policy governance complaints - geh.nhs.uk
TRANSCRIPT
1 Complaints Policy V5
Management of Complaints Policy
ID Reference Number
GOV/POL/007
Category Policy
Classification: Governance
Search Criteria: Complaints
Purpose Defines how directorates manage and respond to complaints made by patients, clients, carers, relatives or friends, or on their behalf by an advocacy service or other bodies or individuals who have consent to act on behalf of the individual the complaint relates to.
Superseded Trust-wide Controlled Documents N/A
Version Number: 5.0
Date Approved by appropriate Group : December 2020 Complaints Policy Task & Finish Group
January 2021 Patient & Carer Experience & Involvement Group (PCEIG)
Date Approved by Controlled Document Review Group
14 January 2021
Date approved by Trust Board if applicable
Review Date: 6 January 2025 unless there is a legislative or evidence based change to practice.
Issue Date: January 2021
Title of Originator/Author Complaints Manager
Associate Director of Nursing
Title of Responsible Director: Director of Nursing
Impact / Equality Impact Assessed Yes
Target Audience All staff
If printed, copied or otherwise transferred from the Trust Intranet, policies and procedural documents will be considered uncontrolled copies. Staff must always consult the most up to date versions registered on the Trust Intranet.
2 Complaints Policy V5
Version Title of Trust Committee/Forum/Body/Group consulted during the development stages of
this controlled document Date
V5 Task and Finish Group established to review documents with all Directorates included. Completed 5.1.21. Raised with PCEIG 6.1.2021
Document Amendment Form
Number Date Page No. Amendment Authorised by
1.
12/21 All Full document review CDRG Jan/2021
2.
3.
4.
5.
6.
7.
8.
9.
10.
3 Complaints Policy V5
Table of Contents
Section Description Page
1 Introduction 4
2 Purpose & Scope 4
3 Policy Intention 4
4 Definitions 5
5 Duties and Responsibilities 5-6
6 Policy Details 7-14
7 Dissemination and Implementation 14
8 Document Control including Archiving Arrangements 14
9 Monitoring 15
10 GEH Associated Documents 15
11 References and Associated Bibliography 16
12 Staff Compliance Statement 16
13 Equality and Diversity Statement 16
13 Equality Impact Assessment Tool 17
14 Appendices: Appendix 1 Parliamentary and Health Service Ombudsman’s Principles for Remedy Appendix 2 Flow Chart Appendix 3 Easy Read - How to make a complaint leaflet
19 20 21-22
4 Complaints Policy V5
1. Introduction
George Eliot Hospital NHS Trust (herein referred to as ‘the Trust’) believes that an open and transparent system for dealing quickly and effectively with complaints about healthcare is one measure of the standard of service we provide to our patients, service users, their families, friends and significant others. Complaints are a way of obtaining the views of our service users and are a valuable source of information about our organisation’s quality of service and an opportunity for improving quality of services. Feedback is important and the Trust actively encourages patients and the public to express their concerns either through the complaints process or if a more immediate solution is needed, the Patient Advice and Liaison Service (PALS). Complaints should be viewed as a positive way to improve services and avoid or reduce the risk of similar situations occurring for others, thus forming part of the Trust’s Clinical Risk Management Strategy. The link between incidents and complaints is important in achieving this. The policy is available to all patients, service users, their families, friends and significant others irrespective of language, ethnicity or disability. No person will be discriminated against on the grounds of ethnicity, gender, age or sexual orientation. There is an easy read leaflet and access to the Trust’s translation service is via [email protected]. Patient care will not be compromised as a result of making a complaint. Where this is suspected, the patient or their representative must report this to the Complaints Service. This policy follows national guidelines and good practice as set out by the Parliamentary and Health Service Ombudsman. The current national pandemic,Coronavirus, SARS-CoV-2, (COVID-19) or other national emergency response situation, may influence reporting requirements not currently nationally determined. 2. Purpose and Scope This policy applies to all staff and services provided by the George Eliot Hospital NHS Trust. It defines how directorates manage and respond to complaints made by patients, clients, carers, relatives or friends, or on their behalf by an advocacy service or other bodies or individuals with consent to act on behalf of the individual. 3. The intention of the complaints policy is to: • Provide a policy that reflects national requirements and local directorate ownership. • Provide a service accessible to all with an easy read patient information leaflet
available (appendix 3). • Deal with complaints in an effective and efficient manner, mindful and sympathetic to
the circumstances. • Use complaints as a means of improving services, grouping and recording themes
and actions taken to address the complaints. • Involve the complainant and maintain regular dialogue as required. • Involving and engaging with the Directorate triumvirates and service management
teams. • Provide a balance between treating staff fairly and maintaining proper accountability
for their actions.
5 Complaints Policy V5
• Provide co-ordinated handling of those complaints which cross health and social care achieving a single response where possible.
4. Definitions Comments: Patients, service users, their families, friends and significant others may have valuable feedback good or bad relating to their experience and may wish to share this with the Trust Concern: Patients, service users, their families, friends and significant others may be worried about an aspect of the care and need some advice or clarification. These are issues that can often be resolved quickly in the interests of the patient and can be addressed informally for the purpose of service improvement. The complaint regulations support this approach. Complaint: A complaint is an expression of dissatisfaction, either in writing or verbally, about healthcare/treatment or services provided which requires an investigation and formal response. The Complaints Procedure referred to in this policy is in conjunction with the Local Authority Social Services and National Health Service Complaints (England) Regulations 2009. 5. Duties and Responsibilities Trust Board
The principal accountability of all providers of NHS-funded care is to patients, service users, their families, friends and significant others. In their fulfilment of this duty, the Trust Board accepts its responsibility to ensure that the Trust operates in the safest manner possible to protect users of its services and members of staff. Part of this responsibility is to ensure that an appropriate system is in place for the responding to formal complaints.
