position of the academy of nutrition anne- nutrition and
TRANSCRIPT

FROM THE ACADEMYPosition Paper
Position of the Academy of Nutrition andDietetics, Dietitians of Canada, and theAmerican College of Sports Medicine: Nutritionand Athletic Performance
ABSTRACTIt is the position of the Academy of Nutrition and Dietetics (Academy), Dietitians ofCanada (DC), and the American College of Sports Medicine (ACSM) that the performanceof, and recovery from, sporting activities are enhanced by well-chosen nutrition stra-tegies. These organizations provide guidelines for the appropriate type, amount, andtiming of intake of food, fluids, and supplements to promote optimal health and per-formance across different scenarios of training and competitive sport. This positionpaper was prepared for members of the Academy, DC, and ACSM, other professionalassociations, government agencies, industry, and the public. It outlines the Academy’s,DC’s, and ACSM’s stance on nutrition factors that have been determined to influenceathletic performance and emerging trends in the field of sports nutrition. Athletesshould be referred to a registered dietitian nutritionist for a personalized nutrition plan.In the United States and in Canada, the Certified Specialist in Sports Dietetics is aregistered dietitian nutritionist and a credentialed sports nutrition expert.J Acad Nutr Diet. 2016;116:501-528.
POSITION STATEMENTIt is the position of the Academy of Nutritionand Dietetics, Dietitians of Canada, and theAmerican College of Sports Medicine that theperformance of, and recovery from, sportingactivities are enhanced by well-chosen nutri-tion strategies. These organizations provideguidelines for the appropriate type, amount,and timing of intake of food, fluids, and di-etary supplements to promote optimal healthand sport performance across different sce-narios of training and competitive sport.
THIS ARTICLE OUTLINES THEcurrent energy, nutrient, andfluid recommendations foractive adults and competitive
athletes. These general recommenda-tions can be adjusted by sports dietitians*
to accommodate the unique issues ofindividual athletes regarding health,nutrient needs, performance goals,physique characteristics (ie, body size,shape, growth, and composition), prac-tical challenges, and food preferences.
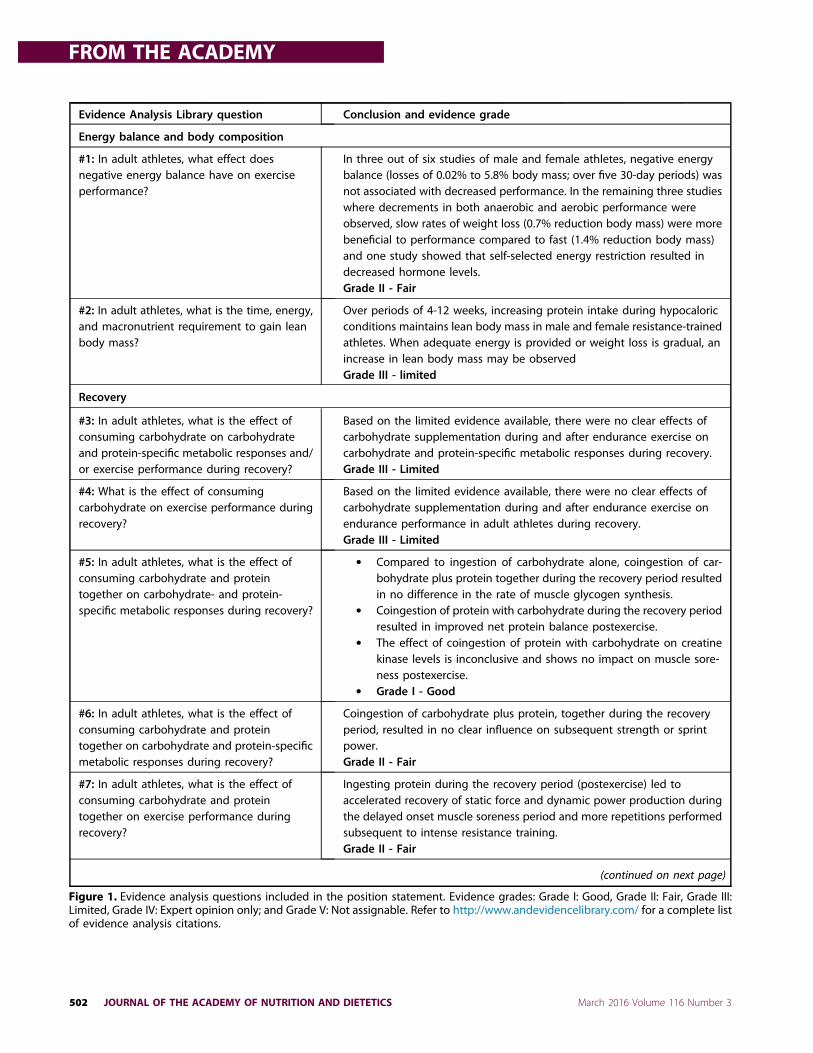
EVIDENCE-BASED ANALYSISThis article was developed using theAcademy of Nutrition and Dietetics(Academy) Evidence Analysis Library(EAL) andwill outline some key themesrelated to nutrition and athletic per-formance. The EAL is a synthesis ofrelevant nutrition research on impor-tant dietetics-related practice ques-tions. The publication range for theevidence-based analysis spannedMarch 2006 to November 2014. For thedetails on the systematic review andmethodology go to www.andevidencelibrary.com. Figure 1 presents the evi-dence analysis questions used in thisposition paper.
NEW PERSPECTIVES IN SPORTSNUTRITIONThe past decade has seen an increase inthe number and topics of publications
This Academy position paper includes theauthors’ independent review of the litera-ture in addition to systematic review con-ducted using the Academy’s EvidenceAnalysis Process and information from theAcademy Evidence Analysis Library (EAL).Topics from the EAL are clearly delineated.The use of an evidence-based approachprovides important added benefits toearlier review methods. The major advan-tage of the approach is the more rigorousstandardization of review criteria, whichminimizes the likelihood of reviewer biasand increases the easewithwhichdisparatearticles may be compared. For a detaileddescription of the methods used in the ev-idence analysis process, access the Aca-demy’s Evidence Analysis Process (http:www.andevidencelibrary.com/eaprocess).
Conclusion Statements are assigned agrade by an expert work group based onthe systematic analysis and evaluation ofthe supporting research evidence. GradeI¼Good; Grade II¼Fair; Grade III¼Limited;Grade IV Expert Opinion Only; and GradeV¼Not Assignable (because there is no ev-idence to support or refute the conclusion).
See grade definitions at www.andevidencelibrary.com/.
Evidence-based information for this andother topics can be found at https://www.andevidencelibrary.com and subscriptionsfor nonmembers are purchasable at https://www.andevidencelibrary.com/store.cfm.
This article is being published concur-rently on the Dietitians of Canadawebsite (www.dietitians.ca/sports) andin Medicine & Science in Sports andExercise!. The articles are identicalexcept for minor stylistic and spellingdifferences in keeping with each jour-nal’s style. Either citation can be usedwhen citing this article.
2212-2672/Copyright ª 2016 by theAcademy of Nutrition and Dietetics,American College of Sports Medicine, andDietitians of Canada.http://dx.doi.org/10.1016/j.jand.2015.12.006
*Because credentialing practices varyinternationally, the term “sports dieti-tian”will be used throughout this articleto encompass all terms of accreditation,including registered dietitian nutritionist(RDN), registered dietitian (RD), profes-sional dietitian (PDt), or Board CertifiedSpecialist in Sports Dietetics (CSSD).
ª 2016 by the Academy of Nutrition and Dietetics, American College ofSports Medicine, and Dietitians of Canada. JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 501
Evidence Analysis Library question Conclusion and evidence grade
Energy balance and body composition
#1: In adult athletes, what effect doesnegative energy balance have on exerciseperformance?
In three out of six studies of male and female athletes, negative energybalance (losses of 0.02% to 5.8% body mass; over five 30-day periods) wasnot associated with decreased performance. In the remaining three studieswhere decrements in both anaerobic and aerobic performance wereobserved, slow rates of weight loss (0.7% reduction body mass) were morebeneficial to performance compared to fast (1.4% reduction body mass)and one study showed that self-selected energy restriction resulted indecreased hormone levels.Grade II - Fair
#2: In adult athletes, what is the time, energy,and macronutrient requirement to gain leanbody mass?
Over periods of 4-12 weeks, increasing protein intake during hypocaloricconditions maintains lean body mass in male and female resistance-trainedathletes. When adequate energy is provided or weight loss is gradual, anincrease in lean body mass may be observedGrade III - limited
Recovery
#3: In adult athletes, what is the effect ofconsuming carbohydrate on carbohydrateand protein-specific metabolic responses and/or exercise performance during recovery?
Based on the limited evidence available, there were no clear effects ofcarbohydrate supplementation during and after endurance exercise oncarbohydrate and protein-specific metabolic responses during recovery.Grade III - Limited
#4: What is the effect of consumingcarbohydrate on exercise performance duringrecovery?
Based on the limited evidence available, there were no clear effects ofcarbohydrate supplementation during and after endurance exercise onendurance performance in adult athletes during recovery.Grade III - Limited
#5: In adult athletes, what is the effect ofconsuming carbohydrate and proteintogether on carbohydrate- and protein-specific metabolic responses during recovery?
" Compared to ingestion of carbohydrate alone, coingestion of car-bohydrate plus protein together during the recovery period resultedin no difference in the rate of muscle glycogen synthesis.
" Coingestion of protein with carbohydrate during the recovery periodresulted in improved net protein balance postexercise.
" The effect of coingestion of protein with carbohydrate on creatinekinase levels is inconclusive and shows no impact on muscle sore-ness postexercise.
" Grade I - Good
#6: In adult athletes, what is the effect ofconsuming carbohydrate and proteintogether on carbohydrate and protein-specificmetabolic responses during recovery?
Coingestion of carbohydrate plus protein, together during the recoveryperiod, resulted in no clear influence on subsequent strength or sprintpower.Grade II - Fair
#7: In adult athletes, what is the effect ofconsuming carbohydrate and proteintogether on exercise performance duringrecovery?
Ingesting protein during the recovery period (postexercise) led toaccelerated recovery of static force and dynamic power production duringthe delayed onset muscle soreness period and more repetitions performedsubsequent to intense resistance training.Grade II - Fair
(continued on next page)
Figure 1. Evidence analysis questions included in the position statement. Evidence grades: Grade I: Good, Grade II: Fair, Grade III:Limited, Grade IV: Expert opinion only; and Grade V: Not assignable. Refer to http://www.andevidencelibrary.com/ for a complete listof evidence analysis citations.
FROM THE ACADEMY
502 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

of original research and review,consensus statements from sportingorganizations, and opportunities forqualification and accreditation relatedto sports nutrition and dietetics. Thisbears witness to sports nutrition as adynamic area of science and practicethat continues to flourish in boththe scope of support it offers to ath-letes and the strength of evidencethat underpins its guidelines. Beforeembarking on a discussion of individ-ual topics, it is valuable to identify arange of themes in contemporarysports nutrition that corroborate andunify the recommendations in thisarticle.
1. Nutrition goals and require-ments are not static. Athletesundertake a periodized pro-gram in which preparation forpeak performance in targetedevents is achieved by inte-grating different types of
workouts in the various cyclesof the training calendar. Nutri-tion support also needs to beperiodized, taking into accountthe needs of daily training ses-sions (which can range fromminor in the case of “easy”workouts to substantial in thecase of high-quality sessions(eg, high-intensity, strenuous,or highly skilled workouts) andoverall nutritional goals.
2. Nutrition plans need to bepersonalized to the individualathlete to take into account thespecificity and uniqueness ofthe event, performance goals,practical challenges, food pref-erences, and responses tovarious strategies.
3. A key goal of training is toadapt the body to developmetabolic efficiency and flexi-bility, whereas competitionnutrition strategies focus on
providing adequate substratestores to meet the fuel de-mands of the event and sup-port cognitive function.
4. Energy availability, which con-siders energy intake in relationto the energy cost of exercise,sets an important foundationfor health and the success ofsports nutrition strategies.
5. The achievement of the bodycomposition associated withoptimal performance is nowrecognized as an important butchallenging goal that needs tobe individualized and perio-dized. Care should be taken topreserve health and long-termperformance by avoiding prac-tices that create unacceptablylow energy availability andpsychological stress.
6. Training and nutrition have astrong interaction in accli-mating the body to develop
Evidence Analysis Library question Conclusion and evidence grade
Energy balance and body composition
#8: In adult athletes, what is the effect ofconsuming protein on carbohydrate- andprotein-specific metabolic responses duringrecovery?
Ingesting protein (approximately 20 to 30 g total protein, or approximately10 g essential amino acids) during exercise or the recovery period(postexercise) led to increased whole body and muscle protein synthesis aswell as improved nitrogen balance.Grade I- Good
Training
#9: In adult athletes, what is the optimal blendof carbohydrates for maximal carbohydrateoxidation during exercise?
Based on the limited evidence available, carbohydrate oxidation wasgreater in carbohydrate conditions (glucose and glucoseþfructose)compared with water placebo, but no differences between the twocarbohydrate blends tested were observed in male cyclists. Exogenouscarbohydrate oxidation was greater in the glucoseþfructose condition vsglucose-only in a single study.Grade III - Limited
#10: In adult athletes, what effect doestraining with limited carbohydrate availabilityhave on metabolic adaptations that lead toperformance improvements?
Training with limited carbohydrate availability may lead to some metabolicadaptations during training, but did not lead to performanceimprovements. Based on the evidence examined, whereas there isinsufficient evidence supporting a clear performance effect, training withlimited carbohydrate availability impaired training intensity and duration.Grade II - Fair
#11: In adult athletes, what effect doesconsuming high or low glycemic meals orfoods have on training-related metabolicresponses and exercise performance?
In the majority of studies examined, neither glycemic index nor glycemicload affected endurance performance nor metabolic responses whenconditions were matched for carbohydrate and energy.Grade I - Good
Figure 1. (continued) Evidence analysis questions included in the position statement. Evidence grades: Grade I: Good, Grade II: Fair,Grade III: Limited, Grade IV: Expert opinion only; and Grade V: Not assignable. Refer to http://www.andevidencelibrary.com/ for acomplete list of evidence analysis citations.
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 503
functional and metabolic ad-aptations. Although optimalperformance is underpinnedby the provision of proactivenutrition support, training ad-aptations may be enhanced inthe absence of such support.
7. Some nutrients (eg, energy,carbohydrate, and protein)should be expressed usingguidelines per kilogram bodymass to allow recommenda-tions to be scaled to the largerange in the body sizes of ath-letes. Sports nutrition guide-lines should also consider theimportance of the timing ofnutrient intake and nutritionalsupport over the day and inrelation to sport rather thangeneral daily targets.
8. Highly trained athletes walk atightrope between traininghard enough to achieve amaximal training stimulus andavoiding the illness and injuryrisk associated with an exces-sive training volume.
9. Competition nutrition shouldtarget specific strategies thatreduce or delay factors thatwould otherwise cause fatiguein an event; these are specificto the event, the environ-ment/scenario in which it isundertaken, and the individ-ual athlete.
10. New performance nutritionoptions have emerged in thelight of developing but robustevidence that brain sensing ofthe presence of carbohydrate,and potentially other nutri-tional components, in the oralcavity can enhance perceptionsof well-being and increase self-chosen work rates. Such find-ings present opportunities forintake during shorter events, inwhich fluid or food intake waspreviously not considered tooffer a metabolic advantage, byenhancing performance via acentral effect.
11. A pragmatic approach to adviceregarding the use of supple-ments and sports foods isneeded in the face of the highprevalence of interest in, anduse by, athletes and the evi-dence that some products canusefully contribute to a sports
nutrition plan and/or directlyenhance performance. Athletesshould be assisted to undertakea cost-to-benefit analysis of theuse of such products and torecognize that they are of thegreatest value when added to awell-chosen eating plan.
THEME 1: NUTRITION FORATHLETE PREPARATIONEnergy Requirements, EnergyBalance, and Energy AvailabilityAn appropriate energy intake is thecornerstone of the athlete’s diet becauseit supports optimal body function, de-termines the capacity for intake ofmacronutrient and micronutrients, andassists in manipulating body composi-tion. An athlete’s energy intake fromfood, fluids, and supplements can bederived from weighed/measured foodrecords (typically 3 to 7 days), a multi-pass 24-hour recall, or from foodfrequency questionnaires.1 There areinherent limitations with all of thesemethods, with a bias to the under-reportingof intakes. Extensive educationregarding the purpose and protocols ofdocumenting intakes may assist withcompliance and enhance the accuracyandvalidityof self-reported information.Meanwhile, an athlete’s energy re-
quirements depend on the periodizedtraining and competition cycle, and willvary from day to day throughout theyearly training plan relative to changesin training volume and intensity. Factorsthat increase energy needs abovenormal baseline levels include exposureto cold or heat, fear, stress, high altitudeexposure, some physical injuries, spe-cific drugs or medications (eg, caffeineand nicotine), increases in fat-free mass(FFM), and possibly the luteal phase ofthe menstrual cycle.2 Aside from re-ductions in training, energy re-quirements are lowered by aging,decreases in FFM, and possibly thefollicular phase of the menstrual cycle.3
Energy balance occurs when totalenergy intake (EI) equals total energyexpenditure (TEE), which in turn con-sists of the summation of basal meta-bolic rate (BMR), the thermic effect offood (TEF), and the thermic effect ofactivity (TEA).TEE[BMRDTEFDTEATEA[Planned Exercise Expendi-
tureDSpontaneous Physical ActivityDNonexercise Activity Thermogenesis
Techniques used to measure or esti-mate components of TEE in sedentaryand moderately active populations canalso be applied to athletes, but there aresome limitations to this approach,particularly in highly competitive ath-letes. Because the measurement of BMRrequires subjects to remainexclusivelyatrest, it is more practical to measurerestingmetabolic rate (RMR),whichmaybe 10% higher. Although population-specific regression equations areencouraged, a reasonable estimate ofBMR can be obtained using either theCunningham4 or the Harris-Benedict5
equations, with an appropriate activityfactor being applied to estimate TEE.Whereas RMR represents 60% to 80% ofTEE for sedentary individuals, it may beas little as 38% to 47% of TEE for eliteendurance athletes whomay have a TEAas high as 50% of TEE.2
TEA includes planned exerciseexpenditure, spontaneous physical ac-tivity (eg, fidgeting), and nonexerciseactivity thermogenesis. Energy expen-diture from exercise can be estimatedin several ways from activity logs(1 to 7 days’ duration) with subjectiveestimates of exercise intensity usingactivity codes and metabolic equiva-lents,6,7 US Dietary Guidelines, 2015,8
and the Dietary Reference Intakes(DRIs).9 The latter two typically un-derestimate the requirements of ath-letes because they fail to cover therange in body size or activity levels ofcompetitive populations. Energy avail-ability (EA) is a concept of recent cur-rency in sports nutrition, whichequates energy intake with re-quirements for optimal health andfunction rather than energy balance.EA, defined as dietary intake minusexercise energy expenditure normal-ized to FFM, is the amount of energyavailable to the body to perform allother functions after the cost of exer-cise is subtracted.10 The concept wasfirst studied in women, where an EA of45 kcal/kg FFM/day was found to beassociated with energy balance andoptimal health; meanwhile, a chronicreduction in EA, (particularly below 30kcal/kg FFM/day) was associated withimpairments of a variety of bodyfunctions.10 Low EA may occur frominsufficient EI, high TEE, or a combi-nation of the two. It may be associatedwith disordered eating, a misguided orexcessively rapid program for loss ofbody mass, or inadvertent failure to
FROM THE ACADEMY
504 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

