practical lessons to develop an stp and acs - jonathan hayden, browne jacobson
TRANSCRIPT
Practical lessons to develop an STP and ACSNew care models, ACSs and ACOs and supporting theirdevelopment through contracts –Jonathan Hayden, Browne Jacobson
New Care Models, ACSs andACOs and supporting theirdevelopment through contracts
Jonathan Hayden, Browne Jacobson29 November 2017
What contractual structures mightunderpin an ACS / ACO• It depends where you are in your development and
what you are trying to achieve …• Important that the structure supports the proposed
new ways of working - form should follow function- but must work within the statutory framework
• Likely to be different options for your structure –and you need to decide which is the mostappropriate / achievable for you
What contractual structures mightunderpin an ACS?
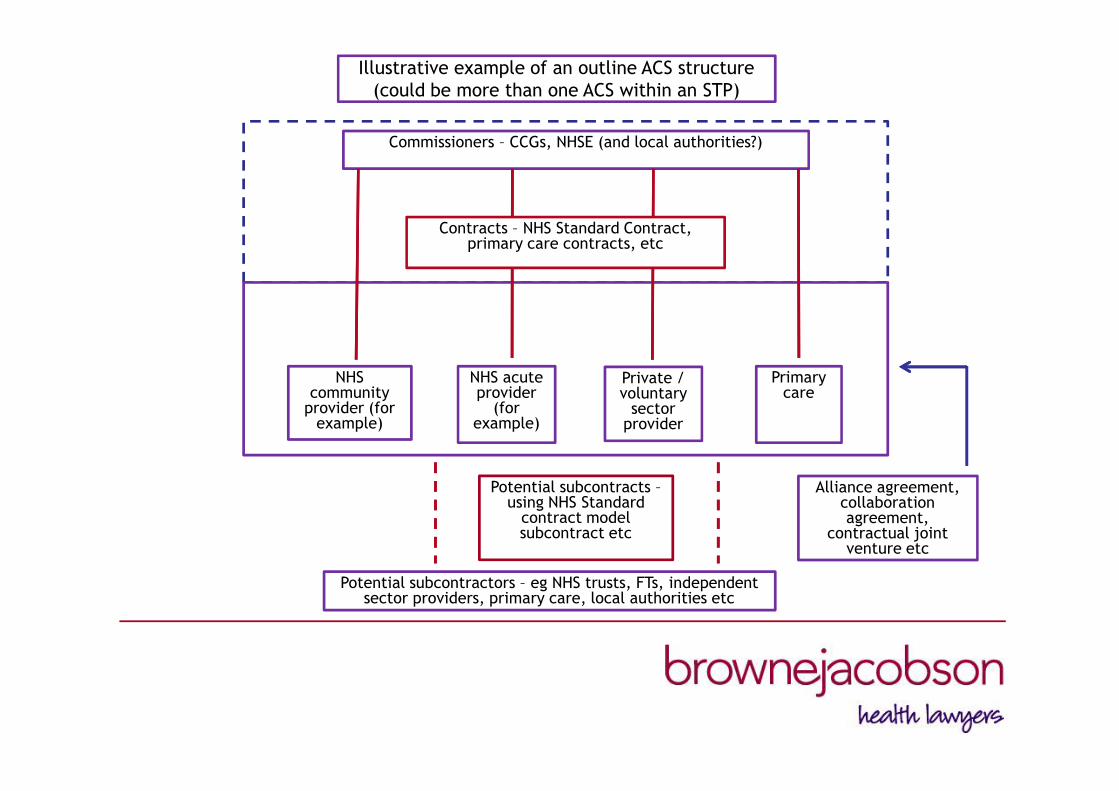
Illustrative example of an outline ACS structure(could be more than one ACS within an STP)
Potential subcontractors – eg NHS trusts, FTs, independentsector providers, primary care, local authorities etc
Potential subcontracts –using NHS Standard
contract modelsubcontract etc
Commissioners – CCGs, NHSE (and local authorities?)
NHScommunity
provider (forexample)
NHS acuteprovider
(forexample)
Private /voluntary
sectorprovider
Primarycare
Alliance agreement,collaborationagreement,
contractual jointventure etc
Contracts – NHS Standard Contract,primary care contracts, etc
What contractual structures mightunderpin an ACS• Examples of what might underpin an ACS:
– Contracts between commissioner(s) and eachprovider in the ACS – for healthcare services, NHSStandard Contracts, primary care contracts etc
– Agreement across the ACS participants – perhaps analliance agreement, collaboration agreement etc
– Other agreements / subcontracts between ACSparticipants or with others
What contractual structures mightunderpin an ACS• Examples of what might underpin an ACS (cont):
– Section 75 agreements?– Governance / decision making structure
will need to work within statutory constraints – detailsfor this may be included in the alliance agreement etc
– Risk share arrangement may be included in the alliance agreement etc
What contractual structures mightunderpin an ACO?
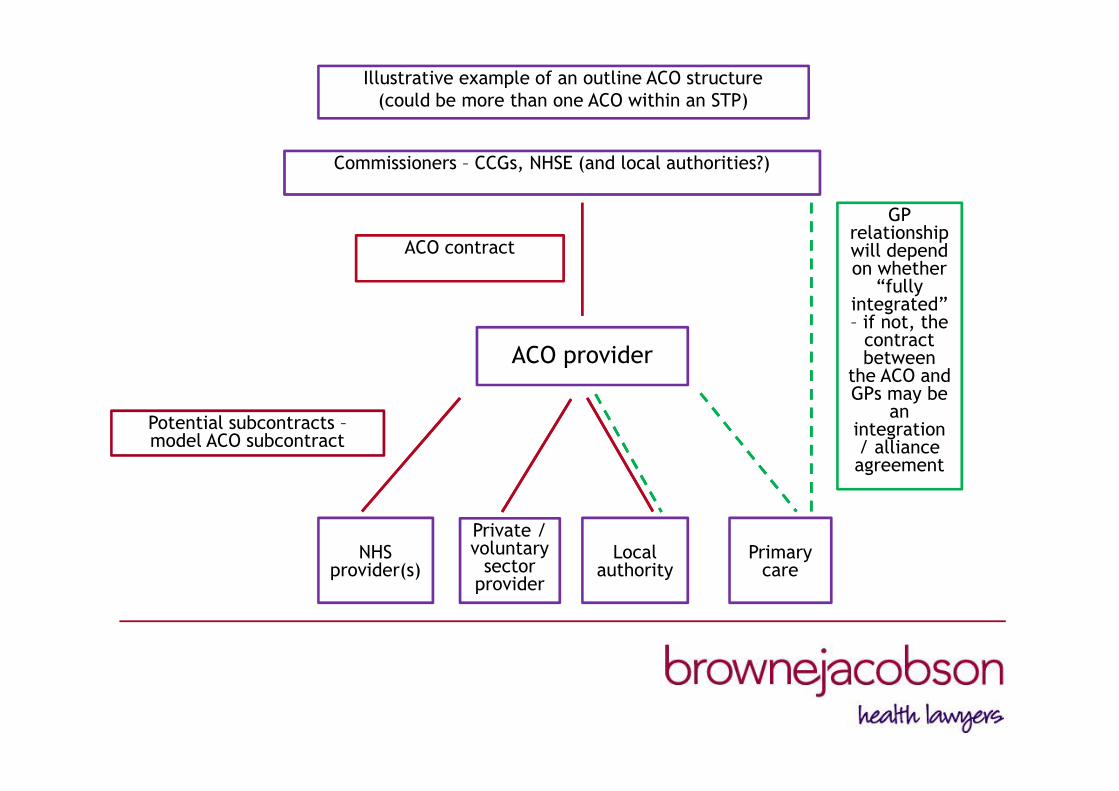
Illustrative example of an outline ACO structure(could be more than one ACO within an STP)
Commissioners – CCGs, NHSE (and local authorities?)
ACO provider
ACO contract
Potential subcontracts –model ACO subcontract
NHSprovider(s)
Private /voluntary
sectorprovider
Localauthority
Primarycare
GPrelationshipwill dependon whether
“fullyintegrated”– if not, the
contractbetween
the ACO andGPs may be
anintegration/ allianceagreement
What contractual structures mightunderpin an ACO• Examples of what might underpin an ACO:
– Contract with the ACO – likely to be the ACOcontract (subject to ISAP - Joint NHSE / NHSIassurance process for novel contract awards)
– Subcontracts between the ACO and other providers(level of subcontracting will depend on scale ofservices ACO will itself provide)

