poison sileshi-3
TRANSCRIPT

Poisonings
Poisoning
Sileshi Mulatu
UNIVERSTY OF GONDAR COLLEGE OF MEDICINE AND HEALTH SCIENCE
DEPARTMENT OF NURSING
Dec, 2015Gondar, Ethiopia 1

DefinitionPresentation outline
oObjectiveoIntroductionoEpidemiologyoRisk factorsoType of poisoningoLead poisoning
o Pesticide poisingo Food poisingo Medication poisoning and o Alcohol poisoningo Evidenceo Reference
2

Definition
Objective– At the end of this session the student will
be able to:Discus the overview of poisoningIdentify the common type of poisoningExplain the cause of poisoningDetermine the effect of poisoning on childrenAnalyze the determinant factors of poisoningDiscus complication of poisoningExplain the management of poisoning
3
DefinitionIntroduction
• Poison; Anything someone eats, drinks, breaths in, orgets in their eyes or on their skin that can causeillness or death if it gets into or on the body.
• A substance (solid, liquid or gas), which if introducedin the living body, or brought into contact to a parttherefore, will produce ill health or death, by itsconstitutional or local effects or both.
4

DEFINITIONIntroduction
• The majority of poisonings are accidental,especially in the under-5 age group
• Intentional overdoses and substance abuse areseen in older children
http://emedicine.medscape.com/pediatrics_general/
5
DEFINITIONIntroduction
• Deaths in children from poisoning are
becoming increasingly rare
• Factors responsible for this decline include:
1. Introduction of child-resistant
containers
2. Reducing the pack sizes
3. More effective management
http://emedicine.medscape.com/pediatrics_general/
6
Examples of Poisons Cont’dExamples of Poisons Household products
Medications Lead
Pesticide
Gases and Fumes
7

Cost
Poisoning in ChildrenDefinition of Poisoning:• Exposure to a chemical or other agent that adversely
affects functioning of an organism.• Poisoning is the third leading cause of unintentional
injury death.• Each year 3,000 young children aged 0 to 14 die of
acute poisoning• Children 5 years and under account for the majority
of all poison exposures with children up to two yearsold especially vulnerable.
8

Cost
Poisoning in Children• The term poisoning is used when cells are injured or
destroyed by inhalation, ingestion, injection orabsorption of a toxic substance.
• Curiosity and the desire to put everything in theirmouths place young children at considerably greaterrisk for poison exposure than adults.
• They like things that smell good and are drawn toattractive packaging and the colorful substances of
many of the products found around the home. 9
Definition• Children are curious and explore their world with alltheir senses, including taste.
• As a result, the home and its surroundings can be adangerous place where poisonous substances areinadvertently ingested.
• Common causes of poisoning in children are householdproducts including kerosene oil, drugs,chemicals(corrosives) and pesticides.
Poisoning in Children
10

Cost• Children are more likely to suffer seriousconsequences because they are smaller, havefaster metabolic rates and their bodies are lesscapable of neutralizing toxic chemicals.
• Circumstances of Exposure can beintentional, accidental, environmental,medicinal or recreational.
• Routes of exposure can be ingestion, injection,inhalation or cutaneous exposure
Poisoning in Children
11
Cost• Most exposures involved oral ingestion (76 percent),occurred in the home (93 percent), and wereunintentional (more than 80 percent).
• Children younger than six years accounted for 51percent of the exposures.
• Of these, 38 percent involved children three years oryounger.
• Most ingestions involved nontoxic substances andwere managed at home.
Poisoning in Children
Tamara Mcgregor, 2009 12

Poisoning Facts in ChildrenEpidemiology In 2004, poisoning caused more than 45 000 deaths
in children and youth under 20 years of age.
In the rate of fatal poisoning is highest for childrenunder one year, with another slight peak around 15years.
In fatal poisoning rates in low-income and middle-income countries are four times that of high-incomecountries.
Common poisoning agents in low-income andmiddle income countries are fuels such as paraffinand kerosene, pharmaceuticals and cleaning agents. 13

Risk Factors for Poisoning
Epidemiology• The prevalence and types of poisoning vary in
different parts of the world based on their economicstatus.
• They depend on industrial development, agriculturalactivities, cultural practices relating to supervision ofchildren and local beliefs and customs.
For example, medicinal drugs are the leading cause of non-fatal poisoning in children in middle income to high-incomecountries, and ingestion of fuels such as kerosene is acommon cause in low income countries. 14

Risk Factors for Poisoning
Risk Factors for Poisoning• Unsupervised home setting
• African American race
• Males less than 5 years old
• Lower level of education
• Substance abuse
• Depressed adolescents
15
Risk Factors for Poisoning
Risk Factors for Poisoning• Young children are particularly susceptible to the
ingestion of poisons, especially liquids.
• Adolescents, on the other hand, are more aware of theconsequences of their actions but peer pressure andrisk taking behavior can lead them to misuse alcohol ordrugs, leading to higher fatality rate
• Younger children are more susceptible to poisoningbecause of their smaller size and less well-developedphysiology and immaturity 16

Risk Factors for Poisoning
Risk Factors for PoisoningOther risk factors for poisoning include thoserelated to the poisoning agent itself, Including toxicity, nature, physical appearance and
storage; season and weather conditions, policies,standards and laws governing the manufacture,labelling, distribution, storage and disposal ofpoisoning agents; and access to quality health carefor treatment.
17
Types of Poisonings
Common Types of Poisonings
18