Chief Executive (CEO) The CEO has overall responsibility for patient experience and ensuring there are safe effective well led processes within the Trust which meet all statutory and regulatory requirements The CEO holds each line manager accountable for meeting objectives and to
work together towards meeting the objectives approved by the Board. Managing Director At George Eliot NHS Hospital Trust, the Managing Director has responsibility for formal complaints and fulfils the role of the responsible person under the Regulations. The Managing Director and the Medical Director are responsible for reviewing and signing off each individual complaint. In their absence the role is delegated to an Executive Member and one of the the Deputy Medical Directors. Director of Nursing The Director of Nursing is the nominated Executive with responsibility for complaints and will act for, and on behalf of the Trust Chief Executive Officer to ensure systems and processes are in place to lead the safe, effective, responsive, caring and well-led care and services for patients and their carers when accessing the complaints process at the Trust. More specifically, they have responsibility for ensuring there is a robust system in place for complaints management, for the regular reporting of complaints against the regulations and
6 Complaints Policy V5
standards set within this policy and to ensure quality improvement is achieved to patient experience and outcomes for our patients. Directorate Management Team The triumvirate which is made up of: Clinical Director General Manager Matron(s) The triumvirate receive all formal complaints relevant to their Directorate to ensure the appropriate investigation, oversight and accountability. Investigation Lead Within each Directorate the complaint will be managed by the nominated Investigation Lead with support from the Clinical Lead and the Governance Co-ordinator Lead. It is their responsibility to carry out a full investigation into issues raised, ensuring all points are addressed, that staff are interviewed/statements obtained from those involved or those with a responsibility for the service. The Investigation Lead will draft or oversee the response letter and provide any action plan/service improvement for those considered upheld or partly upheld. If required they will be supported by the Governance Co-ordinator Lead. Complaints Service
To facilitate the complaints process ensuring we are adhering to policy. The service will co-ordinate all complaints received within the Trust, including acknowledgement/seeking of consent/clarification of issues/response time. They can also act as a point of contact.
To identify where the complaint primarily relates to and circulate to the relevant Directorate Triumvirate for investigation. They will ensure the Directorate adequately addresses all points/questions raised.