meet energy requirements during aperiod of high-volume training orcompetition.10
Example Calculation of EA60 kg body weight (BW), 20% body
fat, 80% FFM (¼48.0 kg FFM), EI¼2,400kcal/day, additional energy expendi-ture from exercise¼500 kcal/dayEA¼(EIeEEE)/FFM¼(2,400e500)
kcal$d/48.0 kg¼39.6 kcal/kg FFM/dayThe concept of EA emerged from the
study of the female athlete triad (Triad),which started as a recognition of theinterrelatedness of clinical issues withdisordered eating, menstrual dysfunc-tion, and low bone mineral density infemale athletes and then evolved into abroader understanding of the concernsassociated with any movement alongthe spectra away from optimal energyavailability, menstrual status, and bonehealth.11 Although not embedded in theTriad spectrum, it is recognized thatother physiological consequences mayresult from one of the components ofthe Triad in female athletes, such asendocrine, gastrointestinal, renal,neuropsychiatric, musculoskeletal, andcardiovascular dysfunction.11 Indeed, anextension of the Triad has been pro-posed—the Relative Energy Deficiencyin Sport (RED-S)—as an inclusivedescription of the entire cluster ofphysiologic complications observed inmale and female athletes who consumeenergy intakes that are insufficient inmeeting the needs for optimal bodyfunction once the energy cost of exercisehas been removed.12 Specifically, healthconsequences of RED-S may negativelyaffect menstrual function; bone health;and endocrine, metabolic, hematologi-cal, growth and development, psycho-logical, cardiovascular, gastrointestinal,and immunological systems. Potentialperformance effects of RED-S mayinclude decreased endurance, increasedinjury risk, decreased training response,impaired judgment, decreased coordi-nation, decreased concentration, irrita-bility, depression, decreased glycogenstores, and decreased muscle strength.12
It is now also recognized that impair-ments of health and function occuracross the continuum of reductions inEA, rather than occurring uniformly atan EA threshold, and require furtherresearch.12 It should be appreciated thatlow EA is not synonymous with negativeenergy balance or weight loss; indeed, ifa reduction in EA is associated with areduction in RMR, it may produce a new
steady-state of energy balance or weightstability at a lowered energy intake thatis insufficient to provide for healthybody function.Regardless of the terminology, it is
apparent that low EA in male and fe-male athletes may compromiseathletic performance in the short andlong-term. Screening and treatmentguidelines have been established formanagement of low EA11,12 and shouldinclude assessment with the EatingDisorder Inventory-3 resource13 or theDiagnostic and Statistical Manual ofMental Disorders, fifth edition, whichincludes changes in eating disordercriteria.14 There is evidence that in-terventions to increase EA are suc-cessful in reversing at least someimpaired body functions; for example,in a 6-month trial with female athletesexperiencing menstrual dysfunction,dietary treatment to increase EA tow40 kcal/kg FFM/day resulted inresumption of menses in all subjects ina mean of 2.6 months.6
Body Composition and SportsPerformanceVarious attributes of physique (bodysize, shape, and composition) areconsidered to contribute to success invarious sports. Of these, body mass(“weight”) and body composition areoften focal points for athletes becausethey are most able to be manipulated.Although it is clear that the assessmentand manipulation of body compositionmay assist in the progression of anathletic career, athletes, coaches, andtrainers should be reminded that ath-letic performance cannot be accuratelypredicted solely based on BW andcomposition. A single and rigid optimalbody composition should not be rec-ommended for any event or group ofathletes.15 Nevertheless, there are re-lationships between body compositionand sports performance that areimportant to consider within an ath-lete’s preparation.In sports involving strength and po-
wer, athletes strive to gain FFM via aprogram of muscle hypertrophy atspecified times of the annual macro-cycle. Whereas some athletes aim togain absolute size and strength per se,in other sports, in which the athletemust move their own body mass orcompete within weight divisions, it isimportant to optimize power to weightratios rather than absolute power.16
Thus, some power athletes also desireto achieve low body fat levels. Insports involving weight divisions (eg,combat sports, lightweight rowing, andweightlifting), competitors typicallytarget the lowest achievable BW cate-gory while maximizing their leanmass within this target.
Other athletes strive to maintain alow body mass and/or body fat level forseparate advantages.17 Distance run-ners and cyclists benefit from a lowenergy cost of movement and a favor-able ratio of weight to surface area forheat dissipation. Team athletes can in-crease their speed and agility by beinglean, whereas athletes in acrobaticsports (eg, diving, gymnastics, anddance) gain biomechanical advantagesin being able to move their bodieswithin a smaller space. In some ofthese sports and others (eg, bodybuilding), there is an element of aes-thetics in determining performanceoutcomes. Although there are demon-strated advantages to achieving acertain body composition, athletes mayfeel pressure to strive to achieve unre-alistically low targets of weight/bodyfat or to reach them in an unrealistictime frame.15 Such athletes may besusceptible to practicing extremeweight control behaviors or continuousdieting, exposing themselves tochronic periods of low EA and poornutrient support in an effort to repeatprevious success at a lower weight orleaner body composition.15,18 Extrememethods of weight control can bedetrimental to health and perfor-mance, and disordered eating patternshave also been observed in these sportscenarios.15,18
Nevertheless, there are scenarios inwhich an athlete will enhance his orher health and performance byreducing BW or body fat as part of aperiodized strategy. Ideally, this occurswithin a program that gradually ach-ieves an individualized optimal bodycomposition over the athlete’s athleticcareer, and allows weight and body fatto track within a suitable range withinthe annual training cycle.18 The pro-gram should also include avoiding sit-uations in which athletes inadvertentlygain excessive amounts of body fat as aresult of a sudden energy mismatchwhen energy expenditure is abruptlyreduced (eg, the off-season or injury).In addition, athletes are warned againstthe sudden or excessive gain in body
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 505

fat that is part of the culture of somesports where a high body mass isdeemed useful for performance.Although body mass index is notappropriate as a body compositionsurrogate in athletes, a chronic interestin gaining weight may put some ath-letes at risk for an obese body massindex, which may increase the risk ofmeeting the criteria for metabolicsyndrome.19 Sports dietitians should beaware of sports that promote theattainment of a large body mass andscreen for metabolic risk factors.19
Methodologies for Body Composi-tion Assessment. Techniques used toassess athlete body compositioninclude dual energy x-ray absorptiom-etry (DXA), hydrodensitometry, airdisplacement plethysmography, skin-fold measurements, and single andmultifrequency bioelectrical imped-ance analysis. Although DXA is quickand noninvasive, issues around cost,accessibility, and exposure to a smallradiation dose limit its utility, par-ticularly for certain populations.20
When undertaken according to stan-dardized protocols, DXA has the loweststandard error of estimate, whereasskinfold measures have the highest; airdisplacement plethysmography (Bod-Pod, Life Measurement, Inc) providesan alternative method that is quick andreliable, but may underestimate bodyfat by 2% to 3%.20 Skinfold measure-ment and other anthropometric dataserve as an excellent surrogate mea-sure of adiposity and muscularity whenprofiling composition changes inresponse to training interventions.20
However, it should be noted that thestandardization of skinfold sites, mea-surement techniques, and calipers varyaround the world. Despite some limi-tations, this technique remains a pop-ular method of choice due toconvenience and cost, with informa-tion being provided in absolute mea-sures and compared with sequentialdata from the individual athlete or, in ageneral way, with normative datacollected in the same way from athletepopulations.20,21
All body composition assessmenttechniques should be scrutinized toensure accuracy and reliability. Testingshould be conducted with the samecalibrated equipment, with a stan-dardized protocol, and by technicians
with known testeretest reliability.Where population-specific predictionequations are used, they should becross-validated and reliable. Athletesshould be educated on the limitationsassociated with body compositionassessment and should strictly followpreassessment protocols. These in-structions, which include maintaininga consistent training volume, fastingstatus, and hydration from test totest20 should be enforced to avoidcompromising the accuracy and reli-ability of body composition measures.Body composition should be deter-
mined within a sports program ac-cording to a schedule that isappropriate to the performance of theevent, the practicality of undertakingassessments, and the sensitivity of theathlete. There are technical errorsassociated with all body compositiontechniques that limit the usefulness ofmeasurement for athlete selection andperformance prediction. In lieu ofsetting absolute body compositiongoals or applying absolute criteria tocategorize groups of athletes, it ispreferred that normative data are pro-vided in terms of ranges.21 Becausebody fat content for an individualathlete will vary over the season andover the athlete’s career, goals for bodycomposition should be set in terms ofranges that can be appropriatelytracked at critical times. When con-ducting such monitoring programs, it isimportant that the communication ofresults with coaches, training staff, andathletes is undertaken with sensitivity,that limitations in measurement tech-nique are recognized, and that care istaken to avoid promoting an unhealthyobsession with body composition.17,18
Sports dietitians have important op-portunities to work with these athletesto help promote a healthy bodycomposition, and to minimize theirreliance on rapid-weight loss tech-niques and other hazardous practicesthat may result in performance decre-ments, loss of FFM, and chronic healthrisks. Many themes should beaddressed and include the creation of aculture and environment that valuessafe and long-term approaches tomanagement of body composition;modification of rules or practicesaround selection and qualification forweight classes;16,19,22 and programsthat identify disordered eating
practices at an early stage for inter-vention, and where necessary, removalfrom play.18
Principles of Altering Body Com-position and Weight. Athletes oftenneed assistance in setting appropriateshort-term and long-term goals, un-derstanding nutrition practices thatcan safely and effectively increasemuscle mass or reduce body fat/weight, and integrating these strategiesinto an eating plan that achieves otherperformance nutrition goals. Frequentfollow up with these athletes may havelong-term benefits, including shep-herding the athlete through short-termgoals and reducing reliance on extremetechniques and fad diets/behaviors.
There is ample evidence in weightsensitive and weight-making sportsthat athletes frequently undertakerapid weight loss strategies to gain acompetitive advantage.20,23,24 Howev-er, the resultant hypohydration (bodywater deficit), loss of glycogen storesand lean mass, and other outcomes ofpathologic behaviors (eg, purging,excessive training, or starving) canimpair health and performance.18
Nevertheless, responsible use of short-term, rapid weight-loss techniques,when indicated, is preferred overextreme and extended energy restric-tion and suboptimal nutrition sup-port.17 When actual loss of BW isrequired, it should be programmed tooccur in the base phase of training orwell out from competition to minimizeloss of performance,25 and should beachieved with techniques that maxi-mize loss of body fat while preservingmuscle mass and other health goals.Such strategies include achieving aslight energy deficit to achieve a slowrather than rapid rate of loss andincreasing dietary protein intake. Inthis regard, the provision of a higherprotein intake (2.3 vs 1 g/kg/day) in ashorter-term (2 week), energy-restricted diet in athletes was foundto retain muscle mass while losingweight and body fat.26 Furthermore,FFM and performance may be betterpreserved in athletes who minimizeweekly weight loss to <1% per week.25
An individualized diet and trainingprescription for weight/fat loss shouldbe based on assessment of goals, pre-sent training and nutrition practices,past experiences, and trial and error.
FROM THE ACADEMY
506 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

Nevertheless, for most athletes, thepractical approach of decreasing en-ergy intake by w250 to 500 kcal/dayfrom their periodized energy needs,while either maintaining or slightlyincreasing energy expenditure, canachieve progress toward short-termbody composition goals over approxi-mately 3 to 6 weeks. In some situa-tions, additional moderate aerobictraining and close monitoring can beuseful.27 These strategies can beimplemented to help augment thediet-induced energy deficits withoutnegatively impacting recovery fromsport-specific training. Arranging thetiming and content of meals to sup-port training nutrition goals and re-covery may reduce fatigue duringfrequent training sessions and mayhelp optimize body composition overtime.18 Overall barriers to bodycomposition management includelimited access to healthy food options,limited skills or opportunity for foodpreparation, lack of daily routine, andexposure to catering featuring unlim-ited portion sizes and energy-densefoods. Such factors, particularly foundin association with the travel andcommunal living experiences in theathlete lifestyle, can promote poordietary quality that thwarts progressand may lead to the pursuit of quickfixes, acute dieting, and extremeweight loss practices.EAL Question #1 (Figure 1) exam-
ined the effect of negative energy bal-ance on sport performance, findingonly fair support for an impairment ofphysical capacity due to a hypo-energetic diet in the currently exam-ined scenarios. However, few studieshave investigated the overlay of factorscommonly seen in practice, includingthe interaction of poor dietary quality,low carbohydrate availability, exces-sive training, and acute dehydration onchronic energy restriction. The chal-lenge of detecting small but importantchanges in sports performance isnoted in all areas of sports nutrition.28
EAL Question #2 summarizes theliterature on optimal timing, energy,and macronutrient characteristics of aprogram supporting a gain in FFMwhen in energy deficit (Figure 1).Again the literature is limited inquantity and range to allow definitiverecommendations to be made,although there is support for the ben-efits of increased protein intake.
Nutrient Requirements for SportEnergy Pathways and TrainingAdaptations. Guidelines for thetiming and amount of intake of mac-ronutrients in an athlete’s diet shouldbe underpinned by a fundamental un-derstanding of how training-nutrientinteractions affect energy systems,substrate availability, and training ad-aptations. Exercise is fueled by an in-tegrated series of energy systems thatinclude nonoxidative (phosphagen andglycolytic) and aerobic (fat and carbo-hydrate oxidation) pathways, usingsubstrates that are both endogenousand exogenous in origin. ATP andphosphocreatine (phosphagen system)provide a rapidly available energysource for muscular contraction, butnot at sufficient levels to provide acontinuous supply of energy for longerthan w10 seconds. The anaerobicglycolytic pathway rapidly metabolizesglucose and muscle glycogen throughthe glycolytic cascade and is the pri-mary pathway supporting high-intensity exercise lasting 10 to 180seconds. Because neither the phospha-gen nor the glycolytic pathway cansustain energy demands to allow mus-cles to contract at a very high rate forlonger lasting events, oxidative path-ways provide the primary fuels forevents lasting longer than w2 minutes.The major substrates include muscleand liver glycogen, intramuscular lipid,adipose tissue triglycerides, andamino acids from muscle, blood, liver,and the gut. As oxygen becomes moreavailable to the working muscle, thebody uses more of the aerobic (oxida-tive) pathways and less of the anaer-obic (phosphagen and glycolytic)pathways. The greater dependenceupon aerobic pathways does notoccur abruptly, nor is one pathway everrelied on exclusively. The intensity,duration, frequency, type of training,sex, and training level of the individual,as well as prior nutrient intake andsubstrate availability, determine therelative contribution of energy path-ways and when crossover betweenpathways occurs. For a more completeunderstanding of fuel systems forexercise, the reader is directed to spe-cific texts.29
An athlete’s skeletal muscle has aremarkable plasticity to respondquickly to mechanical loading andnutrient availability resulting in
condition-specific metabolic and func-tional adaptations.30 These adaptationsinfluence performance nutrition rec-ommendations with the overarchinggoals that energy systems should betrained to provide the most economicalsupport for the fuel demands of anevent while other strategies shouldachieve appropriate substrate avail-ability during the event itself. Adapta-tions that enhance metabolic flexibilityinclude increases in transport mole-cules that carry nutrients acrossmembranes or to the site of their usewithin the muscle cell, increases inenzymes that activate or regulatemetabolic pathways, enhancement ofthe ability to tolerate the side-productsof metabolism, and an increase in thesize of muscle fuel stores.3 Althoughsome muscle substrates (eg, body fat)are present in relatively large quanti-ties, others may need to be manipu-lated according to specific needs (eg,carbohydrate supplementation toreplace muscle glycogen stores).
Carbohydrate. Carbohydrate hasrightfully received a great deal ofattention in sports nutrition due to anumber of special features of its rolein the performance of, and adaptationto training. First, the size of body car-bohydrate stores is relatively limitedand can be acutely manipulated on adaily basis by dietary intake or even asingle session of exercise.3 Second,carbohydrate provides a key fuel forthe brain and central nervous systemand a versatile substrate for muscularwork where it can support exerciseover a large range of intensities due toits use by both anaerobic and oxida-tive pathways. Even when working atthe highest intensities that can besupported by oxidative phosphoryla-tion, carbohydrate offers advantagesover fat as a substrate because it pro-vides a greater yield of ATP per vol-ume of oxygen that can be deliveredto the mitochondria,3 thus improvinggross exercise efficiency.31 Third, thereis significant evidence that the per-formance of prolonged sustained orintermittent high-intensity exercise isenhanced by strategies that maintainhigh carbohydrate availability (ie,match glycogen stores and bloodglucose to the fuel demands of exer-cise), whereas depletion of thesestores is associated with fatigue in theform of reduced work rates, impaired
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 507
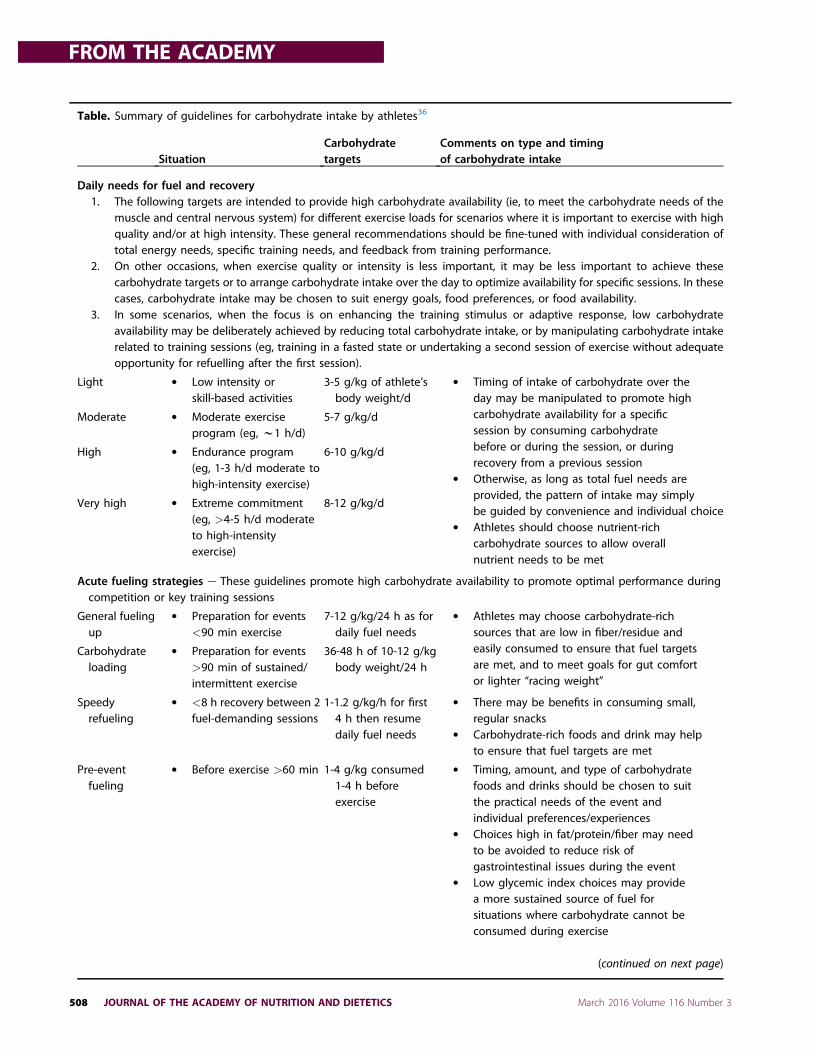
Table. Summary of guidelines for carbohydrate intake by athletes36
SituationCarbohydratetargets
Comments on type and timingof carbohydrate intake
Daily needs for fuel and recovery1. The following targets are intended to provide high carbohydrate availability (ie, to meet the carbohydrate needs of the
muscle and central nervous system) for different exercise loads for scenarios where it is important to exercise with highquality and/or at high intensity. These general recommendations should be fine-tuned with individual consideration oftotal energy needs, specific training needs, and feedback from training performance.
2. On other occasions, when exercise quality or intensity is less important, it may be less important to achieve thesecarbohydrate targets or to arrange carbohydrate intake over the day to optimize availability for specific sessions. In thesecases, carbohydrate intake may be chosen to suit energy goals, food preferences, or food availability.
3. In some scenarios, when the focus is on enhancing the training stimulus or adaptive response, low carbohydrateavailability may be deliberately achieved by reducing total carbohydrate intake, or by manipulating carbohydrate intakerelated to training sessions (eg, training in a fasted state or undertaking a second session of exercise without adequateopportunity for refuelling after the first session).
Light " Low intensity orskill-based activities
3-5 g/kg of athlete’sbody weight/d
" Timing of intake of carbohydrate over theday may be manipulated to promote highcarbohydrate availability for a specificsession by consuming carbohydratebefore or during the session, or duringrecovery from a previous session
" Otherwise, as long as total fuel needs areprovided, the pattern of intake may simplybe guided by convenience and individual choice
" Athletes should choose nutrient-richcarbohydrate sources to allow overallnutrient needs to be met
Moderate " Moderate exerciseprogram (eg, w1 h/d)
5-7 g/kg/d
High " Endurance program(eg, 1-3 h/d moderate tohigh-intensity exercise)
6-10 g/kg/d
Very high " Extreme commitment(eg, >4-5 h/d moderateto high-intensityexercise)
8-12 g/kg/d
Acute fueling strategies e These guidelines promote high carbohydrate availability to promote optimal performance duringcompetition or key training sessions
General fuelingup
" Preparation for events<90 min exercise
7-12 g/kg/24 h as fordaily fuel needs
" Athletes may choose carbohydrate-richsources that are low in fiber/residue andeasily consumed to ensure that fuel targetsare met, and to meet goals for gut comfortor lighter “racing weight”
Carbohydrateloading
" Preparation for events>90 min of sustained/intermittent exercise
36-48 h of 10-12 g/kgbody weight/24 h
Speedyrefueling
" <8 h recovery between 2fuel-demanding sessions
1-1.2 g/kg/h for first4 h then resumedaily fuel needs
" There may be benefits in consuming small,regular snacks
" Carbohydrate-rich foods and drink may helpto ensure that fuel targets are met
Pre-eventfueling
" Before exercise >60 min 1-4 g/kg consumed1-4 h beforeexercise
" Timing, amount, and type of carbohydratefoods and drinks should be chosen to suitthe practical needs of the event andindividual preferences/experiences
" Choices high in fat/protein/fiber may needto be avoided to reduce risk ofgastrointestinal issues during the event
" Low glycemic index choices may providea more sustained source of fuel forsituations where carbohydrate cannot beconsumed during exercise
(continued on next page)
FROM THE ACADEMY
508 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

