powerpoint presentations2.q4cdn.com/772010778/files/doc_presentations/2015/trillium... ·...
TRANSCRIPT
Q4/2015
This presentation may contain forward-looking statements, which reflect Trillium's current expectation regarding future
events. These forward-looking statements involve risks and uncertainties that may cause actual results, events or
developments to be materially different from any future results, events or developments expressed or implied by such
forward-looking statements. Such factors include, but are not limited to, Trillium's ability to obtain financing to advance
the products in its development portfolio; changing market conditions; the successful and timely completion of pre-
clinical and clinical studies; the establishment of corporate alliances; the impact of competitive products and pricing;
new product development risks; uncertainties related to the regulatory approval process or the ability to obtain drug
product in sufficient quantity or at standards acceptable to health regulatory authorities to complete clinical trials or to
meet commercial demand; and other risks detailed from time to time in Trillium's ongoing quarterly and annual
reporting. Forward-looking statements are made only as of the date of this presentation and except as required by
applicable securities laws, Trillium undertakes no obligation to publicly update or revise any forward-looking statements,
whether as a result of new information, future events or otherwise.
2

Investment Highlights
3
Immuno-oncology company developing a next generation immune checkpoint inhibitor
Lead program SIRPαFc targets CD47, a “do not eat” signal tumor cells exploit to escape destruction by the innate immune system
Raised ~$85M (Since 12/2013) from premier US healthcare funds to support clinical development
IND filed in Q3/15
Listed on NASDAQ as “TRIL” in December 2014 (listed on TSX as “TR”)

Experienced Leadership & Veteran Board of Directors
4
Executive Title Joined Trillium
Dr. Niclas Stiernholm President & Chief Executive Officer 2002
Dr. Robert Uger Chief Scientific Officer 2003
Dr. Eric Sievers Chief Medical Officer 2015
Dr. Penka Petrova Chief Development Officer 2003
Mr. James Parsons Chief Financial Officer 2003
Ms. Elizabeth Wieland Senior Director, Clinical Operations 2015
MANAGEMENT
BOARD OF DIRECTORS
Executive Affiliation
Dr. Calvin Stiller, Chair Chair
Dr. Henry Friesen Chair (former)
Dr. Niclas Stiernholm CEO
Dr. Michael Moore CEO (former)
Executive Affiliation
Dr. Robert Kirkman CEO
Dr. Thomas Reynolds CMO (former)
Mr. Luke Beshar CFO (former)
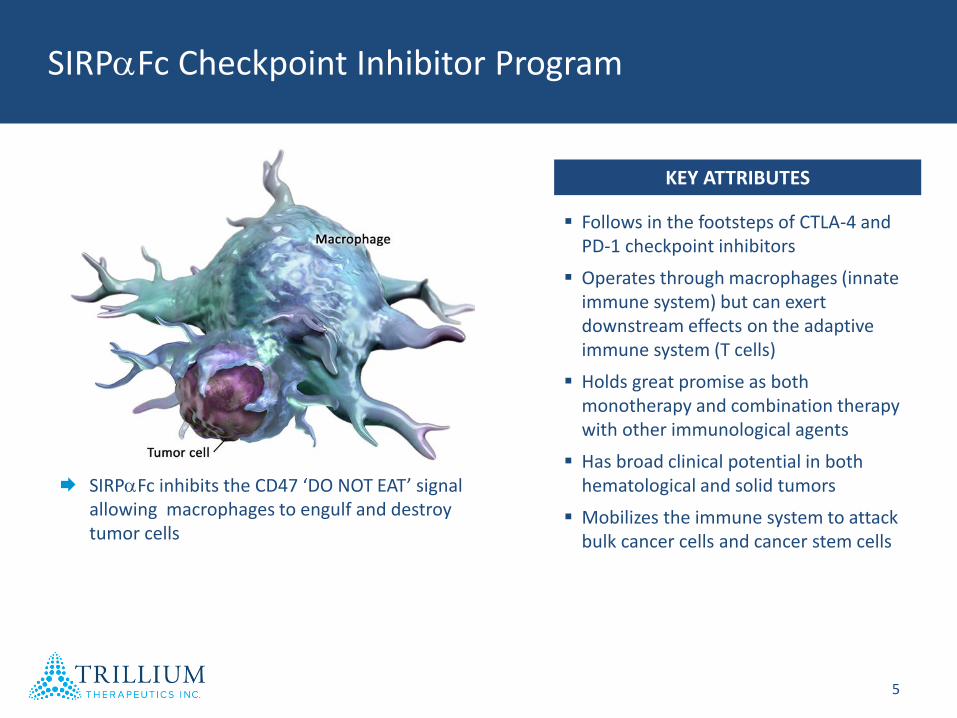
SIRPaFc Checkpoint Inhibitor Program
5
SIRPaFc inhibits the CD47 ‘DO NOT EAT’ signal allowing macrophages to engulf and destroy tumor cells
