe hard, black, gritty enlargement of the bronchialglands immediately at the bifurcation of thetrachea and:
'In some instances the lungs have presented anappearance as if black currants had been dis-tributed throughout the whole substance of them.'
This is still an accurate description of ' classicalsilicosis.' These quotations reveal that thephysicians were already beginning to distinguishbetween simple dust fibrosis and this conditioncomplicated by tuberculosis. Hall (I857) assertsthis quite clearly:
' There is no necessary connexion between theSheffield grinders' disease and thoracic consump-tion, although both affections may be present inthe same individual.'The absolute distinction was not possible until
Koch's discovery of the tubercle bacillus in i882.Since then pathologists have added greatly to
our knowledge of the minute histology of the
lesions and associated changes in the lungs.Considerable controversy, however, has rangedover the separate and combined effects of the dustand tuberculous infection, and this problem re-mains unresolved.From the outset dust was generally recognized
as the noxious agent though Laennec (i8I8) re-jected the idea that dust could be retained in thelungs and so induce disease. Calvert Holland(I843) dismisses this opinion as lack of experienceof manufacturing processes. Summing up thechapter of his book on dust diseases, Thackrah(I832) records:
' Dust is the great bane of manufacture, andwhether it be farina, animal or vegetable fibre, orevolved from minerals, stone, lime, coal or metal,it injures the respiratory organs, in proportion tothe mechanical irritation it induces on thebronchial membrane.'
During the ensuing years the occurrence of thedisease was reported from practically everycountry in which metalliferous mining was carriedon. Presenting evidence before a Royal Com-mission, Haldane (1914) made this significantdeclaration:
' I believe the disease is the same all over theworld, and the end comes through tubercularinfection; ' and'We ought to know what the qualities are in
B2
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

602 POSTGRADUATE MEDICAL JOURNAL December q49
FIG. 2.-Male aged 58 years; china biscuit placer (pottery, pure flirt risk), 45 years.Generalized fine silicosis ;died 4 months later ;mvocardial degeneration;silicosis without tuberculosis; confirmed post-mortem.
the dust which makes it dangerous, so that wemay be able to say with regard to any dust off-hand whether that dust is dangerous or not.'
In the following year Collis (I915) provided partof the answer when, as a result of comprehensiveanalytical studies in various industries, he con-cluded:'While most dusts have an injurious influence,
silica in the form of free silicon dioxide alonestimulates the formation of fibrous tissue.'
So just as Haldane had proclaimed the essentialunity of the pathological process, Collis had de-fined the essential unity of the causative agent.The disease was silicosis and the problem was todiscover the mode of action of the silica particles.Thackrah and Calvert Holland had attributed itto mechanical irritation. McCrae (19I3) haddemonstrated that ' the largest particles whichgained access and became embedded in the lungsdid not exceed io microns in diameter and 70 percent. of all particles were less than i micron.'This enabled Gye and Purdy (I922(a) and I922(b) )to determine: (i) ' that particles lose their sharp-ness when embedded in the phagocytic dustcells,' and (2) ' that the reaction (fibrosis) isnoted at points remote from the presence ofsilica.'They advanced a chemical hypothesis of action:
'Finely divided silica in the lungs slowly formsa silica sol, which acts as a direct cell poison.'While this has proved generally acceptable some
authors (Heffernan and Green, I928, and Heffer-nan, 1946) dissent. Reviewing this aspect of thesubject in I945 King concludes:
' Successful as the solubility theory may be inexplaining the observed facts of silicosis and inindicating new lines of approach, it must berecognized that it does not always appear to workin practice.'
For a time (Middleton, 1936) it was thought, butnow rejected (I.L.O., I938), that alkalis couldaccelerate the action of silica, while Haldane(1917) had suggested that coal dust had an in-hibitory action, a quality which Heffernan andGreen (1928) had likewise attributed to ' claysubstance, carbon and shale dust,' and Kettle(I935) to oxide of iron. This idea has beenadvanced still further in relation to powderedmetallic aluminium (Denny, Robson and Irwin,I937, I939(a) and i939(b)).Gardner (I920) in America represented another
viewpoint, namely, that ' the lung lesion is due toa combined irritant action of the tubercle bacillusand the silica, which action neither of them alonecan produce.' This reflects the other character-istic of the disease which remained unexplained,
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

December 194(9 \IEIKLEJOHN: PuiOtlnl,oeoiosis 6o0
namely, the excessively high incidence of tubercu-losis as a complication of silicosis. Following ex-tensive laboratory observations Gye and Kettle(I922) concluded that ' silica caused a coagulationnecrosis in which all of the tubercle bacilli wereprotected from phagocytosis and enabled tomultiply rapidly with impunity,' a process furtherfacilitated by disorganization of the lymphaticdrainage of the lung.