skill and concentration, and increasedperception of effort. These findingsunderpin the various performancenutrition strategies, to be discussedsubsequently, that supply carbohy-drate before, during, and in the re-covery between events to enhancecarbohydrate availability.Finally, recent work has identified
that in addition to its role as a musclesubstrate, glycogen plays importantdirect and indirect roles in regulatingthe muscle’s adaptation to training.32
The amount and localization ofglycogen within muscle cells alters thephysical, metabolic, and hormonalenvironment in which the signaling re-sponses to exercise are exerted. Specif-ically, starting a bout of endurance
exercise with low muscle glycogencontent (eg, by undertaking a secondtraining session in the hours after theprior session has depleted glycogenstores) produces a coordinated upregu-lation of the transcriptional and post-translational responses to exercise. Anumber of mechanisms underpin thisoutcome, including increasing the ac-tivity of molecules that have a glycogenbinding domain, increasing free fattyacid availability, changing osmoticpressure in the muscle cell, andincreasing catecholamine concentra-tions.32 Strategies that restrict exoge-nous carbohydrate availability (eg,exercising in a fasted state or withoutcarbohydrate intake during the session)also promote an extended signaling
response, albeit less robustly than is thecase for exercise with low endogenouscarbohydrate stores.33 These strategiesenhance the cellular outcomes ofendurance training such as increasedmaximal mitochondrial enzyme activ-ities and/or mitochondrial content andincreased rates of lipid oxidation, withthe augmentation of responses likely tobe explained by enhanced activation ofkey cell signaling kinases (eg, AMPK andp38MAPK), transcription factors (eg,p53 and PPARd) and transcriptionalcoactivators (eg, PGC-1a).33 Deliberateintegration of such training-dietarystrategies (“train low”) within the per-iodized training program is becoming arecognized,34 although potentially mis-used,33 part of sports nutrition practice.
Table. Summary of guidelines for carbohydrate intake by athletes36 (continued)
SituationCarbohydratetargets
Comments on type and timingof carbohydrate intake
During briefexercise
" <45 min Not needed
Duringsustainedhighintensityexercise
" 45-75 min Small amounts,includingmouth rinse
" A range of drinks and sports products canprovide easily consumed carbohydrate
" The frequent contact of carbohydrate withthe mouth and oral cavity can stimulate partsof the brain and central nervous system toenhance perceptions of well-being andincrease self-chosen work outputs
Duringenduranceexercise,including“stop andstart” sports
" 1-2.5 h 30-60 g/h " Carbohydrate intake provides a source offuel for the muscles to supplementendogenous stores
" Opportunities to consume foods and drinksvary according to the rules and natureof each sport
" A range of everyday dietary choices andspecialized sports products ranging in formfrom liquid to solid may be useful
" The athlete should practice to find arefuelling plan that suits his or herindividual goals, including hydration needsand gut comfort
During ultra-enduranceexercise
" >2.5-3 h Up to 90 g/h " As above" Higher intakes of carbohydrate are
associated with better performance" Products providing multiple transportable
carbohydrates (Glucose:fructose mixtures)achieve high rates of oxidation ofcarbohydrate consumed during exercise
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 509

Individualized recommendations fordaily intakes of carbohydrate should bemade in consideration of the athlete’straining/competition program and therelative importance of undertaking itwith high or low carbohydrate accord-ing to the priority of promoting theperformance of high quality exercise vsenhancing the training stimulus oradaptation, respectively. Unfortunately,we lack sophisticated information onthe specific substrate requirements ofmany of the training sessions under-taken by athletes; therefore, we mustrely on guesswork, supported by in-formation on work requirements ofexercise from technologies such asconsumer-based activity and heart ratemonitors,35 power meters, and globalpositioning systems.General guidelines for the suggested
intake of carbohydrate to provide highcarbohydrate availability for desig-nated training or competition sessionscan be provided according to the ath-lete’s body size (a proxy for the size ofmuscle stores) and the characteristicsof the session (see the Table). Thetiming of carbohydrate intake over theday and in relation to training can alsobe manipulated to promote or reducecarbohydrate availability.36 Strategiesto enhance carbohydrate availabilityare covered in more detail in relation tocompetition eating strategies. Never-theless, these fueling practices are alsoimportant for supporting the high-quality workouts within the perio-dized training program. Furthermore, itis intuitive that they add value in fine-tuning intended event eating strate-gies, and for promoting adaptationssuch as gastrointestinal tolerance andenhanced intestinal absorption37 thatallow competition strategies to be fullyeffective. During other sessions of thetraining program, it may be lessimportant to achieve high carbohy-drate availability, or there may be somevalue in deliberately exercising withlow carbohydrate availability toenhance the training stimulus oradaptive response. Various tactics canbe used to permit or promote low car-bohydrate availability, includingreducing total carbohydrate intake ormanipulating the timing of training inrelation to carbohydrate intake (eg,training in a fasted state, undertakingtwo bouts of exercise in close prox-imity without opportunity for refuelingbetween sessions).38
Specific questions examined via theevidence analysis on carbohydrateneeds for training are summarized inthe Table and show good evidence thatneither the glycemic load nor glycemicindex of carbohydrate-rich meals affectsthe metabolic nor performance out-comes of training once carbohydrateand energy content of the diet havebeen taken into account (Question #11).Furthermore, although there is soundtheory behind the metabolic advantagesof exercising with low carbohydrateavailability on training adaptations, thebenefits to performance outcomes arecurrently unclear (Figure 1, Question#10). This possibly relates to the limi-tations of the few available studies inwhich poor periodization of this tacticwithin the training program has meantthat any advantages to training adapta-tions have been counteracted by thereduction in training intensity andquality associated with low carbohy-drate variability. Therefore, a more so-phisticated approach is needed tointegrate this training/nutrient interac-tion into the larger training program.33
Finally, although there is support forconsuming multiple forms of carbohy-drate which facilitate more rapidabsorption, evidence to support thechoice of special blends of carbohydrateto support increased carbohydrateoxidation during training sessions ispremature (Question #9).
Protein. Dietary protein interactswith exercise, providing both a triggerand a substrate for the synthesis ofcontractile and metabolic proteins39,40
as well as enhancing structuralchanges in nonmuscle tissues such astendons41 and bones.42 Adaptationsare thought to occur by stimulation ofthe activity of the protein syntheticmachinery in response to a rise inleucine concentrations and the provi-sion of an exogenous source of aminoacids for incorporation into new pro-teins.43 Studies of the response toresistance training show upregulationof muscle protein synthesis (MPS)for at least 24 hours in response toa single session of exercise, withincreased sensitivity to the intakeof dietary protein over this period.44
This contributes to improvementsin skeletal muscle protein accretionobserved in prospective studies thatincorporate multiple protein feedingsafter exercise and throughout the
day. Similar responses occur followingaerobic exercise or other exercisetypes (eg, intermittent sprint activitiesand concurrent exercise), albeit withpotential differences in the type ofproteins that are synthesized. Recentrecommendations have underscoredthe importance of well-timed proteinintake for all athletes even if musclehypertrophy is not the primarytraining goal, and there is now goodrationale for recommending dailyprotein intakes that are well above theRecommended Dietary Allowance(RDA)39 to maximize metabolic adap-tation to training.40
Although classical nitrogen balancework has been useful for determiningprotein requirements to prevent defi-ciency in sedentary humans in energybalance,45 athletes do not meet thisprofile and achievingnitrogenbalance issecondary to an athlete with the pri-mary goal of adaptation to training andperformance improvement.40 Themodern view for establishing recom-mendations for protein intake in ath-letes extends beyond theDRIs. Focus hasclearly shifted to evaluating the benefitsof providing enough protein at optimaltimes to support tissues with rapidturnover and augment metabolic adap-tations initiated by training stimulus.Future research will further refine rec-ommendations directed at total dailyamounts, timing strategies, quality ofprotein intake, and provide new rec-ommendations for protein supplementsderived from various protein sources.
Protein needs. Current data suggestthat dietary protein intake necessary tosupport metabolic adaptation, repair,remodeling, and for protein turnovergenerally ranges from 1.2 to 2.0 g/kg/day. Higher intakes may be indicated forshort periods during intensified trainingor when reducing energy intake.26,39
Daily protein intake goals should bemet with a meal plan providing a reg-ular spread of moderate amounts ofhigh-quality protein across the day andfollowing strenuous training sessions.These recommendations encompassmost training regimens and allow forflexible adjustments with periodizedtraining and experience.46,47 Althoughgeneral daily ranges are provided, in-dividuals should no longer be solelycategorized as strength or endur-ance athletes and provided with staticdaily protein intake targets. Rather,
FROM THE ACADEMY
510 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

guidelines should be based aroundoptimal adaptation to specific sessionsof training/competition within a perio-dized program, underpinned by anappreciation of the larger context ofathletic goals, nutrient needs, energyconsiderations, and food choices. Re-quirements can fluctuate based on“trained” status (eg, experienced ath-letes requiring less), training (eg, ses-sions involving higher frequency andintensity, or a new training stimulus athigher end of protein range), carbohy-drate availability, and most importantly,energy availability.46,48 The consump-tion of adequate energy, particularlyfrom carbohydrates, to match energyexpenditure, is important so that aminoacids are spared for protein synthesisand not oxidized.49 In cases of energyrestriction or sudden inactivity as oc-curs as a result of injury, elevated pro-tein intakes as high as 2.0 g/kg/dayor higher26,50 when spread over theday may be advantageous in prevent-ing FFM loss.39 More detailed reviewsof factors that influence changing pro-tein needs and their relationship tochanges in protein metabolism andbody composition goals can be foundelsewhere.51,52
Protein timing as a trigger formetabolic adaptation. Laboratory-based studies show that MPS is opti-mized in response to exercise by theconsumption of high biological valueprotein, providing w10 g essentialamino acids in the early recoveryphase (0 to 2 hours after exercise).40,53
This translates to a recommendedprotein intake of 0.25 to 0.3 g/kg BWor 15 to 25 g protein across the typicalrange of athlete body sizes, althoughthe guidelines may need to be fine-tuned for athletes at extreme ends ofthe weight spectrum.54 Higher doses(ie, >40 g dietary protein) have notyet been shown to further augmentMPS and may only be prudent for thelargest athletes, or during weightloss.54 The exercise-enhancement ofMPS, determined by the timing andpattern of protein intake, responds tofurther intake of protein within the24-hour period after exercise,55 andmay ultimately translate into chronicmuscle protein accretion and func-tional change. Whereas proteintiming affects MPS rates, the magni-tude of mass and strength changes
over time are less clear.56 However,longitudinal training studies currentlysuggest that increases in strengthand muscle mass are greatest withimmediate postexercise provision ofprotein.57
Whereas traditional protein intakeguidelines focused on total proteinintake over the day (grams per kilo-gram), newer recommendations nowhighlight that the muscle adaptation totraining can be maximized by ingestingthese targets as 0.3 g/kg BW after keyexercise sessions and every 3 to 5hours over multiple meals.47,54,58
Question #8 (Figure 1) summarizesthe weight of the current literatureof consuming protein on protein-specific metabolic responses duringrecovery.
Optimal protein sources. High-qual-ity dietary proteins are effective for themaintenance, repair, and synthesis ofskeletal muscle proteins.59 Chronictraining studies have shown that theconsumption of milk-based protein af-ter resistance exercise is effective inincreasing muscle strength and favor-able changes in body composi-tion.57,60,61 In addition, there arereports of increased MPS and proteinaccretion with whole milk, lean meat,and dietary supplements, some ofwhich provide the isolated proteinswhey, casein, soy, and egg. To date,dairy proteins seem to be superior toother tested proteins, largely due toleucine content and the digestion andabsorptive kinetics of branched-chainamino acids in fluid-based dairyfoods.62 However, further studies arewarranted to assess other intact high-quality protein sources (eg, egg, beef,pork, and concentrated vegetable pro-tein) and mixed meals on the stimula-tion of mammalian target of rapamycin(mTOR) and MPS following variousmodes of exercise. When whole-foodprotein sources are not convenient oravailable, then portable, third-partytested dietary supplements with high-quality ingredients may serve as apractical alternative to help athletesmeet their protein needs. It is impor-tant to conduct a thorough assessmentof the athlete’s specific nutrition goalswhen considering protein supple-ments. Recommendations regardingprotein supplements should be con-servative and primarily directed atoptimizing recovery and adaptation to
training while continuing to focus onstrategies to improve or maintainoverall diet quality.
Fat. Fat is a necessary component of ahealthy diet, providing energy, essen-tial elements of cell membranes, andfacilitation of the absorption of fat-soluble vitamins. The Dietary Guide-lines for Americans8 and Eating Wellwith Canada’s Food Guide63 have maderecommendations that the proportionof energy from saturated fats be limitedto less than 10% and include sources ofessential fatty acids to meet adequateintake recommendations. Intake of fatby athletes should be in accordancewith public health guidelines andshould be individualized based ontraining level and body compositiongoals.46
Fat, in the form of plasma free fattyacids, intramuscular triglycerides, andadipose tissue provides a fuel sub-strate that is both relatively plentifuland increased in availability to themuscle as a result of endurancetraining. However, exercise-inducedadaptations do not appear to maxi-mize oxidation rates because they canbe further enhanced by dietary stra-tegies such as fasting; acute pre-exercise intake of fat; and chronicexposure to high-fat, low-carbohy-drate diets.3 Although there has beenhistorical64 and recently revived65
interest in chronic adaptation tohigh-fat, low-carbohydrate diets, thepresent evidence suggests thatenhanced rates of fat oxidation canonly match exercise capacity/perfor-mance achieved by diets or strategiespromoting high carbohydrate availabil-ity at moderate intensities,64 whereasthe performance of exercise at thehigher intensities is impaired.64,66 Thisappears to occur as a result of adown-regulation of carbohydratemetabolism even when glycogen isavailable.67 Further research is war-ranted both in view of the current dis-cussions65 and the failure of currentstudies to include an adequate con-trol diet that includes contemporaryperiodized dietary approaches.68
Although specific scenarios may existwhere high-fat diets may offer somebenefits or at least the absence ofdisadvantages for performance, in gen-eral they appear to reduce rather thanenhance metabolic flexibility byreducing carbohydrate availability and
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 511