Will support staff with statement writing/draft responses where needed.
Will ensure public and staff awareness of the complaints process and how to access it, providing any support as necessary.
Will develop and maintain systems which ensure that complaints are managed promptly and effectively with meaningful data held.
To provide complaints performance reports both internally and externally to the Trust.
To ensure we signpost to the Parliamentary and Health Service Ombudsman for complaints that cannot be resolved locally.
Will liaise with the Legal Services Manager and the Head of Risk Management for complaints subject to a serious incident, inquest or litigation.
Produce the quarterly statutory return (KO41a) for the Department of Health and Social Care and reports to the Quality Assurance Committee, Operational Quality and Safety Group and Trust Board as required.
7 Complaints Policy V5
Produce and circulate a Trust-wide Complaints Tracker for Directorate oversight and to help us achieve the response rate.
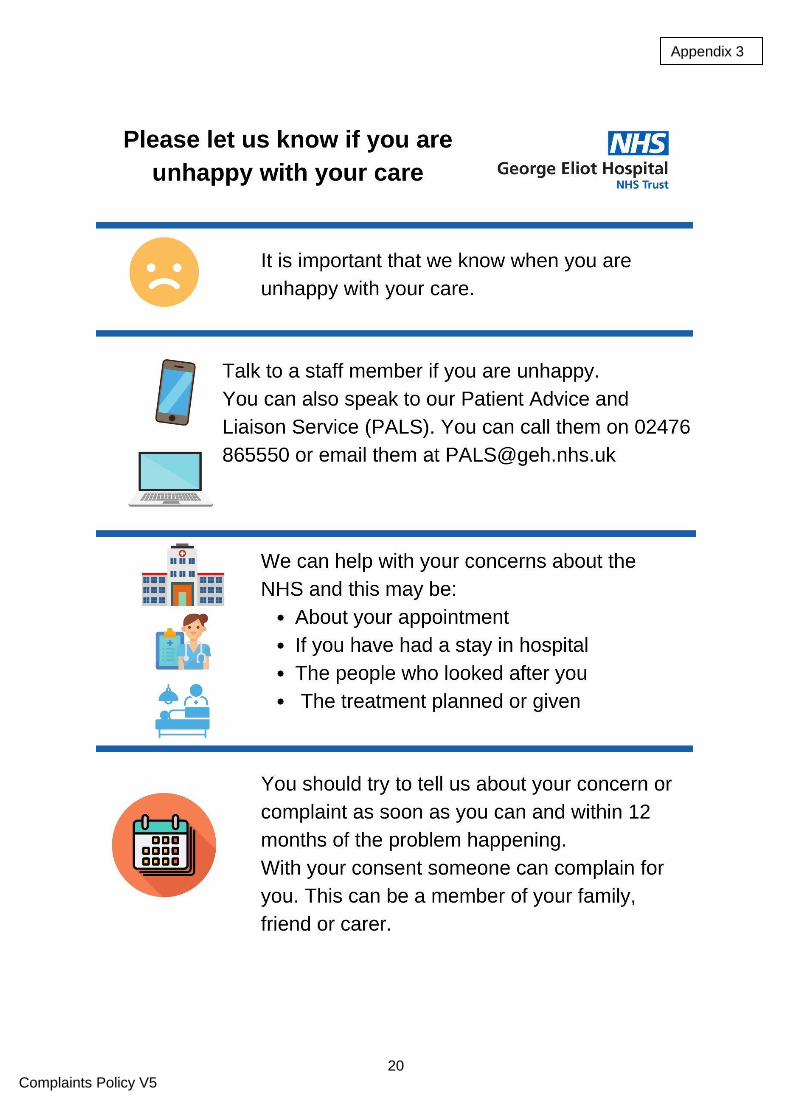
6. Policy Details 6.1 Patient Advice and Liaison Service (PALS) The Patient Advice and Liaison Service (PALS) has an important role in supporting those who wish to raise concerns. Not all issues benefit from being escalated to a formal complaint (e.g. the process does not influence clinical decisions and reprioritise patients) and there is often scope for PALS to seek a quick resolution and avoid the issue becoming a formal complaint. PALS also have a valuable role to play in providing support and advice for anyone wishing to pursue their concern as a complaint. This may be helping a complainant to write their complaint letter, explaining how the complaints process works or attending a complaints meeting, if requested. PALS can be contacted by: Email - [email protected] Telephone - 02476 86550 6.2 Independent Complaints Advocacy Service (ICAS) ICAS are independent organisations whose primary function is to support those making a formal complaint about the NHS. The Trust must make the complainant aware of this service and our local providers:
VoiceAbility Warwickshire - 0300 222 5947
POhWER Leicestershire - 0300 456 2370
Healthwatch Coventry - 0300 012 0315
Healthwatch Staffordshire - 0800 051 8371
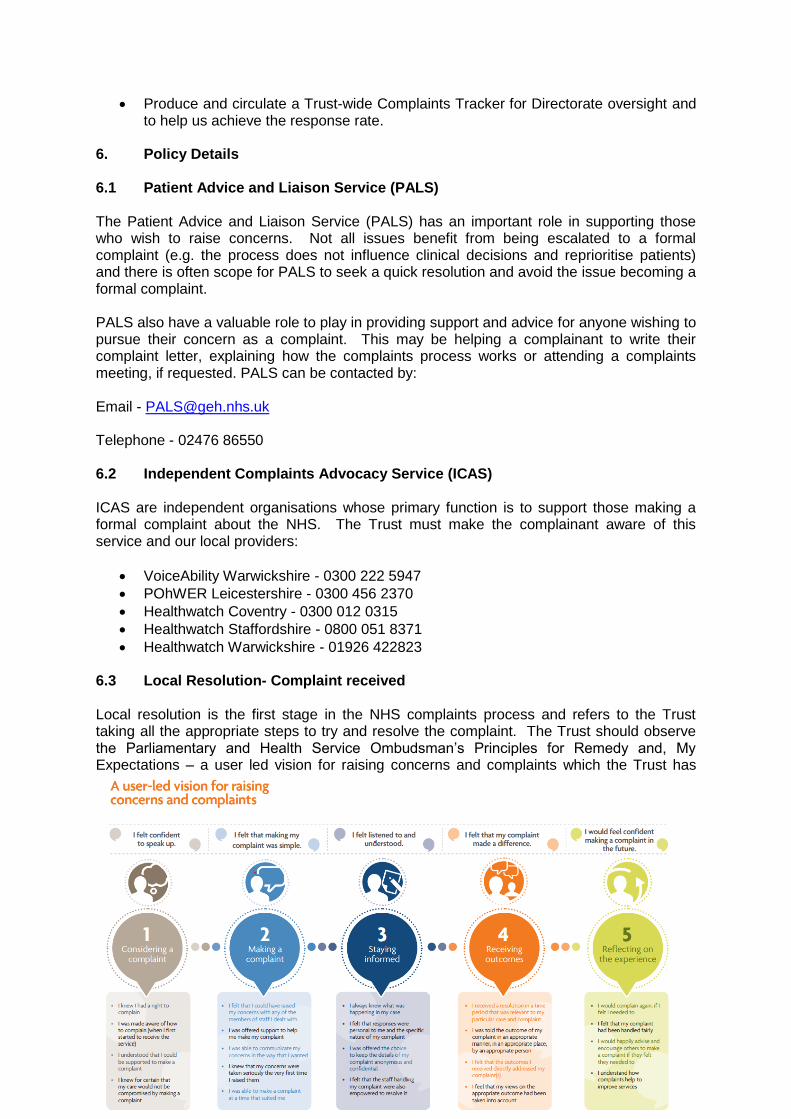
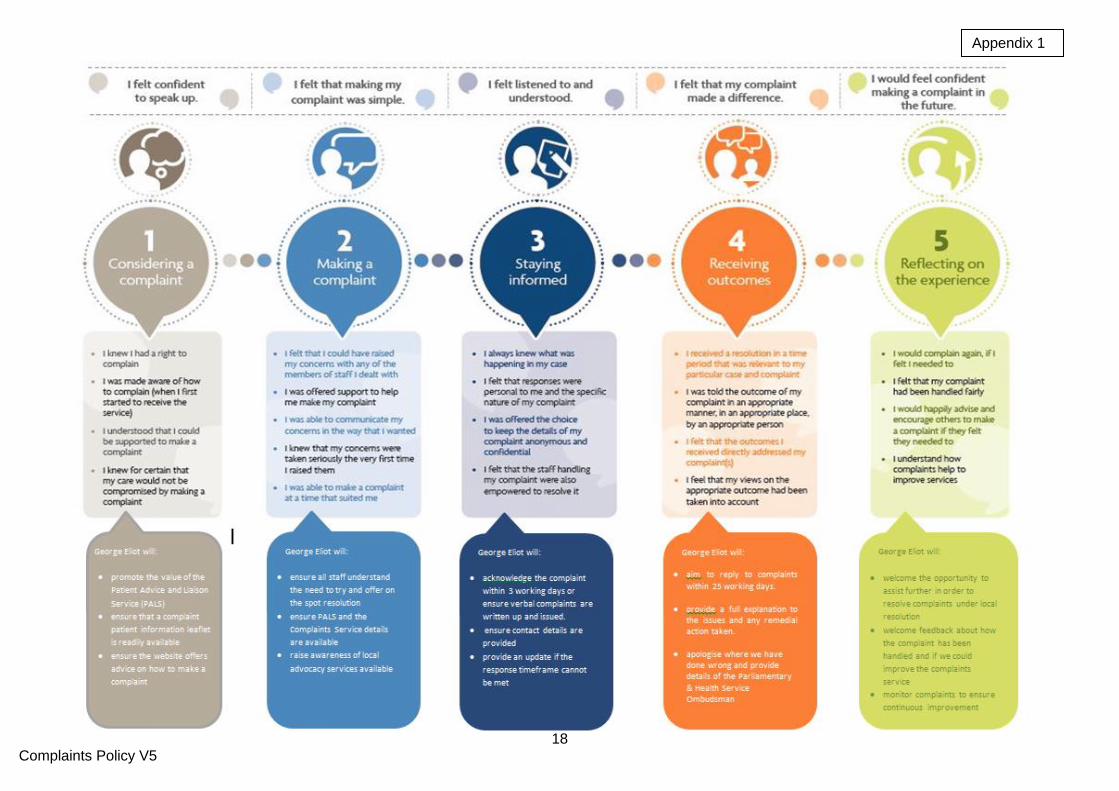
Healthwatch Warwickshire - 01926 422823 6.3 Local Resolution- Complaint received Local resolution is the first stage in the NHS complaints process and refers to the Trust taking all the appropriate steps to try and resolve the complaint. The Trust should observe the Parliamentary and Health Service Ombudsman’s Principles for Remedy and, My Expectations – a user led vision for raising concerns and complaints which the Trust has
8 Complaints Policy V5
added its own commitment to. (Appendix 1).
