pneumonia, prednisone, paradigm
TRANSCRIPT
1
Pneumonia, Prednisone, Paradigm?Corticosteroids in Community-Acquired Pneumonia
Cam Roessner, PharmD StudentMay 28, 2015

2
Learning Objectives
Describe the rationale for adjunctive corticosteroids in the treatment of community-acquired pneumonia
Evaluate and summarize the evidence for adjunctive corticosteroids in community-acquired pneumonia
Recognize the strengths and limitations of available evidence
Prioritize the role of corticosteroids in patients presenting with community-acquired pneumonia

3
Outline
Background
Rationale for Corticosteroids in CAP
Rationale and Evidence for Corticosteroids in Infectious Diseases
Corticosteroid Controversy Review of Current Evidence Discussion and Opinion Remaining Questions
Summary

4
Community-Acquired Pneumonia (CAP)
Infection of the lung parenchyma occurring in patients living independently in the community, including those hospitalized for other reasons for < 48hrs
Symptoms are variable between patients but often patients present with cough, sputum, and dyspnea in the setting of fever and crackles/rales on auscultation
Presence of lobar consolidation with decreased breath sounds and leukocytosis help to confirm the diagnosis
A microbiological cause is established with certainty in approximately 50%
Infection may bacterial, viral, fungal, or parasitic in origin
Limper, A. H. (2012)

5
CAP – Common Infectious Causes
Bacteria Viruses Other
S. pneumoniae† Influenza A and B M. pneumoniae
H. influenzae† Respiratory syncytial virus C. pneumoniae
S. aureus Rhinovirus P. jirovecii
M. catarrhalis† Aspergillus spp.
P. aeruginosa
†Account for > 80% of cases of community-acquired pneumonia
Limper, A. H. (2012), Feldman, C., & Anderson, R. (2015)

6
CAP – Incidence and Costs
Every year community-acquired pneumonia affects 2 to 4 million patients in the U.S., resulting in 500,000 hospital admissions
Hospitalized patients with CAP have a 30-day mortality rate of 10-12%, and in those who survive, the risk of mortality remains elevated at 1 year and up to 3-5 years in those with pneumococcal pneumonia
About 18% of patients are re-admitted to hospital within 30 days of discharge
The treatment of inpatient CAP in the U.S. is estimated to cost $8.6B annually, with a daily fixed cost of $1,448 $USD and an average stay cost of $13,009 $USD
NEJM 371(17), 1619-1628, Curr Med Res Op 25(9), 2151-2157

7
CAP – Risk Factors
Virulence Factors Current or recent influenza virus
infection Bacterial-specific virulence
Drugs Acid-suppression Antipsychotics Corticosteroids
i.e. increased pneumonia risk with ICS in COPD patients
Patient Factors Age Decreased LOC Tobacco smoke Alcohol consumption Cystic fibrosis COPD HIV infection
Cochrane Sys Rev CD006829, European Respiratory Journal, 13(2), 349-355

Ellison, R. T., & Donowitz, G. R. (2015) 8
CAP – Why Corticosteroids?
Pathophysiology of Inflammation in Pneumonia
1. Alveolar and interstitial macrophages mediate the inflammatory response and produce cytokines when invading pathogens overcome their phagocytic abilities
2. Early-response cytokines include tumour necrosis factor-α (TNF- α) and IL-1
3. Cytokines and transcription factors promote pro-inflammatory recruitment of neutrophils to the lung AND anti-inflammatory safety measures aimed at preventing tissue destruction