capacity to use carbohydrate effectivelyas an exercise substrate. Therefore,competitive athletes would be unwiseto sacrifice their ability to undertakehigh-quality training or high-intensityefforts during competition that coulddetermine the outcome.68
Conversely, athletes may choose toexcessively restrict their fat intake inan effort to lose BW or improve bodycomposition. Athletes should bediscouraged from chronic imple-mentation of fat intakes below 20% ofenergy intake since the reduction indietary variety often associated withsuch restrictions is likely to reduce theintake of a variety of nutrients such asfat-soluble vitamins and essential fattyacids,9 especially n-3 fatty acids. If suchfocused restrictiveness around fatintake is practiced, it should be limitedto acute scenarios such as the pre-event diet or carbohydrate-loadingwhere considerations of preferredmacronutrients or gastrointestinalcomfort have priority.
Alcohol. Alcohol consumption may bepart of a well-chosen diet and socialinteractions, but excessive alcoholconsistent with binge drinking patternsis a concerning behavior observedamong some athletes, particularly inteam sports.69 Misuse of alcohol caninterfere with athletic goals in a varietyof ways related to the negative effectsof acute intake of alcohol on the per-formance of, or recovery from, exercise,or the chronic effects of binge drinkingon health and management of bodycomposition.70 Besides the calorie loadof alcohol (7 kcal/g), alcohol suppresseslipid oxidation, increases unplannedfood consumption, and may compro-mise the achievement of body compo-sition goals. Research in this area isfraught with study design concernsthat limit direct translation to athletes.Available evidence warns against
intake of significant amounts of alcoholduring the pre-exercise period andduring training due to the direct nega-tive effects of alcohol on exercisemetabolism, thermoregulation, andskills/concentration.69 The effects ofalcohol on strength and performancemay persist for several hours evenafter signs and symptoms of into-xication or hangover are no longerpresent. In the postexercise phase,where cultural patterns in sport oftenpromote alcohol use, alcohol may
interfere with recovery by impairingglycogen storage,71 slowing rates ofrehydration via its suppressive effect onantidiuretic hormone,72 and impairingthe MPS desired for adaptation andrepair.69,73,74 In cold environments,alcohol consumption increases periph-eral vasodilation resulting in core tem-perature dysregulation75 and there arelikely to be other effects on body func-tion such as disturbances in acid-basebalance and cytokine-prostaglandinpathways, and compromised glucosemetabolism and cardiovascular func-tion.76 Binge drinking may indirectlyaffect recovery goals due to inattentiontoguidelines for recovery. Bingedrinkingis also associated with high-risk behav-iors leading to accidents and antisocialbehaviors that can be detrimental tothe athlete. In conclusion, athletes areadvised to consider both public healthguidelines and team rules regardinguse of alcohol and are encouraged tominimize or avoid alcohol consumptionduring the postexercise period whenissues of recovery and injury repair area priority.
Micronutrients. Exercise stressesmany of the metabolic pathways inwhich micronutrients are required, andtraining may result in muscle bio-chemical adaptations that increase theneed for some micronutrients. Athleteswho frequently restrict energy intake,rely on extreme weight-loss practices,eliminate one or more food groupsfrom their diet, or consume poorlychosen diets, may consume suboptimalamounts of micronutrients and benefitfrom micronutrient supplementa-tion.77 This occurs most frequently inthe case of calcium, vitamin D, iron,and some antioxidants.78-80 Single-micronutrient supplements are gener-ally only appropriate for correction ofa clinically defined medical reason(eg, iron supplements for iron defi-ciency anemia [IDA]).
Micronutrients of key interest:Iron. Iron deficiency, with or withoutanemia, can impair muscle functionand limit work capacity78,81 leading tocompromised training adaptation andathletic performance. Suboptimal ironstatus often results from limited ironintake from heme food sources andinadequate energy intake (approxi-mately 6 mg iron is consumed perw1,000 kcal).82 Periods of rapid
growth, training at high altitudes,menstrual blood loss, foot-strike he-molysis, blood donation, or injury cannegatively influence iron status.79,81
Some athletes in intense training mayalso have increased iron losses insweat, urine, feces, and from intravas-cular hemolysis.
Regardless of the etiology, acompromised iron status can nega-tively influence health, physical andmental performance, and warrantsprompt medical intervention andmonitoring.83 Iron requirements for allfemale athletes may be increased by upto 70% of the estimated averagerequirement.84 Athletes who are atgreatest risk, such as distance runners,vegetarian athletes, or regular blooddonors, should be screened regularlyand aim for an iron intake greaterthan their RDA (ie, >18 mg for womenand >8 mg for men).81,85
Athletes with IDA should seek clin-ical follow-up, with therapies,including oral iron supplementation,86
improvements in diet, and a possiblereduction in activities that influenceiron loss (eg, blood donation or areduction in weight-bearing training tolessen erythrocyte hemolysis).87 Theintake of iron supplements in theperiod immediately after strenuousexercise is contraindicated becausethere is the potential for elevatedhepcidin levels to interfere with ironabsorption.88 Reversing IDA can require3 to 6 months; therefore, it is advan-tageous to begin nutrition interventionbefore IDA develops.78,81 Athletes whoare concerned about iron status or haveiron deficiency without anemia (eg,low ferritin without IDA) should adopteating strategies that promote anincreased intake of food sources ofwell-absorbed iron (eg, heme iron andnonheme ironþvitamin C foods) as thefirst line of defense. Although there issome evidence that iron supplementscan achieve performance improve-ments in athletes with iron depletionwho are not anemic,89 athletes shouldbe educated that routine, unmonitoredsupplementation is not recommended,not considered ergogenic withoutclinical evidence of iron depletion, andmay cause unwanted gastrointestinaldistress.89
Some athletes may experience atransient decrease in hemoglobin atthe initiation of training due to he-modilution, known as dilutional or
FROM THE ACADEMY
512 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

sports anemia, and may not respond tonutrition intervention. These changesappear to be a beneficial adaptation toaerobic training and do not negativelyinfluence performance.79 There is noagreement on the serum ferritin levelthat corresponds to a problematiclevel of iron depletion/deficiency, withvarious suggestions ranging from <10to <35 ng/mL.86 A thorough clinicalevaluation in this scenario is war-ranted because ferritin is an acute-phase protein that increases withinflammation, but in the absence ofinflammation, still serves as the bestearly indicator of compromised ironstatus. Other markers of iron statusand other issues in iron metabolism(eg, the role of hepcidin) are currentlybeing explored.88
Micronutrients of key interest:Vitamin D. Vitamin D regulates cal-cium and phosphorus absorption andmetabolism, and plays a key role inmaintaining bone health. There is alsoemerging scientific interest in the bio-molecular role of vitamin D in skeletalmuscle90 where its role in mediatingmuscle metabolic function91 may haveimplications for supporting athleticperformance. A growing number ofstudies have documented the relation-ship between vitamin D status andinjury prevention,92 rehabilitation,93
improved neuromuscular function,94
increased type II muscle fiber size,94
reduced inflammation,93 decreasedrisk of stress fracture,92,95 and acuterespiratory illness.95
Athletes who live at latitudes >35thparallel or who primarily train andcompete indoors are likely at higherrisk for vitamin D insufficiency (25(OH)D¼20 to 30 ng/mL [50 to 75 nmol/L])and deficiency (25(OH) D <20 ng/mL[<50 nmol/L]). Other factors and life-style habits such as dark complexion,high body fat content, undertaking oftraining in the early morning and eve-ning when ultraviolet B light (UVB)levels are low, and aggressive blockingof UVB exposure (eg, clothing, equip-ment, and screening/blocking lotions)increase the risk for insufficiency anddeficiency.93 Because athletes tend toconsume little vitamin D from thediet93 and dietary interventions alonehave not been shown to be a reliablemeans to resolve insufficient status,96
supplementation above the current
RDA and/or responsible UVB exposuremay be required to maintain sufficientvitamin D status. A recent study ofNational Collegiate Athletic AssociationDivision 1 swimmers and divers re-ported that athletes who started at52 ng/mL (130 nmol/L) and receiveddaily doses of 4,000 IU vitamin D (100mg) were able to maintain sufficientstatus over 6 months (meanchange þ1 ng/mL [þ2.5 nmol/L]),whereas athletes receiving placeboexperienced a mean loss of 20 ng/mL[50 nmol/L].97 Unfortunately, deter-mining vitamin D requirements foroptimal health and performance is acomplex process. Vitamin D bloodlevels from 32 ng/mL (80 nmol/L) andup to 40 ng/mL (100 nmol/L)93 to 50ng/mL (125 nmol/L)94 have beenrecognized as prudent goals foroptimal training-induced adaptation.Although proper assessment andcorrection of deficiency is likely vitalto athlete well-being and athletic suc-cess, current data do not supportvitamin D as an ergogenic aid for ath-letes. Empirical data are still needed toelucidate the direct role of vitamin D inmusculoskeletal health and functionto help refine recommendations forathletes. Until then, athletes with ahistory of stress fracture, bone or jointinjury, signs of overtraining, musclepain or weakness, and a lifestyleinvolving low exposure to UVB mayrequire assessment98 to determine ifan individualized vitamin D supple-mentation protocol is required.
Micronutrients of key interest: Cal-cium. Calcium is especially importantfor growth, maintenance, and repair ofbone tissue; regulation of musclecontraction; nerve conduction; andnormal blood clotting. The risk of lowbone-mineral density and stress frac-tures is increased by low energy avail-ability and, in the case of femaleathletes, menstrual dysfunction, withlow dietary calcium intake contributingfurther to the risk.78,99,100 Low calciumintakes are associated with restrictedenergy intake, disordered eating, and/or the specific avoidance of dairyproducts or other calcium-rich foods.Calcium supplementation should bedetermined after a thorough assess-ment of usual dietary intake. Calciumintakes of 1,500 mg/day and 1,500 to2,000 IU/day vitamin D are needed to
optimize bone health in athletes withlow energy availability or menstrualdysfunctions.12
Micronutrients of key interest: Anti-oxidants. Antioxidant nutrients playimportant roles in protecting cellmembranes from oxidative damage.Because exercise can increase oxygenconsumption by 10- to 15-fold, it hasbeen hypothesized that chronictraining contributes a constant oxida-tive stress on cells.101 Acute exercise isknown to increase levels of lipidperoxide byproducts,101 but also resultsin a net increase in native antioxidantsystem functions and reduced lipidperoxidation.102 Thus, a well-trainedathlete may have a more developedendogenous antioxidant system than aless-active individual and may notbenefit from antioxidant supplemen-tation, especially if consuming a diethigh in antioxidant-rich foods. There islittle evidence that antioxidant sup-plements enhance athletic perfor-mance101 and the interpretation ofexisting data is confounded by issues ofstudy design (eg, a large variability insubject characteristics, training pro-tocols, and the doses and combinationsof antioxidant supplements as well asthe scarcity of crossover designs).There is also some evidence that anti-oxidant supplementation may nega-tively influence training adaptations.103
The safest and most effective strat-egy regarding micronutrient antioxi-dants is to consume a well-chosen dietcontaining antioxidant-rich foods. Theimportance of reactive oxygen speciesin stimulating optimal adaptation totraining merits further investigation,but the current literature does notsupport antioxidant supplementationas a means to prevent exercise-inducedoxidative stress. If athletes decide topursue supplementation, they shouldbe advised not to exceed the TolerableUpper Intake levels because higherdoses could be prooxidative.101 Ath-letes at greatest risk for poor antioxi-dant intakes are those who restrictenergy intake, follow a chronic low-fatdiet, or limit dietary intake of fruits,vegetables, and whole grains.46
In summary of the micronutrients,athletes should be educated thatthe intake of vitamin and mineralsupplements does not improve perfor-mance unless reversing a preexisting
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 513

deficiency78,79 and the literature tosupport micronutrient supplementa-tion is often marred with equivocalfindings and weak evidence. Despitethis, many athletes unnecessarilyconsume micronutrient supplementseven when dietary intake meetsmicronutrient needs. Rather than self-diagnosing the need for micronutrientsupplementation, when relevant, ath-letes should seek clinical assessment oftheir micronutrient status within alarger assessment of their overall di-etary practices. Sports dietitians canoffer several strategies for assessingmicronutrient status based on collec-tion of a nutrient intake history alongwith observing signs and symptomsassociated with micronutrient defi-ciency. This is particularly importantfor iron, vitamin D, calcium, and anti-oxidants. By encouraging athletes toconsume a well-chosen diet focused onfood variety, sports dietitians can helpathletes avoid micronutrient de-ficiencies and gain the benefits of manyother performance-promoting eatingstrategies. Public health guidelinessuch as the DRIs provide micronutrientintake recommendations for sports di-etitians to help athletes avoid bothdeficiency and safety concerns associ-ated with excessive intake. Micro-nutrient intake from dietary sourcesand fortified foods should be assessedalongside micronutrient intake from allother dietary supplements.
THEME 2: PERFORMANCENUTRITION: STRATEGIES TOOPTIMIZE PERFORMANCE ANDRECOVERY FOR COMPETITIONAND KEY TRAINING SESSIONSPre-, During-, and PosteventEatingStrategies implemented in the pre-,during-, and postexercise periods mustaddress a number of goals. First theyshould support or promote optimalperformance by addressing variousfactors related to nutrition that cancause fatigue and deterioration in theoutputs of performance (eg, power,strength, agility, skill, and concentra-tion) throughout or toward the endof the sporting event. These fac-tors include, but are not limited to,dehydration, electrolyte imbalances,glycogen depletion, hypoglycemia, gas-trointestinal discomfort/upset, and dis-turbances to acid-base balance. Fluids
or supplements consumed before, dur-ing, or in the recovery betweensessions can reduce or delay the onsetof these factors. Strategies includeincreasing or replacing key exercisefuels and providing substrates to returnthe body to homeostasis or furtheradapt to the stress incurred during aprevious exercise session. In somecases, pre-event nutrition may need toredress the effects of other activitiesundertaken by the athlete during eventpreparation such as dehydration orrestrictive eating associated with mak-ing weight in weight category sports.A secondary goal is to achieve gutcomfort throughout the event, avoid-ing feelings of hunger or discomfortand gastrointestinal upsets that maydirectly reduce the enjoyment andperformance of exercise and interferewith ongoing nutritional support. Afinal goal is to continue to providenutritional support for health andfurther adaptation to exercise, particu-larly in the case of competitive eventsthat span days and weeks (eg, tourna-ments and stage races).Nutrient needs and the practical
strategies for meeting them beforeduring, and after exercise depend on avariety of factors, including the event(mode, intensity, and duration of exer-cise), the environment, carryover ef-fects from previous exercise, appetite,and individual responses and prefer-ences. In competitive situations, rulesof the event and access to nutritionalsupport may also govern the opportu-nities for food intake. It is beyond thescope of this review to provide furtherdiscussion other than to comment thatsolutions to feeding challenges aroundexercise require experimentation andhabituation by the athlete, and areoften an area in which the foodknowledge, creativity, and practicalexperiences of the sports dietitianmake valuable contributions to anathlete’s nutrition plan. Such scenariosare also where the use of sports foodsand supplements are often most valu-able, because well-formulated productscan often provide a practical form ofnutritional support to meet specializednutrient needs.
Hydration Guidelines: Fluid andElectrolyte BalanceBeing appropriately hydrated contrib-utes to optimal health and exercise
performance. In addition to the usualdaily water losses from respiration,gastrointestinal, renal, and sweatsources, athletes need to replace sweatlosses. Sweating assists with the dissi-pation of heat, generated as a byproductof muscular work but is often exacer-bated by environment conditions, andthus helps maintain body temperaturewithin acceptable ranges.104 Dehydra-tion refers to the process of losingbody water and leads to hypohydra-tion. Although it is common to inter-change these terms, there are subtledifferences since they reflect processand outcome.
Through a cascade of events, themetabolic heat generated by musclecontractions during exercise can even-tually lead to hypovolemia (decreasedplasma/blood volume) and, thus, car-diovascular strain, increased glycogenuse, altered metabolic and central ner-vous system function, and a greaterrise in body temperature.104-106 Al-though it is possible to be hypohy-drated but not hyperthermic (definedas core body temperature exceeding40$C [104$F]),107 in some scenarios theextra thermal strain associated withhypohydration can contribute to anincreased risk of life-threatening exer-tional heat illness (ie, heatstroke). Inaddition to water, sweat contains sub-stantial but variable amounts ofsodium, with lesser amounts of potas-sium, calcium, and magnesium.104 Topreserve homeostasis, optimal bodyfunction, performance, and perceptionof well-being, athletes should strive toundertake strategies of fluid manage-ment before, during, and after exercisethat maintain euhydration. Dependingon the athlete, the type of exercise, andthe environment, there are situationswhen this goal is more or lessimportant.
Although there is complexity and in-dividuality in the response to dehydra-tion, fluid deficits of >2% BW cancompromise cognitive function andaerobic exercise performances, particu-larly in hot weather.104,105,108,109 Decre-ments in the performance of anaerobicor high-intensity activities, sport-specific technical skills, and aerobic ex-ercise in a cool environment are morecommonly seen when 3% to 5% of BW islost due to dehydration.104,105 Severehypohydration with water deficits of 6%to 10% BW has more pronounced effectson exercise tolerance, decreases in
FROM THE ACADEMY
514 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

cardiac output, sweat production, andskin and muscle blood flow.107
Assuming an athlete is in energybalance, daily hydration status may beestimated by tracking early morningBW (measured upon waking and aftervoiding) because acute changes in BWgenerally reflect shifts in body water.Urinary specific gravity and urineosmolality can also be used to approxi-mate hydration status by measuring theconcentration of the solutes in urine.When assessed from a midstreamcollection of the first morning urinesample, a urinary specific gravity of<1.020, perhaps ranging to <1.025 toaccount for individual variability,106 isgenerally indicative of euhydration.Urinary osmolality reflects hypohydra-tion when >900 mOsmol/kg, whereaseuhydration is considered as <700mOsmol/kg.104,106
Before Exercise. Some athletes beginexercise in a hypohydrated state, whichmay adversely affect athletic perfor-mances.105,110 Purposeful dehydrationto make weight may result in a signif-icant fluid deficit, which may be diffi-cult to restore between weigh-in andstart of competition. Similarly, athletesmay be hypohydrated at the onset ofexercise due to recent, prolongedtraining sessions in the heat, or tomultiple events in a day.104,105,108,110
Athletes may achieve euhydrationbefore exercise by consuming a fluidvolume equivalent to 5 to 10 mL/kg BW(w2 to 4 mL/lb) in the 2 to 4 hoursbefore exercise to achieve urine that ispale yellow in color while allowing forsufficient time for excess fluid to bevoided.104,108 Sodium consumed in pre-exercise fluids and foods may helpwith fluid retention. Although someathletes attempt to hyperhydratebefore exercise in hot conditions wherethe rates of sweat loss or restrictionson fluid intake inevitably lead to asignificant fluid deficit, the use ofglycerol and other plasma expandersfor this purpose is now prohibited bythe World Anti-Doping Agency (www.wada-ama.org).
During Exercise. Sweat rates varyduring exercise from 0.3 to 2.4 L/hdependent on exercise intensity, dura-tion, fitness, heat acclimatization, alti-tude, and other environment conditions(eg, heat and humidity).104,106,111,112
Ideally, athletes should drink sufficient
fluids during exercise to replace sweatlosses such that the total body fluiddeficit is limited to <2% BW. Variousfactors may impair the availability offluid or opportunities to consume itduring exercise and for most competi-tive, high-caliber athletes, sweat lossgenerally exceeds fluid intake. However,individual differences are seen indrinking behavior and sweat rates insport, and result in a range of changesin fluid status from substantial dehy-dration to overhydration.110
Routine measurement of pre- andpostexercise BW, accounting for uri-nary losses and drink volume, can helpthe athlete estimate sweat losses dur-ing sporting activities to customizetheir fluid replacement strategies.104 Inthe absence of other factors that alterbody mass during exercise (eg, thesignificant loss of substrate which mayoccur during very prolonged events), aloss of 1 kg BW represents approxi-mately 1 L sweat loss. The fluid planthat suits most athletes and athleticevents will typically achieve an intakeof 0.4 to 0.8 L/h,104 although this needsto be customized to the athlete’stolerance and experience, their oppor-tunities for drinking fluids and thebenefits of consuming other nutrients(eg, carbohydrate) in drink form.Ingestion of cold beverages (0.5$C) mayhelp reduce core temperature and,thus, improve performance in the heat.The presence of flavor in a beveragemay increase palatability and voluntaryfluid intake.Although the typical outcome for
competitive athletes is to develop afluid deficit over the course of an exer-cise session, over the past 2 decadesthere has been an increasing awarenessthat some recreational athletes drink atrates that exceed their sweat losses andoverhydrate. Overdrinking fluids inexcess of sweat and urinary losses is theprimary cause of hyponatremia (plasmasodium <135 mmol/L), also known aswater intoxication, although this can beexacerbated in cases where there areexcessive losses of sodium in sweat andfluid replacement involving low-sodium beverages.113,114 It can also becompounded by excessive fluid intakein the hours or days leading up to theevent. Overhydration is typically seenin recreational athletes because theirwork outputs and sweat rates are lowerthan competitive athletes, whereastheir opportunities and belief in the
need to drink may be greater. Womengenerally have a smaller body sizeand lower sweat rates than men andappear to be at greater risk of over-drinking and possible hyponatremia.104
Symptoms of hyponatremia during ex-ercise occur particularly when plasmasodium levels fall below 130 mEq/L(130 mmol/L) and include bloating,puffiness, weight gain, nausea, vomit-ing, headache, confusion, delirium,seizures, respiratory distress, loss ofconsciousness, and possibly death ifuntreated. Although the prevalenceof hypohydration and hypernatremia isthought to be greater than reports ofhyperhydration and hyponatremia, thelatter are more dangerous and requireprompt medical attention.104,106,114
Sodium should be ingested duringexercise when large sweat sodiumlosses occur. Scenarios include athleteswith high sweat rates (>1.2 L/h), saltysweat, or prolonged exercise exceeding2 hours in duration.105,106,109 Althoughhighly variable, the average concen-tration of sodium in sweat approxi-mates w1 g/L (50 mmol/L) and ishypotonic in comparison to plasmasodium content. Thirst sensation isoften dictated by changes in plasmaosmolality and is usually a good indi-cation of the need to drink but not thatthe athlete is dehydrated.108 Olderathletes may present with age-relateddecreases in thirst sensation and mayneed encouragement to drink duringand postexercise.104
Although skeletal muscle crampsare typically caused by muscle fatigue,they can occur with athletes from alltypes of sports in a range of environ-mental conditions104 and may beassociated with hypohydration andelectrolyte imbalances. Athletes whosweat profusely, especially whenoverlaid with a high sweat sodiumconcentration, may be at greaterrisk for cramping, particularly whennot acclimatized to the heat andenvironment.115
After Exercise. Most athletes finishexercising with a fluid deficit and mayneed to restore euhydration during therecovery period.104,110 Rehydrationstrategies should primarily involve theconsumption of water and sodium at amodest rate that minimizes diuresis/urinary losses.105 The presence of di-etary sodium/sodium chloride (fromfoods or fluids) helps to retain ingested
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 515