Lead Poisoning in Children
19
Objectives Identify sources of lead
Recognize the dangers of lead exposure
Identify signs and symptoms of children whohave been exposed to lead
Identify ways to prevent lead poisoning
1. Recognize ways of treatment of lead poisoning
20

Introduction Lead is a heavy metal with a bluish-grey color.
It has a low melting point, is easily molded and shaped,and can be combined with other metals to form alloys
For these reasons, lead has been used by humans formillennia and is widespread today in products as: pipes; storage batteries; pigments and paints; glazes; vinyl
products; weights, shot and ammunition; cable covers; andradiation shielding.
21
Introduction Lead poisoning is one of the most common and best-recognized
childhood diseases of toxic environmental origin.
Children around the world today are at risk of exposure to leadfrom multiple sources.
Lead poisoning accounts for about 0.6% of the global burden ofdisease (WHO, 2009).
22

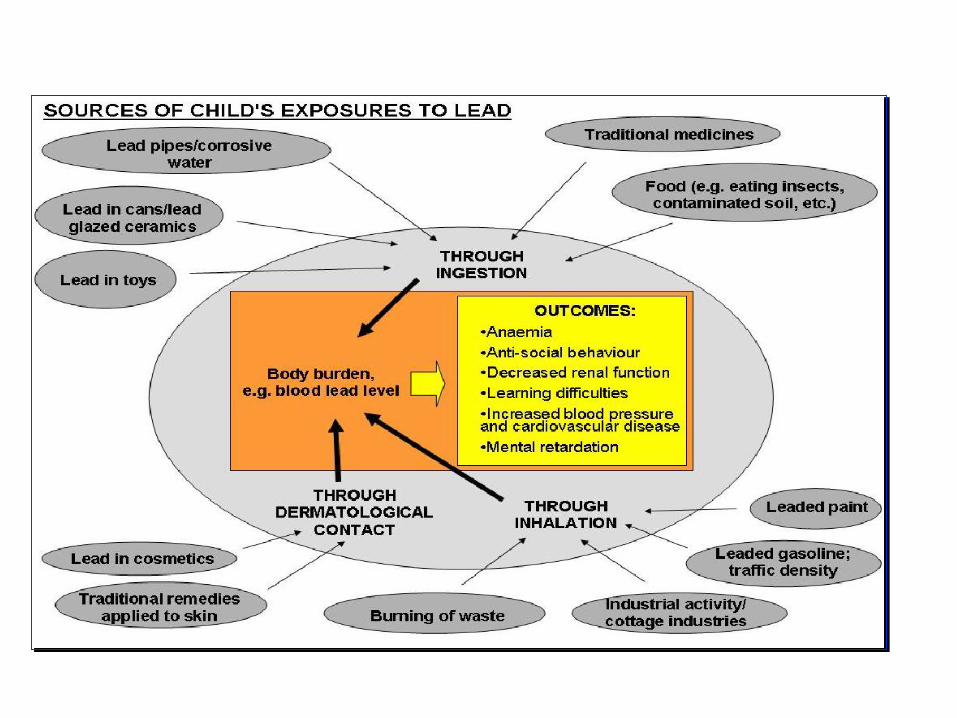
Sources of Lead exposure children lead added to gasoline
lead from an active industry, such as mining (especiallyin soils)
lead-based paints and pigments,
lead solder in food cans
ceramic glazes
drinking-water systems with lead solder and lead pipes
lead in products, such as herbal and traditional medicines23

lead released by incineration of lead-containingwaste
lead in electronic waste (e-waste)
lead in the food chain, via contaminated soil
lead contamination as a legacy of historicalcontamination from former industrial sites.
Some toys, jewelry, hobby and sports objects (likestained glass, ink, paint and plaster) may contain lead.
24
25
Children At Risk Children under the age of 6 years are at the greatest risk.
They grow so rapidly and tend to put their hands or otherobjects into their mouths.
In the low-income world the informal recovery of lead from carbatteries and the open burning of waste are very importantsources of environmental lead contamination.
26

Children At Risk Socioeconomic factors are important predictors of
exposure to lead. Poor families are more likely to expose to lead
Also, they are more likely to dwell on polluted lands, to work inpolluting industries, or to live in older housing with lead-basedpaint.
Finally, poor children are more likely to have iron or calciumdeficient diets, and as a result they may absorb lead more
efficiently. 27
Effect of Lead Poisoning Children can be exposed to lead through inhaling, swallowing
and in some cases, it can be absorbed into the skin.
Once lead is in a child’s system, it is distributed through the bodylike helpful minerals such as zinc and iron.
If lead is in the bloodstream, it can cause damage to red bloodcells and limit their ability to carry oxygen to organs and tissue.
(Kids Health)28
Long Term Effects of Lead Exposure Developmental Delays
Speech and Language Problems
Poor Muscle Coordination
Damage to the nervous system, kidneys and hearing
Decreased bone and muscle growth
Seizures and unconsciousness(Kids Health)
29

