poll everywhere learning objectives - napnap.org€“child‐neck, b ac, b pop fossa, b ankles /...
TRANSCRIPT

1
39th National Conference on Pediatric Health Care
©2018
March 19-22, 2018 CHICAGO
When It’s Not Eczema: Reviewing common and not so common differential diagnosis for Atopic Dermatitis
Rebecca Flynn, MSN, APRN, CPNP‐ PCAPRN III‐ Dermatology Clinic
Children’s Mercy Hospitals and ClinicsKansas City, MO
©2018
Disclosures
• No disclosures to report.
©2018
Poll Everywhere
• https://www.polleverywhere.com/login
©2018
Learning Objectives
1. Review etiology, history, symptoms and treatment of atopic dermatitis.
2. Differentiate various forms of eczema including nummular eczema, dyshidrotic eczema, and papular atopic dermatitis.
3. Identify differential diagnosis of atopic dermatitis including scabies, psoriasis, allergic contact dermatitis, papular urticaria, palmar/ plantar juvenile dermatosis, seborrhea dermatitis, keratosis pilaris and perioral dermatitis.
4. Initiate preliminary treatment plan for common differential diagnosis of atopic dermatitis including scabies, psoriasis, allergic contact dermatitis, papular urticaria, palmar/ plantar juvenile dermatosis, seborrhea dermatitis, keratosis pilaris and perioral dermatitis.
©2018
Atopic Dermatitis
©2018
Atopic Dermatitis
• Dry, rough, itchy skin• Waxes and Wanes• Often begins <2 years of age‐ Some older• Commonly exists with atopy
– Allergies, Asthma, Atopic Dermatitis– Strong Family History
• Responds to Moisture and Topical Steroids• Distribution of dermatitis
– Infant‐ face, scalp, trunk, back, elbows, knees– Child‐ neck, B AC, B pop fossa, B ankles/ feet– Adult‐ Hands, feet

2
©2018
Atopic Dermatitis‐ Treatment
• Sensitive Products– Dye‐free, Scent‐free products: soap, laundry detergent, dryer sheet
• Moisture– Bland ointment/ cream emollient
• Vaseline ointment, Aquaphor ointment• Vanicream, Cetaphil cream
– Daily bathing
• Topical Steroid‐ BID Ointments!– Mild‐ Hydrocortisone 2.5% ointment, Alclometasone ointment– Moderate‐ Triamcinolone 0.1% ointment– Strong‐ Mometasone ointment, Fluocinonide ointment
©2018
Atopic Dermatitis‐ Topical Steroids
Face, axilla, groin
Body only. Not on face, axilla, groin(Tollefson, 2014)
©2018
Atopic Dermatitis‐ Treatment
• Topical Calcineurin Inhibitors
– Elidel cream
– Tacrolimus (Protopic) 0.03%, 0.1% ointment.
– Black box warning
• Crisaborole (Eucrisa)
©2018
Atopic Dermatitis‐ Treatment
• Antihistamines– Daily non‐sedating‐ Zyrtec
• As needed for Allergy control to prevent flares
– Sedation effect to aid sleep• Benadryl• Hydroxyzine• Doxepin
• Melatonin‐ 1‐5 mg nightly• Bleach Baths
– ¼ cup unscented bleach to ½ tub of water
• Topical Antibiotics and Oral Antibiotics (cultures)– Mupirocin 2% ointment– Keflex & Clindamycin
• Wet Wraps
©2018
Variations of Eczema
• Nummular
• Dyshidrotic
• Papular Eczema