fluids, especially extracellular fluids,including plasma volume. Therefore,athletes should not be advised torestrict sodium in their postexercisenutrition particularly when large so-dium losses have been incurred.Because sweat losses and obligatoryurine losses continue during the post-exercise phase, effective rehydrationrequires the intake of a greater volumeof fluid (eg, 125% to 150%) than the finalfluid deficit (eg, 1.25 to 1.5 L fluid forevery 1 kg BW lost).104,106 Excessiveintake of alcohol in the recovery periodis discouraged due to its diuretic ef-fects. However, the previous warningsabout caffeine as a diuretic appear tobe overstated when it is habituallyconsumed in moderate (eg, <180 mg)amounts.104
Carbohydrate Intake GuidelinesBecause of its role as an important fuelfor the muscle and central nervoussystem, the availability of carbohy-drate stores is limiting for the perfor-mance of prolonged continuous orintermittent exercise, and is permis-sive for the performance of sustainedhigh-intensity sport. The depletion ofmuscle glycogen is associated withfatigue and a reduction in the intensityof sustained exercise, whereas inade-quate carbohydrate for the centralnervous system impairs performance-influencing factors such as pacing,perceptions of fatigue, motor skill, andconcentration.3,116 As such, a keystrategy in promoting optimal perfor-mance in competitive events or keyworkouts is matching of body carbo-hydrate stores with the fuel demandsof the session. Strategies to promotecarbohydrate availability should beundertaken before, during, or in therecovery between events or high-quality training sessions.
Achieving Adequate Muscle Glyco-gen Stores. Manipulating nutritionand exercise in the hours and daysbefore an important exercise boutallows an athlete to commence the ses-sion with glycogen stores that arecommensurate with the estimated fuelcosts of the event. In the absence ofsevere muscle damage, glycogen storescan be normalized with 24 hours ofreduced training and adequate fuelintake117 (Table). Events >90 minutes induration may benefit from higher
glycogen stores,118 which can be ach-ieved by a technique known as carbo-hydrate loading. This protocol ofachieving supercompensation of muscleglycogen evolved from the originalstudies of glycogen storage in the 1960sand, at least in the case of trained ath-letes, can be achieved by extendingthe period of a carbohydrate-rich dietand tapering training over 48 hours36
(Table).Carbohydrate consumed in meals
and/or snacks during the 1 to 4 hourspre-exercise may continue to increasebody glycogen stores, particularly liverglycogen levels that have beendepleted by the overnight fast.117 Itmay also provide a source of gutglucose release during exercise.117 Car-bohydrate intakes of 1 to 4 g/kg, withtiming, amount, and food choicessuited to the individual, have beenshown to enhance endurance or per-formance of prolonged exercise(Table).117,119 Generally, foods with alow-fat, low-fiber, and low-moderateprotein content are the preferredchoice for this pre-event menu becausethey are less prone to cause gastroin-testinal problems and promote gastricemptying.120 Liquid meal supplementsare useful for athletes who experiencepre-event nerves or an uncertain pre-event timetable and, thus, prefer amore quickly digested option. Aboveall, the individual athlete shouldchoose a strategy that suits their situ-ation and their past experiences andcan be fine-tuned with furtherexperimentation.The intake of carbohydrate before
exercise is not always straightforwardbecause the metabolic effects of theresulting insulin response include areduction in fat mobilization and useand concomitant increase in carbohy-drate use.119 In some individuals, thiscan cause premature fatigue.121 Strate-gies to circumvent this problem includeensuring at least 1 g/kg carbohydrate inthe pre-event meal to compensate forthe increased carbohydrate oxidation,including a protein source at themeal, including some high-intensity ef-forts in the pre-exercise warm up tostimulate hepatic gluconeogenesis, andconsuming carbohydrate during theexercise.122 Another approach has beensuggested in the form of choosing pre-exercise meals from carbohydrate-richfoods with a low glycemic index,which might reduce the metabolic
changes associated with carbohydrateingestion as well as providing a moresustained carbohydrate release duringexercise. Although occasional studieshave shown that such a strategy en-hances subsequent exercise capacity,123
as summarized by the EAL (Figure 1,Question #11) and others,119 pre-exercise intake of low glycemic indexcarbohydrate choices has not beenfound to provide a universal benefit toperformance even when the metabolicperturbations of pre-exercise carbohy-drate intake are attenuated. Further-more, consumption of carbohydrateduring exercise, as further advised inthe Table, dampens any effects of pre-exercise carbohydrate intake on meta-bolism and performance.124
Depending on characteristics,including the type of exercise, theenvironment, and the athlete’s prepa-ration and carbohydrate tolerance, theintake of carbohydrate during exerciseprovides a number of benefits to exer-cise capacity and performance viamechanisms such as glycogen sparing,provision of an exogenous musclesubstrate, prevention of hypoglycemia,and activation of reward centers in thecentral nervous system.116 Robustliterature on exercise carbohydratefeeding has led to the recognition thatdifferent amounts, timing, and types ofcarbohydrate are needed to achievethese different effects, and that thedifferent effects may overlap in variousevents.36,125 The Table summarizes thecurrent guidelines for exercise fueling,noting opportunities where it may playa metabolic role (events of >60 to 90minutes) and the newer concept of“mouth sensing,” where frequentexposure of the mouth and oral cavityto carbohydrate is likely to be effectivein enhancing workout and pacingstrategies via a central nervous systemeffect.126 Of course, the practicalachievement of these guidelines needsto fit the personal preferences and ex-periences of the individual athlete, andthe practical opportunities providedin an event or workout to obtainand consume carbohydrate-containingfluids or foods. A range of everydayfoods and fluids and formulated sportsproducts that include sports beveragesmay be chosen to meet these guide-lines; this includes newer productscontaining mixtures of glucose andfructose (the so-called multiple trans-portable carbohydrates) that aim to
FROM THE ACADEMY
516 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

increase total intestinal absorption ofcarbohydrates.127 Although this couldbe of use in situations of prolongedexercise where higher rates of exoge-nous carbohydrate oxidation mightsustain work intensity in the face ofdwindling muscle glycogen stores, theEAL found that evidence for benefits iscurrently equivocal (Figure 1, Question#9).Glycogen restoration is one of the
goals of postexercise recovery, partic-ularly between bouts of carbohydrate-dependent exercise where there is apriority on performance in the secondsession. Refueling requires adequatecarbohydrate intake (Table) and time.Because the rate of glycogen resyn-thesis is only w5% per hour, earlyintake of carbohydrate in the recoveryperiod (w1 to 1.2 g/kg/h during thefirst 4 to 6 hours) is useful in maxi-mizing the effective refueling time.117
As long as total intake of carbohydrateand energy is adequate and overallnutritional goals are met, meals andsnacks can be chosen from a variety offoods and fluids according to personalpreferences of type and timing ofintake.36,117 More research is needed toinvestigate how glycogen storagemight be enhanced when energy andcarbohydrate intakes are suboptimal.
Protein Intake GuidelinesProtein consumption in the immediatepre- and postexercise period is oftenintertwined with carbohydrate con-sumption because most athletesconsume foods, beverages, and supple-ments that contain bothmacronutrients.Dietaryprotein consumed in scenarios oflow-carbohydrate availability128 and/orrestricted energy intake53 during theearly postexercise recovery period hasbeen found to enhance and accelerateglycogen repletion. For example, it hasbeen established that recovery of per-formance129 and glycogen repletionrates53 were similar in athletesconsuming 0.8 g carbohydrate/kgBWþ0.4gprotein/kgBWcomparedwithathletes consuming only carbohydrate(1.2 g/kg BW). This may support exerciseperformance and benefit athletesfrequently involved in multiple trainingor competitive sessions over the sameday or successive days.Although protein intake may support
glycogen resynthesis and, when con-sumed in close proximity to strength
and endurance exercise, enhancesMPS,59,130 there is a lack of evidencefrom well-controlled studies that pro-tein supplementation directly im-proves athletic performance.131,132
However, a modest number of studieshave reported that ingesting w50 to100 g protein during the recoveryperiod leads to accelerated recovery ofstatic force and dynamic power pro-duction during delayed onset musclesoreness.133,134 Despite these findingsother studies show no performanceeffects from acute ingestion of proteinat intake levels that are much morepractical to consume on a regular basis.Furthermore, studies that imply posi-tive findings when the control groupreceives a flavored water placebo133 ora placebo that is not isocaloric are un-able to rule out the influence of post-exercise energy provision on theobserved effect.134
Protein ingestion during exerciseand during the pre-exercise periodseems to have less of an influence onMPS than the postexercise provisionof protein but may still enhancemuscle reconditioning depending onthe type of training that takes place.Coingestion of protein and carbohy-drate during 2 hours of intermittentresistance-type exercise has beenshown to stimulate MPS during theexercise period135 and may extend themetabolic adaptation window partic-ularly during ultraendurance-typeexercise bouts.136 Potential benefitsof consuming protein before and dur-ing exercise may be targeted to ath-letes focused on the MPS response toresistance exercise and those lookingto enhance recovery from ultra-endurance exercise.EAL Questions #5 to #7 (Figure 1)
summarize the literature on consumingprotein alone or in combination withcarbohydrate during recovery onseveral outcomes. More work is neededto elucidate the relevance and practi-cality of protein consumption on sub-sequent exercise performance and ifmechanisms in this context are exclu-sive to accelerating muscle glycogensynthesis. The utility of a protein sup-plement should also be measuredagainst the benefits of consuming pro-tein or amino acids from meals andsnacks that are already part of a sportsnutrition plan to meet other perfor-mance goals.
Dietary Supplements andErgogenic AidsExternal and internal motives toenhance performance often encourageathletes to consider the enticing mar-keting and testimonials surroundingsupplements and sports foods. Sportssupplements represent an ever-growing industry, but a lack of regula-tion of manufacture and marketingmeans that athletes can fall victim tofalse advertising and unsubstantiatedclaims.137 The prevalence of supple-mentation among athletes has beenestimated internationally at 37% to89%, with greater frequencies beingreported among elite and older ath-letes. Motivations for use includeenhancement of performance or re-covery, improvement or maintenanceof health, an increase in energy,compensation for poor nutrition, im-mune support, and manipulation ofbody composition,138,139 yet few ath-letes undertake professional assess-ment of their baseline nutrition-relatedhabits. Furthermore, athletes’ supple-mentation practices are often guidedby family, friends, teammates, coaches,the Internet, and retailers, rather thansports dietitians and other sport sci-ence professionals.138
Considerations regarding the use ofsports foods and supplements includean assessment of efficacy and potency.In addition, there are safety concernsdue to the presence of overt and hid-den ingredients that are toxic andthe poor practices of athletes inconsuming inappropriately largedoses or problematic combinations ofproducts. The issue of compliance toantidoping codes remains a concernwith potential contamination withbanned or nonpermissible substances.This carries significant implications forathletes who compete under antidop-ing codes (eg, National CollegiateAthletic Association or World Anti-Doping Agency).139 A supplementmanufacturer’s claim of “100% pure,”“pharmaceutical grade,” “free of ban-ned substances,” “Natural HealthProduct e NHPN/NPN” (in Canada) orpossessing a drug identification num-ber are not reliable indications thatguarantee a supplement is free ofbanned substances. However, com-mercial, third-party auditing programscan independently screen dietarysupplements for banned and restricted
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 517

Category Examples Use Concerns Evidence
Sports food Sports drinksSports barsSports confectionerySports gelsElectrolyte supplementsProtein supplementsLiquid meal supplements
Practical choice to meetsports nutrition goalsespecially when access tofood, opportunities toconsume nutrients, orgastrointestinal concernsmake it difficult toconsume traditional foodand beverages
Cost is greater than wholefoodsMay be used unnecessarily or ininappropriate protocols
Burke andCato(2015)141
Medicalsupplements
Iron supplementsCalcium supplementsVitamin D supplementsMultivitamin/mineraln-3 Fatty acids
Prevention or treatmentof nutrient deficiencyunder the supervision ofappropriate medical/nutrition expert
May be self-prescribedunnecessarily withoutappropriate supervision ormonitoring
Burke andCato(2015)141
Specificperformancesupplements
Ergogenic effects Physiological effects/mechanism ofergogenic effect
Concerns regarding usea Evidence
Creatine Improves performance ofrepeated bouts of high-intensity exercise withshort recovery periods
- Direct effect oncompetitionperformance
- Enhanced capacityfor training
Increases creatine andphosphocreatineconcentrationsMay also have othereffects such asenhancement ofglycogen storage anddirect effect on muscleprotein synthesis
Associated with acute weightgain (0.6-1 kg), which may beproblematic in weight-sensitivesportsMay cause gastrointestinaldiscomfortSome products may notcontain appropriate amounts orforms of creatine
Tarnopolsky(2010)143
Caffeine Reduces perception offatigueAllows exercise to besustained at optimalintensity/output forlonger
Adenosine antagonistwith effects on manybody targets, includingcentral nervous systemPromotes Ca2þ releasefrom sarcoplasmicreticulum
Causes side effects (eg, tremor,anxiety, increased heart rate)when consumed in high dosesToxic when consumed in verylarge dosesRules of National CollegiateAthletic Associationcompetition prohibit the intakeof large doses that produceurinary caffeine levelsexceeding 15 mg/mLSome products do not disclosecaffeine dose or may containother stimulants
Astorino andRoberson(2010)144
Tarnopolsky(2010)143
Burke andcolleagues(2013)145
Sodiumbicarbonate
Improves performance ofevents that wouldotherwise be limited byacid-base disturbancesassociated with high
When taken as an acutedose pre-exercise,increases extracellularbuffering capacity
May cause gastrointestinal side-effects that cause performanceimpairment rather than benefit
Carr andcolleagues(2011)146
(continued on next page)
Figure 2. Dietary supplements and sports foods with evidence-based uses in sports nutrition. These supplements may perform asclaimed but inclusion does not imply endorsement by this position stand.
FROM THE ACADEMY
518 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3
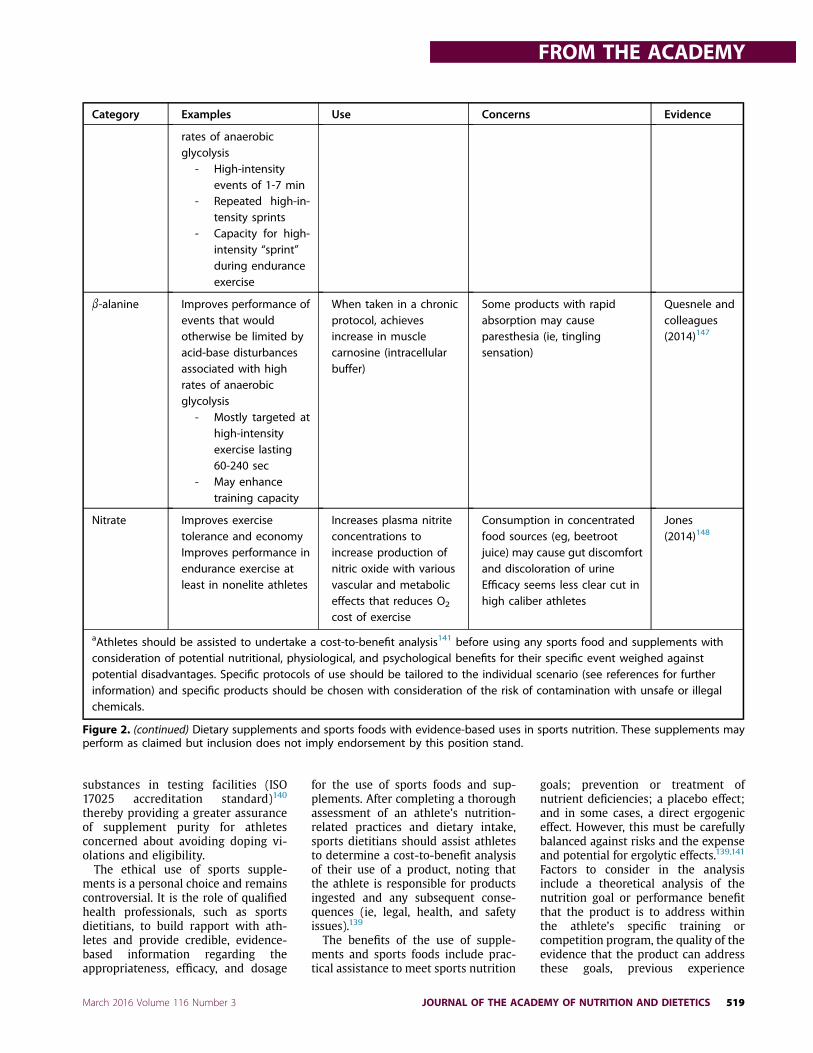
substances in testing facilities (ISO17025 accreditation standard)140
thereby providing a greater assuranceof supplement purity for athletesconcerned about avoiding doping vi-olations and eligibility.The ethical use of sports supple-
ments is a personal choice and remainscontroversial. It is the role of qualifiedhealth professionals, such as sportsdietitians, to build rapport with ath-letes and provide credible, evidence-based information regarding theappropriateness, efficacy, and dosage
for the use of sports foods and sup-plements. After completing a thoroughassessment of an athlete’s nutrition-related practices and dietary intake,sports dietitians should assist athletesto determine a cost-to-benefit analysisof their use of a product, noting thatthe athlete is responsible for productsingested and any subsequent conse-quences (ie, legal, health, and safetyissues).139
The benefits of the use of supple-ments and sports foods include prac-tical assistance to meet sports nutrition
goals; prevention or treatment ofnutrient deficiencies; a placebo effect;and in some cases, a direct ergogeniceffect. However, this must be carefullybalanced against risks and the expenseand potential for ergolytic effects.139,141
Factors to consider in the analysisinclude a theoretical analysis of thenutrition goal or performance benefitthat the product is to address withinthe athlete’s specific training orcompetition program, the quality of theevidence that the product can addressthese goals, previous experience
Category Examples Use Concerns Evidence
rates of anaerobicglycolysis
- High-intensityevents of 1-7 min
- Repeated high-in-tensity sprints
- Capacity for high-intensity “sprint”during enduranceexercise
b-alanine Improves performance ofevents that wouldotherwise be limited byacid-base disturbancesassociated with highrates of anaerobicglycolysis
- Mostly targeted athigh-intensityexercise lasting60-240 sec
- May enhancetraining capacity
When taken in a chronicprotocol, achievesincrease in musclecarnosine (intracellularbuffer)
Some products with rapidabsorption may causeparesthesia (ie, tinglingsensation)
Quesnele andcolleagues(2014)147
Nitrate Improves exercisetolerance and economyImproves performance inendurance exercise atleast in nonelite athletes
Increases plasma nitriteconcentrations toincrease production ofnitric oxide with variousvascular and metaboliceffects that reduces O2
cost of exercise
Consumption in concentratedfood sources (eg, beetrootjuice) may cause gut discomfortand discoloration of urineEfficacy seems less clear cut inhigh caliber athletes
Jones(2014)148
aAthletes should be assisted to undertake a cost-to-benefit analysis141 before using any sports food and supplements withconsideration of potential nutritional, physiological, and psychological benefits for their specific event weighed againstpotential disadvantages. Specific protocols of use should be tailored to the individual scenario (see references for furtherinformation) and specific products should be chosen with consideration of the risk of contamination with unsafe or illegalchemicals.
Figure 2. (continued) Dietary supplements and sports foods with evidence-based uses in sports nutrition. These supplements mayperform as claimed but inclusion does not imply endorsement by this position stand.
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 519