Signs and Symptoms of Lead Poisoning Headaches
abdominal pain
Loss of appetite
Vomiting or nausea
Constipation
Seizures
Weight loss
Lethargy or fatigue Pallor (pale skin) from anemia
(lower than normal RBCs)Metallic taste in mouthMuscle and joint weakness or pain Irritability or behavioral problems Pica (eating of non-nutritious
things such as dirt and paintchips)
30
Siblings of children with lead in their bodies will alsobe tested.
Therapies are used with children who have smallamounts of lead present, in order to allow the body tonaturally eliminate the lead.
Lead Poisoning Treatment
31

Treatment Lead poisoning is treated depending on how much lead is in the
blood.
Some children require hospitalization to receive a medicationcalled a chelating agent.
This medication chemically binds with lead, through an IV tomake the lead weaker so the body can get rid of it naturally.
This is for children with both severe and high levels of lead.
32

General measures Quick assessment
Limit absorption:– Vomiting
– Lavage
– Activated charcoal instillation
Treatment
33
Specific:ABCD’s of Toxicology:– Airway– Breathing– Circulation– Drugs:
– Resuscitation medications if needed– Universal antidotes
– Draw blood: – chemistry, coagulation, blood gases, drug levels
– Decontaminate– Expose / Examine– Full vitals / Monitoring– Give specific antidotes / treatment
Treatment
34

Decontamination:1. Ocular:
– Flush eyes with saline2. Dermal:
– Remove contaminated clothing– Brush off– Irrigate skin
3. Gastro-intestinal:– Activated charcoal:
– May Prevent /delay absorption of some drugs/toxins– Almost always indicated
– Naso/oro-gastric Lavage– Bowel Irrigation:
– Recent ingestions 4-6 hrs– 500 cc NS Children / 2000cc adults– Orally / Nasogastric tube
Treatment
35
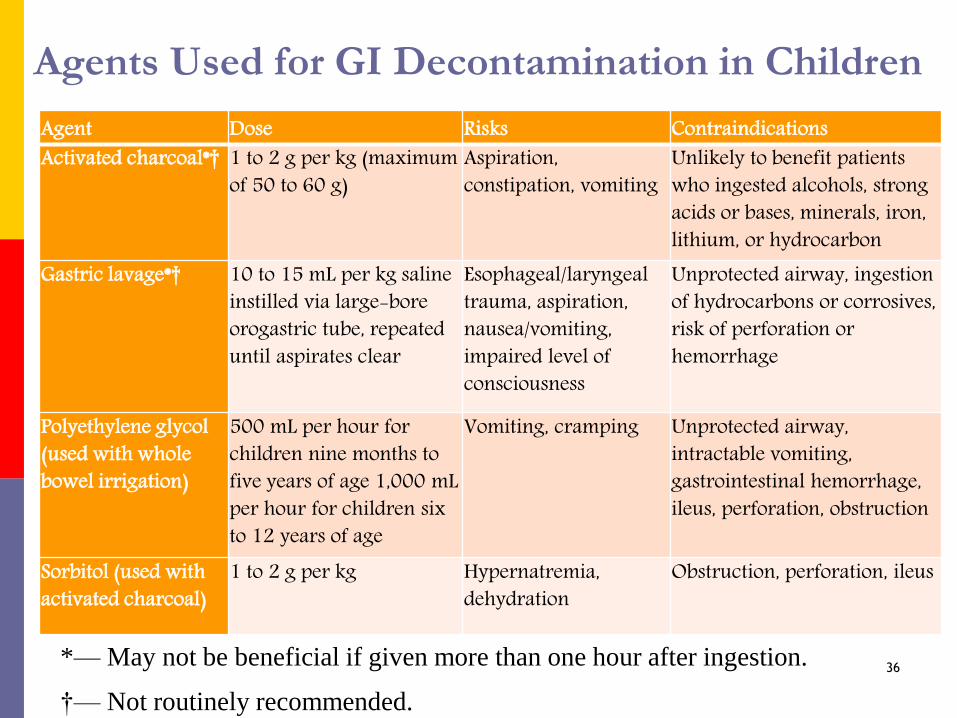
Agents Used for GI Decontamination in Children
Agent Dose Risks ContraindicationsActivated charcoal*† 1 to 2 g per kg (maximum
of 50 to 60 g)Aspiration, constipation, vomiting
Unlikely to benefit patients who ingested alcohols, strong acids or bases, minerals, iron, lithium, or hydrocarbon
Gastric lavage*† 10 to 15 mL per kg saline instilled via large-bore orogastric tube, repeated until aspirates clear
Esophageal/laryngeal trauma, aspiration, nausea/vomiting, impaired level of consciousness
Unprotected airway, ingestion of hydrocarbons or corrosives, risk of perforation or hemorrhage
Polyethylene glycol (used with whole bowel irrigation)
500 mL per hour for children nine months to five years of age 1,000 mL per hour for children six to 12 years of age
Vomiting, cramping Unprotected airway, intractable vomiting, gastrointestinal hemorrhage, ileus, perforation, obstruction
Sorbitol (used with activated charcoal)
1 to 2 g per kg Hypernatremia, dehydration
Obstruction, perforation, ileus
*— May not be beneficial if given more than one hour after ingestion.
†— Not routinely recommended.
36
• Damp-mop floors, damp-wipe surfaces, and frequently wash achild’s hands, pacifiers and toys to reduce exposure to lead
• Avoid using home remedies and cosmetics (such as kohl, alcohol)that contain lead
• Take basic steps to decrease your exposure to lead (for example,by showering and changing clothes after finishing the task), ifyou remodel buildings built before 1978, or if your work orhobbies involve working with lead-based products
Preventing Lead Poisoning
37
Wash children's hands after they play outside, before eatingand going to bed
Clean floors with a wet mop and wipe furniture, windowsillsand other dusty surfaces with a damp cloth.
Restrict where children play.
Don't let them play near major roadways or bridges. Prepare meals that are high in iron and calcium which helps
prevent lead absorption in your children's bodies.38