3
©2018
Case Study #1
• 10 year old patient is evaluated in clinic with sibling dual appointment.
• Chief complaint: rash for 2‐3 months.
• Involved areas include arms, legs, stomach, hands and feet. Pruritis is intense and worse at night. Sibling’s rash started 1 month prior to the patient’s rash. Attempted hydrocortisone 1% ointment which improved itching but rash has continued to spread. Prior to new rash 2‐3 months ago patient had normal skin.
©2018
©2018
Scabies Scabies mites
Working for a living!
©2018
Scabies
• Live 15‐30 days
• Lays 1‐4 eggs per day, hatch 3‐4 days
• 15‐20 minutes close contact‐ transmit scabies
• Incubation‐ 3 weeks
• Pruritis!!!‐ Worse night time
• Papules, nodules, burrows, vesiculopustules– Interdigital space, wrists, ankles, axilla, waist, buttock, groin, palms, soles
HISTORY!©2018
Scabies
• Diagnosis– Clinical symptoms‐ burrows, delta sign– Scabies prep skin scraping
• Treatment– Permethrin 5% cream
• Head/ scalp down in infant, neck down child.• Apply, leave on overnight 8‐14 hours• Do not use under 2 months.• Repeat 7 days later• Treat ALL household members (affected 2 treatments, unaffected 1 tx)
– Sulfur 6% compounded in Vaseline• Safe for infants and pregnant or nursing moms• Apply neck down for 3 consecutive nights. Rinse 24 hours later
– Ivermectin‐ severe infestation resistant to topical treatment (rare)• Not used under 5 years of age

4
©2018
Scabies‐ Before and After
©2018
Case Study #2
• 10 year old patient is evaluated in clinic with chief complaint of new rash. Rash started 3‐4 months ago on arms, legs, scalp, and trunk including umbilicus. Affected areas are mildly pruritic but do not disturb sleep. Attempted Aquaphorointment which decreased dryness of rash but redness has not improved. Rash has worsened over the last 2 weeks and patient has new complaint of headache, sore throat, and stomach ache.
• Previously patient had normal skin with the exception of numerous diaper rashes during infancy.
©2018 ©2018
Psoriasis Vulgaris
• Chronic Immune‐mediated disorder
• Rarely present at birth
– 1/3 of cases present before 20 years old.
• Highly genetic‐ immune activation & cutaneous inflammation
• Known triggers: Streptococcal infection, Staph A. infection, psychological and physical stress.
• Characteristic Rash: round, brightly erythematous, well‐marginated plaque with greyish or silvery‐white overlying scale
©2018
Psoriasis Vulgaris
• Distribution:
– Scalp, elbows, knees, lumbosacral, groin
• Inverse Distribution:
– Axilla, groin, umbilicus
Presents within areas of trauma.
©2018
Psoriasis Vulgaris
• Comorbidities
– Obesity, Early cardiovascular disease/ Metabolic Syndrome, JuvenilleIdiopathic Arthritis, Crohn’s disease, anxiety/ depression.
• Treatment
– Topical corticosteroids (often moderate‐ strong)
– Topical calcineurin inhibitors
– Topical Vitamin D‐ calcipotriene (Dovonex)
– UV light‐ NBUVB therapy
– Systemic therapy‐ Methotrexate, Cyclosporine, Acitretin (Dermatologist)

5
©2018
Guttate Psoriasis
• Often children‐ 1st manifestation of Psoriasis
• Drop‐like (guttate), round/ oval lesions (2‐6mm)
• Symmetrical on trunk, extremities
• Often triggered by Group A Strep infection (throat, skin, anal)
• 40% develop plaque psoriasis
©2018
Guttate Psoriasis
©2018
Case Study #3
• 4 year old patient has developed a new rash on B posterior legs and inner thighs. Rash developed 6‐8 weeks ago. Affected area is highly pruritic and patient often scratches until bleeding. Patient has had many new sleep disturbances related to intense pruritus of skin. No other family members are affected. Patient recently started preschool.
©2018
©2018
Allergic Contact Dermatitis
• Type IV hypersensitive reaction (delayed) generally 8‐12 hours
• Sensitivity after re‐exposure days‐ years
• Most common: poison ivy, nickel, fragrance, dyes, wet wipes, lanolin, antibiotics, rubber, formaldehyde
• Distribution!
• Sharp edges, erythema, vesicles, bullae present.
©2018
Allergic Contact Dermatitis