Just when it appeared that free silica had beenestablished as the single causative noxious agent, aniew dust disease was reported and confirmed.'T'his was asbestosis, fibrosis of the lungs due tothe inhalation of asbestos dust. Asbestos is acomplex mineral silicate, so the whole question ofthe etiology was re-opened in relation to this andother silicates (combined silica as opposed to freesilica) and for a time the term ' silicatosis ' wascurrent. Then Jones (I933 and 1934), followinganalyses of the ash of silicotic lungs, disputed thefree silica hypothesis by submitting that while freesilica might be the causal agent in isolated cases,its action was insignificant compared with that ofa fibrous mineral silicate, known to geologists assericite. 'This hypothesis, in turn, has not with-stood the critical judgment of experts and has notbeen confirmed by animal tests.
Finally the alarming incidence of chronic pul-monary disease among coal-miners, particularly inSouth Wales, focused attention. 'The occurrenceof silicosis among the stone workers in the mineswas well known, but these cases accounted for avery small number of the total. A special inquirywas instituted by which Hart and Aslett (1942)established that among underground workers andcertain others engaged in handlinig coal, thereexists another form of pneumoconiosis, to whichthey applied the name ' dust reticulation,' a termdescriptive of the radiographic and pathologicalchanges. Belt and Ferris (1942) originallydescribed the pathological changes and Gough(1940, I947(a) and I947(b)) has since added con-
siderably to this knowledge. As yet the causativedust constituent has not been defined and isproving a very difficult problem as ' coal' or' mine ' dust is a very complex mixture ot mineraldusts, including not only carbon but free andcombined silica, silicon dioxide and silicates. Inaddition the workmen are exposed to various gasesderived from explosives and to volatile emanationsresulting from the natural decomposition of coal.Moreover, the possible role of associated tubercu-lous infection in the production and course of thedisease remains undiscovered.
Social AspectsThroughout our industrial history the pneumo-
conioses have created serious social problems as
revealed in the classical statistical surveys of Farr(I875) and Ogle (i885). Today, as never before,they constitute a major political problem.Commencing in IgI9 the various forms of
pneumoconiosis have been brought within thescope of workmen's compensation under whichcertification of the disease is solely the re-sponsibility of the Pneumoconiosis Medical Boardof the Ministry of National Insurance. As aresult comprehensive authoritative statistics areavailable and the present position may be con-cisely represented in the following table derivedfrom this source.
CEIRTIFICATES OF TOTAL OR PARTIAlAI)1DSABL,EMEN'INT BYREASON OFTI;HE DISEASE* (1939-1947)
Yearly averageIndustrv or Process No. of (nearest whole
certificates number)
Refractories Industries. 153 17Sandstone Industry .. 306 34Pottery Industrv .. 474 53Asbestos Industrv IO3 IIMetal Grinding In-
dustries .. .. 35 4Coal Mining Industry 1 , 66 2,130Masons and Stone
Dressers .. .. 220 24Sandblasting anid Steel
Dressing .. 2I8 24Metalliferous Mining so8 12Haematite Mining In-
dustry .. 8I 9Slate Mining Industry 157 IOther Industries 210 23All .. .. 20,885 2,32I
* The disease means silicosis, asbestosis or pneumo-coniosis or any of these diseases accompanied bytuberculosis.
The absolute numbers are impressive, but theirrelative significance involves consideration of manyfactors. Thus in the pottery industry 53 cases ina year may not seem a large number unless it isappreciated that they accrue from a population of6,ooo workmen (Meiklejohn, 1949). This is evenmore cogent in relation to sand-blasters and steeldressers (Merewether, I936). By contrast thepopulation at risk underground in coal mines(55o,ooo) helps account for the large total of casesbut does not reveal that the certified cases arealmost entirely derived from South Wales (65,000underground workmen) (Fletcher, I948). Be-tween IgIg and I927 the average annual incidenceof cases in the metal grinding industries inSheffield alone was 30 as against 4 at present forthe whole of Great Britain. This reflects the re-placement of sandstone grindstones by non-siliceous wheels, which has taken place since I928.The related social problems are alarming and
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

604 POSTGRADUATE MEDICAL JOURNAL December I949
admit of no complacency; workmen's com-pensation is no solution. Morris (1947) andMeiklejohn (I947, I949) have dealt with these incoal-miners and pottery workers respectively.Coal-miners may be taken as an example. It isestimated that every single certified case involvescompensation payments to the workman and hisdependants of at least £i,ooo. This means thatthe coal mining industry since I939 has acquiredan average annual liability of £Z2,ooo,ooo. Evenmore important is the fact that the men involvedare the most highly skilled face workers at theheight of their production. Every certified caserepresents the loss of I0 to 20 years' man-output.Many are only partially disabled and require re-settlement in alternative employment, a peculiarlydifficult problem in areas so long restricted toheavy industry.. Most serious of all is the driftof population from the mines and the miningareas; wastage of man-power exceeds recruitment.In varying degree this picture is true of all dan-gerous dusty trades. Over one hundred years agoCalvert Holland (I843) wrote this of Sheffieldgrinders' asthma:
' It will also be obvious, from the various factsbrought under consideration, that the evils mustin various ways be felt by every portion of thecommunity, vice, ignorance and destitution, exerta widely pervading influence. The inability of theartisan to continue his occupation from disease,throws him and, perhaps, a numerous family, uponthe parish for support, not in a few solitary cases,but in hundreds of instances; and it is scarcelynecessary to observe that on his death the samedependence, if not indeed in an aggravated form,becomes indispensable for years. When the parishis not burthened in this stage of suffering, theinjury to society, from the inadequace struggles ofthe afflicted artisan to live, is scarcely in anydegree mitigated. The children, without havingreceived any education at all, are put to work atseven, eight and nine years old, from which cir-cumstances, and the fruitful consequences whichflow from them, in a later stage, additional claimsupon the parish funds are created, or ignoranceand immorality extend, maintaining low and de-praved habits of feeling among the labouringclasses.'