9
CAP – Why Corticosteroids?
In patients admitted with community-acquired pneumonia…
Excessive cytokine production (pro-inflammatory and anti-inflammatory) resulted in an increased risk of sepsis and mortality
The risk of mortality remained elevated at 3-6 months post-discharge
Archives of Internal Medicine, 167(15), 1655-1663,
10
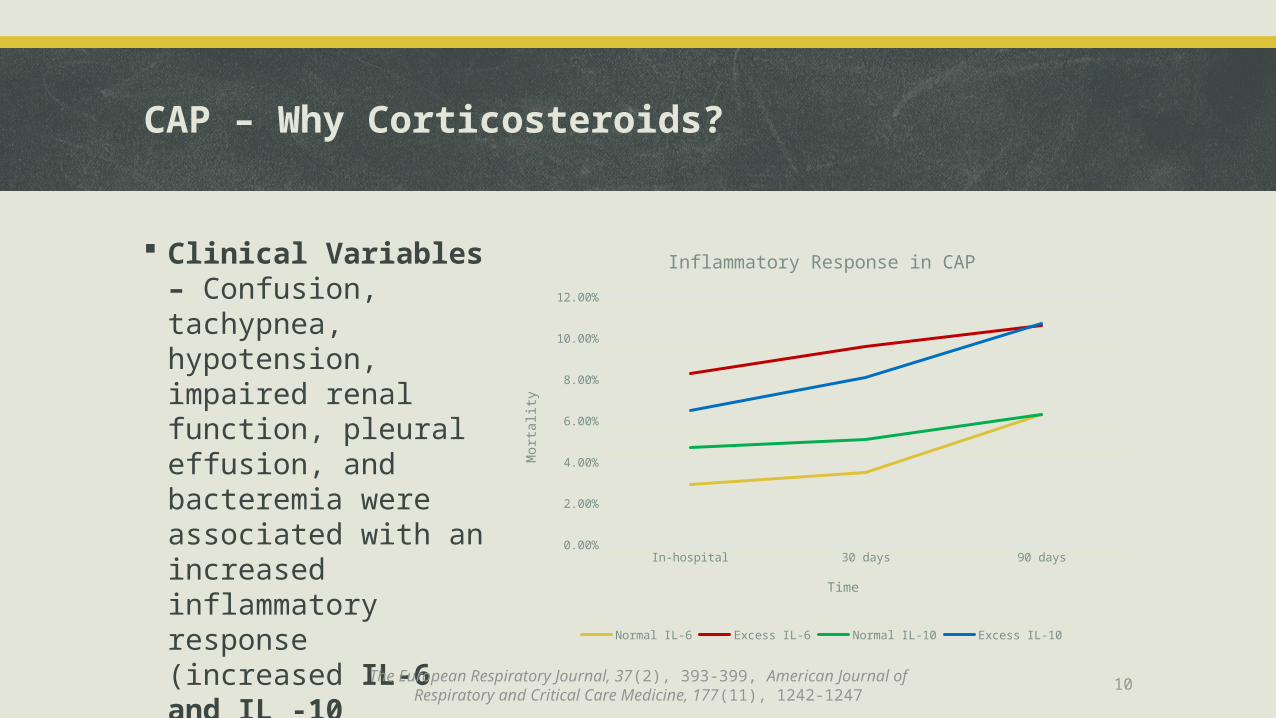
CAP – Why Corticosteroids?
Clinical Variables – Confusion, tachypnea, hypotension, impaired renal function, pleural effusion, and bacteremia were associated with an increased inflammatory response (increased IL-6 and IL -10 cytokines) and increased mortality In-hospital 30 days 90 days
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
Inflammatory Response in CAP
Normal IL-6 Excess IL-6 Normal IL-10 Excess IL-10
Time
Mor
talit
y
The European Respiratory Journal, 37(2), 393-399, American Journal of Respiratory and Critical Care Medicine, 177(11), 1242-1247
11
Adjunctive Corticosteroids in Infectious Diseases
Bacterial meningitis
In experimental models, severity of subarachnoid inflammation (due to the immune response and bacterial lysis following antibiotic administration) lead to worse outcomes
Evidence (dexamethasone) Reduces mortality in patients with S.pneumoniae bacterial meningitis Reduces hearing loss and neurological sequelae in developed countries NOTE: Mortality benefit of dexamethasone in pneumococcal meningitis was due to a
reduced risk of systemic complications (i.e. septic shock, acute respiratory distress syndrome, and pneumonia) and NOT neurological seqeulae
NEJM 347(20), 1549-1556, The Cochrane Database of Systematic Reviews, 6, CD004405, Annals of Internal Medicine, 141(4), 327

12
Adjunctive Corticosteroids in Infectious Diseases
Tuberculous meningitis Similar rationale to bacterial meningitis Evidence
Reduces mortality and disabling residual neurological deficits (i.e. ability to perform ADLs/IADLs) in HIV-negative patients with tuberculous meningitis
Pneumocystis pneumonia Clinical status of patients generally worsen within 3 days of starting anti-pneumocystis
therapy as killed pneumocystis organisms stimulate inflammation Evidence
Reduces mortality in HIV-positive patients with pneumocystis pneumonia and substantial hypoxemia (arterial oxygen partial pressure < 70mmHg)
NNT of 9 without HAART and 23 with HAART
Cochrane Database of Systematic Reviews, (1):CD002244, (4):CD006150

13
Current Guideline Recommendations
Community-Acquired Pneumonia (IDSA) Hypotensive, fluid-resuscitated patients with severe CAP should be screened
for occult adrenal insufficiency. (Moderate recommendation; level II evidence.)
Corticosteroid replacement therapy in patients with severe CAP and septic shock can be used in documented adrenal insufficiency
New IDSA guidelines in development!
Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America, 44 Supplement 2, S27-72

14
CAP – Why Not Corticosteroids?
I want to know if...
In patients with community-acquired pneumonia requiring hospitalization, when added to antibiotic therapy, do
corticosteroids result in improved outcomes when compared to antibiotics alone?