6
©2018
Allergic Contact Dermatitis
©2018
Allergic Contact Dermatitis‐ Treatment
• Identification of trigger
• Topical steroids
• Oral steroids
• Antihistamines
– Zyrtec, Benadryl or hydroxyzine
• Moisturizers
• Avoidance of triggers
©2018
Identification of Triggers
• Patch testing
– 5 day test.
– http://www.smartpractice.com/Apps/WebObjects/SmartPractice.woa/wa/content?f=product‐truetest.html&m=SPA
©2018
Case Study #4
• 7 year old patient presents with new rash on B arms and B legs. Rash has been present for 2‐3 months. Mother reports new, red spots appear on arms and legs. Patient often scratches until bleeding. Rashes often wax and wane. Mother reports it appears as if the rash never completely resolves. Attempted hydrocortisone 1% ointment without much relief. Family has 1 dog and 1 cat in the household.
©2018 ©2018
Papular Urticaria

7
©2018
Papular Urticaria
• Chronic, papular eruption due to hypersensitivity to bug bites
• Highly pruritic
• High risk of secondary infection due to scratching.
• Summer & Late Spring
©2018
Papular Urticaria
• Treatment– Insect Repellent
• Unscented OFF
– Low‐ mid potency topical steroids• Hydrocortisone 2.5% ointment
• Desonide ointment / Alclometasone ointment
• Triamcinolone 0.1% ointment
– Topical antibiotic• Mupirocin 2% ointment
– Antihistamines‐ aid sleep, relieve itch• Benadryl or Hydroxyzine
©2018
Bed Bug
Flea Bites
©2018
Case Study #5
• 2 year old patient presents to clinic with a 3 day history of red, itchy rash diffuse on entire body. Mother reports patient is experiencing difficulties sleeping. The mother reports the family is exhausted because the patient did not sleep well the week before due to a runny nose and cough. The rash started on patients arms the first day but has since spread to the entire body. The patient is very itchy and occasionally scratches until bleeding.
©2018
Viral Exanthum
©2018
Viral Exanthum
• Macules and Papules‐ DIFFUSE!
• Within setting of fever, headache, fatigue, respiratory or GI symptoms
• Resolve within 1 week.
• Gianotti‐Crosti syndrome (viral exanthum)‐ resolve within 8‐12 weeks
• If pruritic‐ mild potentency topical steroids
• Emollients
• New Drugs?

8
©2018 ©2018
Case Study #6
• 11 year old male presents with thick, pruritic, erythematous rash on B soles of feet. Both soles of patient are affected while hands and arms are spared. Family attempted hydrocortisone 1% cream without any relief. Upon examination, sweaty palms and soles are noted. Patient has never had any skin rashes on other areas of his body prior. Rash has been present about 2‐3 months. Occasionally, patient’s feet become so inflamed painful cracks (fissures) develop.
©2018 ©2018
Juvenile Palmar/ Plantar Dermatosis
• “Sweaty‐sock syndrome”
• Distal aspects soles‐ sparing interdigital spaces
• Associated with hyperhidrosis
• Smooth, red, glazed with fine scaling (chronicity‐lichenification)
©2018
Juvenile Palmar/ Plantar Dermatosis
• Treatment–Wear all‐cotton socks
– Change damp socks frequently
– Dust absorbent powder if desired
– Avoid occlusive shoes without cotton barrier
– Apply ointment emollient upon removing shoes
–Moderate potency topical steroid‐ Triamcinolone 0.1% ointment
– Fissures‐ super glue
– Crusting, secondary infection‐ topical antibiotic, Mupirocin ointment
©2018
Case study #7
• 3 month old patient presents to clinic for evaluation of a new rash. Rash appeared 3‐4 weeks ago and seems to have worsened over the last several days. Affected areas include face, neck, arms, legs, axilla, and inguinal folds. Scaling is noted in patient’s scalp. Red patches appear shiny in folds of skin. Mother and father report patient is sleeping well.