Follows in the footsteps of CTLA-4 and PD-1 checkpoint inhibitors
Operates through macrophages (innate immune system) but can exert downstream effects on the adaptive immune system (T cells)
Holds great promise as both monotherapy and combination therapy with other immunological agents
Has broad clinical potential in both hematological and solid tumors
Mobilizes the immune system to attack bulk cancer cells and cancer stem cells
KEY ATTRIBUTES

Key Event Timing
File IND Q3’2015
Initiate Phase I Q4’2015
SIRPaFc Development Strategy
6
AML/MDS
CLL
CML
DLBCL
POTENTIAL ADDITIONAL INDICATIONS
Liquid Tumors
Bladder
Brain
Breast
Colon
Leiomyosarcoma
Solid Tumors
Follicular lymphoma
Mantle cell lymphoma
Multiple myeloma
Liver
Melanoma
Ovarian
Prostate
Renal
Advanced hematologic malignancies in Phase I . . . With broad clinical potential
First indication: lymphoma
Preclinical data in additional indications Q4’2015
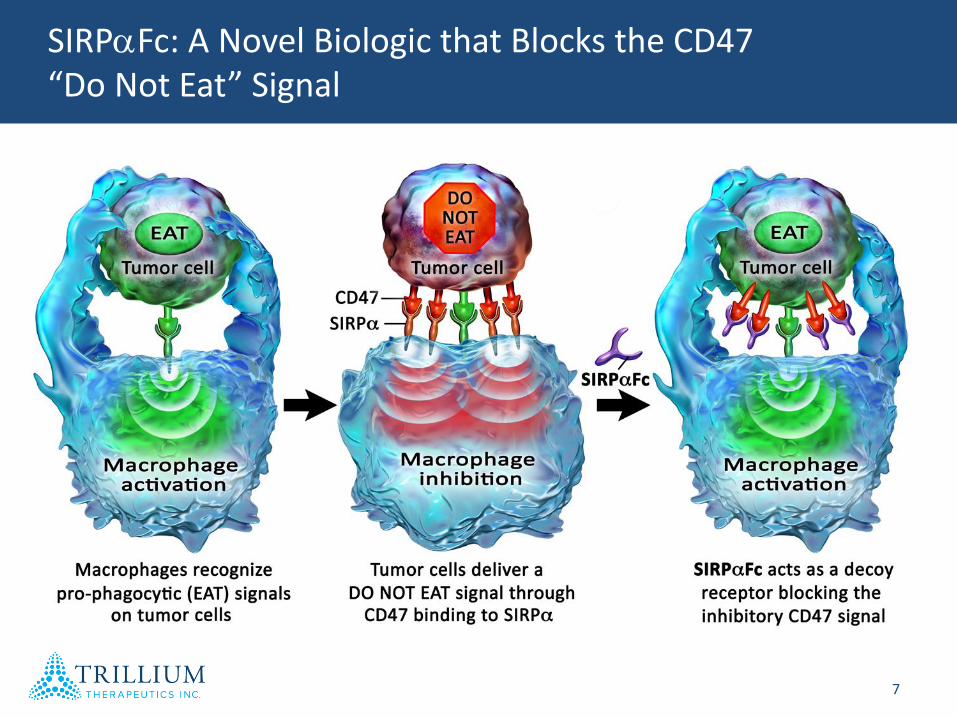
SIRPaFc: A Novel Biologic that Blocks the CD47 “Do Not Eat” Signal
7
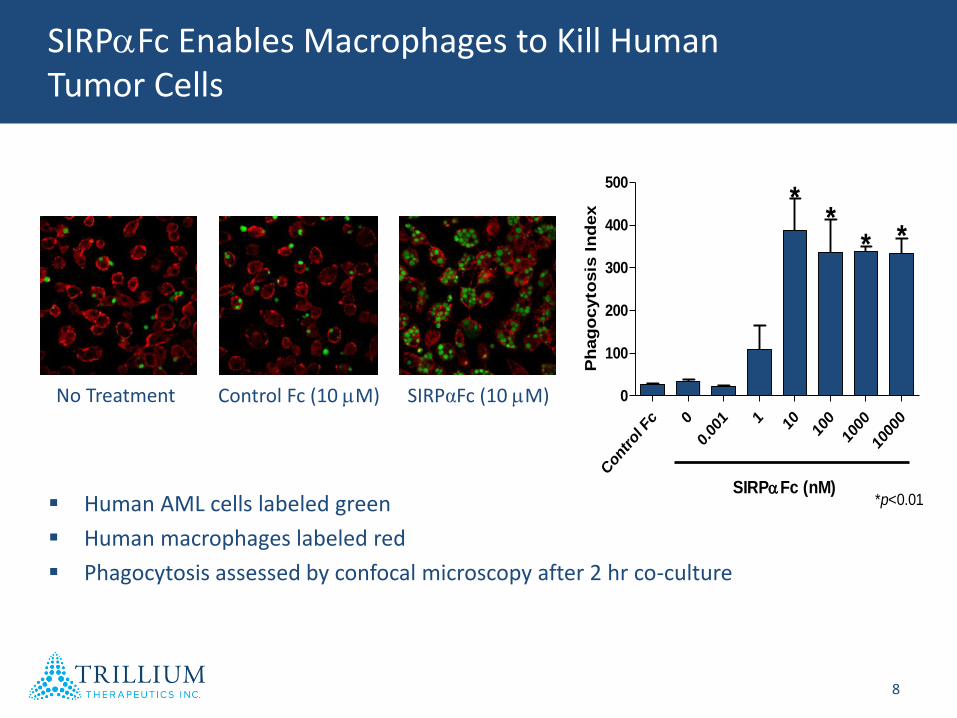
SIRPaFc Enables Macrophages to Kill Human Tumor Cells
8
No Treatment Control Fc (10 mM) SIRPαFc (10 mM)
Human AML cells labeled green
Human macrophages labeled red
Phagocytosis assessed by confocal microscopy after 2 hr co-culture
CD47 Exp 377
Con
trol
Fc 0
0.00
1 1 10 100
1000
1000
0
0
100
200
300
400
500
SIRPaFc (nM)
***
*
*p<0.01
Ph
ag
ocyto
sis
In
dex