What contractual structures mightunderpin an ACO• Examples of what might underpin an ACO:
– Integration agreement eg with primary care (if not fully integrated) or
perhaps with local authority(ies)?
– Risk share arrangement Likely to be in the ACO contract or contracts with
other providers
Implementation – hints and tips• Try to keep it simple
– Work out where you are, noting that you mayalready have some excellent building blocks
– Try to avoid overlaying more structures, committeesetc – can you work with / tailor what you’ve got inplace already?
– Adopt a structure you can easily explain /understand - there will be complexities, but makesure you have a simple overall structure

Implementation – hints and tips• Make sure you understand the law• If you understand the legal opportunities and
constraints you can more easily identify andmanage the related risks
• Key areas to consider include:– Governance - decision making / delegation within
the current legal structure– Consultation / engagement
Implementation – hints and tips• Key areas to consider include (cont):
– Integrated Support and Assurance Process (ISAP) Joint NHSE / NHSI assurance process Does it apply? What impact may it have on timescales? Note revised guidance issued this Autumn

Implementation – hints and tips• Key areas to consider include (cont):
– Procurement Do the Public Contracts Regulations 2015 and/or the
NHS Procurement Patient Choice & CompetitionRegulations 2013 apply?
Where a competitive procurement is necessary,consider:
– the appropriate form of process– realistic timescales– project resource
Implementation – hints and tips• Key areas to consider include (cont):
Even at pre-procurement stage be mindful ofcomplying with the principles of:
– equal treatment– non-discrimination– transparency and proportionality
maintain a level playing field for bidders– additional complexity where bidders are required to
secure integration agreements with primary care

Implementation – hints and tips• Key areas to consider include (cont):
– Conflicts Ensuring clinical input but with conflicts managed Remember local authorities may be commissioners and
providers of relevant services Don’t forget potential for non-clinical conflicts
– HR– Pensions
Implementation – hints and tips• Key areas to consider include (cont):
– Choice– Inequalities– Competition / merger control
More of an issue for providers but, if issues arise, itcan impact on commissioners / procurements too
Don’t ignore – much better to be aware of the issues /risks and take steps to minimise them
Implementation – hints and tips• Key areas to consider include (cont):
– Information governance Especially in light of GDPR
– Tax / VAT Don’t make assumptions about tax treatment – esp
VAT - take advice early
– Wider commercial / finance support
Implementation – hints and tips• Access national / New Business Models resources –
for example, the ACO contract package and relatedresources / guidance:
Alliance agreement Integration agreement Finance / incentives / whole population budgets GP participation Procurement Pensions
www.england.nhs.uk/new-business-models

Get in touch
• Jonathan Hayden, Commercial Health Partner
– [email protected]– 0121 237 4551– 07825 616292