Pesticide poisoning In Children39
Objectives Identify sources of pesticides
Recognize the dangers of Pesticides
Identify possible risk factors for pesticides poisoning
Identify ways to prevent Pesticides poisoning
Recognize ways Pesticides poisoning is treated
40

Introduction
Pesticides are toxic substances designed to kill, inhibit the growthof living organisms
They are used against insects, mammals, plants, fungi, nematodesand other creatures that can pose problems for agriculture, publichealth, or homes, schools, buildings and communities
However, when improperly used or stored, these chemical agentscan also harm humans
Pesticides impair the functioning of biological processes essentialfor life, such as the nervous and reproductive systems 41

Introduction
Key risks are cancer, birth defects, and damage to the nervoussystem and the functioning of the endocrine system.
People can be exposed to excessive pesticide while working; viafood, soil, water or air; or by directly ingesting pesticideproducts.
Pesticides are known to cause millions of acute poisoning casesper year, of which at least one million require hospitalization.
42

Introduction
It has been reported that an estimated 1 to 5 millioncases occur every year, resulting in 20,000 fatalitiesamong agricultural workers.
Most of these poisonings take place in developingcountries, where safeguards typically are inadequate
Although developing countries use 25% of the world’sproduction of pesticides, they experience 99% of thedeaths 43

Sources of Pesticide Poisoning
Once used, pesticides may accumulate in the air or water or onland, where they can harm non-target species and diminishbiodiversity.
Contaminating groundwater, lakes, rivers, and other bodies ofwater, they can pollute drinking supplies, fish and otherresources that can be vital for human well-being.
Polluting soil, they can endanger children at play or at work
44
Risk factors of Pesticide Poisoning
The impact of an exposure to pesticides on human healthdepends on a number of factors, including the class of pesticideinvolved, the specific chemical and formulation, and theamount, route, timing and duration of the dose.
The route of exposure can be via breathing, drinking or eating,or through the skin or mucous membranes.
Other factors include the health of the person poisoned.
Malnutrition and dehydration, for example, increase thesensitivity to pesticides. 45

Why are children at greater risk? Children are often more vulnerable than adults to the effects of
pesticides as a result of several risk factors.
These include their smaller size, greater rates of exposure tofood, soil, water, air, differing metabolism, and rapidly growingand developing organ systems.
They put things in their mouths.
Inexperience, lack of maturity, illiteracy and an inability toassess risk
46
Why are children at risk?
Infants Most infant poisonings are result of adult
error;
Crawlers Explore everything within reach and put things in
their mouth
Toddlers and preschoolers Reach higher, nothing is child-proof, look-alikes are
misleading
Stages of Development
47

Clinical symptomsAcute poisoning can cause a range of symptoms in adults andchildren, depending on the type of pesticide.
For example, commonly used organophosphorus andcarbamate compounds can produce neurobehavioral effects,such as fatigue, dizziness, and blurred vision; intestinal effects,such as nausea; respiratory effects, such as dry throat anddifficulty with breathing; effects involving skin and mucousmembranes, such as stinging eyes, itchy skin, and a burningnose; and muscular symptoms, such as stiffness and weakness 48

TreatmentDifferent treatments are available, depending on the poison.
Activated charcoal – this substance stops the body absorbing thepoison, but must be given within one hour of child swallowingthe poison for it to be effective. It does not work with everysubstance.
Observation – some poisons have a delayed effect and yourchild may have to stay in hospital, possibly overnight.
49
Treatment Monitoring – of heart rhythms and checking other vital signs
such as blood pressure and oxygen levels.
Bloods tests – to check the level of poison in the blood. This helps decide further treatment. In most cases the level is very low and no problems are expected.
Antidote – can be given for some poisons to reverse the effects. Admission – a few children need further treatment in hospital.
50

51

52

Food poisoning, also called foodborne illness,
Infectious organisms — including bacteria, viruses and parasitesor their toxins are the most common causes of food poisoning
Food poisoning symptoms, which can start within hours ofeating contaminated food, often include nausea, vomiting ordiarrhea. Most often, food poisoning is mild and resolveswithout treatment, But some people need to go to the hospital
53

Is any illness resulting from the Ingestion of food or
Drink.
Contaminated with Living bacteria or
Other toxins or
Inorganic chemical substances &
poisons from Plants & animals54

Types Of The Food Poisoning
• Non – bacterial type of the food poisoning
• Bacterial Type of the food poisoning
55
Non – Bacterial Type Of The Food Poisoning
It is caused by the chemicals such as
• Arsenic
• Certain plants & sea foods
• The contamination food by the chemicals such as
Fertilizer
Pesticides
Cadmium
Mercury
56
Bacterial Food – Poisoning
• It is caused by the ingestion of the food contaminated by the
living bacteria or their toxins
• The conventional classification of the bacterial food poisoning in
to the toxic and infective type is becoming increasingly blurred,
with the knowledge that in some types both multiplication and
toxins production can involve.
E.g. Salmonella , Botulism, Staphylococcal are most common
food poisoning
57
Risk factors Child becoms ill after eating contaminated food depends on
the organism, the amount of exposure, the age and health.High-risk groups include:
Older adults. As you get older, your immune system maynot respond as quickly and as effectively to MOs
Pregnant women. During pregnancy, changes in metabolism andcirculation may increase the risk of food poisoning.
Infants and young children. Their immune systems poor
People with chronic disease; as DM, liver disease or AIDS or receivingchemotherapy or radiation therapy for CA reduces immune response 58