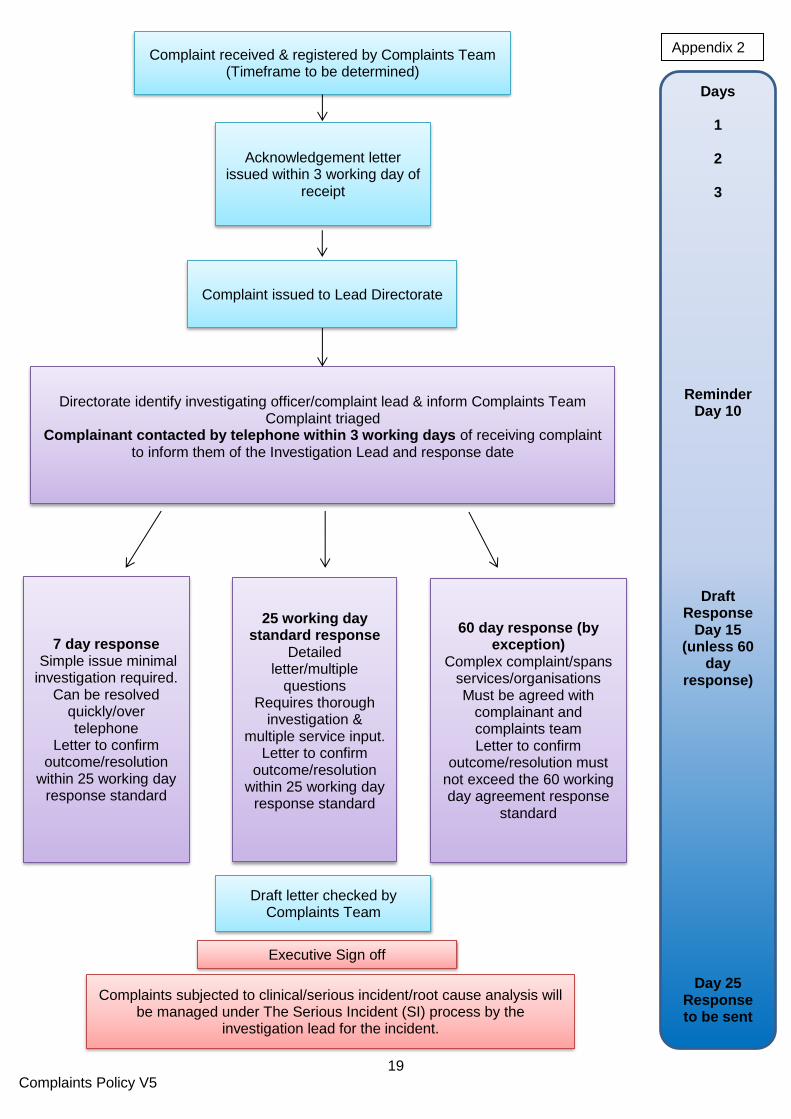
Depending on the complexity of the issues, the Trust will aim to ensure all complaints that are not subject to a serious incident review, are addressed within 7, 25 or 60 working days (Appendix 2 – Flow Chart). If the investigation cannot be completed within this timeframe the complainant will be kept fully informed. The aim is to resolve the issues raised in a timely and fair manner for all parties involved. Good communication is paramount to resolving complaints and this should be effective first and foremost, with the complainant being offered a point of contact. Details for the Complaints Service will be provided but the Investigation Lead for the complaint within the Directorate should try and contact the complainant. There should also be close links with any additional NHS or local government organisation involved to ensure a collaborative approach to responding to complaints. 6.4 Equal Treatment There are occasions when there is an irretrievable breakdown in the clinician/patient relationship, but it is important that a patient’s care is not adversely affected due to making a complaint. Patients or their representative, need to be assured that they can raise concerns without fear of recrimination and they should be encouraged to raise concerns if they consider the patient is being treated differently due to making a complaint. Complaint correspondence must not be filed within the patient’s healthcare records. All registered complaints will be dealt with fairly and effectively and as promptly as possible. However, calls and method of contact may be limited where unreasonable behaviour has been noted as a concern and complainants may need to be managed under the Violence and Aggression Policy. 6.5 Time Limit for Making a Complaint A complaint should generally be made: • Within 12 months of the date when the event being complained about occurred or • Within 12 months of becoming aware of the event The Trust will consider complaints made outside this time, the reasons for this and, whether there is scope to investigate matters fairly and effectively.