15
Adjunct prednisone therapy for patients with community-acquired pneumoniaA multi-center, double-blind, randomized, placebo-controlled trial (Blum et al.)Lancet 2015; 385: 1511–18
16
Population
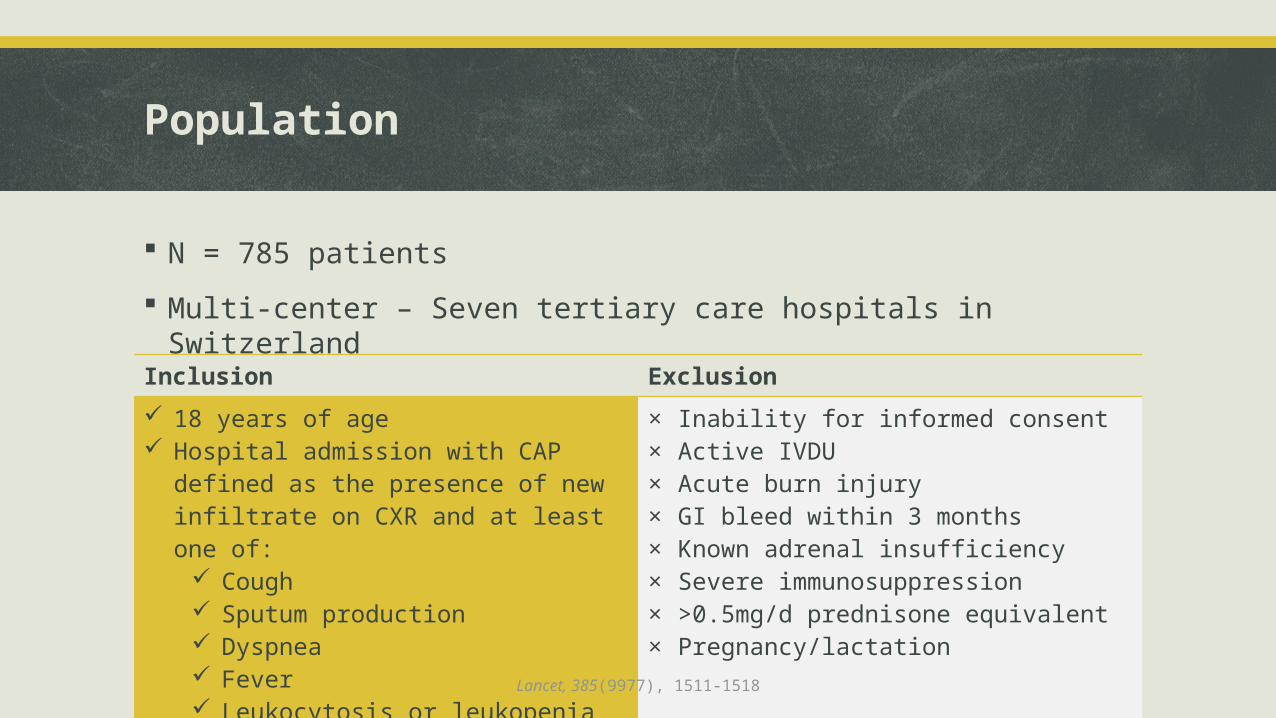
N = 785 patients
Multi-center – Seven tertiary care hospitals in Switzerland
Inclusion Exclusion 18 years of age Hospital admission with CAP defined as the
presence of new infiltrate on CXR and at least one of:
Cough Sputum production Dyspnea Fever Leukocytosis or leukopenia
× Inability for informed consent× Active IVDU× Acute burn injury× GI bleed within 3 months× Known adrenal insufficiency× Severe immunosuppression× >0.5mg/d prednisone equivalent× Pregnancy/lactation
Lancet, 385(9977), 1511-1518

17
Baseline Characteristics
Average Age: 74 years
Majority were male (62%)
No significant differences in days with symptoms (4), clinical presentation, lab values, PSI score, or comorbidities:
DM – 20% COPD – 19% vs. 15% CHF – 20% vs. 16% Renal Insufficiency – 32%
Half of patients were PSI class IV or V Average PSI score of around 90 – A score of 71-90 correlates with a mortality rate of 0.9%
Lancet, 385(9977), 1511-1518

18
Intervention & Comparator
1:1 block randomization, with centrally managed computer-generated allocation concealment to:
1. prednisone 50mg PO once daily for 7 days (n=392)2. identical placebo PO once daily for 7 days (n=393)
Patients, physicians, investigators, and adjudicators were blinded
Empiric antibiotic therapy was started according to ERS/ESCMID guidelines (i.e. amoxi-clav +/- macrolide, ceftriaxone +/- macrolide, etc.) as soon as CAP was confirmed
Treatment was optimized after the susceptibility patterns were known
Lancet, 385(9977), 1511-1518
19
Outcomes
Primary Outcome Time to clinical stability – Number of days until stable vital signs (≤ 37.8ᵒC, HR < 100,
RR < 24, SBP ≥ 90mmHg with no vasopressors, baseline mental status, oral intake, adequate oxygenation on room air) for 24h or longer (all criteria needed to be met)
Secondary Outcomes• Time to effective discharge• Recurrence of pneumonia• Re-admission to hospital• ICU admission• All-cause mortality
• Duration of total and IV antibiotic treatment• CAP Score at day 5 and 30• Incidence of complications• Side-effects of corticosteroids• Time to earliest possible discharge
Lancet, 385(9977), 1511-1518

20
Follow-Up
Until death or 30 days post-discharge
No patients were lost to follow-up for the primary outcome
At Presentation/Hospital Baseline blood samples, nasal swabs for viral PCR, and clinical variables, including those
used to calculate a pneumonia severity index (PSI) Routine laboratory markers of inflammation on days 1, 3, 5, 7 and before discharge Four glucose measurements per day
Community At 30 days, a phone follow-up assessed for infections, recurrent pneumonia, re-
admission to hospital, new onset diabetes or insulin dependence, and new onset hypertension
Lancet, 385(9977), 1511-1518

21
Results
Secondary Outcome Prednisone vs. Placebo Hazard Ratio (95% CI) P-valueTime to effective hospital discharge
6 days (6.0 – 7.0) vs. 7 days (7.0 – 8.0)
1.19 (1.04 – 1.38) 0.012
IV Antibiotic Duration Mean difference of -0.89 days for prednisone arm (-1.57 to -0.20)
0.011
Primary Outcome Prednisone vs. Placebo Hazard Ratio (95% CI) P-valueIntention-to-treat 3 days (2.5 – 3.4) vs. 4.4 days
(4.0 – 5.0)1.33 (1.15 – 1.50) < 0.0001
Per-protocol 3 days (2.5 – 3.2) vs. 4.4 days (4.0 – 5.0)
1.33 (1.16 – 1.56) < 0.0001
Lancet, 385(9977), 1511-1518