9
©2018 ©2018
Seborrhea Dermatitis
• Self‐limiting erythematous, scaly or crusting eruption
• Etiology: unknown‐ overgrowth of yeast (Malassezia)
• Onset: 2‐10 weeks. Peak: 3 months
• Infants– Scalp, intertriginous, flexural, diaper
• Adolescent– Scalp, eyebrow, bridge of nose, nasolabial crease, post‐auricular
• Thin dry scales / well defined red patches with brown, greasy crust
• Pruritis‐ absent or minimal
©2018
Seborrhea Dermatitis
• Treatment
–Most clear spontaneous by 1 year
– Tear‐free shampoo with frequent washing
– Ketoconazole 2% shampoo/ cream
– Low‐potency topical steroids
–Mineral oil‐ removal of scales
©2018
Seborrhea Dermatitis
©2018
Case Study #8
• 15 year old patient presents with concern for new rash on chest. Rash appeared 1 month ago. Over the last month the rash has spread to encompass entire chest extending to B arms and back. Rash is red, slightly scaly and pruritic. Patient attempted hydrocortisone 1% cream OTC for 2‐3 days. Pruritisimproved but rash remained and continued to spread. Patient is active in football. Family has 2 household cats.
©2018

10
©2018
Tinea Incognito (Tinea Corporis)
©2018
Tinea Incognito
• Tinea Corporis‐ morphed due to topical steroids
• Superficial fungal infection
• Risks: contact wrestler, kittens, gerbils
• Species: M. Canis, Trichophyton species
• Annular, red, scaly, central clearing, sharp border
• Topical steroid makes worse, rash spreads (hallmark presentation masked)
©2018
Tinea Incognito
• Treatment
– Dermatophyte culture
– Topical antifungal cream
• Ketoconazole
• Twice daily until clear, additional 1 week
– Oral antifungal
• Griseofulvin
– Change hand towels
– Change shoes
©2018
Case Study #9
• 6 year old patient presents for evaluation of new facial rash. Rash appeared 2‐3 months ago. Initially appeared dry. Family moisturized rash with Vaseline ointment. The rash continued to spread and then became red and pruritic. Family attempted hydrocortisone 2.5% ointment 2 x daily. Rash continued to spread from initially under nose now extending up to surrounding patients eyes and mouth.