Social legislation may have advanced buteffective practice still lags far behind knowledge.
SilicosisSilicosis is the specific variety of pneumo-
coniosis due to the inhalation of silica dust. Itsoccurrence is world-wide, affecting all races, malesand females alike. In relation to the pathologicallesion, Haldane's (I914) assertion that' the diseaseis the same all over the world, and the end comes
through tubercular infection' is fundamentallytrue. The incidence and severity of the diseaseand the accompanying clinical manifestations inparticular communities, however, by reason ofdifferent industrial practices, associated dusts,racial constitution and habits and climatic con-ditions, vary considerably from one country toanother. This is equally true within a singlegeographical area as exemplified by the disease inStaffordshire potters, Cornish tin miners andAberdeen granite masons. Likewise there aredifferences within an industry as observed infoundry workers and even among workers in thesame occupation. These significant matters areall too often overlooked both by writers andreaders. Nevertheless certain facts are of generalapplication and provide the background againstwhich the problem in particular industries orprocesses may be studied.
Silica is widely distributed in nature, forming70 per cent. of the earth's crust. It is the chiefconstituent of many rocks and also# occurs asflint and natural quartzose sands. In addition tobeing abundant, readily available and compara-tively cheap, it has certain qualities peculiarlyvaluable in industry. Thus it is insoluble in allacids except hydrofluoric (pottery manufactureand glass making), highly abrasive (metal grindingand sand blasting) and refractory to very hightemperature (brickmaking for furnace linings andmoulding in foundries).
All processes which involve the manipulation ofsilica, especially in the dry state, in such a waythat it is broken up into minute particles andinhaled, are liable to produce silicosis. Thus inGreat Britain the disease is associated with coaland metalliferous mining in siliceous strata,dressing and cutting of sandstone, grinding ofmetals on sandstone, pottery manufacture, makingof silica bricks (the refractories industries) and infoundries, the cleaning and freeing of castingsfrom adherent sand. In these industries largenumbers of men and women are at risk, but thereare many other operations such as flint crushing,packing of scouring powders, tunnelling and thecleaning of the stonework of sandstone buildingsin which the exposure may be very intense thoughinvolving only a small number of workmen. Aswill appear later the purpose of the occupationalhistory of a patient suspected to be suffering frompneumoconiosis is to define the period, intensityand character of the dust hazard. In the pro-duction of the disease it is generally accepted that:
i. The silica must exist in the crystalline formas free silicon dioxide.
2. To gain entrance to the lungs and establisheffective occupation, the particle size must beunder io microns.
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

lDenember I949 MEIKLEJOHN: Pneumoconiosis -605
~..
FI.3- aeae 3yer;tnelrdilin islcar k,3 ye s. Geeaie core siioi.
3. The dust particles are most active whenunder 2 microns in diameter and freshly fracturedmechanically or by heat at very high temperatures;this ensures the maximum superficial area relativeto size.
4. The intensity and period of exposure are in-versely proportional so that if the dust cloud isvery intense the period necessary for developmentof the disease is correspondingly short and viceversa.
5. The action and reaction are intensified byinfection, notably tuberculosis, and the growth ofthe tubercle b?.ciJ1us is favoured.Under present conditions in Great Britain,
silicosis in a diagnosable stage seldom occurs underI5 to 20 years' exposure to the risk, and so israrely seen under the age of 40 years. If adequateprecautions to control the dust cloud are not takenor effectively maintained then the disease mayoccur in flint crushers, rock tunnellers, sandblasters and scouring powder packers after two tofive years' exposure. The writer once observed agroup of cases in flint crushers after less thantwelve months in the process. While in veryintensive risks it is almost certain that every work-man will be affected, in the ordinary run of in-dustry it is not inevitable that every workmanshould contract the disease in the course of aworking lifetime. There is a personal con-stitutional factor involved in the development and
progression of the disease. This factor has notbeen defined, though infection, especially tubercu-losis, is suspect.
