practical application of pbpk in neonates and infants ... · shi, d., et al. surged expression of...
TRANSCRIPT

Practical Application of PBPK in Neonates and Infants, Including Case Studies
Neil Parrott - 5 May 2014
Presented at the conference : Innovative Approaches to Pediatric Drug Development and Pediatric Medical Countermeasures: A Role for Physiologically-Based PK?

Physiologically based pharmacokinetic model use at Roche
Post-doc. research Pre-clinical group in discovery
M&S expert group + DMPK + formulation
M&S expert group + DMPK +Formulation + Clinical Pharmacology
Training
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
• PBPK modelling now applied routinely during small molecule development
• When PBPK sufficiently verified in adults, pediatric-PBPK is method of choice for PK prediction & dose setting in children
• Pediatric-PBPK is applied in many development projects Ph 2 to aid internal decisions as well as for PIP and PSP
• Allows us to leverage PK knowledge gained in adults and growing physiological knowledge on ontogeny of PK processes

Physiologically based pharmacokinetic models for neonates and infants
• Profound changes in PK processes in infants and neonates make PBPK particularly beneficial for this age group
• However, sparse data and many gaps in our knowledge of this population, especially oral drug absorption including intestinal UGT’s & transporters
Kearns N Engl J Med. 2003
Salem, Johnson, et al. Clin Pharmacokinet. 2014
Mooij, de Wildt et al Expert Opin. Drug Metab. Toxicol. 2012
birth 1 yr

4
Case Study : Oseltamivir use in infants
• Approved for oral treatment of influenza and for prophylaxis in adults and children ≥1 year of age
• In the light of the pandemic, several Health Authorities (e.g. FDA, EMEA, Australia, Canada) issued compassionate use authorization in children <1 of age for oral and > 1 year of age for IV route
• In communications with EMA the agency indicated – For IV registration in the EU-label and IV compassionate use in children <1 year of age
additional pre-clinical data are needed
EMEA requested a repeated dose IV toxicology study in juvenile marmosets
Background

5
Toxicity studies to support IV use in children <1 year
Juvenile studies (n=8) – Single oral dose in rats (PND 7, 14, 24 and 42) – 14-day oral repeat dose in rats (PND 7-21 and 21-49) – Single SC dose in rats (active metabolite; PND 7)
General toxicity studies i.v. – 14-day rat and marmoset (pro-drug & active metabolite adult animals) – Safety Pharmacology (IRWIN mouse and CV dog)
General toxicity studies oral – Single and repeat-dose toxicity in rats (27 wk) and marmoset (39 wk) – Special studies (incl. Safety Pharm.) in mice, rats, guinea pig, rabbit and dog – Reproductive toxicity studies in rats and rabbits – Carcinogenicity studies in mice, rats and transgenic mice
What was available ?
Clinical: Ongoing NIH trial in children <1 year (oral) and IV Compassionate Use in EU

6
Data to support IV use in children
• No pre-clinical juvenile studies by the intravenous route
What is missing?
What do we have to add?
Hardly feasible ?
Ethically justified ?
EMEA request:
repeated dose IV toxicity
in 3 day old marmosets
An alternative?
Building the bridge with M&S • Oral to IV
• Adult to juvenile
• Animal to human
SDPK IV in adult and newborn marmosets