Symptoms of food poisoning
59
Symptoms
Food poisoning symptoms vary with the source of contamination.
Most types of food poisoning cause one or more of the followingsigns and symptoms:
Nausea, Vomiting, Watery diarrhea, Abdominal pain and cramps and Fever
Signs and symptoms may start within hours after eating thecontaminated food, or they may begin days or even weeks later.
Sickness caused by food poisoning generally lasts from a fewhours to several days.
60

Treatment The main treatment for food poisoning is putting
fluids back in the body (rehydration) through an IVand by drinking.
Do not eat solid food while nauseous or vomitingbut drink plenty of fluids.
Anti-vomiting and diarrhea medications
Antibiotics61
Complications The most common serious complication of food poisoning is
dehydration a severe loss of water and essential salts andminerals.
If you're a healthy adult and drink enough to replace fluids youlose from vomiting and diarrhea, dehydration shouldn't be aproblem.
Infants, older adults and people with suppressed immunesystems or chronic illnesses may become severely dehydratedwhen they lose more fluids than they can replace.
In that case, they may need to be hospitalized and receiveintravenous fluids.
62

Golden Rules for Safe Food Preparation
1. Choose foods processed for safety2. Cook food thoroughly3. Eat cooked foods immediately4. Store cooked foods carefully5. Reheat cooked foods thoroughly6. Avoid contact between raw foods and cooked foods7. Wash hands repeatedly8. Keep all kitchen surfaces meticulously clean9. Protect foods from insects, rodents, and other animals10. Use safe water
63

Safe Preservation of Food
Refrigeration Drying Canning (Tin) Salting Preserving Smoking Chemicals (Sugar, salts, Citric acid, Benzoic acid)
64

Prevention & Control(A)Food Sanitation
1. Food/ Meat Inspection
2. Personal Hygiene
3. Medical Inspection of Food handlers.
4. Food handling Technique (Golden rules).
5. Sanitary improvements.
6. Health Education
(B) Refrigeration65

1. Keep hands and nails clean
We need to: wash hands and nails thoroughly
with warm, running water and soap
dry hands thoroughly
Strategies to prevent food poisoning
66
When cleaning plates and equipment, we need to: scrape and rinse off surface food wash in clean, soapy water rinse in clean water air dry where possible if drying immediately, use only a clean, dry towel.Pest control and animals stop pests such as cockroaches and mice coming into the area
where food is kept discourage pests by not leaving food or dirty dishes out on the
benches keep animals out of the kitchen.
Keeping the k i tchen c lean
67
avoid preparing food when sick or feeling unwell
keep raw meats, poultry and seafood
separated from cooked food and food to be eaten raw
protect food in the refrigerator by placing in covered
containers or covering with plastic wrap
use clean equipment, plates or containers to prevent
contamination of cooked food
use clean equipment, rather than hands, to pick up food
wear clean clothes or a clean apron
wash fruit and vegetables to be
eaten raw under running water.
Handl ing food sa fe ly
68
®
© 2013 National Safety Council
Medication poisoningin children
69

© 2013 National Safety Council
70
70

© 2013 National Safety Council
71
Introduction◦ Medicine is safe in the right amount for the right person.
◦ A child should be told that medicine is to make them feel better.
◦ We know it can be a struggle to give medication to a resistantchild, but never “fake” a child into taking medicine by calling it“candy.” this may lower a child's fear or respect for a medication,they may ingest it on their own, which may cause a toxic overdose.
71
© 2013 National Safety Council
72
Introduction◦ Each year more than 60,000 children are treated in
emergency departments after getting into medicinewhile adults were not looking
◦ In recent years, the number of accidental overdoses inyoung children has increased by 20 percent.
72

© 2013 National Safety Council
73
Most common medicines and VitaminsPain relievers◦ Ibuprofen, Acetaminophen, Aspirin
Cough and cold medicines◦ Decongestants, Cough Suppressants, Antihistamines
Heart, blood pressure drugs
Psychotropic
Vitamins – especially iron73
© 2013 National Safety Council
74
General- evaluation◦ recognition of poisoning
◦ identification of agents which was taken
◦ assessment of severity
◦ prediction of toxicity

© 2013 National Safety Council
75
General- management
◦ provision of supportive care
◦ prevention of poison absorption
◦ enhancement of elimination of poison
◦ administration of antidotes
© 2013 National Safety Council
76
Supportive care
◦ ABC
◦ Vital signs, mental status, and pupil size
◦ Pulse oximetry, cardiac monitoring
◦ Protect airway
◦ Intravenous access
◦ cervical immobilization if suspect trauma
◦ Rule out hypoglycaemia
© 2013 National Safety Council
77
The common medication poisoningIron Poisoning
◦ Iron poisoning is the most common cause ofdeath due to poisoning in young children.
◦ It is also a significant problem inadolescents and adults.
© 2013 National Safety Council
78
Iron Poisoning
◦ Ingestion of a number of tablets of ferrous sulphate may causeacute poisoning.
◦ Lethal dose is 300 mg/kg of iron.
◦ Severe vomiting and diarrhea occur.
◦ These may contain blood due to extensive gastrointestinal bleeding.
◦ The child may go into severe shock, hepatic and renal failurewithin a few hours or after a latent period of 1 to 2 days