Pathology and Course of SilicosisWith every breath the workman inhales the
dust, sometimes the concentration is high, some-times low. The coarse particles are arrested andrejected bv the natural defences of the respiratorytract, whiie the finest particles gain access to thealveoli from wbich they are transferred byscavenger cells and aggregated in the lymph nodeswithin the lung parenchyma under the pleura andat the hilum. Over a period of years the attackgoes on and the occupation of the lungs by thedust advances. All the while a reaction is oc-curring in the lymph nodes, which is finally re-vealed by the appearance of tiny spherical nodulesof fibrosis. Slowly these nodules increase indiameter and others appear elsewhere. Individualnodules achieve a size up to 5 mm.; contiguousnodules become confluent and in the most ad-vanced stages large ' cricket ball' masses result.These fibrous areas diminish the amount of func-tional lung so the healthy areas try to compensate.The lung between the fibrous areas becomesemphysematous and bullae appear along the freemargins. The bed of the pulmonary circulationbecomes greatly extended and narrowed and thisis reflected by hypertrophy of the right ventricle.
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

6o6 POSTGRADUATE MEDICAL JOURNAL December I94)
SX.
.2 f>
FIG. 4.-Male aged 72 years; coal-miner (Scotland),56 years. Bilateral massive silicosis with bullousemphysema at apices.
(Reprodutced by couirtesy of Drs. Sutherland and Tyrrell, Pncumno-coniosis Medical Board)
An indolent pleurisy anchors the lungs to thechest wall,9 diaphragm, pericardium and media-stinum. At first the changes are localized in theroot zone or the upper lobe of one lung, usuallythe right, but slowly and inevitably the diseaseappears in the contralateral lung and so it advancesin both. But it is not necessarily an orderlyadvance, indeed it rarely is; from the stage oflocalized nodulation massing may result evenbefore the nodulation has extended elsewhere.This is usually suggestive of an infective process.At any stage overt tuberculosis may appear andlead to a fatal outcome. In the absence of tubercu-losis the advance is slow but death may be pre-cipitated by acute intercurrent disease such as in-fluenza or pneumonia, while in older patientsdeath may occur from cardiac failure.The foregoing description indicates a slowly
developing continuous process and some maywonder why so long a period elapses before thedisease can be diagnosed. The explanation wouldappear to be that a substantial period is necessaryto complete the silica reaction. Moreover, in thebeginning the individual nodules are very minuteand the fibrous tissue immature. The actualidentification of the disease during life depends onthe appearance of abnormal radiographic opacitiesin the lung fields and presumably these must be
FIG. 5.-Male aged 50 years.; colliery fireman 21 years,then steel-dresser i2 years. Massive silicosis anddust reticulation.
(Reprodiuced by courtesy of Drs. Suitherland and lyrrell)
of a certain minimum size and radio-opacity(maturity of fibrous tissue) before they can bedistinguished from the normal structures of thelungs. These are personal opinions but aresupported by the fact that occasionally at necropsythe extent of the disease is considerably greaterthan is revealed by a recent radiograph, andindeed histological examination may establish thepresence of the disease when the radiograph is con-sidered normal. This is particularly true in acuterisks such as sand-blasters. The fact that patho-logical examination is more precise than radio-graphic examination does not invalidate the factthat during life the diagnosis of the disease mustinclude demonstrable X-ray changes in the lungs.
DiagnosisIn life the diagnosis depends on the following
triad, and while any of these may lead one tosuspect the presence of the disease, it mustultimately be firmly based on all three. Anyanomaly should raise doubt in the mind of thephysician, indicating the need for further investiga-tion and even for a visit to the place of work toinvestigate the actual environmental circumstancesof the particular case.
i. Clinical history and examination with specialreference to symptomatology.
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

Derember 1949 MEIKLEJOHN: Pneumoconiosis 607
...
FIe. 6. Male aged 39 years; flint crusherman for I4 months; no other dust risk.Massive silicosis; died 4 years later of congestive heart failure; diagnosis ofsilicosis without tuberculosis confirmed post-mortem.
2. The history of the occupational risk to defineprecisely the period and intensity of the silicarisk.
3. Radiographic examination of the chest.
Clinical and Related AspectsFor a period of years, save in very serious dust
hazards, the workman, though inhaling silicaparticles regularly at his job, is unaware of anyinjury to health; the pathological process islatent, the onset of the disease insidious. Duringthis phase radiographic examination of the chestmay disclose definite silicotic changes but thepatient denies any inconvenience. This, however,is not strictly true for close questioning will usuallyreveal that he is troubled by a cough and slightbreathlessness on exertion. He is fully aware ofthese symptoms but has dismissed them as due tosmoking or his ' age.' The cough is dry andharsh, occurring in bouts first thing in the morningor last thing at night. The shortness of breath isreflected by the fact that he now prefers to ridewhere he had previously walked, or if he does walkhis pace is slower and he is aware of the hills.Then suddenly and indirectly the disease in thelungs is discovered. The workman suffers from a' cold' or an attack of influenza; recovery is de-layed while the cough and breathlessness areaggravated. Even so his general condition is
good; he is not sick, only distressed. At thisjuncture he becomes the victim of a host of ex-traneous aggravating circumstances. Con-valescence is prolonged and sick benefits in-adequate; the family begins to run into debt.The doctor advises an X-ray examination of thechest and the diagnosis of early silicosis is con-firmed. Anxious as the workman may be to re-turn to work, this must be postponed for thedoctors and his trade union have advised a claimfor compensation. This involves more delay dur-ing which his domestic problems increase and hismind is focused on his chest. All the while thework habit is slowly being lost. He is sick withfear and worry; he knows the doctors are notmistaken because 'it is on the X-ray.' Some-where and to someone this tragedy happens everyday, a tragedy in which the practice of the art ofmedicine and the well-being of an individual andhis family are sacrified on the altars of scientificmedicine and the welfare state. Facts triumph overjudgment, life becomes more important than living.The change to an easy cough with muco-
purulent sputum, occasionally blood-stained, lossof appetite, weakness and wasting indicateassociated tuberculosis. The patient is nowobviously a sick man and thenceforth deteriorationis rapid.
