postmenopausal osteoporosis overview bruce ettinger, md senior investigator division of research...
TRANSCRIPT

Postmenopausal Postmenopausal Osteoporosis OverviewOsteoporosis Overview
Bruce Ettinger, MD Bruce Ettinger, MD Senior InvestigatorSenior Investigator
Division of ResearchDivision of Research
Kaiser Permanente Medical Care ProgramKaiser Permanente Medical Care Program
Oakland, CaliforniaOakland, California

Summary of Summary of PresentationPresentation
Importance of Osteoporotic FractureImportance of Osteoporotic Fracture Making the diagnosisMaking the diagnosis Drug TreatmentsDrug Treatments
what workswhat works who should be treatedwho should be treated changing treatmentschanging treatments

* * Morphometric 3SD deformities Morphometric 3SD deformities Wasnich RD: Primer Metabolic Bone Diseases and Disorders of Mineral Wasnich RD: Primer Metabolic Bone Diseases and Disorders of Mineral Metabolism. 1999 Metabolism. 1999
Incidence Rates for Vertebral, Wrist and Hip Fractures in Women
After Age 50
4.04.0
3.03.0
2.02.0
1.01.0
Vertebrae*Vertebrae*
HipHip
WristWrist
Annual Annual incidence/100incidence/100
50 60 50 60 Age (yrs) 70 80Age (yrs) 70 80

Effect of Preexisting Vertebral Effect of Preexisting Vertebral Fracture on Risk of Subsequent Fracture on Risk of Subsequent
Vertebral FractureVertebral Fracture
R Lindsay, et al. R Lindsay, et al. JAMAJAMA 2001;285:320-23 2001;285:320-23
2725 2725 postmenopausal women randomized to placebo.postmenopausal women randomized to placebo.
00
55
1010
1515% % new new
vertebralvertebralfracturefracture
Number baseline vertebral fracturesNumber baseline vertebral fractures
RR = 7.3RR = 7.3
RR = 2.6RR = 2.6
00 11 22

Cumulative Hip Fracture Cumulative Hip Fracture ProbabilityProbability
20.720.7 21.421.4
10.610.610.310.3
00
55
1010
1515
2020
2525
HawaiiHawaii MinnesotaMinnesota HawaiiHawaii All JapanAll Japan
CaucasianCaucasian JapaneseJapanese

Relative Risk of Death Following Relative Risk of Death Following FracturesFractures
Fracture Intervention Trial (FIT)* Fracture Intervention Trial (FIT)*
JA Cauley, et al. JA Cauley, et al.
Osteoporos IntOsteoporos Int. 2000;11:556-61.. 2000;11:556-61.*6459 *6459 postmenopausal women, 55-81 yr, postmenopausal women, 55-81 yr, followed for an average of 3.8 years.followed for an average of 3.8 years.
Any ClinicalAny Clinical
Age-Adjusted Relative Risk (95% CI)Age-Adjusted Relative Risk (95% CI)00 1.01.0 2.02.0 5.05.0
Non-spineNon-spine
OtherOther
ForearmForearm
SpineSpine
HipHip
10.010.0
6.76.7
8.68.6

Mortality Rates by Number Mortality Rates by Number of of
Prevalent Vertebral Prevalent Vertebral FracturesFractures
Age-adjustedAge-adjustedmortalitymortality (per 1000 (per 1000
person-years)person-years)
DM Kado, et al. DM Kado, et al. Arch Intern MedArch Intern Med 1999;159:1215-20 1999;159:1215-20
Number baseline vertebral fracturesNumber baseline vertebral fracturesp for trend <.001
00
55
1010
1515
2020
2525
3030
3535
4040
00 11 22 33 44 5+5+
45

KyphosisKyphosis
Height loss Height loss
Ribs compress Ribs compress abdomen abdomen
Acute and chronic pain Acute and chronic pain
Limited activityLimited activity
Breathing difficultiesBreathing difficulties
Indigestion Indigestion Gastric refluxGastric reflux
Depression Depression
Impaired quality of lifeImpaired quality of life
Consequences of Vertebral Fractures