© 2013 National Safety Council
79
Iron PoisoningFive Stages but variable
Stage 1
Gastro-intestinal stage: within 30 mints to 6hrs of ingestion:abdominal pain, fluid loss, bleeding, shock(acidosis,
tachycardia +/- hypotension)
Fever, Lethargy and Coma

© 2013 National Safety Council
80
Iron Poisoning
Stage 2◦ Latent stage: 4-48hrs
A period where there is a small apparent improvement in the patient’s GI condition.
◦ It is often tempting to discharge such patients.
◦ However, in the seriously poisoned, a metabolic acidosis is evolving.
◦ This may be compounded by a lack of adequate fluid resuscitation.

© 2013 National Safety Council
81
Iron Poisoning-Stage 3
Circulatory collapse : 48-96 hrs
◦ Loss of adequate tissue perfusion and multi organfailure: most deaths occur during this stage.
◦ Shock occurs secondary to gastrointestinalhemorrhage, vomiting, vasodilation, and reducedcardiac output (due to myocardial toxicity).

© 2013 National Safety Council
82
Iron Poisoning-Stage 3
Multi organ failure related to inadequate perfusion anddirect toxicity ensues and results in:Altered mental status / coma
Seizure
Acute renal failure
Pulmonary edema

© 2013 National Safety Council
83
Iron Poisoning- Stage 4:◦ Hepatic failure: 96hrs
Increased mortality
Hepatic dysfunction is a poor prognostic sign.
Patients suffer related:Hypoglycemia
Coagulopathy and hemorrhage
Jaundice
Hepatic encephalopathy / coma
© 2013 National Safety Council
84
Iron Poisoning
STAGE 5:
◦Bowel obstruction 2-6 wks
◦Due to scarring
Gastric outlet obstruction
Small intestinal obstruction
◦May not pass through stage 4
© 2013 National Safety Council
85
Pathophysiology◦ Iron is potent catalyst of free radical formation and is
capable of oxidizing a wide range of substrates ,includinglipid, protein, DNA, and various biomolecules.
Typical iron poisoning targets:
◦GI, CVS, Liver, CNS, Hematopoietic system and Metabolicacidosis

© 2013 National Safety Council
86
Diagnosis
Clinical, History, physical exam
laboratory:
-abdominal radiograph,
-serum iron concentration,
-ABG, CBC, BS, BUN, Cr, Coagulation profiles, LFT, electrolytes
Differential diagnosis:
◦ consider metabolic acidosis, structural, infectious and other poisoning with GI
symptoms Gastroenteritis Hepatic failure
© 2013 National Safety Council
87
Laboratory Studies◦ It is a clinical diagnosis
◦Little is known about the absorption rate of iron in an
overdose or the timing of peak serum iron level
Serum levels Of :
Mild - Less than 300 µg/dl
Moderate - 300-500 µg/dl
Severe - More than 500 µg/dl

© 2013 National Safety Council
88
◦Detailed history and physical including
a rectal exam for frank blood.
◦Aggressive fluid resuscitation and intravenous access.
◦Whole bowel irrigation
◦ Laboratory analysis for CBC, chemistry, and iron levels (peak around 4 hours)
◦Will often require repeat levels with a repeat chemistry
Iron Poisoning - Management
© 2013 National Safety Council
89
Iron Poisoning
Management:1. Gastric decontamination:
Forced emesis
Gastric lavage with 5% NaHCO3
No activated charcoal
2. Secure good IV
3. Get initial the 4hrs levels and TBC
4. Chelate with Deferoxamine if levels> 300mg/dl

© 2013 National Safety Council
90
Iron Poisoning
Management:
Chelate with Deferoxamine:
Stable pts : levels< 500 mg/dl 40mg/kg IM/IV
Unstable: bleeding/ level > 500
• Give 20cc/kg NS/RL
• Deferoxamine at 15 mg/kg IV over 1hr
• Continuous drip at 15mg/kg/hr
• Continue till “vin rose” urine color disappears.

© 2013 National Safety Council
91
Iron PoisoningManagement:
Observe for:
◦ Systemic BP
◦ ECG
Signs of hepatic failure:
◦ Bleeding
◦ Glucose intolerance
◦ Hyper ammonemia and Encephalopathy

© 2013 National Safety Council
92
TreatmentEMERGENCY STABILIZATION
◦ Emergency stabilization begins with checking the ABCs (airway,breathing, and circulation), followed by a thorough physicalexamination and laboratory testing. Because the patient’s statuscan change rapidly, it is essential to reassess the patient often andmonitor the need for ventilator support.
92

© 2013 National Safety Council
93
Treatment1. Stabilize patient as needed
2. Estimate risk for systemic toxicity by amount of elemental iron
3. IV access
4. Laboratory exam
5. GI decontamination: whole bowel irrigation if tablets are seen onradiograph
6. Chelation