22
Results
Probability of Attaining Clinical Stability
Lancet, 385(9977), 1511-1518

23
Results
Side Effects of Corticosteroids
Adverse Event Prednisone vs. Placebo
Risk Increase (95% CI) P-value NNH
Any 24% vs. 16% 1.58 (1.14 – 2.17) 0.002 11
In-hospital hyperglycemia needing new insulin
19% vs. 11% 1.77 (1.22 – 2.92) 0.001 12
• Hyperglycemia• In-hospital and needing insulin start• New insulin dependence at day 30
• Hypertension
• Nosocomial infections• Weight gain• Gastrointestinal bleeding• Delirium
Lancet, 385(9977), 1511-1518

24
Commentary: Strengths
Largest trial to date of adjunctive corticosteroids for community-acquired pneumonia Reduced risk of a type II error, although not powered to detect a difference in mortality
Randomization, allocation concealment, and blinding was well done
Patients were analyzed according to the group they were randomized to (ITT) as well as according to treatment protocol (per-protocol)
Length of follow-up was reasonable (data has been collected for 180 days)
No patients were lost to follow-up for the primary outcome and only 4 (0.5%) were lost at 30 days
Amoxi-clav or ceftriaxone +/- clarithromycin were the antibiotics of choice (>90%)
Time to clinical stability can be considered a patient-important outcome (although the definition itself is a composite of surrogate markers)
Lancet, 385(9977), 1511-1518

25
Commentary: Limitations
Patients had lower severity pneumonia than previous studies (Average PSI score of 93 and 86) At baseline, average temperature, heart rate, respiratory rate, and blood pressure were stable already! About 65% of patients in each group had ≤ 2 instability criteria at baseline
Primary endpoint was combined (fever, tachycardia, tachypnea, normotensive, etc.) Concurrent medications were not discussed at all – some could impact patient “stability” (i.e. beta-blockers,
antipyretics, antiemetic)
Did not evaluate patients for a history of pneumococcal or influenza vaccinations, interventions thought to have a beneficial impact on pneumonia severity and mortality outcomes
What about patient risk factors for community-acquired pneumonia? Smoking and alcohol consumption were not discussed and are not a part of the risk scoring systems used (i.e. CAP
score)
Did not perform a sub-group analysis specific to an infectious organism – S.pneumoniae was the most commonly identified organism (12.% vs. 12.7%)
Are corticosteroids more effective against certain infectious etiologies? S.pneumonia?Lancet, 385(9977), 1511-1518, Archives of Internal Medicine, 167(18), 1938-1943, The American Journal of Medicine, 115(6), 454-461

26
Conclusions
Benefit on time to clinical stability regardless of age, CRP concentration, or severity of pneumonia (PSI score)
Trend towards increased benefit in patients with sepsis
Although complications were few (i.e. empyema, ARDS, pneumonia persistence) they tended to be (non-significant) lower in the treatment group
Discharged on average 1 day sooner, a previously described outcome with dexamethasone in community-acquired pneumonia
Short-term administration resulted in higher rates of hyperglycemia requiring insulin treatment however, other adverse effects were similar between groups
Lancet, 385(9977), 1511-1518, Jama, 313(7), 677-686
27
Effect of Corticosteroids on Treatment Failure AmongHospitalized Patients With Severe Community-AcquiredPneumonia and High Inflammatory ResponseA Randomized Clinical Trial (Torres et al.)JAMA. 2015;313(7):677-686

28
Design & Population
Multicenter, randomized, double-blind, placebo controlled trial
N = 120 patients at 3 Spanish teaching hospitalsInclusion Exclusion ≥ 18 years of age Clinical symptoms suggestive of CAP (cough,
fever, pleuritic chest pain, dyspnea) New infiltrate on CXR Severe pneumonia or PSI score of V CRP > 150mg/L at admission
× Prior treatment with corticosteroids× Nosocomial pneumonia× Severe immunosuppression× Medical condition with life expectancy < 3
months× Uncontrolled diabetes× GI bleed within 3 months× > 1mg/kg/d baseline methylprednisolone
Jama, 313(7), 677-686

29
Baseline Characteristics
Average age of ≈65 years
Majority were male (62%)
Less patients with septic shock in treatment group 17% vs. 31% Remaining clinical variables were similar
On average patients had a more sever presentation Higher respiratory rate and heart rate on average than study by Blum et al.
A majority were PSI class IV and V (≥70%) Average PSI score of 108 between the two groups – A PSI score of correlates with a
mortality rate of 9.3% (the study by Blum et al. had a PSI-related risk of 0.9%!)
Jama, 313(7), 677-686

30
Intervention & Comparator
1:1 randomization to pre-numbered boxes containing dosing units of either:1. methylprednisolone 0.5mg/kg IV q12h for 5 days started within 36 hours of
admission (n=61)2. identical placebo IV q12h for 5 days started within 36 hours of admission (n=59)
Patients, investigators, and adjudicators were blinded
Empiric antibiotic therapy was started according to IDSA 2007 community-acquired pneumonia guidelines (i.e. ceftriaxone + macrolide, fluoroquinolone)
Jama, 313(7), 677-686

31
Outcomes
Primary Outcome Rate of treatment failure – Early treatment failure (<72 hours of treatment), late
treatment failure (72 – 120 hours), or both Definition – Development of shock, need for invasive mechanical ventilation, or death
(late also included radiographic progression and persistence of severe respiratory failure)
Secondary Outcomes• Time to clinical stability• Length of ICU and hospital stay• In-hospital mortality
*Definition of time to clinical stability was similar to the previous study
Jama, 313(7), 677-686