Vertebral Fractures Are Vertebral Fractures Are OverlookedOverlooked
Radiologist fail to diagnose vertebral Radiologist fail to diagnose vertebral deformities in routine x-raysdeformities in routine x-rays
Physicians fail to diagnose vertebral Physicians fail to diagnose vertebral fractures clinicallyfractures clinically Back pain is commonBack pain is common Painful vertebral fractures are Painful vertebral fractures are
not common not common Height and stature are not assessedHeight and stature are not assessed

Symptoms:Symptoms:• Acute and severeAcute and severe• Mid-back Mid-back • Localized Localized • May radiate anteriorlyMay radiate anteriorly
Signs:Signs:• Point tenderness over specific vertebraPoint tenderness over specific vertebra• Tender paravertebral muscles Tender paravertebral muscles • Pain increases with motionPain increases with motion
Distinguishing Vertebral Distinguishing Vertebral Fracture Fracture
From Other Back ProblemsFrom Other Back Problems

Prevalence and Site of Prevalence and Site of Vertebral FractureVertebral Fracture
0
10
20
30
40
T4 T5 T6 T7 T8 T9 T10 T11 T12 L1 L2 L3 L4 L5
0
10
20
30
40
T4 T5 T6 T7 T8 T9 T10 T11 T12 L1 L2 L3 L4 L5
0
10
20
30
40
T4 T5 T6 T7 T8 T9 T10 T11 T12 L1 L2 L3 L4 L5
Japanese in HawaiiJapanese in Hawaii
Japanese in HiroshimaJapanese in Hiroshima
Caucasian in MinnesotaCaucasian in Minnesota
WEDGE
ENDPLATE
CRUSH

Case FindingCase Findingfor Primary Care for Primary Care
PhysiciansPhysicians
ThinnessThinness SmokingSmoking Family historyFamily history History of fracturesHistory of fractures
HistoryHistory Height lossHeight loss KyphosisKyphosis Lateral spine filmLateral spine film Bone densityBone density
ExaminationExamination

Review of Clinical Trials of Review of Clinical Trials of Drugs for Treatment of Drugs for Treatment of
OsteoporosisOsteoporosis Double-blind, placebo-controlledDouble-blind, placebo-controlled Adequate power to detect effectAdequate power to detect effect Fracture endpointFracture endpoint
spine fracturesspine fractures non-spine fracturesnon-spine fractures