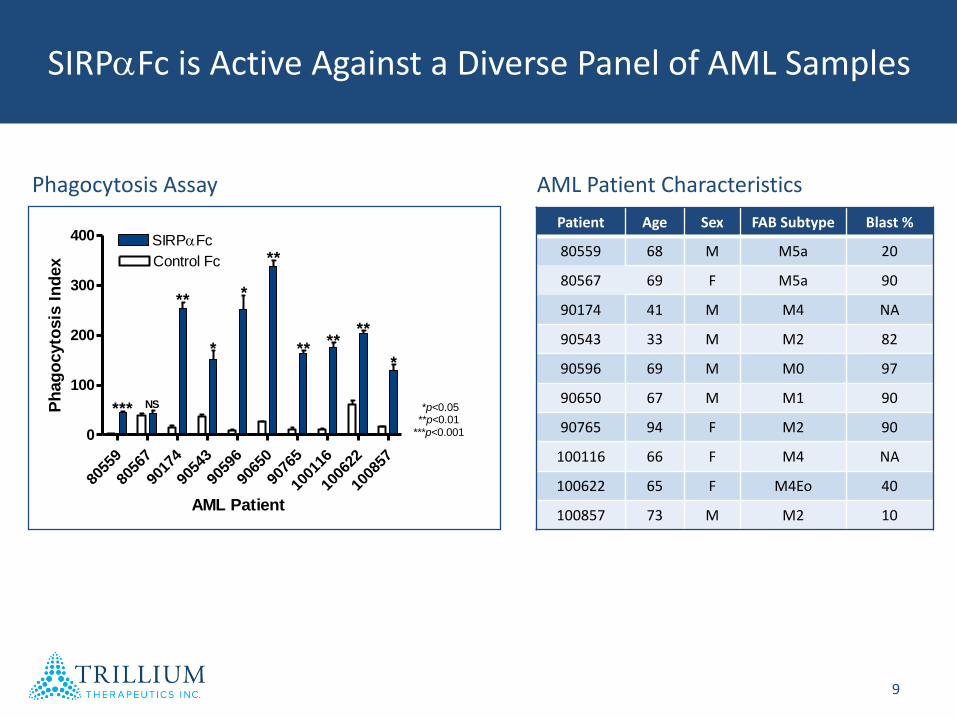
SIRPaFc is Active Against a Diverse Panel of AML Samples
9
8055
9
8056
7
9017
4
9054
3
9059
6
9065
0
9076
5
1001
16
1006
22
1008
57
0
100
200
300
400
Control Fc
SIRPaFc
*** NS
**
**
****
**
**
*
*p<0.05**p<0.01
***p<0.001
AML Patient
Ph
ag
ocyto
sis
In
dex
Patient Age Sex FAB Subtype Blast %
80559 68 M M5a 20
80567 69 F M5a 90
90174 41 M M4 NA
90543 33 M M2 82
90596 69 M M0 97
90650 67 M M1 90
90765 94 F M2 90
100116 66 F M4 NA
100622 65 F M4Eo 40
100857 73 M M2 10
Phagocytosis Assay AML Patient Characteristics
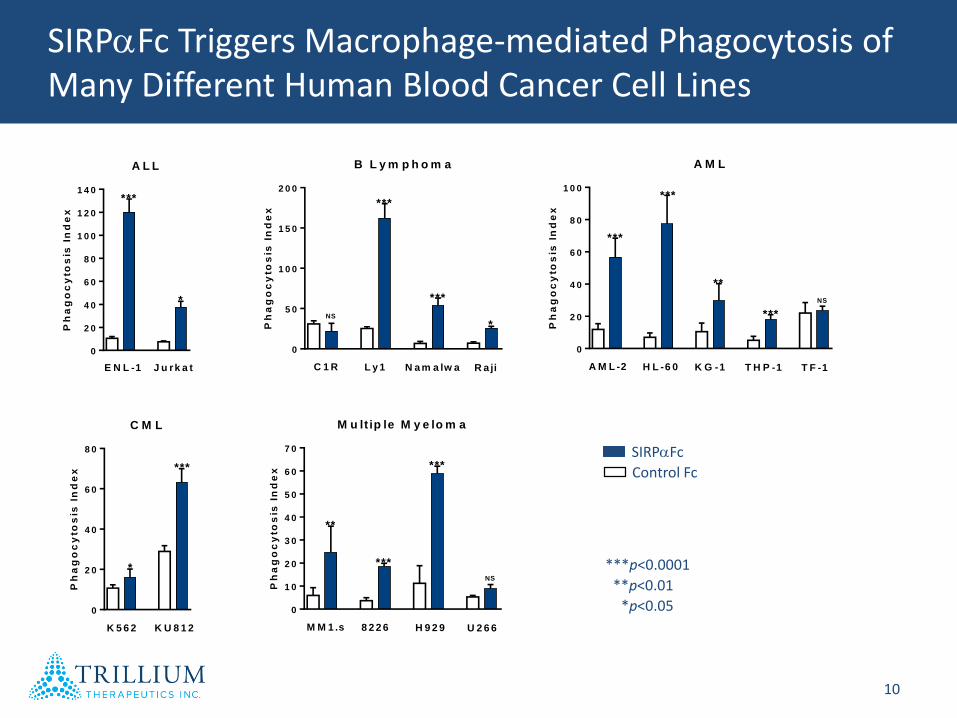
SIRPaFc Triggers Macrophage-mediated Phagocytosis of Many Different Human Blood Cancer Cell Lines
10
0
2 0
4 0
6 0
8 0
1 0 0
A M L
Ph
ag
oc
yto
sis
In
de
x
A M L -2 H L -6 0 K G -1 T H P -1 T F -1
***
***
**
***
NS
0
5 0
1 0 0
1 5 0
2 0 0
B L y m p h o m a
Ph
ag
oc
yto
sis
In
de
x
C 1 R L y 1 N a m a lw a R a ji
***
***
*NS
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
M u lt ip le M y e lo m a
Ph
ag
oc
yto
sis
In
de
x
M M 1 .s 8 2 2 6 H 9 2 9 U 2 6 6
***
***
NS
**
0
2 0
4 0
6 0
8 0
C M L
Ph
ag
oc
yto
sis
In
de
x
K 5 6 2 K U 8 1 2
***
*
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
A L L
Ph
ag
oc
yto
sis
In
de
x
E N L -1 J u rk a t
***
*
SIRPaFc
Control Fc
***p<0.0001
**p<0.01
*p<0.05

SIRPaFc Induces Tumor Cell-Specific Phagocytosis
11
CD47 Exp 381
0
50
100
150
200
250