• Patient’s medication list: acetaminophen, hydrocortisone 2.5% ointment, Flovent disk, albuterol.
©2018 ©2018
Case Study #9
• 6 year old patient presents for evaluation of new facial rash. Rash appeared 2‐3 months ago. Initially appeared dry. Family moisturized rash with Vaseline ointment. The rash continued to spread and then became red and pruritic. Family attempted hydrocortisone 2.5% ointment 2 x daily. Rash continued to spread from initially under nose now extending up to surrounding patients eyes and mouth.
• Patient’s medication list: acetaminophen, hydrocortisone 2.5% ointment, Flovent disk, albuterol.
11
©2018
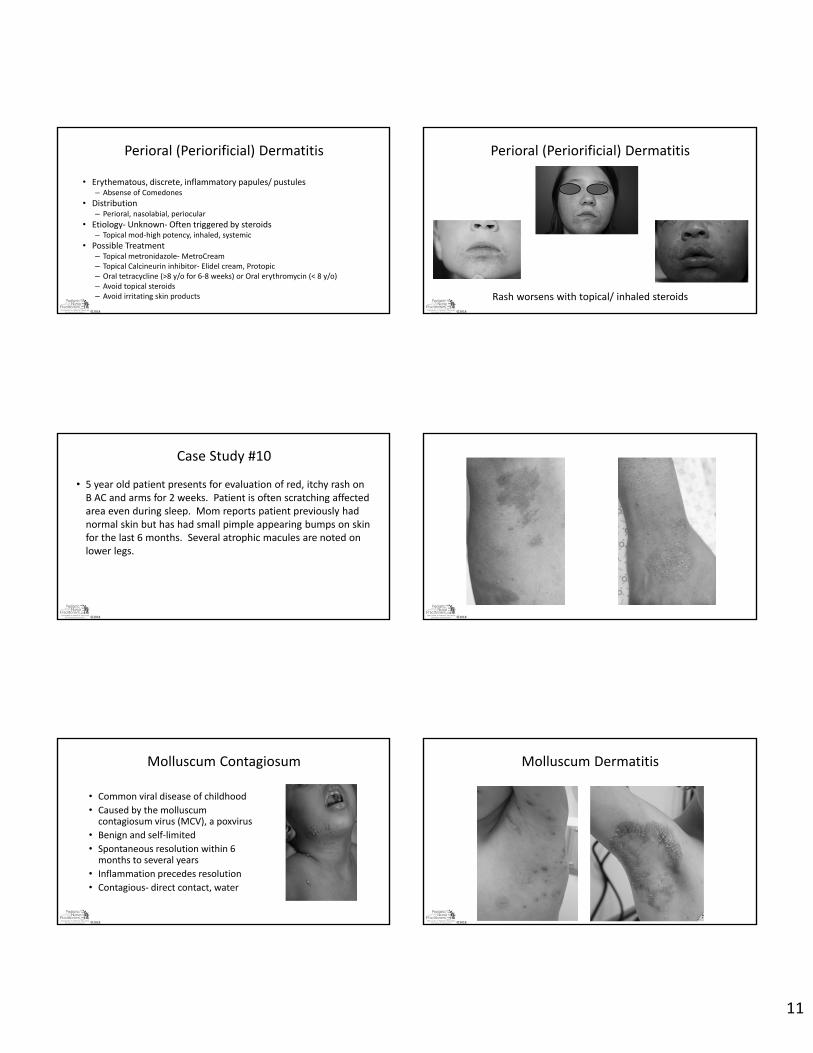
Perioral (Periorificial) Dermatitis
• Erythematous, discrete, inflammatory papules/ pustules– Absense of Comedones
• Distribution– Perioral, nasolabial, periocular
• Etiology‐ Unknown‐ Often triggered by steroids– Topical mod‐high potency, inhaled, systemic
• Possible Treatment– Topical metronidazole‐ MetroCream– Topical Calcineurin inhibitor‐ Elidel cream, Protopic– Oral tetracycline (>8 y/o for 6‐8 weeks) or Oral erythromycin (< 8 y/o)– Avoid topical steroids– Avoid irritating skin products
©2018
Perioral (Periorificial) Dermatitis
Rash worsens with topical/ inhaled steroids
©2018
Case Study #10
• 5 year old patient presents for evaluation of red, itchy rash on B AC and arms for 2 weeks. Patient is often scratching affected area even during sleep. Mom reports patient previously had normal skin but has had small pimple appearing bumps on skin for the last 6 months. Several atrophic macules are noted on lower legs.
©2018
©2018
Molluscum Contagiosum
• Common viral disease of childhood
• Caused by the molluscumcontagiosum virus (MCV), a poxvirus
• Benign and self‐limited
• Spontaneous resolution within 6 months to several years
• Inflammation precedes resolution
• Contagious‐ direct contact, water
©2018
Molluscum Dermatitis