Osteoporosis DrugsOsteoporosis Drugs
Calcium with Vitamin DCalcium with Vitamin D Hormone TherapyHormone Therapy RaloxifeneRaloxifene BisphosphonatesBisphosphonates
alendronatealendronate risedronaterisedronate
Parathyroid hormone-teriparatideParathyroid hormone-teriparatide
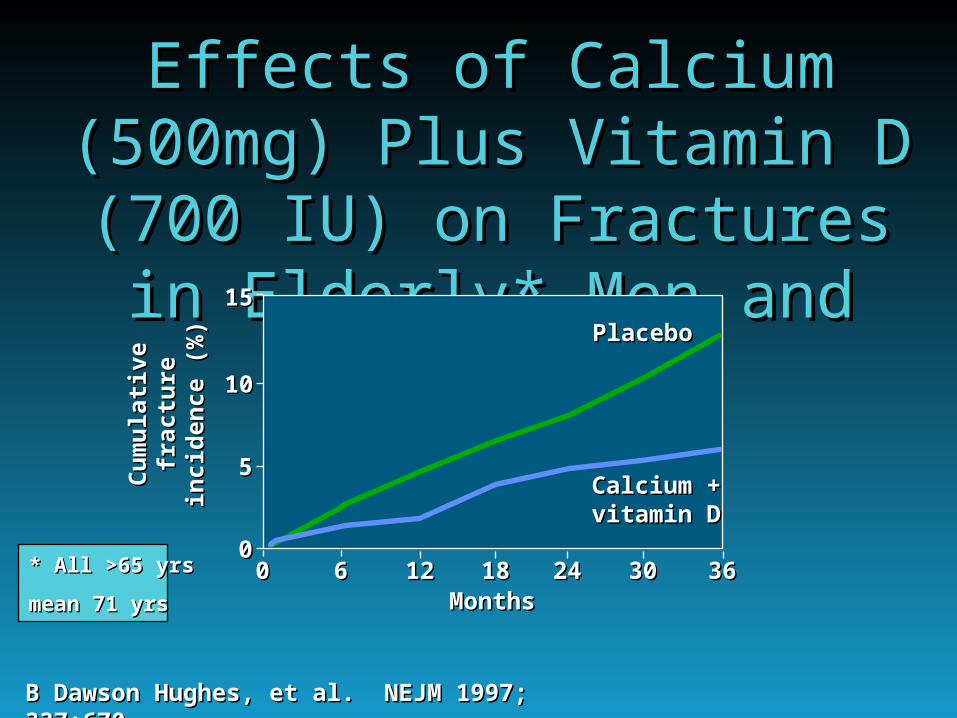
Effects of Calcium (500mg) Effects of Calcium (500mg) Plus Vitamin D (700 IU) on Plus Vitamin D (700 IU) on Fractures in Elderly* Men Fractures in Elderly* Men
and Womenand Women
00 66 1212 1818 2424MonthsMonths
3030 3636
1515
1010
55
00
Calcium +Calcium +vitamin Dvitamin D
PlaceboPlacebo
Cu
mu
lati
veC
um
ula
tive
frac
ture
frac
ture
inci
den
ce (
%)
inci
den
ce (
%)
B Dawson Hughes, et al. NEJM 1997; 337:670B Dawson Hughes, et al. NEJM 1997; 337:670
* * All >65 yrsAll >65 yrs
mean 71 yrsmean 71 yrs

Effects of Vitamin D (800 IU) and Effects of Vitamin D (800 IU) and Calcium (1200 mg) in Elderly* Calcium (1200 mg) in Elderly*
WomenWomen
TreatmentTreatment PlaceboPlacebo % Reduction% Reduction
FracturesFractures n=872n=872 n=893n=893 in riskin risk
HipHip 109109 155155 2929
Non-vertebralNon-vertebral 218218 284284 2424
36 36 Months Follow-upMonths Follow-up
MC Chapuy, et al. NEJM 1992;327:1637MC Chapuy, et al. NEJM 1992;327:1637MC Chapuy, et al. BMJ 1994;308:1081MC Chapuy, et al. BMJ 1994;308:1081
**All in care centersAll in care centers
Mean age 84 yrsMean age 84 yrs

Use Combination of Calcium Use Combination of Calcium and Vitamin D in the Elderlyand Vitamin D in the Elderly
After age 65, calcium intake is low After age 65, calcium intake is low and absorption is inefficient. and absorption is inefficient.
Vitamin D alone does not reduce Vitamin D alone does not reduce fracture risk. * fracture risk. *
Calcium with Vitamin D form the Calcium with Vitamin D form the cornerstone of treatment but may cornerstone of treatment but may not be enough. not be enough.
* * HE Meyer, et al. JBMR 2002;17:709HE Meyer, et al. JBMR 2002;17:709* P Lips, et al. Ann Intern Med 1996;124:400* P Lips, et al. Ann Intern Med 1996;124:400

MORE StudyMORE StudyMMultiple ultiple OOutcomes of utcomes of RRaloxifene aloxifene
EEvaluationvaluation Multicenter, double-blind, placebo-controlled- 4 year studyMulticenter, double-blind, placebo-controlled- 4 year study Raloxifene 60 mg, 120 mg, or placebo (with calcium and Raloxifene 60 mg, 120 mg, or placebo (with calcium and
vitamin D)vitamin D) 7705 women, mean age 67-68 years7705 women, mean age 67-68 years
EndpointsEndpoints Primary: Primary: vertebral fracturevertebral fracture BMD BMD Secondary: Secondary: non-vertebral fracturenon-vertebral fracture, , CVD, breast cancer, uterine safety, CVD, breast cancer, uterine safety, cognitive function cognitive function