In simple silicosis even when the changes in
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from
6o8 POSTGRADUATE MEDICAL JOURNAL December 1949
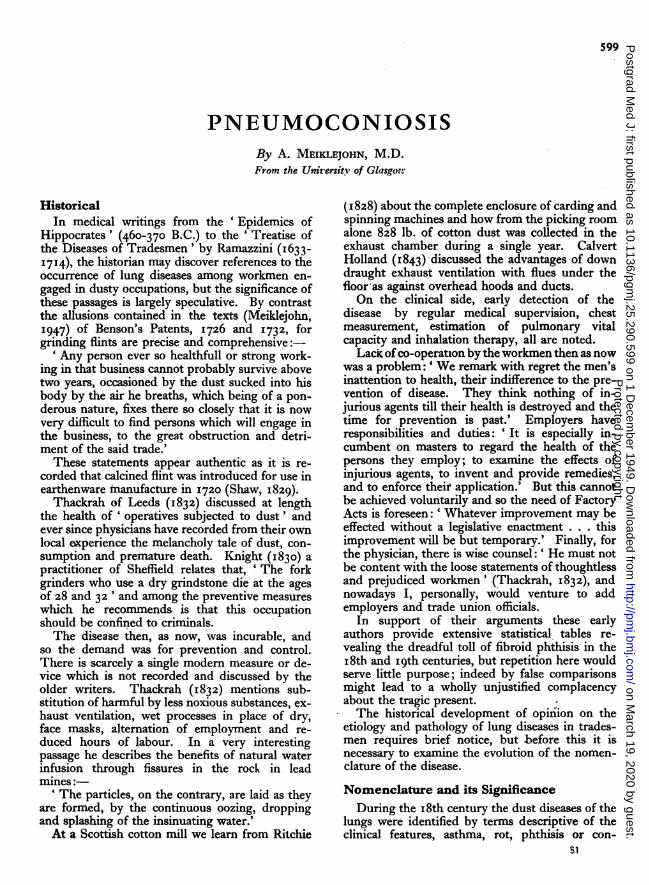
FIG. 7.- Female aged 32 years; china polisher (potterypure flint risk), I9 years. No specific appearancesof silicosis.
the lungs and pleura are gross, clinical examinationof the chest yields remarkably little information;it is a silent disease. Inspection properly carriedout as a definite technique is probably superior toall other methods of examination, but un-fortunately so few doctors nowadays take time tolook at the patient. The excerpt quoted fromCalvert Holland (see page 6oo) is a salutary reminderof how much we have sacrificed to instrumentalaids. Important points to note are the generalcondition and facies, response to the effortof undressing, configuration and movement ofthe chest, line of the trachea and, if visible, theposition and extent of the cardiac impulse.Cyanosis occurs only in advanced disease and thenonly if associated with cardiac embarrassment;clubbing of the fingers is very exceptional. Areasof fibrosis cannot be mapped out by percussionbut when massing has occurred near the apex ofthe upper lobe dulness may be noted posteriorlywith resonance, due to emphysema, anteriorly. Onauscultation one is impressed by the patchydiminution or absence of breath sounds andadventitia due to bronchitis and pleurisy are rarelyaudible. The heart is seldom displaced or en-larged; obvious enlargement usually signifies con-
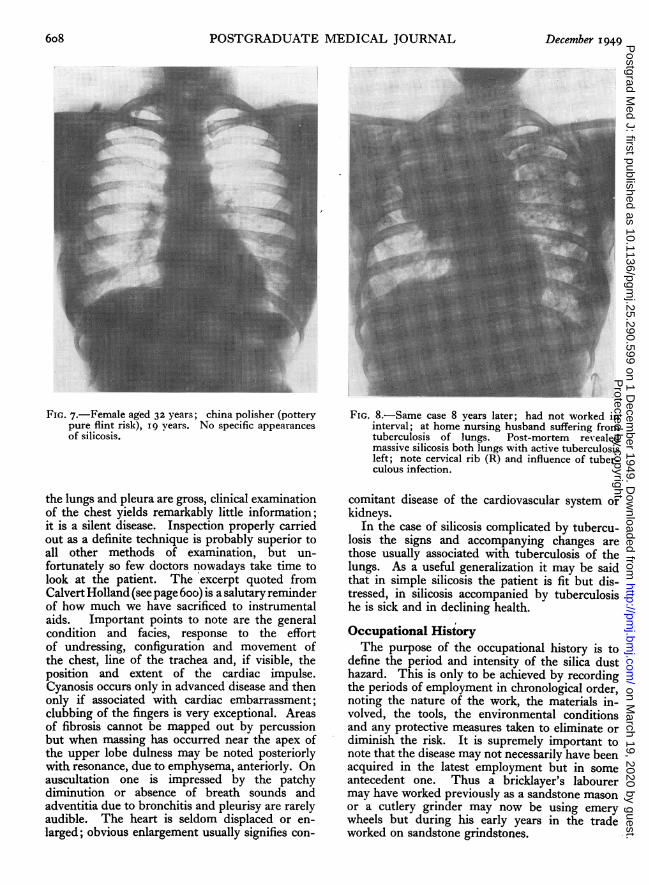
FIG. 8.-Same case 8 years later; had not worked ininterval; at home nursing husband suffering fromtuberculosis of lungs. Post-mortem reI-ealedmassive silicosis both lungs with active tuberculosisleft; note cervical rib (R) and influence of tuber-culous infection.