300
Control Fc
SIRPaFc
AML cells Normal monocytes
*
Ph
ag
ocyto
sis
In
dex
AML + SIRPαFc Normal cells + SIRPαFc
Results consistent with a model in which CD47 blockade enables macrophages to kill only target cells that express pro-phagocytic signals (i.e, tumor cells)

Evaluating SIRPaFc Efficacy In Vivo
12
AML cells from cancer patient
NOD.SCID mouse
Intrafemoral
injection
SIRPαFc
treatment
Measure leukemia by flow cytometry
Isolate bone marrow & spleen
Xenografts in NOD.SCID mice: the “gold standard” model in AML
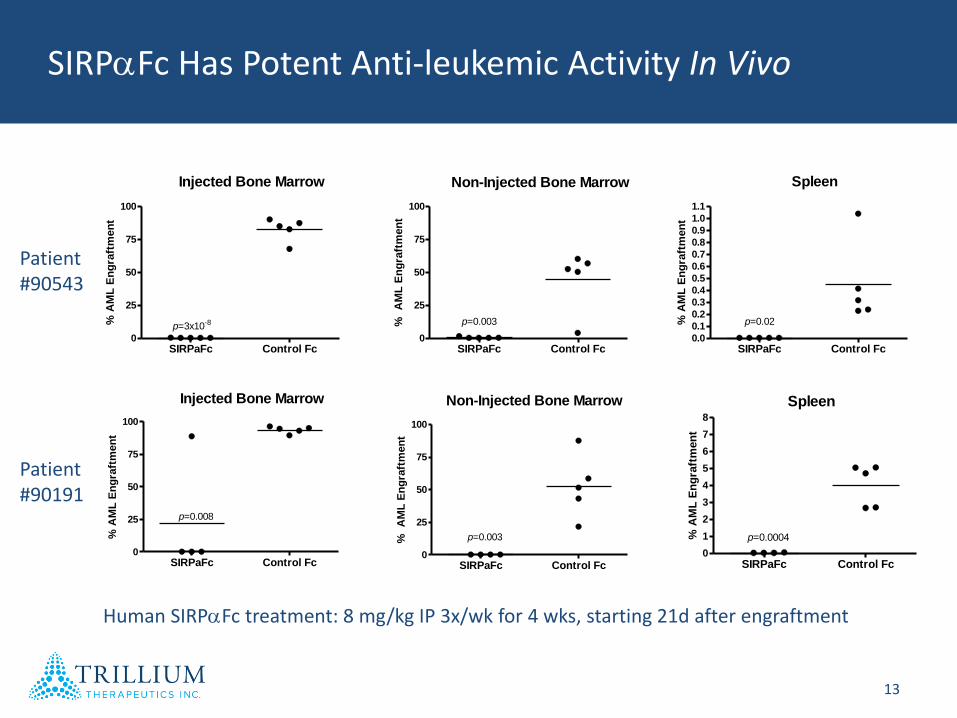
SIRPaFc Has Potent Anti-leukemic Activity In Vivo
13
SIRPaFc Control Fc0
25
50
75
100
p=3x10-8
Injected Bone Marrow
% A
ML
En
gra
ftm
en
t
SIRPaFc Control Fc0
25
50
75
100
p=0.003
Non-Injected Bone Marrow
%
AM
L E
ng
raft
men
t
SIRPaFc Control Fc0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
Spleen
p=0.02% A
ML
En
gra
ftm
en
t
SIRPaFc Control Fc0
25
50
75
100
p=0.008
Injected Bone Marrow
% A
ML
En
gra
ftm
en
t
SIRPaFc Control Fc0
25
50
75
100
p=0.003
Non-Injected Bone Marrow%
A
ML
En
gra
ftm
en
t
SIRPaFc Control Fc0
1
2
3
4
5
6
7
8
Spleen
p=0.0004% A
ML
En
gra
ftm
en
t
Patient#90543
Patient#90191
Human SIRPaFc treatment: 8 mg/kg IP 3x/wk for 4 wks, starting 21d after engraftment
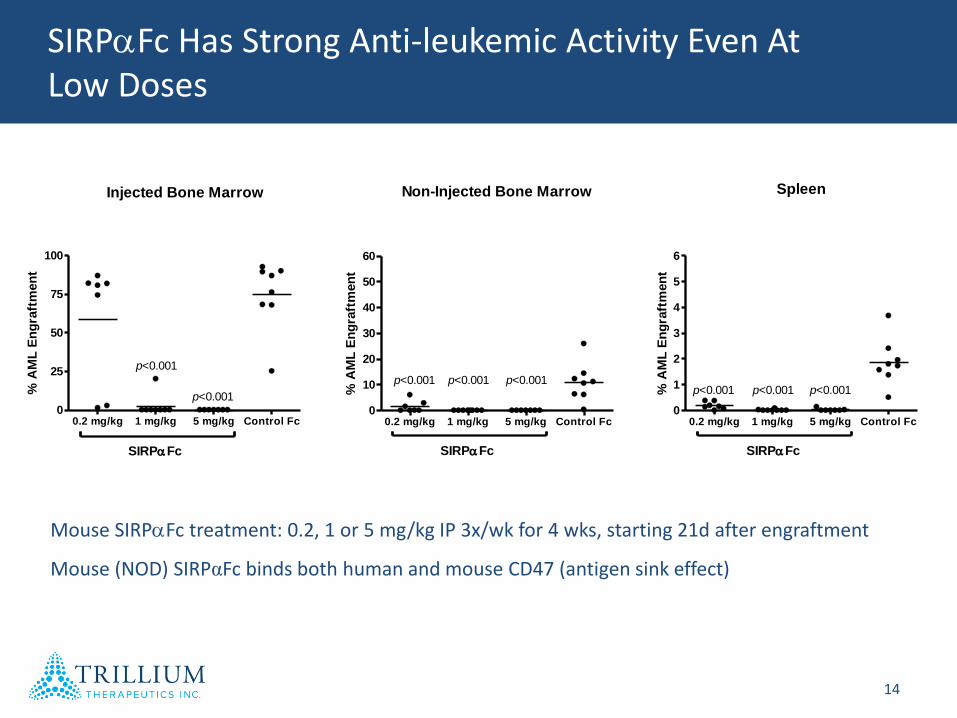
SIRPaFc Has Strong Anti-leukemic Activity Even At Low Doses
14
Injected Bone Marrow