32
Follow-Up
At Presentation: Sputum, urine, blood (× 2), and nasopharyngeal swabs CBC, renal and liver function tests, electrolytes, blood glucose, and CRP IL-6, -8, -10, procalcitonin, and CRP were obtained on treatment days 1, 3, and 7
Patients were evaluated daily for treatment failure and time to clinical stability until day 7 to assess for rebound inflammation following corticosteroid discontinuation
Jama, 313(7), 677-686
33
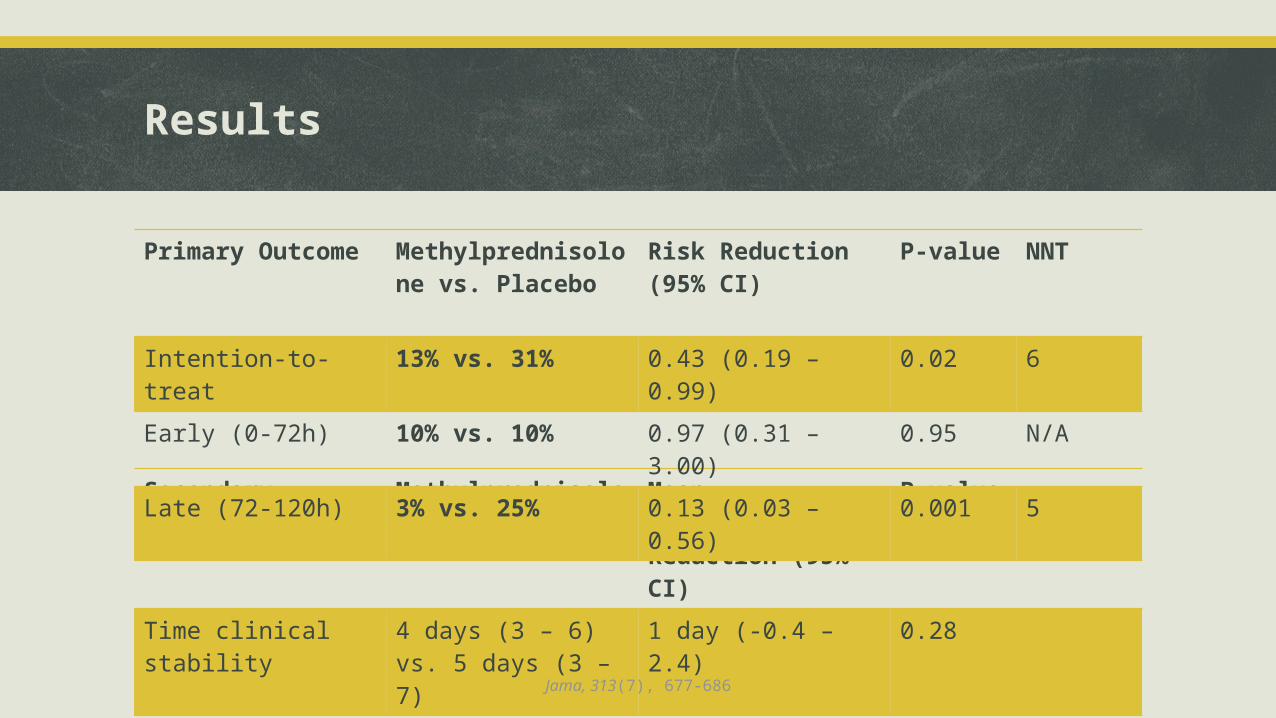
Results
Secondary Outcome Methylprednisolone vs. Placebo
Mean Difference/Risk Reduction (95% CI)
P-value
Time clinical stability 4 days (3 – 6) vs. 5 days (3 – 7)
1 day (-0.4 – 2.4) 0.28
In-hospital mortality 10% vs. 15% 0.64 (0.23 – 1.81) 0.37
Primary Outcome Methylprednisolone vs. Placebo
Risk Reduction (95% CI) P-value NNT
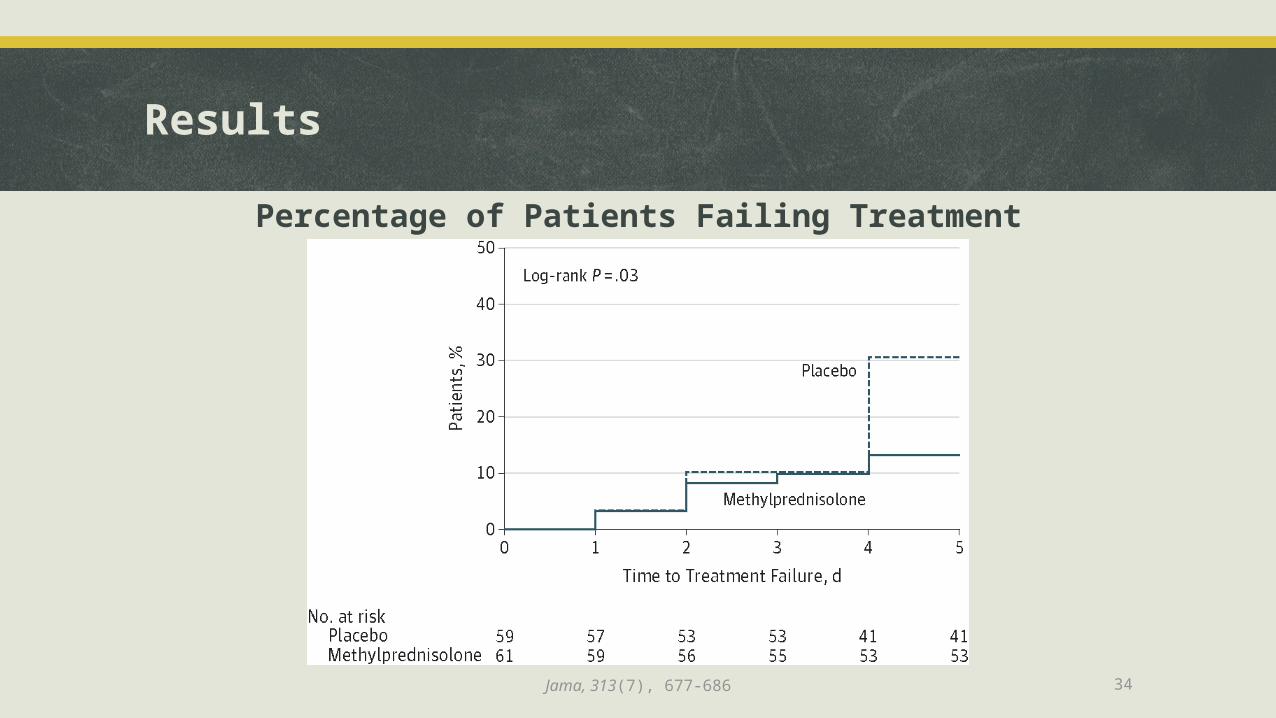
Intention-to-treat 13% vs. 31% 0.43 (0.19 – 0.99) 0.02 6
Early (0-72h) 10% vs. 10% 0.97 (0.31 – 3.00) 0.95 N/A
Late (72-120h) 3% vs. 25% 0.13 (0.03 – 0.56) 0.001 5
Jama, 313(7), 677-686
34
Results
Percentage of Patients Failing Treatment
Jama, 313(7), 677-686