12
©2018
Molluscum Dermatitis
• Reassurance– <1% intact molluscum are bacterially infected
• Vaseline ointment/ Aquaphor– Refrigeration
• Avoid mid‐high potency topical steroids– Can use mild potency topical steroids for pruritis
– Hydrocortisone 1%, 2.5% ointment
• Antihistamines– Benadryl, hydroxyzine
©2018
Case Study #11
• 13 year old patient presents for new skin rash on face, arms, legs and buttocks. Affected areas are very dry and bumpy. Rash seems to remain fixed, does not wax and wane. Affected area is occasionally pruritic but does not disturb sleep. Rash can appear red especially when patient is hot and sweaty.
©2018 ©2018
Keratosis Pilaris
• Asymptomatic‐ no pruritis
• Cosmetically distressing!!!
• Dry, bumpy skin “chicken skin”
• Follicular hyperkeratosis
• Not present at birth. Appears childhood
• Familial inheritance
• Face, extensor arms, lateral legs
– Can be widespread
©2018
Keratosis pilaris
• Treatment–Moisturizers‐ cream, ointment
– Avoid irritants‐ fragrances, dyes
– Keratolytic agents• Ammonium lactate 12% cream
• Salicylic acid
• Glycolic acid
• Urea
– Potential for irritation‐ resulting in erythema (BALANCE)
–Must maintain therapy to achieve remission
©2018
Keratosis Pilaris
13
©2018
Case Study #12
• 16 year old patient presents for evaluation of new rash on B legs. Red rash appeared 3‐4 months ago. Affected area is not pruritic but rash appears to be spreading on both legs. The patient is not involved in sports activities but enjoys playing video games on a laptop for extended periods of time.
©2018
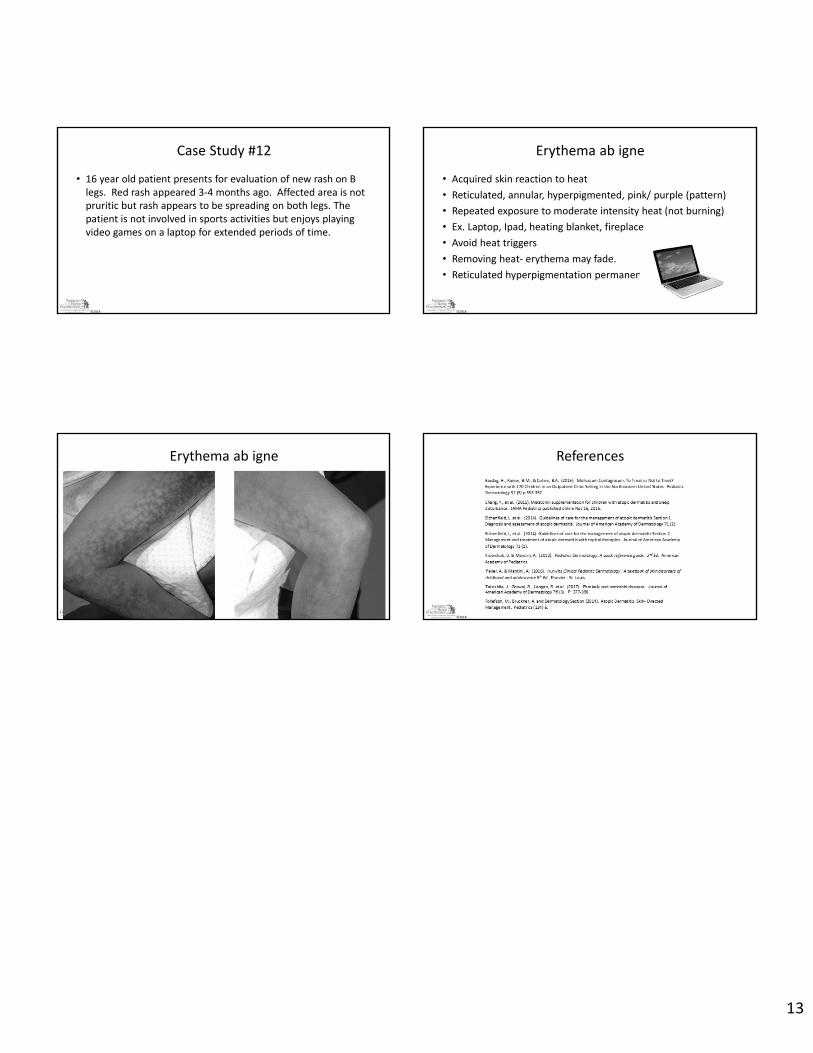
Erythema ab igne
• Acquired skin reaction to heat
• Reticulated, annular, hyperpigmented, pink/ purple (pattern)
• Repeated exposure to moderate intensity heat (not burning)
• Ex. Laptop, Ipad, heating blanket, fireplace
• Avoid heat triggers
• Removing heat‐ erythema may fade.
• Reticulated hyperpigmentation permanent
©2018
Erythema ab igne
©2018
References