regarding individual responsiveness,and the health and legal consequences.Relatively few supplements that
claim ergogenic benefits are supportedby sound evidence.139,141 Researchmethodologies on the efficacy of sportssupplements are often limited by smallsample sizes, enrollment of untrainedsubjects, poor representation of athletesubpopulations (eg, women, olderathletes, and athletes with disabilities),performance tests that are unreliableor irrelevant, poor control of con-founding variables, and failure toinclude recommended sports nutritionpractices or the interaction with othersupplements.139,141 Even when there isa robust literature on a sports supple-ment, it may not cover all applica-tions that are specific to an event,environment, or individual athlete.Supplement use is best undertaken asan adjunct to a well-chosen nutritionplan. It is rarely effective outside theseconditions and not justified in the caseof young athletes who can make sig-nificant performance gains via matu-ration in age, sports experience, andthe development of a sports nutritionplan.It is beyond the scope of this article
to address the multitude of sportssupplements used by athletes and ca-veats surrounding sport-specific rulesallowing their use. The AustralianInstitute of Sport has developed aclassification system that ranks sportsfoods and supplement ingredientsbased on significance of scientific evi-dence and whether a product is safe,legal, and effective in improving sportsperformance.142 Figure 2 serves as ageneral guide to describe the ergogenicand physiologic effects of potentiallybeneficial supplements and sportfoods.141,143-148 This guide is not meantto advocate specific supplement use byathletes and should only be consideredin well-defined situations.
THEME 3: SPECIALPOPULATIONS ANDENVIRONMENTSVegetarian AthletesAthletesmay opt for a vegetarian diet forvarious reasons from ethnic, religious,and philosophical beliefs to health, foodaversions, and financial constraints or todisguise disordered eating. As with anyself-induced dietary restriction, it wouldbe prudent to explore whether the
vegetarian athlete also presents withdisordered eating or a frank eating dis-order.13,14 A vegetarian diet can benutritionally adequate containing highintakes of fruits, vegetables, wholegrains, nuts, soy products, fiber, phyto-chemicals, and antioxidants.149 Cur-rently, research is lacking regarding theinfluence on athletic performance fromlong-termvegetarianism among athleticpopulations.150
Depending on the extent of die-tary limitations, nutrient concerns forvegetarianism may include energy, pro-tein, fat, iron, zinc, vitaminB-12, calcium,n-3 fatty acids,149 and low intakes ofcreatine and carnosine.151 Vegetarianathletes may have an increased riskof lower bone mineral density andstress fractures.152 Additional practicalchallenges include gaining access tosuitable foods during travel, restaurantdining, and at training camps andcompetition venues. Vegetarian athletesmaybenefit fromcomprehensivedietaryassessments and education to ensuretheir diets are nutritionally sound tosupport training and competitiondemands.
AltitudeAltitude exposure (ie, daily or inter-mittent exposure to >2,000 m [>6,600ft]) may be a specialized strategywithin an athlete’s training program orsimply their daily training environ-ment.153 One of the goals of specializedaltitude training blocks is to naturallyincrease red blood cell mass (erythro-poiesis) so that greater amounts ofoxygen can be carried in the blood toenhance subsequent athletic perfor-mances.112 Initial exposure to altitudeleads to a decrease in plasma volumewith corresponding increases in he-moglobin concentration. Over timethere is a net increase in red cell massand blood volume therefore greateroxygen carrying capacity.154 However,possessing sufficient iron stores beforealtitude training is essential to enablehematological adaptations.154 Con-sumption of iron-rich foods with orwithout iron supplementation may berequired by athletes before and duringaltitude exposure.Specific or chronic exposure to a high-
altitude environment may increase therisk of illness, infection, and suboptimaladaptation to exercise due to direct ef-fects of hypobaric hypoxic conditions,an unaccustomed volume and intensity
of training, interrupted sleep, andincreased UV light exposure.155 The ef-fects are greater with higher elevationand require more acclimatization tominimize the risk of specific altitudeillness. Adequate nutrition is essential tomaximize the desired effect from alti-tude training or to supportmore chronicexposure to a high-altitude environ-ment. Key nutrition-related concernsinclude the adequacyof intake of energy,carbohydrate, protein, fluids, iron, andantioxidant-rich foods.112 An increasedrisk of dehydration at altitude is associ-ated with initial diuresis, increasedventilation, and low humidity, and ex-ercise sweat losses. Some experts sug-gest daily fluid needs as high as 4 to 5 Lwith altitude training and competition,whereas others encourage individualmonitoring of hydration status to deter-mine fluid requirements at altitude.112
Extreme EnvironmentsExtreme environment-related chal-lenges (eg, heat, cold, humidity, andaltitude) require physiological, behav-ioral, and technological adaptationsto ensure athletes are capable ofperforming at their best. Changes inenvironmental conditions stimulatethermoregulatory neuronal activity inthe brain to increase heat loss (sweatingand skin vasodilation), prevent heat loss(skin vasoconstriction), or induce heatgain (shivering). Sympathetic neuralactivation triggers changes in skin bloodflow to vary convective heat transferfrom the core to the skin (or vice versa)as required for maintaining an optimalcore temperature. Unique consider-ations of nutrition-related concerns arepresented when exercising in hot orcold environments.107,155,156
Hot Environments. When ambienttemperature exceeds body tempera-ture, heat cannot be dissipated by ra-diation; furthermore, the potential todissipate heat by evaporation of sweatis substantially reduced when therelative humidity is high.107,156 Heatillness from extreme heat exposure canresult in appetite changes and serioushealth implications (ie, heat exhaustionand exertional heat stroke). Heatexhaustion is characterized by theinability to sustain cardiac outputrelated to exercise-heat stress causingelevated skin temperatures with orwithout hyperthermia (>38.5$C).Symptoms of heat exhaustion can
FROM THE ACADEMY
520 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

include anxiety, dizziness, and fainting.Exertional heat stroke (body core hy-perthermia, typically >40$C) is themost serious and leads to multiorgandysfunction, including brain swelling,with symptoms of central nervoussystem abnormalities, delirium, andconvulsions, thus can be life-threatening.107,156
Athletes competing in lengthy eventsconducted in hot conditions (eg, tennismatch or marathon) and those forcedto wear excessive clothing (eg, Amer-ican football players or BMX competi-tors) are at greatest risk of heatillness.111 Strategies to reduce high skintemperatures and large sweat (fluidand electrolyte) losses are required tominimize cardiovascular and hyper-thermic challenges that may impairathletic performance when exercisingin the heat; athletes should be regu-larly monitored when at risk for heat-related illness.107,156 Specific strategiesshould include acclimatization, indi-vidualized hydration plans, regularmonitoring of hydration status, begin-ning exercise euhydrated, consumingcold fluids during exercise, andpossibly the inclusion of electrolytesources.107,156
Cold Environments. Athletic perfor-mance in cold environments may pre-sent several dietary challenges thatrequire careful planning for optimalnutritional support. A large number ofsports train and compete in the cold,ranging from endurance athletes (eg,Nordic skiers) to judged events (eg, freestyle ski). Furthermore, drastic, unex-pected environment changes can turn awarm-weather event (eg, cross countrymountain bike race or triathlon) intoextreme cold conditions in a shortperiod of time, leaving unpreparedathletes confronted with performing inthe cold.Primary concerns of exercising in a
cold environment are maintenance ofeuhydration and body temperature.156
However, exercise-induced heat pro-duction and appropriate clothing aregenerally sufficient to minimize heatloss.155,156 When adequately prepared(eg, removing wet clothing and keep-ing muscles warm after exercisewarm-up) athletes can tolerate severecold in pursuit of athletic success.Smaller, leaner athletes are at greaterrisk of hypothermia due to increasedheat production required to maintain
core temperature and decreasedinsulation from lower body fat. Meta-bolically, energy requirements (fromcarbohydrates) are increased, espe-cially when shivering, to maintaincore temperature.155,156
Several factors can increase the riskof hypohydration when exercising inthe cold, such as cold-induced diuresis,impaired thirst sensation, reduceddesire to drink, limited access to fluids,self-restricted fluid intake to minimizeurination, sweat losses from over-dressing, and increased respirationwith high altitude exposure.In the cold, hypohydration of 2% to 3%
BW loss is less detrimental to enduranceperformances than similar losses occur-ring in the heat.104,155,156 Severe coldexposure may be problematic ontraining vs competition days becausetraining duration may exceed competi-tion duration and officials may delaycompetitions in inclement weather, yetathletes may continue to train in similarconditions. Athletes’ energy, macronu-trient, and fluid intakes should be regu-larly assessed and changes in BW andhydration statuswhen exercising in bothhot and cold environments. Educatingathletes about modifying their energy,carbohydrate intakes, and recoverystrategies according to training andcompetition demands promotes optimaltraining adaptation and maintenance ofhealth. Practical advice for preparationand selection of appropriate foods andfluids that withstand cold exposurewill ensure athletes are equipped tocope with weather extremes.
THEME 4: ROLES ANDRESPONSIBILITIES OF SPORTSDIETITIANSSports nutrition practice requirescombined knowledge in several topics:clinical nutrition, nutrition science,exercise physiology, and application ofevidence-based research. Increasingly,athletes and active individuals seekprofessionals to guide them in makingoptimal food and fluid choices to sup-port and enhance their physical per-formances. An experienced sportsdietitian demonstrates the knowledge,skills, and expertise necessary to helpathletes and teams work toward theirperformance-related goals.The Commission on Dietetic Regis-
tration (the credentialing agency forthe Academy) has created a unique
credential for registered dietitian nu-tritionists who specialize in sportsdietetic practice with extensive expe-rience working with athletes. TheBoard Certified Specialist in SportsDietetics credential is designed as thepremier professional sports nutritioncredential in the United States and isavailable internationally, includingCanada. Specialists in sports dieteticsprovide safe, effective, evidence-basednutrition assessments, guidance, andcounseling for health and perfor-mance for athletes, sport organizations,and physically active individualsand groups. For Board CertifiedSpecialist in Sports Dietetics certifica-tion details refer to the Commission onDietetic Registration (www.cdrnet.org).Enhancement of sports nutritionknowledge and continuing educationcan also be achieved by completingrecognized postgraduate qualificationssuch as the 2-year distance learningdiploma in sports nutrition offeredby the International Olympic Commit-tee. For more information refer toSports Oracle (www.sportsoracle.com/Nutrition/Home/).
The Academy157 describes the com-petencies of sports dietitians as “[to]provide medical nutrition therapy indirect care and design, implement andmanage safe and effective nutritionstrategies that enhance lifelong health,fitness, and optimal physical perfor-mance.” Roles and responsibilities ofsports dietitians working with athletesare outlined in Figure 3.
SUMMARYThe following summarizes the evi-dence presented in this position paper:
" Athletes need to consume energythat is adequate in amount andtiming of intake during periods ofhigh-intensity and/or long-duration training to maintainhealth and maximize trainingoutcomes. Low energy availabilitycan result in unwanted loss ofmuscle mass; menstrual dysfunc-tion and hormonal disturbances;suboptimal bone density; anincreased risk of fatigue, injury,and illness; impaired adaptation;and a prolonged recovery process.
" The primary goal of a trainingdiet is to provide nutritional sup-port to allow an athlete to stayhealthy and injury-free while
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 521

Role of sports dietitian Responsibilities
Assessment of nutritionneeds and current dietarypractices
" Energy intake, nutrients, and fluids before, during, and after training and competitions" Nutrition-related health concerns (eg, eating disorders, food allergies or intolerances,
gastrointestinal disturbances, injury management, muscle cramps, and hypoglycemia) andbody composition goals
" Food and fluid intake as well as estimated energy expenditure during rest, taper, and traveldays
" Nutrition needs during extreme conditions (eg, high altitude training or environment-related concerns)
" Adequacy of athlete’s body weight and metabolic risk factors associated with low bodyweight
" Supplementation practices" Basic measures of height and body weight, with possible assessment of body composition
Interpretation of testresults (eg, biochemistryand anthropometry)
" Blood, urine analysis, body composition, and physiological testing results, includinghydration status
Dietary prescription andeducation
" Dietary strategies to support behavior change for improvements with health, physicalperformance, body composition goals, and/or eating disorders
" Dietary recommendations prescribed relative to athlete’s personal goals and chief con-cerns related to training, body composition, and/or competition nutrition, tapering, and/orperiodized fat/weight loss
" Quantity, quality, and timing for food and fluid intake before, during, and after trainingand/or competition to enhance exercise training capacity, endurance, and performance
" Medical nutrition therapy advice pertaining to unique dietary considerations (eg, eatingdisorders, food allergies, diabetes, and gastrointestinal issues)
" Menu planning, time management, grocery shopping, food preparation, food storage, foodbudgeting, food security, and recipe modification for training and/or competition days
" Food selection related to travel, restaurants, and training and competition venue choices" Supplementation, ergogenic aids, and fortified foods regarding legality, safety, and efficacy" Sport nutrition education, resource development, and support may be with individual
athletes; entire teams; and/or with coaches, athletic trainers, physiologists, or foodservicestaff
Collaboration andintegration
" Contribution as a member of a multidisciplinary team within sport settings to integratenutrition programming into a team or athlete’s annual training and competition plan
" Collaboration with the health care team/performance professionals (eg, physicians, athletictrainer, physiologists, and psychologists) for the performance management of athletes
Evaluation andprofessionalism
" Evaluation of scientific literature and provision of evidence-based assessment andapplication to athletic performance
" Development of oversight of nutrition policies and procedures" Documentation of measurable outcomes of nutrition services" Recruitment and retention of clients and athletes in practice" Provision of reimbursable services (eg, diabetes medical nutrition therapy)" Promotion of career longevity for active individuals, collegiate, and professional athletes" Serve as a mentor for developing sports dietitians" Maintenance of credential(s) by actively engaging in profession-specific continuing
education activities
Figure 3. Sports dietitian roles and responsibilities.
FROM THE ACADEMY
522 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