Effect of Raloxifene in WomenEffect of Raloxifene in WomenWith or Without Prevalent FracturesWith or Without Prevalent Fractures
Four YearsFour Years
No Prevalent FracturesNo Prevalent Fractures Prevalent FracturesPrevalent Fractures
%
% In
cid
ent
Fra
ctu
reIn
cid
ent
Fra
ctu
re
RR 0.51RR 0.51
RR 0.66RR 0.66
RR 0.62RR 0.62
RR 0.54RR 0.54
00
55
1010
1515
2020
2525
PlaceboPlaceboRLX 60RLX 60RLX120RLX120
K Harper, K Harper, ASBMR,ASBMR, 2000 2000

Efficacy of Raloxifene Through 4 Years
PD Delmas, et al. JCEM 87: 3609-17, 2002PD Delmas, et al. JCEM 87: 3609-17, 2002
Months of ExposureMonths of Exposure00 2424 3636 4848
00
55
1010
1515
Incidence of New Incidence of New Vertebral Fractures Vertebral Fractures
(%)(%) PlaceboPlaceboRLX 60 mg/dRLX 60 mg/d
1212
First Scheduled First Scheduled RadiographRadiograph
P<0.001P<0.001

Design of the Design of the Fracture Fracture
Intervention TrialIntervention Trial
FIT-1FIT-1 FIT-2FIT-2
Follow-up: 4.25 yearsFollow-up: 4.25 yearsFollow-up: 3 yearsFollow-up: 3 years
Vertebral fracture armVertebral fracture arm
n=2027n=2027
Baseline visitsBaseline visits BMDBMD EligibilityEligibility Spinal radiographSpinal radiograph
Clinical Fracture armClinical Fracture arm
n=4432n=4432
DM Black, et al. DM Black, et al. Lancet Lancet 348:1535, 1996348:1535, 1996

Effect of Alendronate* on RiskEffect of Alendronate* on Riskof Vertebral Fracturesof Vertebral Fractures
FIT-1 & FIT-2FIT-1 & FIT-2
DM Black,et al. DM Black,et al. Lancet Lancet 348:1535, 1996348:1535, 1996SR Cummings, et al. SR Cummings, et al. JAMA JAMA 280:2077, 1998280:2077, 1998
No Prevalent FracturesNo Prevalent Fractures Prevalent FracturesPrevalent Fractures
%
% In
cid
ent
Fra
ctu
reIn
cid
ent
Fra
ctu
re
RR 0.56RR 0.56
RR 0.54RR 0.54
00
55
1010
1515
2020
PlaceboPlaceboAlendronateAlendronate
* 5* 5mg/day for 2 yr, mg/day for 2 yr, then 10mg/daythen 10mg/day

VERT StudyVERT Study
5 5 years post-menopausalyears post-menopausal 85 years of age85 years of age Multi-National (n = 1226)Multi-National (n = 1226)**
2 vertebral fractures (T4-L4)2 vertebral fractures (T4-L4) North American (n = 2458)North American (n = 2458)****
2 vertebral fractures (T4-L4), or2 vertebral fractures (T4-L4), or 1 vertebral fracture and lumbar 1 vertebral fracture and lumbar
spine T-score spine T-score -2 -2
Inclusion CriteriaInclusion Criteria
* * J-Y Reginster, et al. J-Y Reginster, et al. Osteopor Int Osteopor Int 11:83, 200011:83, 2000** ** ST Harris, et al. ST Harris, et al. JAMA JAMA 282:1344, 1999282:1344, 1999