6.6 Receipt of Complaints The Trust will accept complaints made in writing, orally or by e-mail. Complaints made in writing are preferable to ensure the Trust receives the complainant’s views first hand rather than try and interpret them and represent them in the form of a summary. It is recognised that some people may need support in writing/making a complaint and the complainant should be made aware of the Advocacy Service linked to their area and, the Patient Advice and Liaison Service (PALS). If a verbal complaint is accepted the issues shared should be typed up and forwarded to the complainant within 3 working days for verification. The investigation will not commence until the issues have been agreed, signed and returned. All written complaints will be acknowledged in writing by the Complaints Service within 3 working days.
9 Complaints Policy V5
6.7 Persons who may make a Complaint A complaint may be made by:
Anyone who is receiving or has received care or treatment from the Trust.
A person who is affected or likely to be affected by an action, omission or decision of the Trust in relation to care or treatment.
A third party e.g. MP, relative, friend, carer, independent advocate on behalf of the patient.
A complaint may be made by a representative where that person:
• has died • is a child • is unable by reason of physical or mental incapacity to make the complaint
themselves • has requested the person to act on their behalf
6.8 Consent GDPR (General Data Protection Regulation) is important to the Trust and we have a duty to ensure that any information shared is for a legitimate purpose especially in circumstances where a complaint is made on behalf of a patient. If the patient is in a position to provide consent this must be obtained before an investigation commences. Where the complaint is made in respect of a person who has died the Trust will ask for the Executor or the Personal Representative to provide written consent along with supporting documentation such as the Grant of Probate or Last Will and Testament. When these are not in place a decision must be made by the Trust about the appropriateness of the person
making the complaint and the right to confidential information. When a patient lacks capacity to make a complaint themselves, the Trust must consider the role/relationship of the representative and that they are acting in the interests of the patient and, have a legitimate right to confidential information. The Caldicott Guardian may need to be involved to consider the position of the Trust and the person making the request. Please see the Information Governance Policy 2019. 6.9 Complaints Handling – Investigation - Outcome Incorporating the Parliamentary and Health Service Ombudsman Principles for Remedy and My Expectations is fundamental to resolving the complaint in the interests of both the Trust and the complainant. It is important that we:
invite the complainant to get in touch if a discussion would be helpful following receipt of their letter
establish what happened
what should have happened
establish if the issues need to be passed to the Risk Management Team and subject to review by the Serious Incident Group (SIG)
10 Complaints Policy V5
who was involved
obtain comments from those involved verbal or preferably written in response to all of the issues raised
seek comments if appropriate from those not directly involved but with a responsibility for the service or a more senior opinion
provide a written reply to the concerns in full within 25 or 60 working days with the exception of when a meeting being agreed in preference and the complainant is not available within the timescale.
make sure an appropriate and sincere apology is made if we have done wrong
identify any lessons learned and where applicable any actions which can be implemented
determine whether the complaint should be upheld, partially upheld or not upheld. Ideally the person who leads/investigates the complaint should arrive at this decision and input the ‘outcome’ code but may need to seek clinical advice on complex issues
ensure the time taken to respond to a complaint does not exceed 6 months. 6.10 Duty of Candour (Being Open and Transparent) In November 2014 and following the Francis Inquiry (2013) it is a legal requirement for Trusts under Duty of Candour to be open and transparent with people who use the services when something goes wrong that may have caused or lead to, significant harm in the future. Complaints are often linked to Duty of Candour and the Trust must be honest and open in its dealings with its patients and ensure staff know their responsibilities as set out in the Duty of Candour Policy and Process. 6.11 Potential Serious Incident (SI) All complaints are serious to those making them but it is recognised that some issues highlight a potentially serious clinical, procedural failure or allegation and are not known as the subsequent care has taken place at another provider. If the issue is not already being investigated under our Governance arrangements the Complaints Service will ensure that: • An incident is completed. • The complainant is informed (if Duty of Candour has not already been performed)
that a Root Cause Analysis (RCA) is to be undertaken which takes 60 working days to complete and that the Risk Management Team will be taking over the case with the appropriate Investigation Lead contacting them to see if they would like to contribute to the investigation with contact details for the Investigation Lead provided.
6.12 Disciplinary Action Staff must be supported in any complaint received but it is recognised that some complaints may lead to disciplinary and conduct procedures being instigated separately. It is not the Trust’s policy to share this action and any outcome with the complainant. The complainant can be advised that if disciplinary action or performance management is indicated they will not be informed of the outcome but that the staff member may be subject to further Trust policies/procedures. 6.13 Further Local Resolution Although the aim of following the above process is that the complaint will be resolved, the Trust recognises that complainants may not always be satisfied with the explanations and any remedial action identified. It is also possible that the information provided may lead to

11 Complaints Policy V5
further concerns being raised. The complaint response should provide the opportunity for the complainant to approach the Trust again and if a meeting is not indicated a further written response should, where possible, be provided within 25 working days. It is beneficial to receive from the complainant the outstanding issues in order to reply further or, to place the correct staff in a meeting to ensure a helpful discussion can take place. 6.14 Parliamentary and Health Services Ombudsman (PHSO) review Local Resolution is not always possible even when further responses or a meeting have been provided. The details for the PHSO must be given within the first response to the complaint in the event the complainant remains dissatisfied and does not wish to engage further with the Trust. The Trust equally, can reach the point where local resolution has been exhausted and consider the complainant will benefit from the independence of the PHSO. In the interests of resolving the complaint the Trust needs to fully cooperate with any requests made by the PHSO. The contact details for the PHSO are: The Parliamentary and Health Service Ombudsman Millbank Tower Millbank London SW1P 4QP Telephone 0345 015 4033 Email - [email protected] 6.15 Care Quality Commission (CQC) The Health and Social Care Act (2008) (Regulated Activities) Regulations (2014), Regulation 16, is to ensure that people can make a complaint about their care and treatment. To meet this regulation we have to ensure we have an effective and accessible system to manage complaints that must be thoroughly investigated with actions taken where failings are identified. Although not involved in investigating complaints, it is recognised that the CQC may be contacted by a complainant and may need to request details of the complaint or, seek reassurance the matter is/has been dealt with. The Trust needs to comply with any requests made by the CQC. 6.16 Publicity The Trust has a statutory duty to make information available to the public on the complaints process. Information is detailed on the Trust’s website and an easy read leaflet on how to make a complaint is available throughout the Trust. This provides contact details on the Independent Complaints Advocacy Service (ICAS) and Patient Advice and Liaison Service (PALS). It is important to be aware that complainants may be unable to write, may not have English as their first language or have disabilities which make writing formal complaints difficult. PALS and ICAS can assist with these issues by sourcing services to assist complainants who need to communicate verbally, who require interpreting or translation services, services for blind/partially sighted or deaf/impaired hearing and for those unable to put their complaint in writing.