maximizing the functional andmetabolic adaptations to a perio-dized exercise program that pre-pares him or her to better achievethe performance demands of theevent. Whereas some nutritionstrategies allow athletes to trainhard and recover quickly, othersmay target an enhanced trainingstimulus or adaptation.
" The optimal physique, includingbody size, shape, and composi-tion (eg, muscle mass and bodyfat levels), depends upon the sex,age, and heredity of the athlete,and may be sport- and event-specific. Physique assessmenttechniques have inherent limi-tations of reliability and validity,but with standardized measure-ment protocols and carefulinterpretation of results, theymay provide useful information.Where significant manipulationof body composition is required,it should ideally take place wellbefore the competitive season tominimize the influence on eventperformance or reliance on rapidweight loss techniques.
" Body carbohydrate stores pro-vide an important fuel source forthe brain and muscle during ex-ercise, and are manipulated byexercise and dietary intake.Recommendations for carbohy-drate intake typically range from3 to 10 g/kg BW/day (and up to12 g/kg BW/day for extreme andprolonged activities), dependingon the fuel demands of trainingor competition, the balance be-tween performance and trainingadaptation goals, the athlete’stotal energy requirements andbody composition goals. Targetsshould be individualized to theathlete and his or her event, andalso periodized over the week,and training cycles of the sea-sonal calendar according tochanges in exercise volume andthe importance of high carbo-hydrate availability for differentexercise sessions.
" Recommendations for proteinintake typically range from 1.2to 2.0 g/kg BW/day, but havemore recently been expressedin terms of the regular spacingof intakes of modest amounts ofhigh-quality protein (0.3 g/kg
body weight) after exercise andthroughout the day. Such in-takes can generally be met fromfood sources. Adequate energyis needed to optimize proteinmetabolism, and when energyavailability is reduced (eg, toreduce BW or fat), higher pro-tein intakes are needed to sup-port MPS and retention of FFM.
" For most athletes, fat intakesassociated with eating styles thataccommodate dietary goals typi-cally range from 20% to 35% oftotal energy intake. Consuming%20% of energy intake from fatdoes not benefit performanceand extreme restriction of fatintake may limit the food rangeneeded to meet overall healthand performance goals. Claimsthat extremely high-fat, carbo-hydrate-restricted diets provide abenefit to the performance ofcompetitive athletes are notsupported by current literature.
" Athletes should consume dietsthat provide at least the RDA orAdequate Intake for all micro-nutrients. Athletes who restrictenergy intake or use severeweight-loss practices, eliminatecomplete food groups from theirdiet, or follow other extreme di-etary philosophies are at greatestrisk of micronutrient deficiencies.
" A primary goal of competitionnutrition is to address nutrition-related factors that may limitperformance by causing fatigueand a deterioration in skill orconcentration over the course ofthe event. For example, in eventsthat are dependent on musclecarbohydrate availability, mealseaten in the day(s) leading up toan event should provide suffi-cient carbohydrate to achieveglycogen stores that arecommensurate with the fuelneeds of the event. Exercise ta-per and a carbohydrate-rich diet(7 to 12 g/kg BW/day) cannormalize muscle glycogenlevels within w24 hours,whereas extending this to 48hours can achieve glycogensupercompensation.
" Foods and fluids consumed inthe 1 to 4 hours before an eventshould contribute to body car-bohydrate stores (particularly, in
the case of early morning eventsto restore liver glycogen after theovernight fast), ensure appro-priate hydration status, andmaintain gastrointestinal com-fort throughout the event. Thetype, timing, and amount offoods and fluids included in thispre-event meal and/or snackshould be well trialed and indi-vidualized according to thepreferences, tolerance, and ex-periences of each athlete.
" Dehydration/hypohydration canincrease the perception of effortand impair exercise perfor-mance; thus, appropriate fluidintake before, during, and afterexercise is important for healthand optimal performance. Thegoal of drinking during exerciseis to address sweat losses thatoccur to assist thermoregulation.Individualized fluid plans shouldbe developed to use the oppor-tunities to drink during aworkout or competitive event toreplace as much of the sweatloss as is practical; neitherdrinking in excess of sweat ratenor allowing dehydration toreach problematic levels. Afterexercise, the athlete shouldrestore fluid balance by drinkinga volume of fluid that is equiva-lent to w125% to 150% of theremaining fluid deficit (eg, 1.25to 1.5 L fluid for every 1 kg BWlost).
" An additional nutrition-relatedstrategy for events of >60 mi-nutes’ duration is to consumecarbohydrate according to itspotential to enhance perfor-mance. These benefits are ach-ieved via a variety of mechanismsthat may occur independently orsimultaneously and are generallydivided into metabolic (providingfuel to the muscle) and central(supporting the central nervoussystem). Typically, an intake of 30to 60 g/h provides benefits bycontributing to muscle fuel needsand maintaining blood glucoseconcentrations, although in veryprolonged events (2.5þ hours) orother scenarios where endoge-nous carbohydrate stores aresubstantially depleted, higher in-takes (up to 90 g/h) are associ-ated with better performance.
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 523
Even in sustained high-intensityevents of 45 to 75 minuteswhere there is little need forcarbohydrate intake to play ametabolic role, frequent exposureof the mouth and oral cavity tosmall amounts of carbohydratecan still enhance performance viastimulation of the brain andcentral nervous system.
" Rapid restoration of perfor-mance between physiologicallydemanding training sessions orcompetitive events requiresappropriate intake of fluids,electrolytes, energy, and carbo-hydrates to promote rehydrationand restore muscle glycogen. Acarbohydrate intake of w1.0 to1.2 g/kg/h, commencing duringthe early recovery phase andcontinuing for 4 to 6 hours, willoptimize rates of resynthesis ofmuscle glycogen. The availableevidence suggests that the earlyintake of high-quality proteinsources (0.25 to 0.3 g/kg BW)will provide amino acids to buildand repair muscle tissue andmay enhance glycogen storage insituations where carbohydrateintake is suboptimal.
" In general, vitamin and mineralsupplements are unnecessary forathletes who consume a dietproviding high energy availabilityfrom a variety of nutrient-densefoods. A multivitamin/mineralsupplement may be appropriatein some cases when these condi-tions do not exist; for example, ifan athlete is following an energy-restricted diet or is unwilling orunable to consume sufficient di-etary variety. Supplementationrecommendations should beindividualized, realizing that tar-geted supplementation may beindicated to treat or prevent defi-ciency (eg, iron and vitamin D).
" Athletes should be counseledregarding the appropriate use ofsports foods and nutritional er-gogenic aids. Such productsshould only be used after carefulevaluation for safety, efficacy,potency, and compliance withrelevant antidoping codes andlegal requirements.
" Vegetarian athletes may be atrisk for low intakes of energy,protein, fat, creatine, carnosine,
n-3 fatty acids, and key micro-nutrients such as iron, calcium,riboflavin, zinc, and vitamin B-12.
References1. Deakin V, Kerr D, Boushey C. Measuring
nutritional status of athletes: Clinicaland research perspectives. In: Burke L,Deakin V, eds. Clinical Sports Nutrition.5th ed. North Ryde, Australia: McGraw-Hill; 2015:27-53.
2. Manore M, Thompson J. Energy re-quirements of the athlete: Assessmentand evidence of energy efficiency. In:Burke L, Deakin V, eds. Clinical SportsNutrition. 5th ed. Sydney, Australia:McGraw-Hill; 2015:114-139.
3. Spriet LL. New insights into the interac-tion of carbohydrate and fat metabolismduring exercise. Sports Med.2014;44(suppl 1):S87-S96.
4. Cunningham JJ. A reanalysis of the fac-tors influencing basal metabolic rate innormal adults. Am J Clin Nutr.1980;33(11):2372-2374.
5. Roza AM, Shizgal HM. The Harris Bene-dict equation reevaluated: Resting energyrequirements and the body cell mass.Am J Clin Nutr. 1984;40(1):168-182.
6. Guebels CP, Kam LC, Maddalozzo GF,Manore MM. Active women before/afteran intervention designed to restoremenstrual function: Resting metabolicrate and comparison of four methods toquantify energy expenditure and energyavailability. Int J Sport Nutr Exerc Metab.2014;24(1):37-46.
7. Ainsworth BE, Haskell WL, Whitt MC,et al. Compendium of physical activities:An update of activity codes and METintensities. Med Sci Sports Exerc.2000;32(9 suppl):S498-S504.
8. US Department of Health and HumanServices and US Department of Agricul-ture. 2015 e 2020 Dietary Guidelines forAmericans. 8th Edition. December 2015.http://health.gov/dietaryguidelines/2015/guidelines/. Accessed February 5, 2016.
9. Institute of Medicine, Food and NutritionBoard. Dietary Reference intakes for En-ergy, Carbohydrate, Fiber, Fat, Fatty Acids,Cholesterol, Protein, and Amino Acids.Washington, DC: The National Acade-mies Press; 2005.
10. Loucks AB. Energy balance and energyavailability. In: Maughan RJ, ed. SportsNutrition, The Encyclopaedia of SportsMedicine, an IOC Medical CommissionPublication. West Sussex, UK: John Wiley& Sons, Ltd; 2013:72-87.
11. De Souza MJ, Nattiv A, Joy E, et al. 2014Female Athlete Triad Coalitionconsensus statement on treatment andreturn to play of the female athletetriad: 1st International Conference heldin San Francisco, California, May 2012and 2nd International Conference heldin Indianapolis, Indiana, May 2013. Br JSports Med. 2014;48(4):289.
12. Mountjoy M, Sundgot-Borgen J,Burke L, et al. The IOC consensusstatement: Beyond the female athletetriad—Relative Energy Deficiency inSport (RED-S). Br J Sports Med.2014;48(7):491-497.
13. Garner DM. Eating Disorder Inventory-3:Professional Manual. Lutz, FL: Psycho-logical Assessment Resources, Inc; 2004.
14. American Psychiatric Association. Diag-nostic and Statistical Manual of MentalDisorders, 5th Edition: DSM-5. Arlington,VA: American Psychiatric Association;2013.
15. Sundgot-Borgen J, Meyer NL,Lohman TG, et al. How to minimise thehealth risks to athletes who compete inweight-sensitive sports review and po-sition statement on behalf of the Ad HocResearch Working Group on BodyComposition, Health and Performance,under the auspices of the IOC MedicalCommission. Br J Sports Med.2013;47(16):1012-1022.
16. Stellingwerff T, Maughan RJ, Burke LM.Nutrition for power sports: Middle-distance running, track cycling, rowing,canoeing/kayaking, and swimming.J Sport Sci. 2011;29(suppl 1):S79-S89.
17. O’Connor H, Slater G. Losing, gaining andmaking weight for athletes. In: Lanham-New S, Stear S, Sherriffs M, Collins A, eds.Sport and Exercise Nutrition. West Sussex,UK: Wiley-Blackwell; 2011:210-232.
18. Sundgot-Borgen J, Garthe I. Elite athletesin aesthetic and Olympic weight-classsports and the challenge of bodyweight and body compositions. J SportSci. 2011;29(suppl 1):S101-S114.
19. Steffes GD, Megura AE, Adams J, et al.Prevalence of metabolic syndrome riskfactors in high school and NCAA divisionI football players. J Strength ConditiongRes. 2013;27(7):1749-1757.
20. Ackland TR, Lohman TG, Sundgot-Borgen J, et al. Current status of bodycomposition assessment in sport: Re-view and position statement on behalf ofthe ad hoc research working group onbody composition health and perfor-mance, under the auspices of the I.O.C.Medical Commission. Sports Med.2012;42(3):227-249.
21. Santos DA, Dawson JA, Matias CN, et al.Reference values for body compositionand anthropometric measurements inathletes. PloS ONE. 2014;9(5):e97846.
22. Turocy PS, DePalma BF, Horswill CA,et al. National Athletic Trainers’ Associ-ation position statement: Safe weightloss and maintenance practices in sportand exercise. J Athletic Train. 2011;46(3):322-336.
23. Slater G, Rice A, Jenkins D, Hahn A. Bodymass management of lightweight row-ers: Nutritional strategies and perfor-mance implications. Br J Sports Med.2014;48(21):1529-1533.
24. Wilson G, Drust B, Morton JP, Close GL.Weight-making strategies in profes-sional jockeys: Implications for physicaland mental health and well-being.Sports Med. 2014;44(6):785-796.
25. Garthe I, Raastad T, Refsnes PE, Koivisto A,Sundgot-Borgen J. Effect of two differentweight-loss rates on body compositionand strength and power-related perfor-mance in elite athletes. Int J Sport NutrExerc Metab. 2011;21(2):97-104.
26. Mettler S, Mitchell N, Tipton KD.Increased protein intake reduces leanbody mass loss during weight loss in
FROM THE ACADEMY
524 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3

athletes. Med Sci Sports Exerc. 2010;42(2):326-337.
27. Thomas DM, Martin CK, Lettieri S, et al.Can a weight loss of one pound a weekbe achieved with a 3500-kcal deficit?Commentary on a commonly acceptedrule. Int J Obes (Lond). 2013;37(12):1611-1613.
28. Hopkins WG, Hawley JA, Burke LM.Design and analysis of research on sportperformance enhancement. Med SciSports Exerc. 1999;31(3):472-485.
29. Maughan RJ, Gleeson M. The BiochemicalBasis of Sports Performance. Oxford,United Kindom: Oxford UniversityPress; 2010.
30. Hawley JA, Burke LM, Phillips SM,Spriet LL. Nutritional modulation oftraining-induced skeletal muscle adapta-tions. J Appl Physiol. 2011;110(3):834-845.
31. Cole M, Coleman D, Hopker J, Wiles J.Improved gross efficiency during longduration submaximal cycling following ashort-term high carbohydrate diet. Int JSports Med. 2014;35(3):265-269.
32. Philp A, Hargreaves M, Baar K. Morethan a store: Regulatory roles forglycogen in skeletal muscle adaptationto exercise. Am J Physiol EndocrinolMetab. 2012;302(11):E1343-E1351.
33. Bartlett JD, Hawley JA, Morton JP. Car-bohydrate availability and exercisetraining adaptation: Too much of a goodthing? Eur J Sport Sci; 2014:1-10.
34. Stellingwerff T. Contemporary nutritionapproaches to optimize elite marathonperformance. Int J Sports Physiol Perform.2013;8(5):573-578.
35. Lee JM, Kim Y, Welk GJ. Validity ofconsumer-based physical activity moni-tors. Med Sci Sports Exerc. 2014;46(9):1840-1848.
36. Burke LM, Hawley JA, Wong SH,Jeukendrup AE. Carbohydrates fortraining and competition. J Sports Scis.2011;29(suppl 1):S17-S27.
37. Cox GR, Clark SA, Cox AJ, et al. Dailytraining with high carbohydrate avail-ability increases exogenous carbohydrateoxidation during endurance cycling.J Appl Physiol. 2010;109(1):126-134.
38. Burke LM. Fueling strategies to optimizeperformance: Training high or traininglow? Scan J Med Sci Sports. 2010;20(suppl 2):48-58.
39. Phillips SM, Van Loon LJ. Dietary proteinfor athletes: From requirements to op-timum adaptation. J Sports Sci.2011;29(suppl 1):S29-S38.
40. Phillips SM. Dietary protein requirementsand adaptive advantages in athletes. BrJ Nutr. 2012;108(suppl 2):S158-S167.
41. Miller BF, Olesen JL, Hansen M, et al.Coordinated collagen and muscle pro-tein synthesis in human patella tendonand quadriceps muscle after exercise.J Physiol. 2005;567(pt 3):1021-1033.
42. Babraj J, Cuthbertson DJ, Rickhuss P,et al. Sequential extracts of human boneshow differing collagen synthetic rates.Biochem Soc Transact. 2002;30(2):61-65.
43. Churchward-Venne TA, Burd NA,Mitchell CJ, et al. Supplementation of asuboptimal protein dose with leucine or
essential amino acids: Effects on myofi-brillar protein synthesis at rest andfollowing resistance exercise in men.J Physiol. 2012;590(pt 11):2751-2765.
44. Burd NA, West DW, Moore DR, et al.Enhanced amino acid sensitivity ofmyofibrillar protein synthesis persistsfor up to 24 h after resistance exercisein young men. J Nutr. 2011;141(4):568-573.
45. World Health Organization and Foodand Agriculture Organization of theUnited Nations, United Nations Univer-sity. Joint WHOFAOUNUEC. Protein andamino acid requirements in humannutrition. World Health OrganizationTechnical Report Series. Geneva,Switzerland: World Health Organiza-tion; 2007(935):1-265, back cover.
46. Rosenbloom CA, Coleman EJ. SportsNutrition: A Practice Manual for Pro-fessionals. Chicago, IL: Academy ofNutrition & Dietetics; 2012.
47. Moore DR, Phillips SM, Slater G. Protein.In: Deakin V, Burke L, eds. Clinical SportsNutrition. 5th ed. Sydney, Australia:McGraw-Hill Education; 2015:94-113.
48. Areta JL, Burke LM, Camera DM, et al.Reduced resting skeletal muscle proteinsynthesis is rescued by resistance exerciseand protein ingestion following short-term energy deficit. Am J Physiol Endo-crinol Metab. 2014;306(8):E989-E997.
49. Rodriguez NR, Vislocky LM, Gaine PC.Dietary protein, endurance exercise, andhuman skeletal-muscle protein turn-over. Curr Opin Clin Nutr Metab Care.2007;10(1):40-45.
50. Wall BT, Morton JP, van Loon LJ. Strate-gies to maintain skeletal muscle mass inthe injured athlete: Nutritional consid-erations and exercise mimetics. Eur JSport Sci. 2015;15(1):53-62.
51. Phillips SM, Moore DR, Tang JE. A criticalexamination of dietary protein re-quirements, benefits, and excesses inathletes. Int J Sport Nutr Exerc Metab.2007;17(suppl 17):S58-S76.
52. Tipton KD, Witard OC. Protein re-quirements and recommendations forathletes: Relevance of ivory tower ar-guments for practical recommendations.Clin Sports Medicine. 2007;26(1):17-36.
53. Beelen M, Burke LM, Gibala MJ, vanLoon LJ. Nutritional strategies to pro-mote postexercise recovery. Int SportNutr Exerc Metab. 2010;20(6):515-532.
54. Moore DR, Robinson MJ, Fry JL, et al.Ingested protein dose response of mus-cle and albumin protein synthesis afterresistance exercise in young men. Am JClin Nutr. 2009;89(1):161-168.
55. Areta JL, Burke LM, Ross ML, et al. Timingand distribution of protein ingestionduring prolonged recovery from resis-tance exercise alters myofibrillar proteinsynthesis. J Physiol. 2013;591(pt 9):2319-2331.
56. Schoenfeld BJ, Ratamess NA,Peterson MD, Contreras B, Sonmez GT,Alvar BA. Effects of different volume-equated resistance training loadingstrategies on muscular adaptations inwell-trained men. J Strength ConditionRes. 2014;28(10):2909-2918.
57. Josse AR, Tang JE, Tarnopolsky MA,Phillips SM. Body composition andstrength changes in women with milkand resistance exercise. Med Sci SportsExerc. 2010;42(6):1122-1130.
58. Phillips SM. A brief review of critical pro-cesses in exercise-induced muscular hy-pertrophy. Sports Med. 2014;44(suppl 1):S71-S77.
59. Tipton KD, Elliott TA, Cree MG,Aarsland AA, Sanford AP, Wolfe RR.Stimulation of net muscle protein syn-thesis by whey protein ingestion beforeand after exercise. Am J Physiol Endo-crinol Metab. 2007;292(1):E71-E76.
60. Hartman JW, Tang JE, Wilkinson SB, et al.Consumption of fat-free fluid milk afterresistance exercise promotes greaterlean mass accretion than does con-sumption of soy or carbohydrate inyoung, novice, male weightlifters. Am JClin Nutr. 2007;86(2):373-381.
61. Josse AR, Atkinson SA, Tarnopolsky MA,Phillips SM. Increased consumption ofdairy foods and protein during diet- andexercise-induced weight loss promotesfat mass loss and lean mass gain inoverweight and obese premenopausalwomen. J Nutr. 2011;141(9):1626-1634.
62. Pennings B, Boirie Y, Senden JM,Gijsen AP, Kuipers H, van Loon LJ. Wheyprotein stimulates postprandial muscleprotein accretion more effectively thando casein and casein hydrolysate inolder men. Am J Clin Nutr. 2011;93(5):997-1005.
63. Health Canada. Eating Well with Cana-da’s Food Guide. http://www.hc-sc.gc.ca/fn-an/food-guide-aliment/index-eng.php. Accessed July 7, 2015.
64. Phinney SD, Bistrian BR, Evans WJ,Gervino E, Blackburn GL. The humanmetabolic response to chronic ketosiswithout caloric restriction: Preservationof submaximal exercise capabilitywith reduced carbohydrate oxidation.Metab Clin Experiment. 1983;32(8):769-776.
65. Volek JS, Noakes T, Phinney SD.Rethinking fat as a fuel for enduranceexercise. Eur J Sport Sci. 2014:1-8.
66. Havemann L, West SJ, Goedecke JH, et al.Fat adaptation followed by carbohydrateloading compromises high-intensitysprint performance. J Appl Physiol.2006;100(1):194-202.
67. Stellingwerff T, Spriet LL, Watt MJ, et al.Decreased PDH activation and glyco-genolysis during exercise following fatadaptation with carbohydrate restora-tion. Am J Physiol Endocrinol Metab.2006;290(2):E380-E388.
68. Burke LM. Re-examining high-fat dietsfor sports performance: Did we call the“nail in the coffin” too soon? Sports Med.2015;45(1):33-49.
69. Barnes MJ. Alcohol: Impact on sportsperformance and recovery in male ath-letes. Sports Med. 2014;44(7):909-919.
70. Lourenco S, Oliveira A, Lopes C. The ef-fect of current and lifetime alcohol con-sumption on overall and central obesity.Eur J Clin Nutr. 2012;66(7):813-818.
71. Burke LM, Collier GR, Broad EM, et al.Effect of alcohol intake on muscle
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 525