comitant disease of the cardiovascular system' orkidneys.
In the case of silicosis complicated by tubercu-losis the signs and accompanying changes arethose usually associated with tuberculosis of thelungs. As a useful generalization it may be saidthat in simple silicosis the patient is fit but dis-tressed, in silicosis accompanied by tuberculosishe is sick and in declining health.
Occupational HistoryThe purpose of the occupational history is to
define the period and intensity of the silica dusthazard. This is only to be achieved by recordingthe periods of employment in chronological order,noting the nature of the work, the materials in-volved, the tools, the environmental conditionsand any protective measures taken to eliminate ordiminish the risk. It is supremely important tonote that the disease may not necessarily have beenacquired in the latest employment but in someantecedent one. Thus a bricklayer's labourermay have worked previously as a sandstone masonor a cutlery grinder may now be using emerywheels but during his early years in the tradeworked on sandstone grindstones.
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

December 1949 MEIKLEJOHN: Pneumoconiosis 609
Radiographic Examination of the ChestIt is generally accepted that the radiographic
findings in'silicosis afford the most reliable singlepiece of evidence in establishing the existence andactual stage of the disease in any particular case.This, however, is only true if the radiograph istechnically satisfactory, properly exposed and care-fully processed. The, radiographic appearancesare represented by changes which reflect thecharacteristic pathological lesion. In the earlystages they comprise small opacities, variouslydescribed as nodulation or mottling, at firstlocalized and later in classical silicosis involvingthe whole lung fields, thus presenting a ' snow-storm) appearance. When the disease is con-fluent, massive. shadows appear usually in theroot or' sub-apical zone; it is very rare for anisolated opacity to occur in the basal area. Whenactive tuberculosis supervenes the whole pictureis modified and continues to alter with the advanceof the tuberculous process.
Frequently when the patient is first seen thewhole clinical and radiographic picture is that ofextensive tuberculosis of the lungs, but chiefly forreasons related to workmen's compensation theclinician must decide whether or not silicosis ispresent. It is useless to believe that in suchcases one can distinguish radiographically betweensilicotic and tuberculous opacities. In such cir-cumstances a presumptive diagnosis only ispossible based almost entirely upon a criticalassessment of the occupational risk.
Differential DiagnosisIf the case is investigated as outlined above, then
almost absolute accuracy can be achieved in therecognition of silicosis and its complications.Difficulty only arises in the earliest stage in an'attempt to anticipate the disease radiographicallyand in the determination of associated tubercu-losis. It is usual, however, to record that thedisease must be differentiated from miliarytuberculosis of the lungs (acute and chronic), car-cinoma of the lung especially miliary carcino-matosis, haemosiderosis in mitral disease, sar-coidosis, bronchomycoses, virus infection of thelungs, tropical eosinophiiia, bilharziasis, ascariasisand retained radio-opaque dust. While it is truethat these conditions may on occasion closelysimulate the radiographic appearances, X-rayexamination of the chest, absolutely indispensableas it is, is only a single factor in clinical diagnosisand must be recognized as such. While it is trueto say that radiology has contributed more thanany other method to the accurate recognition ofthe disease, it is no less true that the dramaticradiographic appearances have warped clinical
judgment and obsessed trade union officials oftento the detriment of the individual patient.
