positive deviance unleashing creative action at the front line history and theory katie procter
TRANSCRIPT

Positive DevianceUnleashing Creative Action at the Front Line
History and Theory
Katie Procter



Millions of people worldwide are suffering from infections
acquired in hospitals and other healthcare settings.
Some Canadian Statistics
• Each year in Canada, more than 220,000 healthcare associated infections result in 8,500-12,000 deaths, and the rates are rising.
• One in nine hospital patients in Canada get a healthcare associated infection.
• Infections are the fourth leading cause of death in Canada.
• From Healthcare Acquired Infections – Canadian Union of Public Employees report 2009
MRSA
• “Superbug” – common, deadly and relentless• Some successful eradication of MRSA in some
Northern European countries and very isolated American institutions
• Positive Deviance Initiative and Plexus Institute to explore using PD in healthcare facilities

August 2005
• PD Institute promoted the use of the PD approach to reduce MRSA in 40 hospitals around the world
• PDI collaborated with Veterans Administration to work in 6 hospitals in the US
• Used the MRSA bundle – hand hygiene, active surveillance, contact precautions and environmental cleaning
It’s easier to ACT your way into a
new way of THINKING than to THINK your way
into a new way of ACTING!!
• Focus on practice rather than knowledge
Modified Focus Groups
• Discovery and Action Dialogues
• Improvisation
• Theory of Inventive Problem-Solving (TIPS) or TRIZ in Russian

13
USA Trial Results Clinical results: 35% average drop in MRSA infection
•The Billings Clinic incidence rate declined by 88%•Albert Einstein Medical Center infections dropped 35% so,•57 people went back to their families, homes and lives.
Expected organizational results•Hand hygiene and gowns & gloves use improved at all sites•Self-report data on performance & employee satisfaction
improvedUnexpected benefits
• Improved nursing recruitment into tough units• Improved process for on-call scheduling
14
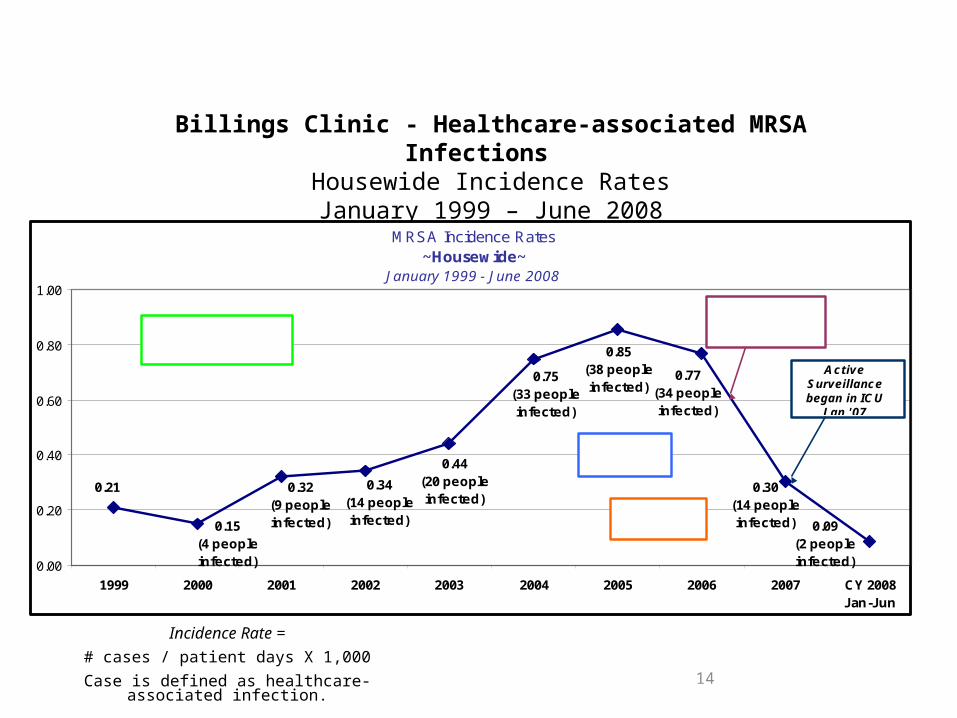
Billings Clinic - Healthcare-associated MRSA Infections Housewide Incidence RatesJanuary 1999 – June 2008
Incidence Rate =
# cases / patient days X 1,000
Case is defined as healthcare-associated infection.
MRSA Incidence Rates~Housewide~
January 1999 - June 2008
0.09(2 peopleinfected)
0.77(34 peopleinfected)
0.85(38 peopleinfected)
0.75(33 peopleinfected)
0.44(20 peopleinfected)
0.34(14 peopleinfected)
0.21
0.15(4 peopleinfected)
0.32(9 peopleinfected)
0.30(14 peopleinfected)
0.00
0.20
0.40
0.60
0.80
1.00
1999 2000 2001 2002 2003 2004 2005 2006 2007 CY 2008Jan-Jun
Active Surveillance began in ICU
J an '07
May 2006 PD/MRSA
Project began
2005-2007 65% decrease
2006-2007 55% decrease
J an 1, 2005-J une 30, 2008 89% reduction in HA
MRSA Infections
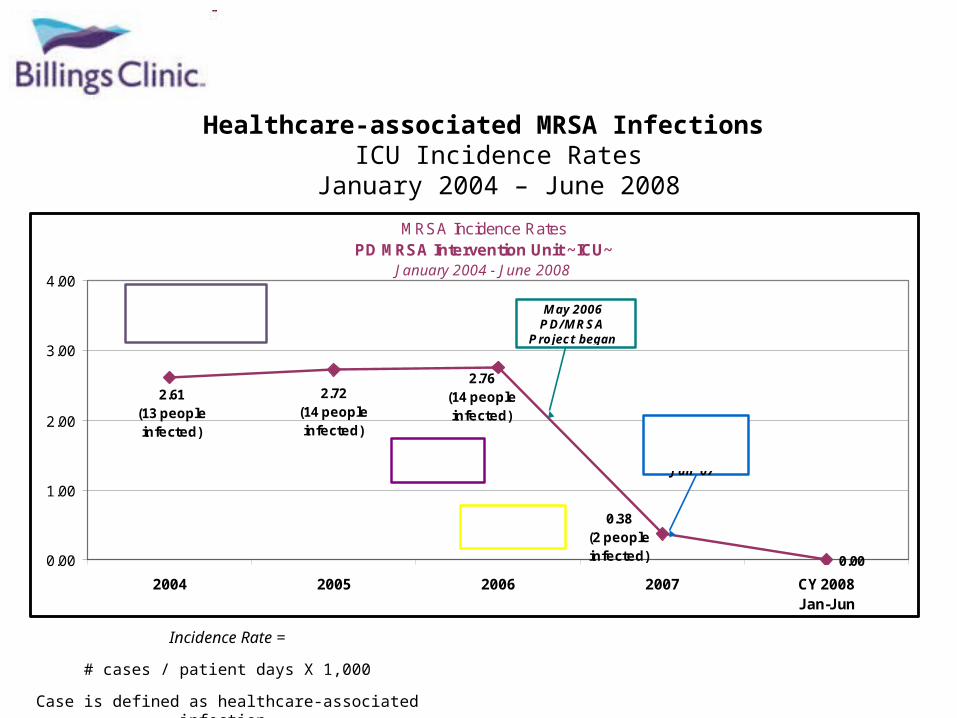
Healthcare-associated MRSA Infections ICU Incidence Rates
January 2004 – June 2008
Incidence Rate =
# cases / patient days X 1,000
Case is defined as healthcare-associated infection.
MRSA Incidence RatesPD MRSA Intervention Unit ~ICU~
January 2004 - June 2008
0.00
0.38(2 peopleinfected)
2.76(14 peopleinfected)
2.72(14 people infected)
2.61(13 peopleinfected)
0.00
1.00
2.00
3.00
4.00
2004 2005 2006 2007 CY 2008Jan-Jun
May 2006 PD/MRSA
Project began
Active Surveillance began in ICU
J an '072006-2007 86%
decrease
2007-2008 100% decrease
J an 1, 2006-J un 30, 2008 100% reduction in HA
MRSA Infections