glycogen storage after prolonged exer-cise. J Appl Physiol. 2003;95(3):983-990.
72. Hobson RM, Maughan RJ. Hydrationstatus and the diuretic action of a smalldose of alcohol. Alcohol Alcoholism.2010;45(4):366-373.
73. Parr EB, Camera DM, Areta JL, et al.Alcohol ingestion impairs maximal post-exercise rates of myofibrillar proteinsynthesis following a single bout ofconcurrent training. PloS ONE.2014;9(2):e88384.
74. Burke LM, Read RS. A study of dietarypatterns of elite Australian footballplayers. Can J Sport Sci. 1988;13(1):15-19.
75. Graham T. Alcohol ingestion and man’sability to adapt to exercise in a coldenvironment. Can J Appl Sport Sci.1981;6(1):27-31.
76. Verster JC. The alcohol hangover—Apuzzling phenomenon. Alcohol Alco-holism. 2008;43(2):124-126.
77. Farajian P, Kavouras SA, Yannakoulia M,Sidossis LS. Dietary intake and nutri-tional practices of elite Greek aquaticathletes. Int J Sport Nutr Exerc Metab.2004;14(5):574-585.
78. Lukaski HC. Vitamin and mineral status:Effects on physical performance. Nutri-tion. 2004;20(7-8):632-644.
79. Volpe SL, Bland E. Vitamins, minerals,and exercise. In: Rosenbloom CA,Coleman EJ, eds. Sports Nutrition: APractice Manual for Professionals. 5th ed.Chicago, IL: Academy of Nutrition andDietetics; 2012:75-105.
80. Woolf K, Manore MM. B-vitamins andexercise: Does exercise alter re-quirements? Int J Sport Nutr Exerc Metab.2006;16(5):453-484.
81. Haymes E. Iron. In: Driskell J, Wolinsky I,eds. Sports Nutrition: Vitamins and TraceElements. New York, NY: CRC/Taylor &Francis; 2006:203-216.
82. Beard J, Tobin B. Iron status and exercise.Am J Clin Nutr. 2000;72(2 suppl):594S-597S.
83. McClung JP, Karl JP, Cable SJ, et al. Ran-domized, double-blind, placebo-controlled trial of iron supplementationin female soldiers during militarytraining: Effects on iron status, physicalperformance, and mood. Am J Clin Nutr.2009;90(1):124-131.
84. DellaValle DM. Iron supplementation forfemale athletes: Effects on iron statusand performance outcomes. Curr SportsMed Rep. 2013;12(4):234-239.
85. Cowell BS, Rosenbloom CA, Skinner R,Summers SH. Policies on screening fe-male athletes for iron deficiency inNCAA division I-A institutions. Int J SportNutr Exerc Metab. 2003;13(3):277-285.
86. Peeling P, Dawson B, Goodman C,Landers G, Trinder D. Athletic inducediron deficiency: New insights into therole of inflammation, cytokines andhormones. Eur J Appl Physiol.2008;103(4):381-391.
87. Sim M, Dawson B, Landers G, Trinder D,Peeling P. Iron regulation in athletes:Exploring the menstrual cycle and ef-fects of different exercise modalities on
hepcidin production. Int J Sport NutrExerc Metab. 2014;24(2):177-187.
88. Peeling P, Sim M, Badenhorst CE, et al.Iron status and the acute post-exercisehepcidin response in athletes. PloS ONE.2014;9(3):e93002.
89. Burden RJ, Morton K, Richards T,Whyte GP, Pedlar CR. Is iron treatmentbeneficial in, iron-deficient but non-anaemic (IDNA) endurance athletes? Ameta-analysis. Br J Sports Med.2015;49(21):1389-1397.
90. Pojednic RM, Ceglia L. The emergingbiomolecular role of vitamin D in skel-etal muscle. Exerc Sport Sci Rev.2014;42(2):76-81.
91. Sinha A, Hollingsworth KG, Ball S,Cheetham T. Improving the vitamin Dstatus of vitamin D deficient adults isassociated with improved mitochondrialoxidative function in skeletal muscle.J Clin Endocrinol Metab. 2013;98(3):E509-E513.
92. Ruohola JP, Laaksi I, Ylikomi T, et al.Association between serum 25(OH)Dconcentrations and bone stress fracturesin Finnish young men. J Bone MineralRes. 2006;21(9):1483-1488.
93. Larson-Meyer DE, Willis KS. Vitamin Dand athletes. Curr Sports Med Rep.2010;9(4):220-226.
94. Cannell JJ, Hollis BW, Sorenson MB,Taft TN, Anderson JJ. Athletic perfor-mance and vitamin D. Med Sci SportsExerc. 2009;41(5):1102-1110.
95. Halliday TM, Peterson NJ, Thomas JJ,Kleppinger K, Hollis BW, Larson-Meyer DE. Vitamin D status relative todiet, lifestyle, injury, and illness in col-lege athletes. Med Sci Sports Exerc.2011;43(2):335-343.
96. Lagowska K, Kapczuk K, Friebe Z,Bajerska J. Effects of dietary interven-tion in young female athletes withmenstrual disorders. J Int Soc SportsNutr. 2014;11:21.
97. Lewis RM, Redzic M, Thomas DT. Theeffects of season-long vitamin D sup-plementation on collegiate swimmersand divers. Int J Sports Nutr Exerc Metab.2013;23(5):431-440.
98. Moran DS, McClung JP, Kohen T,Lieberman HR. Vitamin D and physicalperformance. Sports Med. 2013;43(7):601-611.
99. Nickols-Richardson SM, Beiseigel JM,Gwazdauskas FC. Eating restraint isnegatively associated with biomarkersof bone turnover but not measurementsof bone mineral density in youngwomen. J Am Diet Assoc. 2006;106(7):1095-1101.
100. Nattiv A, Loucks AB, Manore MM, et al.American College of Sports Medicineposition stand. The female athlete triad.Med Sci Sports Exerc. 2007;39(10):1867-1882.
101. Peternelj TT, Coombes JS. Antioxidantsupplementation during exercisetraining: Beneficial or detrimental?Sports Med. 2011;41(12):1043-1069.
102. Watson TA, MacDonald-Wicks LK,Garg ML. Oxidative stress and antioxi-dants in athletes undertaking regular
exercise training. Int J Sports Nutr ExercMetab. 2005;15(2):131-146.
103. Draeger CL, Naves A, Marques N, et al.Controversies of antioxidant vitaminssupplementation in exercise: Ergogenicor ergolytic effects in humans? J Int SocSports Nutr. 2014;11(1):4.
104. American College of Sports Medicine,Sawka MN, Burke LM, Eichner ER, et al.American College of Sports Medicineposition stand. Exercise and fluidreplacement. Med Sci Sports Exerc.2007;39(2):377-390.
105. Shirreffs SM, Sawka MN. Fluid andelectrolyte needs for training, competi-tion, and recovery. J Sports Sci.2011;29(suppl 1):S39-S46.
106. KenefickRW,Cheuvront SN.Hydration forrecreational sport and physical activity.Nutr Rev. 2012;70(suppl 2):S137-S142.
107. American College of Sports Medicine,Armstrong LE, Casa DJ, Millard-Stafford M, et al. American College ofSports Medicine position stand. Exer-tional heat illness during training andcompetition. Med Sci Sports Exerc.2007;39(3):556-572.
108. Goulet ED. Dehydration and enduranceperformance in competitive athletes.Nutr Rev. 2012;70(suppl 2):S132-S136.
109. Jeukendrup A, Carter J, Maughan RJ.Competition fluid and fuel. In: Burke L,Deakin V, eds. Clinical Sports Nutrition.5th ed. North Ryde NSW, Australia:McGraw-Hill Australia Pty Ltd; 2015:377-419.
110. Garth AK, Burke LM. What do athletesdrink during competitive sporting activ-ities? Sports Med. 2013;43(7):539-564.
111. Mountjoy M, Alonso JM, Bergeron MF,et al. Hyperthermic-related challengesin aquatics, athletics, football, tennis andtriathlon. Br J Sports Med. 2012;46(11):800-804.
112. Koehle MS, Cheng I, Sporer B. CanadianAcademy of Sport and Exercise Medicineposition statement: Athletes at highaltitude. Clin J Sports Med. 2014;24(2):120-127.
113. Jeukendrup AE. Nutrition for endurancesports: Marathon, triathlon, and roadcycling. J Sports Sci. 2011;29(suppl 1):S91-S99.
114. Hew-Butler T, Rosner MH, Fowkes-Godek S, et al. Statement of the ThirdInternational Exercise-Associated Hypo-natremia Consensus Development Con-ference, Carlsbad, California, 2015. Clin JSports Med. 2015;25(4):303-320.
115. Bergeron MF. Exertional heat cramps:Recovery and return to play. J SportRehab. 2007;16(3):190-196.
116. Cermak NM, van Loon LJ. The use ofcarbohydrates during exercise as an er-gogenic aid. Sports Med. 2013;43(11):1139-1155.
117. Burke LM, Kiens B, Ivy JL. Carbohydratesand fat for training and recovery. J SportsSci. 2004;22(1):15-30.
118. Hawley JA, Schabort EJ, Noakes TD,Dennis SC. Carbohydrate-loading andexercise performance. An update. SportsMed. 1997;24(2):73-81.
FROM THE ACADEMY
526 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3
119. Ormsbee MJ, Bach CW, Baur DA. Pre-exercise nutrition: The role of macronutri-ents, modified starches and supplementson metabolism and endurance perfor-mance. Nutrients. 2014;6(5):1782-1808.
120. Rehrer NJ, van Kemenade M, Meester W,Brouns F, Saris WH. Gastrointestinal com-plaints in relation to dietary intake in tri-athletes. Int J Sports Nutr. 1992;2(1):48-59.
121. Foster C, Costill DL, Fink WJ. Effectsof preexercise feedings on enduranceperformance.Med Sci Sports. 1979;11(1):1-5.
122. Coyle EF. Timing and method ofincreased carbohydrate intake to copewith heavy training, competition andrecovery. J Sports Sci. 1991;9(summer):29-51. discussion 51-22.
123. Thomas DE, Brotherhood JR, Brand JC.Carbohydrate feeding before exercise:Effect of glycemic index. Int J Sports Med.1991;12(2):180-186.
124. Burke LM, Claassen A, Hawley JA,Noakes TD. Carbohydrate intake duringprolonged cycling minimizes effect ofglycemic index of preexercise meal.J Appl Physiol. 1998;85(6):2220-2226.
125. Stellingwerff T, Cox GR. Systematic re-view: Carbohydrate supplementation onexercise performance or capacity ofvarying durations. Appl Physiol NutrMetab. 2014;39(9):998-1011.
126. Burke LM, Maughan RJ. The Governorhas a sweet tooth—Mouth sensing ofnutrients to enhance sports perfor-mance. Eur J Sport Sci. 2014:1-12.
127. Jeukendrup AE. Carbohydrate and ex-ercise performance: The role of multi-ple transportable carbohydrates. CurrOpin Clin Nutr Metab Care. 2010;13(4):452-457.
128. Betts JA, Williams C. Short-term recov-ery from prolonged exercise: exploringthe potential for protein ingestion toaccentuate the benefits of carbohydratesupplements. Sports Med. 2010;40(11):941-959.
129. Berardi JM, Noreen EE, Lemon PW. Re-covery from a cycling time trial isenhanced with carbohydrate-proteinsupplementation vs. isoenergetic carbo-hydrate supplementation. J Int Soc SportsNutr. 2008;5:24.
130. Tipton KD, Rasmussen BB, Miller SL,et al. Timing of amino acid-carbohydrateingestion alters anabolic response ofmuscle to resistance exercise. Am JPhysiol Endocrinol Metab. 2001;281(2):E197-E206.
131. van Essen M, Gibala MJ. Failure of pro-tein to improve time trial performancewhen added to a sports drink. Med SciSports Exerc. 2006;38(8):1476-1483.
132. Ivy JL, Res PT, Sprague RC, Widzer MO.Effect of a carbohydrate-protein sup-plement on endurance performance
during exercise of varying intensity. Int JSports Nutr Exerc Metab. 2003;13(3):382-395.
133. Etheridge T, Philp A, Watt PW. A singleprotein meal increases recovery ofmuscle function following an acuteeccentric exercise bout. Appl Physiol NutrMetab. 2008;33(3):483-488.
134. Hoffman JR, Ratamess NA, Tranchina CP,Rashti SL, Kang J, Faigenbaum AD.Effect of a proprietary protein supple-ment on recovery indices followingresistance exercise in strength/powerathletes. Amino Acids. 2010;38(3):771-778.
135. Beelen M, Koopman R, Gijsen AP, et al.Protein coingestion stimulates muscleprotein synthesis during resistance-typeexercise. Am J Physiol Endocrinol Metab.2008;295(1):E70-E77.
136. van Loon LJ. Is there a need for proteiningestion during exercise? Sports Med.2014;44(suppl 1):S105-S111.
137. Health Canada. Pathway for licensingnatural health products making modernhealth claims. http://www.hc-sc.gc.ca/dhp-mps/prodnatur/legislation/docs/modern-eng.php#a11. Accessed August 19, 2015.
138. Braun H, Koehler K, Geyer H, Kleiner J,Mester J, Schanzer W. Dietary supple-ment use among elite young Germanathletes. Int J Sport Nutr Exerc Metab.2009;19(1):97-109.
139. Maughan RJ. Risks and rewards of di-etary supplement use by athletes. In:Maughan RJ, ed. Sports Nutrition, TheEncyclopaedia of Sports Medicine, an IOCMedical Commission Publication. 1st ed.West Sussex, UK: John Wiley & Sons Ltd;2014.
140. International Organization for Standardi-zation and International ElectrotechnicalCommission. General requirements forthe competence of testing and calibrationlaboratories, Switzerland. ISO/IEC 17025:2005 (E). ISO; 2005.
141. Burke LM, Cato L. Supplements andsports foods. In: Burke LM, Deakin V,eds. Clinical Sports Nutrition. 5th ed.North Ryde NSW, Australia: McGraw-Hill Pty Ltd.; 2015:493-591.
142. Australian Institute of Sport. Supplements.http://www.ausport.gov.au/ais/nutrition/supplements. Accessed July 7, 2015.
143. Tarnopolsky MA. Caffeine and creatineuse in sport. Ann Nutr Metab.2010;57(suppl 2):1-8.
144. Astorino TA, Roberson DW. Efficacy ofacute caffeine ingestion for short-termhigh-intensity exercise performance: Asystematic review. J Strength Condition-ing Res. 2010;24(1):257-265.
145. Burke L, Desbrow B, Spriet L. Caffeine forSports Performance. Champagne, IL: Hu-man Kinetics; 2013.
146. Carr AJ, Hopkins WG, Gore CJ. Effects ofacute alkalosis and acidosis on perfor-mance: A meta-analysis. Sports Med.2011;41(10):801-814.
147. Quesnele JJ, Laframboise MA, Wong JJ,Kim P, Wells GD. The effects ofbeta-alanine supplementation on per-formance: A systematic review of theliterature. Int J Sport Nutr Exerc Metab.2014;24(1):14-27.
148. Jones AM. Influence of dietary nitrate onthe physiological determinants of exer-cise performance: A critical review. ApplPhysiol Nutr Metab. 2014;39(9):1019-1028.
149. Craig WJ, Mangels AR; ; American Di-etetic Association. Position of theAmerican Dietetic Association: Vege-tarian diets. J Am Diet Assoc.2009;109(7):1266-1282.
150. Berning JR. The vegetarian athlete. In:Maughan RJ, ed. The Encyclopaedia ofSports Medicine: An IOC Medical Com-mission Publications, Sports Nutrition.West Sussux, United Kingdom: Wiley;2014:382-391.
151. Burke DG, Chilibeck PD, Parise G,Candow DG, Mahoney D, Tarnopolsky M.Effect of creatine and weight training onmuscle creatine and performance invegetarians. Med Sci Sports Exerc.2003;35(11):1946-1955.
152. Wentz L, Liu PY, Ilich JZ, Haymes EM.Dietary and training predictors of stressfractures in female runners. Int J SportNutr Exerc Metab. 2012;22(5):374-382.
153. Ross ML, Martin DS. Heat and altitude.In: Deakin V, Burke L, eds. ClinicalSports Nutrition. 5th ed. Sydney,Australia: McGraw-Hill Education;2015:767-791.
154. Bergeron MF, Bahr R, Bartsch P, et al.International Olympic Committeeconsensus statement on thermoregula-tory and altitude challenges for high-level athletes. Br J Sports Med.2012;46(11):770-779.
155. Meyer NL, Manore MM, Helle C. Nutri-tion for winter sports. J Sports Sci.2011;29(suppl 1):S127-S136.
156. Cheuvront SN, Ely BR, Wilber RL. Envi-ronment and exercise. In: Maughan RJ,ed. Sports Nutrition, The Encyclopaedia ofSports Medicine, an IOC Medical Com-mission Publication. 1st ed. West Sussex,United Kingdom: John Wiley & Sons Ltd;2014:425-438.
157. Steinmuller PL, Kruskall LJ, Karpinski CA,Manore MM, Macedonio MA, Meyer NL.Academy of Nutrition and Dietetics:Revised 2014 Standards of Practice andStandards of Professional Performancefor registered dietitian nutritionists(competent, proficient, and expert) insports nutrition and dietetics. J Acad NutrDiet. 2014;114(4):631-641. e643.
FROM THE ACADEMY
March 2016 Volume 116 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 527

This Academy of Nutrition and Dietetics, Dietitians of Canada (DC), and American College of Sports Medicine (ACSM) position statement wasadopted by the Academy House of Delegates Leadership Team on July 12, 2000, and reaffirmed on May 25, 2004, and February 15, 2011;approved by DC on November 17, 2015, and approved by the ACSM Board of Trustees on November 20, 2015. This position statement is in effectuntil December 31, 2019. Position papers should not be used to indicate endorsement of products or services. All requests to use portions of theposition or republish in its entirety must be directed to the Academy at [email protected].
Authors: Academy of Nutrition and Dietetics: D. Travis Thomas, PhD, RDN, CSSD (College of Health Sciences, University of Kentucky, Lexington);Dietitians of Canada: Kelly Anne Erdman, MSc, RD, CSSD (Canadian Sport Institute Calgary/University of Calgary Sport Medicine Centre, Calgary,AB, Canada); American College of Sports Medicine: Louise M. Burke, OAM, PhD, APD, FACSM (AIS Sports Nutrition/Australian Institute of SportAustralia and Mary MacKillop Institute of Health Research, Australian Catholic University, Melbourne, Australia).
Reviewers: Academy of Nutrition and Dietetics: Sports, Cardiovascular, and Wellness Nutrition dietetic practice group (Jackie Buell, PhD, RD, CSSD,ATC Ohio State University, Columbus); Amanda Carlson-Phillips, MS, RD, CSSD (EXOS, Phoenix, AZ); Sharon Denny, MS, RD (Academy KnowledgeCenter, Chicago, IL); D. Enette Larson-Meyer, PhD, RD, FACSM (University of Wyoming, Laramie); Mary Pat Raimondi, MS, RD (Academy PolicyInitiatives & Advocacy, Washington, DC). Dietitians of Canada: Ashley Armstrong, MS, RD (Canadian Sport Institute Pacific, Vancouver, Victoria,and Whistler, BC, Canada); Susan Boegman, RD, IOC Dip Sport Nutrition (Canadian Sport Institute Pacific, Victoria, BC, Canada); Susie Langley MS,RD, DS, FDC (retired, Toronto, ON, Canada); Marielle Ledoux, PhD, PDt (professor, University of Montreal, Montreal, QC, Canada); EmmaMcCrudden, MSc (Canadian Sport Institute Pacific, Vancouver, Victoria, and Whistler, BC, Canada); Pearle Nerenberg, MSc, PDt (Pearle SportsNutrition, Montreal, QC, Canada); Erik Sesbreno, RD, IOC Dip Sport Nutrition (Canadian Sport Institute Ontario, Toronto, ON, Canada). AmericanCollege of Sports Medicine: Dan Benardot, PhD, RD, LD, FACSM (Georgia State University Atlanta); Kristine Clark, PhD, RDN, FACSM (The Penn-sylvania State University, University Park); Melinda M. Manore, PhD, RD, CSSD, FACSM (Oregon State University, Corvallis); Emma Stevenson, PhD(Newcastle University, Newcastle upon Tyne, Tyne and Wear, United Kingdom).
Academy Positions Committee Workgroup: Connie Diekman, MEd, RD, CSSD, LD, FADA, FAND (chair) (Washington University, St Louis, MO);Christine A. Rosenbloom, PhD, RDN, CSSD, FAND (Georgia State University, Atlanta); Roberta Anding, MS, RD, LD, CDE, CSSD, FAND (contentadvisor) (Texas Children’s Hospital, Houston, and Houston Astros MLB Franchise, Houston, TX).
The authors thank the reviewers for their many constructive comments and suggestions. The reviewers were not asked to endorse this positionor the supporting article.
FROM THE ACADEMY
528 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2016 Volume 116 Number 3