Prognosis, Management and Treatment.Simple silicosis, even of advanced degree, is
compatible with many years of life and con-siderable capacity for work in the patient's ownskilled job. There is no reliable evidence thatsilicotic patients are more liable to acute respiratoryinfections than their fellows and even if they are,the danger of contracting these is no greater atwork than in their own homes or at the streetcorner. If they do suffer such an illness recovery isoften delayed and bronchopneumonia may befatal. The important issue which arises is whatadvice should be given to a patient about his job.On first principles he should not again exposehimself to any dusty work. This is the advicewhich is regularly given, but it altogether ignoresa whole host of equally important social factors.He must work, not for economic reasons alone, butparadoxically because work is the only treatment'ofany real value for him and, strangely enough, forhis wife and family. If under the age of 40 years,an age at which he is still adaptable and has youngdependants, he should seek alternative employ-ment, but this is supremely important, he shouldnot give up his work until he is assured that thealternative job is available, secure and suited to hiscapacity. Over 40, unless he is fortunate infinding a suitable alternative job, then he shouldcontinue in his own skilled work. It is the job heknows and can accomplish with the minimumeffort. If the hours of work can be adjusted forhim so much the better. Craftsmanship, self-respect and happy living are inseparable and alltoo often to sacrifice one's craft is to lose all. Itis not disputed that there is danger in continuing towork in the dust, but the danger is relative andmust be assessed accordingly. The craftsman isintelligent and if left to make the choice prefers towear rather than rust out.
Active tuberculosis may become manifest atany stage so it is important that the silicotic work-man should be under regular periodical medicalsupervision. As a means of detecting the transitionfrom simple to complicated silicosis E.S.R.(erythrocyte sedimentation rate) tests have beenadvocated but, in this matter, there is nothingsuperior to the shrewd clinical observation andjudgment of the experienced physician.
In silicosis accompanied by tuberculosis theworkman must give up his employment not onlyto safeguard himself but his fellows. As a generalrule this is no undue hardship as he is or soon willbe totally unfit for work and present rates of com-pensation and additional benefits approximate tohis previous earnings.
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from

61o POSTGRADUATE MEDICAL JOURNAL December i949
Treatment is almost entirely restricted to reliefof symptoms. In the case of the partially dis-abled workman emphasis has already been made onthe importance of work. Therapy by means ofinhalations of powdered metallic aluminium is atpresent under trial in Canada and in this country,but the method is still in the experimental stage.
Prevention and ControlThis is the only satisfactory approach to
the problem and the principles are reasonablywell-defined. Wherever possible non-injuriousmaterials should be substituted for silica; thus incutlery grinding, carborundum and alundum havereplaced sandstone grindstones, in china manu-facture alumina has replaced flint and in sandblasting non-siliceous abrasives have been sub-stituted for quartzose sand. It should be notedthat due to the chronic nature of the disease thebeneficial results of these measures are not im-mediately reflected in morbidity and mortalitystatistics; one must wait the passing of the oldgeneration. Mechanization of processes is anothervaluable method whereby the number of men atrisk is substantially reduced. The intensity of thenoxious dust cloud can be reduced by effective
exhaust ventilation and the use of wet methods inplace of dry. Respirators are of limited valueeither because they fail to arrest the most dan-gerous minute particles or because they are un-comfortable for continuous wear during heavywork. Other aids are comprised in good house-keeping in the factory. Inhalation of powderedaluminium metal for therapeutic purposes hasalready been mentioned. The same method isbeing applied as a prophylactic measure, but dueto the nature and course of the disease many yearsmust elapse before any opinion as to its value canbe pronounced.
ConclusionThe foregoing account has necessarily been
restricted to general consideration of the subject..Particular occupations and centres of industryhave individual characteristics and social prob-lems. Some of these will appear in the con-tributions which follow.
AcknowledgmentI am greatly indebted to the Ministry of
National Insurance for permission to publish thetable on page 603.
BILIOGRAPHYAct to amend, consolidate and extend the law relating to miners'
phthisis (1946), South Africa, No. 47.AGRICOLA, G. (ISS7), 'De Re Metallica.'BELT, T. H., and FERRIS, A. A. (1942), ' Spec. Rep. Ser. Med.
Res. Coun.,' London, No. 243.COLLIS, E. L. (I'9I5), ' Industrial Pneunonoconioses, with special
reference to Dust Phthisis,' Milroy Lectures, IgIs, H.M.S.O.,London, I9 I9.
DENNY, J. J., ROBSON, W. D., and IRWIN, D. A. ('937),'Prevention of Silicosis by Metallic Aluminium; PreliminaryReport,' Canad. Med. Ass. 37., 37, '.
DENNY J. J., ROBSON, W. D., and IRWIN, D. A. (1939a),' Prevent n of Silicosis by Metallic Aluminium,' Ibid., 40, 213.DENNY, J. J., ROBSON, W. D., and IRWIN, D. A. (1939b),
Industr. Med 8, 133.DIEMERBROER, quoted by Thackrah (I832), pp. 85-86.FARR (I875), 'Fifth Report of the Registrar General,' H.M.S.O.,
London x87SFLETCHER, C. M. (I948), 'Pneumoconiosis of Coalminers,'
Brit. Med.7 I,I,OI5, I065.GARDNER, L. 1J. (1920), 'Studies in Relation of Mineral Dusts
to Tuberculosis,' Amer. Rev. Tuberc. Balt., 4, 734-755.GOUGH, J. (1940),.Y. Path. Bact., 51, 277.GOUGH, J. (I947a), Occup. Med., 4, 86.GOUGH, J. (I947b), 'Proc. Instn. Min. Engrs. and Instn. Min.