35
Results
Causes of Treatment Failure
Jama, 313(7), 677-686

36
Results
Incidence of other adverse events (GI bleed, infection, delirium, AKI, acute hepatic injury) were similar between groups
Likely not powered to detect differences in adverse events
Adverse Event Methylprednisolone vs. Placebo
Risk Increase (95% CI) P-value
Hyperglycemia 18% vs. 12% 1.52 (0.59 – 3.92) 0.34
Jama, 313(7), 677-686

37
Commentary: Strengths
Patients were analyzed according to the group they were randomized to (ITT) and according to treatment protocol (per-protocol)
Randomization, allocation concealment, and blinding was well done
Addressed more baseline risk factors for community-acquired pneumonia including current smoking status
Adjusting for baseline differences (rates of septic shock in placebo group) still resulted in reduced treatment failure with methylprednisolone
Primary outcome addressed morbidity and mortality associated with treatment failure (shock, ventilation, death)
BUT, what can we make of reduced late (72-120h) radiographic progression, the outcome driving statistical significance? Does it lead to worse outcomes?
Jama, 313(7), 677-686, Jama, 313(7), 673-674

38
Commentary: Limitations
Treatment failure is a composite endpoint
Initial antibiotic adequacy was lower in the placebo group (94%) when compared to the methylprednisolone group (100%) after culture results were known
Poor applicability due to inclusion of patients with a high inflammatory response (CRP > 150mg/L) – 24% of screened patients were excluded for CRP < 150mg/L
Did not evaluate patients for a history of pneumococcal or influenza vaccinations, interventions thought to have a beneficial impact on severity and mortality outcomes
Follow-up was only done in hospital, post-discharge complications were not assessed
Low proportion of patients received a macrolide combination (24% vs. 23%) Anti-inflammatory action of macrolides? Mortality benefit with macrolides? About 63% received a macrolide in the study by Blum et al…
No subgroup analysis according to infectious cause – S.pneumoniae was the most common infectious agent (20% vs. 26%)
Jama, 313(7), 677-686, Critical Care Medicine, 42(2), 420-432
39
Conclusions
Included more information on baseline characteristics (i.e. smokers), but…
Trial was small (n=120), and although it offers some insight into the treatment of a specific patient group, enrollment was difficult for this subset (took 8 years) and resulted in a lack of power to detect possible differences
Patients community-acquired pneumonia with a greater inflammatory response showered lower risk of treatment failure, although it is hard to apply the benefit of reduced radiographic progression
Does it mean lower incidence of acute respiratory distress syndrome? Reduce inflammatory response to a Jarisch-Herxeimer reaction?
Is it applicable when only about 24% of patients received macrolides (a common guideline and resource recommendation for hospitalized CAP in North America)?
Jama, 313(7), 677-686, NEJM 354(16), 1671-1684, Travel Medicine and Infectious Disease, 11(4), 231-237
40
Corticosteroids in the Treatment of Community-AcquiredPneumonia in AdultsA Meta-Analysis (Nie et al.)PLoS One. 2012; 7(10): e47926

41
Design & Results
Nine RCTs and quasi-RCTs involving 1001 patients with CAP receiving either adjunctive corticosteroids or placebo in addition to standard treatment
Four trials included only patients with severe CAP
Hydrocortisone, dexamethasone, prednisolone, or methylprednisolone were used with a duration ranging from 1 to 9 days
Primary outcome measure was mortality (8 trials, n=970) OR 0.62 (95% CI 0.37-1.04), p=0.07, I2=13%, NSS
GI bleeding and infection rates were not different, however hyperglycemia was more common in the corticosteroid groups
PLoS One. 2012; 7(10): e47926
42
Severe CAP & Prolonged Therapy
A subgroup analysis showed a significant association between severe community-acquired pneumonia and reduced mortality with adjunctive corticosteroids
OR 0.26 (95% CI 0.11-0.64), p=0.003, I2=0%
Prolonged courses of treatment (> 5 days) also resulted in reduced mortality OR 0.51 (95% CI 0.26-0.97), p=0.04, I2=37%
Keep in mind: Only 4 trials assess severe community-acquired pneumonia Only 5 trials looked at prolonged treatment
7 days (4) 9 days (1)
PLoS One. 2012; 7(10): e47926