PBPK is optimal method for species scaling of PK
7 PREDICTION ACCURACY ~ 75%, n=34
0.1
1
10
100
1000
10000
100000
1000000
0.1 1
10
10
0
10
00
10
00
0
10
00
00
10
00
00
0
Observed AUC (hr*ug/L)
Pre
dic
ted
AU
C (
hr*
ug
/L)
8
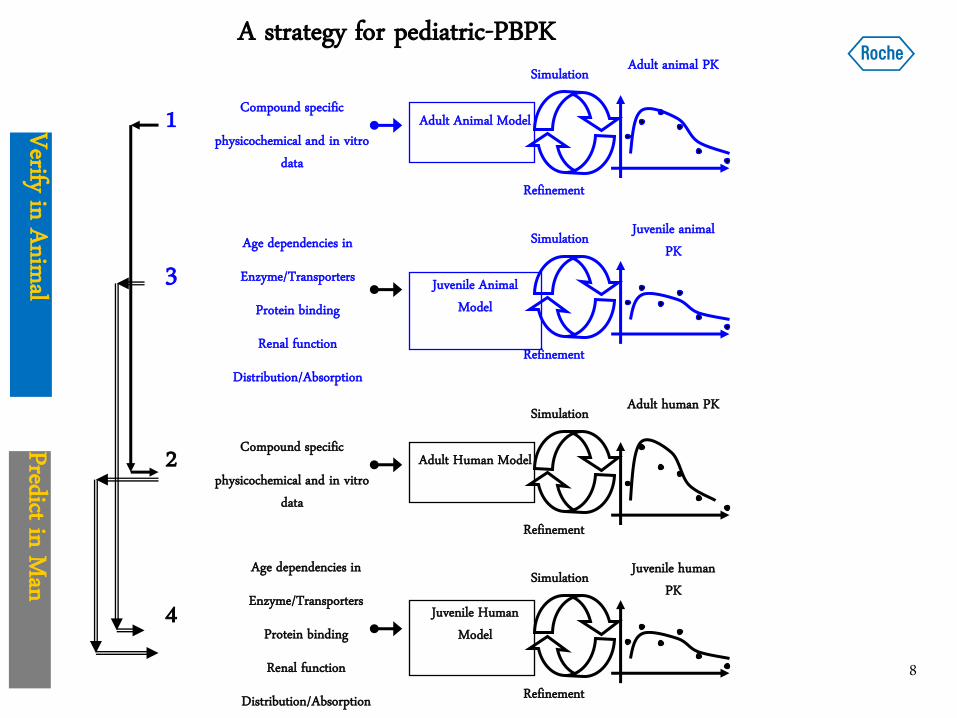
Compound specific
physicochemical and in vitro data
1 Adult Animal Model
Refinement
Simulation Adult animal PK
Age dependencies in
Enzyme/Transporters
Protein binding
Renal function
Distribution/Absorption
3 Juvenile Animal Model
Refinement
Simulation Juvenile animal PK
Compound specific
physicochemical and in vitro data
2 Adult Human Model
Refinement
Simulation Adult human PK
Age dependencies in
Enzyme/Transporters
Protein binding
Renal function
Distribution/Absorption
4 Juvenile Human Model
Refinement
Simulation Juvenile human PK
A strategy for pediatric-PBPK
Verify in Animal Predict in Man

9
oseltamivir carboxylate (OC)
Log D = -2.25
Base 8.2, Acid 3.6
very low permeability
oseltamivir (Os)
Log D = 0.36
Base 7.7
good permeability
Physicochemical & in vitro properties
carboxylesterase
Conversion of pro-drug in liver in both monkey and human
active metabolite pro-drug

10
PBPK models for pro-drug and metabolite run in parallel
Renal elimination
of OC
Renal elimination
of Os
HA = Hepatic Artery
LU = Lung
ART = Arterial Supply
VEN = Venous Return
AD = Adipose
MU = Muscle
LI = Liver
ACAT = Gut
SP = Spleen
HE = Heart
BR = Brain
KI = Kidney
SK = Skin
REP = Repro Organs
REDM = Red Marrow YELM = Yellow Marrow
ROB = Rest Of Body
oseltamivir oseltamivir carboxylate
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
Model for OModel for OC
Conversion of
O to OC in
liver
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
LU
SP ART
LI
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
Model for OModel for OC
Conversion of
O to OC in
liver
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
Model for OModel for OC
Conversion of
O to OC in
liver
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
LU
SP ART
LI
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
LU
SP ART
LI
ACAT
AD
HE
KI
MU
BR
SKREP
YELMREDM
ROB
VEN
HA
Model for OModel for OC
Conversion of
O to OC in
liver

11
PBPK model refinement in the monkey
• Metabolism scaling from in vitro verified in monkey
• Liver disposition for poorly permeable OC verified in monkey
OC
O
PBPK Liver model for Os PBPK Liver model for OC
Intracellular space Intracellular space
Extracellular space Extracellular space
Conversion
scaled from
in vitro
O O O O O
O O O O O O crosses cellular
membrane easily but once
converted to OC exit is
permeability limited
Permeability barrier
no barrier
to diffusion
Model verification in the animal is an essential step in PBPK

12
PBPK model refinement in the monkey
Model verification in the animal is an essential step in PBPK
1. Model verification for OC dosed IV refinement of renal CL
2. Addition of conversion of Os->OC & simulation
3. Refinement of Os->OC conversion
4. Refinement of OC release from liver
1.
2. 3 & 4