Canadian Research Project• 6 beta sites to start – 2 in BC – Vancouver
General and Kelowna General – 5 stayed for the long haul
• All submitted data and came up with very creative ideas
• Toronto East General very successful• Now projects dotted all across Canada
Canadian Research Project• In general, the rates of infection have come
down across all sites in the preliminary data• Vancouver General Hospital was the only
hospital that reported hand hygiene compliance – there was an increase from 35% to 83% and has settled back to about 75%
• Faster response by staff to infection break out
To get started you need!
• Complete top to bottom commitment• Management that agrees to just remove
the boulders• A coach with skilled facilitation in leading the techniques• A strong PD core team made up of
volunteer interdisciplines – 4 – 6 is ideal
Some kind of a kick off and regular meetings
• Information to staff as to what you are doing• Some kind of kick-off• Regular core team/coach meetings – suggest once a
week for 4 – 6 months then drop back to every 2 weeks/reassess
• Regular core team/staff meetings as well – suggest once a week for 4 – 6 months then assess what you need based on the energy and work being done – tie these to:
Reporting of the data by the STAFF that makes sense to their process
changes and how it makes sense to their needs.
Good facilitators have NO HOMEWORK – THE STAFF DO!

Some challenges• Complete shift for practitioners – from being the
expert to being facilitator asking questions• Need comfort with power sharing and letting go of
control• Strategies to scale up• Time and human resources to have the
conversations• Need comfort with uncertainty• You can’t predict all outcomes and • consequences• It’s a slower process
Unleashing is all about Engaging your PEOPLE,
developing SKILLS, changing BEHAVIOR,
INSPIRING & MOBILIZING them

This is about LOCAL change, NOT borrowing from other institutions
Unusual Suspects
• This is about finding local people or pockets of positivity where the job gets done who have no more resources than anyone else then spread peer-to-peer
• It might be someone who surprises you. Ask around!
You use it when you know that:You have a Wicked
Important Problem that is Seemingly Unsolvable
Behavior needs to change NOT knowledge
Skilled facilitation is
available
Progress is measureable, it
just might be different
When you want different outcomes•FROM
•Problems•Best practices•Buy-in•Education•Shame and Blame•Knowledge•Big initiatives•Telling•Periscoped purpose•Prescription•Top down•Standard outcomes
•TO•Solutions•Local emergence•Ownership•Learning•Celebrating local success•Behavior•Small changes•Asking•Shared purpose•Discovery•Unusual suspects•Joyful, shared meaning & extraordinary results
When you want different conversations•Nothing will make a difference!
•We’re doing everything we can do!
•We don’t have time!
•We don’t have the resources!
•You’ll never get them to change!
•Just tell us what to do!
•Don’t tell me what to do!
•We will always have this problem!•ETC ETC ETC
•We can make a difference!
•We can do more!
•We actually do have time!
•We don’t need anymore resources!
•We CAN change!
•We CAN do!
•We can fix this problem!
http://www.positivedeviance.org/pdf/Newsletter/October2012newsletter.pdf