Effect of Risedronate on Effect of Risedronate on Incident Vertebral FracturesIncident Vertebral Fractures
VERT - North American VERT - North American VERT - Multi-National VERT - Multi-National
%
% w
tih
fra
ctu
rew
tih
fra
ctu
re
MonthsMonths MonthsMonths
J-Y Reginster et al, Osteopor Int 11:83, 2000J-Y Reginster et al, Osteopor Int 11:83, 2000ST Harris et al, ST Harris et al, JAMAJAMA 282: 1344, 1999 282: 1344, 1999
** 5.0 5.0 mg vs. mg vs. placeboplacebo p < 0.01 p < 0.01
00
55
1010
1515
2020
2525
3030
00 1212 2424 3636
**
**
**
00
55
1010
1515
2020
2525
3030
00 1212 2424 3636
**
**
**
PlaceboPlacebo Risedronate 5 mgRisedronate 5 mg
65% 65%
41% 41% 61% 61%
49% 49%

Secondary Endpoint: Secondary Endpoint: Incident Non-Vertebral Incident Non-Vertebral
FractureFracture
Ascertained by direct questioning Ascertained by direct questioning at each clinic visit at each clinic visit
ExcludedExcluded fractures due to severe traumafractures due to severe trauma finger, toe, face, and skull finger, toe, face, and skull
fracturesfractures pathologic fracturespathologic fractures

Effect of Raloxifene on Effect of Raloxifene on Risk of Risk of
Non-Vertebral FracturesNon-Vertebral FracturesFour YearsFour Years
RR=0.99RR=0.99
RR=0.87RR=0.87
00
22
44
66
88
1010
1212
1414
PlaceboPlacebo RaloxifeneRaloxifene60 mg60 mg
RaloxifeneRaloxifene120 mg120 mg
%
% In
cid
ent
Fra
ctu
reIn
cid
ent
Fra
ctu
re
PD Delmas, et al. JCEM 87: 3609-17, 2002PD Delmas, et al. JCEM 87: 3609-17, 2002

Risk of Nonvertebral* Fracture Risk of Nonvertebral* Fracture in Women With Baseline SQ in Women With Baseline SQ
Grade 3Grade 3MORE Trial - 3 YearsMORE Trial - 3 Years
00
55
1010
1515
2020
% % with with 1 1 non-vertebral fracturenon-vertebral fracture
RH = 0.53RH = 0.53 ( 0.29-0.99)( 0.29-0.99)
PlaceboPlacebo Raloxifene 60 mg/dRaloxifene 60 mg/d
* * Clavicle, humerus, wrist, pelvis, hip, legClavicle, humerus, wrist, pelvis, hip, leg
P Delmas, et al. Osteoporosis Int, 2002, Suppl.1 (presented at IOF)P Delmas, et al. Osteoporosis Int, 2002, Suppl.1 (presented at IOF)

Effect of Alendronate on Effect of Alendronate on RiskRisk of Non-vertebral Fracturesof Non-vertebral Fractures
FIT-1 plus selected FIT-2FIT-1 plus selected FIT-2
00 66 1212 1818 2424 3030 3636
1616
1010
66
00
MonthsMonths
AlendronateAlendronate
%
% In
cid
ent
Fra
ctu
reIn
cid
ent
Fra
ctu
re PlaceboPlacebo
D Black, et al. D Black, et al. JCEMJCEM 85:4118, 2000 85:4118, 2000
44
88
1212
1414
22
27%27%

Alendronate Fracture Risk Alendronate Fracture Risk ReductionReduction
Depends on Degree of Depends on Degree of OsteoporosisOsteoporosis
Relative risk vs. placeboRelative risk vs. placebo
Femoral Neck t-score Vert. Fx Clinical FxFemoral Neck t-score Vert. Fx Clinical Fx -1.6 to - 2.0 -1.6 to - 2.0 0.80.8 1.11.1 -2.5 to - 2.0-2.5 to - 2.0 0.50.5 1.01.0 below - 2.5below - 2.5 0.50.5 0.60.6
FIT-2FIT-2
SR Cummings, et al. SR Cummings, et al. JAMA JAMA 280:2077, 1998 280:2077, 1998