12 Complaints Policy V5
6.17 Exclusions Exclusions from the Trust’s Complaints Policy:
a complaint that has already been investigated under the NHS Complaints Procedure
complaints by a responsible body1
complaints regarding NHS employment
private healthcare.
a complaint made orally that is resolved satisfactorily
complaints regarding requests under the Freedom of Information Act 2000 6.18 Complaints involving more than one organisation When a complaint is received that involves more than one NHS organisation and/or social care the recommendation is to provide a coordinated response having established who should lead and communicate with the complainant. Due to the varying response timeframes across the organisations this may not always prove possible and Trusts on occasion, may need to reply in isolation. Permission should be sought from the complainant in advance of sharing the complaint with any other provider. If a complaint is received by the Trust that is solely about the services provided by another organisation the complainant must be referred to the relevant organisation and informed by letter or email as appropriate.
6.19 Unreasonable behaviour The Trust is committed to dealing with complaints fairly and compassionately to any clinical conditions the person may have. Persistent complainants can however occur and place undue stress on NHS staff with little hope of resolution. Whilst there may be substance to the complaint and this must be dealt with in accordance with the regulations. We do not expect staff to endure difficult situations or behaviour that is offensive, abusive or frequent in nature. We may, on occasion need to restrict how someone can contact us. It is important that as a Trust we:
Record any incident of unreasonable behaviour or excessive contact on DATIX so that we can monitor the frequency and nature of the contact and who is involved.
Confirm the issues to ensure they are appropriate to the NHS Complaints Procedure, are within time and have not already been subject to the process
Exhaust all reasonable efforts to engage with the complainant to resolve the issues
Provide details of an advocacy service.
Determine whether we need to restrict contact in the form of nominating a particular person or service, method of contact eg written correspondence only and if a timescale needs to be attached to the restriction. This needs to be done in writing and with a letter from the Chief Operating Officer or their representative.
Inform the complainant why we believe their behaviour is unacceptable and what action we have decided to take eg written correspondence only.
Where needed invoke the Management of Violence and Aggression Policy
1 Responsible body means Local Authority, NHS Body, Primary Care provider or Independent provider.
13 Complaints Policy V5
6.20 Litigation or allegations relating to serious misconduct If litigation is indicated or commenced, the Trust will need to ensure that the complaints process will not prejudice any legal or judicial action. It is unusual for complaints and legal action to run concurrently but if there are no contra-indicators, the complaint investigation can commence alongside litigation. Where a complaint alleges serious misconduct or issues of a criminal nature the relevant Director should be notified immediately to enable decisions on the most appropriate way forward as the complaints process may no longer remain relevant.
6.21 Learning from Complaints Remedial Action and Compensation It is important to share all complaints even those which are not considered upheld and that we learn from those that are with foundation. The Directorate must detail within their responses, a full explanation to the issues raised coupled with any action that has been taken as a result of the complaint. If the complaint is subject to a root cause analysis (RCA) the final report overseen by the Risk Management Team will be made available to the complainant. Any concerns outside of the scope of the RCA will be investigated by the Directorate and included in a covering letter with the RCA. Complaints must be discussed at ward and departmental meetings, directorate governance meetings and reports will be received at Operational Quality and Safety Group and Quality Assurance Committee to ensure ward to board feedback. Not all complaints require financial remedy and complainants often seek an apology when we have done wrong. The Trust should consider all forms of remedy, such as acknowledging if a mistake has been made, an explanation of events, action taken as a result and, where appropriate, financial reimbursement. Ex-gratia payments in respect of expenses incurred by patients should also be considered where the Trust is found to be at fault. The PHSO may also recommend redress for the complainant in instances where they partly uphold or fully uphold a complaint following investigation. Complainants seeking compensation for a non-quantifiable loss, eg negligence and distress are to be advised to seek independent legal advice. 6.22 Retention of Complaints Documentation Registered complaint files will be kept for 10 years in the archive storage area. It is imperative that complaint correspondence is not filed in a patient’s health records. A copy of a complaint file can be requested under GDPR. 6.23 Complaints Reporting The Complaints Service will provide reports for the relevant committees for oversight and assurance purposes and reporting will include:
Monthly reports for the Directorates
A quarterly K041a report
14 Complaints Policy V5
Contribute to the quarterly Patient Experience Report which feeds into Operational Quality & Safety Group and Quality Assurance Committee. The Complaints Manager will contribute to an Annual Patient Experience Report.
This report will include:
Numbers of complaints received.
Categories and areas complained about.
Whether the complaint was upheld, partly upheld or not upheld
Any complaints referred to the Parliamentary and Health Service Ombudsman and their decision.
Any significant lessons learned and actions taken.
Response rate
7. Dissemination and Implementation The Policy will be saved on the Trust’s intranet system and is available to all Trust staff. Key risk committees will receive notification of its renewal and the Policy will be signed off by the Controlled Document Review Group, (unless there are any significant changes made to the National Policy in the interim). Training will be available to staff to ensure they understand the requirements of the NHS Complaints Procedure and their responsibilities. 8. Document Control/Archiving The document will be managed as per the process described within the Trust’s Policy for the Development and Management of Controlled Documents. This policy will be reviewed at the date specified or earlier if circumstances dictate. This document will be included on the Trust intranet site under the Master Policy Library.