43
Conclusions
Although Blum et al. showed a benefit regardless of pneumonia severity, the 2012 meta-analysis by Nie et al. demonstrated a mortality benefit in severe CAP or those given prolonged corticosteroid treatment > 5 days
Other than an increased risk of hyperglycemia in the corticosteroid group, rates of GI bleeding and superinfection were the same
Heterogeneity was low, but is it reasonable to combine data from 4 different continents (Europe, North America, Africa, and Asia) where antibiotic/antiviral usage, etiologies, resistance rates, and populations likely differ?
Perhaps it is better left to a large, specific, well-designed RCT?
PLoS One. 2012; 7(10): e47926

44
Corticosteroids for Community-Acquired PneumoniaPutting it all together

45
Discussion
It is still unclear what cohort of patients will benefit most, as there are many variables that can affect pneumonia risk, severity, and morbidity/mortality
Clinical criteria needs to be more specific to better answer the question
If the question of corticosteroids and mortality in CAP is to be adequately addressed, much larger RCTs need to be conducted
More power to detect differences in a more representative patient sample
Although there is unclear evidence for a mortality benefit in any severity of CAP, even a 1 day reduction in hospital stay carries significant cost savings, however, at the expense of in-hospital hyperglycemia requiring insulin

46
Remaining Questions
What about patients with CAP and septic shock with adrenal insufficiency?
Do corticosteroids reduce the incidence of acute respiratory distress syndrome secondary to CAP?
Are corticosteroids more effective in Staphylococcus aureus pneumonia than in Streptococcus pneumonia? What about viral pneumonia? Atypical pneumonia?
Does immunization or smoking status play a large role?
Outpatient vs. Inpatient vs. ICU?
Chest, 136(6), 1631-1643
47
Summary
The most recent randomized controlled trial evidence suggests reduced in-hospital instability, length of stay, and treatment failure when using short term corticosteroids for the treatment of community-acquired pneumonia. Even though a recent meta-analysis suggest a possible mortality benefit in severe pneumonia and with prolonged treatment, it is difficult to apply the meaning of these endpoints to patients in clinical practice.
At best there is evidence for potential cost savings due to reduced length of stay, but weighed against the risk of in-hospital hyperglycemia requiring insulin
Until a more definitive conclusion is drawn, there is no clear role for corticosteroids in the treatment of community-acquired pneumonia and they should not be routinely used
Lancet 2015; 385: 1511–18, Jama, 313(7), 677-686, PLoS One. 2012; 7(10): e47926

48
Questions?

49
References
Limper, A. H. (2012). Overview of Pneumonia. In L. Goldman, & A. I. Schafer, Goldman's Cecil Medicine, Twenty-Fourth Edition (pp. 587-596). Philadelphia: Elsevier.
Feldman, C., & Anderson, R. (2015). Community-acquired pneumonia: Pathogenesis of acute cardiac events and potential adjunctive therapies. Chest, doi:10.1378/chest.15-0484; 10.1378/chest.15-0484
Raut, M., Schein, J., Mody, S., Grant, R., Benson, C., & Olson, W. (2009). Estimating the economic impact of a half-day reduction in length of hospital stay among patients with community-acquired pneumonia in the US. Current Medical Research and Opinion, 25(9), 2151-2157. doi:10.1185/03007990903102743; 10.1185/03007990903102743
Nannini, L. J., Lasserson, T. J., & Poole, P. (2012). Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. The Database of Systematic Reviews, 9, CD006829. doi:10.1002/14651858.CD006829.pub2; 10.1002/14651858.CD006829.pub2
Almirall, J., Bolibar, I., Balanzo, X., & Gonzalez, C. A. (1999). Risk factors for community-acquired pneumonia in adults: A population-based case-control study. The European Respiratory Journal, 13(2), 349-355.
Ellison, R. T., & Donowitz, G. R. (2015). Acute Pneumonia. In J. E. Bennett, R. Dolin, & M. J. Blaser, Mandell's Priniciples and Practice of Infectious Diseases (pp. 823-846). Philadelphia: Elsevier.
Kellum, J. A., Kong, L., Fink, M. P., Weissfeld, L. A., Yealy, D. M., Pinsky, M. R., et al. (2007). Understanding the inflammatory cytokine response in pneumonia and sepsis: Results of the genetic and inflammatory markers of sepsis (GenIMS) study. Archives of Internal Medicine, 167(15), 1655-1663. doi:10.1001/archinte.167.15.1655
Yende, S., D'Angelo, G., Kellum, J. A., Weissfeld, L., Fine, J., Welch, R. D., et al. (2008). Inflammatory markers at hospital discharge predict subsequent mortality after pneumonia and sepsis. American Journal of Respiratory and Critical Care Medicine, 177(11), 1242-1247. doi:10.1164/rccm.200712-1777OC; 10.1164/rccm.200712-1777OC