0.2 mg/kg 1 mg/kg 5 mg/kg Control Fc0
25
50
75
100
SIRPaFc
p<0.001
p<0.001
% A
ML
En
gra
ftm
en
t
Non-Injected Bone Marrow
0.2 mg/kg 1 mg/kg 5 mg/kg Control Fc0
10
20
30
40
50
60
SIRPaFc
p<0.001 p<0.001p<0.001
% A
ML
En
gra
ftm
en
t
Spleen
0.2 mg/kg 1 mg/kg 5 mg/kg Control Fc0
1
2
3
4
5
6
SIRPaFc
p<0.001 p<0.001p<0.001% A
ML
En
gra
ftm
en
t
Mouse (NOD) SIRPαFc binds both human and mouse CD47 (antigen sink effect)
Mouse SIRPaFc treatment: 0.2, 1 or 5 mg/kg IP 3x/wk for 4 wks, starting 21d after engraftment
A Second Clinical Pathway: SIRPaFc Combination Therapy
SIRPαFc-mediated enhancement of innate immunity could be synergistic with other immune therapies, such as:
Approved cancer antibodies (e.g., Rituxan®)
T cell checkpoint inhibitors (e.g., anti-PD-1)
Cancer vaccines
Oncolytic viruses
CAR T cells
Preliminary evidence suggests that CD47 blockade can enhance the potency of anti-cancer antibodies and promote T cell responses
We are evaluating SIRPαFc in preclinical combination studies
15
Competition
Trillium is the only group developing a SIRPαFc fusion protein and has developed IP around this approach
Three others are pursuing anti-CD47 antibodies:
Stanford, through a non-commercial entity (CIRM grant)
Celgene (licensed from Inhibrx)
Novimmune (bispecific anti-CD47/anti-CD19 antibody)
Trillium’s SIRPαFc has much lower binding to human RBCs compared to anti-CD47 mAbs – potential best in class through:
Lower hemotoxicity
More favorable PK (no RBC “antigen sink”)
16

SIRPaFc Has a Favorable Low Binding Profile to Human RBCs Compared to CD47 Antibodies
17
Binding of SIRPαFc and anti-CD47 mAbs to human RBCs (n=43 donors)
SIR
PaF
c
Fc co
ntrol
BRIC
126
2D3
CC2C
6
B6H
12 5F9
mIg
G1
mIg
G2b
100
101
102
103
104
105
106
CD47 mAbs mAb
Controls
Mean
F
luo
rescen
ce I
nte
nsit
y
Donor Characteristics (n=43)Male (n=32)Female (n=11)Type A blood group (n=11)Type B blood group (n=13)Type AB blood group (n=5)Type O blood group (n=14)Rh+ blood group (n=20)Rh- blood group (n=13)
2015 Milestones
Pre-IND meeting with the FDA – Q1’15
Initiate GLP toxicology studies – Q1’15
AACR presentation – Q2’15
Production and release of bulk GMP lot – Q2’15
IND filing – Q3’15
Preclinical data supporting additional clinical indications – Q4’15
Initiate Phase I trial – Q4’15
18
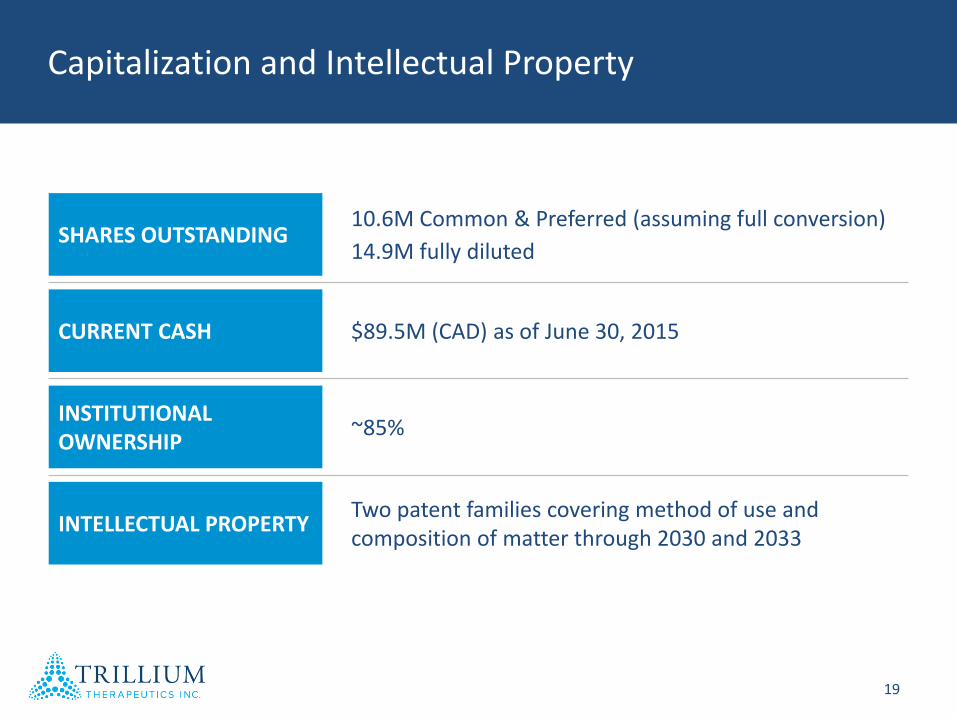
SHARES OUTSTANDING10.6M Common & Preferred (assuming full conversion)
14.9M fully diluted
CURRENT CASH $89.5M (CAD) as of June 30, 2015
INSTITUTIONAL OWNERSHIP
~85%
INTELLECTUAL PROPERTYTwo patent families covering method of use and composition of matter through 2030 and 2033
Capitalization and Intellectual Property
19

Trillium Therapeutics Inc. (NASDAQ:TRIL/TSX:TR) is an immuno-oncology company dedicated to the discovery and
development of novel and innovative cancer therapies.