© 2013 National Safety Council
94
◦ Iron salts are chelated with desferrioxamine IV at15mg/kg/hour until the serum iron is <300 mg/dl or till24 hours after the child has stopped passing thecharacteristic ‘vin rose’ colored urine.
◦ Presence of ‘vin rose’ color to urine indicates significantpoisoning.
Treatment
© 2013 National Safety Council
95
Indications for Deferoxamine treatment - shock, altered mental status, persistent GI symptoms,
metabolic acidosis, pills visible on radiographs, serumiron level greater than 500 µg/dl, or estimated dosegreater than 60 mg/kg of elemental iron
- if a serum iron level is not available and symptoms arepresent

© 2013 National Safety Council
96
◦ If the patient is in shock, remember to at least type and screen (if not
cross match) for blood.
◦ Deferoxamine was derived from streptomyces pilosus.
◦ Ferrioxamin :This complex imparts a reddish, vin rosé, color to the
urine
◦ Hypotension and allergic reactions are seen.
◦ ARDS is a known complication and usually limit its use to 24 hours
or less.
Indications for Deferoxamine………
© 2013 National Safety Council
97
Complications
◦ Infectious -Yersinia enterocolitica septicemia
◦ Pulmonary - Acute respiratory distress syndrome (ARDS)
◦Gastrointestinal - Fulminant hepatic failure, hepaticcirrhosis, pyloric or duodenal stenosis
© 2013 National Safety Council
98
Prevention◦Keep out of reach of children
◦Put it up, Lock it up
◦Use child-resistant caps
◦ Follow dosing instructions
◦Be aware of multiple ingredients
98

®
© 2013 National Safety Council
Alcohol poisoning in children

© 2013 National Safety Council
100
Depressant
Contains intoxicating substance called ethyl alcohol orethanol
Slows down the functions of the brain and other parts ofthe nervous system
Produced by a fermentation process
What is Alcohol
100

© 2013 National Safety Council
101
Alcohol poisoning is a serious and sometimes deadly consequenceof drinking large amounts of alcohol
Alcohol poisoning occurs when a person drinks a toxic amount ofalcohol, usually over a short period of time.
Alcohol poisoning can also occur if a person drinks householdproducts that contain alcohol
If you suspect someone has alcohol poisoning, call for emergencymedical help right away
Alcohol Poisoning
101

© 2013 National Safety Council
102
If you're with someone who has been drinking a lot of alcohol• Call local emergency number immediately. • Never assume that a person will sleep off alcohol poisoning. • Be sure to tell hospital or emergency personnel the kind and
amount of alcohol the person drank, and when. • Don't leave an unconscious person alone. • While waiting for help, don't try to make the person vomit
because he or she could choke. 102

© 2013 National Safety Council
103
• Young children put everything in their mouths.
• It is not uncommon for children to accidentally swallow alcohol.
• But even a small amount of alcohol can cause alcohol poisoning in
children.
• This can result in serious illness and sometimes death.
• Children’s bodies absorb alcohol rapidly.
• it can occur in less than 30 minutes.
Alcohol and Infant/Toddler, Child
103

© 2013 National Safety Council
104
Effects of Alcohol◦Heart/Blood Vessels
Short term
◦Perspiration increases and skin becomes flushed
Long Term
◦High BP and damage to the heart muscle; blood vessels harden and become less flexible
© 2013 National Safety Council
105
More Effects◦Brain/Nervous System
Short Term◦ Speech is slurred and difficulty walking
Long Term◦ Brain cells are destroyed and unable to be replaced; damage to
nerves in body resulting in numbness in hands and feet

© 2013 National Safety Council
106
…The Rest of Alcohol Effects◦Liver
Short Term ◦ Liver changes alcohol into water and carbon dioxide
Long Term ◦ Liver is damaged possibly resulting in cirrhosis (scarring and
destruction of the liver)

© 2013 National Safety Council
107
Liver◦ Can only oxidize about 1 serving of alcohol an hour
◦ NO WAY to speed up this process
◦ Until liver has had time to oxidize all of the alcohol ingested, itkeeps circulating through the bloodstream
◦ Alcohol interferes with body’s ability to break down fats.
◦ Excess fat blocks flow in liver resulting in reduced oxygen and celldeath can be REVERSED when drinking stops
© 2013 National Safety Council
108
…The Rest of Alcohol Effects◦Stomach/Pancreas
Short Term ◦ Stomach acids increase, which often results in nausea
and vomiting
Long Term◦ Irritation occurs in the stomach lining, causing open
sores called ulcers; pancreas becomes inflamed
© 2013 National Safety Council
109
Symptoms can include confusion, vomiting, and seizures.
The child may have difficulty breathing and flushed or pale skin.
Alcohol impairs the gag reflex.
This can cause choking.
Alcohol may also cause low blood sugar in children.
This can result in a coma from the alcohol and/or the low sugar
Symptoms
109
© 2013 National Safety Council
110
• Slow down brain functions so one can lose his/her balance.
Irritate the stomach which causes vomiting and it stops gag reflex
from working properly
Affect the nerves that control your breathing and heartbeat, it can
stop both.
Dehydrate you, which can cause permanent brain damage.
Lower the body’s temperature, which can lead to hypothermia.
Lower your blood sugar levels, so you could suffer seizures.
Complication
110