13
Simulations in adult human
15 mg infused over 1 hour
1
10
100
1000
0 6 12 18 24
Plasma Conc. (ng/mL)
Tim
e (
hrs
)
OC
Os 1
10
100
1000
10000
0 2 4 6 8
Time (hrs)
Pla
sm
a C
on
c. (n
g/m
L)
1
10
100
1000
10000
0 2 4 6 8
Time (hrs)
Pla
sm
a C
on
c. (n
g/m
L)
1
10
100
1000
0 6 12 18 24
Plasma Conc. (ng/mL)
Tim
e (
hrs
)
100 mg oral dose
OC
Os
1
10
100
1000
10000
0 2 4 6 8
Time (hrs)
Pla
sm
a C
on
c. (n
g/m
L)
1
10
100
1000
10000
0 2 4 6 8
Time (hrs)
Pla
sm
a C
on
c. (n
g/m
L)
Good simulations in adult human using model refinements scaled from monkey

14
0 1 2 3 4 5
1 day
3 weeks
6 weeks
3 months
4 years
Ag
e
Intrinsic clearance (uL/min/mg protein)
Development of metabolism with age
Integration of age dependencies
0
100
200
300
400
500
600
700
1-2
days
2-4
wks
2 mo
6 mo
1 yr
2 yr
6 yr
12 yr
PA
H C
leara
nce (
mL
/min
/1.7
m2)
0
20
40
60
80
100
120
140
160
GF
R (
mL
/min
/1.7
m2)
Maturation of renal function
1
10
100
1000
10000
100000
0 2 4 6 8
Time (hrs)
Pla
sma
Con
c. (n
g/m
L)
Simulation/Verification in newborn marmoset
Development of body and organ size with age

15
Simulated tissue concentration verification
Liver/plasma ratio difference with age is driven by balance of metabolism and release from liver
Terminal liver concentrations of Os and OC provided further verification of the hepatic disposition model

16
Development of esterases in human
Yang, D. et al, Human carboxylesterases HCE1 and HCE2: Ontogenic expression, inter-individual variability and differential hydrolysis of oseltamivir, aspirin, deltamethrin and permethrin. Biochemical pharmacology, 2009. 7(7): p. 238 – 247.
Shi, D., et al. Surged expression of carboxylesterase-1 (CES1) during the neonatal stage and significance in the activation of the anti-influenza pro-drug oseltamivir. J Infect Dis. 2011 Apr 1;203(7):937-42
Tamiflu cleavage is approx. 10-fold reduced in human newborns – similar to marmosets

17
Simulation of oral dosing in infants
A dose of 3 mg/kg b.i.d. given to infants of < 2 years
0
1
10
100
1000
36 41 46 51 56
Time (hrs)
Pla
sm
a C
on
c. (n
g/m
L)
.
AUC12 for OC
(ng.hr/mL)
Reported 4326 +/- 1878
Simulated 5700
Acosta, Edward P., P. Jester, P. Gal, J. Wimmer, J. Wade, Richard J. Whitley, and David W. Kimberlin, Oseltamivir Dosing for Influenza Infection in Premature Neonates. The Journal of Infectious Diseases, 2010. 202(4): p. 563-566.
The simulated steady state AUC is within the reported range

18
Simulation of oral dosing in newborns
A dose of 1.73 mg/kg b.i.d. given to premature neonates
1
10
100
1000
10000
96 108 120
Time (hrs)
Pla
sm
a C
on
c. (n
g/m
L) AUC12 for OC
(ng.hr/mL)
Reported 9250
Simulated 23000
The simulated steady state AUC approx 2x the reported value
Acosta, Edward P., P. Jester, P. Gal, J. Wimmer, J. Wade, Richard J. Whitley, and David W. Kimberlin, Oseltamivir Dosing for Influenza Infection in Premature Neonates. The Journal of Infectious Diseases, 2010. 202(4): p. 563-566.

19
• PBPK model simulations were verified sequentially in adult marmoset, adult human and newborn marmosets
• Simulations in human newborns were in line with the limited available clinical data
• Slow IV infusion produces plasma profiles of OC close to those of oral dosing while levels of Os are approx. 3-fold increased
Conclusions
In view of safety margins IV doses are not expected to have higher safety risk than the oral dose

20
• The modeling and simulation work was documented in a comprehensive report including an overview of all available non-clinical and clinical safety data
• The comprehensive report also stressed the technical feasibility & ethical concerns of a repeated dose toxicological study in newborn marmosets
• The report was submitted to the EMEA rapporteur
Impact
EMA withdrew request for the IV tox. study and accepted existing data and M&S as sufficient to support IV use in infants < 1 year

21
Acknowledgements

Doing now what patients need next