Metall. Silicosis Conf.,' London. P- 7,GREGORY, J. C. (I831), 'Case of peculiar Black Infiltration of the
whole Lungs resembling Melanosis,' Edinburgh Med. Y., 36,w8 Q-34GYE?, M. EI., and KETTLE, E. H. (I922), Brit. 37. Exper. Path.,3, 241.
GYE, W. E., and PURDY W. J. (I922), Ibid., 3,75-94.GYE W. E., and PURDY, W. J. (1924), Ibid., 5, 238-250.HALbANE, J. S. (I914), as quoted in 'Second Report of the
Royal Conmmission in Metelliferous Mines and Quarries,' p. 14T,H.M.S.O., London, 1914.HALDANE, J. S. (1917), Trans. Inst. Min. Eng., 55, 264.HALL, J. C. (I857), 'On the Prevention and Treatment of the
Sheffield Grinders' Disease,' London, I857.HART, P. D'ARCY, and ASLETT, E. A. (1942), ' Spec. Rep. Ser.
Med. Res. Counc.,' London No. 243.HEFFERNAN, P. (1946), Brit. wed:j., x, 928.HEFFERNAN, P., and GREEN, A. T. (1928), 'The Method of
Action of Silica Dust in the Lungs,' 7. Industr. Hyg., to,272-278.
HOLLAND, G. C. (1843), ' Diseases of the Lungs from MechanicalCauses,' John Churchill, London.
INTERNATIONAL L,ABOUR OFFICE (1938), 'Studies andReports, Series F (Industrial Hygiene),' No. 17, Geneva, 1940.
JONES, W. R. (I933), 'Silicotic Lungs: Minerals they Contain,'J. Hyg., 33, 307-329.
JONES, W. R. (I934.), 'Silicosis: The Harmful Dusts whichCause It,' Trans. Brit. Ceram. Soc., 34, 303.
KETTLE, E. H. (I935), J. Path. Bact., 35, 395.KING, E. J. (1945), 'Spec. Rep. Ser. Med. Res. Coun.,' London,
No. 250.KNIGHT, A. J. (I830), North of England Medical and Surg. J.,
.I 174.LAENNEC, R. T. H. (i8i8), Traitide l'Auscultation mediate. Tomb.
I, p. 212.McCRAE, J. (I913), 'The Ash of Silicotic Lungs,' S. African Inst.
Mes. Res.MEIKLEJOHN, A. (I947), 'Silicosis in North Staffordshire
Pottery Industry,' Trans. Brit. Ceramic Soc., 46, 132.MEIKLEJOHN, A. (1949), 'Health Problems of the Potteries,'
University of Manchester .7. Industr. Nurses, I, 24.MEREWETHER, E. R. A. (I936), 'The Risk of Silicosis in Sand-
blasters,' Tubercle, pp. 385-39I.MIDDLETON, E. L. (1936),' Industrial Pulmonary Disease due to
Inhalation of Dust with Special Reference to Silicosis,' (MilroyLecture), Lancet,. 2, I, 59 (Lit. of Silicosis) (I940), Proc.Internat. Conf. Silicosis, London.
MORRIS, J. N. (I947), 'Coalminers,' Lancet, 2, 341.NATIONAL INSURANCE (INDUSTRIAL INJURIES) ACT,
1946.OGLE (I88s), 'Sixth Report of the Registrar General,' H.M.S.O.,
London.PENDERGRASS, E. P., and LEOPOLD, S. S. (1945), 'Benign
Pneumoconiosis,'_7. Amer. Med. Ass., X27, 701.RITCHIE, C. (1828) 'Remarks on the Medical Topography of
the Parish of Neilston,' Glasgow Med. 3., s, 286, 371.ROVIDA, C. L. (0871), 'Un caso di silicosi del pulmone, con
analisi chimica,' Annali di Chimica applicata alla med., p. 102,Milan.
SHAW, S. (I829), 'History of the Staffordshire Potteries and theRise and Progress of the Manufacture of Pottery and Porcelain,'re-issued by Scott, Greenwood and Co., London, Igoo.
STRATTON, T. (1838), 'Case of Anthracosis or Black Infiltrationof the Whole Lung,' Edinburgh Med. and Surg.J7., 59, 490-491.
THACKRAH, C. T. (1832), 'The Effects of Arts, Trades andProfessions and of Civic States and Habits of Living on Healthand Longevity,' Longmans London, 2nd edition.
VISCONTI, reported by ROViDA (s87'i), ' Un caso di silicosi delpuimone, con analisi chimica,' Annali di Chimica applicataalla med., p. Ia z, Milan.
ZENKER, F. A. (x866), 'Staubinhalations Krankheiten derLungen.'
Protected by copyright.
on March 19, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.599 on 1 D
ecember 1949. D
ownloaded from