Effect of Risedronate on Risk Effect of Risedronate on Risk of of
Non-Vertebral Fractures Non-Vertebral Fractures
MonthsMonths MonthsMonths
00
55
1010
1515
2020
00 1212 2424 363600
55
1010
1515
2020
00 1212 2424 3636
North American North American Multi-National Multi-National
%
% w
ith
Fra
ctu
rew
ith
Fra
ctu
re
Harris et. al. Harris et. al. JAMA.JAMA. 1999;282(14):1344-52. 1999;282(14):1344-52. Reginster et al. Reginster et al. Osteoporos IntOsteoporos Int. 2000;11:83-91.. 2000;11:83-91.
PlaceboPlacebo Risedronate 5 mgRisedronate 5 mg

Effect of Risedronate Effect of Risedronate on Incidence of Hip Fractureon Incidence of Hip Fracture
39%39%
%
% w
ith
fra
ctu
rew
ith
fra
ctu
re
PlaceboPlacebo
RisedronateRisedronate
00
11
22
33
44
55
66
00 66 1212 1818 2424 3030 3636
MonthsMonths
Low Bone Density Group (Group 1)Low Bone Density Group (Group 1)
MR McClung, et al. MR McClung, et al. NEJMNEJM 344:333, 2001 344:333, 2001

Risedronate May Not Reduce Hip Fracture Risedronate May Not Reduce Hip Fracture
Risk in Non-Osteoporotic WomenRisk in Non-Osteoporotic Women
Risk Reduction Risk Reduction Cohort Cohort Hip Fracture Hip Fracture 70-79 years with70-79 years with t-score <3.0 t-score <3.0 39% 39% 80+ years80+ years
allall 18% 18% t-score <2.5t-score <2.5 26% 26%
M McClung, et al. NEJM 344:333, 2001M McClung, et al. NEJM 344:333, 2001

Fracture Risk Reductions Fracture Risk Reductions Observed Observed
in Trials of Anti-resorptive in Trials of Anti-resorptive TherapiesTherapies
SpineSpine
3 yr 1 yr3 yr 1 yr
45% 60%45% 60%
43% 68%*43% 68%*
45% 63%45% 63%
AlendronateAlendronate
RaloxifeneRaloxifene
RisedronateRisedronate
Non-SpineNon-Spine
3 yr 3 yr
12, 22, 27%12, 22, 27%
12, 48%12, 48%
12, 33, 18, 39%12, 33, 18, 39%
* * M Maricic, et al. Arch Intern Med 162:1140-1143, 2002M Maricic, et al. Arch Intern Med 162:1140-1143, 2002

EEvista vista VVersus ersus AAlendronatelendronate
EVAEVA Outcome- any osteoporotic Outcome- any osteoporotic
fracturefracture 3000 osteoporotic women3000 osteoporotic women
(hip t-score -2.5 to - 4.0) (hip t-score -2.5 to - 4.0) Start 2002, Finish 2007Start 2002, Finish 2007

CASE 1CASE 1
50 50 year-old womanyear-old woman Natural menopause 2 years agoNatural menopause 2 years ago Vasomotor symptomsVasomotor symptoms Bone density: t-score -1.6Bone density: t-score -1.6 Tried HRT but stopped due to Tried HRT but stopped due to
breast tenderness and bloatingbreast tenderness and bloating
Not a candidate for raloxifene or alendronateNot a candidate for raloxifene or alendronate

CASE 2CASE 2
65 65 year-old womenyear-old women Concerned about memoryConcerned about memory No menopausal symptomsNo menopausal symptoms Wrist fracture 3 years agoWrist fracture 3 years ago Bone density: t-score -3.0Bone density: t-score -3.0
High risk of fracture- requires treatmentHigh risk of fracture- requires treatment

Rationale for Raloxifene Use for Rationale for Raloxifene Use for Postmenopausal Women with Postmenopausal Women with
OsteoporosisOsteoporosis
To reduce risk of osteoporotic fractureTo reduce risk of osteoporotic fracture To reduce the risk of breast cancerTo reduce the risk of breast cancer To reduce risk of CHDTo reduce risk of CHD To prevent cognitive declineTo prevent cognitive decline Long-term safety and acceptanceLong-term safety and acceptance