15 Complaints Policy V5
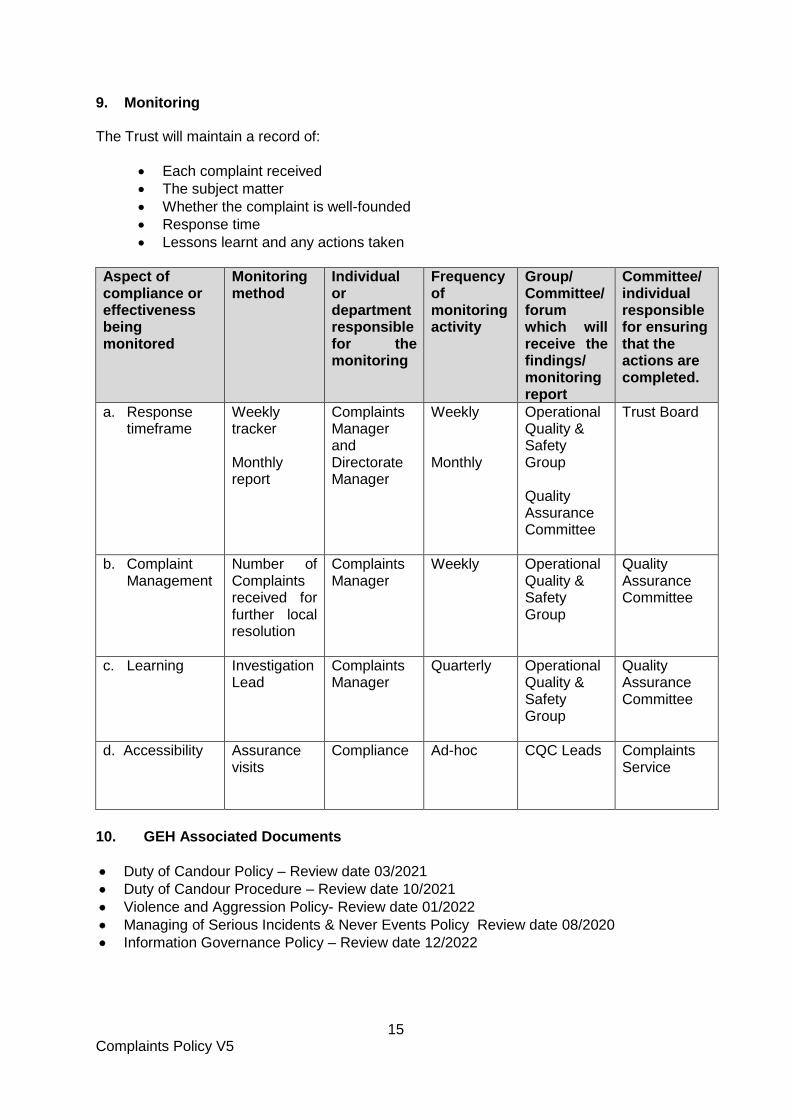
9. Monitoring The Trust will maintain a record of:
Each complaint received
The subject matter
Whether the complaint is well-founded
Response time
Lessons learnt and any actions taken
Aspect of compliance or effectiveness being monitored
Monitoring method
Individual or department responsible for the monitoring
Frequency of monitoring activity
Group/ Committee/ forum which will receive the findings/ monitoring report
Committee/ individual responsible for ensuring that the actions are completed.
a. Response timeframe
Weekly tracker Monthly report
Complaints Manager and Directorate Manager
Weekly Monthly
Operational Quality & Safety Group Quality Assurance Committee
Trust Board
b. Complaint Management
Number of Complaints received for further local resolution
Complaints Manager
Weekly Operational Quality & Safety Group
Quality Assurance Committee
c. Learning Investigation Lead
Complaints Manager
Quarterly Operational Quality & Safety Group
Quality Assurance Committee
d. Accessibility Assurance visits
Compliance Ad-hoc CQC Leads Complaints Service
10. GEH Associated Documents
Duty of Candour Policy – Review date 03/2021
Duty of Candour Procedure – Review date 10/2021
Violence and Aggression Policy- Review date 01/2022
Managing of Serious Incidents & Never Events Policy Review date 08/2020
Information Governance Policy – Review date 12/2022
16 Complaints Policy V5
11. References and Associated Bibliography
Care Quality Commission (2016) Learning, candour and accountability. Available at: http://www.cqc.org.uk/sites/default/files/20161213-learning-candour-accountability-full-report.pdf (Accessed: 11 January 2021). Freedom of Information Act 2000, c. 36. Available at: https://www.legislation.gov.uk/ukpga/2000/36/contents (Accessed: 12 January 2021). Health and Social Care Act 2008, c. 14. Available at: http://www.legislation.gov.uk/ukpga/2008/14/contents (Accessed: 11 January 2021). Local Government Ombudsman (2014) My Expectations for Raising Concerns and Complaints. Available at: https://www.ombudsman.org.uk/sites/default/files/Report_My_expectations_for_raising_concerns_and_complaints.pdf (Accessed: 11 January 2021). Parliamentary and Health Service Ombudsman (2009) Principles for Remedy. Available at: https://www.mbudsman.org.uk/about-us/our-principles/principles-remedy (Accessed: 11 January 2021). The Local Authority Social Services and National Health Service Complaints (England) Regulations 2009. (SI 2009/309). Available at: http://www.legislation.gov.uk/uksi/2009/309/contents/made (Accessed: 11 January 2021). The Mid Staffordshire NHS Foundation Trust Public Enquiry (2013) Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry (Francis Report). Available at: https://www.gov.uk/government/publications/report-of-the-mid-staffordshire-nhs-foundation-trust-public-inquiry (Accessed: 12 January 2021).