50
References
Martinez, R., Menendez, R., Reyes, S., Polverino, E., Cilloniz, C., Martinez, A., et al. (2011). Factors associated with inflammatory cytokine patterns in community-acquired pneumonia. The European Respiratory Journal, 37(2), 393-399. doi:10.1183/09031936.00040710; 10.1183/09031936.00040710
de Gans, J., & van, d. B. (2002). Dexamethasone in adults with bacterial meningitis. N Engl J Med, 347(20), 1549-1556. doi:10.1056/NEJMoa021334 Brouwer, M. C., McIntyre, P., Prasad, K., & van de Beek, D. (2013). Corticosteroids for acute bacterial meningitis. The Cochrane Database of Systematic Reviews, 6,
CD004405. doi:10.1002/14651858.CD004405.pub4; 10.1002/14651858.CD004405.pub4 van de Beek, D., & de Gans, J. (2004). Dexamethasone and pneumococcal meningitis. Annals of Internal Medicine, 141(4), 327. Prasad, K., & Singh, M. B. (2008). Corticosteroids for managing tuberculous meningitis. The Cochrane Database of Systematic Reviews,(1):CD002244. doi(1),
CD002244. doi:10.1002/14651858.CD002244.pub3; 10.1002/14651858.CD002244.pub3Ewald, H., Raatz, H., Boscacci, R., Furrer, H., Bucher, H. C., & Briel, M. (2015). Adjunctive corticosteroids for pneumocystis jiroveci pneumonia in patients with HIV infection. The Cochrane Database of Systematic Reviews, 4, CD006150. doi:10.1002/14651858.CD006150.pub2; 10.1002/14651858.CD006150.pub2
Mandell, L. A., Wunderink, R. G., Anzueto, A., Bartlett, J. G., Campbell, G. D., Dean, N. C., et al. (2007). Infectious diseases society of America/American thoracic society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America, 44 Suppl 2, S27-72. doi:10.1086/511159
Blum, C. A., Nigro, N., Briel, M., Schuetz, P., Ullmer, E., Suter-Widmer, I., et al. (2015). Adjunct prednisone therapy for patients with community-acquired pneumonia: A multicentre, double-blind, randomised, placebo-controlled trial. Lancet, 385(9977), 1511-1518. doi:10.1016/S0140-6736(14)62447-8; 10.1016/S0140-6736(14)62447-8
Johnstone, J., Marrie, T. J., Eurich, D. T., & Majumdar, S. R. (2007). Effect of pneumococcal vaccination in hospitalized adults with community-acquired pneumonia. Archives of Internal Medicine, 167(18), 1938-1943. doi:10.1001/archinte.167.18.1938
Herzog, N. S., Bratzler, D. W., Houck, P. M., Jiang, H., Nsa, W., Shook, C., et al. (2003). Effects of previous influenza vaccination on subsequent readmission and mortality in elderly patients hospitalized with pneumonia. The American Journal of Medicine, 115(6), 454-461.
Meijvis, S. C., Hardeman, H., Remmelts, H. H., Heijligenberg, R., Rijkers, G. T., van Velzen-Blad, H., et al. (2011). Dexamethasone and length of hospital stay in patients with community-acquired pneumonia: A randomised, double-blind, placebo-controlled trial.Lancet, 377(9782), 2023-2030. doi:10.1016/S0140-6736(11)60607-7; 10.1016/S0140-6736(11)60607-7Torres, A., Sibila, O., Ferrer, M., Polverino, E., Menendez, R., Mensa, J., et al. (2015).

51
References
Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: A randomized clinical trial. Jama, 313(7), 677-686. doi:10.1001/jama.2015.88; 10.1001/jama.2015.88dex
Wunderink, R. G. (2015). Corticosteroids for severe community-acquired pneumonia: Not for everyone. Jama, 313(7), 673-674. doi:10.1001/jama.2015.115; 10.1001/jama.2015.115
Sligl, W. I., Asadi, L., Eurich, D. T., Tjosvold, L., Marrie, T. J., & Majumdar, S. R. (2014). Macrolides and mortality in critically ill patients with community-acquired pneumonia: A systematic review and meta-analysis. Critical Care Medicine, 42(2), 420-432. doi:10.1097/CCM.0b013e3182a66b9b; 10.1097/CCM.0b013e3182a66b9b
Steinberg, K. P., Hudson, L. D., Goodman, R. B., Hough, C. L., Lanken, P. N., Hyzy, R., et al. (2006). Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. The New England Journal of Medicine, 354(16), 1671-1684. doi:10.1056/NEJMoa051693
Belum, G. R., Belum, V. R., Chaitanya Arudra, S. K., & Reddy, B. S. (2013). The jarisch-herxheimer reaction: Revisited. Travel Medicine and Infectious Disease, 11(4), 231-237. doi:10.1016/j.tmaid.2013.04.001; 10.1016/j.tmaid.2013.04.001
Nie, W., Zhang, Y., Cheng, J., & Xiu, Q. (2012). Corticosteroids in the treatment of community-acquired pneumonia in adults: A meta-analysis. PloS One, 7(10), e47926. doi:10.1371/journal.pone.0047926; 10.1371/journal.pone.0047926
Meduri, G. U., Annane, D., Chrousos, G. P., Marik, P. E., & Sinclair, S. E. (2009). Activation and regulation of systemic inflammation in ARDS: Rationale for prolonged glucocorticoid therapy. Chest, 136(6), 1631-1643. doi:10.1378/chest.08-2408; 10.1378/chest.08-2408

Limper, A. H. (2012) 52
Severe Community-Acquired Pneumonia
Minor criteria• Respiratory rate > 30 breaths/min• PaO2/FiO2 ratio ≤250• Multi-lobar infiltrates• Confusion/disorientation• Uremia (BUN level ≥20 mg/dL)• Leukopenia (WBC count <4000 cells/mm3)• Thrombocytopenia (platelet count <100,000
cells/mm3)• Hypothermia (core temperature <36ᵒC)• Hypotension requiring aggressive fluid
resuscitation
Major Criteria• Invasive mechanical ventilation• Septic shock with need for vasopressors
Criteria for severe community-acquired pneumonia*
*Require 3 minor criteria or 1 major