CASE 3CASE 3
75 75 year-old womanyear-old woman prior wrist fractureprior wrist fracture presents with a painful L-1 crush presents with a painful L-1 crush
fracturefracture X-ray shows wedging T-7 and T-8X-ray shows wedging T-7 and T-8 Bone density t-score -3.5Bone density t-score -3.5
Needs strong, rapidly acting osteoporosis drugNeeds strong, rapidly acting osteoporosis drug
Antiresorptive Drugs Increase Antiresorptive Drugs Increase BMD but Not Bone VolumeBMD but Not Bone Volume
• Early BMD increase is due to filling in of remodelling Early BMD increase is due to filling in of remodelling (resorption) space(resorption) space
• Later BMD increase is due to increased mineralization Later BMD increase is due to increased mineralization of BMUof BMU
• Most of BMD effect can be explained by mineralizationMost of BMD effect can be explained by mineralization
GY Boivin, et al. Bone 27:687-694, 2000GY Boivin, et al. Bone 27:687-694, 2000CJ Hernandez, et al. Bone 29:511-516, 2001CJ Hernandez, et al. Bone 29:511-516, 2001

Excessive Suppression of Bone TurnoverExcessive Suppression of Bone Turnover
ProlongedProlongedMineralizationMineralization
Insufficient RepairInsufficient Repairof Microdamageof Microdamage
Damage AccumulationDamage Accumulation
Decrease in Bone ToughnessDecrease in Bone Toughness
Long-term Safety?Long-term Safety?
Relationship Between Excessive Suppression Of Bone Turnover and Damage Accumulation

Hypothetical Effects of Hypothetical Effects of Increasing Bone Mineralization Increasing Bone Mineralization
DisplacementDisplacementCH Turner Osteoporos Int 13:97-104, 2002CH Turner Osteoporos Int 13:97-104, 2002
ForceForce
OptimumOptimum
Hypo-mineralizedHypo-mineralized
Hyper-mineralizedHyper-mineralizedxx
xx
xx

Hypothetical Effects of Hypothetical Effects of Increasing Bone Mineralization Increasing Bone Mineralization
Percentage MineralizationPercentage Mineralization
ResistanceResistance to fracture to fracture forcesforces
Improved resistance to Improved resistance to bending = stiffnessbending = stiffness
Increasing brittlenessIncreasing brittleness

Safety Concerns Safety Concerns RegardingRegarding
Long-term AlendronateLong-term Alendronate Rate of clinical spine fractures during Rate of clinical spine fractures during
years 5-7 was 3 times higher years 5-7 was 3 times higher than during years 1-3than during years 1-3
Height loss (1.2mm/yr) during Height loss (1.2mm/yr) during years 5-7 tended to be higheryears 5-7 tended to be higherthan during years 1-3 (1.0mm/yr)than during years 1-3 (1.0mm/yr)
RP Tonino, et al. JCEM 85:3109, 2000RP Tonino, et al. JCEM 85:3109, 2000

Eff
icac
yE
ffic
acy
TimeTime00
Drug ADrug A
Drug BDrug B
Concept of Sustained vs. Concept of Sustained vs. Unsustained EfficacyUnsustained Efficacy

For Severe Osteoporosis:For Severe Osteoporosis:Prescribe SequentiallyPrescribe Sequentially
Short-termShort-term “quick-fix” with a strong “quick-fix” with a strong bone-specific agentbone-specific agent
Long-termLong-term bone maintenance with bone maintenance with a milder (and safer) effect:a milder (and safer) effect: multipurpose drug - raloxifenemultipurpose drug - raloxifene

Key Messages for Key Messages for Primary Care PhysiciansPrimary Care Physicians
Osteoporosis is frequently overlookedOsteoporosis is frequently overlooked Osteoporosis is treatableOsteoporosis is treatable Drug treatment should be encouraged Drug treatment should be encouraged
for those at highest risk for those at highest risk