Department of Health and Social Care (2021) NHS complaints guidance. Available at: https://www.gov.uk/government/publications/the-nhs-constitution-for-england/how-do-i-give-feedback-or-make-a-complaint-about-an-nhs-service (Accessed: 12 January 2021). 12. Staff Compliance Statement All staff must comply with the Trust-wide controlled document and failure to do so maybe considered a disciplinary matter leading to action being taken under the Trust’s Disciplinary Procedure. Actions which constitute breach of confidence, fraud, misuse of NHS resources or illegal activity will be treated as serious misconduct and may result in dismissal from employment and may in addition lead to other legal action against individual concerned. 13. Equality and Diversity Statement The Trust aims to design and implement services, policies and measures that meet the diverse needs of the needs of our service, population and workforce, ensuring that none are placed at a disadvantage over others.
17 Complaints Policy V5
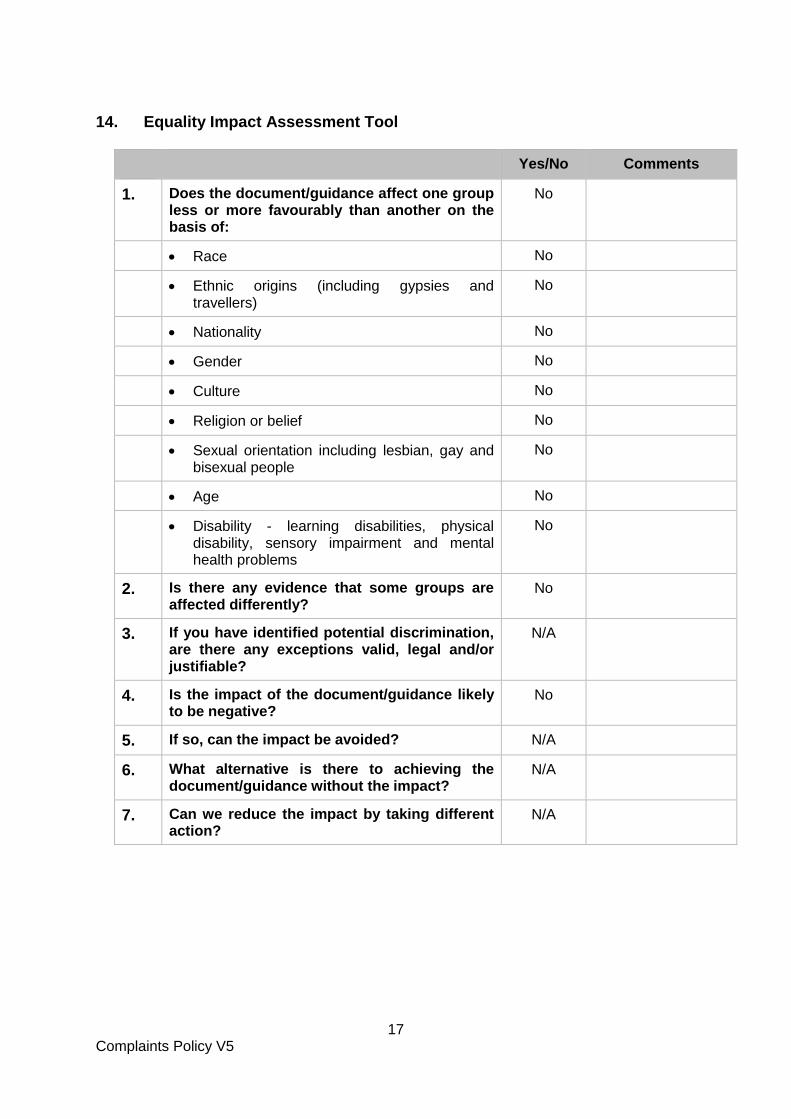
14. Equality Impact Assessment Tool
Yes/No Comments
1. Does the document/guidance affect one group less or more favourably than another on the basis of:
No
Race No
Ethnic origins (including gypsies and travellers)
No
Nationality No
Gender No
Culture No
Religion or belief No
Sexual orientation including lesbian, gay and bisexual people
No
Age No
Disability - learning disabilities, physical disability, sensory impairment and mental health problems
No
2. Is there any evidence that some groups are affected differently?
No
3. If you have identified potential discrimination, are there any exceptions valid, legal and/or justifiable?
N/A
4. Is the impact of the document/guidance likely to be negative?
No
5. If so, can the impact be avoided? N/A
6. What alternative is there to achieving the document/guidance without the impact?
N/A
7. Can we reduce the impact by taking different action?
N/A
18 Complaints Policy V5
Appendix 1
19 Complaints Policy V5
Appendix 2 Complaint received & registered by Complaints Team
(Timeframe to be determined)
7 day response Simple issue minimal investigation required.
Can be resolved quickly/over telephone
Letter to confirm outcome/resolution
within 25 working day response standard
25 working day standard response
Detailed letter/multiple
questions Requires thorough
investigation & multiple service input.
Letter to confirm outcome/resolution
within 25 working day response standard
60 day response (by exception)
Complex complaint/spans services/organisations Must be agreed with
complainant and complaints team Letter to confirm
outcome/resolution must not exceed the 60 working day agreement response
standard
Complaints subjected to clinical/serious incident/root cause analysis will be managed under The Serious Incident (SI) process by the
investigation lead for the incident.
Acknowledgement letter issued within 3 working day of
receipt
Complaint issued to Lead Directorate
Directorate identify investigating officer/complaint lead & inform Complaints Team Complaint triaged
Complainant contacted by telephone within 3 working days of receiving complaint to inform them of the Investigation Lead and response date
Draft letter checked by Complaints Team
Executive Sign off
Days
1
2
3
Reminder Day 10
Draft
Response Day 15
(unless 60 day
response)
Day 25 Response to be sent
20 Complaints Policy V5
Appendix 3

21 Complaints Policy V5
Appendix 1