© 2013 National Safety Council
111
• Alcohol ingestion in children needs to be treated immediately.
• Glucose may be given intravenously (IV).
• Sometimes a tube is inserted into the stomach to remove the
contents of the stomach.
• Children are observed until they recover.
• Some children may need to be stay in the hospital for evaluation.
• If there is evidence of neglect, child protective services may be
notified.
Treatment
111
© 2013 National Safety Council
112
1. Know what products in your home contain alcohol.
2. Keep all alcoholic drinks on a high shelf, out of your child’s reach.
3. Preferably, store them in locked cabinets.
4. All liquids should be kept in their original, labeled containers.
5. Avoid leaving them out on a counter.
6. Return all liquids to locked cabinets immediately after use.
7. Discard used containers where child will not find them.
8. Teach child the dangers of sampling any substance without your permission
Preventing Alcohol poisoning
112

Studies show that between 14% and 51% of adolescentattempters repeat their attempts depending partially onlength of follow-up period
Urban exposure can be significant, largely as a result of the use ofinsecticides for the control of flies, fleas, cockroaches and otherpests in the home, whether they are from household sprays orpesticides applied by professional exterminators.
Meriel Watts, 2013
Evidence
113
EvidenceA recent study in Australia found that there was widespreadchronic exposure of preschool children to organophosphate andpyrethroid insecticides and that, although most exposures werehigher in the rural area, urban children’s exposure tochlorpyrifos and bifenthrin was just as great, probably becausethey are used widely in domestic situations as well as in
agriculture.
(Babina et al 2012).114

Evidencestudy showed that age 01- 05years is the major group involved inpoisoning (59%) as compared to ages 6-10 years( 23%) and agebetween 11-15 years is (18%) .
Kerosene oil poisoning is most common (27%) followed byorganophosphates, corrosives, naphthalene and unknownpoisoning. Ayesha Asghar, 2010
Signs and symptoms of ingestion include burning and irritation oforal mucosa, nausea, vomiting, gastric irritation, jitteriness,breathing difficulties, and change in level of consciousness
115

EvidenceGeneral management of poisoning included supportive care andABC’s, treatment obtaining a history of exposure, vital signs
assessment, routine lab assessment, toxicology lab assessment, useof antidotes, skin decontamination, gastric decontamination, wholebowel irrigation, post diuresis and urinary pH manipulation,dialysis and hemoperfusion.
116

EvidenceThe study in West Bengal, India, revealed that consumption of foodfrom contaminated areas was another source of chronic Aspoisoning, since food products like vegetables and rice werecultivated using As-contaminated ground water.
Rahman et al., 2003The study showed that the average IQ of 720 children in the
endemic area was 92.07 compared to 93.78 children in thecontrol area, with 10.38% falling into the “low” IQ category versus4.24% in the control area. Yongping Li, 2008117
EvidenceA 2010 meta-analysis of 15 studies on residential pesticide useand childhood leukemia finds an association with exposure duringpregnancy, as well as to insecticides and herbicides. An associationis also found for exposure to insecticides during childhood.
Turner, M.C., et al. 2010.A meta-analysis study by scientists at the Harvard University’sSchool of Public Health finds that children’s exposure to pesticidesin and around the home results in an increased risk of developingcertain childhood cancers.
Chen M, Chi-Hsuan C, Tao L, et al. 2015.118

Evidence
A 2010 analysis observed that women who use pesticides in theirhomes or yards were two times more likely to have children withneural tube defects than women without these reported exposures.
Brender, JD., et al. 2010
One 2014 analysis of 129 preschool children, ages 20 to 66months, found that children were exposed to indoorconcentrations of pyrethroids, organophosphates andorganochlorines pesticides which were detected in soil, dust andindoor air.
Lu, C. et al. 2008.119

Reference difficult to use the la1. Accidental poisoning in children health Emergency department factsheets
2. Poisoning in Children Khurshid Ahmad Wani MD; Mushtaq Ahmad MD; Rauf-ur-Rashid Kaul MD; A S
Sethi MD; Shabnum MBBS
3. Federal Democratic Republic of Ethiopia Ministry of Health Food Hygiene and Safety Measures
Extension Package, 2004
4. A comparative retrospective study of poisoning cases in central, zonal and district hospitals Deepak
Pokhrel, Sirjana Pant, Anupama Pradhan, Saffar Mansoor, 2008
5. Dr K Berry Poisoning in children, 2008
6. AAea. Accidental Poisoning In Children J Biomed Sci and Res 2010;12(4):284-9.
7. Rahman, M.M.; Mandal, B.K.; Chowdhury, T.R.; Sengupta, M.K.; Chowdhury, U.K.; Lodh, D.; Chanda,
C.R.; Basu, G.K.; Mukherjee, S.C.; Saha, K.C.; Chakraborti, D. Arsenic groundwater contamination and
sufferings of people in North 24-Parganas, one of the nine arsenic affected districts of West Bengal,
India. J. Environ. Sci. Health, 2003, A38, 25–59.
8. Brender, JD., et al. 2010. Maternal Pesticide Exposure and Neural Tube Defects in Mexican Americans.
Ann Epidemiol. 20(1):16-22
9. Turner, M.C., et al. 2010. Residential pesticides and childhood leukemia: a systematic review and meta-
analysis. Environ Health Perspect 118(1):33-41
10. Lowengart, R., et al. 1987. “Childhood Leukemia and Parent’s Occupational and Home
Exposures,” Journal of the National Cancer Institute 79:39.
120

121